
Abstract
Background:
Injuries to the hamstring complex most commonly involve the proximal musculotendinous junction of the long head of the biceps femoris (MTJ-BFlh). Nonoperative management of these injuries is associated with prolonged rehabilitation and high risk of recurrence. To our knowledge, the surgical management of acute MTJ-BFlh injuries has not been previously reported.
Hypothesis:
Surgical repair of acute MTJ-BFlh injuries enables return to sporting activity with low risk of recurrence.
Study Design:
Case series; Level of evidence, 4.
Methods:
A total of 64 patients (42 male and 22 female) undergoing surgical repair of acute MTJ-BFlh injuries were included. Predefined outcomes were recorded at regular intervals after surgery. Mean follow-up time after surgery was 29.2 months (range, 24.0-37.1 months).
Results:
All study patients returned to their preinjury levels of sporting activity. Mean ± SD time from surgical intervention to return to sporting activity was 13.4 ± 5.1 weeks. Three patients had reinjury at the operative site: 1 (1.6%) with MTJ-BFlh injury and 2 (3.2%) with myofascial tears. At 3 months after surgery, patients had improved mean passive straight-leg raise (72.0° ± 11.4° vs 24.1° ± 6.8°; P < .001); increased mean isometric hamstring muscle strength at 0° (84.5 % ± 10.4% vs 25.9% ± 8.9%; P < .001), 15° (89.5% ± 7.3% vs 41.2% ± 9.7%; P < .001), and 45° (93.9% ± 5.1% vs 63.4% ± 7.6%; P < .001); higher mean Lower Extremity Functional Scale scores (71.5 ± 5.0 vs 29.8 ± 6.3; P < .001); and improved mean Marx activity rating scores (9.8 ± 2.2 vs 3.8 ± 1.9; P < .001), as compared with preoperative scores. High patient satisfaction and functional outcome scores were maintained at 1 and 2 years after surgery.
Conclusion:
Surgical repair of acute MTJ-BFlh injuries enables return to preinjury level of sporting function with low risk of recurrence at short-term follow-up.
The hamstring muscles (semimembranosus, semitendinosus, and biceps femoris) are the most commonly injured muscle group in professional athletes and account for approximately one-third of all muscle injuries sustained during sprinting, soccer, and rugby.14,17,21 The proximal musculotendinous junction of the long head of the biceps femoris (MTJ-BFlh) is most frequently injured, 15 as attributed to its long, narrow aponeurosis, which leads to poor dissipation of force from the muscle belly to the tendon at this interface.18,26,30 Nonoperative management of these injuries includes rest, nonsteroidal anti-inflammatory drugs, protected range of movement, and eccentric muscle exercises. 9 Shockwave therapy or injections with corticosteroids or plasma-rich protein have also been used with varying degrees of success.9,30 Limitations of nonoperative treatment include large variations in time for convalescence and high risk of recurrence on return to sporting activity.18,22,35,37,42 Nonoperative treatment is also associated with residual muscle weakness, neurological complications secondary to tethering of the sciatic nerve, and poor return to preinjury level of function.3,4,10,16,31,42 In professional athletes, these injuries are often regarded as career threatening and may lead to premature retirement from sporting activity.37,42
Operative treatment of proximal hamstring injuries is most commonly reserved for injuries that remain refractory to nonoperative treatment or are associated with large, displaced avulsion fractures.13,26,32 Surgical techniques to repair these injuries include reattachment of the avulsed tendon with anchors, debridement of residual tendon with fixation of the injured muscle belly to the adjacent hamstring muscles, endoscopic repair of the avulsed tendon, and iliotibial grafts to reattach chronic retracted tendons to the ischial tuberosity.6,11,13,24,26,27,32 Surgical repair for partial or complete avulsion injuries of the proximal hamstrings is associated with high patient satisfaction, rapid return to sporting activity, and low rates of complications at short-term follow-up.6,12,24,35 However, to our knowledge, there are no existing studies that assess the effect of surgical repair of MTJ-BFlh injuries on postoperative outcomes.
The rationale for undertaking operative intervention in these patients is the prolonged rehabilitation period and high risk of recurrence with nonoperative management of these injuries, as reported within the existing literature and based on the operating surgeon’s experience.37,42,43 Before study commencement, 34 of the 112 patients (21.4%) undergoing nonoperative management of MTJ-BFlh injuries had recurrence of the primary injury within 2-year follow-up. This prompted a change in practice from nonoperative to operative treatment for high-grade MTJ-BFlh injuries. The current study assesses a comprehensive and robust range of study outcomes in a series of patients with high-grade MTJ-BFlh injuries undergoing acute surgical repair and standardized postoperative rehabilitation. The findings of this study will provide an improved understanding of the effects of acute surgical repair of MTJ-BFlh injuries on return to preinjury level of sporting activity, injury recurrence, and functional performance at short-term follow-up.
The primary objective of this study was to assess the effect of operative repair of acute MTJ-BFlh injuries on injury recurrence. The study hypothesis was that operative repair of MTJ-BFlh injuries would lead to low risk of injury recurrence at short-term follow-up. Secondary objectives were to assess the effect of surgical intervention on return to sporting function, patient satisfaction, hamstring muscle strength, straight-leg raise, functional performance, and complications.
Methods
Patient Selection
This prospective study included 64 patients undergoing surgical treatment for acute MTJ-BFlh injuries between March 2015 and September 2016 (Table 1).
Demographics and Baseline Data on Patients Undergoing Surgical Repair of Injuries to the Proximal Musculotendinous Junction of the Long Head of Biceps Femoris a
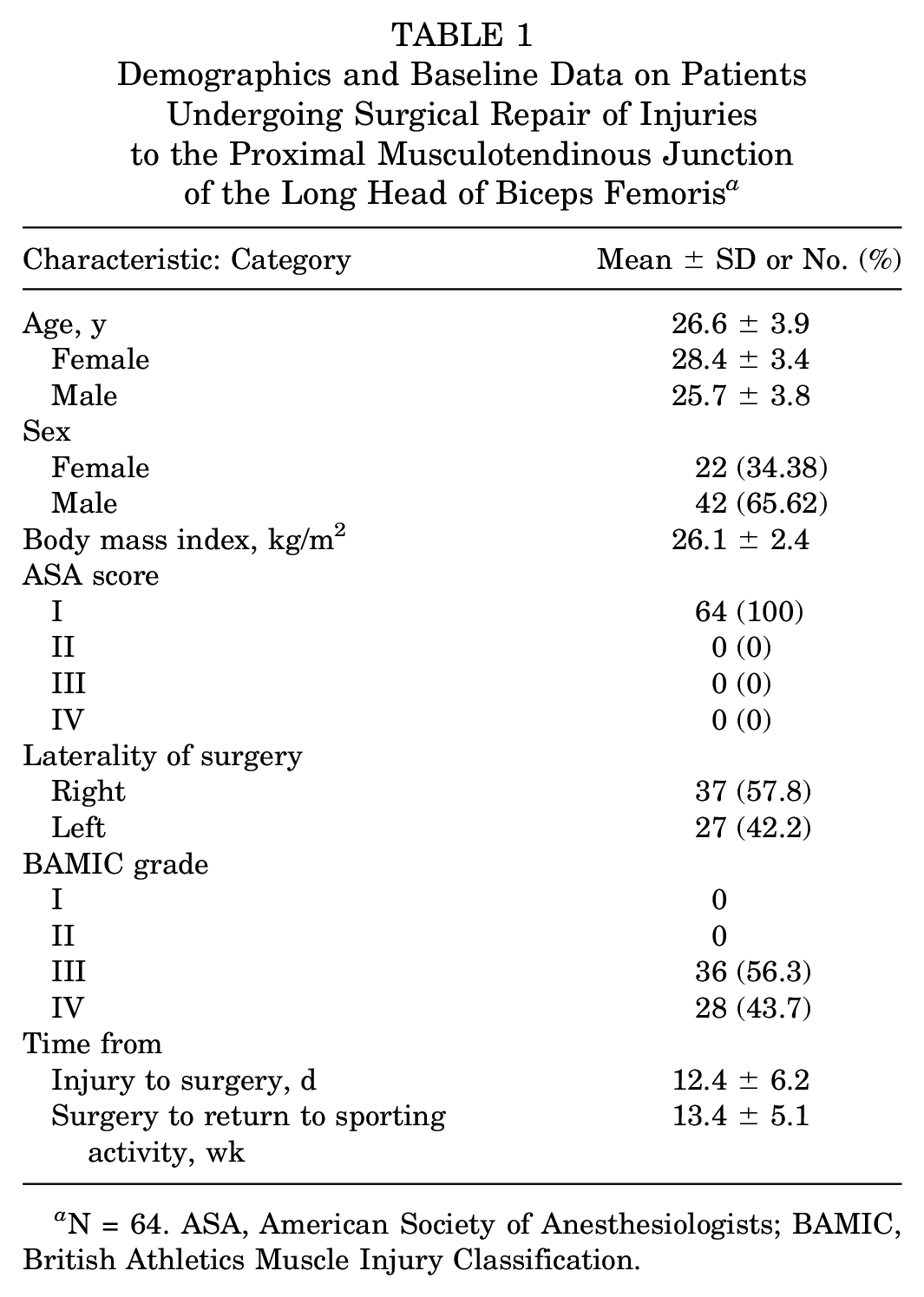
N = 64. ASA, American Society of Anesthesiologists; BAMIC, British Athletics Muscle Injury Classification.
This study included 51 professional athletes (29 rugby players, 14 football players, 3 sprinters, 3 cricketers, and 2 weight lifters) and 13 amateur athletes (8 football players, 4 middle-distance runners, and 1 rugby player). All study patients underwent preoperative magnetic resonance imaging (MRI) scans to confirm diagnosis, assess for any concurrent injuries, and plan operative intervention (Figure 1). All MTJ-BFlh injuries were graded with the British Athletics Muscle Injury Classification (BAMIC) system 33 (Table 2).
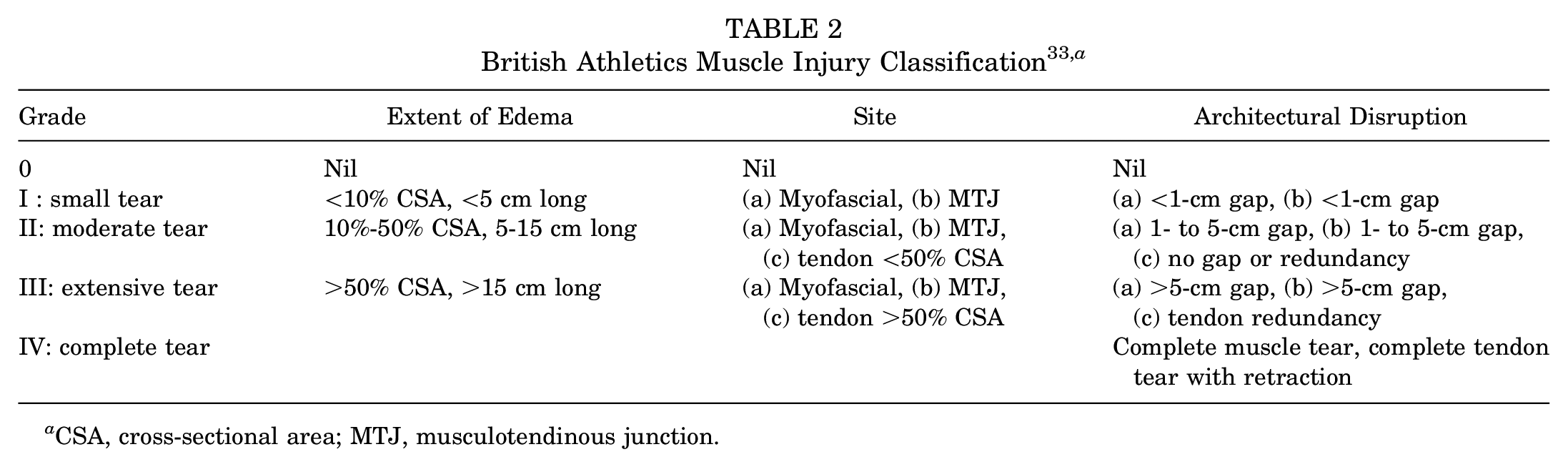
CSA, cross-sectional area; MTJ, musculotendinous junction.
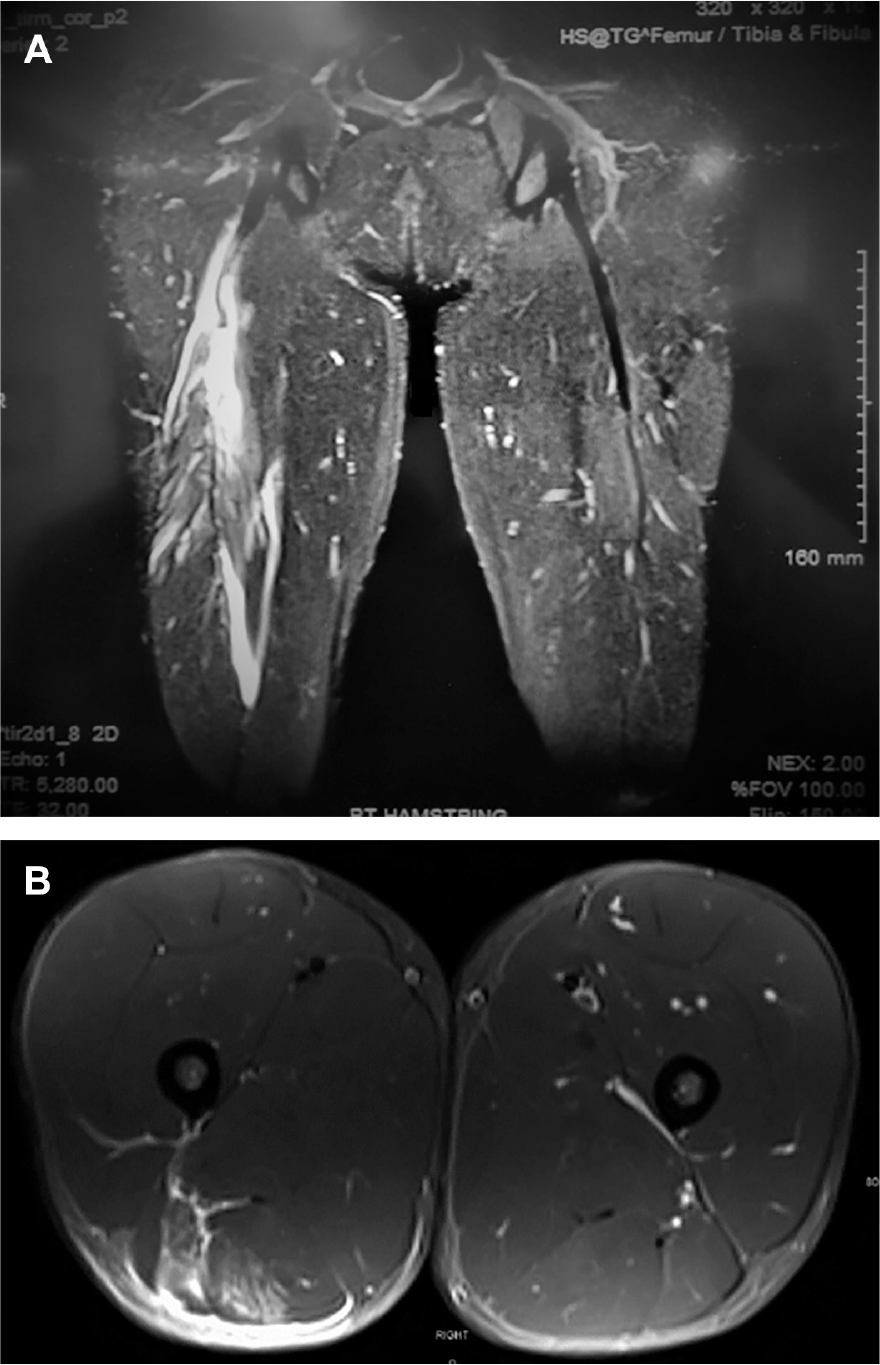
(A) Coronal section T2-MRI slice shows BAMIC grade IV injury through the right proximal musculotendinous junction of the long head of the biceps. (B) Transverse section T2-MRI slice of BAMIC grade III-b injury through the proximal musculotendinous junction of the long head of the biceps with nearly 60% of cross section involved. BAMIC, British Athletics Muscle Injury Classification; MRI, magnetic resonance imaging.
The inclusion criteria for study participation were as follows: acute hamstring injury within 4 weeks of presentation; preoperative MRI scan to confirm BAMIC grade IIIB, IIIC, or IV tear of the proximal MTJ-BFlh (Table 2); clinical loss of strength and/or flexibility of the hamstring muscle group; and operative intervention undertaken by the senior author (F.S.H.). Exclusion criteria included the following: MTJ-BFlh injuries sustained >4 weeks before surgical intervention (n = 6), recurrent MTJ-BFlh injury or previous hamstring surgery (n = 4), BAMIC grade I-IIIA MTJ-BFlh injuries (n = 9), nontraumatic tendinitis of the proximal biceps femoris (n = 3), and patient residence abroad (n = 4).
Informed consent was obtained from all study patients. Hospital ethical review board approval was obtained before commencement of the study.
Surgical Technique
All operative procedures were performed with the patient in the prone position under general anesthetic. The gluteal skin crease was marked and an 8- to 10-cm longitudinal incision performed distal to this (Figure 2). The underlying subcutaneous tissue and gluteal fascia were divided with electrocautery and the inferior border of the gluteus maximus muscle exposed. Care was taken to preserve the posterior cutaneous nerve of the thigh during dissection. The gluteus maximus was then retracted superiorly to expose the underlying fascia over the hamstring muscles. Caution was taken not to place the retractor deep on the ischium to minimize risk of injury to the inferior gluteal nerve. A longitudinal incision was performed in the hamstring fascia and any traumatic hematoma evacuated. The hamstring tendons were explored to confirm preoperative clinical and MRI findings and assess for any additional injuries within the operative field. The sciatic nerve was intact in all cases. The insertion of the biceps femoris was tracked down to the zone of injury at the MTJ-BFlh. The knee was flexed to 30°, and 2 No. 5 Ethibond (Ethicon) braided nonabsorbable sutures were used to close the defect without tension at the MTJ through the modified Kessler technique. The knee was then fully extended to ensure satisfactory tension in the biceps femoris throughout the arc of motion. The wound was copiously irrigated with normal saline. The overlying fascia, subcutaneous tissue, and skin were closed in layers with an absorbable suture, and a pressure dressing was applied to the wound.
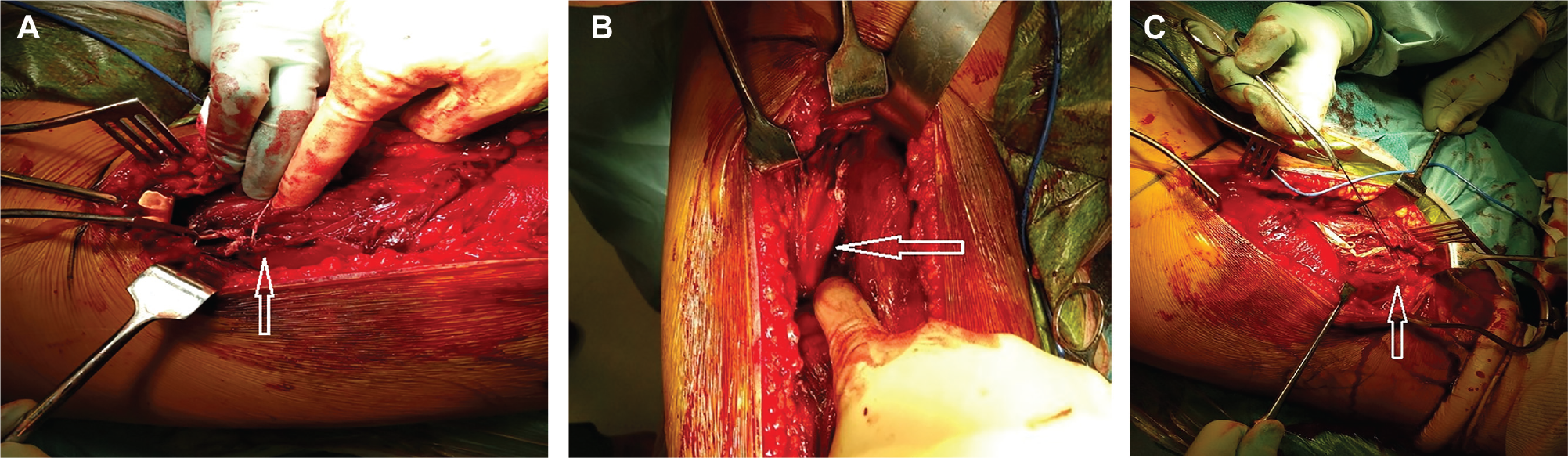
Intraoperative photographs. (A) Complete tear through the proximal musculotendinous junction of the long head of the biceps femoris (arrow). (B) Medial retraction of biceps femoris to confirm continuity of sciatic nerve (arrow). (C) Sutures to the proximal portion of the tear through the proximal musculotendinous junction of the long head of the biceps femoris (arrow).
Postoperative Rehabilitation
All patients received a standardized milestone-based rehabilitation program supervised by an experienced sports physical therapist. The rehabilitation program was divided into 4 distinct phases:
Phase 1: RICE (rest, ice, compression, and elevation), partial weightbearing with crutches, aspirin (75 mg, once daily), limited excessive combined hip flexion and knee extension, normalization of gait. A hinged knee brace was provided only if requested by the patient or physical therapist.
Phase 2: Pain-free range of motion, full weightbearing, concentric and eccentric training, core strengthening.
Phase 3: Muscle strengthening with resistance exercises, double- and single-leg squats, quadriceps extension, and hamstring curls. Aerobic conditioning with light jogging, cycling, and swimming. Sport-specific training.
Phase 4: Return to full sporting activity when full pain-free range of motion was achieved, muscle strength was 90% of uninjured limb, and there were no concerns with sport-specific training.
Outcome Measures
All study patients were clinically reviewed by the operating surgeon at regular intervals until return to play. Study outcomes were recorded by a specialist nurse practitioner preoperatively and predefined intervals after surgery. All outcomes at 3 months and 1 year after surgery were collected during clinical consultation, and outcomes at 2-year follow-up were collated by telephone conversation, given the wide geographical location of study patients.
Patient Satisfaction
Patient satisfaction was recorded at 3 months, 1 year, and 2 years after surgery with the Musculoskeletal Outcomes Data Evaluation and Management System, which scores patient satisfaction on a scale of 1 to 5 (1, very unsatisfied; 2, unsatisfied; 3, neutral; 4, satisfied; 5, very satisfied). 20
Hamstring Strength
Isometric hamstring strength was tested pre- and postoperatively at 3 months and 1 year. The patient was placed in the prone position with a handheld dynamometer (Hoggan Scientific LLC) positioned over the ipsilateral calcaneus. Maximum resisted knee flexion force (newtons) was recorded at 0°, 15°, 45°, and 90°. This technique was repeated 3 times and the mean flexion force at each angle in the injured limb was calculated. All values were compared with the contralateral uninjured limb to calculate the percentage of normal hamstring muscle strength.
Passive Straight-Leg Raise
Maximum angle of passive straight-leg raise (PSLR) was tested pre- and postoperatively at 3 months and 1 year. In the supine position, the uninjured limb was passively elevated inducing flexion at the hip while maintaining extension at the knee joint to the point of failure secondary to pain or elastic limit of the limb. The maximum attainable PSLR (degrees) was measured with a standard goniometer and compared with the maximum PSLR in the contralateral injured limb. The deficit in PSLR between the limbs was recorded.
Functional Progress and Return to Function
All study patients completed the Lower Extremity Functional Scale (LEFS) and Marx activity rating score (MARS) preoperatively and at 3 months, 1 year, and 2 years after surgery.5,29 The LEFS is a validated and effective questionnaire for assessing specific lower limb function. It has an 80-point scale, with 20 questions and 4 points allocated to each question and with a minimum clinical difference of 9 points. 5 The MARS measures patient activity level and knee function independent of age, sex, and type of sporting activity. Scores of 0 to 4 are assigned to 4 activities (running, changing direction, decelerating, and pivoting) with a total score of 16. 29 Time from surgical intervention to full return to sporting activity was collected in all study patients.
All patients recruited into this study completed follow-up. Mean follow-up time was 29.2 months (range, 24.0-37.1 months) from date of surgery.
Statistical Analysis
Paired t tests were used to compare study outcomes found to be normally distributed, while the Mann-Whitney U test was used for continuous outcomes not normally distributed. Categorical outcomes were compared with the Fisher exact test. Statistical significance was set at a P value <.05 for all analyses, and all statistical analysis was performed with SPSS (v 24; IBM Corp).
Results
Return to Function and Recurrence
All study patients returned to their preinjury level of sporting activity. Mean ± SD time from surgical intervention to return to sporting activity was 13.4 ± 5.1 weeks. At 1- and 2-year follow-up, all study patients were still participating at their preinjury levels of sporting activity.
Three patients (4.8%) developed sharp, localized pain over the operative site during postoperative rehabilitation. These were investigated with urgent MRI scans. Of these, 1 patient had complete rupture through the operated MTJ-BFlh site at 6 weeks after surgery. This patient underwent revision surgery through the previous incision, followed by debridement of residual scar tissue and re-repair of the MTJ-BFlh injury with the surgical technique described earlier. The patient went back into the rehabilitation program and returned to full sporting activity at 19 weeks after revision surgery without any further complications. The remaining 2 patients sustained myofascial tears at 1 and 4 months after primary surgery. Both patients were treated nonoperatively with a graded exercise rehabilitation program and made full return to sporting activity within 4 weeks of reinjury.
Patient Satisfaction
Surgical repair of MTJ-BFlh injuries was associated with high patient satisfaction at 1 and 2 years after surgery. At 1-year follow-up, 2 patients were unsatisfied with the outcomes of their surgery: 1 patient had rerupture requiring further surgical intervention, and 1 patient was frustrated at the pace of rehabilitation. At 2 years after surgery, all patients were either satisfied (18.8%) or very satisfied (81.2%) with the outcomes of their surgery.
Hamstring Strength
Surgical intervention was associated with improved hamstring muscle strength at 3 months after surgery as compared with preoperative strength (Table 3, Figure 3). At 1-year follow-up, all patients had restored hamstring muscle strength to >90% of the contralateral side.
Changes in Hamstring Strength (vs Contralateral Limb) During Study Intervals a
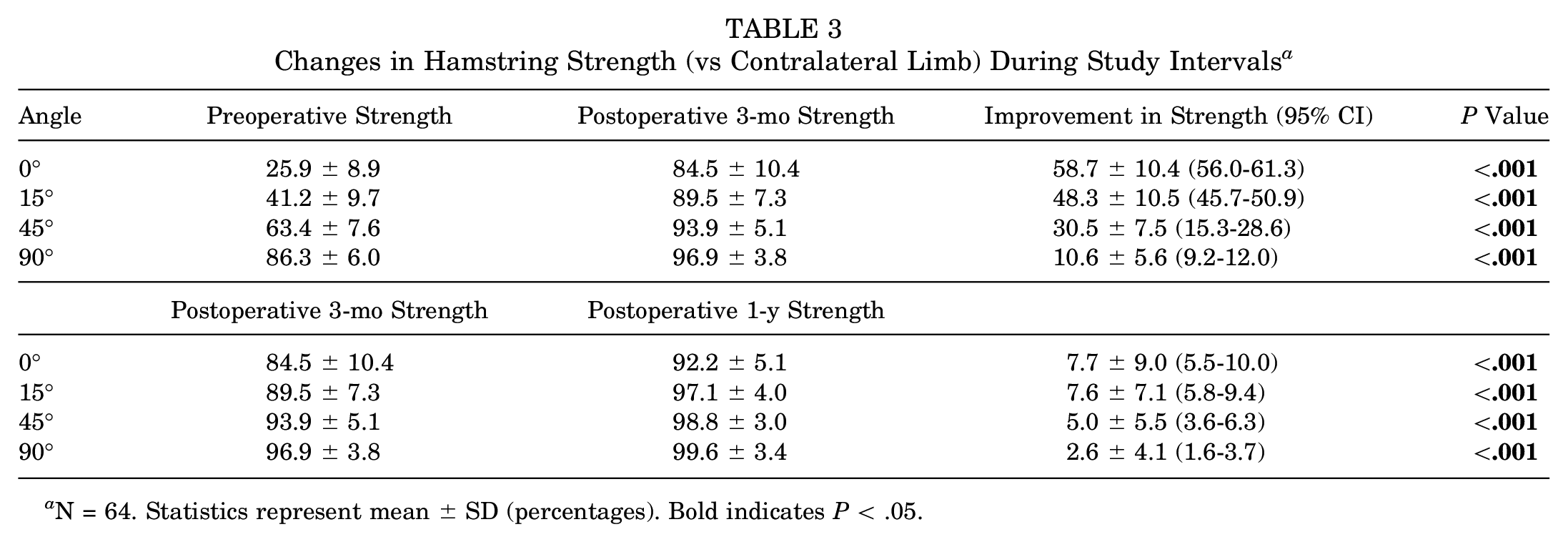
N = 64. Statistics represent mean ± SD (percentages). Bold indicates P < .05.
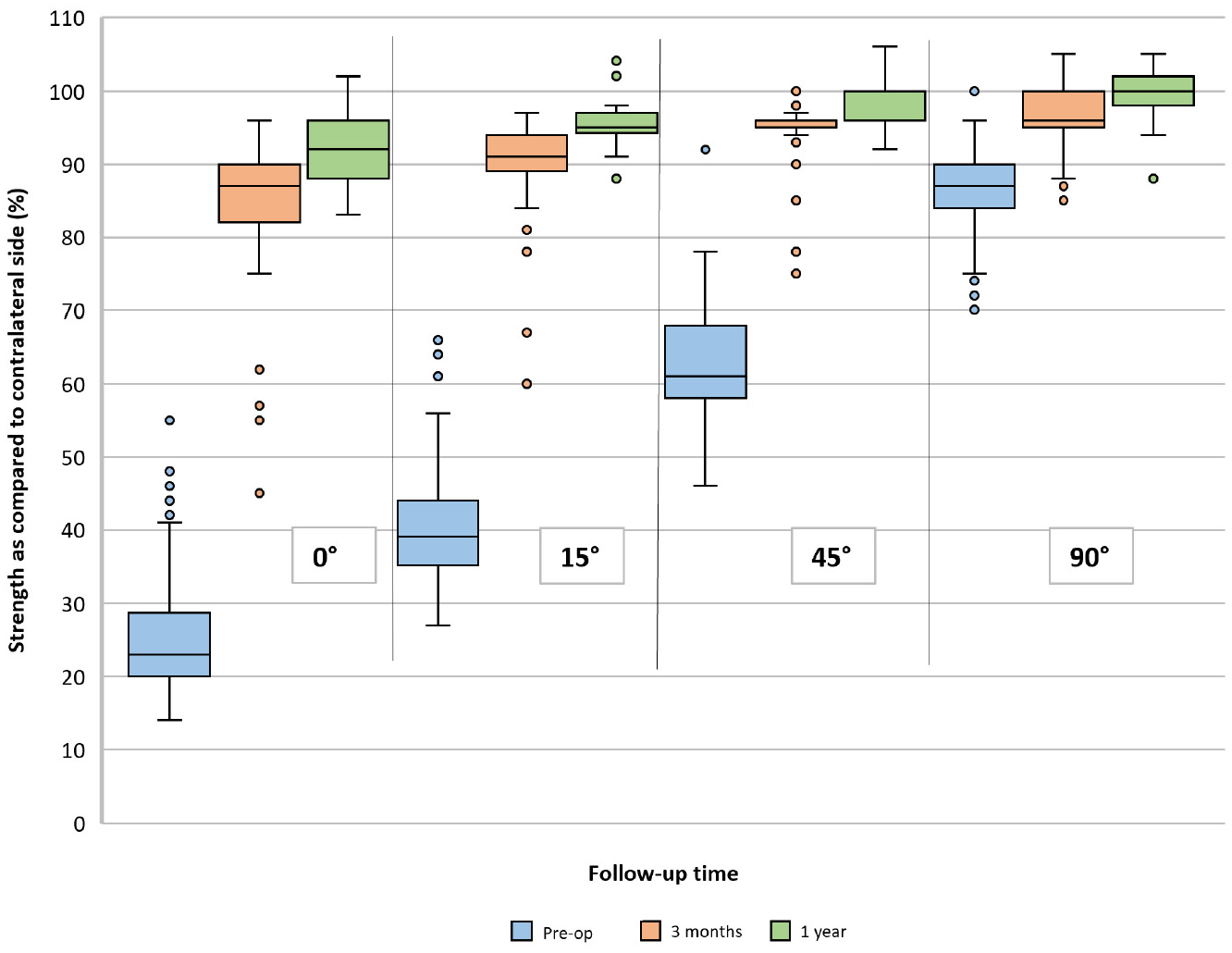
Box plot shows percentage hamstring muscle strength as compared with contralateral side at various angles of knee flexion in patients undergoing surgical repair of proximal musculotendinous injuries at the long head of the biceps femoris. Values are presented as median (line), interquartile range (box), 95% CI (error bars), and outliers (circles).
Passive Straight-Leg Raise
Surgical intervention was associated with improved PSLR and decreased PSLR deficit at 3-month follow-up as compared with preoperative values (Table 4).
Changes in Time to PSLR During Study Intervals a
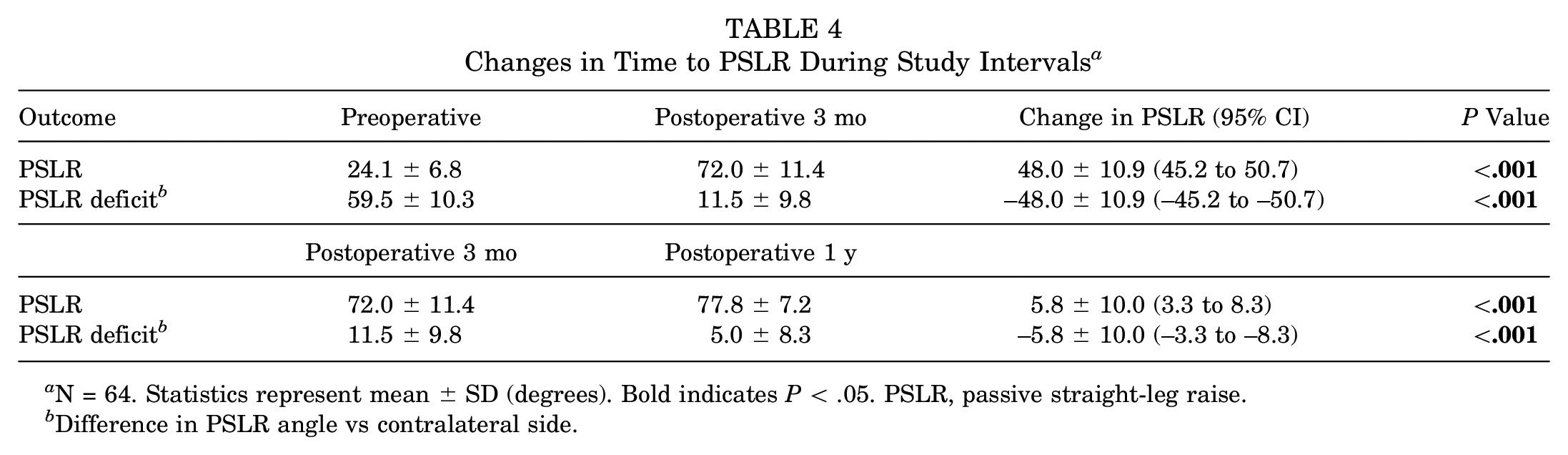
N = 64. Statistics represent mean ± SD (degrees). Bold indicates P < .05. PSLR, passive straight-leg raise.
Difference in PSLR angle vs contralateral side.
Of note, at 3-month follow-up, 5 patients had straight-leg raise of <30°: 2 with myofascial tears of the MTJ-BFlh, 1 with complete rerupture of the MTJ-BFlh, and 2 with chronic lumbar back pain. At 1-year follow-up, only 1 patient with chronic lumbar back pain was unable to achieve PSLR >30°. There were further improvements in straight-leg raise at 1 year after surgery as compared with 3-month follow-up (Figure 4).
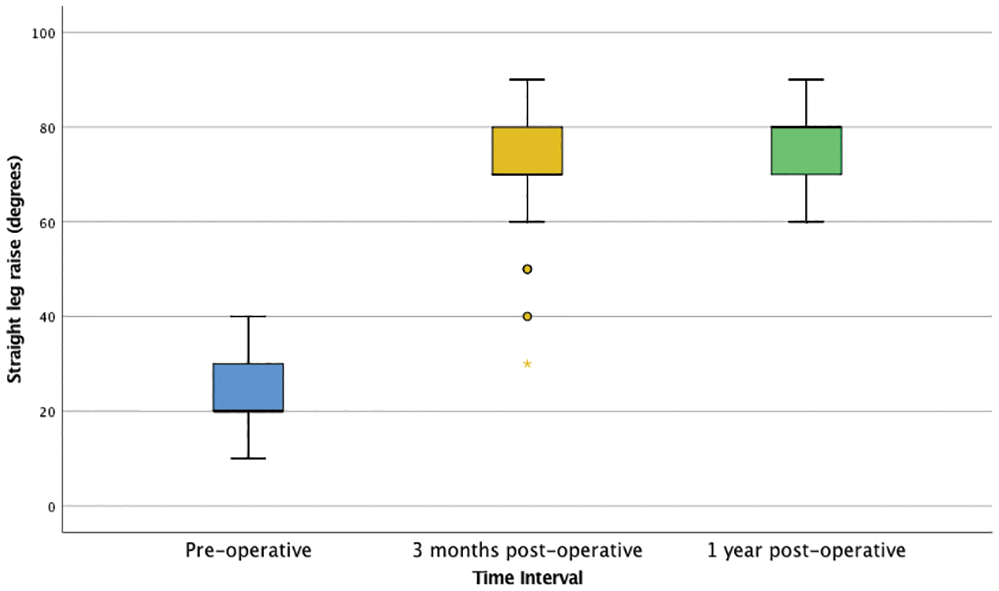
Box plot shows passive straight-leg raise angle (degrees) in patients undergoing surgical repair of proximal musculotendinous injuries at the long head of the biceps femoris. Values are presented as median (line), interquartile range (box), 95% CI (error bars), and outliers (asterisk and circles).
Functional Progress
At 3 months after surgery, mean LEFS and MARS outcomes improved as compared with their preoperative values (Table 5).
Changes in LEFS and MARS Scores During Study Intervals a
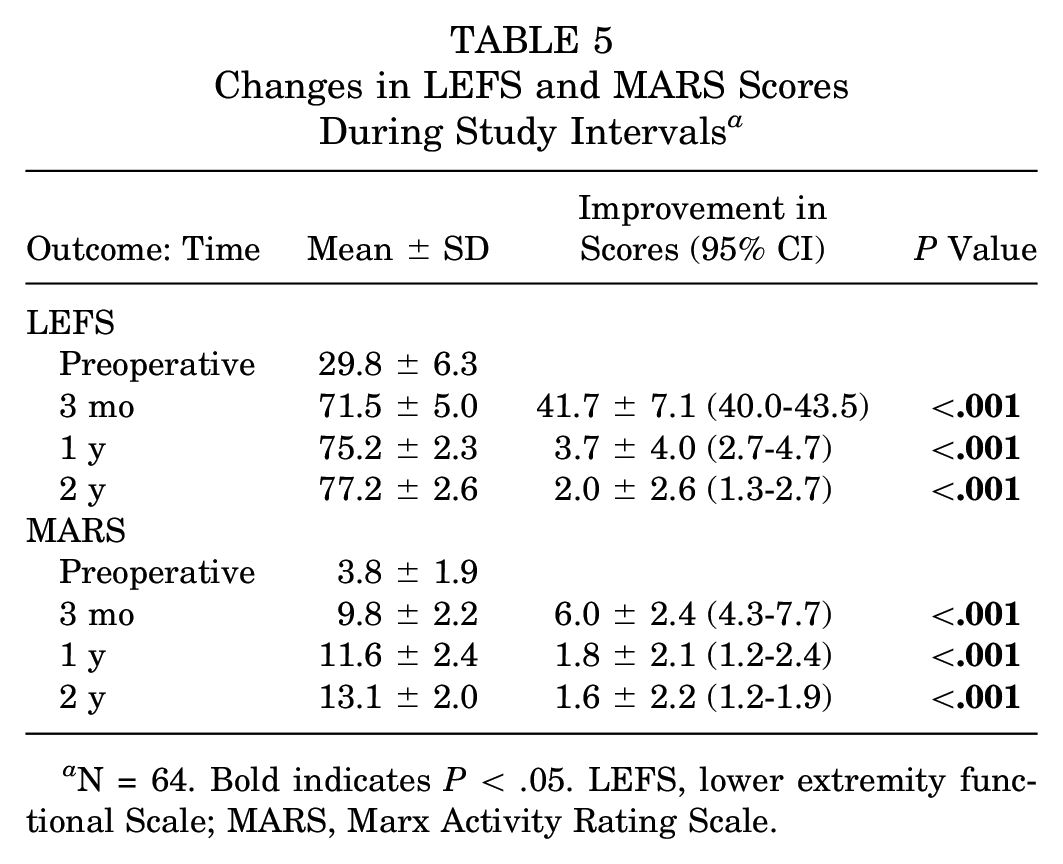
N = 64. Bold indicates P < .05. LEFS, lower extremity functional Scale; MARS, Marx Activity Rating Scale.
Statistically significant improvements in LEFS and MARS were observed at 3 months, 1 year, and 2 years after surgery (Figure 5). At 1 year follow-up, 7 patients (10.9%) had an LEFS score of 80 (out of 80), and 33 patients (51.6%) had a score >75. At 2-year follow-up, 20 patients (31.3%) had an LEFS score of 80, and 37 (57.8%) had a score >75.
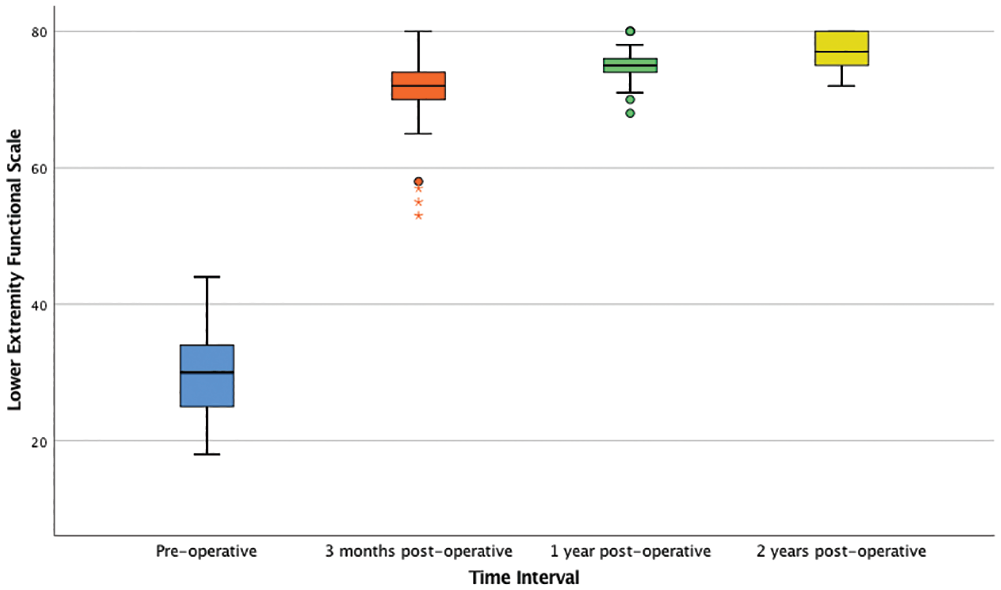
Box plot shows Lower Extremity Functional Scale score in patients undergoing surgical repair of proximal musculotendinous injuries at the long head of the biceps femoris. Values are presented as median (line), interquartile range (box), 95% CI (error bars), and outliers (asterisks and circles).
Complications
In addition to the aforementioned 3 patients with recurrence, 12 patients had postoperative hematomas distal to the wound incision, and 4 patients had neurapraxia over the distribution of the posterior cutaneous nerve of the thigh. These complications were managed nonoperatively and fully resolved within 8 weeks of surgery. No other complications were reported during the 2-year follow-up period.
Discussion
This study found that surgical intervention in acute MTJ-BFlh injuries enabled return to preinjury level of function with low risk of recurrence, high patient satisfaction, increased hamstring muscle strength, and improved functional outcome scores at short-term follow-up. To our knowledge, this is the first study to report on the operative management of acute MTJ-BFlh injuries, and it provides important prognostic information on functional outcomes and return to sporting activity after the surgical repair of these injuries.
Nonoperative treatment of biceps femoris injuries is associated with highly variable rehabilitation times and uncertainty in time to return to sporting activity.1,2,13,27 Askling et al 2 reviewed outcomes in 18 elite sprinters with biceps femoris injuries treated nonoperatively and found that the median time to preinjury level of function was 16 weeks (range, 6-50 weeks). Comin et al 14 reviewed outcomes in 62 elite Australian rules football players with acute hamstring injuries, which included 45 patients with biceps femoris injuries, and reported that the median recovery time was 10 weeks (interquartile range, 6-18 weeks) with central tendon involvement, as compared with 3 weeks (interquartile range, 1-3 weeks) without central tendon disruption. Malliaropoulos et al 28 reviewed outcomes in 90 elite track and field athletes with hamstring abnormalities identified on ultrasonography, which included 68 patients with biceps femoris injuries. The authors found that return to full sporting function ranged between 2 and 6 weeks, depending on preoperative degree of range of motion deficit. In our study, mean time to return to sporting activity was 13.4 ± 5.1 weeks, which is longer than the range for the previously cited nonoperative management.2,14,28 However, direct comparisons of rehabilitation times in this study with those reporting on nonoperative management are not possible, owing to differences in the grade and location of biceps femoris injury, variations in rehabilitation protocols, and inconsistencies in the definition of return to sporting activity. Furthermore, different sporting activities place different physiological demands on the hamstring complex; therefore, the sporting profile of each study group may influence time to return to sporting activity. Overall, surgical repair of MTJ-BFlh injuries did increase time to return to sporting activity but markedly reduced recurrence rates as compared with nonoperative management.
Injuries to the musculotendinous junction are associated with hematoma formation and residual scar tissue at the site of injury. Remodeling of the injured scar tissue occurs, but the tendinous portion remains vulnerable, as the healing process through the tendon is slower than within the muscle portion. This increases the risk of rerupture through the weakened portion of the musculotendinous junction.2,25 Nonoperative treatment of proximal hamstring injuries is associated with high risk of rerupture at short-term follow-up.22,32,37,42 Gibbs et al 19 reported that nonoperative management of biceps femoris injuries resulted in recurrence in 5 of 13 patients (38.5%) within 28 days of the initial injury. Pollock et al 34 reviewed outcomes in 44 elite track and field athletes with 65 proximal hamstring injuries, which included 28 patients with injuries to the long head of the biceps femoris. Nonoperative management resulted in 13 reinjuries (20%) during rehabilitation or immediately after return to sporting activity. In our treatment center, before undertaking this study, 112 patients (21.4%) with BAMIC grade III and IV injuries were treated nonoperatively, and 34 (21.4%) of them had recurrence of the primary injury within 2-year follow-up. Direct comparison of the current study findings with this historical control group undergoing nonoperative management is not possible given the limited number of functional outcomes recorded in the control group. Nevertheless, transitioning from nonoperative to operative management of these high-grade injuries led to a markedly reduced recurrence rate of 4.8% in the current study. In our study, 1 patient (1.6%) required revision surgery for MTJ-BFlh reinjury, and 2 patients (3.2%) received nonoperative treatment for myofascial tears during postoperative rehabilitation. All 3 patients required further rehabilitation but were able to make a full return to sporting activity. These complications highlight the importance of close observation and early referral for appropriate imaging during postoperative rehabilitation and return to sporting activity.
The timing of surgical intervention in proximal hamstring injuries is paramount. Acute operative intervention (within 4 weeks of injury) in proximal hamstring avulsion injuries is associated with improved patient satisfaction, better pain control, increased muscle strength, and earlier return to sporting activity as compared with chronic operative repair (after 4 weeks of injury).7,41 Nonoperative treatment in avulsion injuries is associated with reduced patient satisfaction and reduced return to preinjury level of function as compared with acute and chronic repairs. 7 Furthermore, nonoperative treatment and delays in surgical intervention are both associated with secondary problems, such as muscle weakness and fibrosis of scar tissue to the sciatic nerve, leading to neurological complications such as foot drop or paresthesia of the lower limb.12,23,42 Bowman et al 8 reported outcomes in 17 patients undergoing surgical repair of partial proximal hamstring injuries refractory to 6 months of nonoperative treatment and found that 5 of them developed postoperative paresthesia. Sarimo et al 36 reviewed the outcomes of surgical treatment in 41 patients with acute or chronic complete proximal hamstring avulsion injuries and found that chronic cases were associated with the torn muscle having a macroscopically abnormal appearance with a hardened fibrotic texture. The authors also indicated that time from injury to operative intervention was 2.4 months in patients reporting good and excellent results but 11.7 months in patients with poor or moderate outcomes (P < .001). In our study, all patients underwent surgical intervention within 3 weeks of surgery, which helped to limit the formation of scar tissue and tethering of the sciatic nerve to fibrous tissue. None of the study patients undergoing primary surgery required neurolysis, and there were no residual neurological complications at 2-year follow-up.
This study found high patient satisfaction, with 62 patients indicating that they were satisfied or very satisfied with the outcomes of their surgery at 1-year follow-up. One patient who underwent revision surgery for rerupture described the outcomes as unsatisfactory at 1-year follow-up, but this improved to satisfactory at 2-year follow-up. Revision surgery was associated with improved pain and hamstring muscle strength to 90% of the contralateral side at 3-month follow-up. The high patient satisfaction cited in this study is consistent with other studies reporting on surgical management of hamstring avulsion injuries.1,10,26 Lempainen et al 26 documented outcomes in 48 patients undergoing surgical repair of proximal hamstring injuries and found that outcomes of the operation were scored as excellent in 33 patients, good in 9, fair in 4, and poor in 2 at 36-month follow-up (range, 6-72 months). Aldridge et al 1 reviewed outcomes in 23 patients undergoing repair of partial proximal hamstring tears with suture anchors, finding that patient satisfaction was 81%, hamstring strength increased from 64% to 88% of the contralateral side, and endurance improved by 50% as compared with preoperative findings at follow-up of 3.1 years (range, 2.0-7.0 years).
Surgical intervention for acute MTJ-BFlh injuries was associated with marked improvements in functional scores. At 1-year follow-up, 33 of the 64 patients had an LEFS score >75 out of 80, and 7 of these patients had an LEFS score of 80. The LEFS score is designed to assess everyday activities; thus, given the low ceiling effect of the LEFS score, we also used the MARS to assess more specialized sporting activities that were self-reported as functional outcomes. These findings are consistent with existing literature reporting on surgical repair of acute and chronic hamstring injuries.13,38 -40 Sonnery-Cottet et al 39 found that surgical repair of proximal or distal hamstring injuries in 10 professional athletes was associated with return to preinjury level of sporting activity at 3.4 months (range, 2-5 months). The authors also found a mean LEFS score of 80 and MARS score of 16 at 3-month follow-up, which are similar to the values cited in this study. Cohen et al 13 followed 52 patients undergoing suture anchor repair of proximal hamstring avulsion injuries and found a mean LEFS score of 75 (range, 50-80) at 33-month follow-up (range, 12-76 months). Bowman et al 8 indicated that operative management of partial hamstring tears was associated with a mean MARS of 6.5 ± 5.3 at 32-month follow-up (range, 12-51 months). The patients had a mean age of 43 years (range, 19-64 years) and had failed 6 months of nonoperative treatment, which may have led to the reduced MARS as compared with those in this study.
Several limitations of this study need to be considered when interpreting the findings. First, there was no control group of patients undergoing nonoperative management; therefore, it is difficult to ascertain the benefit of surgical repair as compared with nonoperative treatment by using the standardized rehabilitation program alone. Based on our previous experience and the existing literature, nonoperative treatment of these injuries is associated with prolonged periods of rehabilitation and high risk of recurrence. All study patients were high-performance athletes who did not want randomization and potential allocation to nonoperative management. These patients preferred to make their own decisions about treatment; as such, prospectively randomizing these patients to a control group with nonoperative management was not possible. However, this is the largest study to date on the operative management of proximal musculotendinous injuries; all study patients were selected per their BAMIC injury grade; surgery was undertaken by a single surgeon using a standardized approach; and functional outcomes were recorded at regular intervals after a standardized rehabilitation program. Second, study outcomes were not correlated with preoperative clinical findings or radiological grade of injury. Third, additional imaging, such as ultrasound or MRI, was not used to assess MTJ-BFlh healing during follow-up.
Conclusion
Surgical intervention in acute MTJ-BFlh injuries enabled return to preinjury level of function with low risk of recurrence, high patient satisfaction, increased hamstring muscle strength, and improved functional outcome scores at short-term follow-up. Surgical repair of MTJ-BFlh injuries is associated with increased time to return to preinjury level of sporting activity but markedly reduced recurrence rates as compared with nonoperative management as reported in the existing literature.
Footnotes
Submitted June 30, 2019; accepted February 28, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: F.S.H. is a paid consultant and receives royalties from Stryker, Smith & Nephew, Corin, and Matortho. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.