
Abstract
Background:
Patella alta has been identified as an important risk factor for lateral patellar instability and medial patellofemoral complex (MPFC) reconstruction failure.
Purpose:
To evaluate the length changes of the MPFC at multiple possible reconstruction locations along the extensor mechanism in varying degrees of patella alta throughout knee motion.
Study Design:
Controlled laboratory study.
Methods:
Eight fresh-frozen cadaveric knees were used in this study. The MPFC was identified and dissected with the patellar tendon and quadriceps tendon. A custom-made jig was utilized to evaluate lengths from 0° to 90° of flexion with physiological quadriceps loading. Length was measured with a 3-dimensional robotic arm at 4 possible reconstruction locations along the extensor mechanism: the midpoint patella (MP), the MPFC osseous center (FC), the superior medial pole of the patella (SM) at the level of the quadriceps insertion, and 1 cm proximal to the SM point along the quadriceps tendon (QT). These measurements were repeated at 0°, 20°, 40°, 60° and 90° of flexion. Degrees of increasing severity of patella alta at Caton-Deschamps index (CDI) ratios of 1.0, 1.2, 1.4, and 1.6 were then investigated.
Results:
Patella alta and MPFC attachment site location significantly affected changes in MPFC length from 0° to 90° of flexion (P< .0005). Length changes at attachment MP showed no difference when CDI 1.0 was compared with all patella alta values (CDI 1.2, 1.4, 1.6; P > .05). Similarly, FC showed no difference in length change from 0° to 90° until CDI 1.6, in contrast to proximal attachments (SM, QT), which demonstrated significant changes at CDI 1.4 and 1.6. When length changes were analyzed at each degree of flexion (0°, 20°, 40°, 60°, 90°), Spearman correlation analysis showed a moderate negative linear correlation for QT at CDI 1.0 (r= −0.484; P = .002) and 1.6 (r = −0.692; P < .0005), demonstrating constant loosening at the QT point at normal and elevated patellar height. In contrast, no differences in length were observed for MP at CDI 1.0 throughout flexion, and at CDI 1.6, there was a difference only at 0° (P < .05). Points FC and MP at CDI 1.6 had similar length change properties to points SM and QT at CDI 1.0 (P > .05), suggesting that distal attachments in the setting of patella alta may provide similar length changes to proximal attachmentswith normal height.
Conclusion:
Anisometry of the MPFC varies not only with attachment location on the extensor mechanism but also with patellar height. Increased patellar height leads to more significant changes in anisometry in the proximal MPFC attachment point as compared with the distal component. In the setting of patella alta, including a CD ratio of 1.6, the osseous attachments of the MPFC remain nearly isometric wheras the proximal half length changes increase significantly.
Clinical Significance:
The results of this study support the idea that the MPFC should be considered as 2 separate entities (proximal medial quadriceps tendon femoral ligament and distal medial patellofemoral ligament) owing to their unique length change properties.
Keywords
Patellar instability is one of the most common orthopaedic problems among young athletes, occurring at a rate of 2.29 per 100,000 person-years in the United States and with a peak incidence between 15 and 19 years of age. 18 Unfortunately, patellar dislocation recurrence rates have been reported to range from 10% to 70% after primary dislocation, generally in young patients with chronic instability, anterior knee pain, and apprehension. 11 Recurrence varies greatly according to individual risk factors, including patellar height, long leg alignment, soft tissue laxity, and trochlear dysplasia.5-7
The medial patellofemoral ligament (MPFL) has been commonly described and is the primary constraint to lateral displacement. 1 The medial quadriceps tendon femoral ligament (MQTFL) has been described more recently and attaches proximal to the patella. 16 These 2 structures form the medial patellofemoral complex (MPFC), which represents the entirety of the soft tissue restraints that prevent lateral patellar translation. The length changes, or anisometry, of the different aspects of the MPFC vary along the length of the complex, with the proximal aspect becoming relatively looser in early flexion as compared with the distal aspects.
Patella alta has been reported to be present in up to 75% of first-time lateral patellar dislocations and constitutes a significant risk factor for patellar instability recurrence.2-4,8,14 Specifically, 1 study reported that patella alta was the most commonly identified risk factor in a lateral patellar dislocation cohort. 3 It is thought that increased patellar height predisposes patients to patellar instability owing to the MPFC's being required to work through larger degrees of flexion before the patella engages in the trochlea.
Importantly, the role of patella alta in MPFC reconstruction complications remains poorly understood. It is suspected that the rate of complications after MPFC reconstruction in patients with concurrent patella alta is higher than previously reported, as patella alta may result in a more anisometric reconstruction when compared with MPFC reconstruction in patients with normal patellar height, potentially causing chondrosis, graft elongation, tunnel enlargement, and eventual recurrent dislocation. 12 In this regard, limited evidence exists regarding the length changes of different fixation points of the MPFC along the extensor mechanism with increasing degrees of patella alta. An understanding of these changes could affect graft attachment position choice in MPFL reconstruction when patella alta is present. In addition, these surgical alterations could improve postoperative patellar tracking and patient outcomes and avoid the need to perform distalization to correct patella alta.
The purpose of this study was to evaluate anisometry of the MPFC at multiple possible reconstruction locations along the extensor mechanism in varying degrees of patella alta severity. We hypothesize that the length will differ according to the location of the insertion site on the patella and that anisometric values will be accentuated with increasing degrees of patella alta.
Methods
This study was exempt from institutional review at Rush University Medical Center because of its utilization of deidentified cadaveric specimens. The specimens used in this study were donated to a tissue bank for the purpose of medical research and then purchased by our institution. Eight (n = 8) nonpaired fresh-frozen knees were obtained with the following exclusion criteria: age <65 years, cancer history, bedridden donor, surgical scars, and recent knee trauma. Before testing, the knees were evaluated for gross signs of osteoarthritis and anatomic abnormalities via arthroscopy and fluoroscopy. Specimens were stored at −20°C and thawed at room temperature for 24 hours before dissection. Initially, the femoral diaphysis was sectioned 20 cm from the joint line, and all soft tissues beyond 15 cm of the joint line were removed.
Dissection Technique
The cadaveric knees were dissected to isolate the patellar tendon, patella, MPFC, and quadriceps tendon (QT). A medial incision was made through the skin and subcutaneous tissue. The sartorius fascia was transected, allowing visualization of the pes anserinus tendons. The tendons were then retracted, and the superficial medial collateral ligament was identified and followed to its insertion on the medial femoral condyle. 10 The MPFC was then identified on the femoral attachment and followed laterally to the extensor mechanism. The MPFC, QT, and patellar tendon were then visualized, and all soft tissue surrounding these structures was removed.
Specimen Preparation
After MPFC identification, the anatomic footprint of the MPFC at the femoral attachment point—the sulcus between the medial epicondyle and abductor tubercle that was located by palpation of osseous structures—was marked with a threaded screw. The following attachments on the extensor mechanism were subsequently marked: midpoint patella (MP), MPFC osseous footprint center (FC), superior medial pole of the patella (SM) at the level of the quadriceps insertion, and 1 cm proximal to the SM point along the QT (Figure 1). After the femoral and patellar attachments were landmarked for standardized measurement, the MPFC was removed by clean dissection.
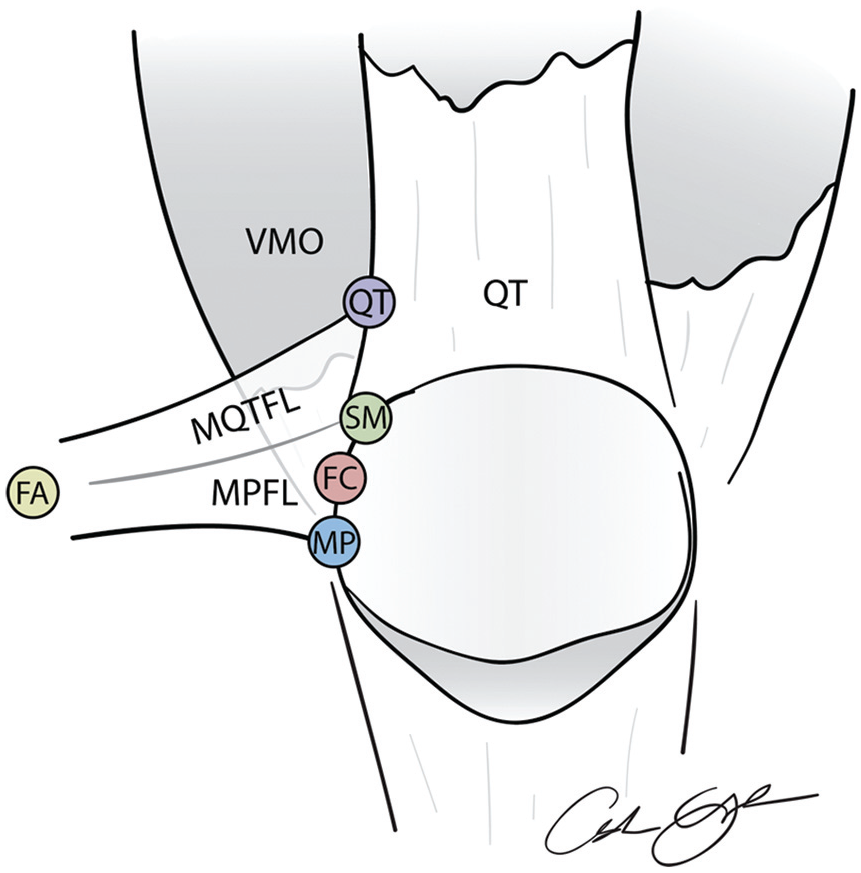
The medial patellofemoral complex (MPFC) attachment sites on the extensor mechanism: midpoint patella (MP), MPFC osseous center (FC), superior medial pole of the patella (SM), and 1 cm proximal to this along the quadriceps tendon (QT). FA, femoral attachment location; MPFL, medial patellofemoral ligament; MQTFL, medial quadriceps tendon femoral ligament; VMO, vastus medialis obliquus.
In each specimen, the native Caton-Deschamps index (CDI) was calculated to be approximately 1.0 by obtaining a perfect lateral radiograph of the knee (ie, by aligning the posterior aspects of the femoral condyles). The specimen was then loaded into a custom-machined jig (Figure 2). The femoral shaft was potted in polymethyl methacrylate (PMMA) to ensure rigid fixation. The femoral PMMA cylinder was modified for passage of the sutures (1-0 FiberWire; Arthrex) to secure the QT (Krackow locking suture), allowing a 10-lb weight (45 N) to be attached and thus mimicking the physiologic loading of the QT in a similar manner to previous studies9,13 The distance between the femoral and patellar MPFC attachment sites was measured with a 3-dimensional measurement device (MicroScribe; Solution Technologies) at knee flexion angles of 0°, 20°, 40°, 60°, and 90°, as confirmed with a goniometer during testing.

Experimental setup. The knee was potted in polymethyl methacrylate (PMMA) and placed in a custom-made jig that allowed for 0° to 90° of flexion.
Specimen Testing
The CDI was standardized to ratios of 1.0, 1.2, 1.4, and 1.6 according to the perfect lateral radiographs and Image J software (National Institutes of Health). Suture anchors were secured to the distal pole of the patellar tendon, passed through the adjacent tibial tuberosity, and brought through the patella for fixation on the superior patellar border. The patellar tendon was excised, and the remaining suture anchors were tied to specific lengths to obtain the desired CDI. The 3-dimensional distances of the MPFC attachment site were then measured with imaging analysis software (OsiriX) and compared with the data obtained from the pretesting measurements.
Statistical Analysis
Statistics were conducted with SPSS (v 25; IBM). A 2-way repeated measures analysis of variance was used to investigate the relationship between extensor mechanism attachment site and CDI on change in MPFC length from 0° to 90° of flexion. Pairwise comparisons were then performed with a Bonferroni correction for multiple comparisons. The data were normally distributed, as tested with the Shapiro-Wilk test of normality on studentized residuals. Paired t tests were used to compare adjacent attachment sites and the relationship between sites in patella alta and the native anatomic sites at CDI 1.0. Paired t tests were used to evaluate differences between 2 CDI ratios at 1 location at a particular degree of flexion. Length at QT and MP through flexion at each tested CDI value was analyzed with a Friedman test because of the presence of nonnormally distributed data. Finally, a Spearman correlation was used to evaluate the relationship between degree of flexion (from 0° to 90°) at QT at CDI 1 and QT at CDI 1.6. Significance was set at P < .05.
Results
Eight cadaveric knees were utilized in this study. Imaging information, as measured on computed tomography, for the included specimens is provided in Table 1.
TT-TG and Dejour Classification for the Specimen as Measured on Computed Tomography a
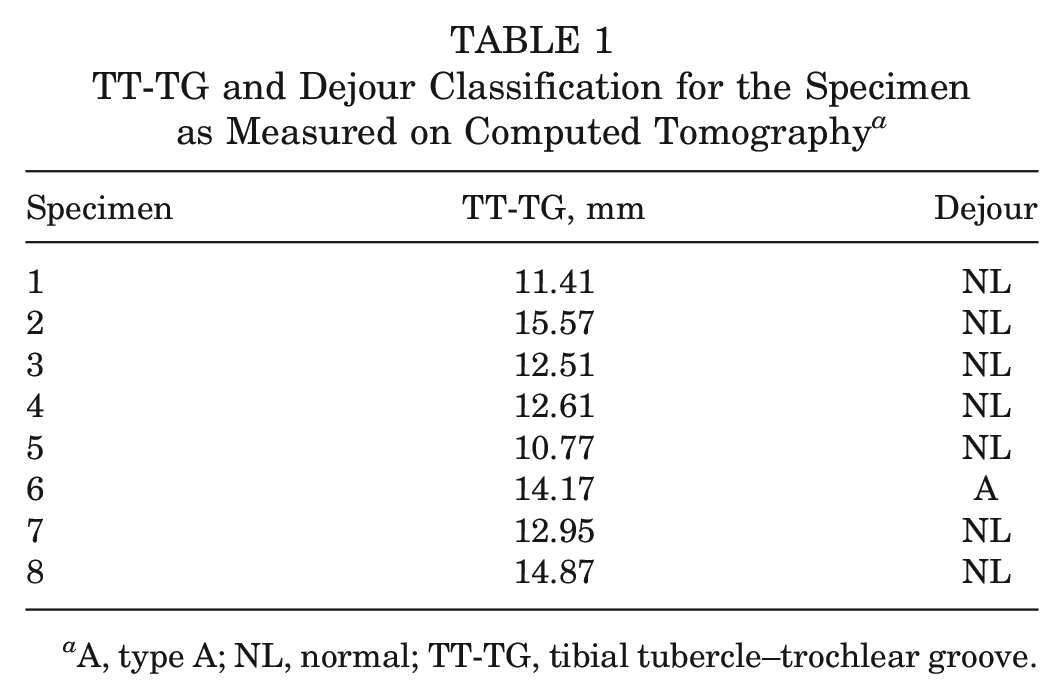
A, type A; NL, normal; TT-TG, tibial tubercle–trochlear groove.
Effect of Location on Length Changes From 0° to 90° of Flexion
The mean length changes occurring between 0° and 90° of knee flexion are shown in Table 2. A 2-way repeated measures analysis of variance revealed that extensor mechanism attachment site and CDI both significantly affected changes in MPFC length from 0° to 90° (P < .0005). Point QT displayed the greatest length change (mean ± SD, 13.90 ± 2.98 mm) at CDI 1.0. In contrast, mean length change at point MP (2.72 ± 4.43 mm) was relatively isometric, with minimal changes in length seen throughout flexion at CDI 1.0.
Mean Changes in Length for the MPFC at Each Extensor Mechanism Attachment Site Occurring Between 0° and 90° of Knee Flexion a
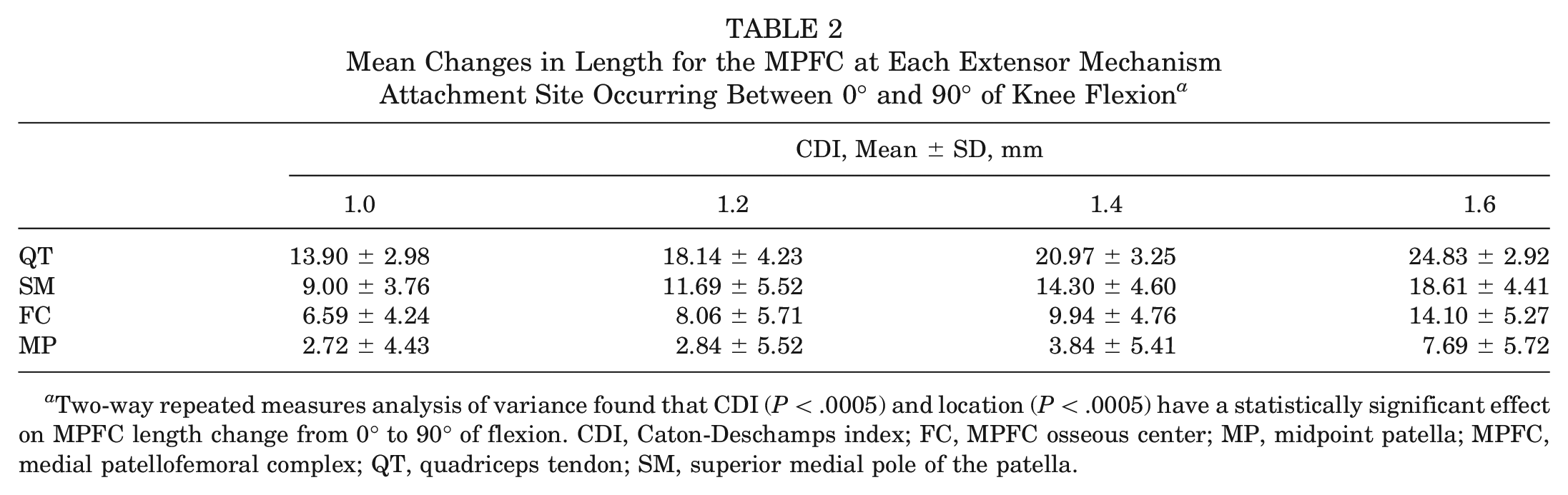
Two-way repeated measures analysis of variance found that CDI (P < .0005) and location (P < .0005) have a statistically significant effect on MPFC length change from 0° to 90° of flexion. CDI, Caton-Deschamps index; FC, MPFC osseous center; MP, midpoint patella; MPFC, medial patellofemoral complex; QT, quadriceps tendon; SM, superior medial pole of the patella.
Effect of Patella Alta on Length Changes From 0° to 90° of Flexion
Length changes based on CDI and extensor attachment location are presented in Figure 3. To evaluate the relationship between CDI and MPFC change in length from 0° to 90° of flexion, pairwise comparisons were analyzed among CDI cohorts. There was a significant difference in change in length between CDI 1.0 and 1.4 (P = .038) and 1.0 and 1.6 (P = .004). No statistically significant differences were seen between CDI 1.0 and 1.2 (P = .351). Length changes among CDIs were then investigated at each extensor attachment site (Table 3). At the proximal locations (QT and SM), comparisons among all the CDI combinations yielded significance (P < .05), except when CDI 1.0 and 1.2 were compared at both locations. In the distal locations (FC and MP), fewer CDI comparisons yielded statistical significance.
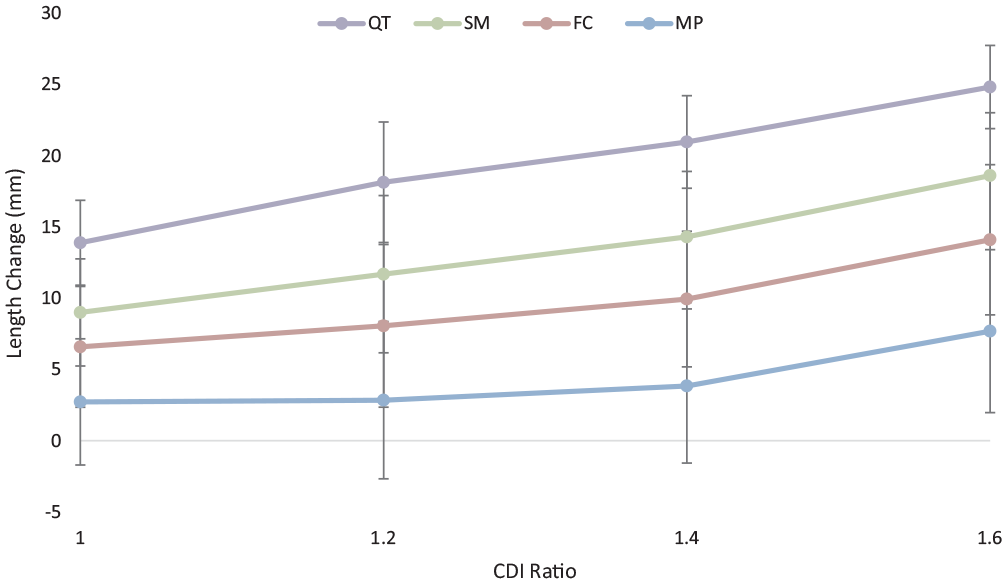
The length change from 0° to 90° for 4 points along the medial patellofemoral complex extensor mechanism— midpoint patella (MP), patellar footprint center (FC), superior medial pole of the patella (SM), and quadriceps tendon (QT)—relative to Caton-Deschamps index (CDI) 1.0, 1.2, 1.4, and 1.6. MPFL, medial patellofemoral ligament.
Results of Comparing Length Changes at Each Location by CDI Value a
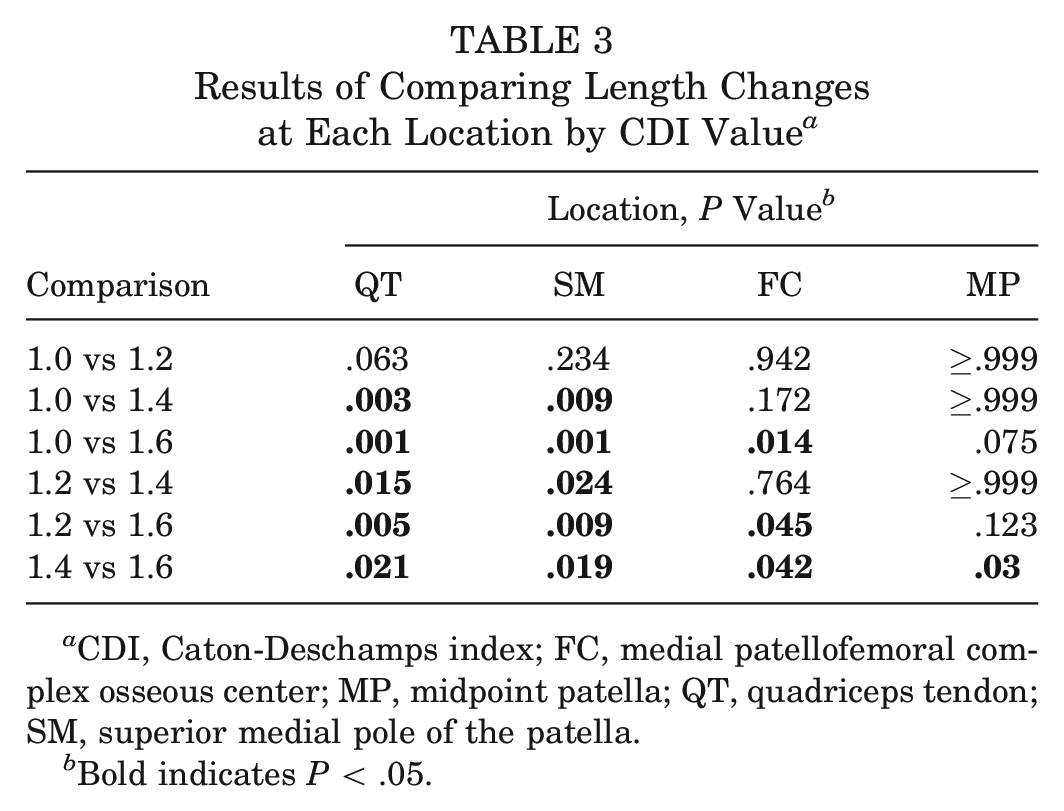
CDI, Caton-Deschamps index; FC, medial patellofemoral complex osseous center; MP, midpoint patella; QT, quadriceps tendon; SM, superior medial pole of the patella.
Bold indicates P < .05.
Equivalent Extensor MPFC Attachment Points at Different Patellar Heights
MPFC length changes at CDI 1.0 were compared with length changes under patella alta conditions from 0° to 90° of flexion with paired t tests. As CDI increased, the length changes of the distal locations (MP and FC) were similar (P > .05) to the proximal length changes at CDI 1.0 (Table 4, Figure 4). For example, the length change at the QT location at CDI 1.0 was similar to that of the FC location at CDI 1.6 (P = .928).
Results of Comparing Length Changes With Each Location at CDI 1.0 a
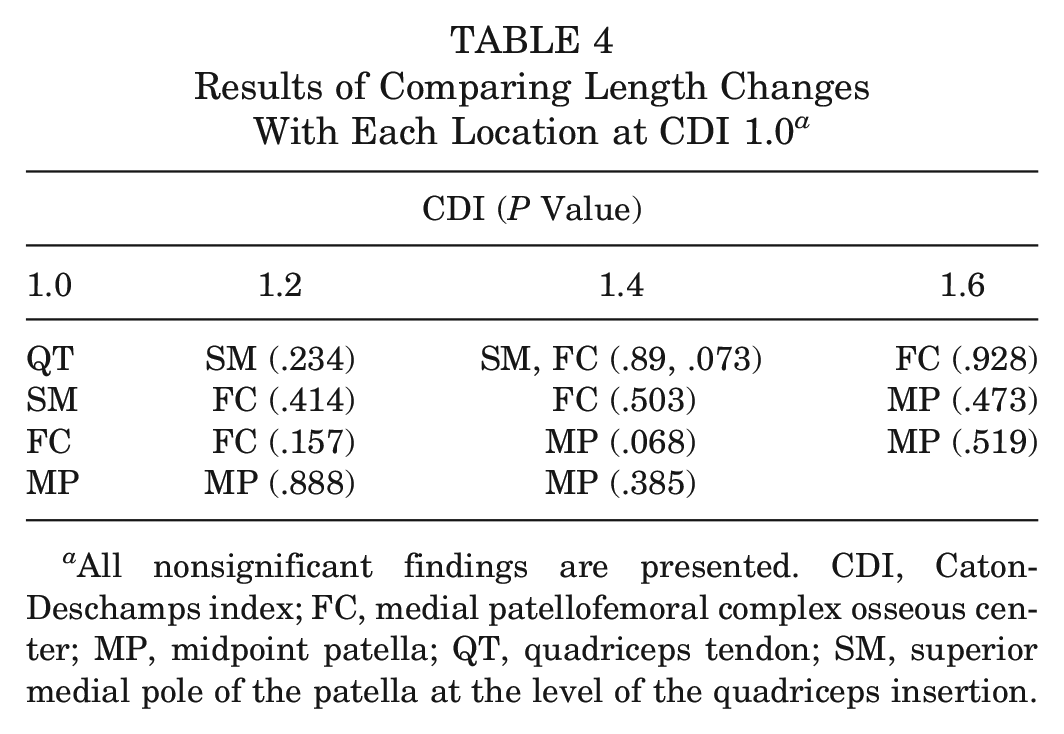
All nonsignificant findings are presented. CDI, Caton-Deschamps index; FC, medial patellofemoral complex osseous center; MP, midpoint patella; QT, quadriceps tendon; SM, superior medial pole of the patella at the level of the quadriceps insertion.
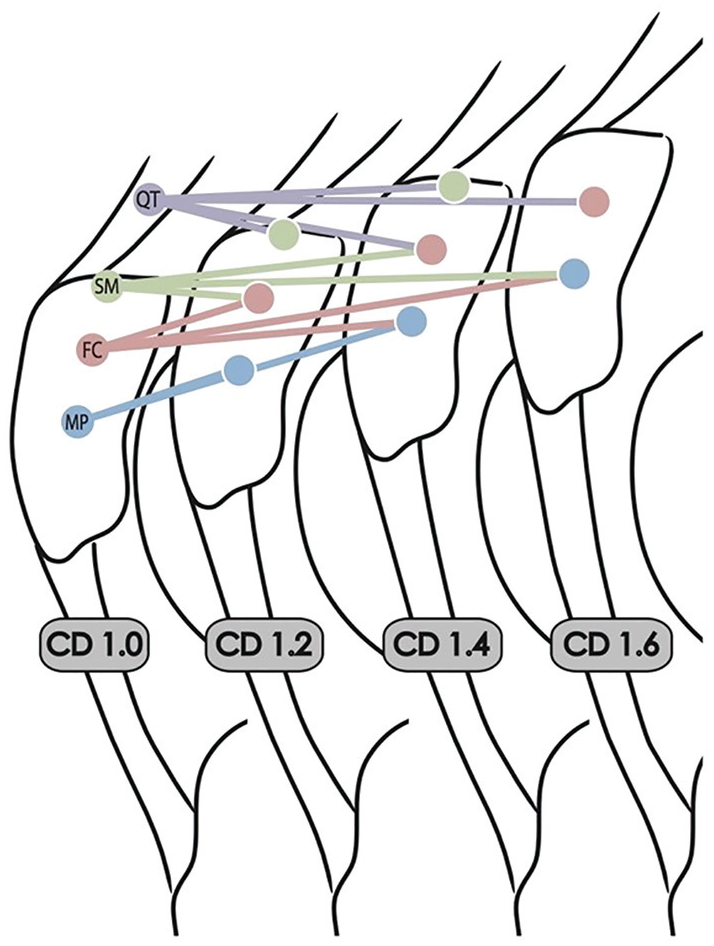
Relative patellar height with increased patella alta and where each attachment point is aligned with its equivalent position in each setting. Each circle represents the location of the measurement at each Caton-Deschamps index (CD). Each line represents locations that had similar length changes (P > .05). FC, medial patellofemoral complex osseous center; MP, midpoint patella; QT, quadriceps tendon; SM, superior medial pole of the patella.
Effect of Patella Alta on Length Changes Throughout Knee Flexion
The most distal (MP) and proximal (QT) locations were then compared at CDI extremes of 1 and 1.6 to evaluate the relationship between MPFC length and flexion angle (Figure 5). A negative linear relationship was observed between degree of flexion and MPFC length at the QT point with CDI 1.0 (r = −0.484; P = .002) and 1.6 (r = −0.692; P < .0005), illustrating constant loosening through flexion (Table 5). No statistically significant differences were observed when the length at the MP location at CDI 1.0 and 1.6 was compared at varying degrees of flexion, except at 0° of flexion (P = .017). In contrast, length difference was significant at all degrees of flexion at the QT location in CDI 1.0 as compared with 1.6. Analysis of the MP location at CDI 1.0 showed no significant differences in length at different degrees of flexion. In contrast, at the MP location at CDI 1.6, significant differences were only seen at 0° (vs 90°, P = .027; vs 60°, P = .044; vs 40°, P = .016; vs 20°, P = .044). At the QT location at CDI 1.0, there were significant differences at 0° and 20° (0° vs 60°, P = .001; 0° vs 90°, P < .0005; 20° vs 90°, P = .005). At CDI 1.6 at the QT location, significant differences were also observed at 0° and 20° (0° vs 60°, P < .0005; 0° vs 90°, P < .0005; 20° vs 90°, P = .03). An evaluation of length change between degree increments showed similar results, although changes at QT 1.0 did not reach significance (Table 5).
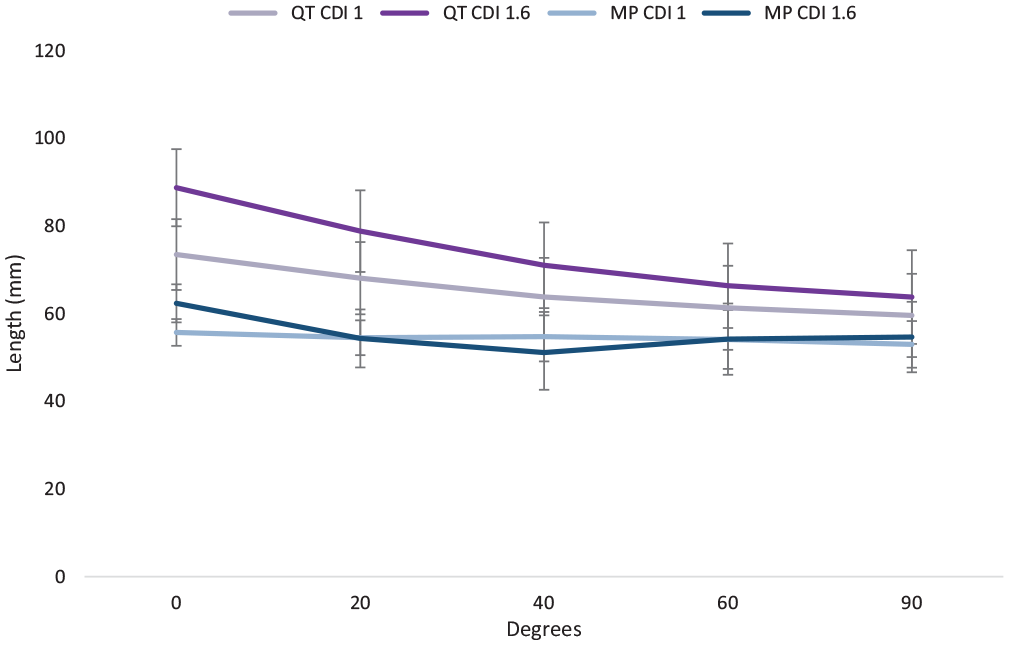
Absolute length of the most proximal (quadriceps tendon [QT]) and distal (midpoint patella [MP]) aspects of the extensor mechanism presented at 2 Caton-Deschamps index (CDI) ratios (1 and 1.6). MPFL, medial patellofemoral ligament.
Median Length Change for the QT and MP Through Flexion at Each Tested CDI Value a
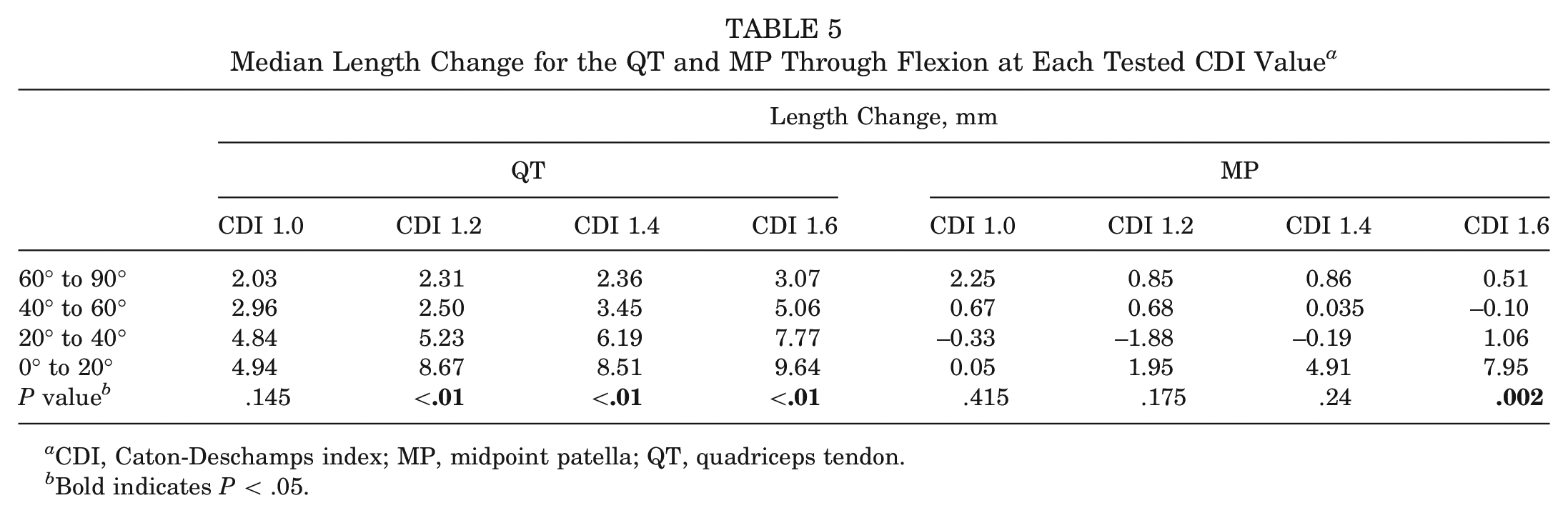
CDI, Caton-Deschamps index; MP, midpoint patella; QT, quadriceps tendon.
Bold indicates P < .05.
Discussion
The main finding of this study was that patella alta significantly affects MPFC length changes, and these changes were exaggerated in the more proximal patellar attachment points (QT and SM). In particular, this study showed that the proximal aspects (QT and SM) of the MPFC, which attach to the QT, have a significantly greater change in length as compared with the distal aspects, which attach to the MP. Furthermore, these differences in length changes are amplified as patella alta increases in severity (increasing CDI values). In addition, our results suggest a progressive loosening at the QT point during flexion from 0° to 90° at CDI 1.0 and CDI 1.6. In contrast, the distal aspect of the MPFC at the MP location at CDI 1.0 exhibited no significant change in length through flexion. With significant patella alta (CDI 1.6), the MPFC demonstrated isometry at MP from 20° to 90°, with 0° being the only point where a significant length difference was observed.
For the aforementioned reasons, the MPFC may more accurately be viewed as 2 entities, given the differences in length changes through flexion at the proximal and distal aspects of the MPFC. We hypothesized that the length of the distal MPFC corresponds with the curvature of the femur (Figure 6). Based on this model, the proximal points, such as point QT, will increase in length linearly as they track along the linear aspect of the femur. In comparison, the more distal points, such as point MP, track along the radial curvature of the femur, thus causing its length to remain relatively constant. However, in the presence of significant patella alta (CDI 1.6), the distal MPFC now has to track along the linear aspect of the femur, increasing its relative length. This model explains the significant change in length seen at the MP point at CDI 1.6 between 0° and all other degrees of measured flexion.
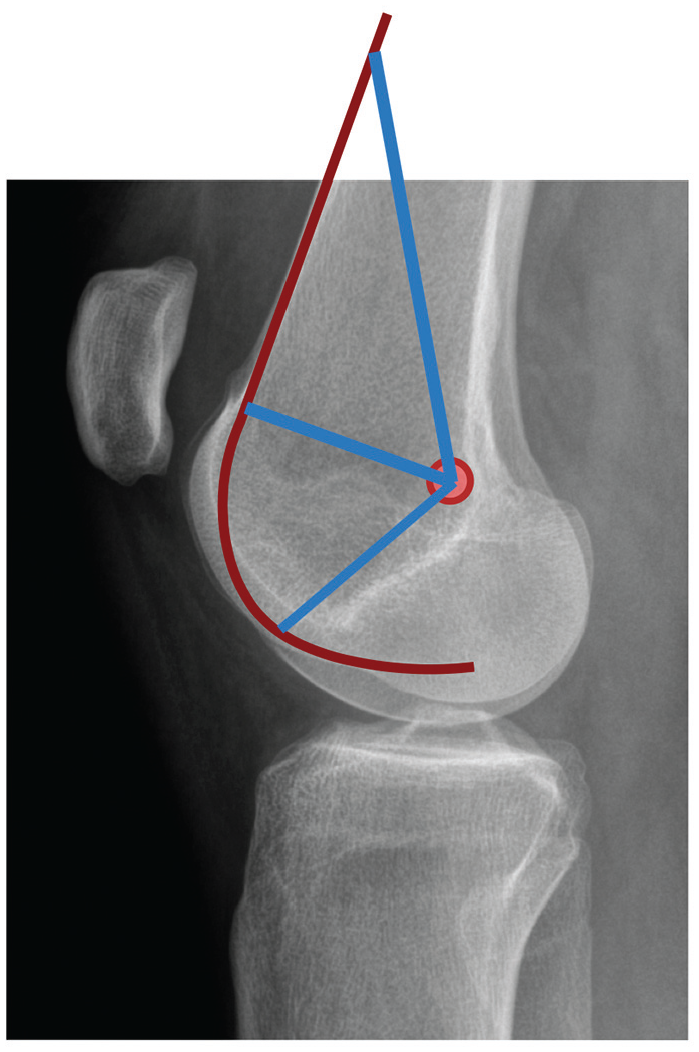
The proposed relationship between femoral curvature and medial patellofemoral complex length.
These findings are important when considering graft attachment sites in patients with moderate to severe patella alta who are undergoing MPFL or MQTFL reconstruction, as using an alternative attachment site or decreasing the magnitude of patella alta may provide superior biomechanical results. Our results suggest that the length changes at varying CDI ratios are not linear as distances increase more quickly as the patella moves proximal to the cam region of the distal femur. Furthermore, our findings suggest a length change equivalence from proximal extensor mechanism attachments at CDI 1 (QT, SM) to distal sites (FC, MP) at higher CDI. This illustrates that it is important to understand the differing biomechanical properties of the different aspects of the MPFC, and one should consider setting lengths individually when using 2 bundles for a MPFC reconstruction (MQTFL and MPFL).
Our results are analogous to previous studies demonstrating that MPFL length changes occur when the femoral fixation location is altered. For example, in a biomechanical study, Stephen et al 15 showed that shifting the attachment point of an MPFL graft distally resulted in a length change of 9.1 mm, while moving the insertion proximally resulted in a 6.4-mm length change. This idea has also been investigated clinically. Matsushita et al 12 analyzed 44 knees and found that nearly 30% showed unfavorable isometry patterns, in part defined as a large length change from 0° to 90°. Furthermore, they found that alterations in femoral positioning of the graft was the largest contributor to having an unfavorable length pattern. These studies reinforce the clinical significance of the present study’s findings.
A reliable clinical algorithm has not yet been defined for the treatment of patellar instability, especially in the presence of patella alta. Recent studies have suggested that adjustment of the femoral fixation site may be appropriate when reconstructing knees with elevated patellar heights. 17 However, our results support the idea that the MPFC should be considered as 2 separate entities (proximal MQTFL and distal MPFL) because of their unique length change properties and should thus be set accordingly intraoperatively. In addition, an alternative distal graft insertion location may be considered in patients with severe patella alta when it is not being corrected. An improved understanding of how patella alta affects the anisometry of the MPFC may help determine the proper surgical management of patellar instability and advance techniques in MPFL reconstruction. In this light, proximal soft tissue–based reconstructions will show more loosening before engagement in the trochlea in the setting of patella alta as compared with patella-based reconstructions. Future studies are needed to evaluate the clinical correlates of these findings.
There are several limitations with this study. First, this is a cadaveric model; therefore, it is possible that our model does not perfectly reflect load distribution of the quadriceps in a native knee. Second, all knees in this study were manipulated to create different CDI values of patella alta. Native patella alta may have slightly dissimilar biomechanical properties that are not reflected in our model of patella alta. Furthermore, the tension in the patellar tendon and in the FiberWire configuration were not compared and may have been different. However, the FiberWire construct remained taut and allowed for adequate patellar tracking through flexion, so it is unlikely that this had any effect on our results. Last, this study heavily relies on the accuracy of identifying the femoral footprint of the MPFC, and slight inaccuracies could affect our findings.
In conclusion, anisometry varies with location of the patellar attachment and with patella alta within the MPFC. Specifically, the proximal aspect of the MPFC demonstrated constant loosening through flexion at normal height and with patella alta. In contrast, the distal aspect of the MPFC retains a relatively constant length at 0° to 90° of flexion at a CDI 1.0 and from 20° to 90° at CDI 1.6. Furthermore, distal sites (MP and FC) at CDI 1.6 were found to have a similar length change to proximal sites (QT and SM) at CDI 1.0, illustrating that distal attachments in the setting of patella alta may have similar length changes to proximal attachments in patients with normal patellar height. Therefore, proximal soft tissue–based reconstructions will demonstrate significantly greater length changes in the setting of patella alta as compared with osseous-based reconstructions. Further clinical outcomes are necessary to determine the clinical relevance of these findings and their effect on different types of MPFC reconstruction techniques.
Footnotes
Submitted October 4, 2019; accepted February 4, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.J.C. has received research support from Aesculap/B. Braun, Arthrex, National Institutes of Health, and Regentis; other financial or material support from Athletico, JRF Ortho, and Smith & Nephew; royalties from Arthrex and DJO; consulting fees from Acumed, Anika Therapeutics, Arthrex, Bioventus, Flexion Therapeutics, Geistlich Pharma, Genzyme, Pacira Pharmaceuticals, Smith & Nephew, Vericel, and Zimmer Biomet; speaking fees from Arthrex and Lifenet Health; hospitality payments from GE Healthcare; educational support from Medwest; and honoraria from Vericel. B.J.C. also holds stock or stock options in Bandgrip Inc, Ossio, and Regentis. J.F. has received research support from Active Implants, Arthrex, Fidia, JRF Ortho, Vericel, and ZimmerBiomet; consulting fees from Aastrom Biosciences, Aesculap/B. Braun, Arthrex, Cartiheal, Cook Biotech, DePuy Orthopaedics, Exactech, Moximed, Norvartis, Organogenesis, Regentis, RTI Surgical, Samumed Inc, and Orthopedics Inc; and royalties from Arthrex Inc, Biopoly LLC, DePuy Synthes, and Organogensis. J.F. also holds stock or stock options in Ortho Regenerative Tech Inc and MedShape Inc. K.C. has received education payments from Arthrex. J.C. has received education payments from Arthrex and Smith & Nephew. A.B.Y. has received research support from Arthrex and Organogenesis; consulting fees from JRF Ortho and Aastrom Biosciences; and education support from Smith & Nephew, Arthrex, and Medwest Associates. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.