
Abstract
Background:
Arthroscopic anterior cruciate ligament (ACL) reconstruction (ACLR) with a bone–patellar tendon–bone graft (BTB) is a reliable surgical option for the control of anterior knee laxity after ACL injury. The addition of a lateral extra-articular tenodesis (LET) may improve control of rotation knee laxity and improve short-term graft survival in high-risk patients.
Purpose:
The aims of this study were to compare long-term patient-reported outcomes, graft survival, and risk of osteoarthritis between ACLR with and without LET.
Study Design:
Randomized controlled trial; Level of evidence, 2.
Methods:
This study included 121 consecutive knees (120 patients) presenting to a single center with an ACL rupture between 1998 and 1999. In total, 61 knees were randomized to an isolated BTB ACLR, and 60 knees were randomized to a BTB ACLR with an extra-articular lateral tenodesis with gracilis tendon (modified Lemaire).
Results:
Eighty knees in 79 patients (66%) were available for follow-up at a postoperative mean of 19.4 years (range, 19-20.2). Of those patients, 43 had a clinical examination and completed patient-reported outcome questionnaires, and the other 37 patients were evaluated through the questionnaires alone. Standard radiographs were available for 45 patients and laximetry (TELOS) for 42 patients. Mean subjective International Knee Documentation Committee score at last follow-up was 81.8, and no differences were noted between the BTB and BTB-LET groups (P = .7). Two-thirds of patients were still participating in pivoting sports. A total of 17 knees (21%) experienced a graft failure, 5 of which (6%) underwent revision ACLR. There was no significant difference in graft failure risk between the BTB group (29%) and the BTB-LET group (13%; P = .1). Lateral tibiofemoral osteoarthritis was significantly more frequent in the BTB-LET group (59%) as compared with the BTB group (22%; P = .02). Lateral compartment osteoarthritis was correlated with partial lateral meniscectomy.
Conclusion:
There were no significant differences in long-term patient-reported outcomes after ACLR with or without an LET. LET may increase the risk of lateral compartment osteoarthritis at long-term follow-up. There was a trend toward decreased graft failure risk with the addition of LET but this study was underpowered to assess this outcome.
Keywords
Rupture of the anterior cruciate ligament (ACL) is a common sports injury. The natural evolution of chronic ACL deficiency is a progressive degeneration of the articular cartilage. 7 Osteoarthritis (OA) is observed in 60% to 100% of patients 20 years after the initial injury.19,20,29 After ACL reconstruction (ACLR), up to 50% of patients still develop OA.4,16,22 Known risk factors for OA are meniscectomy during ACLR, age at the time of injury, and delay between ACL rupture and surgery.27,28 Arthroscopic ACLR with bone–patellar tendon–bone (BTB) autograft is a reliable surgical option to control anterior laxity associated with ACL deficiency,6,14,33 but it has not been shown to protect against the subsequent development of OA. Factors that influence the persistent OA risk may include failure to restore proprioception, further joint damage attributed to the surgical procedure, and failure to completely restore native knee joint stability. Patients who experience a subsequent graft tear are among the highest-risk groups for poor patient-reported outcomes after ACLR. 31
The renewed interest in the anterolateral ligament in the past 10 years has brought back into focus the concept of anterolateral rotatory instability.1,2,8,13 Sonnery-Cottet et al 30 showed that anterolateral ligament reconstruction increases ACL graft survival in high-risk patients at 2-year follow-up. In our department, we have long believed that surgical restoration of rotational control is critical and that lateral extra-articular tenodesis (LET) can help control anterolateral instability and reduce the pivot shift.25,32 We have been performing LET for decades in patients with a high graft failure risk: patients undergoing revision ACLR, those with a high-grade pivot shift, and those participating in high-level cutting and pivoting sports.
Several techniques for LET have been described. One of the earliest techniques was described by Lemaire 15 in 1967 and later performed in combination with intra-articular ACLRs.3,18 Concerns of an increased risk of OA, stiffness, and donor site morbidity have been raised about the Lemaire procedure. However, studies differ on the clinical effect of LET, 35 and the long-term effect on graft survival and OA has been evaluated only in noncontrolled studies.11,21,34,36
At the time of ACL rupture, 70% of patients are <35 years old. 23 They often expect to remain physically active and practice sports for >20 years. Few studies have evaluated long-term results of ACLR with or without lateral tenodesis.17,21,34,36 We hypothesized that the addition of LET to intra-articular ACLR with a BTB autograft improves patient-reported outcomes and long-term graft survival without an increased risk of OA. The objective of this study was to compare long-term clinical and radiological outcomes between patients who underwent an isolated intra-articular BTB ACLR (BTB group) and patients who underwent an intra-articular BTB ACLR with the addition of an extra-articular tenodesis with the gracilis tendon (BTB-LET group).
Methods
Study Design
This is a single-center randomized controlled trial. It included 121 consecutive knees (120 patients) that underwent surgery between January 1, 1998, and September 30, 1999. The inclusion criterion was a complete isolated primary ACL rupture with a plan for arthroscopic ACLR. All ACL ruptures were confirmed preoperatively by magnetic resonance imaging. Exclusion criteria were a history of ACL repair or reconstruction, associated tears of the posterior cruciate ligament, or injuries of the collateral ligaments requiring surgical treatment. Presumed risk factors for graft failure (eg, competition sports, positive pivot-shift test result) were not considered in the patient selection or randomization process.
Unblinded block randomization at inclusion of the 121 knees allocated them to 1 of 2 groups: the BTB group (n = 61), in which an isolated arthroscopic intra-articular ACLR was performed with a bone-tendon-bone autograft, and the BTB-LET group (n = 60), in which the intra-articular BTB graft was combined with an LET.
Surgical Technique
In all patients, a BTB graft harvest was performed through a single skin incision centered on the patellar tendon. A 10-mm graft was harvested from the central third of the patellar tendon, with a rectangular bone block from the distal patella (20 × 8 × 8 mm) and a trapezoidal bone block from the tibial tuberosity (25 × 15 × 10 mm). Anterolateral and anteromedial arthroscopic portals were then created, and remaining ACL tissue was debrided from the femoral and tibial footprints to prepare for the tunnels. Meniscal tears, if present, were repaired when possible or treated with partial meniscectomy when necessary. Outside-in drill guides were used to prepare both tunnels. A 10-mm femoral tunnel was drilled toward the anatomic femoral footprint via a short incision proximal to the lateral epicondyle, and a 9-mm tibial tunnel was drilled medial to the anterior tibial tuberosity and into the anatomic tibial footprint. The ACL graft was introduced through the femoral tunnel and pulled into the tibial tunnel. The trapezoidal end of the tibial bone block was impacted into the femoral tunnel to achieve press-fit fixation. The knee was then placed at 10° of flexion, and the proximal tibia was pushed posteriorly during tibial fixation. The bone block was fixed in the tibial tunnel with an absorbable interference screw, reinforced with a metal wire passed through the bone block, and secured by a unicortical screw next to the tunnel.
For the BTB-LET group, an extra-articular tenodesis was added with the gracilis tendon (Figure 1). The graft, at least 15 cm long, was prepared with a nonabsorbable suture. It was passed through a 4.5-mm drill hole in the tibial bone block before its impaction into the femoral tunnel, which achieved the femoral fixation of the LET graft. The incision for the femoral tunnel was extended to the Gerdy tubercle. Both gracilis bundles were then passed under the lateral collateral ligament and through both sides of a tibial tunnel under the Gerdy tubercle. The extra-articular graft was then sutured onto itself with nonabsorbable suture at 30° of flexion in neutral rotation to not overconstrain the lateral compartment. 21
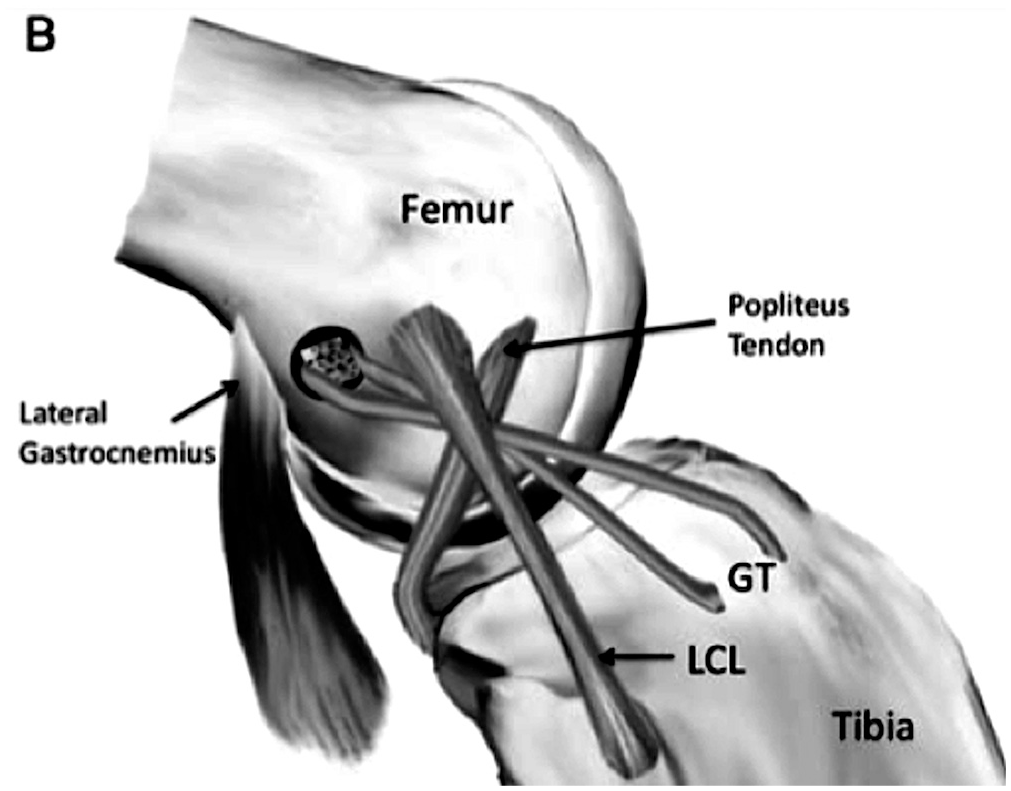
Illustration of the reconstruction technique: bone–patellar tendon–bone graft and lateral extra-articular tenodesis. Patellar tendon graft is used for anterior cruciate ligament reconstruction; gracilis tendon is passed through the proximal bone block and attached at the Gerdy tubercle (GT). LCL, lateral collateral ligament.
Outcome Evaluation
Patients were routinely evaluated at 2 months, 6 months, 1 year, and 2 years postoperatively. Short- and medium-term follow-ups have been presented as communications for the French Orthopedic Surgery Society meetings but, given the extensive loss to follow-up, have not been previously published. This study describes the most recent follow-up of this cohort at a mean 19 years after ACLR. An examiner independent from the original surgeon recorded patient-reported outcome scores (subjective International Knee Documentation Committee [IKDC] score, Lysholm score, and “forgotten knee” score 10 ) and subsequent surgical procedures (including revision ACLR). Patients willing to return for on-site evaluation underwent a standard clinical examination of the operated and contralateral knees, which included range of motion, Lachman test, and pivot-shift test. Patients also completed subjective IKDC, Lysholm, and forgotten knee scores. When possible, radiographs were obtained, including standard anteroposterior and lateral weightbearing views and skyline views, with TELOS bilateral radiographic laximetry testing.
The primary outcome measure was subjective IKDC score. Secondary outcomes included Lysholm score, forgotten knee score, graft failure, and OA. Graft failure was defined by the presence of at least 1 of the following criteria: subsequent revision ACLR, recurrent instability (>1 episode), a difference in anterior knee laxity (TELOS) >10 mm, a soft endpoint in the Lachman test, or a 3+ pivot-shift test (gross pivot shift) on physical examination.
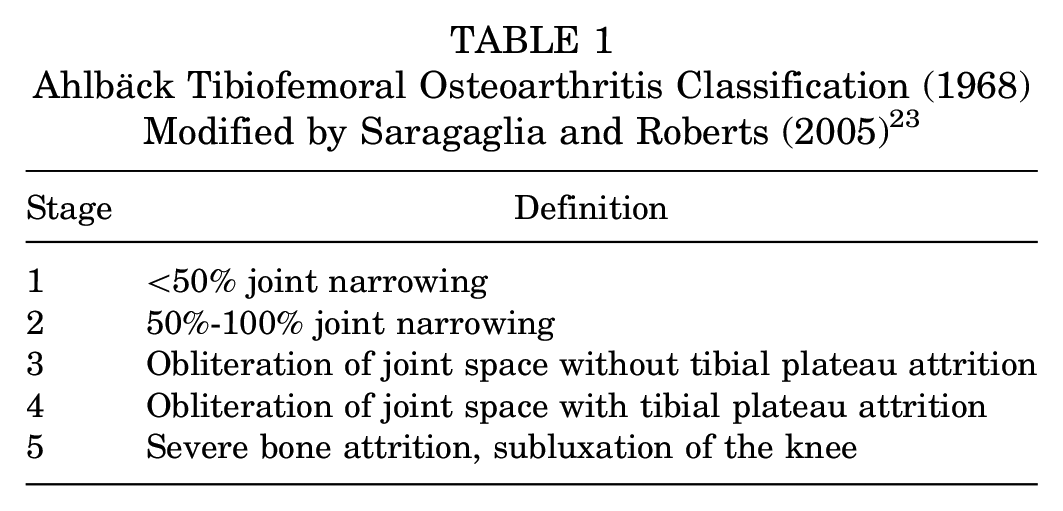
Tibiofemoral OA was evaluated on weightbearing radiographs and graded according to the modified Ahlbäck classification (Table 1). Patellofemoral OA was graded on a skyline view according to the Iwano classification. 12 OA was defined as Ahlbäck or Iwano stage 1 or worse for each compartment.
Ahlbäck Tibiofemoral Osteoarthritis Classification (1968) Modified by Saragaglia and Roberts (2005) 23
Statistics
Statistical analysis was performed with EasyMedStat (www.easymedstat.com). Categorical data were compared with Fisher exact tests. Continuous data were tested for normality and compared with either Student t tests or Mann-Whitney tests depending on normality. The log-rank nonparametric test was used to compare survival differences between the BTB and BTB-LET groups. P values <.05 were considered statistically significant. A power analysis was performed for the primary outcome measure (subjective IKDC score). To achieve a minimum 80% power with α = .05, a minimum sample size of 58 patients was required to detect the minimum clinically important difference of 10 points in the subjective IKDC score.
Results
Demographics and Follow-up
At the time of ACLR, patients in the BTB (61 knees) and BTB-LET (60 knees) groups were similar in regard to demographics, previous surgery, meniscal status, and sports participation (Table 2). Before ACLR, 10 knees (8.3%) had a history of surgery, including 5 medial meniscectomies, 3 arthroscopies, 1 arthrolysis, and 1 arthroscopic repair of a tibial spine avulsion fracture.
Patient Characteristics, Sports Participation, and Meniscal Status at Inclusion a
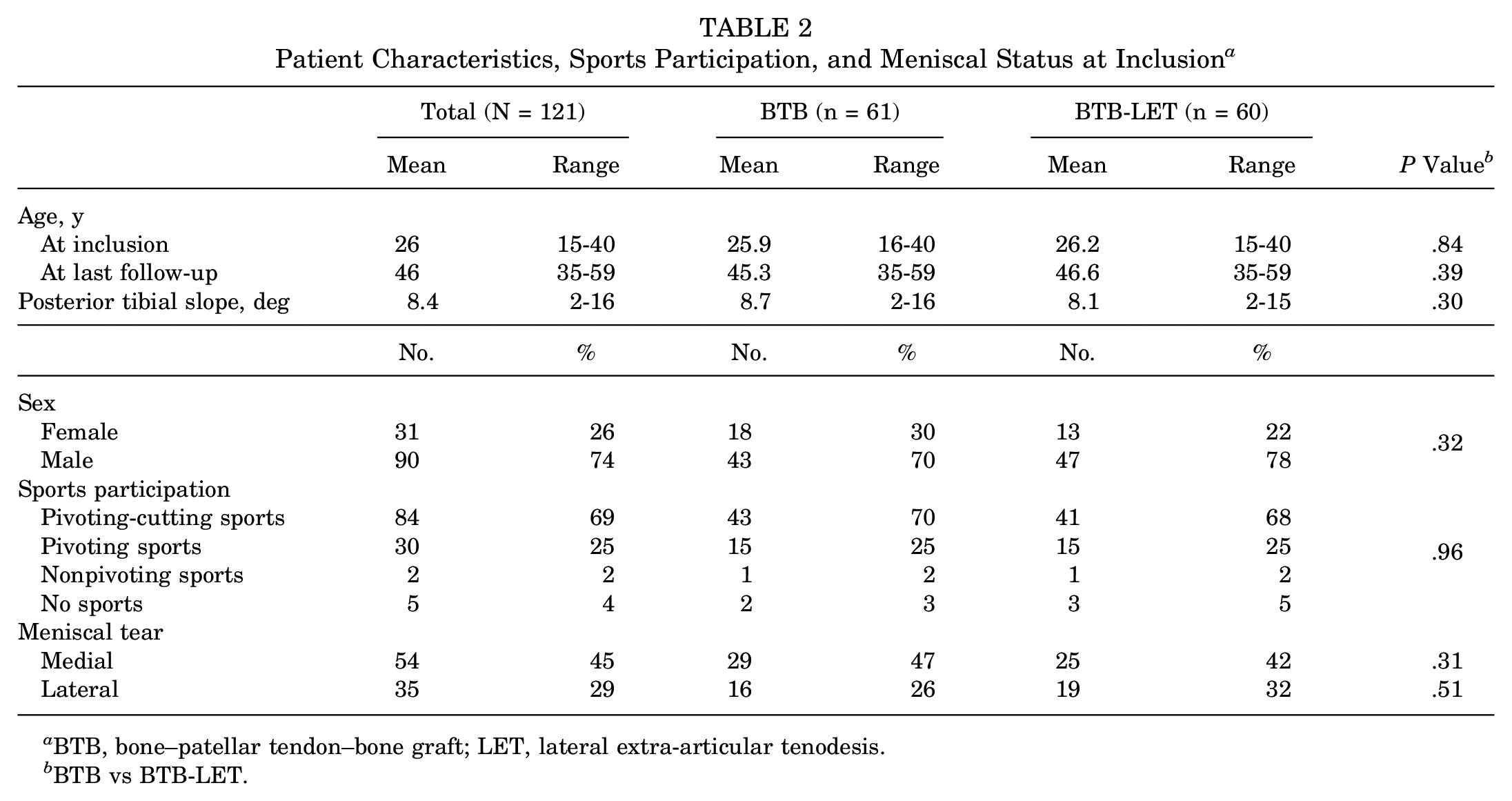
BTB, bone–patellar tendon–bone graft; LET, lateral extra-articular tenodesis.
BTB vs BTB-LET.
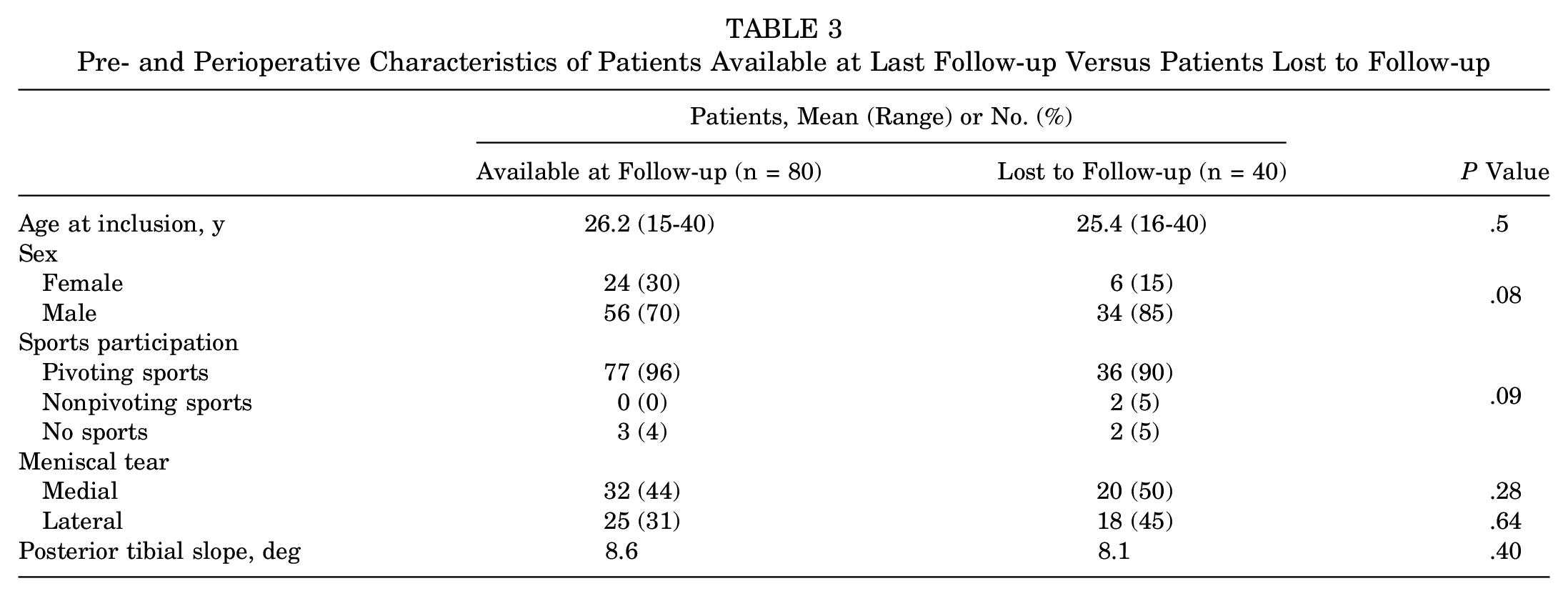
At a mean 19.4 years (range, 19-20.2 years) after ACLR, 80 patients (81 knees; 67%) were available for follow-up. One patient underwent a total knee replacement 18 years after the ACLR and was excluded from the analysis. A total of 41 patients (34%) were lost to follow-up; 79 patients (80 knees) completed the patient-reported outcomes questionnaire; and 43 patients (36%) underwent a clinical evaluation. Standard radiographs were obtained in 45 patients (37%), and laximetry data were available for 42 patients (35%) (Figure 2). Preoperative characteristics of the patients available for follow-up were not statistically different from patients lost to follow-up (Table 3).
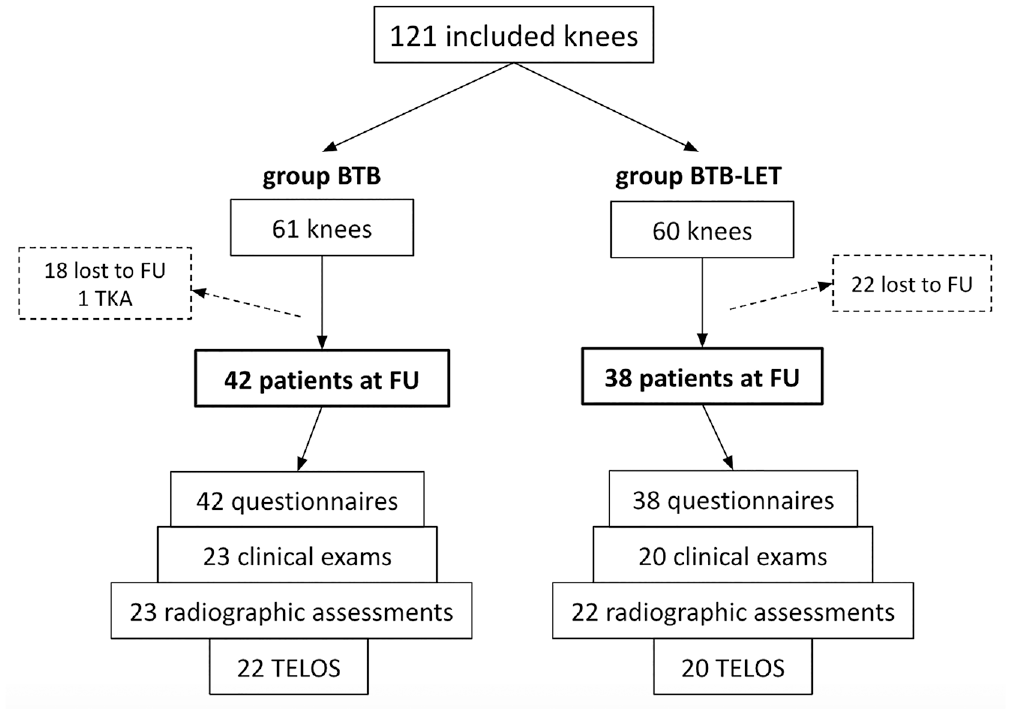
Flowchart for follow-up. BTB, bone–patellar tendon–bone graft; FU, follow-up; LET, lateral extra-articular tenodesis; TKA, total knee arthroplasty.
Pre- and Perioperative Characteristics of Patients Available at Last Follow-up Versus Patients Lost to Follow-up
Patient-Reported Outcome Scores and Sports Participation
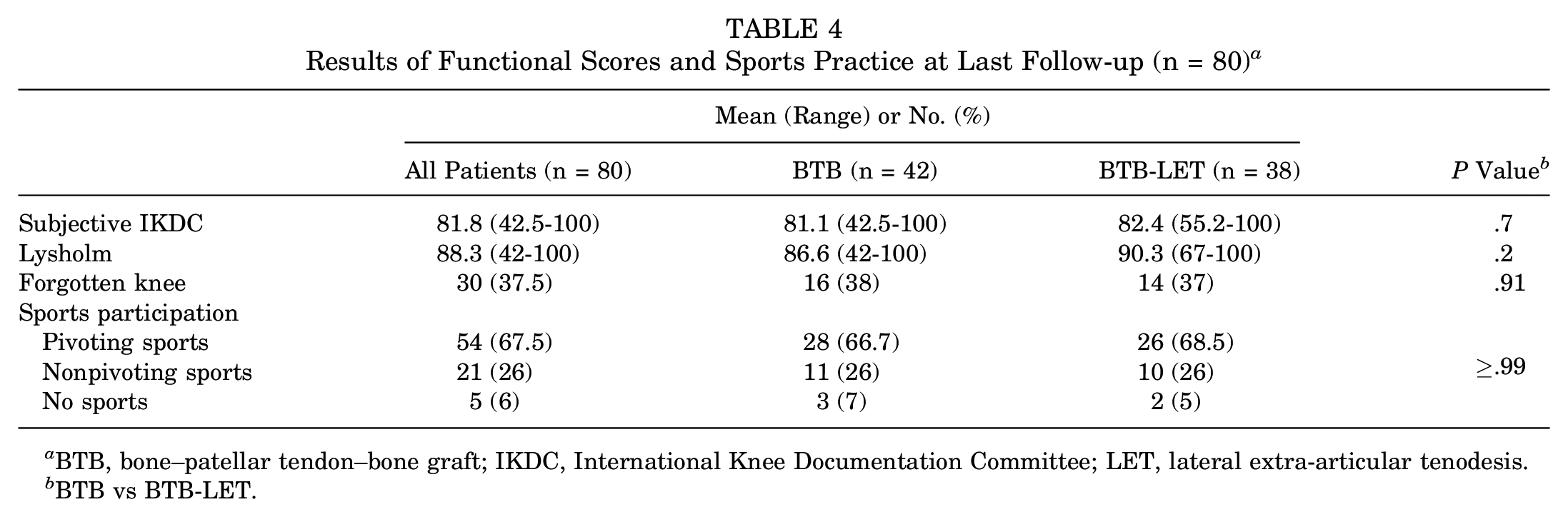
There were no significant differences in subjective IKDC, Lysholm, or forgotten knee scores between the BTB and BTB-LET groups at follow-up (Table 4). The 12 patients with graft failure who had not undergone revision had a mean Lysholm score of 78.5 versus 91.5 for patients without graft failure (P = .0004). Mean subjective IKDC score was 72 in the nonrevised graft failure group versus 84.5 in that without graft failure (P = .003). Before ACL rupture, 94% of patients regularly participated in pivoting sports. At last follow-up, 67.5% had returned to play in pivoting sports.
Results of Functional Scores and Sports Practice at Last Follow-up (n = 80) a
BTB, bone–patellar tendon–bone graft; IKDC, International Knee Documentation Committee; LET, lateral extra-articular tenodesis.
BTB vs BTB-LET.
Meniscal Status
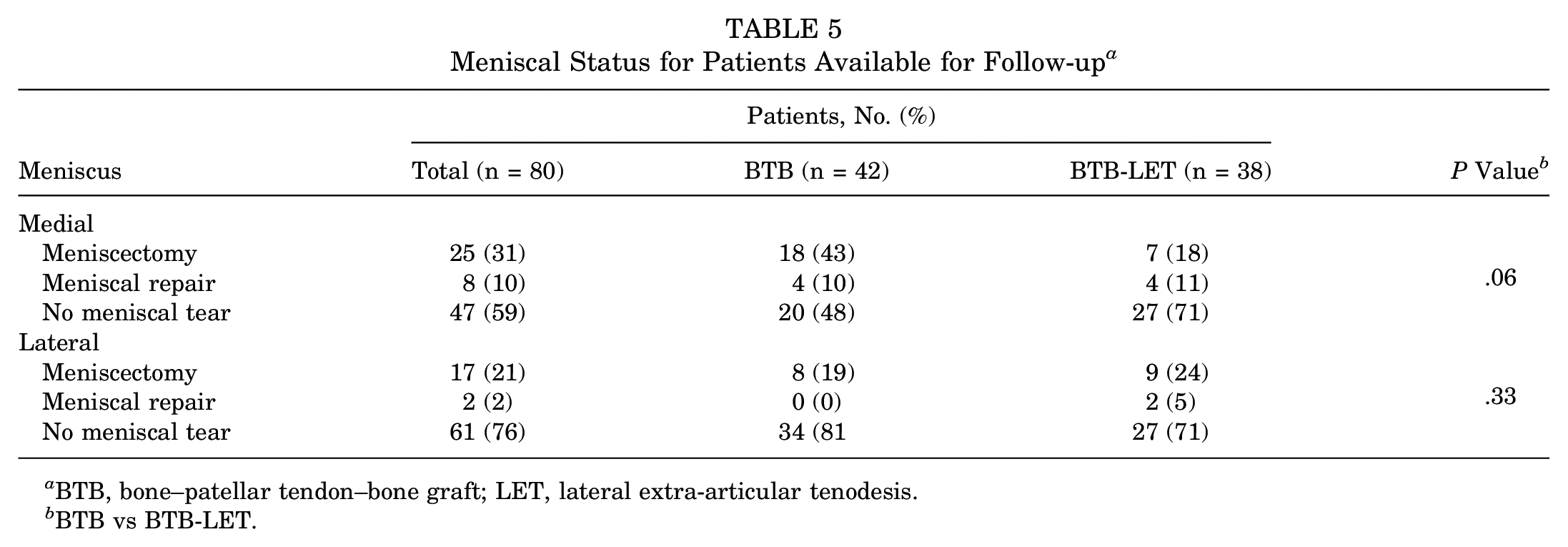
Of the 80 knees available at last follow-up, 25 (31%) had a medial meniscectomy before (1), during (20), and/or after (7) primary ACLR (Table 5). A total of 17 knees had a lateral meniscectomy during (13) and/or after (5) primary ACLR. Meniscal resections were as minimal as possible. There was a trend toward an increased incidence of medial meniscectomy in the BTB group as compared with the BTB-LET group (P = .06). Postoperative meniscectomies were not associated with graft failure (P = .6), nor were postoperative lateral meniscectomies (P≥ .99). Lateral meniscal status was similar between the groups. However, when only patients with radiological data at last follow-up were considered, there were 11 perioperative lateral meniscectomies out of 22 knees (50%) in the BTB-LET group versus 4 lateral meniscectomies out of 23 knees (17.4%) in the BTB group (P = .03).
Meniscal Status for Patients Available for Follow-up a
BTB, bone–patellar tendon–bone graft; LET, lateral extra-articular tenodesis.
BTB vs BTB-LET.
Graft Failure
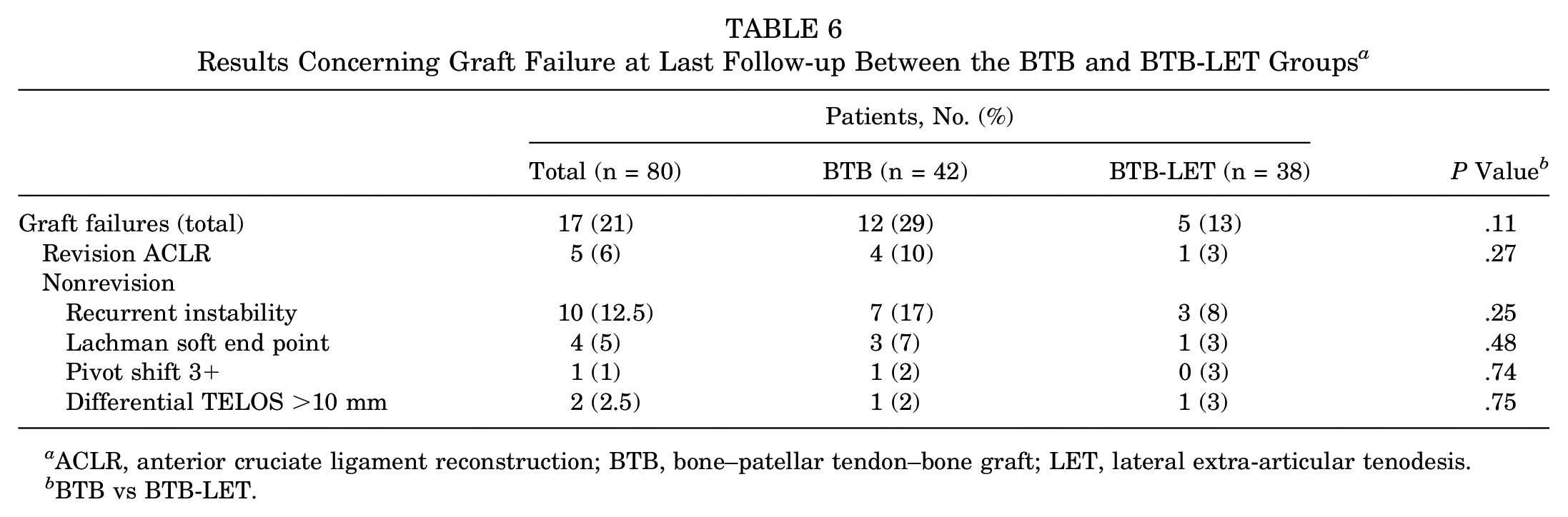
At final follow-up, graft failure had occurred in 17 of 80 knees (21%) (Table 6). Five of these patients underwent revision ACLR between 5 and 12 years postoperatively. Ten patients had symptoms of recurrent instability but had not undergone revision. The remaining 2 patients had no symptoms of instability but a differential laximetry (TELOS) >10 mm. Graft failure occurred in 12 of 42 knees (29%) in the BTB group and 5 of 38 knees (13%) in the BTB-LET group (P = .1). A positive pivot-shift test result was not correlated with the lateral tenodesis (P≥ .99). Revision reconstruction was performed in 4 of 42 knees (10%) in the BTB group and 1 of 38 knees (3%) in the BTB-LET group. Graft survival (without revision reconstruction) at 19 years was 90% in the BTB group and 97% in the BTB-LET group (P = .2).
Results Concerning Graft Failure at Last Follow-up Between the BTB and BTB-LET Groups a
ACLR, anterior cruciate ligament reconstruction; BTB, bone–patellar tendon–bone graft; LET, lateral extra-articular tenodesis.
BTB vs BTB-LET.
Osteoarthritis
The overall incidence of medial tibiofemoral OA (71%) and patellofemoral OA (67%) was high at follow-up but similar to that of the contralateral knees (67% and 49%, respectively) (Table 7). The incidence of lateral tibiofemoral OA was significantly higher in the operated knee (40%) than in the nonoperated knee (4%; P < .0001) (Table 7). Tibiofemoral OA was Ahlbäck stage 1 in 31 patients and stage 2 in 4 patients. Patellofemoral OA was Iwano grade 1 in 15 patients, grade 2 in 12 patients, and grade 3 in 3 patients.
Osteoarthritis at Last Follow-up Between the Operated and Contralateral Knees and Between the BTB and BTB-LET Groups (n = 45) a
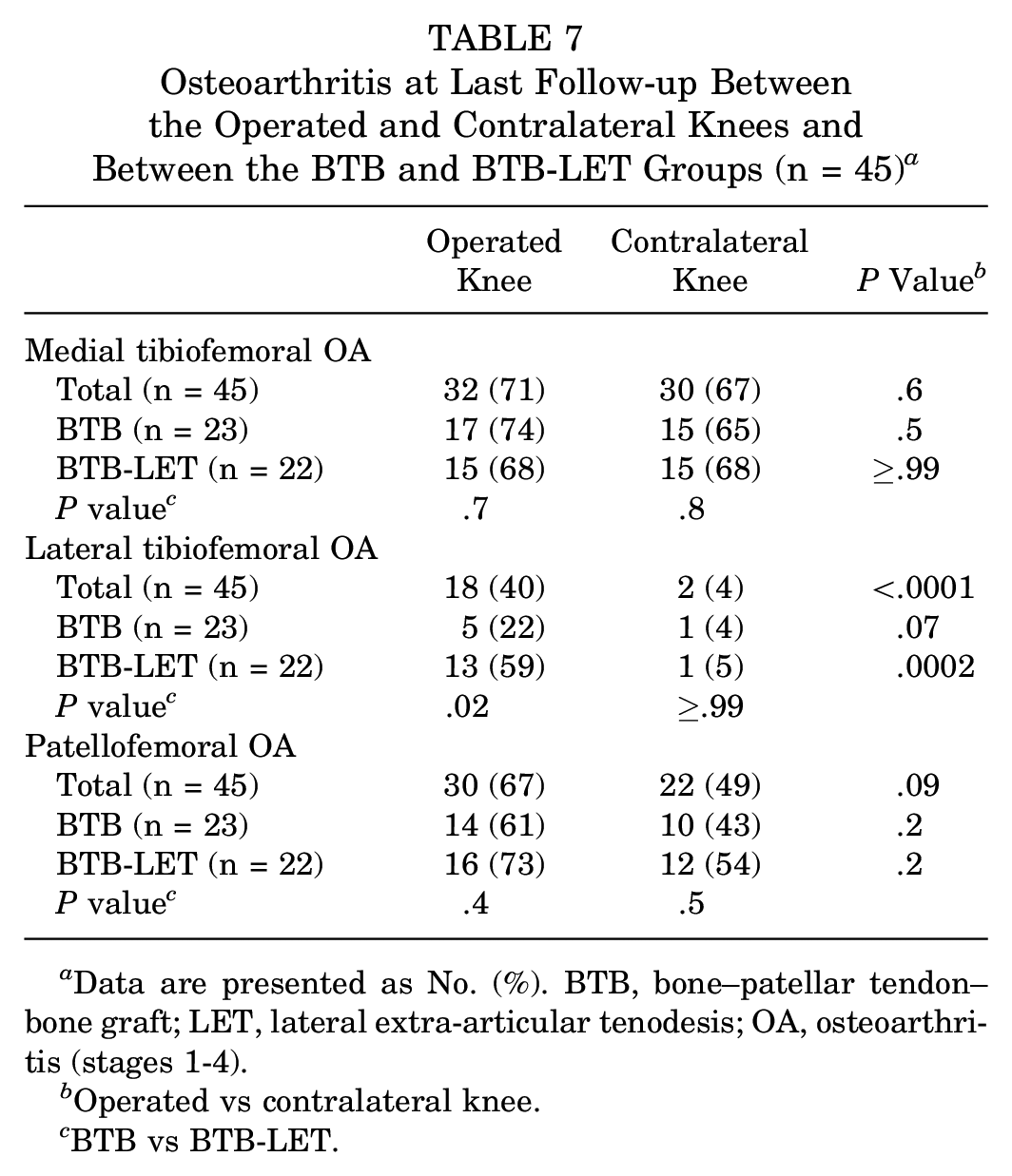
Data are presented as No. (%). BTB, bone–patellar tendon–bone graft; LET, lateral extra-articular tenodesis; OA, osteoarthritis (stages 1-4).
Operated vs contralateral knee.
BTB vs BTB-LET.
The incidence of lateral tibiofemoral OA in the operative knee was higher in the BTB-LET group (59%) than in the BTB group (22%; P = .02). No significant differences in OA in the medial or patellofemoral compartments were noted between the treatment groups (Table 7).
There was no significant correlation between medial meniscectomy and the incidence of medial compartment OA. There was an increased incidence of lateral compartment OA in patients who underwent a lateral meniscectomy (P = .04). In the BTB-LET group, 6 of 13 patients presenting with lateral OA had undergone a partial lateral meniscectomy.
Discussion
The most important finding of this randomized controlled trial is that there is no difference in patient-reported outcomes at 19 years after ACLR with or without the addition of an LET. The study demonstrates a trend toward decreased risk of graft failure in the isolated BTB-LET group (13%) versus the isolated BTB group (29%; P = .1). This study is underpowered for this outcome measure. The study did demonstrate a significantly increased risk of lateral compartment OA in the ACLR-LET group, but this finding is confounded by the increased number of partial lateral meniscectomies performed in it.
Relatively good patient-reported outcome scores and knee function were noted in both groups nearly 20 years after ACLR. Two-thirds of patients who underwent surgery have maintained participation in a pivoting sport almost 20 years after ACL surgery, while 94% participated in such sports preinjury. Patients with nonoperated graft failure had worse patient-reported outcome scores. At the time of failure, most did not undergo revision ACLR because of their age. Recent studies have reported good functional results after ACL surgery in older patients, 5 perhaps indicating that some of these patients may benefit from revision. Despite satisfying mean subjective scores (>80 out of 100), only one-third of the reviewed patients had a “forgotten knee.” 10
Among all operated knees at 19-year minimum follow-up, 78% had stage 1 or 2 tibiofemoral OA (lateral and/or medial). The addition of an LET was associated with a significantly increased risk of lateral tibiofemoral OA; however, partial lateral meniscectomy was significantly associated with lateral OA, and lateral meniscal lesions were significantly more frequent in the BTB-LET knees with radiographs than in the BTB group. Several previous studies have documented the biomechanical effects of the addition of an LET. Engebretsen et al 9 demonstrated a decreased load on an intra-articular graft with the addition of an LET. However, this study and other works raise the concern of overconstraint of the lateral compartment of the knee and subsequent increased risk of OA with the addition of a lateral extra-articular procedure. 26 We believe that these studies speak to the need to fix the lateral tenodesis with the knee in neutral rotation rather than in an externally rotated position as was classically described.
Few long-term series have evaluated OA after ACLR, and most studies did not evaluate the lateral, medial, and patellofemoral compartments separately. Yamaguchi et al 34 reported 71% OA at 24-year follow-up. Pernin et al 21 reported 54% grade C or D OA at 24.5-year follow-up.
Zaffagnini et al 36 found a mean 3.6-mm medial joint space and 5.3-mm lateral joint space at 20-year follow-up and reported 17% OA (Kellgren and Lawrence stage 3) in 26 patients at final follow-up. Mihelic et al 17 retrospectively reviewed 32 patients at 17 to 20 years after an ACL tear treated surgically with bone-tendon-bone autograft ACLR. Nine (28%) had IKDC C or D OA at final follow-up. There is no previous evidence of increased OA in the lateral compartment with LET. In our series, the only significant difference concerning OA between the operated knee and the contralateral non–ACL deficient knee was in the lateral compartment.
Almost half of the patients in this series underwent partial meniscectomy before, during, or after the ACLR. Meniscal repair was rare, as partial meniscectomy was the standard treatment at the time of this study. We did not find an association between medial meniscal lesions and OA,4,21 probably because of the relatively high incidence of medial compartment OA in all knees (operative and contralateral) at follow-up.
This study did not demonstrate a difference in ACL graft failure risk with the addition of an LET but was underpowered for this outcome. There is no consensus concerning criteria for graft failure, but the overall graft failure risk in the BTB-LET group in this study (13%) was similar to that of previously published results. To our knowledge, 3 studies have described long-term results (≥20 years) of combined intra- and extra-articular ACLR. Yamaguchi et al 34 reviewed 27 patients 24 years after primary ACLR with LET (iliotibial tract graft). One patient had revision ACL surgery, and 5 of the 26 remaining patients (20%) had a soft endpoint on Lachman examination and a side-to-side KT-1000 difference of at least 5 mm at last follow-up. Pernin et al 21 reviewed 100 of 148 patients 24 years after a bone-tendon-bone ACLR combined with LET (iliotibial band graft). They found a 20% incidence of graft failure, defined solely as a positive pivot-shift finding. Zaffagnini et al 36 reviewed 52 of 60 patients at a minimum of 20 years after an over-the-top ACLR with LET (double-stranded hamstring tendon graft). Of 29 patients available for clinical examination, 4 had positive Lachman and pivot-shift test results (14%). Of 26 patients, 3 had a KT-2000 side-to-side difference >5 mm (12%). Of 52 reviewed patients, 1 had undergone revision ACLR.
There are several limitations in this study. First, one-third of the enrolled patients were lost to follow-up, and only a portion of the contacted patients were available for on-site evaluation and radiographs. While expected at nearly 20 years postoperatively, this loss to follow-up could bias our results. Enough patients were available to evaluate the primary outcome measures, but the study remains underpowered to address the key question of whether graft failure risk is decreased by the addition of a lateral extra-articular procedure. A final limitation of the study is the uneven distribution of lateral meniscal lesions between groups in the patients available for imaging at follow-up. The increased incidence of meniscal pathology in the BTB-LET group confounds the evaluation of OA risk based on surgical technique. The strengths of this study are its randomized prospective design and long-term follow-up of a relevant clinical question.
Conclusion
There are no significant differences in long-term patient-reported outcomes after ACLR with or without an LET. LET may increase the risk of lateral compartment OA at long-term follow-up. There is a trend toward decreased graft failure risk with the addition of LET, but this study was underpowered to assess this outcome.
Footnotes
Submitted August 4, 2019; accepted February 12, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: E.S. is an occasional consultant for Smith & Nephew and Corin. S.L. is a consultant for Smith & Nephew and received institutional research support from Corin and Amplitude. P.N. is a consultant for Smith & Nephew, receives royalties from Tornier-Wright, and receives institutional research support from Tornier-Wright and Amplitude. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.