
Abstract
Background:
Core muscle injury (CMI), often referred to as a sports hernia, is a common cause of groin pain in athletes characterized by concomitant injury to the insertion of the adductor longus and the rectus abdominis muscles. Currently, the literature on CMI is sparse with no standardized physical examination tests used in the diagnosis of this type of injury.
Purpose:
To determine the diagnostic accuracy of various physical examination tests in the diagnosis of CMI.
Study Design:
Cohort study (Diagnosis); Level of evidence, 3.
Methods:
A consecutive series of patients evaluated by the senior author with symptoms consistent with CMI were included. Four physical examination tests were routinely performed in these patients by the senior author and were noted in each patient’s chart as positive or negative: (1) pain with resisted cross-body sit-up in figure-of-4 position, (2) pain with straight-leg sit-up, (3) pain with resisted hip flexion in external rotation (external rotation Stinchfield test), and (4) the presence of an adductor contracture. CMI was independently diagnosed by a reference standard (magnetic resonance imaging [MRI]). All MRI scans were read by a musculoskeletal fellowship-trained radiologist. The sensitivity and specificity of each physical examination test alone and in combination were calculated based on this reference standard.
Results:
A total of 81 patients were included in this study. MRI was positive for a CMI in 39 patients (48%) overall. Both the cross-body sit-up test and the presence of an adductor contracture were found to have a sensitivity of 100% (specificity, 3% for both). The external rotation Stinchfield test was found to have the highest specificity of 60% (sensitivity, 15%). The sensitivity of all 4 physical examination tests in combination was found to be 100% (specificity, 0%).
Conclusion:
Certain physical examination maneuvers can be used to assist in the diagnosis of a CMI. The cross-body sit-up test and the presence of an adductor contracture are highly sensitive but nonspecific tests for CMI and therefore should be used in conjunction with diagnostic imaging before deciding on an appropriate treatment course.
Core muscle injury (CMI), also known as athletic pubalgia, is a common cause of groin pain in athletes.11,14 Traditionally known as a “sports hernia,” these injuries often involve abdominal wall weakening or tearing with no abdominal hernia. 8 Rather, these injuries are characterized by concomitant injury to the insertion of the adductor longus and the rectus abdominis muscles on the pubis. First-line treatment for CMI is always nonoperative management, with elective sports hernia repair reserved for refractory cases.3,15
Despite treatment success, the clinical diagnosis of CMI is challenging. This is because of the complex anatomy of the abdominopelvic structures and the many root causes of groin pain, which can include infectious, inflammatory, neoplastic, and traumatic causes. 12 CMI can often be associated with other hip conditions, such as femoroacetabular impingement (FAI).14,16 In addition, referred pain from the lumbar spine as a result of lumbar stenosis at the L2-3 or L3-4 levels, or sacroiliac dysfunction may share similar clinical signs and symptoms.5,8 Abdominal hernias and referred pain from visceral-related causes, such as testicular torsion, are additional sources of groin pain and should be considered. Therefore, accurate and specific physical examination tests are important for the appropriate diagnosis and treatment of CMI. Currently, the literature on CMI is sparse with no standardized physical examination tests used in the diagnosis of this type of injury. The purpose of this study was to determine the diagnostic accuracy of various physical examination tests in the diagnosis of CMI.
Methods
Patient Selection
After institutional review board approval, we performed a retrospective analysis of prospectively collected data on CMI patients. The clinical database of a single sports medicine fellowship–trained orthopaedic surgeon was queried for all patients who underwent CMI repair between June 2016 and April 2019. All surgically treated patients were evaluated by the senior author (A.J.S.) and had symptoms consistent with CMI (ie, groin and/or pubic pain worsened with exertion). These patients were found to have positive findings for CMI on ultrasonogram and were indicated for surgery after 3 months of unsuccessful nonoperative treatment. This included rest and activity modification, nonsteroidal anti-inflammatory drugs, physical therapy, and injections. From the queried list, patients who underwent magnetic resonance imaging (MRI), positive or negative, were extracted and included for final analysis (n = 81). Regardless of the MRI results, patients underwent surgery if there was high suspicion for CMI based on history, physical examination, and ultrasound findings. For all patients, surgical treatment consisted of CMI repair via a mini-open approach, which has been previously described. 15 Given that the mechanism of injury for CMI typically occurs during resisted hip flexion and adduction, this surgical correction involved lengthening of the adductor longus tendon, because of its relationship with the conjoined tendon, and direct repair of the rectus abdominis to the pubis. 15 Correction of both anatomic structures has shown favorable outcomes among patients with rectus abdominis and adductor longus injuries.9,10
Variables
All patients who had symptoms consistent with CMI underwent a thorough physical examination. To narrow the differential diagnoses, the hip, pelvic, groin, and thigh region were assessed. Among CMI patients, point tenderness was often localized about the pubic symphysis, the lower rectus abdominis musculature, the anteromedial thigh, the external ring of the inguinal canal, and the pubic tubercle. Four physical examination tests were documented in each patient’s chart as positive or negative: (1) pain with resisted cross-body sit-up in figure-of-4 position, (2) pain with straight-leg sit-up, (3) pain with resisted hip flexion in external rotation (external rotation Stinchfield test), and (4) the presence of an adductor contracture (Figure 1). The presence of an adductor contracture was assessed by placing the patient supine and in a figure-of-4 position. The test was considered positive if (1) the affected leg could not be positioned parallel to the floor and (2) the adductor region was tight upon palpation. This was to ensure that the limited range of hip motion was because of the adductor musculature and not a consequence of intra-articular hip pathology. The results of the physical examination tests were extracted to calculate their respective sensitivity and specificity. Other tests, including the impingement test (flexion adduction internal rotation), were performed to assess for FAI. Concomitant CMI repair and arthroscopic labral repair/femoroplasty was performed under the same anesthetic in patients with a positive impingement test, less than 10° of internal rotation, and labral tears on MRI and radiographs consistent with hip impingement (Figure 2). In these cases, repair of the CMI was performed first, after which the patient was redraped and the hip arthroscopy procedure was performed.
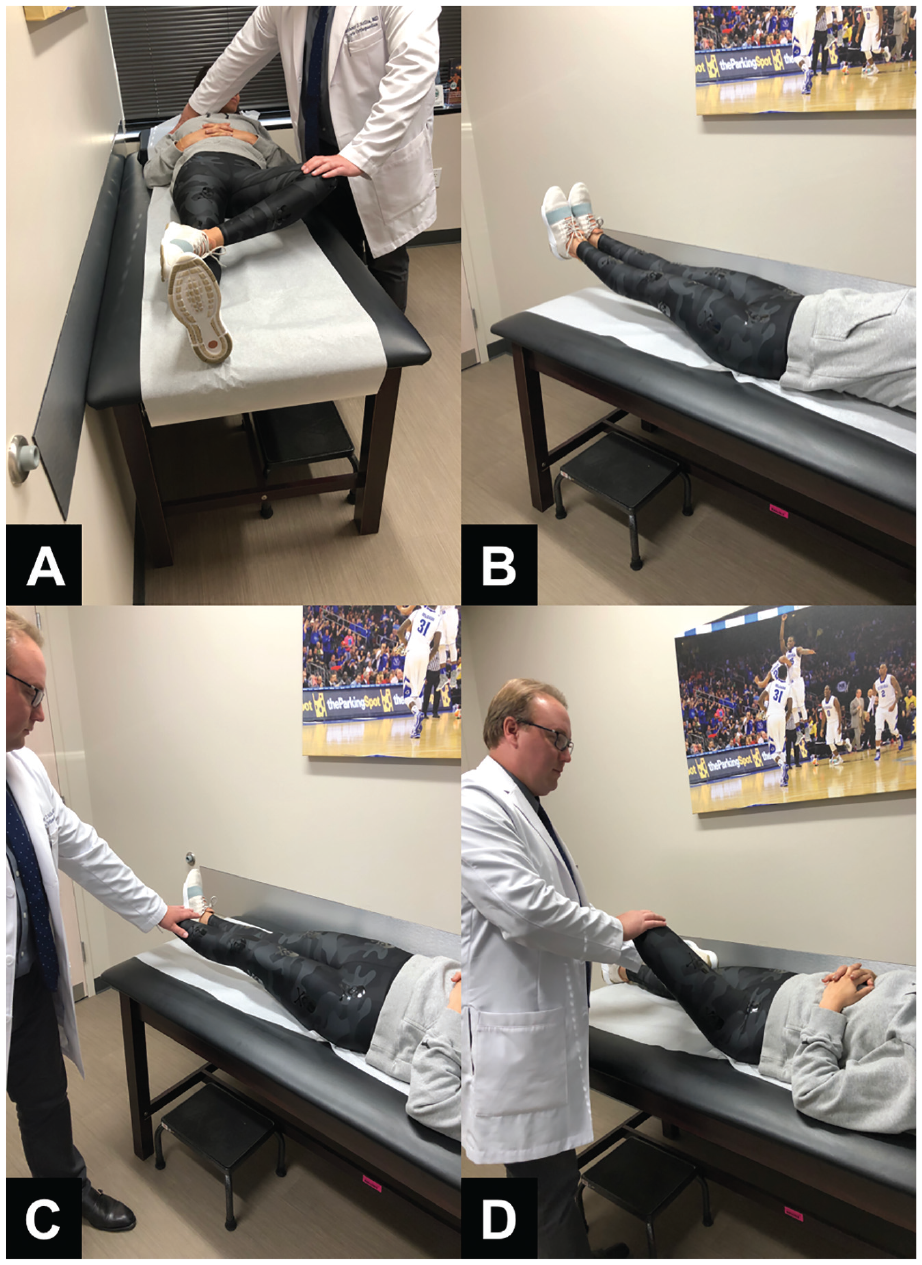
Physical examination tests. (A) A resisted cross-body sit-up is performed by bringing the contralateral shoulder to the knee on the affected side against resistance. Pubic/groin pain indicates a positive test. (B) A straight-leg sit-up is an abdominal crunch with legs and shoulders elevated 8 to 10 inches off the examining table. Pubic/groin pain indicates a positive test. (C) The external rotation Stinchfield test is performed with resisted hip flexion with the leg in external rotation. Pubic/groin pain indicates a positive test. (D) The presence of an adductor contracture is measured in the figure-of-4 position.
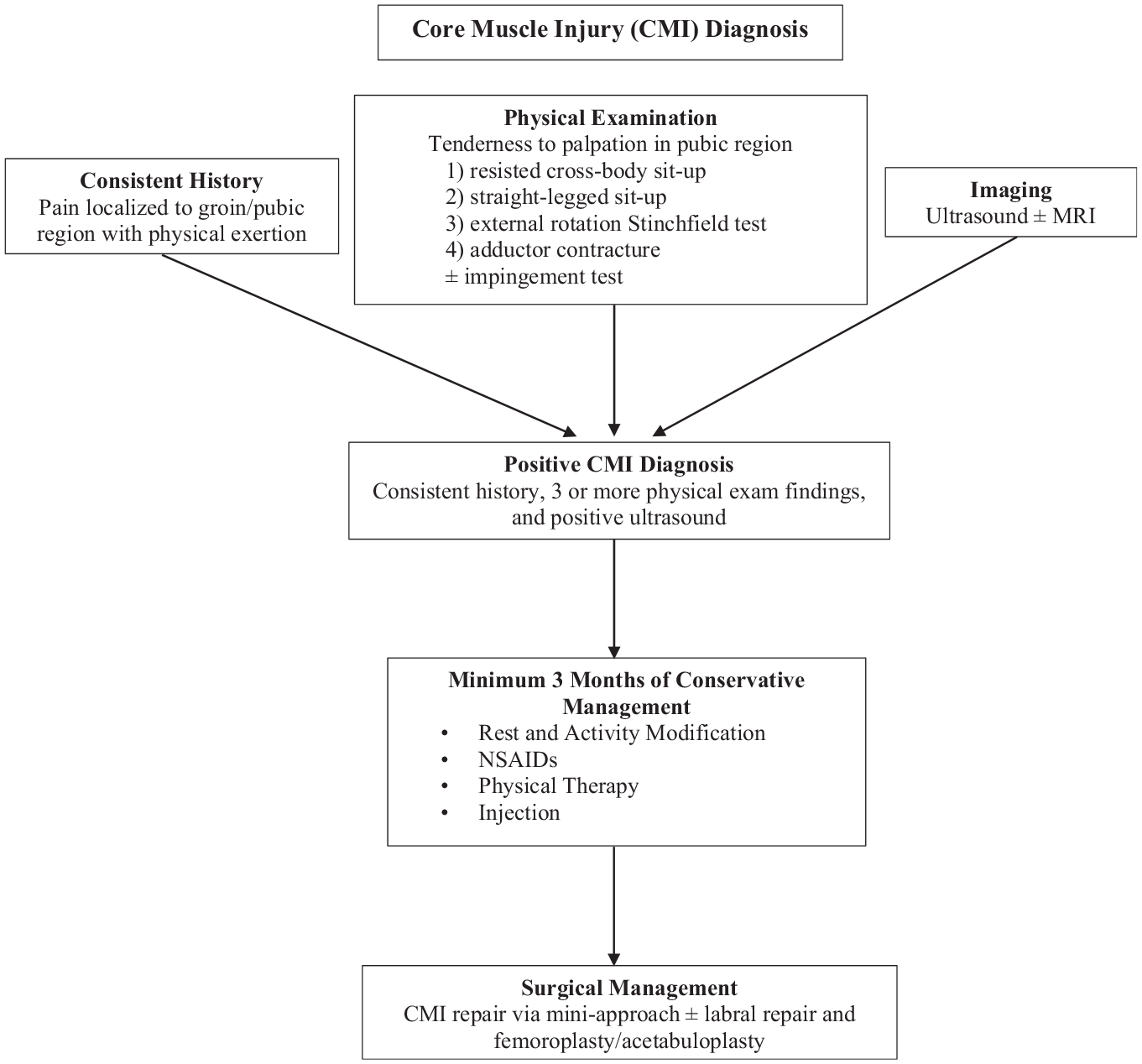
Systematic algorithm to diagnose and treat core muscle injury. MRI, magnetic resonance imaging; NSAID, nonsteroidal anti-inflammatory drug.
Imaging Protocol
Each patient underwent an ultrasonogram by a fellowship-trained, board-certified sports medicine specialist (M.A.K.). Ultrasound was considered positive for CMI if hypoechoic areas along the distal rectus insertion and the proximal adductor longus tendon were observed on transverse and linear views (Figure 3). In addition, each patient underwent an MRI survey of the pelvis. The MRI scan was read by a musculoskeletal fellowship-trained radiologist and used as a reference standard. Specifically, the MRI examination was considered positive if a tear along the rectus abdominis-adductor aponeurosis was visualized. Other findings associated with an aponeurotic lesion, including abnormal marrow signal intensity and a secondary cleft sign, were also noted as a positive MRI examination. 12 On MRI scans, some patients had bone marrow edema or osteitis pubis, FAI, and/or irregularities of the symphysis, but tears of the rectus abdominis and adductor longus tendons were not appreciated and were therefore considered negative. MRI was chosen as the reference standard as it is currently accepted as an appropriate imaging study for the diagnosis of CMI. The current literature supports MRI as an appropriate diagnostic tool, as the sensitivity and specificity for rectus abdominis and adductor injuries range from 68% to 100%. 2 All patients in this study underwent surgery for a CMI taking into account a combination of history and physical examination, positive ultrasound findings, and MRI findings. Thus, no single test was considered the “gold standard” in making a diagnosis of CMI. Rather, a combination of history, physical examination, and imaging findings were collectively used to arrive at a diagnosis.
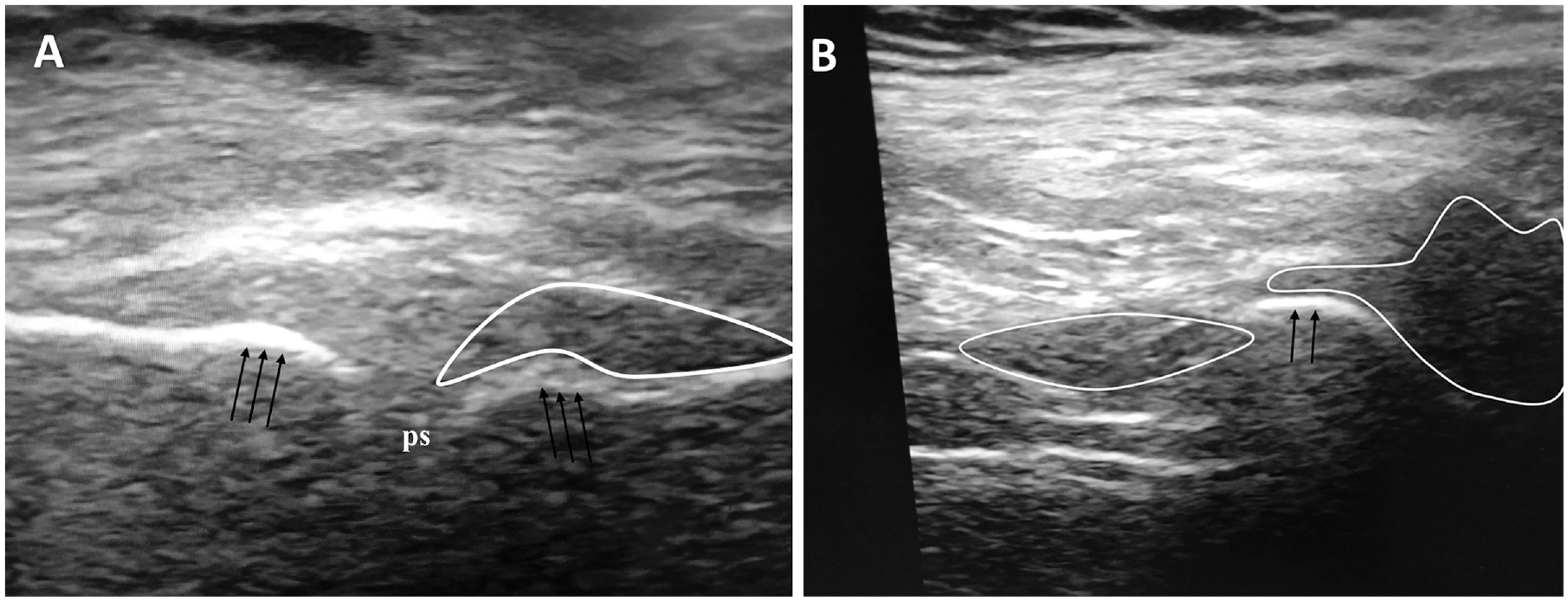
(A) Transverse ultrasound demonstrating hypoechoic area (white outline) about the right pubic body (black arrows) consistent with core muscle injury. (B) Longitudinal ultrasound demonstrating asymmetric hypoechoic heterogeneous areas of soft tissue (white outlines) over the pubic symphysis (ps; black arrows) indicating core muscle injury.
Statistical Analysis
All data were de-identified in an Excel spreadsheet (Microsoft Corp). Data analysis was performed utilizing SPSS version 20 (IBM Corp). The sensitivity and specificity of each physical examination test alone and in combination were calculated based on the reference standard of MRI. An α value of <.05 was considered statistically significant.
Results
A total of 81 patients met inclusion criteria for this study, with a mean age of 32.7 years at the time of surgery (Table 1). Men accounted for 78 of the 81 (96%) patients included. MRI scans were read as positive for a CMI in 39 patients overall (48%). A total of 75 patients (93%) were evaluated because of a sports-related injury, while 6 patients (7%) were seen for reasons unrelated to sporting activities. Soccer was the most common sport played among injured patients (27%), followed by weight lifting (15%). Although 16% of patients practiced high-performance sports, most patients played sports recreationally. A total of 15 patients had a diagnosed symptomatic labral tear and underwent arthroscopic labral repair and femoroplasty at the time of the CMI repair.
Patient Characteristics a
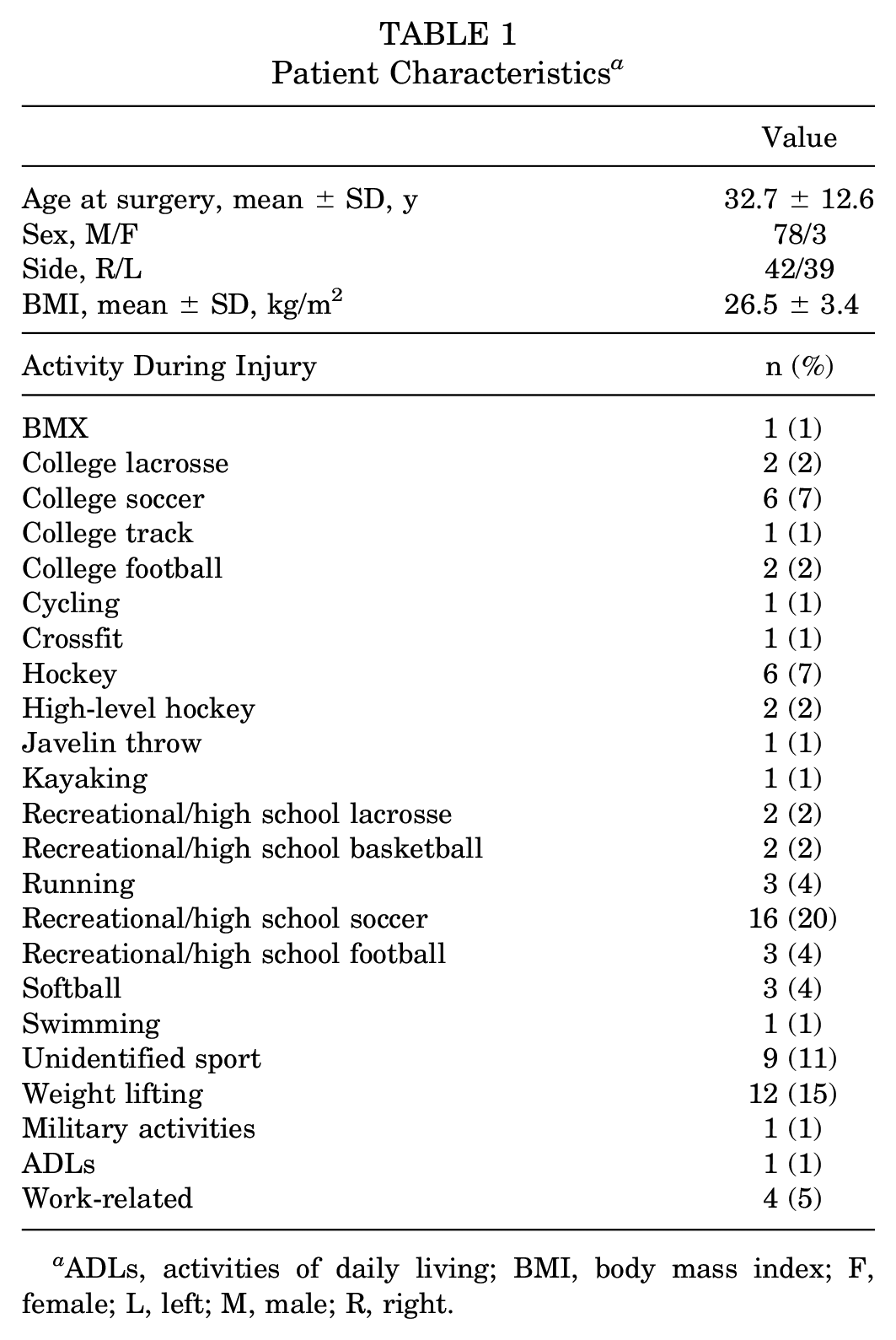
ADLs, activities of daily living; BMI, body mass index; F, female; L, left; M, male; R, right.
Both the cross-body sit-up test and the presence of an adductor contracture were found to have a sensitivity of 100% (0 false negatives) (Table 2). The external rotation Stinchfield test was found to have the highest specificity of 60% (Table 3). The sensitivity of all 4 physical examination tests in combination was found to be 100% for a positive MRI examination for CMI (specificity, 0%).
Physical Examination Test Results a
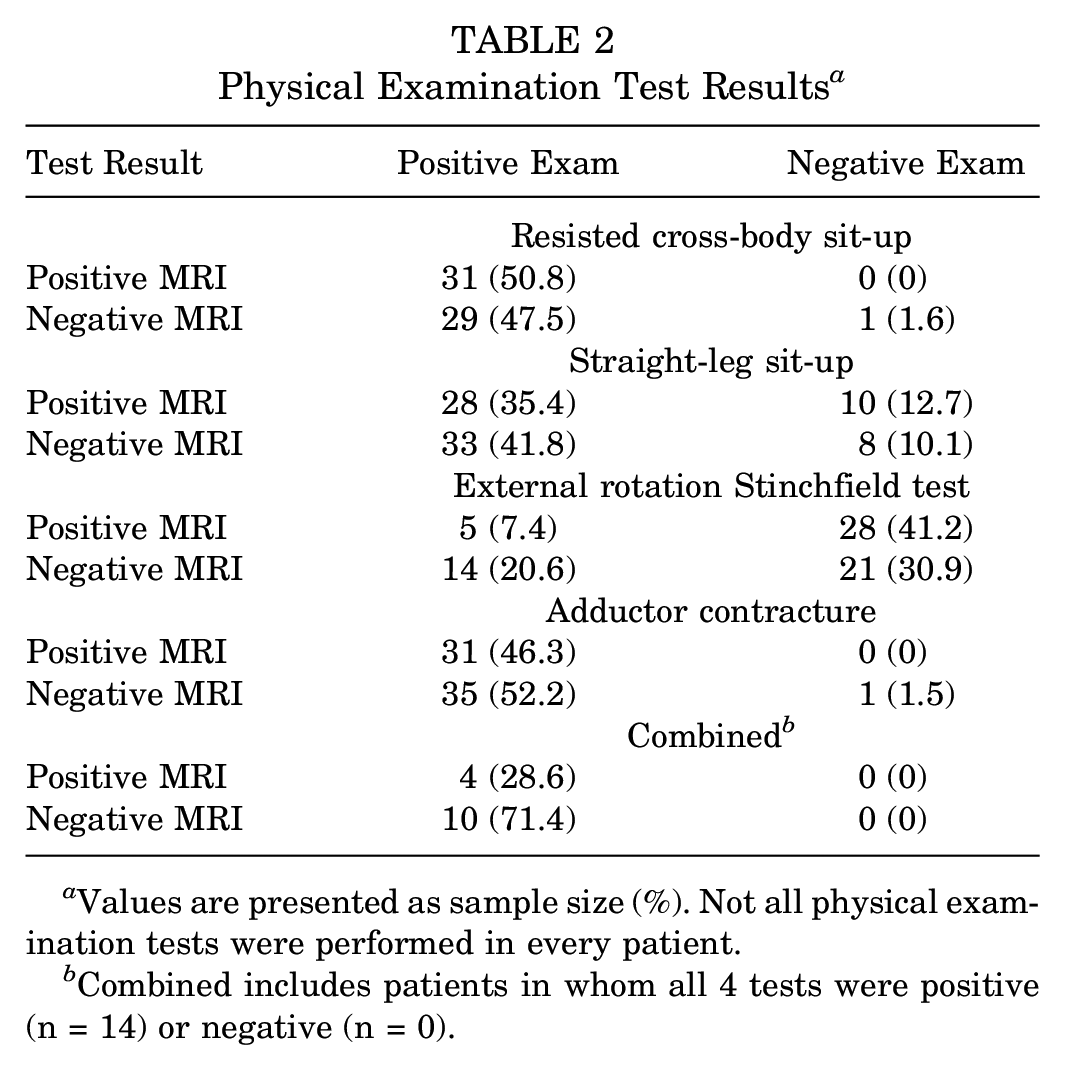
Values are presented as sample size (%). Not all physical examination tests were performed in every patient.
Combined includes patients in whom all 4 tests were positive (n = 14) or negative (n = 0).
Physical Examination Diagnostic Test Results a
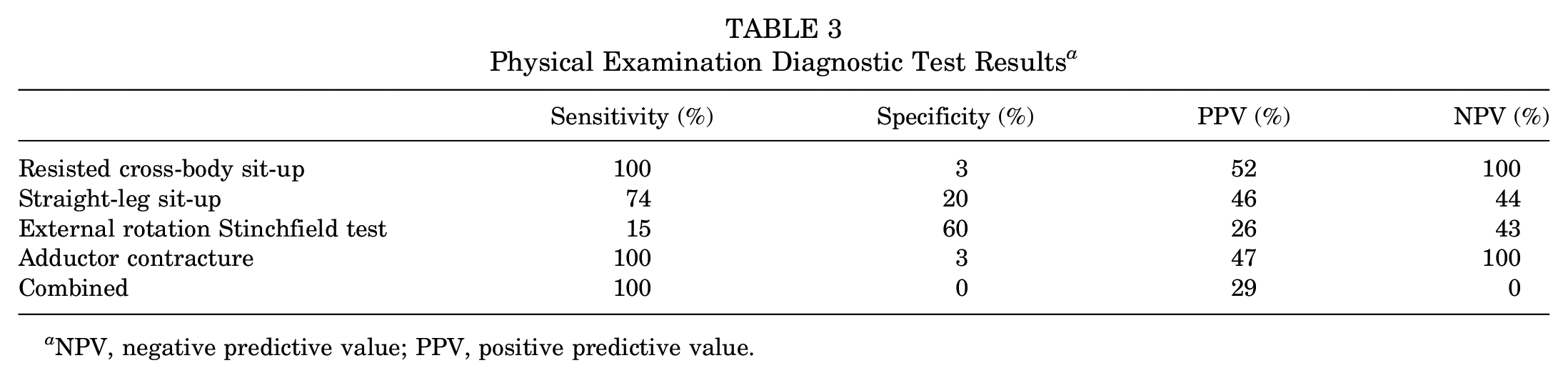
NPV, negative predictive value; PPV, positive predictive value.
Discussion
Groin pain after a sports-related injury can be secondary to CMI, otherwise known as a sports hernia.6,13,14 Twisting motions, sudden core movements, and rapid changes in direction and speed characteristically result in this type of injury. 7 Despite its prevalence among athletes, CMI remains difficult to diagnose. Challenges in making a definitive diagnosis arise because of the nonspecific symptoms and clinical findings during examination. 1 As a result, there is a lack of standardized physical examination tests for the diagnosis of CMI. Therefore, this study evaluated the diagnostic accuracy of several physical examination tests to improve the detection of CMI. Our results demonstrated that the cross-body sit-up test and the presence of an adductor contracture were correlated with a high sensitivity, while the external rotation Stinchfield test was associated with moderate specificity in the diagnosis of CMI.
Several studies have cited the utilization of a resisted sit-up or crunch to re-create symptoms and assist in the diagnosis of CMI. Garvey et al 4 described the clinical presentation of sportsman hernia and noted the re-creation of symptoms with this maneuver. In another prospectively collected database study, Meyers et al 10 evaluated 276 patients who underwent evaluation for suspected athletic pubalgia, or sports hernia. Of the 157 patients who underwent rectus abdominis tendon repairs, 72 (46%) had pain with a resisted sit-up. 10 In a review article, Ross et al 14 described specific physical examination maneuvers to assist in the identification of CMI. The authors stated that resisted range of motion maneuvers, including hip adduction in both flexion and extension, may elicit pain in relation to the implicated abdominopelvic structures. 14 However, no study has made mention of the cross-body sit-up test or the presence of an adductor contracture. In the present study, the authors found a 100% sensitivity of both of these tests in diagnosing CMI using MRI.
Our study also demonstrated that the test with the highest specificity was the external rotation Stinchfield test, that is, resisted hip flexion in external rotation. This physical examination maneuver has not been readily cited as a standard technique in the clinical diagnosis of CMI. The external rotation Stinchfield manuever tests both the rectus abdominis (via resisted hip flexion) and the adductor attachments (via hip external rotation), making it a more specific test for this type of injury. A thorough history and physical examination are the most important aspects in accurately identifying the root cause of an athlete’s groin pain and determining the appropriate treatment. By improving the clinical evaluation of CMI, we can reinforce our diagnostic capabilities and treatment options and allow athletes to return to sports earlier. Nonetheless, the best diagnostic tests are those with both high sensitivity and high specificity. Given that this is challenging in clinical practice, our goal was to determine how to best diagnose CMI. Our results show favorable but imperfect results. In particular, the specificity of the resisted cross-body sit-up test and the presence of an adductor contracture were each 3%, and the specificity of the combination of all tests was 0%. Thus, a positive finding cannot be relied upon to rule in a CMI with regard to these tests. Despite this, we believe this study adds to the literature and will serve as a stepping-stone in improving the diagnosis of CMI.
The limitations of this study should be noted. The authors included the term “sports hernia” to describe this type of injury. This term is considered a misnomer, as there is no true hernia in this condition, 1 and we recognize its misuse in this context. However, we included the term nonetheless because historically CMI was described in this manner and much of the literature labels this injury as a sports hernia. Additionally, we utilized MRI as the reference standard in diagnosing CMI. However, MRI findings may be nonspecific, and pathologic findings may not always appear on MRI. As such, MRI scans were mainly used to exclude other possible causes of groin pain. However, improved knowledge regarding the anatomic structures and pathophysiological changes associated with CMI has allowed improved imaging techniques. 12 In a clinical review article, Elattar et al 2 reported a 68% sensitivity and 100% specificity for rectus abdominis injuries and 86% sensitivity and 89% specificity for adductor pathology. As such, we believe that MRI scans read by a musculoskeletal fellowship-trained radiologist was the most appropriate diagnostic reference for this study. However, MRI may result in false-negative results and ultrasound may provide further utility in the diagnosis of CMI variance. Last, this is a single-surgeon series, and to broaden the applicability of these tests in the diagnosis of CMI, participation of multiple centers specializing in the treatment of these patients could further validate our results.
Conclusion
Certain physical examination maneuvers can be used to assist in the diagnosis of a CMI. The cross-body sit-up test and the presence of an adductor contracture are highly sensitive but nonspecific tests for CMI and therefore should be used in conjunction with diagnostic imaging before deciding on an appropriate treatment course.
Footnotes
Acknowledgements
The authors would like to acknowledge Edward Milman, MD, for reading all MRIs for the patients in this study.
Submitted September 15, 2019; accepted March 24, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.A.K. has received royalties from Zimmer Biomet; hospitality payments from Zimmer Biomet, Lima USA, Flexion Therapeutics, UOC USA Inc, Pacira Pharameuticals Inc, and Think Surgical Inc; consulting fees from Zimmer Biomet, Flexion Therapeutics, Pacira Pharaceuticals Inc, and Medical Device Business Services; honoraria from Pacira Pharmaceuticals Inc; and fees for services other than consulting from Pacira Pharmaceuticals Inc and Mallinckrodt. T.T. has received hospitality payments from Covidien. A.J.S. has received research support from Isto Biologics; is a paid consultant for Mitek; and has received consulting fees from Medical Device Business Services, DePuy Synthes, and DePuy Orthopaedics, and hospitality payments from DePuy Synthes, DePuy Orthopaedics, and Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.