
Abstract
Background:
Dog-ear and bird-beak deformities are common after transosseous-equivalent repair (suture bridge technique). The natural course of deformities after rotator cuff (RC) repair using the suture bridge technique is unclear. The remodeling potential of these deformities has not been investigated.
Purpose:
To evaluate remodeling and retear rates associated with deformities after RC repair.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Between November 2011 and February 2012, we studied 99 consecutive shoulders. All patients underwent arthroscopic RC repair via the suture bridge technique with or without additional sutures. Two groups were formed: no deformity (n= 46) and deformity (n = 53). Deformity was defined as marginal detachment and protrusion of the RC after repair, involving inappropriate compression of the suture limbs from the anchors. Tendon height was measured from the highest point of the most protruding portion of the cuff to the cortex on semi-coronal magnetic resonance imaging (MRI) scan. Change in tendon height was evaluated on MRI scan at 1 week and 6 months postoperatively. Clinical assessment at every patient visit included the American Shoulder and Elbow Surgeons (ASES) score, Constant shoulder score, and visual analog scale for pain (pVAS) score.
Results:
No significant differences were found in age, sex, symptom duration, tear size, and preoperative ASES, Constant, and pVAS scores (P > .05) between the 2 groups. The initial tendon height was 7.4 ± 1.5 mm in the no-deformity group and 9.3 ± 2.0 mm in the deformity group. Follow-up height was 6.3 ± 2.1 mm in the no-deformity group and 6.4 ± 1.6 mm in the deformity group. Mean postoperative tendon heights were 90.1% ± 23.8% of the initial height in the no-deformity group and 73.2% ± 15.1% in the deformity group. Clinical scores (ASES, Constant, and pVAS) were not significantly different between the groups at 6 months. There were 4 shoulders in each group that experienced retearing (types 4 and 5 according to the Sugaya classification) at 6 months postoperatively. There was no difference in retear rate (P > .999).
Conclusion:
Most deformities after RC repair were remodeled with no effect on retears. Clinical outcomes were not affected by deformities.
The transosseous-equivalent technique using suture anchors (suture bridge technique) is widely used for rotator cuff (RC) repair. This technique allows the surgeon to maximize the utility of a single-row construct by using the suture limbs from the medial mattress sutures to bridge and compress the repaired tendon. 16 Compared with single-row constructs, suture bridge constructs have been shown to improve contact pressure on the restored tendon-bone interface 17 and provide superior biomechanical characteristics. 18 However, redundancies in the RC tissue, so-called “dog-ear” and “bird-beak” deformities, are quite common after RC repair, especially when the suture bridge technique is used. 9 Commonly encountered in the surgical wound as well, these deformities are the result of an asymmetric repair or crumpling of the substance of the tendon.
In general, the length of the RC tear margin is longer than the footprint, and thus these dog-ear or bird-beak deformities are formed after repair. This tendency increases as the mismatch increases. Although some articles have addresses this issue, most have concentrated on techniques to reduce the deformity quantitatively and numerically, and the effect of the deformity on repair integrity has not been widely investigated.9,10,21 Surgeons try to reduce this deformity because they are concerned that it might adversely affect the repair integrity or clinical outcome. However, the effect of this deformity on outcomes is not known. No previous report has demonstrated the natural course of such deformities.
With this in mind, we sought to evaluate the remodeling rate of deformities after RC repair using postoperative magnetic resonance imaging (MRI) and to assess the retear rate associated with deformities after the suture bridge technique. The hypothesis of this study was that there would be no differences in functional outcomes and retear rates between the deformity group and no-deformity group after arthroscopic RC repair using the suture bridge technique.
Methods
Patient Enrollment and Characteristics
The inclusion criteria used in this study were as follows: (1) a full-thickness tear or partial-thickness tear involving at least 50% of the tendon (grade 3 according to the Ellman classification 6 ) as demonstrated using preoperative MRI or magnetic resonance arthrography; (2) complete repair (type 1 or 2 repair according to the Yoo classification 26 ) performed arthroscopically by use of the suture bridge technique; and (3) the availability of 2 postoperative MRI results (3.0-T, Achieva; Philips) obtained at our institution: an initial MRI (obtained within 1 week after surgery) and a follow-up MRI (obtained approximately 6 months after surgery).
The exclusion criteria were (1) a partial-thickness tear that was not converted to a complete tear before repair; (2) any open procedure; (3) any history of previous surgery, infection, fracture, or dislocation of the involved shoulder; (4) arthritic changes of the glenohumeral joint; (5) inflammatory joint disease of the involved shoulder, including rheumatoid arthritis; and (6) any workers’ compensation case. Approval from the institutional review board at our institution was obtained before data collection in the retrospective study.
Between November 2011 and February 2012, 148 consecutive shoulders underwent arthroscopic RC repair by a single senior surgeon (J.C.Y.) using the suture bridge technique. Both MRI scans were available in 118 patients. According to the inclusion criteria, 8 patients were excluded (repair type 3 or 4). A further 4 patients were excluded according to the exclusion criteria, and 7 patients were excluded because comparative measurement was not available to 3-mm cutting distance. In total, 99 patients were ultimately included in the analysis. They were divided into 2 groups (the no-deformity group and the deformity group).
Deformity was defined arthroscopically and radiologically as a protrusion of the RC tissue after repair, involving inappropriate compression of the suture limbs from the anchors. The dog-ear deformity was diagnosed when the width of the protrusion was greater than the height; conversely, the bird-beak deformity was diagnosed when the height was greater than the width (Figure 1).
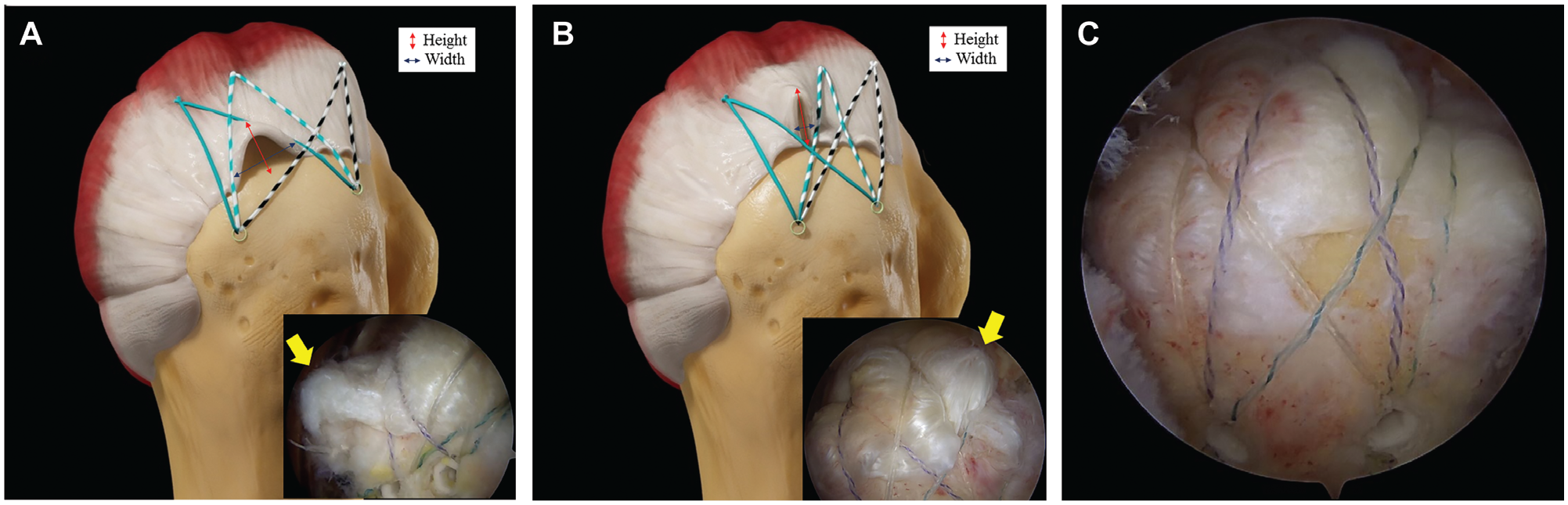
(A) The dog-ear deformity was diagnosed when the width of the protrusion was greater than the height. (B) The bird-beak deformity was diagnosed when the height of the protrusion was greater than the width. (C) The favorable repair configuration.
In the no-deformity group, 46 shoulders were included at a mean of 18.0 ± 8.6 months (range, 6-34 months) after surgery. The mean age at the time of surgery was 57.8 ± 10.3 years (range, 31-71 years). In the deformity group, 53 shoulders were included for evaluation at a mean of 18.9 ± 8.2 months (range, 6-36 months) after surgery (dog-ear deformity, 46 patients; bird-beak deformity, 11 patients; mixed, 4 patients). The mean age at the time of surgery was 60.7 ± 7.9 years (range, 40-73 years). According to Post et al, 20 RC tear size was classified as partial to small in 9shoulders, medium in 29, and large in 8 in the no-deformity group and as partial to small in 5 shoulders, medium in 33, and large in 15 in the deformity group.
Mean tear size (anteroposterior) was 23.1 ± 11.1 mm in the no-deformity group and 24.9 ± 10.1 mm in the deformity group (P = .194). Retraction length was 19.4 ± 9.1 mm in the no-deformity group and 20.4 ± 9.7 mm in the deformity group (P = .277).
Except for preoperative external rotation, no differences were noted in any preoperative data points including age,sex, symptom duration, dominant arm involvement, underlying disease (diabetes, hypertension, and thyroid disease), size distribution of the RC tear, preoperative American Shoulder and Elbow Surgeons (ASES) score, Constant shoulder score, and visual analog scale for pain (pVAS) score between the 2 groups (Table 1).
Patient Characteristics: Preoperative Status a
ASES, American Shoulder and Elbow Surgeons; pVAS, visual analog scale for pain.
The tear size was classified according to the tear diameter, by use of the classification system of Post et al. 20
Clinical and Radiological Evaluations
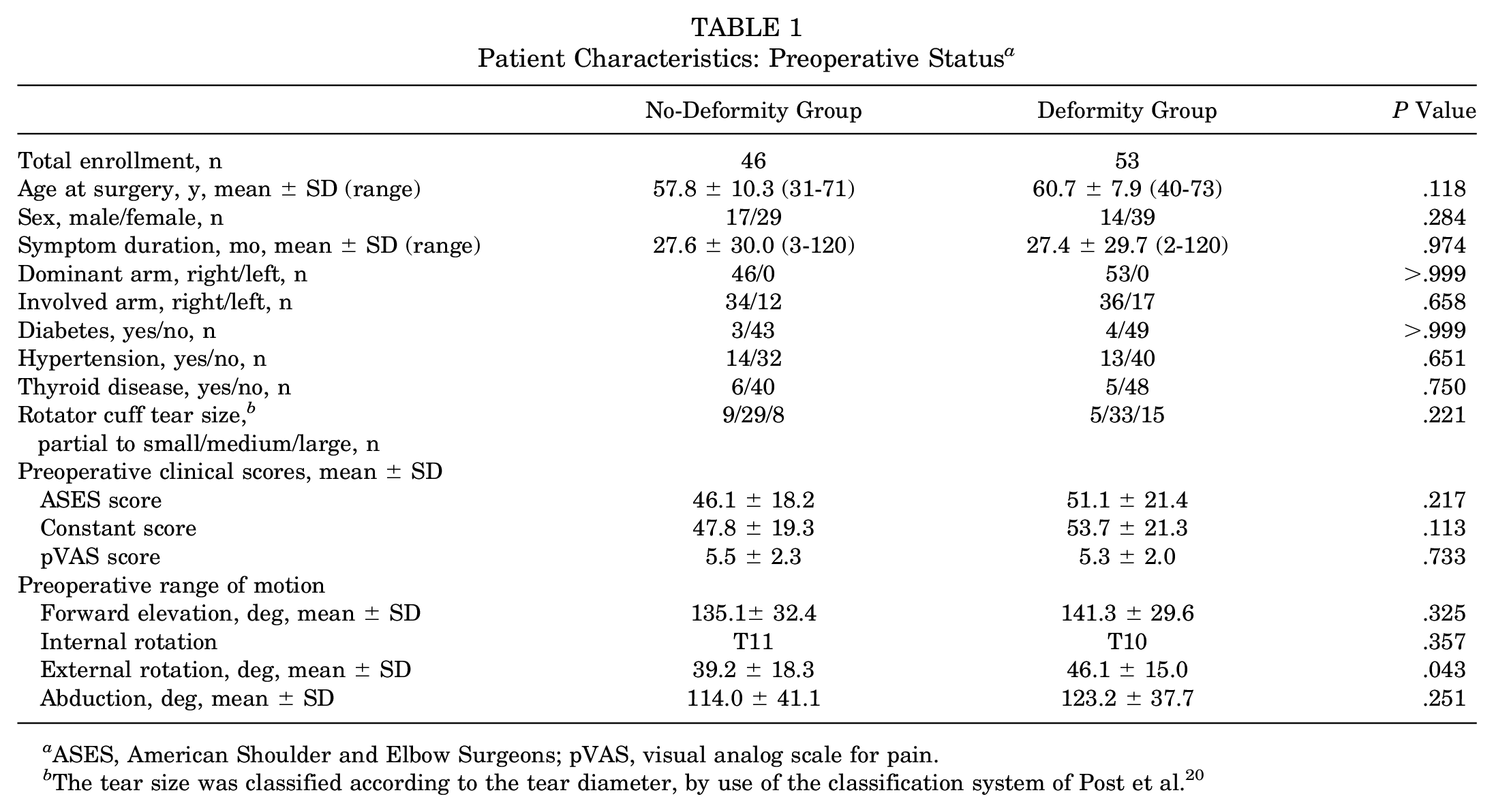
Tendon height was measured from the highest point of the most protruding portion of the cuff to the cortex on coronal oblique MRI scan. The change in tendon height from initial to follow-up MRI scan was evaluated in both groups (Figure 2). Clinical assessments were performed at every patient visit through use of the ASES score, 22 Constant shoulder score, 5 and pVAS score. Patient satisfaction after surgery was assessed at the final follow-up as excellent, good, fair, or poor.
(A) Schematic of measuring the highest point of the repaired rotator cuff tendon from the cortex. (B) Initial magnetic resonance imaging scan after rotator cuff repair on the right shoulder and (C) magnetic resonance imaging scan of same shoulder at follow-up.
Surgical Techniques and Rehabilitation Protocol
All patients underwent surgery while under general anesthesia in the semilateral decubitus position. The greatest dimension of each RC tear was measured intraoperatively using an arthroscopic ruler after debridement. Small-sized tears, including partial-thickness RC tears, were repaired with 1 double polyethylene thread–loaded or triple-loaded suture anchor as a medial row. Medium-sized tears were repaired with 1 or more double- or triple-loaded suture anchors as a medial row. The first medial anchor position was the posterior area of the bicipital groove and the lateral aspect of the articular cartilage on the supraspinatus footprint. The second and third medial anchor positions were determined based on the size and pattern of the RC tear (Figure 3).
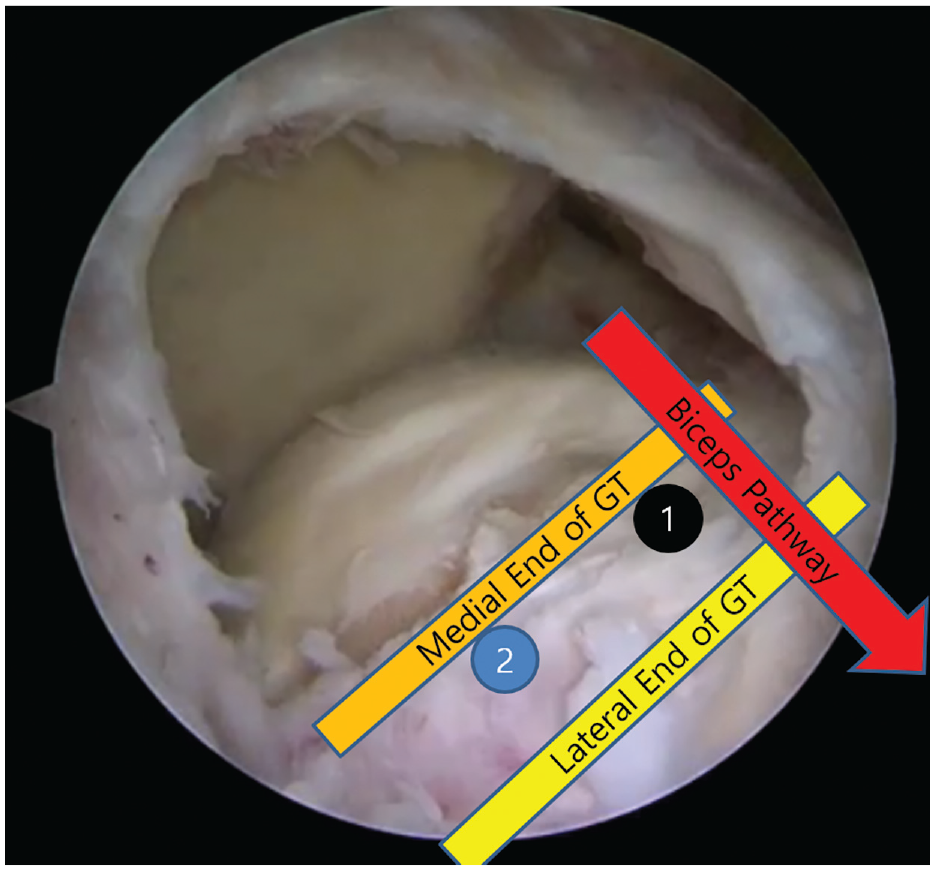
Placement of medial anchors during arthroscopic rotator cuff repair of the right shoulder. The first anchor (1) was placed at the posterior area of the bicipital groove and the lateral aspect of the articular cartilage on the supraspinatus footprint. The second anchor (2) was placed at least 10mm posterior to the first anchor and was determined based on the size and the pattern of the rotator cuff tear. GT, greater tuberosity.
An anterior leading edge of a supraspinatus tendon was secured with polyethylene threads from the first suture anchor (Figure 4). An interval tie construct was formed to avoid medial row strangulation. 12 The first lateral anchor position was the posterior aspect of the bicipital groove, and the distance from the footprint to the lateral anchor was determined according to the size and pattern of the RC tear, shape of the greater tuberosity, and repair configuration that allowed the polyethylene sutures to compress the tendon properly on the footprint. The second lateral anchor position was determined based on the repair configuration and RC tear characteristics.
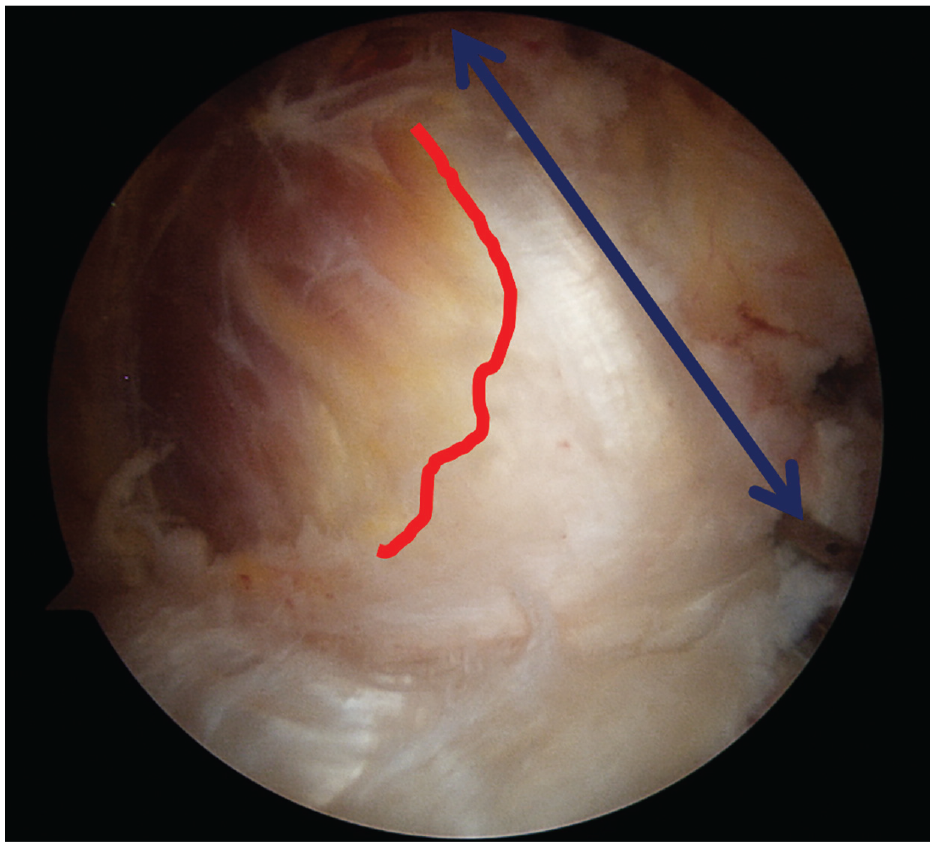
Design of the repair before suture passage. An anterior leading edge of the supraspinatus tendon was identified with a tendon grasper (blue line with arrows), and the musculotendinous junction of the supraspinatus (red line) was visible through arthroscopy.
If repair of the subscapularis tendon tear was required, 1 or 2 medial suture anchors were used in a mattress repair fashion with or without 1 lateral anchor. 19 At least 2 suture anchors (PopLok; Conmed Linvatec) for supraspinatus, infraspinatus, and teres minor tendon repair were used as a lateral anchor in all cases.
A routine rehabilitation protocol was followed by all patients, with immobilization for 4 weeks followed by active-assisted passive range of motion exercises. Stretching and active strengthening exercises were performed after full range of motion was achieved.
Statistical Analysis
To compare the patient data between the 2 groups, a 2-sample t test or the Mann-Whitney U test was performed. Sex, RC tear size distribution, and underlying diseases were analyzed through use of the chi-square test or Fisher exact test. Preoperative and postoperative clinical scores (ASES, Constant, and pVAS) were compared by use of paired t tests or the Wilcoxon signed rank test. Acromioplasty, biceps procedure, subscapularis tendon procedure, satisfaction, and retear rate were analyzed using the chi-square or Fisher exact test. The number of bird-beak deformities was small; therefore, the different deformities were not analyzed separately. All statistical analyses were performed with SPSS version 20.0 (SPSS Inc) with 95% CIs.
Results
Patient Characteristics and Clinical Scores
The total numbers in the no-deformity and deformity groups were 46 and 53, respectively. The following findings were not significantly different between the 2 groups: rates of combined acromioplasty (39 patients [84.8%] in the no-deformity group and 49 patients [92.5%] in the deformity group; P = .226), biceps procedure (debridement or no procedure/tenotomy/tenodesis: 18/17 [37.0%] /11[23.9%] in the no-deformity group and 18/19 [35.8%] /16[30.2%] in the deformity group; P = .762), and subscapularis tendon repair (no procedure or debridement/repair: 38/8 [17.4%] in the no-deformity group and 44/9 [17.0%] in the deformity group; P > .999).
In the no-deformity group, type 1 repair (complete repair with the tendon mobilized to the far lateral end of the greater tuberosity covering nearly all of the original footprint) was performed in 34 shoulders (73.9%), and type 2 repair (complete repair with the tendon mobilized to the medial one-half or less of the greater tuberosity) was performed in 12 shoulders (26.1%); these values were 35 (66.0%) and 18 (34.0%) in the deformity group, respectively. 26 Repair status according to the Yoo classification was not different between the 2 groups (P = .511). Repair configuration was not significantly different between the 2 groups (number of medial × lateral row anchors, 1×2/2×2/3×2/3×3: 13/27/4/2 in the no-deformity group and 11/36/5/1 in the deformity group; P = .703). No difference was found between the 2 groups in the number of polyethylene sutures used for repair (3.9 ± 1.5 in the no-deformity group and 4.0 ± 1.4 in the deformity group; P = .305).
At the 6-month postoperative MRI, the healing integrity of the repaired tendon (according to the Sugaya classification) was not significantly different between the 2 groups (type 1/2/3: 11/18/13 in the no-deformity group and 16/13/20 in the deformity group; P = .260).
We noted that 4 shoulders in the no-deformity group and 4 in the deformity group experienced retears (measured as types 4 and 5 in accordance with Sugaya et al 24 ) on MRI scans at 6 months postoperatively. No difference in the retear rate was seen between the 2 groups (P > .999) (Table 2).
Patient Characteristics: Surgery Associated
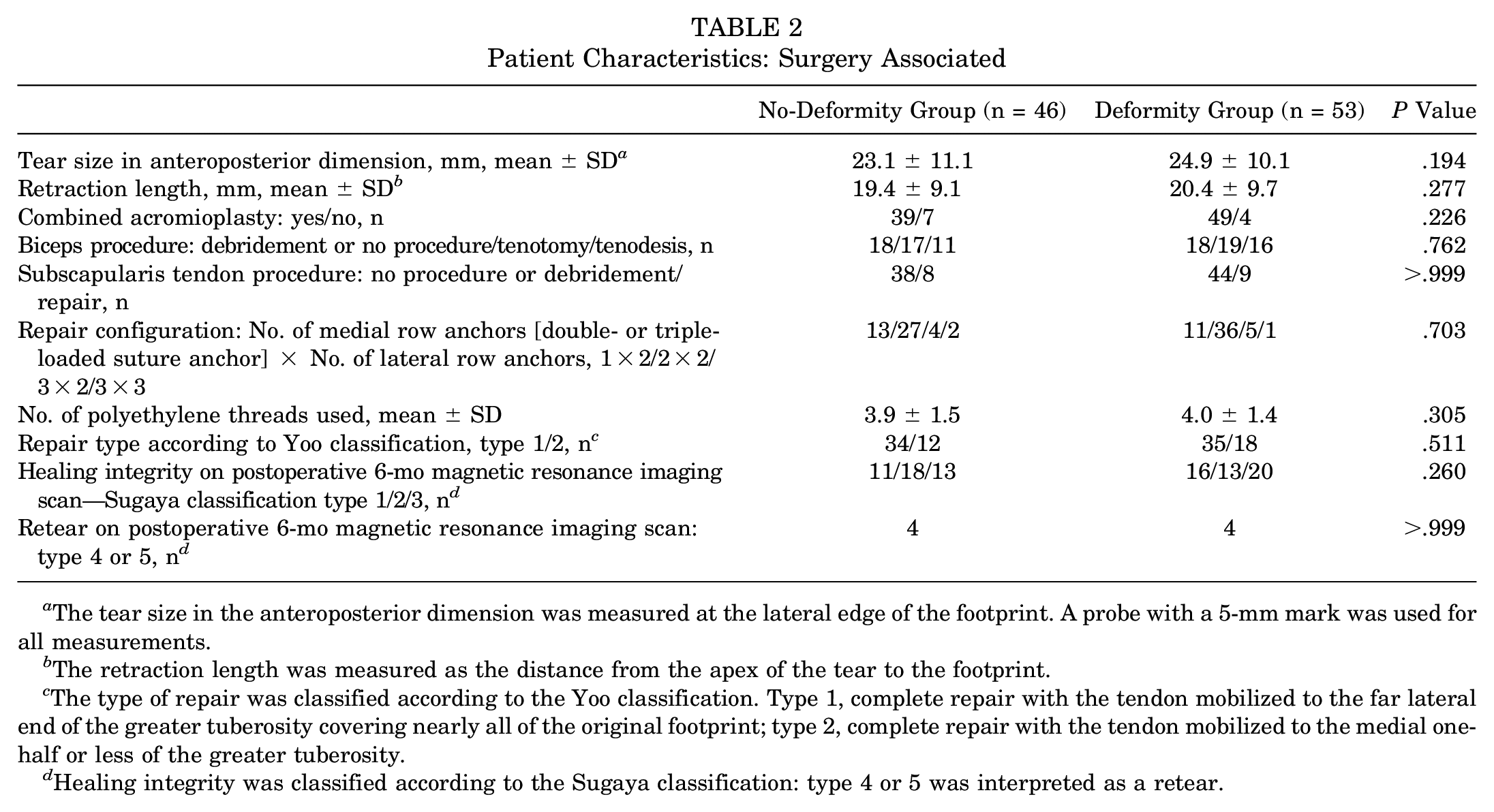
The tear size in the anteroposterior dimension was measured at the lateral edge of the footprint. A probe with a 5-mm mark was used for all measurements.
The retraction length was measured as the distance from the apex of the tear to the footprint.
The type of repair was classified according to the Yoo classification. Type 1, complete repair with the tendon mobilized to the far lateral end of the greater tuberosity covering nearly all of the original footprint; type 2, complete repair with the tendon mobilized to the medial one-half or less of the greater tuberosity.
Healing integrity was classified according to the Sugaya classification: type 4 or 5 was interpreted as a retear.
In the deformity group, 3 retear cases were type 1 (retear on the tendon-bone interface) and the other retear case was type 2 (the remnant cuff tissue remained at the insertion site). 3 The mean height of the deformity was 9.7 ± 1.8 mm (range, 7.9-12.1 mm). No statistical difference in the total mean height of the deformity group was found (P = .344). In the no-deformity group, 2 retear cases were type 1 and the other 2 retear cases were type 2. No statistical difference in preoperative tear size was found between the 2 groups (27.0 ± 11.9 in the deformity group and 33.0 ± 11.6 in the no-deformity group; P = .249).
The initial tendon height (according to 1-week postoperative MRI scans) in the no-deformity group was 7.4 ± 1.5 mm (range, 3.8-10.8 mm), while that in the deformity group was 9.3 ± 2.0 mm (range, 5.3-13.7 mm). Follow-up height (according to the 6-month postoperative MRI scans) had decreased to 6.4 ± 1.6 mm (range, 4.0-9.2 mm) in the no-deformity group and 6.3 ± 2.1 mm (range, 3.9-9.3 mm) in the deformity group (Table 3).
Change of Tendon Height From Postoperative 1 Week to 6 Months a
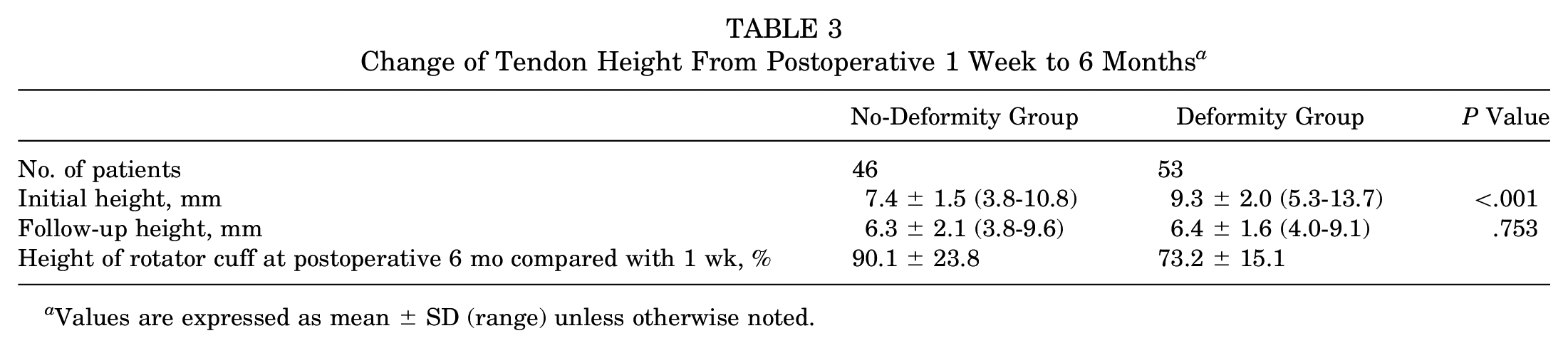
Values are expressed as mean ± SD (range) unless otherwise noted.
Mean postoperative tendon heights were 90.1% ± 23.8% of initial height in the no-deformity group and 73.2% ± 15.1% in the deformity group. A significant change in the height of the tendon was seen from 1 week to 6 months postoperatively in both groups (P < .001) (Figure 5).
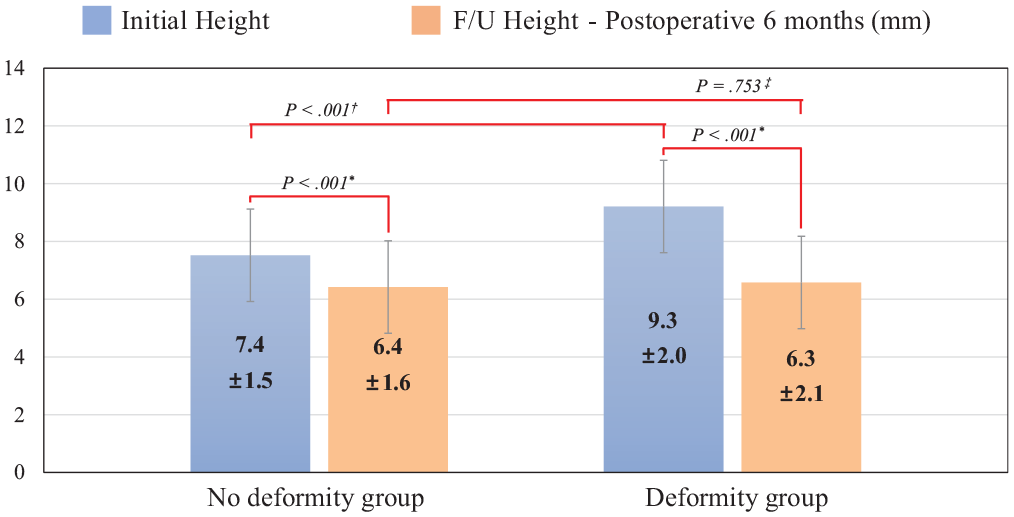
Comparison of initial and postoperative 6-month tendon height between the 2 groups. Both groups showed a significant decrease of tendon height at the postoperative 6-month follow-up (F/U) compared with the initial measurement. The significant differences in tendon height at 1 week between the 2 groups were not found at the 6-month follow-up. *P value between the height of the tendon at 1 week and 6 months postoperatively. †P value between initial height of the no-deformity group and deformity group. ‡P value between the follow-up height of the no-deformity group and deformity group.
ASES, Constant, and pVAS scores significantly improved in both groups by the final follow-up evaluation (P < .001), and no differences were seen between the 2 groups (P > .05) (Table 4).
Comparison of Last Follow-up Clinical Scores Between Groups a
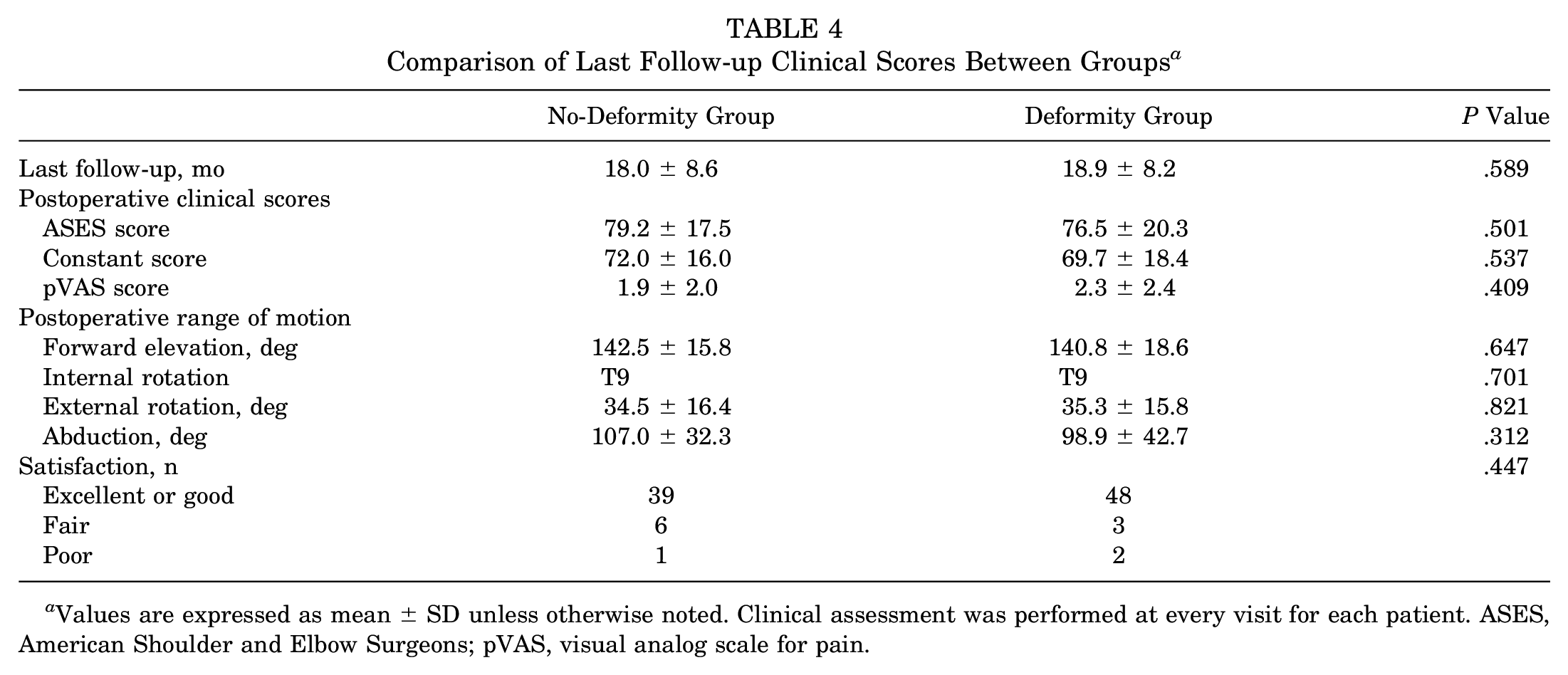
Values are expressed as mean ± SD unless otherwise noted. Clinical assessment was performed at every visit for each patient. ASES, American Shoulder and Elbow Surgeons; pVAS, visual analog scale for pain.
Discussion
The main finding of the present study was that tendon height on the footprint of the greater tuberosity decreased in both groups and that change in height was greater in the deformity group. The significant differences in tendon height at the 1-week initial MRI assessment between the 2 groups were not found at the 6-month MRI follow-up. No differences were seen in the retear rate and clinical outcomes between the 2 groups. These findings suggest that deformities with a height of <13.7 mm are likely remodeled without any effect on retearing and do not affect the postoperative outcomes of arthroscopic RC repair.
Dog-ear and bird-beak deformities are common after transosseous-equivalent repair (suture bridge technique). 9 Most surgeons are concerned that this deformity might adversely affect the repair integrity or clinical outcome in the future. Thus, various repair techniques have been introduced with the aim of reducing the occurrence of these deformities.10,23,25 However, deformities are essentially inevitable in cases involving specific tear configurations, such as when the mediolateral length of the tear is greater than its anterior to posterior length. 9
The best construct for RC repair is one that firmly secures the entire footprint without introducing a deformity. The use of the correct number of polyethylene sutures at regular intervals to cover the entire footprint is essential to prevent deformities. An insufficient number of sutures can lead to dog-ear deformities with a wide noncontact area at the bone-tendon interface. Such deformities can be managed with additional salvage sutures. Dog-ear or bird-beak deformities may be inevitable even if a sufficient number of sutures is used to allow complete coverage of the footprint. However, sufficient sutures can limit the size of the deformity because the noncontact area of the tendon-bone interface is narrower and, therefore, significantly less problematic.
In contrast, if too many sutures are used, 2 different kinds of problem can occur. One is related to blood flow at the repaired site. Fealy et al 7 reported that the site of the bleeding bony bed into which the RC tendon is repaired had consistently low vascular flow. If too many sutures were used to cover and compress the footprint, a significant decrease in vascular flow was observed that might interfere with healing at the tendon-bone interface.4,7,14 The other problem is related to medial row strangulation, which can cause retears close to the musculotendinous junction.3,8 Although the use of a medial knot-tying construct is biomechanically stronger than a nontying construct, 15 the use of multiple knots can lead to strangulation in the medial tendinous portion and result in the subsequent deterioration of tendon viability. 3 To avoid excessive medial row strangulation, a minimal or interval-tie construct may be useful in the suture bridge technique. 12 Using the appropriate number of sutures to form a durable construct is vital for successful repair, and selecting the correct number to provide favorable outcomes after arthroscopic RC repair using the suture bridge technique is a constant challenge for shoulder surgeons.
Another consideration for reducing the formation of dog-ear deformities is the use of a vector to reduce the retracted RC tendon. The torn RC tendon is retracted in the posteromedial direction, not just the medial direction. 2 Thus, to allow repair and to minimize tissue redundancies secondary to length inequalities between the torn cuff and footprint, the retracted tendon should be reduced in the anterolateral direction, not just the lateral direction. This is especially true in the case of larger tears. Selecting the correct position for the first medial anchor is vital in this process.
In the shoulders included in this study, the first medial anchor was inserted at the posterior area of the bicipital groove and an area between the articular cartilage of the humeral head and the footprint of the greater tuberosity. Then, the anterior leading edge of the supraspinatus tendon was secured, and appropriate knot-tying was performed. Next, the second medial anchor position was determined according to tear size and pattern. The first lateral anchor position was the posterior aspect of the bicipital groove. The distance from the footprint to the anchor depended on the tear size and pattern and the shape of the greater tuberosity. Finally, the second lateral anchor position was determined according to the repair configuration and tear pattern.
Kim et al 9 stated that a central bird-beak deformity may be considered as an articular-side partial-thickness RC tear and a marginal dog-ear deformity as a bursal-side partial-thickness RC tear. However, any differences between the deformity group and no-deformity group were not identified in this study. When a suture bridge construct is used, substantial biomechanical load is placed on the medial grasping suture, and the medial anchor delivers minimal traction to the lateral aspect of the tendon-bone interface.1,15 However, in a preoperative partial-thickness RC tear, traction is delivered directly around the torn tendon-bone interface. Thus, although noncontact area was produced at the tendon-bone interface after repair using the suture bridge technique with medial grasping sutures, it could not be concluded that the noncontact area caused by the deformity was a preoperative partial-thickness RC tear.
A previous study reported that the uninjured supraspinatus tendon thickness is 6.6 to 7.4 mm in healthy individuals. 13 In the current study, postoperative supraspinatus tendon thickness in both groups had recovered to near native status. In the no-deformity group, although the change was small, consistent height reduction was observed overall, and the mean change was statistically significant. These findings indicate that remodeling might have occurred in repaired tendon regardless of whether the repair configuration was optimal.
The present study has several limitations. First, retearing was evaluated over a short period (6 months postoperatively). Although a previous study showed no difference in repaired RC tendon integrity between 6 months and 19 months, 11 a longer follow-up period would reinforce the results of this study. Second, the diagnosis of deformities was somewhat subjective. To overcome this limitation, cases that were ambiguous were discussed among a group of shoulder surgeons until consensus was reached. Third, being retrospective in nature, this study did not include deformities evenly. Bird-beak and dog-ear deformities were not analyzed separately owing to the small and skewed sample. Fourth, tear shape was not considered. Some classification of tear shape could reveal correlations between this variable and the rate of deformities. Fifth, no large deformities were included in the sample, limiting the ability to generalize the results to all deformity sizes. Sixth, the last clinical follow-up was shorter than 2 years. Despite these limitations, this study is the first to report the natural course of deformities occurring after arthroscopic repair using the suture bridge technique.
Although anatomic repair is desired, the present study demonstrated that most deformities that did not exceed 13.7 mm in height were remodeled without any effect on the retear rate after arthroscopic RC repair using the suture bridge technique. Furthermore, clinical outcomes were not affected by dog-ear or bird-beak deformities. Surgeons should try to reduce the occurrence of deformities when using the suture bridge technique by individualizing the technique according to the size and pattern of the RC tear. However, if a deformity does occur and is not large, it should be assumed that it will not negatively affect the patient’s clinical and radiological outcomes.
Conclusion
Most deformities after RC repair were remodeled with no effect on retears. Clinical outcomes were not affected by deformities.
Footnotes
Submitted December 3, 2018; accepted February 10, 2020.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.