
Abstract
Background:
It is unclear which structural parameters determine the development or the absence of chronic pseudoparalysis (PP) in patients with massive rotator cuff tears (mRCTs).
Purpose:
To determine whether scapular morphologic characteristics and extent of rotator cuff tearing are independent factors associated with chronic PP.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
In this retrospective case-control study, 50 patients with chronic mRCT (≥2 fully detached tendons) and active scapular plane abduction less than 90° (PP group) were age- and sex-matched with a cohort of 50 patients with chronic mRCT and an active scapular plane abduction greater than 90° (non-PP; NPP group). Analysis of standardized, plain radiographs included measurement of the critical shoulder angle (CSA) and the acromiohumeral distance (ACHD) on anteroposterior views and measurement of posterior acromial tilt, anterior and posterior acromial coverage, and posterior acromial height on standardized outlet views. Measurements on magnetic resonance imaging included fatty muscle infiltration, anterior (subscapularis) and posterior (infraspinatus/teres minor) tear extension, and global tear extension (anterior + posterior tear extension) in the parasagittal plane.
Results:
Overall, no significant difference was found in patients’ demographic characteristics (P > .05). Univariate analyses confirmed significant differences between the PP and NPP groups in active scapular plane abduction (51°± 22° vs 135°± 29°; P < .001). Multivariate analyses revealed independent factors associated with PP compared with the NPP group: CSA (38.2°± 4.6° vs 35.2°± 3.7°; P = .001); ACHD (4.7 ± 2.2 vs 7.3 ± 2.6 mm; P < .001); posterior acromial height (22 ± 10 vs 17 ± 7 mm; P = .005); and anterior (–9°± 21° vs 25°± 12°; P < .001) and posterior (–18°± 14° vs 2°± 14°; P < .001) tear extension. The NPP group had significantly less involvement and fatty infiltration of the subscapularis (1.4 ± 0.6) compared with the PP group (2.2 ± 0.9) (P < .001).
Conclusion:
This study confirms that global RCT extension and the quality of the inferior half of the subscapularis are significantly associated with chronic pseudoparalysis. The study further shows that acromial morphologic characteristics are relevant in the development of pseudoparalysis. Patients with pseudoparalysis have a larger CSA, less ACHD, and a higher positioned acromion in the sagittal plane.
Keywords
Almost half of all treated rotator cuff tears (RCTs) are classified as massive rotator cuff tears (mRCTs).16,17,28 The definition of mRCT is not universally agreed upon and can be based on the diameter of the tear (ie, >5 cm) 9 or the number of tendons detached from the tuberosities (ie, ≥2 tendons). 24
The clinical presentation of patients with mRCT varies substantially and can be associated with painful disability, with or without loss of active range of motion. It is necessary to distinguish acute mRCTs from chronic mRCTs. In the acute setting, loss of active range of motion is mainly due to pain and can often be reversed by early arthroscopic repair.14,40 In chronic tears, a subset of patients develop a pain-free inability to actively elevate the arm to 90°. This is often accompanied by anterosuperior escape of the humeral head but not by neurological impairment or restricted passive range of motion. The main disability is loss of active overhead function rather than pain. This condition should be referred to as chronic pseudoparalysis (PP). 43 It appears that this chronic condition can be treated reliably only by reverse total shoulder arthroplasty.15,18,19,22,33,38,43
It is still unknown why patients with similar, chronic RCT patterns develop different shoulder dysfunctions. A clear association between chronic PP and the size and location of the RCT has been described. Of key importance is the deficiency of the inferior half of the subscapularis (SSC) tendon.10,13,44 The role of the acromion in association with PP has not been investigated so far, although some studies have shown its association with mRCT. 2 The lateral extension of the acromion in the coronal plane has been investigated clinically and biomechanically and has been identified as a risk factor for RCTs in patients with a high critical shoulder angle (CSA).4,31,32,35 More recently, a specific morphologic state of the posterior acromion in the sagittal plane has been described as a risk factor for mRCT, where patients with RCT have a wider posterior acromial coverage of the humeral head. 2
The goal of this study was to identify independent factors associated with PP based on a multivariate analysis of a matched-pair cohort. It was hypothesized that RCT size and location, and the bony anatomic features of the acromion in the coronal and sagittal plane, are independent factors associated with PP.
Methods
Study Population
For review, all patients gave written consent and the study was approved by the responsible review board.
Between January 2005 and December 2014, a total of 926 consecutive patients with mRCT underwent reverse total shoulder arthroplasty or rotator cuff repair. The definition of mRCT included a complete tear of 2 or more tendons, 24 which was identified on magnetic resonance arthrography and verified intraoperatively. Inclusion criteria were RCT involving at least 2 tendons without history of acute trauma, absence of restriction of passive glenohumeral range of motion, failed nonoperative treatment for at least 6 months, magnetic resonance arthrography of the shoulder, serial plain radiographs including anteroposterior and true lateral (supraspinatus outlet or Neer) 34 views taken under fluoroscopic control, complete report of active and passive shoulder movement, and photographic documentation. Patients were excluded (n = 680) if they had a traumatic RCT, if they reported stiffness and pain on attempted elevation, if the tear was acute (<3 months), and if complete data were not available.
On the basis of these criteria, 246 patients were included. Of those, 50 shoulders had active scapular plane abduction less than 90° and constituted the PP group. They were case matched by age (within 5 years) and sex to 50 patients with active scapular plane abduction greater than 90° (non-PP; NPP group). The reported measurements of active and passive ranges of motion were collected in an institutionally standardized manner by use of a handheld goniometer while the patient was seated. Each included patient had photographic documentation of shoulder range of motion, and the reported measurements were validated by these photographs.
Radiographic Evaluation
Two blinded observers (R.E.N., L.E.) undertook all measurements on plain radiographs and magnetic resonance arthrography. True anteroposterior radiographs were controlled for scapular malrotation inferior to 20° of internal rotation or extension and inferior to 20° of external rotation or flexion. 31 Plain, true lateral radiographs that had been obtained under fluoroscopic control were assessed as to whether the acromion and the coracoid processes created symmetric upper limbs of a Y-shape with the humeral head not overlaying the supraspinatus outlet region and whether the central beam was in line with the supraspinatus fossa. Magnetic resonance arthrography was performed on a 1.5-T or 3.0-T magnetic resonance imaging (MRI) unit (Symphony; Siemens).
Measurements on anteroposterior views included the CSA,4,23,31,32,36 the acromiohumeral distance (ACHD), 11 and the assessment of the degree of osteoarthritis according to Hamada et al. 29 Measurement of the orientation of the acromion in the sagittal plane was conducted as previously described 30 and included measurement of the posterior acromial tilt, the anterior and posterior acromial coverage (AAC and PAC), and the posterior acromial height (PAH) (Figure 1).
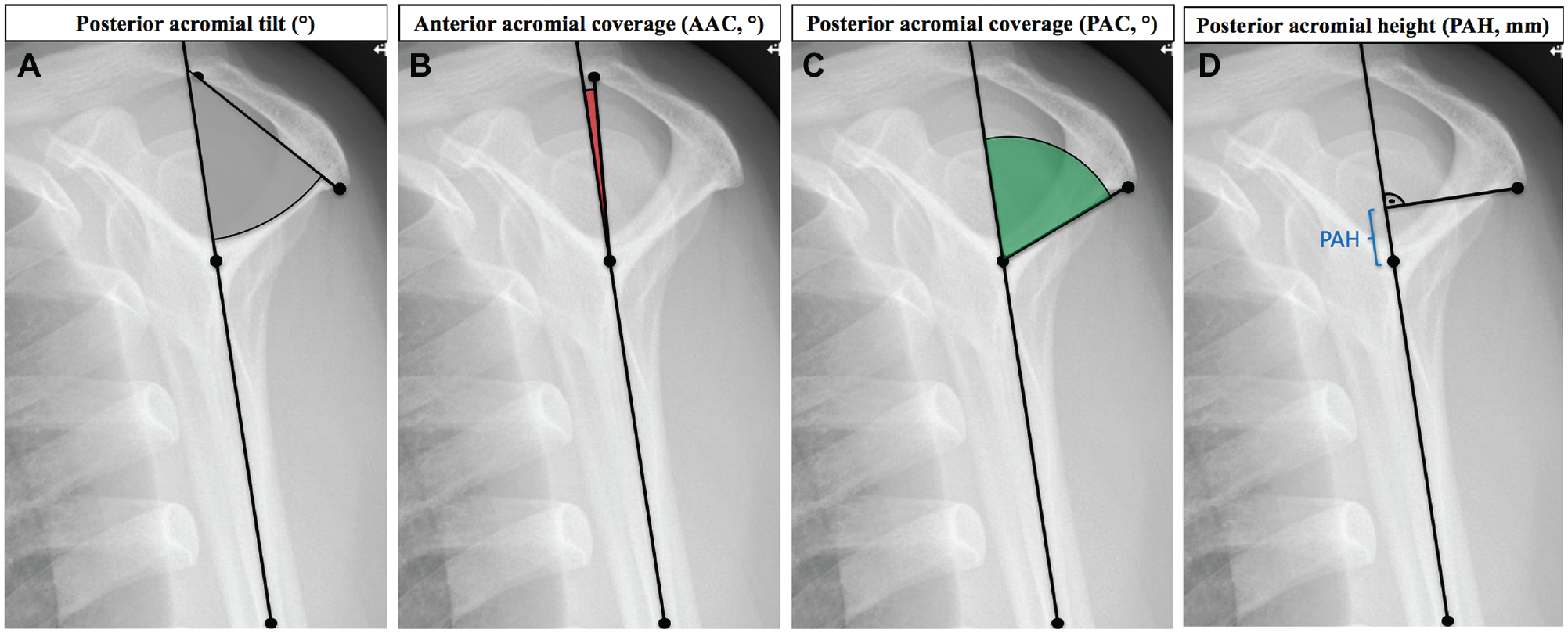
Measurement of posterior acromial morphologic characteristics on true lateral radiographs. (A) Posterior acromial tilt is the angle formed by the reference line (connecting the inferior angle of the scapula with the center of the intersection of the small arms of the Y) and a line connecting the most posterior point to the most anterior point of the inferior aspect of the acromion (gray area). (B) Anterior acromial coverage (AAC) is the angle formed by the reference line and a line from this intersection to the most anterior point of the acromion (red area). (C) Posterior acromial coverage (PAC) is the angle formed between the reference line and the most posterior point of the acromion (green area). (D) A perpendicular line is drawn from the reference line to the most posterior point of the acromion. Posterior acromial height (PAH; bracket) is the distance between this line and the center of the intersection of the small arms of the Y.
Measurements on magnetic resonance arthrography included fatty infiltration of the rotator cuff, according to the MRI adaptation of the Goutallier classification,20,26 and anterior, posterior, and global RCT extension. 44 The exact degree of the anterior (SSC) and posterior (infraspinatus, ISP; teres minor, TM) tear extension was defined by a specific angle between the equatorial line of the humeral head and the remaining anterior and remaining posterior tendon attachment. 44 The angle between the equator and the remaining superior border of the SSC defined the anterior tear extension, and the angle between the equator and the remaining superior border of the ISP/TM defined the posterior tear extension (Figure 2).
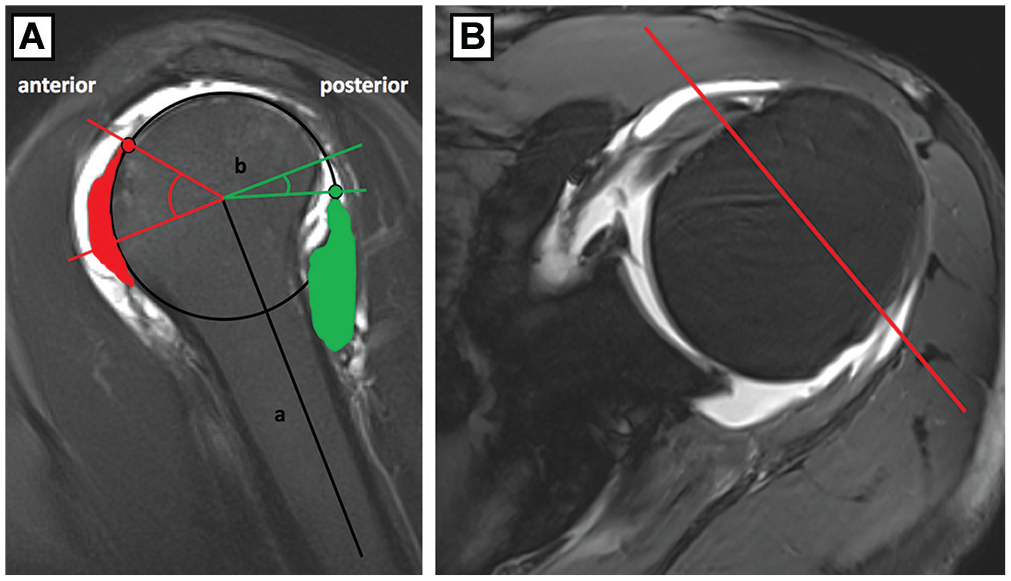
Measurement of tear extension (remaining subscapularis, red area; remaining infraspinatus and teres minor, green area) on parasagittal magnetic resonance arthrography. (A) The equatorial line (b) of the humeral head (perpendicular to the longitudinal axis of the humerus (a), was defined as the reference line. Anterior tear extension was defined as the angle between the equator and the upper border of the remaining subscapularis (red dot), and posterior tear extension was defined as the angle between the equator and the upper border of the remaining infraspinatus (green dot). (B) Corresponding axial plane.
Zero degrees was considered if the tear extension was confined by the equatorial line, and a negative value indicated a tear extension inferior to this line (positive if superior). The global tear extension was calculated with the following formula: 180 – (Anterior + Posterior Tear Extension). The relation of the remaining anterior force of the SSC versus the combined posterior forces of the ISP/TM was graded by dividing the anterior and posterior tear extension into 25% increments from grade 0 (no tear) to grade 4 (complete tear). The ratio of the anterior and posterior tear extension was calculated and defined as the force couple: A ratio of 1 indicates a balanced situation; a ratio greater than 1 indicates a shift toward stronger posterior rotator cuff; and a ratio less than 1 indicates a shift toward stronger anterior rotator cuff. 44
Statistical Analysis
On the basis of previously published data concerning RCT extension, 44 CSA, 31 and posterior acromial morphologic features, 2 an a priori power analysis revealed that for a significance level of .05 (type I error), a sample size of 50 patients in each group was sufficient to provide a desired power of 80% to determine significant differences in RCT extension, CSA, and posterior acromial morphologic characteristics.
The PP and NPP groups were matched according to their age (within 5 years) and sex (FUZZY extension, SPSS Statistics, version 24; IBM). Normal distribution of data was assessed as per the Shapiro-Wilks test. Normally distributed data were compared with the paired t test, and nonnormally distributed data were compared with the Wilcoxon signed rank test. A multivariate logistic regression analysis to determine independent factors associated with the outcome variable (PP) was conducted on all measured anatomic factors that were significant in the univariate analysis. Goodness of fit of the binary logistic regression models was assessed via the Hosmer-Lemeshow test. Significance was set at P < .05, and all P values were 2-tailed.
Interobserver reliability was measured for CSA, ACHD, Hamada stages, posterior acromial tilt, AAC, PAC, PAH, and anterior and posterior tear extension by means of the intraclass correlation coefficient for absolute agreement, with 1 indicating perfect reliability.
Results
Clinical Analysis
There were 29 women and 21 men in each group. The mean age was 69 years (range, 51-87 years) in the PP group and 67 years (range, 50-85 years) in the NPP group (P = .060).
Univariate analyses confirmed significant differences between the PP and NPP groups for active scapular plane abduction (51°± 22° vs 135°± 29°; P < .001).
Radiographic Analysis
Univariate analysis of radiographic parameters showed significant differences between the PP and NPP groups for CSA (38.2°± 4.6° vs 35.2°± 3.7°; P = .002), ACHD (4.7 ± 2.2 vs 7.3 ± 2.6 mm; P < .001), Hamada stages (2.2 ± 1.2 vs 1.7 ± 0.9; P = .009), and PAH (22 ± 10 vs 17 ± 7 mm; P = .013).
Univariate analysis of magnetic resonance arthrography data showed relevant differences between the PP and NPP groups in terms of fatty infiltration of the SSC (2.2 ± 0.9 vs 1.4 ± 0.6; P < .001) and ISP (3.3 ± 0.6 vs 2.7 ± 0.6; P < .001) as well as anterior (–9°± 21° vs 25°± 12°; P < .001), posterior (–18°± 14° vs 2°± 14°; P < .001), and global RCT extension (207°± 26° vs 152°± 19°; P < .001). The anterior tear extension was graded 2.6 ± 0.9 (range, 1-4) in the PP group and 1.3 ± 0.5 (range, 1-2) in the NPP group (P < .001). Posterior tear extension was graded 2.8 ± 0.7 (range, 2-4) in the PP group and 2.2 ± 0.5 (range, 1-3) in the NPP group (P < .001). The global tear extension was greater than 200° in 33 (66%) of the patients in the PP group compared with no patient in the NPP group. Except for 1 patient, none of the PP group had a global tear extension less than 160° and no patient in the NPP group had a global tear extension greater than 180° (Figure 3).
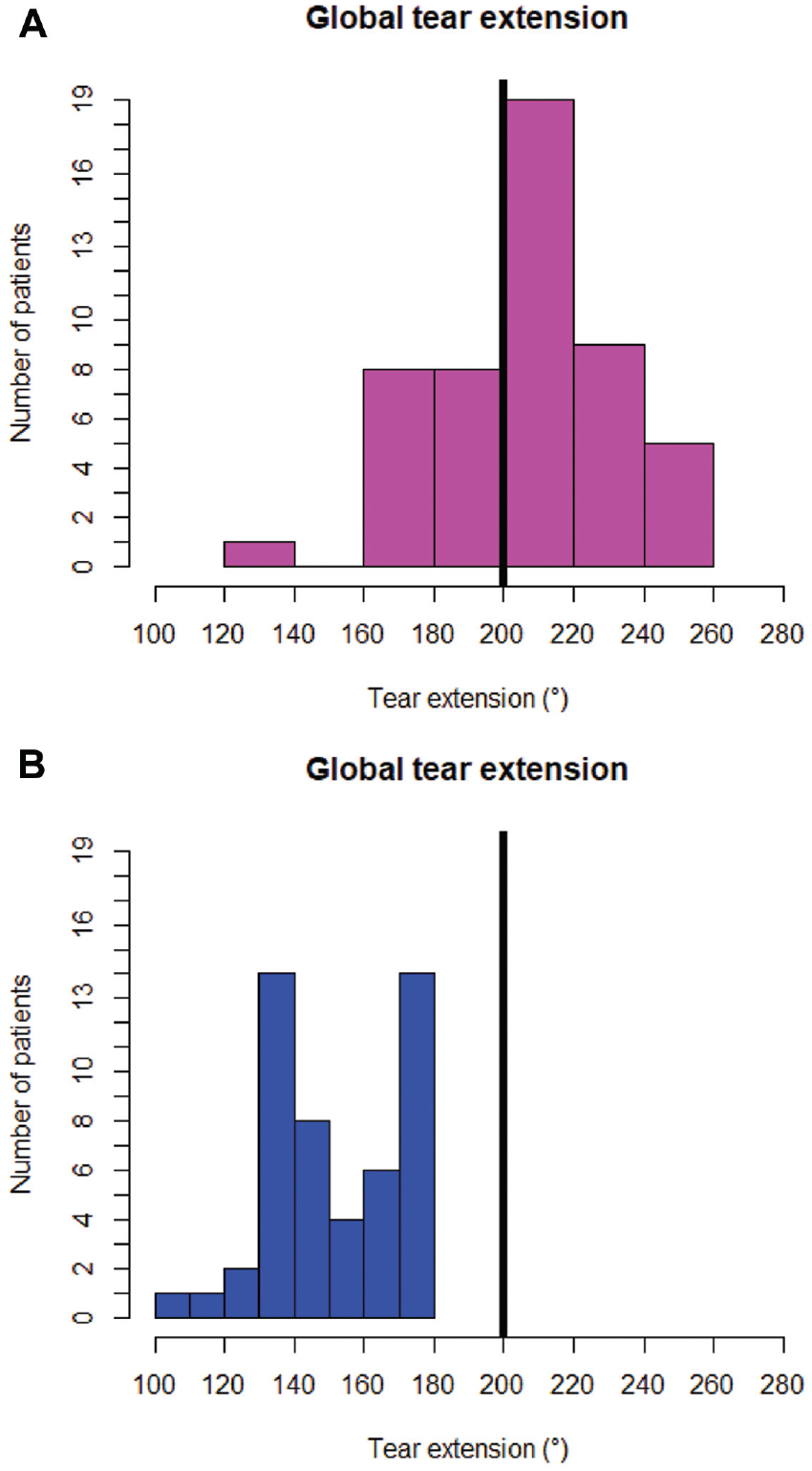
Distribution of global tear extension in patients with pseudoparalysis (PP) compared with those without PP. The black bar indicates 200° of global tear extension. (A) The global tear extension was greater than 200° in 33 (66%) of the patients with PP, and except for 1 patient, none in the PP group had a global tear extension less than 160°. (B) No patient in the group without PP had a global tear extension greater than 180°.
The calculated force couple ratio showed less SSC involvement in the NPP group (0.6 ± 0.2) compared with the PP group (1 ± 0.4; P < .001). Further details are shown in Table 1.
Radiographic Assessment Comparing Patients With Pseudoparalysis Versus Patients Without Pseudoparalysis a
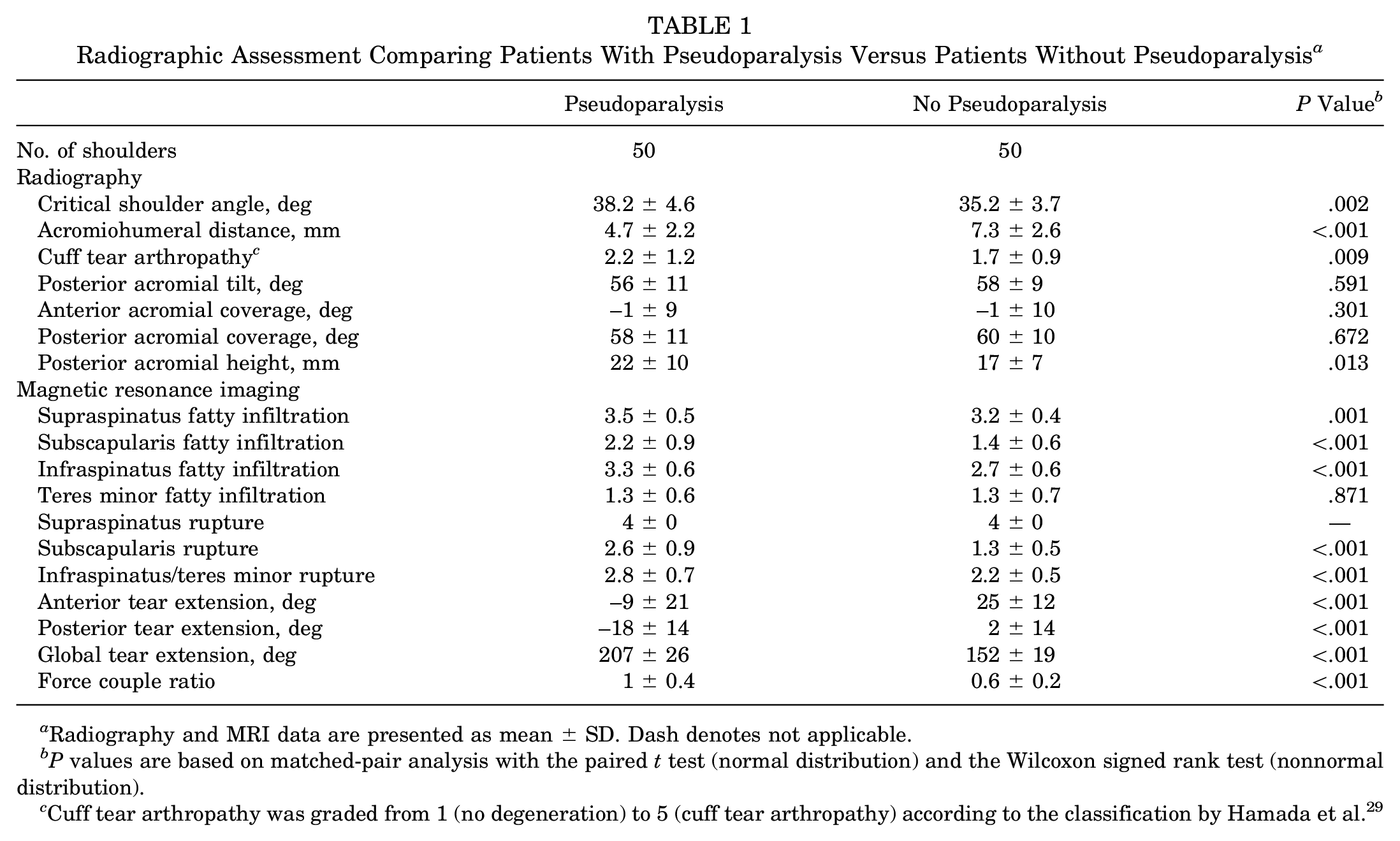
Radiography and MRI data are presented as mean ± SD. Dash denotes not applicable.
P values are based on matched-pair analysis with the paired t test (normal distribution) and the Wilcoxon signed rank test (nonnormal distribution).
Cuff tear arthropathy was graded from 1 (no degeneration) to 5 (cuff tear arthropathy) according to the classification by Hamada et al. 29
Multivariate analysis showed that the CSA (P = .001), ACHD (P < .001), PAH (P = .005), and anterior (P < .001) and posterior (P < .001) tear extension were independent factors associated with PP (Figure 4). The Hosmer-Lemeshow test confirmed goodness of fit of the model (P = .999).
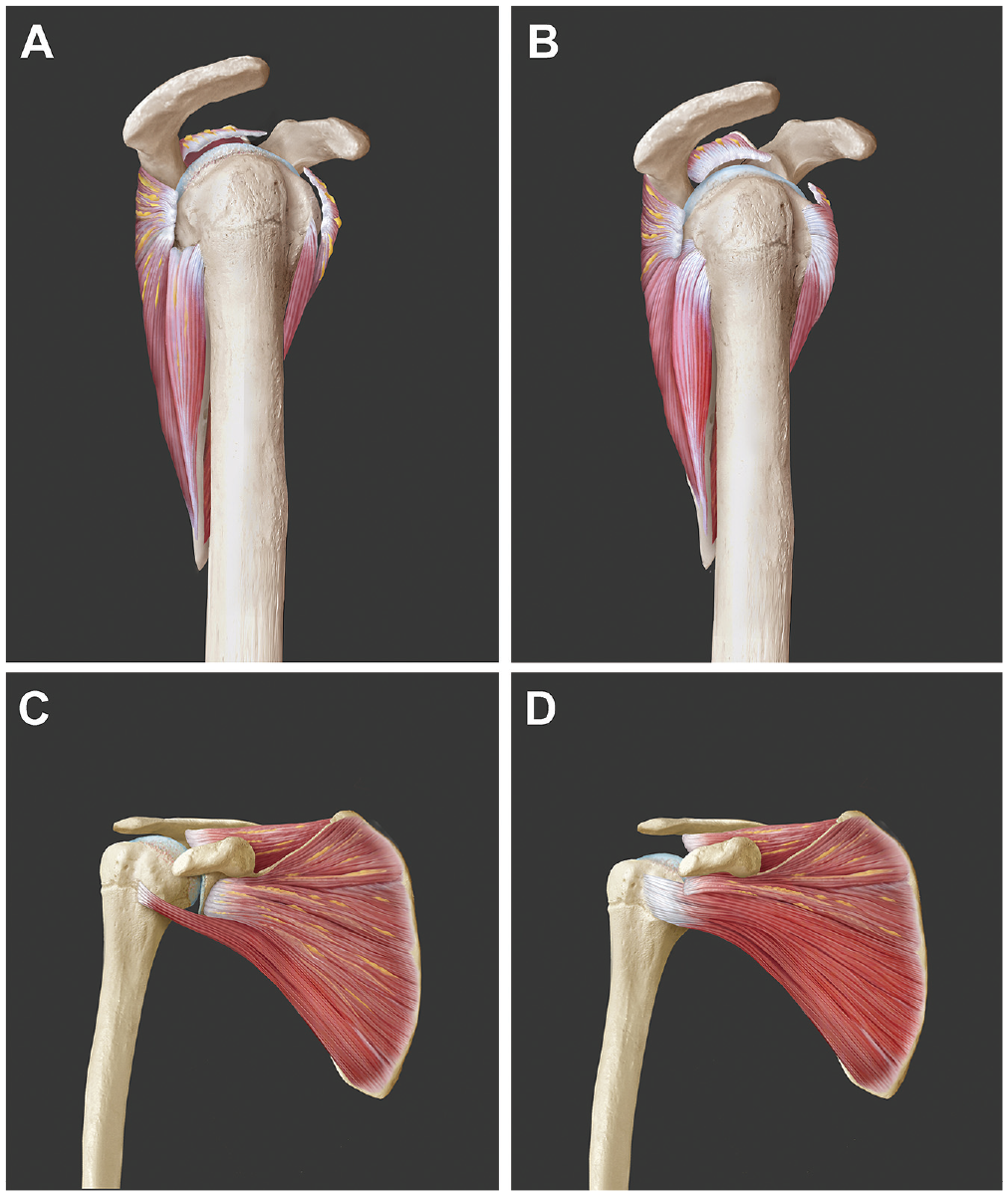
Specific characteristic of scapular morphologic characteristics and rotator cuff tear pattern in patients with pseudoparalysis (PP) compared with those without PP. In the sagittal plane, patients (A) with PP showed a significantly higher mean global rotator cuff tear extension and fatty infiltration, with involvement of the inferior half of the subscapularis tendon, and a higher oriented acromion compared with patients (B) without PP. In the coronal plane, patients (C) with PP showed a significantly higher critical shoulder angle and less acromiohumeral distance compared with patients (D) without PP.
Interobserver reliability was either very good or good for the CSA (r = 0.83; 95% CI, 0.60-0.93), ACHD (r = 0.74; 95% CI, 0.40-0.89), posterior acromial tilt (r = 0.85; 95% CI, 0.62-0.94), AAC (r = 0.82; 95% CI, 0.58-0.92), PAC (r = 0.81; 95% CI, 0.56-0.92), PAH (r = 0.87; 95% CI, 0.69-0.95), Hamada stages (r = 0.89; 95% CI, 0.73-0.95), and anterior (r = 0.79; 95% CI, 0.53-0.91) and posterior tear extension (r = 0.82; 95% CI, 0.52-0.93).
Discussion
This study confirms that tearing and degeneration of the SSC, especially of its inferior half, and also of the ISP and TM tendons are strongly associated with loss of active scapular plane abduction to more than 90°. New findings of this study are that the bony anatomic nature of the acromion is significantly different in patients with PP compared with those without PP: Patients with PP have a larger CSA, less ACHD, and a higher acromion, which is oriented in the sagittal plane.
A large CSA has been identified as an important anatomic predictor for degenerative RCTs, especially supraspinatus tears.1,5,12,23,31,39 Experimental studies showed that a large CSA was associated with increased loads on the supraspinatus tendon during abduction to elevate or stabilize the arm in space.25,36,41 Theoretically, this leads to tendon overloading and is compatible with tendon degeneration in larger CSAs. The remaining components of the rotator cuff, namely, ISP/TM and SSC, center the humeral head against the decentering deltoid vector until failure of the ISP, which is the strongest abductor of the rotator cuff. 21 If the tear expands into the inferior half of the SSC, the head is no longer stabilized against anterior displacement upon attempted abduction, and PP is very likely with loss of control of the center of rotation.
The mean CSA in the PP group was significantly larger compared with the NPP group. Reduction of an abnormally large CSA could reduce the vertical thrust of the deltoid, allowing generation of a better abduction moment for the deltoid muscle with more biomechanical synergism with the residual cuff. Whether lateral acromioplasty in the situation of debridement of irreparable mRCTs 42 has the potential to increase the role of the deltoid to the extent that PP can be reversed is unknown, but formerly published results of acromionectomy in mRCT repair are compatible with this hypothesis. 6 The feasibility and safety of arthroscopic correction of the CSA through lateral acromioplasty were proven in vivo. 23
Recently, more attention has been paid to the morphologic characteristics of the posterior acromion in the sagittal plane.2,3,30 A wider posterior acromial coverage of the humeral head has been described as a risk factor for RCT. 2 We found no significant difference in terms of anterior or posterior acromial coverage between patients with PP and those without PP. Conversely, acromia of patients with PP were significantly higher with respect to the center of the glenoid than in patients without PP. The biomechanical meaning of a higher position of the acromion on rotator cuff mechanics and glenohumeral stability is not yet fully understood and is the subject of ongoing biomechanical studies.
The current analysis of the relationship of RCT size and pattern with PP is in line with previous studies.10,13,44 Patients with PP had a significantly greater mean global RCT extension, by more than 50°, and except for one patient, none of the PP patients had a global tear extension less than 160°. In contrast, none of the NPP group had a global tear extension greater than 180°. It seems that with a global tear extension less than 160°, the shoulder can be kept centered and functionally compensated. If the tear exceeds 200°, decompensation is highly likely, especially if the inferior half of the SSC is compromised. Wieser et al 44 reported a 21-fold higher odds ratio for PP if more than 25% of the SSC was involved in the setting of mRCT (≥2 tendons involved), and others showed that 80% of patients were pseudoparalytic if a complete SSP tear extended into the inferior SSC. 10 We also found significantly more fatty infiltration and tear extension of the SSC in patients with PP compared with the NPP group. The calculated force couple ratio showed less SSC involvement in the NPP group, which is in contrast to the force couple theory of Burkhart.7,8 Rather than a balanced size of the remaining anterior and posterior rotator cuff, a stronger anterior rotator cuff seems to be essential for retaining reasonable shoulder function, but this issue requires further biomechanical investigation. To preserve a mechanical fulcrum to allow the deltoid muscle to abduct the arm, partial SSC repair might be considered to retain shoulder function.13,24,37
A main limitation of this study is the lack of shared understanding of the definition of pseudoparalysis. The current definition includes the inability to actively elevate to 90° a pain-free shoulder that has normal passive range of motion and no neurological deficit. 43 Because maintaining 90° of scapular plane abduction corresponds to about 55% of full active elevation, 27 critics have raised concerns about the validity of this cutoff value. Further, measurement inaccuracy could appear due to calculation errors of angles or distances. Another limitation is the retrospective design of this study with its associated biases. Given that this is a matched-pair analysis with sufficient power based on an a priori analyses, the effect of these potential biases is limited. Finally, this study did not examine the ability of surgical intervention to treat the natural history of mRCT, and the clinical importance of the current finding is therefore speculative.
Conclusion
This study confirms that global rotator cuff tear extension and the quality of the inferior half of the subscapularis tendon are significantly associated with chronic pseudoparalysis. The study further shows that the acromial morphologic state is another relevant factor in the development of pseudoparalysis. Patients with pseudoparalysis have a larger critical shoulder angle, smaller acromiohumeral distance, and a higher positioned acromion in the sagittal plane.
Footnotes
Submitted October 14, 2019; accepted April 1, 2020.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.