
Abstract
Background:
Anterior cruciate ligament (ACL) injuries and reconstruction (ACLR) promote quadriceps muscle atrophy and weakness that can persist for years, suggesting the need for more effective rehabilitation programs. Whether neuromuscular electrical stimulation (NMES) can be used to prevent maladaptations in skeletal muscle size and function is unclear.
Purpose:
To examine whether early NMES use, started soon after an injury and maintained through 3 weeks after surgery, can preserve quadriceps muscle size and contractile function at the cellular (ie, fiber) level in the injured versus noninjured leg of patients undergoing ACLR.
Study Design:
Randomized controlled trial; Level of evidence, 1.
Methods:
Patients (n = 25; 12 men/13 women) with an acute, first-time ACL rupture were randomized to NMES (5 d/wk) or sham (simulated microcurrent electrical nerve stimulation; 5 d/wk) treatment to the quadriceps muscles of their injured leg. Bilateral biopsies of the vastus lateralis were performed 3 weeks after surgery to measure skeletal muscle fiber size and contractility. Quadriceps muscle size and strength were assessed 6 months after surgery.
Results:
A total of 21 patients (9 men/12 women) completed the trial. ACLR reduced single muscle fiber size and contractility across all fiber types (P < .01 to P < .001) in the injured compared with noninjured leg 3 weeks after surgery. NMES reduced muscle fiber atrophy (P < .01) through effects on fast-twitch myosin heavy chain (MHC) II fibers (P < .01 to P < .001). NMES preserved contractility in slow-twitch MHC I fibers (P < .01 to P < .001), increasing maximal contractile velocity (P < .01) and preserving power output (P < .01), but not in MHC II fibers. Differences in whole muscle strength between groups were not discerned 6 months after surgery.
Conclusion:
Early NMES use reduced skeletal muscle fiber atrophy in MHC II fibers and preserved contractility in MHC I fibers. These results provide seminal, cellular-level data demonstrating the utility of the early use of NMES to beneficially modify skeletal muscle maladaptations to ACLR.
Clinical Relevance:
Our results provide the first comprehensive, cellular-level evidence to show that the early use of NMES mitigates early skeletal muscle maladaptations to ACLR.
Registration:
NCT02945553 (ClinicalTrials.gov identifier)
Keywords
Anterior cruciate ligament (ACL) injuries and reconstruction (ACLR) promote muscle weakness that can persist for years despite rehabilitation.25,31 Persistent muscle weakness contributes to dissatisfaction with ACLR 16 and may hasten the progression of osteoarthritis, 31 suggesting the need for improvements in current rehabilitation programs.
Neuromuscular electrical stimulation (NMES), which initiates muscle contraction by passing a current through electrodes placed over muscles, is often used as an adjunct to rehabilitation programs to circumvent neural activation deficits after injuries and surgery. 20 However, more extensive use of NMES in a more proactive manner after the index injury and surgical repair may produce greater benefits, as NMES prevents muscle atrophy in patients after orthopaedic injury/surgery.10,14,21 Despite these benefits, clinicians may be reluctant to prescribe NMES, as its ability to prevent atrophy and improve strength remains controversial. For instance, when NMES is added as an adjunct to standard rehabilitation beginning several weeks after surgery, no additive benefit to improve strength has been noted. 26 A recent meta-analysis revealed that NMES is more effective at improving muscle strength and function when instituted earlier after surgery. 15 In this context, it appears the benefits of NMES to prevent muscle atrophy and weakness may be realized when it is instituted closer to periods of muscle disuse and trauma related to the ACL injury and ACLR.
Testing the efficacy of rehabilitation interventions instituted early after an injury and surgery on muscle size and strength is complicated by clinical and practical limitations. Maximal or near maximal voluntary contractions are contraindicated because of the potential for further injuries 2 and are unreliable because of neural activation deficits. 20 To circumvent these problems, we can study muscle at the cellular (ie, fiber) level. Fundamentally, whole muscle strength is a function of the size and contractility of its constituent fibers. Muscle fiber size and contractility, in turn, are determined by the quantity and type of myofilament proteins expressed (eg, myosin and actin) and their contractility. As myofilament proteins are the end effectors of contraction, 11 any change in their quantity and/or contractility modifies the base functionality of the muscle. 11 Accordingly, muscle fiber size and contractility set absolute functional limits on muscle, making them useful outcome measures to test the efficacy of early rehabilitation interventions.
Our primary objective was to evaluate whether NMES, instituted soon after an injury and maintained through 3 weeks after ACLR, can preserve skeletal muscle fiber size and contractility. We assessed muscle fiber size and contractility because, as detailed above, they are important determinants of whole muscle function, and because of methodological and practical limitations in assessing whole skeletal muscle size and functionality at this early postsurgical time point using conventional tissue imaging and whole muscle functional assays. We hypothesized that the early use of NMES after injuries and surgery would mitigate muscle fiber atrophy and prevent contractile dysfunction secondary to disuse and trauma related to both the index injury and surgery. A secondary objective was to explore whether early NMES use enhances whole muscle strength at later time points.
Methods
This study was designed as a prospective, randomized, sham-controlled, blinded trial (NCT02945553) in which data were available for each patient on both the injured, surgical leg and the contralateral, noninjured leg. For a priori sample size calculations, using published 21 and preliminary data in other orthopaedic surgical patients, we expected reductions in the injured leg in muscle fiber cross-sectional area (CSA) of –30% and –40% in myosin heavy chain (MHC) I and MHC II fibers, respectively, as well as reductions in maximal isometric tension (–50%) and contractile velocity (–30%) in MHC II fibers. From data in previous publications8,10,14 and our preliminary work, we hypothesized that NMES would prevent atrophy in MHC I (0%) and MHC II (–10%) fibers and reduce losses in maximal isometric tension (–40%) and increase contractile velocity (+20%) in MHC II fibers. The detection of group differences in muscle fiber CSA guided the final cohort size, requiring 20 participants with a power of 87% at an alpha of .05. We planned to enroll 24 patients, assuming an approximately 20% loss to follow-up.
Patients
Enrollment started in November 2016 and ended in December 2018, with the last follow-up visit in July 2019. A total of 79 patients with an acute, first-time ACL rupture were screened (Figure 1). Inclusion criteria included the following: (1) 18-50 years of age; (2) body mass index <35 kg/m2; (3) acute (<3 weeks from injury), first-time ACL rupture with or without a meniscal injury; and (4) scheduled to undergo surgical reconstruction with any type of graft material. Exclusion criteria included the following: (1) history of knee/lower extremity surgery; (2) abnormal laxity of any knee ligament at surgery other than the injured ACL; (3) signs or symptoms of arthritis, autoimmune/inflammatory disease, or diabetes; (4) grade ≥IIIb articular cartilage lesions (International Cartilage Repair Society criteria) to the tibiofemoral joint; and/or (5) women who are/plan on becoming pregnant.
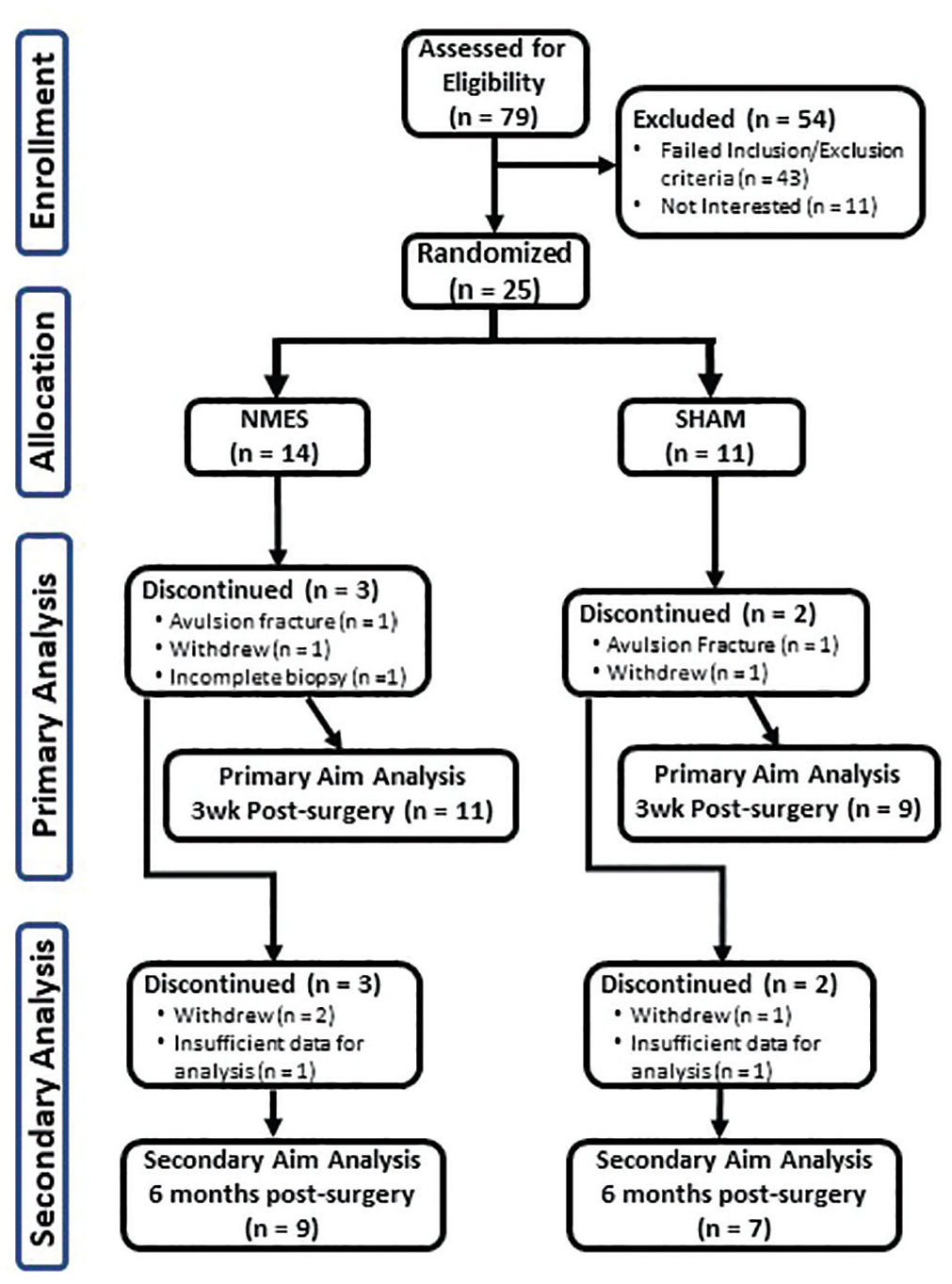
CONSORT (Consolidated Standards of Reporting Trials) diagram. NMES, neuromuscular electrical stimulation.
Patients were randomized (1:1) using a covariate adaptive approach to receive NMES or sham (simulated microcurrent electrical nerve stimulation [MENS]) treatment with stratification for age, sex, and graft material. There were 2 unblinded study personnel (T.W.T., R.H.C.) who enrolled volunteers, assigned them to intervention arms, and trained them to undergo NMES or MENS (sham). All personnel performing assessments on patients/tissue or responsible for analysis of data were blinded to group assignment. Of the 25 (12 men/13 women) patients enrolled and randomized (14 NMES/11 sham), 20 (11 NMES/9 sham) completed 3-week postsurgical testing and were included in primary analyses (single muscle fiber size and contractility), and 16 (9 NMES/7 sham) completed 6-month postsurgical testing with data for secondary analyses (whole muscle strength). All protocols were approved by our institutional ethics committee and written informed consent obtained from each patient before participation.
Protocol
Patients were evaluated twice before surgery, at the time of enrollment and within 1 week before surgery, and 3 weeks and 6 months after surgery. Presurgical testing at enrollment consisted of muscle strength on the noninjured leg and clinical and patient-oriented assessments. Testing at 1 week before surgery was identical but included bilateral muscle strength testing. Weightbearing physical activity was measured by accelerometry for three 5-day periods both between the time of enrollment and surgery and during the first 3 weeks after surgery. At 3 weeks after surgery, bilateral, percutaneous biopsy specimens were taken from the vastus lateralis muscles and computed tomography performed. For one 5-day period during postsurgical months 2 through 5, weightbearing activity was assessed by accelerometry. At 6 months after surgery, whole muscle strength and size were measured bilaterally, whole leg function was assessed by a single-leg hop, and clinical and patient-oriented assessments were performed
Treatment Interventions
Patients randomized to NMES on the quadriceps of their injured/operative leg (Continuum; Empi) began the intervention within 3 weeks of injury and continued until 3 weeks after surgery. NMES was discontinued just before surgery and resumed within 72 hours after surgery. Patients underwent NMES at home 5 days per week for 60 minutes per day (5-minute warm-up, 50-minute stimulation session, and 5-minute cool down). The device administered symmetrical, biphasic pulses (400 µs at 50 Hz), with a duty cycle of 25% (10 seconds on, 30 seconds off), with parameters based on our previous work. 30 Electrode pads (7.5 × 13.5 cm) were placed horizontally on the proximal and distal aspects of the quadriceps. A bolster was placed under the knee joint and an ankle weight used to immobilize the leg at approximately 40° relative to full knee extension, 2 with the goal of obtaining tetanic isometric contractions within pain tolerance.
To remove the bias of patients anticipating a benefit from an active treatment, patients randomized to MENS (300PV; Empi) (Appendix Figure A1, available in the online version of this article) underwent sham stimulation (ie, device administered no electrical current) and were told that the device administered imperceptible MENS for pain mitigation. Patients in the NMES group were told that, in addition to causing contractions, NMES had pain-mitigating effects to distribute any placebo effect equally across groups. Participants underwent MENS (sham) at home 5 days per week for 60 minutes per day.
Each patient demonstrated proficiency using the device while supervised by unblinded study personnel and was contacted within 72 hours of training to ensure proficiency, with regular weekly contacts thereafter to encourage adherence and assess problems. Adherence to the NMES or MENS (sham) intervention was tracked with the compliance monitoring feature of the device software.
All participants underwent ACLR rehabilitation with similar goals and benchmarks, as described. 3 Restrictions after surgery were weightbearing to tolerance, except for patients undergoing meniscal repair, in whom restrictions were 50% weightbearing with crutches for 4 weeks after surgery and then progressing to partial weightbearing with 1 crutch through week 5 and full weightbearing by week 6. A patient with a meniscus root avulsion was nonweightbearing for 6 to 8 weeks after surgical repair.
Knee Extensor Muscle Function
Isometric (70°) and isokinetic (60 and 180 deg/s) peak torque about the knee were evaluated using a HUMAC NORM 770 dynamometer (CSMi Solutions), as described previously 31 and in detail in the Appendix (available online).
Physical Activity
Weightbearing activity was measured with a uniaxial accelerometer (GT1M; ActiGraph) using raw activity counts, with details described in the online supplement.
Thigh Muscle Size
Thigh muscle tissue CSA was measured by computed tomography, as described previously 4 and in detail in the Appendix (available online).
Muscle Biopsy
Percutaneous biopsies of the vastus lateralis muscles were performed bilaterally, as previously described 12 and detailed in the Appendix (available online). A portion of the muscle was frozen in embedding medium (optimal cutting temperature; Sakura Finetek) and stored at −80°C until analysis. Another portion of the sample was placed immediately into cold (4°C) dissecting solution, dissected into small fiber bundles, chemically skinned, and then stored for single fiber contractile assessments, with procedures and solutions as described. 5
Muscle Fiber Size
Single muscle fiber size was assessed using immunohistochemistry, as described previously 22 and detailed in the Appendix (available online). We chose to assess skeletal muscle CSA because it is the base measure of overall muscle size, which is an essential determinant of whole muscle functionality. More specifically, single muscle fiber CSA provides an index of the content of myofilaments, which are the end effectors of contraction and, as such, a fundamental determinant of muscle functionality.
Muscle Fiber Contractility
Segments (~2-3 mm) of chemically skinned fibers were isolated and cellular-level contractility measured (25°C) within 3 weeks of the biopsy, as described previously 5 and in detail in the Appendix (available online). Measurements were conducted under maximal Ca2+-activated conditions and included maximal isometric force production (Fmax), maximal isometric tension (Tmax; force production per fiber CSA), maximal shortening velocity (Vmax), and maximal power production (Pmax) using isotonic load clamps. These indices represent the basic mechanical/contractility indices that describe the functional patency of skeletal muscle, and the assessment of these indices in chemically skinned single fiber preparation provides a clear indication of the functionality of myofilament proteins that have historically been used in the muscle physiology field and shown to determine whole muscle functionality. 18 All fibers were analyzed to determine the MHC isoform composition by gel electrophoresis, as described previously 23 and in detail in the online supplement.
Lower Extremity Function and Patient- and Clinician-Reported Outcomes
Single-leg hop tests were conducted, as previously described 31 and detailed in the Appendix (available online). Patient-reported assessments of their knee were performed using the Knee injury and Osteoarthritis Outcome Score 28 and International Knee Documentation Committee (IKDC) 2000 subjective form. 17 Knee range of motion was measured by goniometry with the participant supine and a knee examination performed according to the IKDC 2000 knee examination form. 17
Statistical Analysis
For variables with multiple observations within a participant (eg, muscle fiber size and contractility), repeated-measures mixed-model analyses of variance were used, with leg (injured and noninjured) and treatment group (sham and NMES) as factors. Analyses were limited to fibers expressing MHC I, MHC IIA, and MHC IIA/IIX because other MHC isotype fibers (I/IIA, I/IIA/IIX, and IIX) were too few to permit analyses. Whole muscle CSA and strength data were expressed as injured relative to noninjured leg, with the former evaluated using unpaired t tests and the latter using analyses of covariance, with quadriceps CSA as a covariate. Strength in the noninjured leg over time was evaluated using repeated-measures analyses of variance, with time and treatment group as factors. Data were analyzed using SAS (v 9.4; SAS Institute) or SPSS (v 23; IBM) and presented as mean ± SE.
Results
Patient Characteristics and Interventions
Treatment groups were similar for sex distribution, age, height, and weight and did not differ for time between milestones (Table 1). Data are not shown for 2 participants who withdrew after enrollment and 2 who were excluded (3 men/1 woman). For primary aim analysis, 2 patients in the NMES group had insufficient muscle tissue to allow fiber contractility assessments in 1 leg. For secondary aim analysis, 3 participants withdrew before 6-month testing, and 2 lacked whole muscle size data because of technical or scheduling problems. Additionally, 1 patient was not medically cleared to, and 2 others chose not to, complete single-leg hop testing. No adverse events or unanticipated problems occurred with the NMES or sham intervention. Adherence in the NMES group was 85% ± 5% (range, 42%-100%) and was 63% ± 8% (range, 19%-98%) in the sham group. The intervention period was similar in the NMES (58 ± 7 days) and sham (57 ± 7 days) groups. Of note, we did not restrict individual therapists’ treatment of patients to exclude electrotherapy (eg, NMES, transcutaneous electrical nerve stimulation) but asked patients to report any use of these modalities. No patient reported undergoing electrotherapy outside of that provided by the study interventions.
Physical and Clinical Characteristics of Patients a
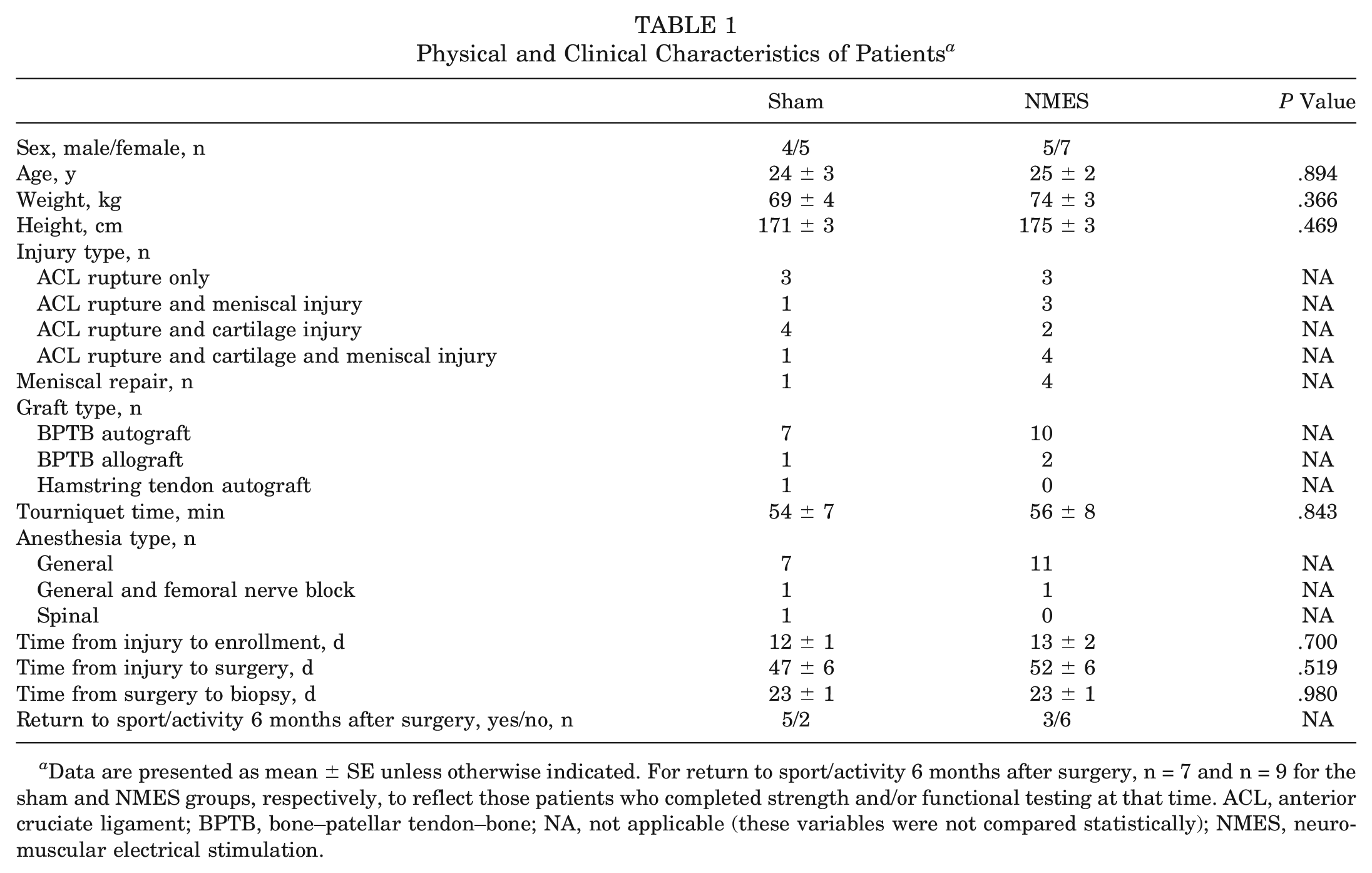
Data are presented as mean ± SE unless otherwise indicated. For return to sport/activity 6 months after surgery, n = 7 and n = 9 for the sham and NMES groups, respectively, to reflect those patients who completed strength and/or functional testing at that time. ACL, anterior cruciate ligament; BPTB, bone–patellar tendon–bone; NA, not applicable (these variables were not compared statistically); NMES, neuromuscular electrical stimulation.
Physical Activity
No group differences were found in physical activity level before surgery or during the first 3 weeks after surgery nor the slope of the activity/time relationship from 1 to 5 months after surgery (Table 2).
Physical Activity Measured by Accelerometry a
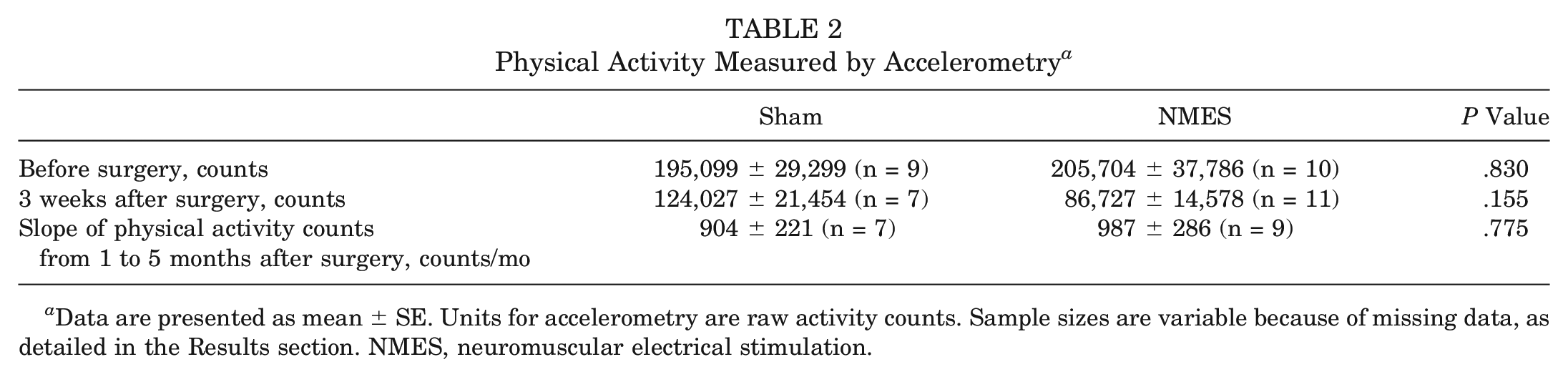
Data are presented as mean ± SE. Units for accelerometry are raw activity counts. Sample sizes are variable because of missing data, as detailed in the Results section. NMES, neuromuscular electrical stimulation.
Single Muscle Fiber Size 3 Weeks After ACLR
We found leg effects (ie, comparison between injured and noninjured legs; all P < .001) for lower muscle fiber CSA in the injured leg for all fiber types (Figure 2). Additionally, we observed leg × group interaction effects for single muscle fiber CSA for all fiber types pooled (P < .01) and in MHC IIA (P < .01) and MHC IIA/IIX (P < .001) fibers. The interaction effect was driven by reduced atrophy in the NMES group, although atrophy remained apparent in both groups (P < .001 to P < .01).
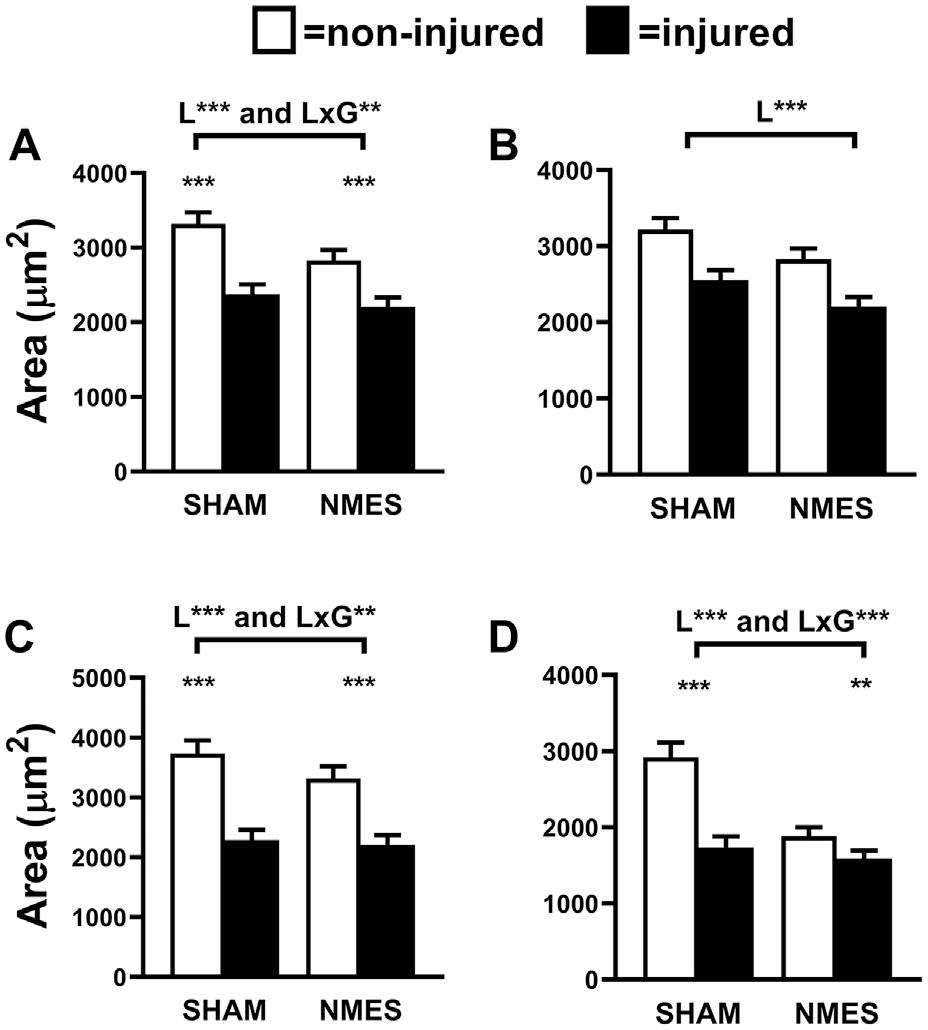
Skeletal muscle fiber size in (A) pooled, (B) myosin heavy chain (MHC) I, (C) MHC IIA, and (D) MHC IIA/IIX fibers in noninjured (clear) and injured (filled) legs of participants randomized to sham (simulated microcurrent electrical nerve stimulation) and neuromuscular electrical stimulation (NMES) interventions. Leg (L) and leg by group (L × G) interaction effects are indicated above the brackets. Pairwise analysis of differences between legs, where L × G interaction effects were apparent, are indicated by symbols directly above bars. Data represent mean ± SE. **P < .01. ***P < .001.
Single Muscle Fiber Contractility 3 Weeks After ACLR
Leg effects were found for lower muscle fiber Fmax in the injured leg for all fiber types (MHC I: P < .01; MHC IIA: P < .001; MHC IIA/IIX: P < .001) (Table 3). Given muscle fiber atrophy (Figure 2), we evaluated whether deficits in Fmax were explained by atrophy by normalization to CSA (ie, Tmax). Leg effects were found for lower muscle fiber Tmax (P < .001) in the injured leg across fiber types, with no leg × group interaction effects for Fmax (MHC I: P = .14; MHC IIA: P = .50; MHC IIA/IIX: P = .49) or Tmax (MHC I: P = .37; MHC IIA: P = .63; MHC IIA/IIX: P = .66).
Skeletal Muscle Fiber Function at 3 Weeks After Surgery a

Data are presented as mean ± SE. For leg × group interaction effects, symbols indicating pairwise differences between legs are placed next to the value for the injured leg. n = 10 for the NMES group because of inadequate tissue. Fmax, maximal isometric force production; MHC, myosin heavy chain; NMES, neuromuscular electrical stimulation; Pmax, maximal power production; Tmax, maximal isometric tension; Vmax, maximal shortening velocity.
P < .01.
P < .001.
Leg effects for Vmax were observed for MHC IIA (P < .001) and MHC IIA/IIX (P < .01) fibers, reflecting reductions in both fiber types in the injured leg (Table 3). Leg × group effects were found for Vmax in MHC I fibers. Pairwise comparisons showed that this interaction effect reflected a reduction in sham (P < .001) and an increase in NMES (P < .001).
Finally, leg effects for Pmax were found for MHC IIA and IIA/IIX fibers (both P < .001), reflecting reduced Pmax in both fiber types of the injured leg (Table 3). Leg × group effects were found for Pmax in MHC I fibers, with pairwise comparisons showing that this interaction effect was caused by a reduction in sham (P < .01).
Whole Muscle Size and Function 6 Months After ACLR
We observed no group × time interaction effects for any knee extensor muscle strength parameter throughout the study in the noninjured leg (Appendix Figure A2, available online). We found no group differences in the ratio of injured-to-noninjured leg quadriceps CSA at 3 weeks after surgery (Appendix Table A1, available online), but the ratio was lower (P < .05) in the NMES group 6 months after surgery. There were no group differences in knee flexor muscle CSA at 3 weeks or 6 months after surgery.
No group effects were found for isometric or isokinetic strength measurements 6 months after surgery when adjusting for quadriceps muscle CSA (Appendix Table A2, available online). We also found no group differences in patient- or clinician-reported outcomes or single-leg hop performance (Appendix Table A3, available online) 6 months after surgery.
Discussion
Our study is novel in starting NMES near the time of injury and continuing it into the early postsurgical period. This contrasts with the more common clinical use of NMES as an adjunct to standard rehabilitation to address neural activation deficits. To our knowledge, this is the first study to provide mechanistic cellular data in the setting of a randomized, sham-controlled, blinded trial that demonstrates the efficacy of NMES to beneficially modify both muscle fiber size and contractility.
Skeletal Muscle Fiber Size
ACL injuries and ACLR caused marked muscle fiber atrophy (–26%), with more prominent atrophy in fast-twitch MHC II fibers (–29% to −35%). Considering this, as well as reports that MHC II fibers do not regain size by the time that patients return to activity, 24 the effect of NMES to mitigate atrophy specifically in MHC II fibers is clinically significant, as atrophy prevention is a goal of orthopaedic rehabilitation. Of note, although baseline fiber size was higher in the noninjured leg in the sham group for some fiber types, this likely did not affect differences between legs, as baseline muscle fiber size in the noninjured leg did not correlate with the ratio of injured-to-noninjured muscle fiber size across fiber types (P = .838 to .345). To our knowledge, only 1 other study evaluated the effects of NMES on muscle fiber size in ACL-injured patients. 1 In that study, NMES combined with isometric contractions at 6 weeks after surgery reduced muscle atrophy in women, but not men, compared with isometric contractions alone. 1 However, the surgical leg was cast immobilized during the intervention, which is an outdated clinical practice that could influence responsiveness to NMES. Similar to our results, NMES mitigates atrophy in patients undergoing total knee arthroplasty 21 or in those with lower extremity fractures 10 when started soon after surgery/casting. Thus, using NMES closer to the index injury and surgery may derive benefits in preventing muscle atrophy in patients undergoing ACLR.
Many studies show that NMES completely prevents muscle atrophy,8,10,21 although our data suggest a more modest antiatrophic effect. One key difference is that most previous work evaluated whole muscle size, which could suffer bias from fluid infiltration into muscle, which would register as muscle tissue. 27 The amount of fluid infiltration into muscle could vary among patients by surgical trauma/tissue edema, degree of muscle disuse, or other factors. Indeed, one could speculate that NMES might modulate the fluid content of muscle in patients, with effects in either direction: reducing the fluid content via rhythmic contractions or increasing tissue fluid through contraction-induced muscle damage. 9 Examples of this potential bias are shown in disagreements between whole muscle and cellular muscle size estimates in studies evaluating the effects of NMES in orthopaedic and nonorthopaedic populations,8,10,24 including the current study. Because of this potential bias, we urge caution in the interpretation of whole muscle size data and suggest single muscle fiber assessments as a more rigorous approach to evaluate the effects of NMES, particularly during the early postsurgical period.
Skeletal Muscle Fiber Function
ACL injuries and ACLR reduced all single fiber contractile indices across all major fiber types, sometimes markedly. These results agree with recent studies that show reduced single muscle fiber force production and tension in patients undergoing ACLR compared with noninjured control patients. 13 Importantly, this study showed that these variables were reduced from the time of surgery until 6 months after surgery, with a nadir at 1 month after surgery. Together, these results suggest that the function of myofilament proteins (eg, myosin, actin), the end effectors of muscle contraction, are severely impaired after an injury and surgery. Accordingly, intrinsic muscle fiber contractility is a suitable target for clinical rehabilitation. To this point, NMES prevented reductions in single muscle fiber Pmax and increased Vmax in MHC I fibers. We originally hypothesized that NMES would affect MHC II fibers, as they are thought to be more important determinants of whole muscle strength 18 and, in turn, gains in strength with NMES. 15 MHC I fibers, however, may become a more prominent modulator of whole muscle function in patients with orthopaedic conditions, as we have shown correlations between whole muscle function and single MHC I fiber function (Vmax) in older adults with knee osteoarthritis 6 as well as between MHC I fiber contractility 3 weeks after surgery and whole muscle isometric and isokinetic strength 6 months after surgery in a separate cohort of patients undergoing ACLR (Tourville et al. unpublished data). Indeed, MHC I fibers may limit whole muscle power output. 18 Collectively, these results uncover a novel role for MHC I fiber contractility in whole muscle strength/performance in orthopaedic populations as well as NMES to benefit slow-twitch MHC I fiber contractility in patients undergoing ACLR.
Whole Muscle Strength
We found no effect of NMES to alter isometic or isokinetic knee extensor torque 6 months after surgery. However, we urge caution in the interpretation of these results, as loss of patients to follow-up meant that we did not have adequate statistical power to detect differences in strength between groups. Additionally, functional recovery, as reflected in the numbers of patients returning to sport/activity in both groups (see Table 1), may have differed between the 2 groups. To this latter point, this may be because the extent of meniscal injuries was not perfectly balanced between the groups. Another reason for the failure to realize improvements in whole muscle strength is that our NMES regimen was only maintained until 3 weeks after ACLR. Recent recommendations suggest testing for neural activation deficits 3 weeks after surgery and continuing NMES in patients with persistent neural activation deficits. 29 Accordingly, the use of NMES longer than 3 weeks after surgery, or more frequently throughout our intervention, may have led to improvements in whole muscle strength. 15
Our study has important strengths, including the following: (1) carefully selected eligibility criteria to avoid confounding from previous knee injuries; (2) a sham, control intervention; (3) assessments of physical activity throughout the study; and (4) measurements of the quadriceps muscle at the cellular level to evaluate NMES effects in the early postsurgical period. However, there are limitations that must be acknowledged. First, the extent of concomitant meniscal injuries was not perfectly balanced by randomization. More meniscal injuries and repair in the NMES group could affect postsurgical weightbearing. While no group differences in physical activity were noted, mean activity was 30% lower in the NMES than sham group during the first 3 weeks after surgery. If anything, this would bias against finding an effect of NMES on primary outcomes. That we still observed effects of NMES underscores the robustness of these effects. Group differences in meniscal injuries/repair and, in turn, weightbearing could affect whole muscle strength measurements at 6 months, although the effects of the degree of trauma on whole muscle function is controversial. 19 Second, our study was not adequately powered to assess group differences in whole leg function (ie, single-leg hop) or patient-reported outcomes/satisfaction because of patients lost from the 3-week to 6-month postsurgical assessments. Third, the effects of NMES to alter contractility of the uninjured limb 7 could affect the detection of group differences in whole muscle strength, although we found no group difference in knee extensor function in the noninjured leg soon after the injury up to 6 months after surgery. Finally, the generalizability of our results is limited to the confines of our cohort: namely, active patients with no history of significant knee trauma who suffered their first severe, acute ACL disruption and underwent ACLR with a bone–patellar tendon–bone graft (both autograft and allograft).
In conclusion, our study shows that both muscle fiber size and contractility were markedly reduced 3 weeks after surgery. These results are clinically relevant, as they suggest that both should be targeted by rehabilitation programs. Additionally, we found that early NMES after ACL injury and ACLR surgery beneficially modified adaptations in both muscle size and contractility at the cellular (ie, muscle fiber) level. While antiatrophic effects align with clinical indications for NMES use, we provide novel evidence for the effects of NMES on single fiber contractility. The functional implications of these beneficial effects of NMES on single muscle fiber size and function are unclear, as differences in whole muscle strength were not discerned 6 months after ACLR. Future trials are needed to determine whether these beneficial effects of NMES on intrinsic muscle fiber size and function early after ACLR, when patients are rapidly advancing their rehabilitation, translate into improved whole muscle function and patient-reported outcomes or the prevention of reinjuries or progression toward posttraumatic knee osteoarthritis. The use of NMES over a longer time interval after surgery, or more frequent daily/weekly use, may better maintain muscle size and strength and limit limb asymmetries when patients begin to return to sports and preinjury activity levels, in turn possibly protecting against future joint abnormalities. 31
Supplemental Material
DS_10.1177_0363546520933622 – Supplemental material for Utility of Neuromuscular Electrical Stimulation to Preserve Quadriceps Muscle Fiber Size and Contractility After Anterior Cruciate Ligament Injuries and Reconstruction: A Randomized, Sham-Controlled, Blinded Trial
Supplemental material, DS_10.1177_0363546520933622 for Utility of Neuromuscular Electrical Stimulation to Preserve Quadriceps Muscle Fiber Size and Contractility After Anterior Cruciate Ligament Injuries and Reconstruction: A Randomized, Sham-Controlled, Blinded Trial by Michael J. Toth, Timothy W. Tourville, Thomas B. Voigt, Rebecca H. Choquette, Bradley M. Anair, Michael J. Falcone, Mathew J. Failla, Jennifer E. Stevens-Lapslaey, Nathan K. Endres, James R. Slauterbeck and Bruce D. Beynnon in The American Journal of Sports Medicine
Footnotes
Acknowledgements
The authors thank all of the volunteers who dedicated their valuable time to this study.
Submitted November 12, 2019; accepted April 16, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was funded by a National Institutes of Health grant to M.J.T. and B.D.B. (AR069199). N.K.E. reports education and hospitality funds from Smith & Nephew and Prodigy Surgical (Arthrex) and hospitality funds from Zimmer Biomet, Synthes, RTI Surgical, Stryker, and DePuy Orthopaedics. J.R.S. reports education payments from Prodigy Surgical (Arthrex) and hospitality funds from Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.