
Abstract
Background:
Association among generalized ligamentous laxity (GLL), hip microinstability, and patient-reported outcomes (PROs) after hip arthroscopy has yet to be completely established.
Purposes:
(1) To report minimum 2-year PROs in patients with GLL who underwent hip arthroscopy in the setting of symptomatic labral tears and femoroacetabular impingement syndrome and (2) to compare clinical results with a matched-pair control group without GLL.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Data from a prospectively collected database were retrospectively reviewed between August 2014 and December 2016. Patients were considered eligible if they received primary arthroscopic treatment for symptomatic labral tears and femoroacetabular impingement. Inclusion criteria included preoperative and minimum 2-year follow-up scores for the following PROs: modified Harris Hip Score (mHHS), Non-arthritic Hip Score (NAHS), and visual analog scale for pain (VAS). From the sample population, 2 groups were created: the GLL group (Beighton score ≥4) and the control group (Beighton score <4). Patients were matched in a 1:2 ratio via propensity score matching according to age, sex, body mass index, Tönnis grade, and preoperative lateral center-edge angle. Patient acceptable symptomatic state (PASS) and minimal clinically important difference (MCID) for mHHS, Hip Outcome Score–Sports Specific Scale (HOS-SSS), and International Hip Outcome Tool–12 (iHOT-12) were calculated.
Results:
A total of 57 patients with GLL were matched to 88 control patients. Age, sex, body mass index, and follow-up times were not different between groups (P > .05). Preoperative radiographic measurements demonstrated no difference between groups. Intraoperative findings and procedures between groups were similar except for capsular treatment, with the GLL group receiving a greater percentage of capsular plications (P = .04). At minimum 2-year follow-up, both groups showed significant improvement in PROs and VAS (P < .001). Furthermore, the postoperative PROs at minimum 2-year follow-up and the magnitude of improvement (delta value) were similar between groups for mHHS, NAHS, HOS-SSS, and VAS (P > .05). Moreover, groups reached comparable rates of MCID and PASS for mHHS, HOS-SSS, and iHOT-12.
Conclusion:
Patients with GLL after hip arthroscopy for symptomatic femoroacetabular impingement and labral tears may expect favorable outcomes with appropriate labral and capsular management at minimum 2-year follow-up. When compared with a pair-matched control group without GLL, results were comparable for mHHS, NAHS, HOS-SSS, and VAS and reached PASS and/or MCID for mHHS, HOS-SSS, and iHOT-12.
Keywords
Historically, the hip joint has been considered an inherently stable joint, with bony deficiency or hip dysplasia being a clear reason for instability.48,49,84 However, features of microstability may be present even in the presence of appropriate acetabular coverage. 37 The concept of microinstability, defined as extraphysiologic hip motion as a consequence of bony deficiency and/or soft tissue damage or loss, has evolved from an abstract notion to a recognized source of symptoms in the hip.72,74 A relationship between generalized ligamentous laxity (GLL) and its potential causation of hip micro-instability has been proposed.30,36 GLL, defined as more-than-normal range of movement and usually measured with the Beighton score, 58 has been linked to several musculoskeletal injuries in knees and shoulders.9,34,39,41,82 Bin Abd Razak et al 6 reported >3-times higher likelihood of such musculoskeletal injuries in patients with GLL. On the basis of a cohort of 1381 patients, Saadat et al 71 recently reported the prevalence of GLL (Beighton score ≥4) in patients who underwent hip arthroscopy surgery, and they found that 18.9% were in fact patients with GLL.
In hip arthroscopy, the importance of capsule management has been increasingly acknowledged and may be critical in high-risk patients with GLL and/or features of some degree of acetabular dysplasia.2,19,32,49,62 Arthroscopic capsular plication has been described as an effective procedure to address microinstability in the hip.13,23,80 Regarding GLL and outcomes after hip arthroscopy, there is a paucity in the current literature, with only a few studies reporting favorable results, most of which are limited by small series and relative short-term follow-up.43,67,75
The purposes of the current study were (1) to report minimum 2-year patient-reported outcomes (PROs) in patients with GLL who underwent hip arthroscopy in the setting of symptomatic labral tears and femoroacetabular impingement syndrome (FAI) and (2) to compare clinical results with a matched-pair control group without GLL.
We hypothesized that (1) patients with GLL would experience favorable PROs at minimum 2-year follow-up and (2) clinical results in this group would be similar to those of a pair-matched control group without GLL.
Methods
Patient Selection
Data from a prospectively collected database at the American Hip Institute Hip Preservation Registry were retrospectively reviewed for patients who underwent hip arthroscopy between August 2014 and December 2016. All patients were considered eligible if they received primary arthroscopic treatment for labral tears in the setting of FAI and labral tears during this period. GLL was defined as Beighton score ≥4. 71 Patients were included if they had preoperative scores and minimum 2-year follow-up scores for the following PROs: modified Harris Hip Score (mHHS), 1 Non-arthritic Hip Score (NAHS), 15 and visual analog scale for pain (VAS). 12 Patients were excluded from analysis if they had a diagnosed ipsilateral hip condition (eg, avascular necrosis, Legg-Calvé-Perthes disease, or slipped capital femoral epiphysis), had concomitant surgery, underwent previous hip surgery, had a lateral center-edge angle (LCEA) <25°, 55 had workers’ compensation status, or had an unavailable Beighton score.
Participation in the American Hip Institute Hip Preservation Registry
While the present study represents a unique analysis, data on some patients in this study may have been reported in other studies.14,64,71 All data collection received institutional review board approval (ID No. 5276).
Physical Examination
The senior surgeon (B.G.D.) performed a comprehensive physical examination on all patients during their preoperative clinic appointments. 52 This evaluation included assessment of the patient’s gait, as well as the hip’s range of motion—internal rotation, external rotation, flexion, abduction, and adduction—as measured with the patient in the supine position. Hips were also evaluated with anterior, lateral, and posterior impingement tests, as well as for the presence of painful internal snapping with the hip flexed, abducted, and externally rotated. Additionally, the Beighton score was used preoperatively by the senior surgeon to assess ligamentous laxity.5,51,71
Radiographic Imaging
A series of radiographic images were requested before surgery, including the standing and supine anteroposterior pelvis, modified 45° Dunn, and false-profile view.16,25,57,77 Evaluations of these images were performed with General Electric Healthcare’s Picture Archiving and Communication System.
The anteroposterior supine view was used to assess the following: the LCEA of Wiberg 83 as modified by Ogata et al, 61 the level of osteoarthritis as graded with the Tönnis system, 20 acetabular version as measured by the presence of crossover, and ischial spine and posterior wall signs. 45 Cam deformity was assessed on the 45° Dunn lateral view by measuring the alpha angle and the head-neck offset and defined as an alpha angle >55°.50,66 Anterior center-edge angle of Lequesne and de Seze 44 was measured on the false-profile view. The institution’s radiographic measurements demonstrated good interobserver reliability in previously published studies.22,69,70 Additionally, labral tears and other potential extra- and intra-articular defects were determined using magnetic resonance arthrography for all patients.
Surgical Indication and Technique
Patients were recommended arthroscopic surgery if radiographic imaging, history, and physical examination indicated evidence of FAI or labral tears. Specifically, patients experiencing moderate to severe pain were required to undergo at least 3 months of nonsurgical treatment, including physical therapy, nonsteroidal anti-inflammatory drugs, and activity modification. Patients were then recommended for surgery if the 3 months of nonoperative treatment failed.8,28
All arthroscopies were performed by the senior author (B.G.D.). During surgery, patients were situated in the modified supine position.17,40 A well-padded perineal post was used to aid in hip joint distraction. The anterolateral portal was created under fluoroscopic guidance to vent the joint and was followed by the midanterior and interportal capsulotomy under direct visualization. 46 A diagnostic arthroscopy was undertaken to make a full assessment of the hip joint. Ligamentum teres damage was graded using the Domb and Villar classifications.7,27 Labral tears were measured and graded using the Seldes classification system. 73 The chondrolabral junction damage was graded using acetabular labrum articular disruption, while acetabular or femoral head chondral damage was recorded using the Outerbridge classifications.54,63,76
Procedures were undertaken according to the intraoperative findings of hip pathology. Labral tears were debrided, repaired, or reconstructed on the basis of the size of the labrum, the extent of tearing, and the morphology/quality of the labrum.21,47 Acetabuloplasty and femoral osteoplasty were performed under fluoroscopic guidance to treat pincer- and cam-type impingement, respectively.50,68 Capsular plication was performed in all patients except those with excessive stiffness, adhesive capsulitis, or insufficient capsular tissue.13,23 The technique for capsular plication was performed with the hip flexed to 45° and using absorbable sutures (2.0 coated Vicryl, polyglactin 910; Ethicon) and the 70° SlingShot Suture Manager (Pivot Medical, Inc).
One by one, 4 to 6 sutures were passed from the midanterior portal through the acetabular capsular side and retrieved from the distal anterolateral accessory portal through the capsular femoral side. All sutures were passed first from medial to lateral and tied in the same order. Preoperative characteristics, such as age, sex, body mass index (BMI), occupation, and desired activity level, also went into this multifactorial algorithm.
Rehabilitation Protocol
The postoperative protocol was tailored to accommodate recovery on the basis of the procedures performed, ranging from 2 to 8 weeks of recovery. All patients wore a brace for stability (DJO Global) and were limited to 20 lb (9 kg) of foot-flat weightbearing activity with crutches. Daily stationary bicycle usage was recommended for a total of 8 weeks postoperatively. Physical therapy began as early as 1 day after surgery.
Surgical Outcome Tools and Survivorship
Patients were prospectively assessed preoperatively, 3 months postoperatively, and annually thereafter using questionnaires to assess their outcomes. Patients completed the mHHS, NAHS, Hip Outcome Score–Sports Specific Scale (HOS-SSS), 53 and VAS outcome questionnaires pre- and postoperatively. Additionally, latest follow-up findings of the International Hip Outcome Tool–12 (iHOT-12), the Veterans RAND 12-Item Health Survey Physical Component Summary and Mental Component Summary, and the 12-Item Short Form Health Survey (SF-12) (Physical Component Summary and Mental Component Summary) were recorded. 29 Postoperative patient satisfaction on a scale from 0 to 10 and surgical complications were also recorded. The percentage of patients achieving the patient acceptable symptomatic state (PASS) and minimal clinically important difference (MCID) was found for the mHHS (PASS, ≥74 points; MCID, delta [Δ] ≥8 points)20,21 and the HOS-SSS 10 (PASS, ≥65 points; MCID, Δ≥6 points). Additionally, the PASS of iHOT-12 (≥63 points) was calculated. 60
Revision arthroscopic surgery was recorded for patients. Kaplan-Meier analysis was used to depict survivorship of the cohort, and comparisons were made using the log-rank test.
Statistical Analysis
Patients were matched on the logit of the propensity score via a nearest-neighbor (Euclidean distance) match algorithm. Matching was performed without replacement in a 1:2 ratio, and a strict caliper of 0.2 times the standard deviation of the logit propensity scores was used. Patients who were outside the caliper (“propensity range”) were removed from consideration.3,4 The covariates were age at surgery, sex, BMI, Tönnis grade, and preoperative LCEA. Descriptive statistics were reported for patient characteristics, intraoperative findings, procedures performed, radiographic measurements, and PROs. A statistically significant difference was noted if P < .05. Continuous variables were reported in mean and standard deviations accompanied by 95% CIs. Parametricity and variance were assessed using the Shapiro-Wilk test and the F test, respectively. Normally distributed samples with equal variances were analyzed using a 2-tailed t test, whereas nonparametric data were compared using a nonparametric equivalent test. Chi-square (χ2) or Fisher exact test was used for all categorical variables. Based on the assumption that a mean difference of 8 points in follow-up mHHS between groups was clinically important, an a priori power analysis was used to determine that in a 1:2 matching ratio, 13 GLL cases and 26 control cases were necessary to achieve at least 80% power. 65 Statistical analysis was performed in Python (Version 3.7; Python Software Foundation) and R (Version 3.6.0; R Foundation).
Results
Patient Characteristics
During the study period, 275 patients satisfied the inclusion criteria, of whom 234 had adequate follow-up (85.1%). The patient selection flowchart is depicted in Figure 1. Of the 234 patients, 72 had a Beighton score ≥4. Patients with GLL were matched in a 1:2 ratio to those without GLL (control). Given the strict caliper, 57 patients with GLL were matched to 88 control patients. Characteristic data are presented in Table 1. The matched groups showed no significant differences in sex, age, BMI, Tönnis grade, and follow-up time (P > .05). Mean Beighton scores for the GLL and control groups were 5.68 and 0.96, respectively.
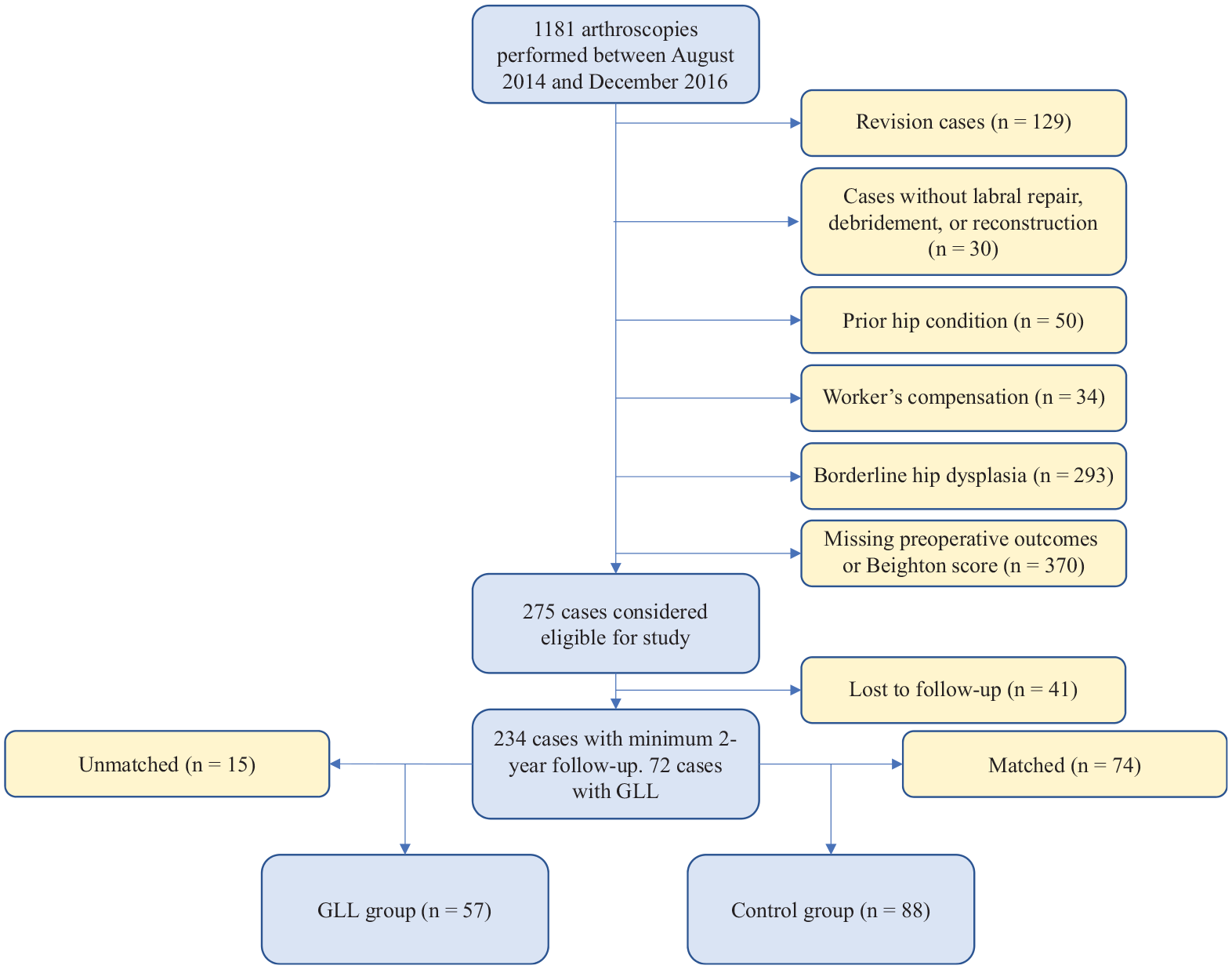
Patient selection flowchart. GLL, generalized ligamentous laxity.
Characteristics of the GLL and Control Groups After Propensity Score Matching a
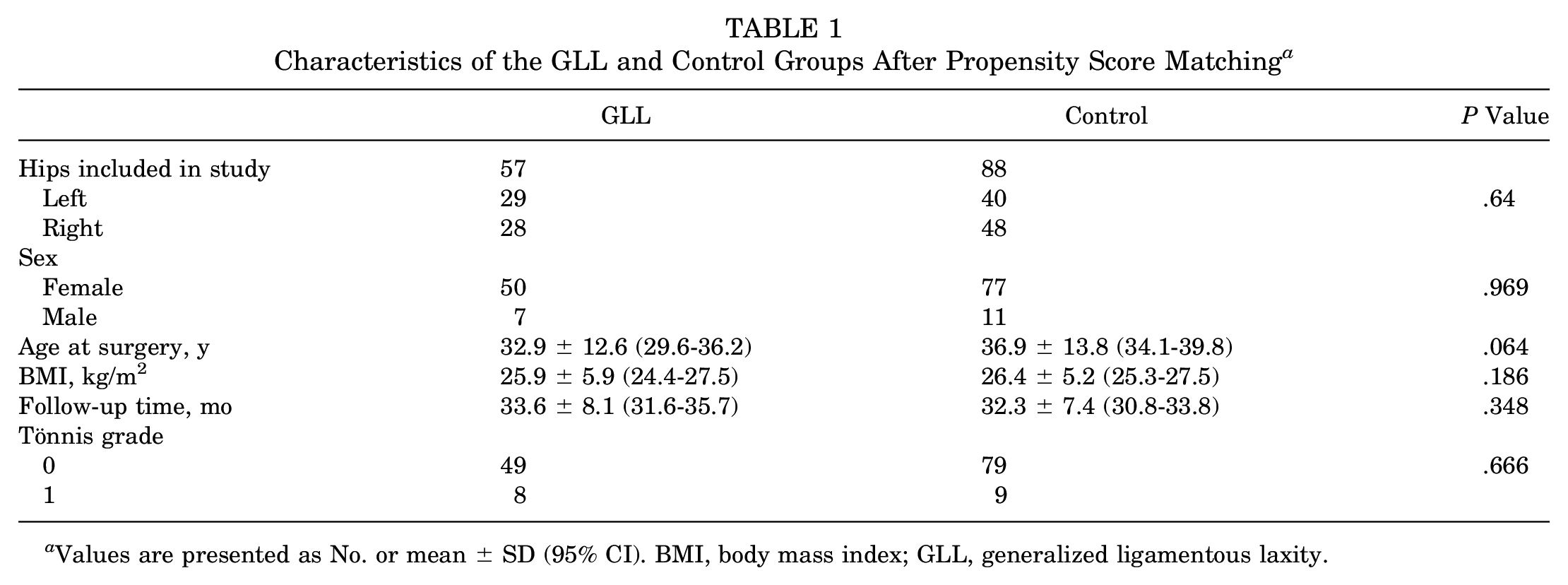
Values are presented as No. or mean ± SD (95% CI). BMI, body mass index; GLL, generalized ligamentous laxity.
Intraoperative Findings and Procedures
Intraoperative diagnostic data, presented in Table 2, demonstrated no difference between groups in labral tear type, acetabular or femoral head cartilage damage, or ligamentum teres injuries (P > .05). The procedures performed between groups were similar, with the exception of capsular treatment. A greater percentage of patients in the GLL group received capsular plications (P = .04) (Table 3).
Intraoperative Findings of the GLL and Control Groups After Propensity Score Matching a
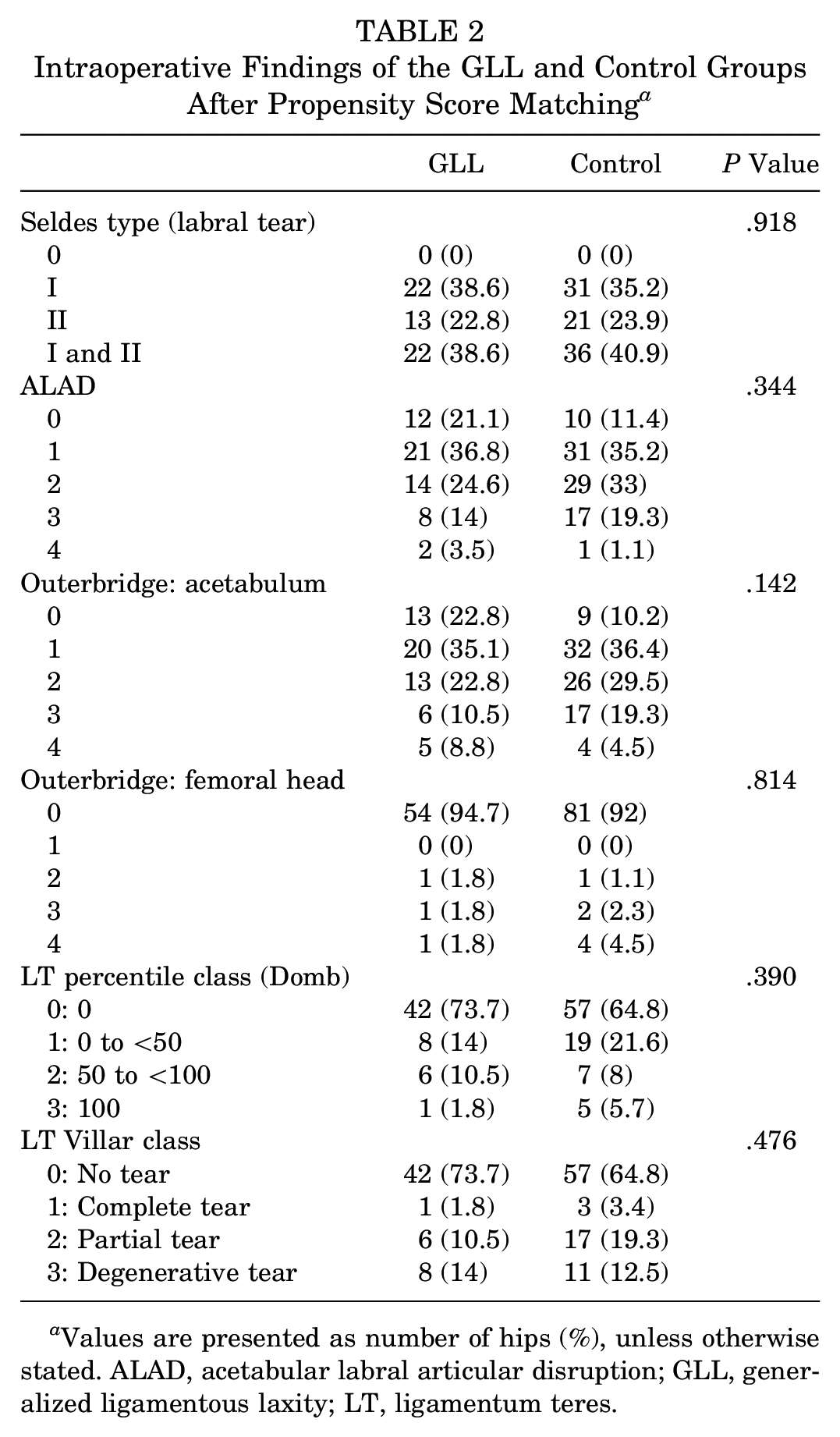
Values are presented as number of hips (%), unless otherwise stated. ALAD, acetabular labral articular disruption; GLL, generalized ligamentous laxity; LT, ligamentum teres.
Intra-articular Procedures of the GLL and Control Groups After Propensity Score Matching
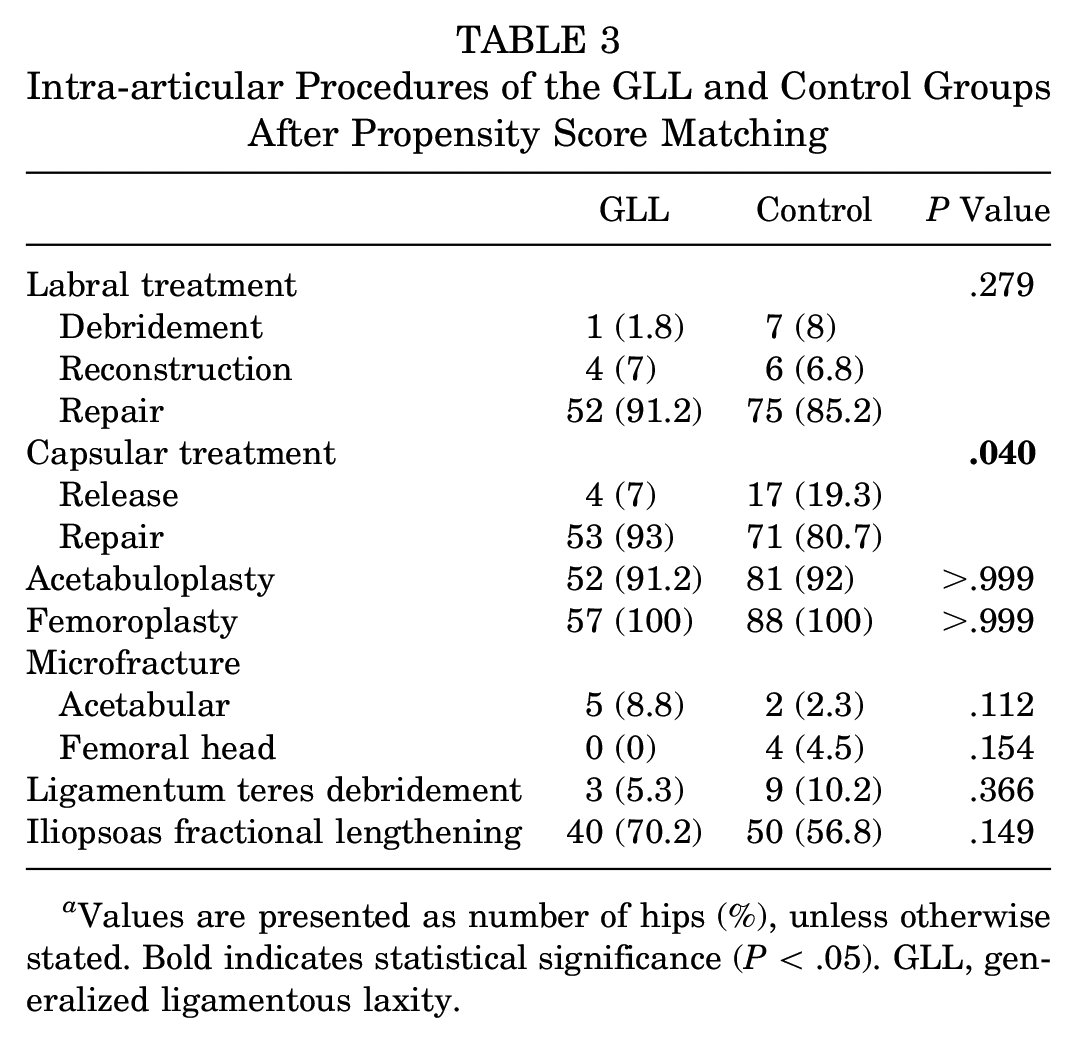
Values are presented as number of hips (%), unless otherwise stated. Bold indicates statistical significance (P < .05). GLL, generalized ligamentous laxity.
Radiographic Findings
There were no significant differences between the groups in pre- or postoperative radiographic measurements (Table 4). Both groups showed significant reductions in alpha angle (P < .001).
Radiographic Findings of the GLL and Control Groups After Propensity Score Matching a
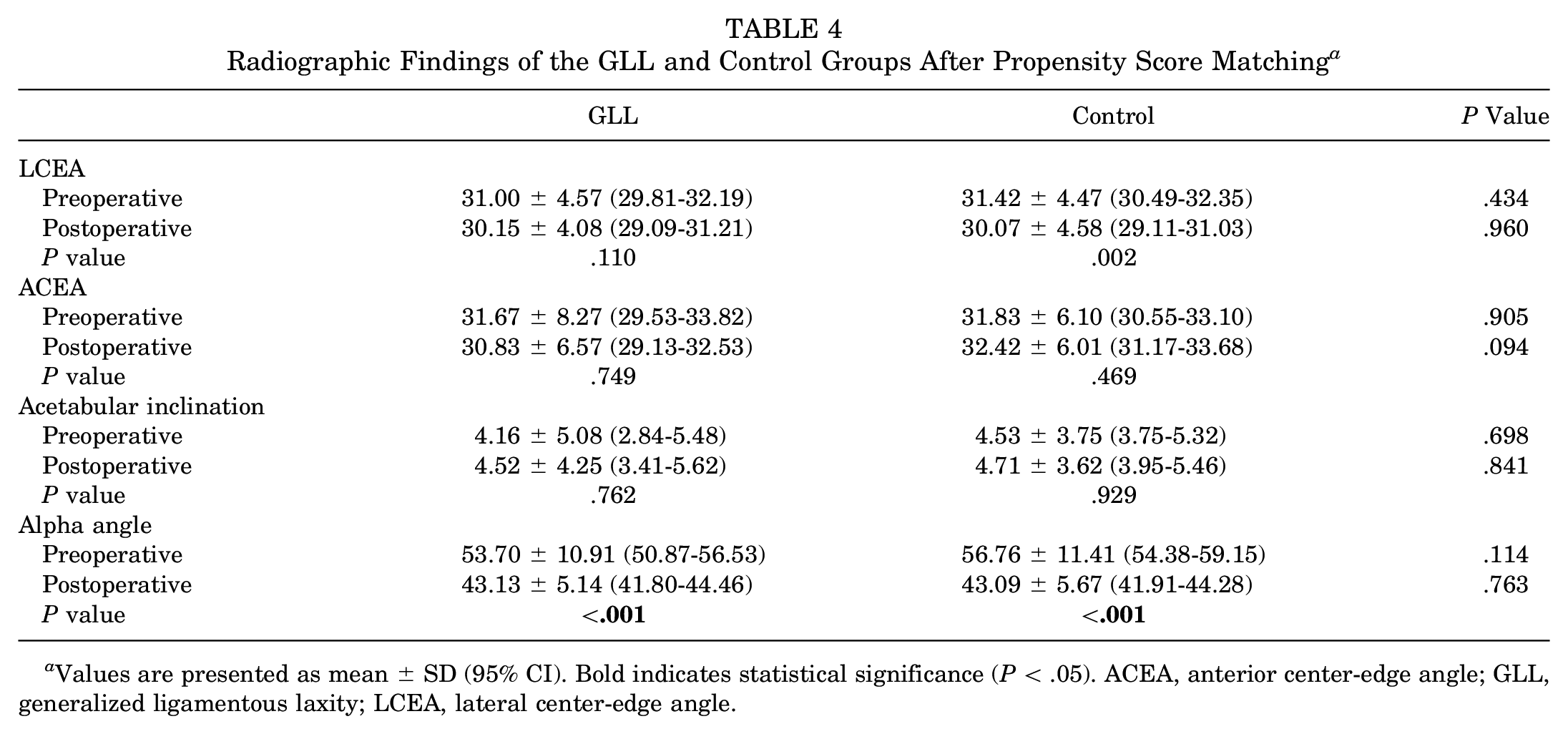
Values are presented as mean ± SD (95% CI). Bold indicates statistical significance (P < .05). ACEA, anterior center-edge angle; GLL, generalized ligamentous laxity; LCEA, lateral center-edge angle.
Surgical Outcomes
Pre- and postoperative recorded outcomes are presented in Table 5. Both groups reported significant increases for mHHS, NAHS, HOS-SSS, and VAS from baseline to minimum 2-year follow-up (P < .001). The minimum 2-year outcomescores showed no differences between the groups (P > .05). Similarly, the magnitude of improvement (Δ value) was comparable between groups (P > .05) (Figure 2).
Baseline and Minimum 2-Year Patient-Reported Outcomes of the GLL and Control Groups After Propensity Score Matching a
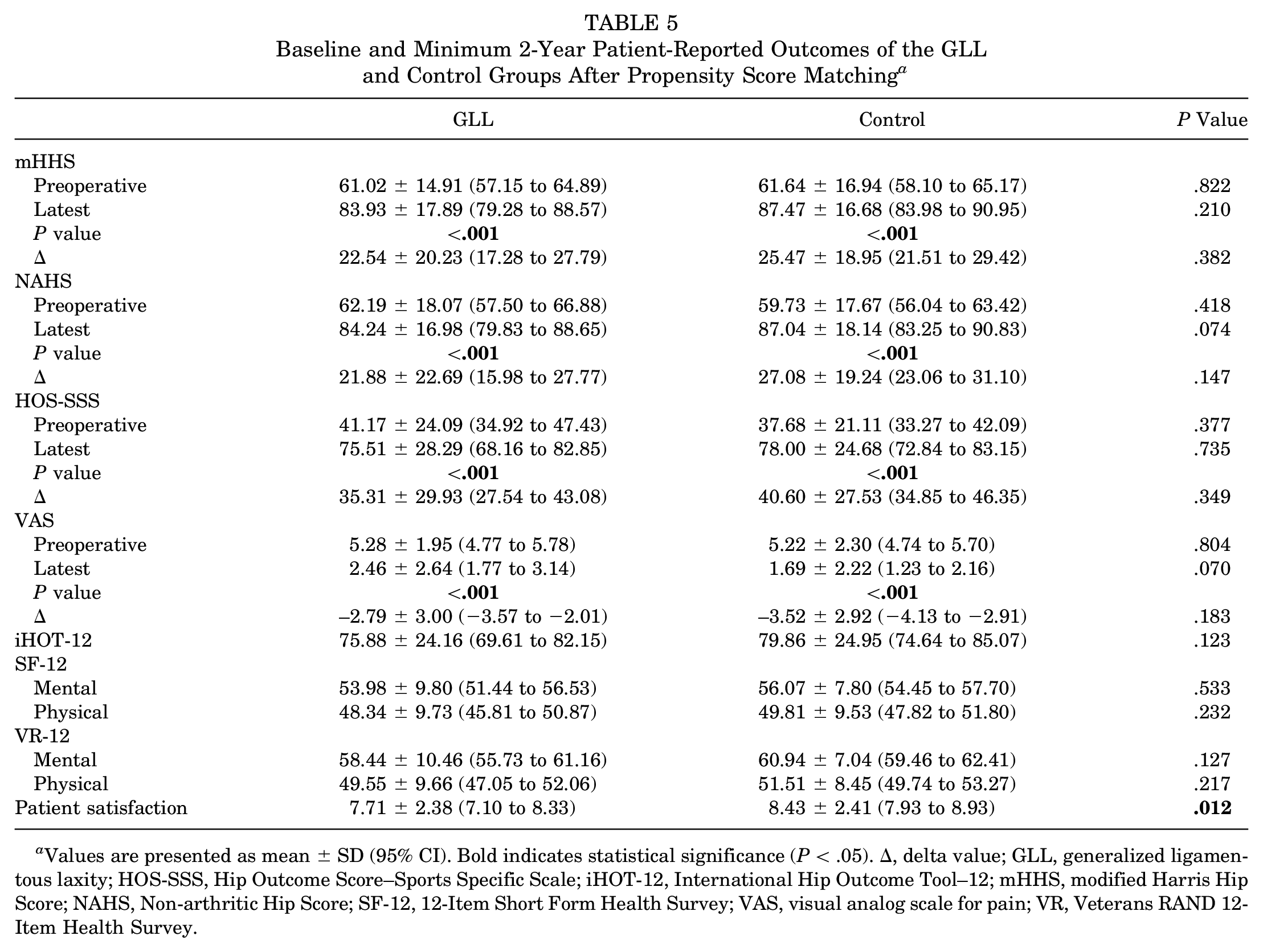
Values are presented as mean ± SD (95% CI). Bold indicates statistical significance (P < .05). Δ, delta value; GLL, generalized ligamentous laxity; HOS-SSS, Hip Outcome Score–Sports Specific Scale; iHOT-12, International Hip Outcome Tool–12; mHHS, modified Harris Hip Score; NAHS, Non-arthritic Hip Score; SF-12, 12-Item Short Form Health Survey; VAS, visual analog scale for pain; VR, Veterans RAND 12-Item Health Survey.
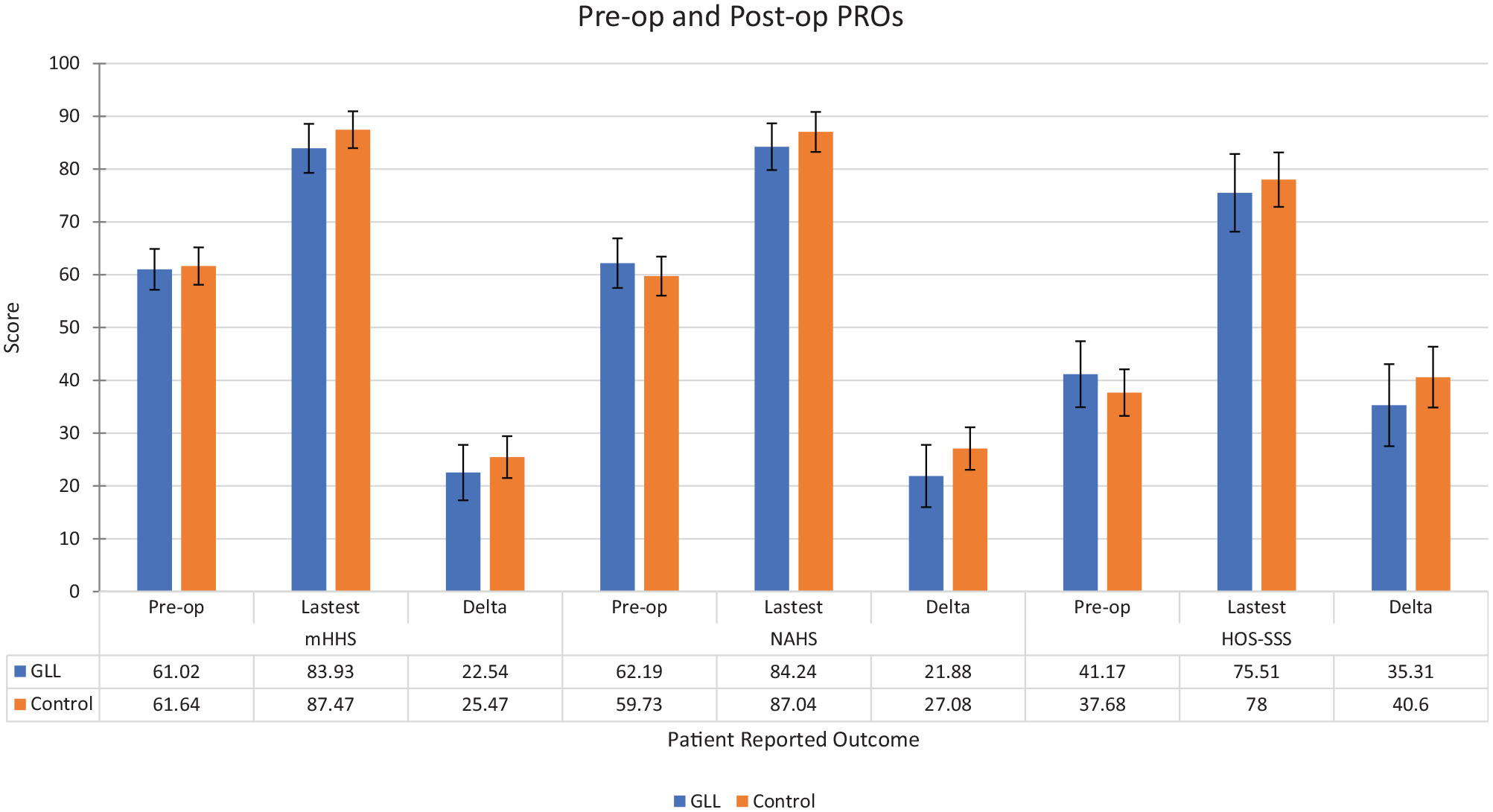
Mean preoperative (Pre-op) and postoperative (Post-op) patient-reported outcomes (PROs) and 95% CIs for the generalized ligamentous laxity (GLL) and control groups. HOS-SSS, Hip Outcome Score–Sports Specific Scale; mHHS, modified Harris Hip Score; NAHS, Non-arthritic Hip Score.
There were no differences between the groups for the following PROs: iHOT-12, Veterans RAND 12-Item Health Survey (physical and mental), and SF-12 (physical and mental health) (P > .05). However, patient satisfaction scores between the groups were significantly different (P = .012) (Table 5).
When outcomes were translated to clinical terms, both groups reached similar levels for PASS and/or MCID for mHHS, HOS-SSS, and iHOT-12 (Table 6).
MCID and PASS of the Generalized Ligamentous Laxity and Control Groups After Propensity Score Matching a
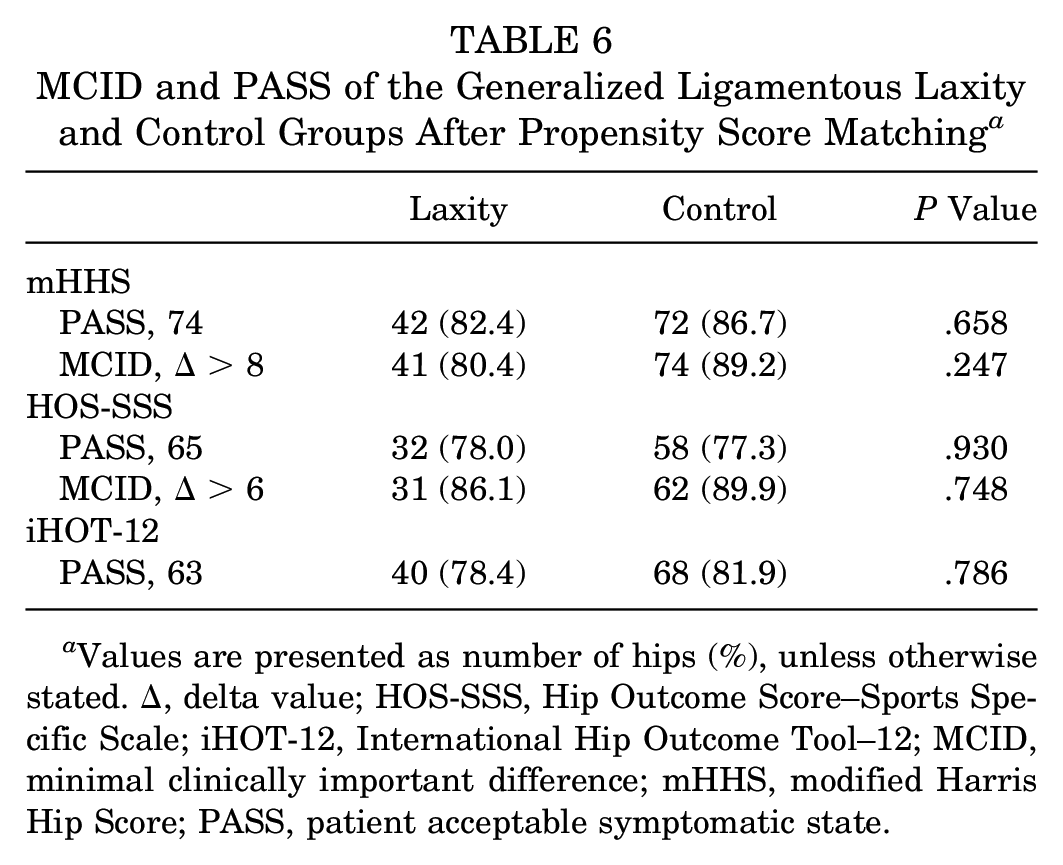
Values are presented as number of hips (%), unless otherwise stated. Δ, delta value; HOS-SSS, Hip Outcome Score–Sports Specific Scale; iHOT-12, International Hip Outcome Tool–12; MCID, minimal clinically important difference; mHHS, modified Harris Hip Score; PASS, patient acceptable symptomatic state.
Survivorship Analysis
Of the patients in the GLL group, 6 (10.5%) required a revision arthroscopy at a mean 16.35 months after findings of a retorn labrum in all 6, stiffness in 1, recalcitrant trochanteric bursitis in 1, and hip flexor tendinitis in 1. No patients with GLL converted to total hip replacement (total hip arthroplasty) at minimum 2-year follow-up. Of the patients in the control group, 4 (4.5%) required revision surgery at a mean 16.07 months, after the findings of a retorn labrum in all 4 and stiffness in 1. One (1.1%) patient in the control group converted to total hip arthroplasty at 32.12 months (Table 7). Figure 3 provides a Kaplan-Meier analysis demonstrating comparable conversions to revision arthroscopy between the groups.
Secondary Surgery of the GLL and Control Groups After Propensity Score Matching a
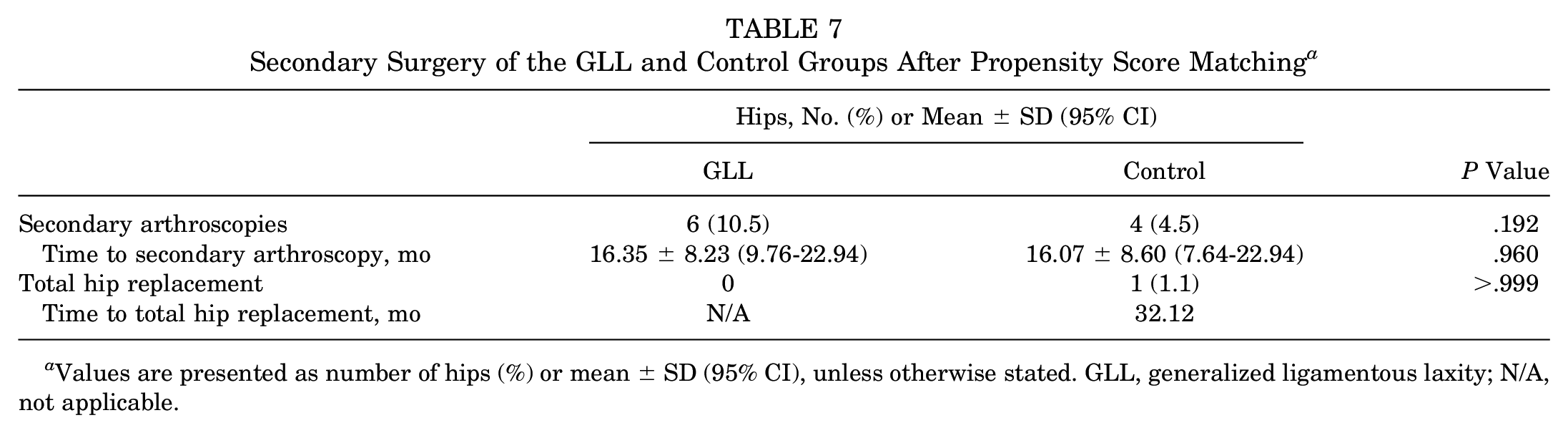
Values are presented as number of hips (%) or mean ± SD (95% CI), unless otherwise stated. GLL, generalized ligamentous laxity; N/A, not applicable.
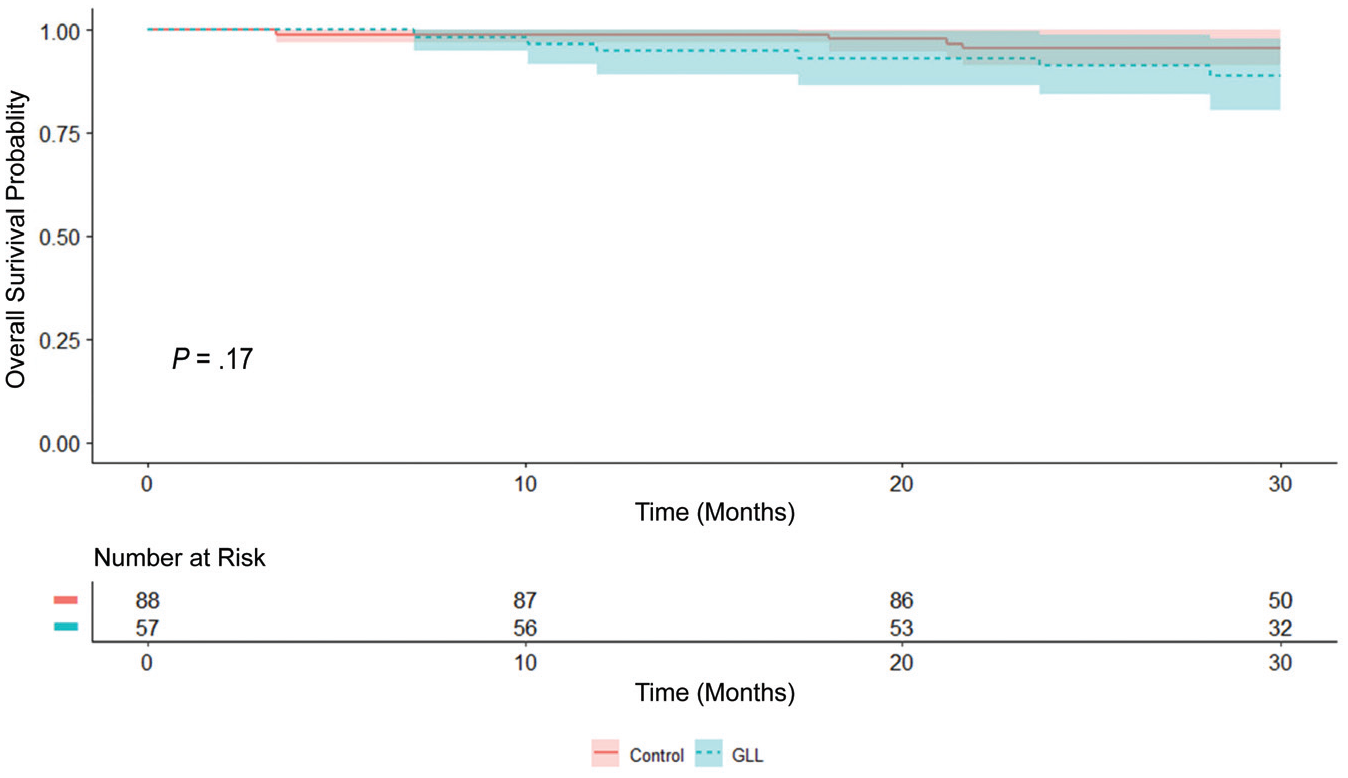
Kaplan-Meier estimate of conversion to revision arthroscopy. Curves are accompanied by 95% CIs (Greenwood). GLL, generalized ligamentous laxity.
Discussion
The present study demonstrated that patients who underwent primary hip arthroscopy in the setting of FAI, labral tears, and GLL had favorable and significant improvements in PROs and VAS from baseline to minimum 2-year follow-up (P < .001 for mHHS, NAHS, HOS-SSS, VAS). In addition, favorable findings were demonstrated for patient satisfaction. Furthermore, when these improvements were translated to a clinical point of view, patients with GLL obtained favorable results in terms of MCID and/or PASS for mHHS, HOS-SSS, and iHOT-12. When the GLL group was compared with a pair-matched control group without GLL based on age, sex, BMI, Tönnis grade, and preoperative LCEA, no differences were observed in several PROs or VAS. Furthermore, the magnitude of improvement was comparable between groups in terms of mHHS, NAHS, HOS-SSS, and VAS. Moreover, no differences were observed between groups for the following clinical parameters: PASS and MCID for mHHS and HOS-SSS and PASS for iHOT-12.
Pontiff et al 67 reported results on arthroscopic management in women with GLL (Beighton score ≥4) and FAI. The authors compared 35 women with GLL and a group of 131 woman without GLL (Beighton score <4) and observed favorable and similar scores in HOS–Activities of Daily Living and iHOT-33. However, results were limited by the fact that the follow-up of the study was only 6 months, only 2 PROs for nonarthritic hips were assessed, and the groups were not matched.
With longer follow-up, Stone et al 75 recently published their results regarding patients with GLL (Beighton score ≥4) who underwent hip arthroscopy. The authors reported similar improvement in outcomes at average 2-year follow-up to a matched control group based on Δ value for mHHS (P = .913), HOS-SSS (P = .944), HOS–Activities of Daily Living (P = .618), and VAS (P = .512). Nonetheless, data regarding baseline PROs were not provided. In addition, the GLL group was composed of just 25 patients; only female patients were included for both groups; and details regarding follow-up differences between groups were not addressed. The baseline PROs were provided in the current study, and no differences were obtained between the matched groups. As mentioned before, comparable Δ values were obtained for the same PROs between groups. Regarding latest follow-up specific to hip preservation–designed PRO results, no differences were found. The authors of the previous study 75 stated that appropriate capsular management is essential to achieve good results in GLL populations, and we agree with this concept in addition to the combination of labral function/seal restoration.2,24,59 In almost 94% of the patients, the capsule was plicated. The larger sample size, improved matching process, and longer follow-up made the results of the present study more generalizable than its predecessor. 75 Even in the presence of extreme capsular laxity (Ehlers-Danlos syndrome), meticulous capsular plication, FAI correction, and labral function restoration may lead to favorable short-term outcomes as reported by Larson et al. 43
Microinstability of the hip has evolved from an abstract concept to a recognized potential cause of pain and disability.37,72 The association between GLL and microinstability has been proposed.71,79 Trends show that capsular plication is becoming the standard in hip arthroscopy, and it is critical in high-risk populations, such as patients with GLL.18,23,26,62,81 Many cadaveric/biomechanics studies have investigated the relationship between capsular management and its role in the treatment of microinstability.35,36,80 Jackson et al 35 found that the capsular shift procedure decreased internal rotation at low flexion angles, ease of distraction, and extension based on 8 fresh-frozen cadaveric hip dissections. Johannsen et al, 36 in a study with 8 hips, created a capsular laxity model and found a significant increase in femoral rotation and femoral head displacement. The authors concluded that the anterior hip capsule plays an important role in controlling hip rotation and femoral head displacement.
Recently, Saadat et al 71 established the prevalence of GLL in patients undergoing hip arthroscopy. In a cohort of 1381 patients, there were 1120 patients with Beighton scores from 0 to 3 and 261 patients with Beighton scores ≥4 (GLL). In the GLL group, 92.7% of the patients were female. The likelihood of having GLL was almost 7 times higher for female versus male patients. This association between hip instability and sex has already been demonstrated by others.2,42,49,78 The authors also reported lower age (mean ± SD: 38.9 ± 15.2 vs 31.0 ± 13.3 years; P < .0001) and BMI (26.7 ± 5.4 vs 24.9 ± 5.1 kg/cm2; P < .0001) for the GLL group. Additionally, they found that patients with GLL had greater hip range of motion and smaller intraoperative labral size and tear dimensions. Patients with GLL were also more likely to undergo labral repair, capsular plication, and iliopsoas fractional lengthening. However, the study was a cross-sectional design with no PRO analysis presented, a task addressed with the current investigation.
Strengths
Several notable strengths of the ongoing study must be mentioned. First, this is one of the few studies to report PROs specifically for patients with GLL at minimum 2-year follow-up. Second, these results were compared with a matched-pair control group without GLL to insulate the influence of GLL on outcomes. Third, based on an a priori power analysis, the sample sizes for both groups were adequately representative to detect meaningful differences, which drastically increases generalizability of the results. Fourth, the use of several PROs that were designed to detect outcomes in active patients with nonarthritic hips limited ceiling effects and warrants generalizability of the results. 38 Fifth, as statistical significance does not equate to clinical importance, the proportion of patients who achieved the MCID and/or PASS for mHHS, HOS-SSS, iHOT-12, and VAS was also calculated. 31 Finally, while favorable outcomes have been reported with arthroscopic management of “borderline” hip dysplasia with FAI and labral tear, the potential confounding factor of any degree of dysplasia was eliminated by excluding any patients with an LCEA <25°.19,33,49
Limitations
Limitations of the current study must be acknowledged. First, this was a nonrandomized study. As such, additional confounding variables may have influenced the results. Second, although data collection was done in a prospective manner, this is a retrospective study, which introduces bias. Third, the analysis was based on the patients of a single high-volume surgeon who specializes in hip preservation surgery, which may limit the generalizability of the results. 56 Fourth, capsular treatment was not included as a variable for the matching process and could have introduced confounding bias. Fifth, the present study included minimum 2-year follow-up, although longer follow-up is required to determine durability of the results. Surgical techniques involved in our treatment of patients with and without GLL have evolved and improved over time. As a result, while the GLL and control groups contain some patients who underwent capsulotomy without repair and labral debridement, today almost all such patients would be treated with capsular plication and an alternative for labral restoration (labral reconstruction/augmentation). 11 Sixth, because revision surgery was considered an endpoint outcome, PROs for these patients were not included in the PRO analysis. Seventh, the use of the Beighton score as a unique tool to address GLL is controversial. 81 Eighth, Beighton scores were not available for the entire population; thus, these patients were excluded from analysis, resulting in a decrease of power of the study and potential bias. Ninth, GLL is not equal to microinstability 72 ; as such, the methodology of the present study was designed to address only the potential effect of GLL syndrome in patients who underwent hip arthroscopy in the setting of symptomatic labral tears and FAI. Last, dysplasia assessment based only on LCEA may be oversimplistic. 55
Conclusion
Patients with GLL after hip arthroscopy for symptomatic FAI and labral tears may expect favorable outcomes with appropriate labral and capsular management at minimum 2-year follow-up. When compared with a pair-matched control group without GLL, results were comparable for mHHS, NAHS, HOS-SSS, and VAS and reached the PASS and/or MCID for mHHS, HOS-SSS, and iHOT-12.
Footnotes
Submitted October 9, 2019; accepted February 4, 2020.
This study was performed in accordance with the ethical standards in the 1964 Declaration of Helsinki. This study was carried out in accordance with relevant regulations of the US Health Insurance Portability and Accountability Act. Details that might disclose the identity of the patients under study have been omitted. This study was approved by the institutional review board (ID 5276).
One or more of the authors has declared the following potential conflict of interest or source of funding: The American Hip Institute Research Foundation funded this research. B.G.D. has had ownership interests in Hinsdale Orthopaedics, the American Hip Institute, SCD#3, North Shore Surgical Suites, and Munster Specialty Surgery Center; has received research support from Arthrex, ATI, the Kauffman Foundation, Stryker, and Pacira Pharmaceuticals; has received consulting fees from Adventist Hinsdale Hospital, Arthrex, MAKO Surgical, Medacta, Pacira Pharmaceuticals, and Stryker; has received educational support from Arthrex, Breg, and Medwest; has received speaking fees from Arthrex and Pacira Pharmaceuticals; and receives royalties from Arthrex, DJO Global, MAKO Surgical, Stryker, and Orthomerica. B.G.D. is the medical director of hip preservation at St Alexius Medical Center and a board member for the American Hip Institute Research Foundation, AANA Learning Center Committee, the Journal of Hip Preservation Surgery, and the Journal of Arthroscopy. A.C.L. has received educational support from Medwest and Smith & Nephew; research support from Arthrex and Stryker; food and beverage from Smith & Nephew, Stryker, Zimmer Biomet, and Arthrex; travel and lodging from Stryker and Arthrex; and consulting fees from Arthrex and Graymont Medical. D.R.M., J.S., and P.J.R. have received hospitality payments from Arthrex, Stryker, and Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.