
Abstract
Background:
The purpose of this study was to evaluate the clinical score and stability after meniscal allograft transplantation (MAT) after a previous anterior cruciate ligament (ACL) reconstruction.
Hypothesis:
Medial MAT would improve anteroposterior stability, and lateral MAT would improve rotational stability.
Study Design:
Cohort study; Level of evidence, 3.
Method:
We retrospectively investigated 31 cases of MAT after a previous total or nearly total meniscectomy and ACL reconstruction between November 2008 and June 2017. Cases were divided into medial (16 cases) and lateral (15 cases) MAT groups. The patients were assessed preoperatively and at the 2-year follow-up.
Results:
In the medial MAT group, the International Knee Documentation Committee, Lysholm, Lysholm instability, and Tegner scores improved significantly at the 2-year follow-up, and there were also significant improvements in the anterior drawer, Lachman, and pivot-shift tests. In the lateral MAT group, the Lysholm and Tegner scores improved significantly at the 2-year follow-up, as had the anterior drawer and Lachman tests but not the pivot-shift test. The medial MAT group showed significant improvement in side-to-side difference on Telos stress radiographs, from 6.5 mm (preoperatively) to 3.6 mm (2-year follow-up) (P = .001), while the lateral MAT group showed no significant change. There was no progression of arthritis in either group.
Conclusion:
Medial MAT improved not only anteroposterior stability but also rotational stability in the meniscus-deficient ACL-reconstructed knee. Lateral MAT showed improvements in the anterior drawer and Lachman tests but not in the pivot-shift test or side-to-side difference on Telos stress radiographs in meniscus-deficient ACL-reconstructed knees. Instability and pain are indications for MAT in meniscus-deficient ACL-reconstructed knees.
At least half of all patients with anterior cruciate ligament (ACL) ruptures also sustain meniscal tears, and 65% of the patients with meniscal tears undergo meniscectomies. 13 Long-term studies of ACL reconstruction have noted poorer knee stability in patients with combined meniscal and ACL injury.1,7-9 In vivo studies have also shown increased rotatory instability after meniscal removal in the setting of ACL reconstruction.12,17 Many studies have shown that meniscal deficiency increases the forces on the ACL graft, leading to secondary failure of ACL reconstruction.13,14
The importance of the medial meniscus in restraining anteroposterior translation of the tibia relative to the femur in the ACL-deficient knee has been well-documented.8,9 In comparison, the lateral meniscus is a more important restraint during a pivot shift. 11
The biomechanics of removing the medial and lateral menisci in the setting of an ACL-deficient knee are well-known and have led some surgeons to address meniscal deficiencies in the setting of ACL reconstruction. However, few studies have examined whether meniscal allograft transplantation (MAT) restores biomechanical deficits in a meniscus-deficient ACL-reconstructed knee. A cadaveric study by Spang et al 17 showed that MAT lowered the strain on the native ACL, thereby providing evidence supporting the use of MAT in ACL-reconstructed knees. However, no clinical studies have examined the effects of MAT after ACL reconstruction.
Therefore, the present study aimed to evaluate clinical scores and stability after MAT in knees that had previously undergone ACL reconstruction. We hypothesized that medial MAT would restore anteroposterior stability and lateral MAT would restore rotational stability.
Methods
Patient Selection and Study Design
The present study retrospectively evaluated 62 patients who underwent medial or lateral MAT after ACL reconstruction with a subtotal/total meniscectomy between 2008 and 2017. This study was approved by the institutional review board of Kyung Hee University Hospital (KHUH 2019-09-034).
Indications for MAT after ACL reconstruction were unicompartmental pain and instability attributed to insufficiency of the unilateral meniscus. 19 Symptoms of instability included discomfort when performing pivoting motion in daily or sports activities and episodes of giving way. Contraindications for MAT were arthritic change or chondral damage of Outerbridge grade III or more. The status of the reconstructed ACL graft was checked with magnetic resonance imaging, physical examination under anesthesia, and arthroscopy in patients undergoing MAT after ACL reconstruction. If the patient had grade 3 anterior drawer test or Lachman test or if the ACL graft was movable for >5 mm upon probing, revision ACL reconstruction was considered instead of MAT. We excluded patients who had concurrent MAT with revision ACL reconstruction (n = 8), revision MAT (n = 2), or concomitant anterolateral ligament reconstruction (n = 17). Four patients were lost to follow-up. Ultimately, this study enrolled 31 male patients: 16 underwent medial MAT and 15 underwent lateral MAT (Figure 1). The time between ACL reconstruction with meniscectomy and MAT was shorter in the lateral MAT group (P = .043) (Table 1).
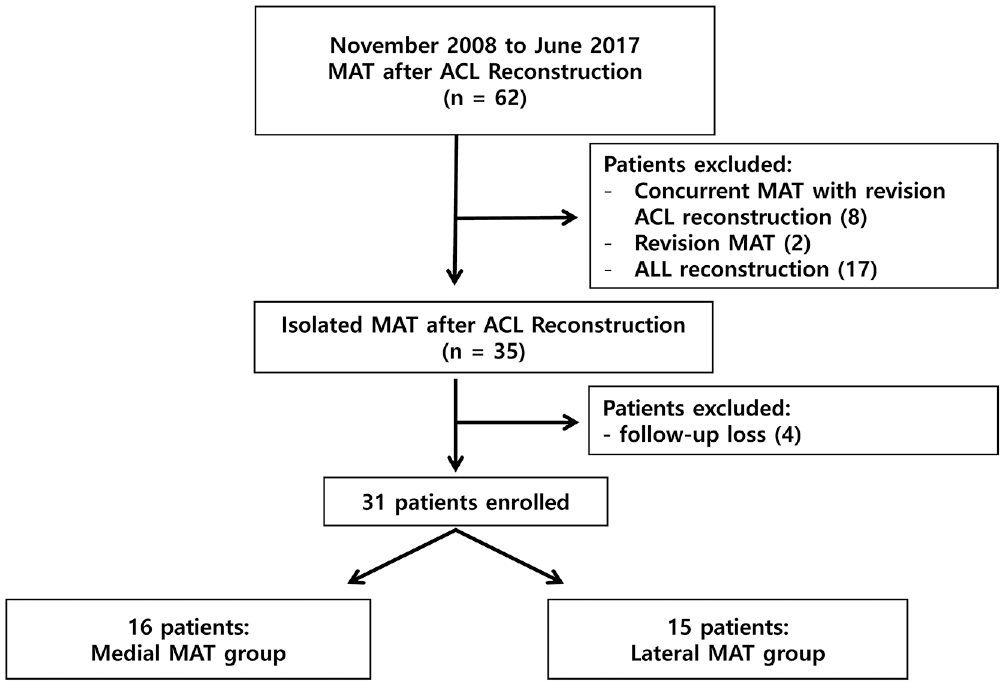
Flowchart of patient enrollment. ACL, anterior cruciate ligament; ALL, anterolateral ligament; MAT, meniscal allograft transplantation.
Characteristics of the 2 Patient Groups a
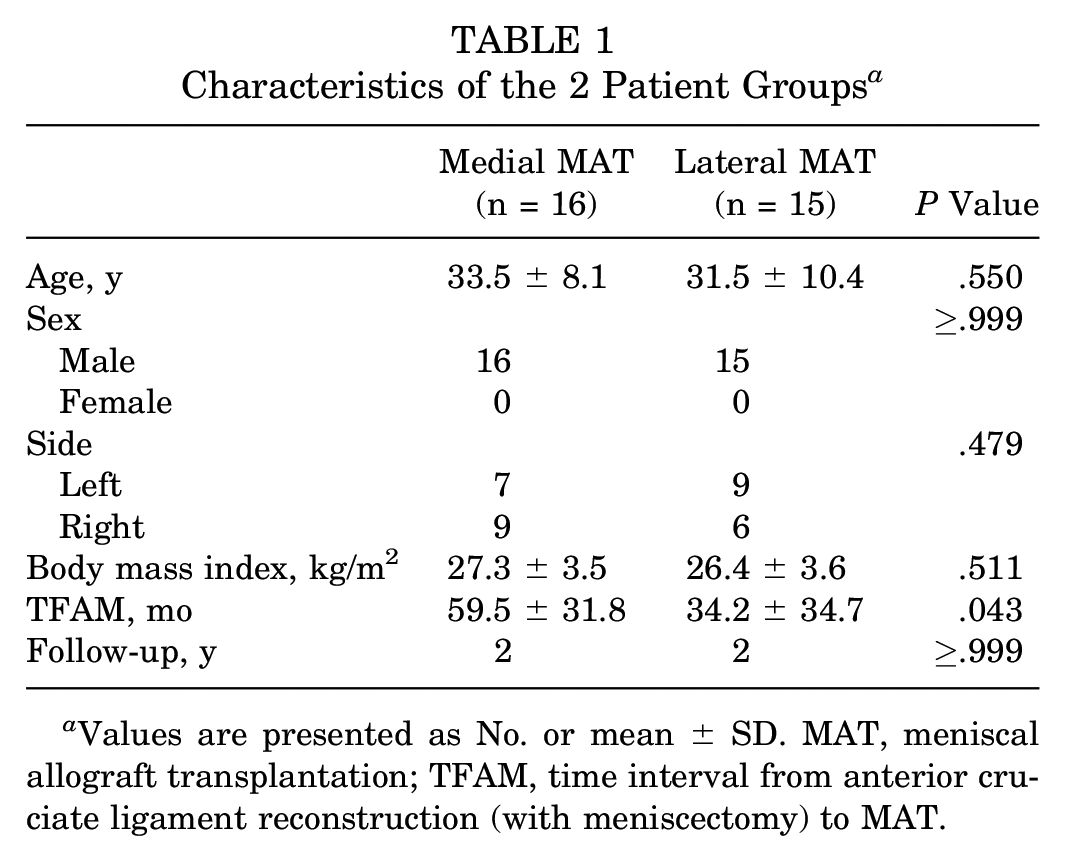
Values are presented as No. or mean ± SD. MAT, meniscal allograft transplantation; TFAM, time interval from anterior cruciate ligament reconstruction (with meniscectomy) to MAT.
Operative Technique for MAT
Fresh-frozen meniscal allografts were used in all the cases. The surgical procedures were performed by a single surgeon (K.H.Y.). As surgical methods, the keyhole technique was used in the lateral MAT group and the bone plug technique in the medial MAT group. Details on preoperative sizing, operative technique, and the rehabilitation protocol are provided in a previous study. 18
Clinical Evaluation Protocol
Patients were followed up at 6 weeks and 6, 12, and 24 months after surgery. Clinical scores included the International Knee Documentation Committee (IKDC) subjective score, 5 Lysholm score, and Tegner activity score. The instability subscale of the Lysholm score was assessed separately. 10 Physical examinations, including anterior drawer, Lachman, and pivot-shift tests, were assessed by the main surgeon (K.H.Y.). Anterior drawer and Lachman tests were categorized as such: 0 (0-2 mm), 1 (approximately 3-5 mm), 2 (approximately 6-10 mm), or 3 (approximately >10 mm). Pivot-shift tests were categorized as follows: 0 (not present), 1 (smooth glide with slight shift), 2 (jump back, moderate shift), or 3 (transient locked). To evaluate the clinical results, preoperative and 24-month follow-up scores were compared.
Radiographic Evaluation Protocol
Standing radiographs were taken preoperatively and 2 years postoperatively. The degree of osteoarthritis was checked preoperatively and 2 years postoperatively using the Kellgren-Lawrence (K-L) classification system. Joint stability was assessed according to side-to-side difference (STSD) in anterior tibial translation on Telos stress radiographs, and 134 N of anterior loading force was applied in the Lachman test position with the knee in 20° of flexion. All radiographic images were digitally acquired and assessed with a picture archiving and communication system. The minimum difference that the software could detect was 0.1 mm in length.
Statistical Analysis
SPSS software (v 12.0; IBM) was used for the statistical analyses. Chi-square linear-by-linear association analysis was used to determine the significance of trends over time in categorical data, while the Mann-Whitney U and Wilcoxon signed rank tests were used to analyze continuous data. Values are presented as mean ± SD for continuous data. P values <.05 were considered statistically significant.
Results
In the medial MAT group, the mean subjective IKDC score improved from 56.7 preoperatively to 76.2 (P < .0001) at the 2-year follow-up, while the mean Lysholm score improved from 53.6 to 79.7 (P < .0001), the mean instability score from 15 to 20 (P = .037), and the mean Tegner score from 3.6 to 5.1 (P = .007). In the lateral MAT group, the mean IKDC score increased from 68.6 to 74.2 (P = .424) at the 2-year follow-up, while the mean Lysholm score improved from 60.9 to 83.4 (P = .025), the mean instability score from 14.3 to 20.0 (P = .156), and the mean Tegner score from 4.1 to 6.0 (P = .001) (Table 2).
Clinical Scores of the 2 Groups: Preoperatively and at the 2-Year Follow-up a
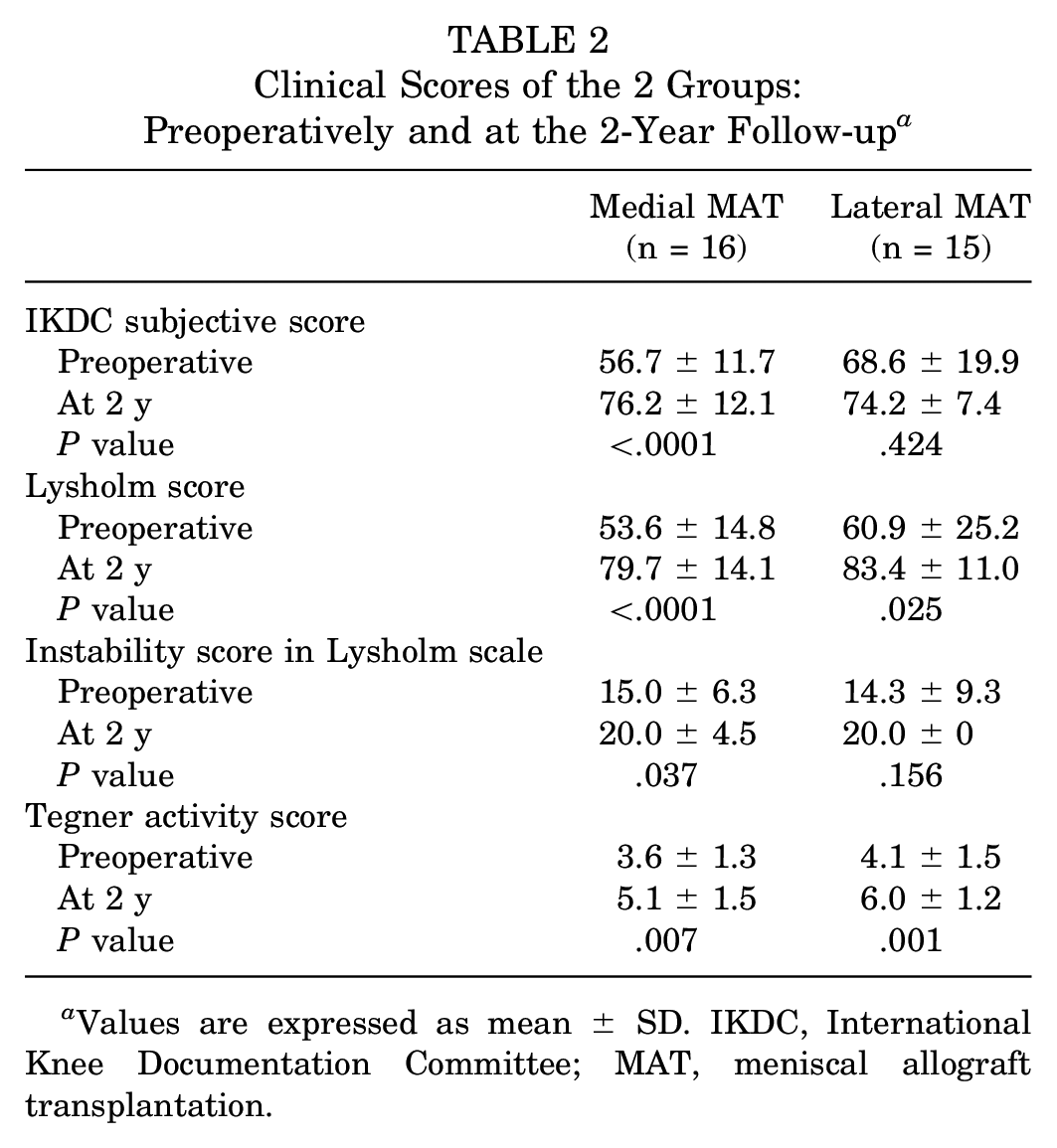
Values are expressed as mean ± SD. IKDC, International Knee Documentation Committee; MAT, meniscal allograft transplantation.
The medial MAT group showed a significant improvement from presurgery to the 2-year follow-up in the anterior drawer (P = .004), Lachman (P < .0001), and pivot-shift (P = .015) tests. The lateral MAT group also showed improvement from presurgery to the 2-year follow-up in the anterior drawer (P = .011) and Lachman (P = .002) tests, but no improvement was seen in the pivot-shift test (P = .325) (Table 3).
Stability in the 2 Groups: Preoperatively and at the 2-Year Follow-up a
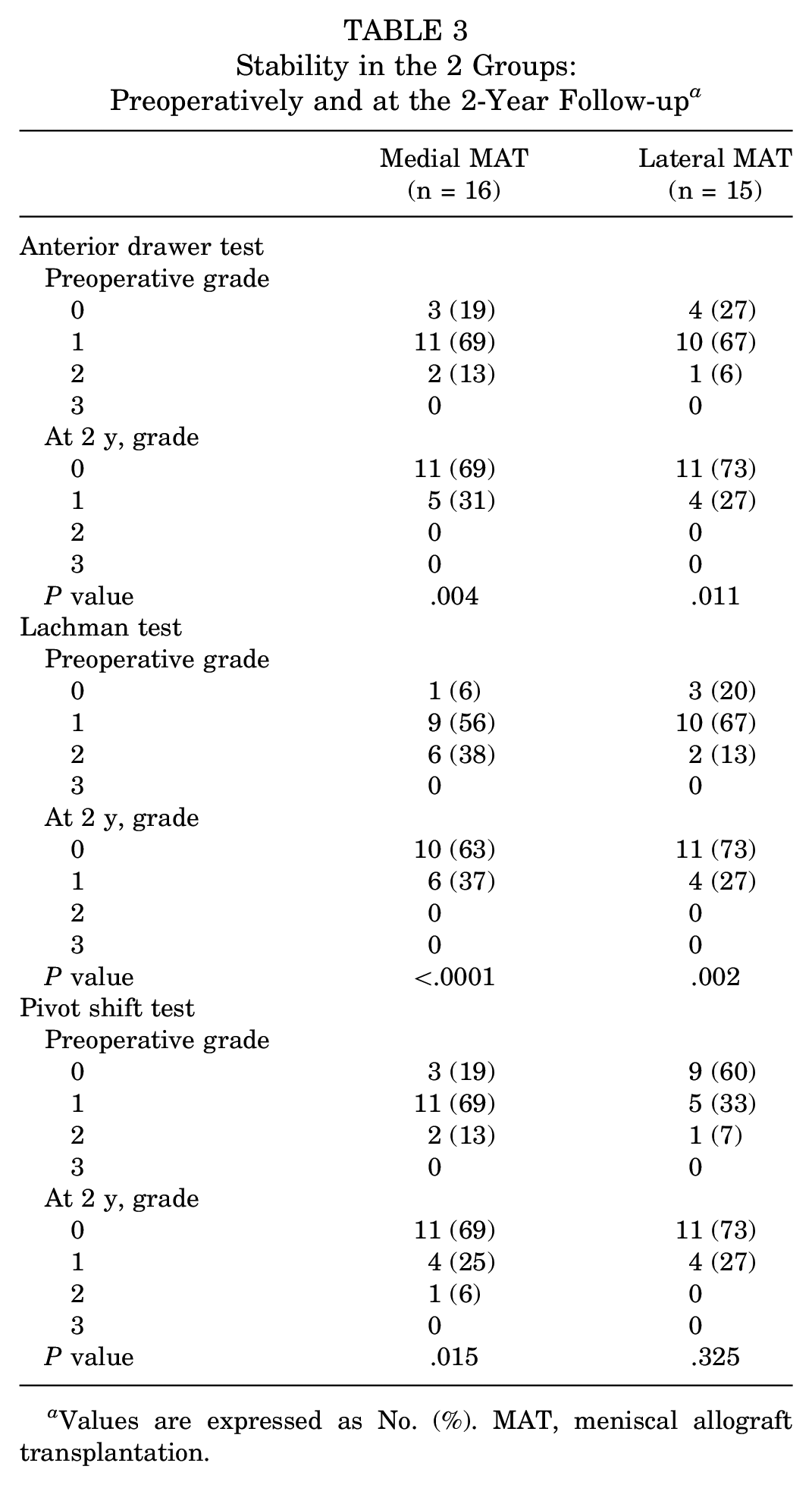
Values are expressed as No. (%). MAT, meniscal allograft transplantation.
The medial MAT group showed a significant improvement from presurgery to the 2-year follow-up in STSD on Telos radiographs (P = .001), while the lateral MAT group did not (Figure 2). Preoperatively, the medial MAT group had significantly greater STSD on Telos radiographs than the lateral MAT group (P < .0001) (Table 4).
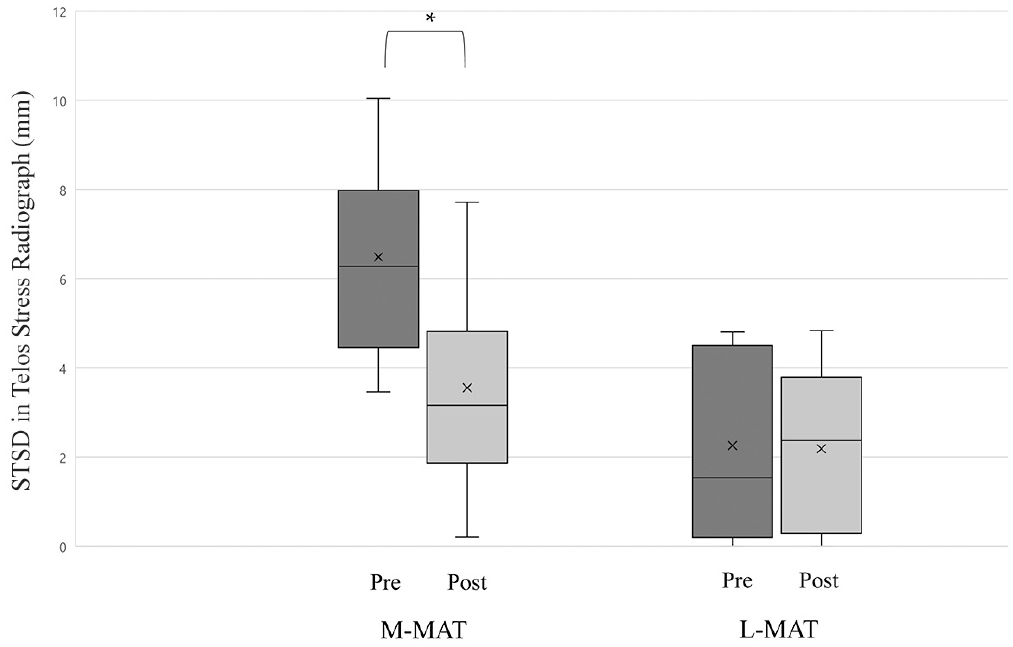
Preoperative and 2-year follow-up values of STSD in Telos stress radiographs: medial and lateral meniscal allograft transplantation groups. Bar with an asterisk represents statistical difference (P < .05). ×, mean; line, median; box, interquartile range; error bars, 95% CI. L-MAT, lateral meniscal allograft transplantation; M-MAT, medial meniscal allograft transplantation; STSD, side-to-side difference.
Radiological Results of the 2 Groups: Preoperatively and at the 2-Year Follow-up a
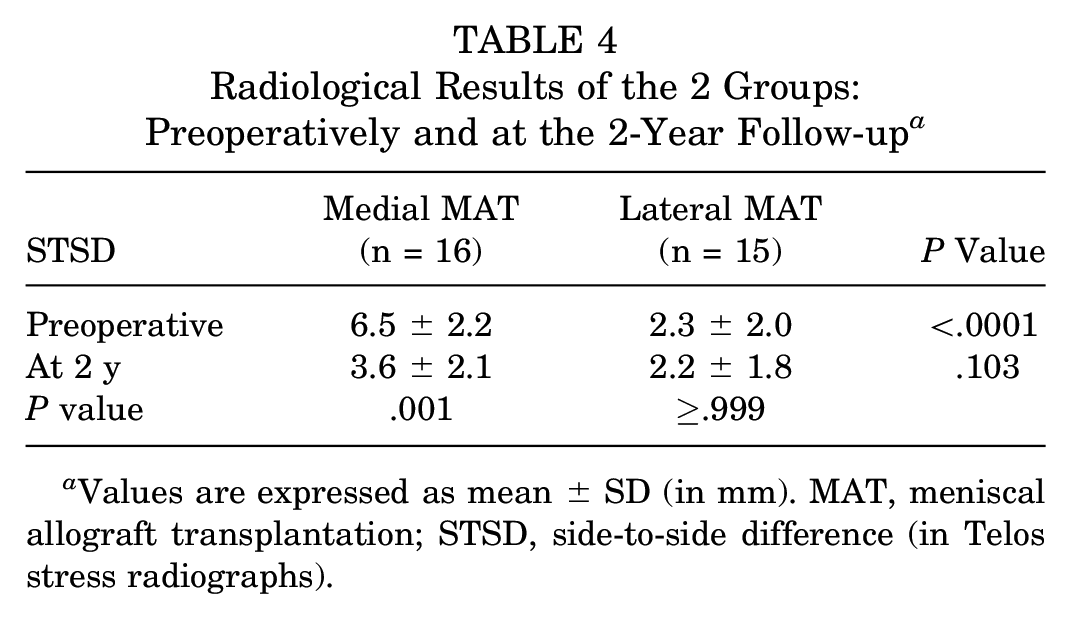
Values are expressed as mean ± SD (in mm). MAT, meniscal allograft transplantation; STSD, side-to-side difference (in Telos stress radiographs).
One patient in the medial MAT group sustained a complex tear of the meniscal transplant at 1.5 years postoperatively and underwent partial meniscectomy of the transplant graft.
Preoperative K-L grade of patients in both groups ranged from 0 to 2. The 2 groups did not show any significant difference in K-L grade. None of the patients in either group showed any progression of K-L grade at postoperative 2 years (Table 5).
Osteoarthritis in the 2 Groups: Preoperatively and at the 2-Year Follow-up a
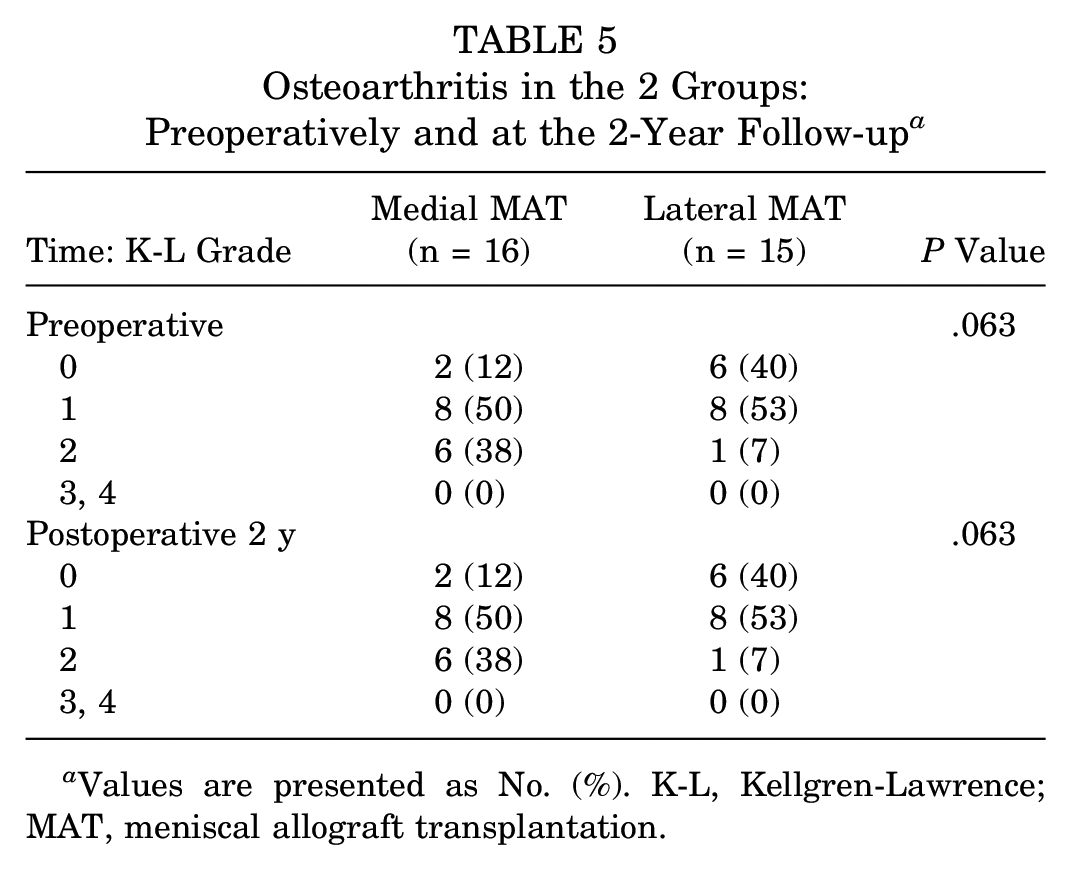
Values are presented as No. (%). K-L, Kellgren-Lawrence; MAT, meniscal allograft transplantation.
Discussion
The most important finding of this study was that medial MAT improved not only anteroposterior stability but also rotational stability in meniscus-deficient ACL-reconstructed knees. Lateral MAT showed improvements in anterior drawer and Lachman tests but not in the pivot-shift test or STSD on Telos stress radiographs in meniscus-deficient ACL-reconstructed knees.
Yoon et al 18 suggested that while the primary indication for medial and lateral MAT was unicompartmental pain, instability should be considered when performing medial MAT. The present study suggests that while medial MAT acts as an important secondary stabilizer of the knee in the setting of ACL reconstruction, lateral MAT may play a less crucial role in terms of the stability of the ACL reconstruction.
The importance of the medial meniscus for restraining anteroposterior translation of the tibia relative to the femur in the ACL-deficient knee has been well-documented.1,2,4,8 Impairment of the ACL substantially increases the forces on the medial meniscus and predisposes patients to meniscal tears. 1 ACL reconstruction dramatically reduces the strain on the menisci as compared with the cruciate-deficient knee. 4 Papageorgiou et al 14 suggested that the interplay between the ACL and meniscus is sufficiently substantial such that loss of one of these structures could predispose the other to injury.
In a biomechanics study, Spang et al 17 demonstrated that medial meniscectomy significantly increased tibial displacement at 30° and 90° of knee flexion. Moreover, they found that medial MAT restored the tibial displacement to the intact state at 30° and 90° of knee flexion. 2 In the present study, there was significant improvement in the anterior drawer test, Lachman test, and STSD on Telos stress radiographs.
Lorbach et al 9 showed that the medial meniscus significantly affected not only anterior tibial translation but also the results of a simulated pivot-shift test. In a biomechanics study, Seon et al 15 showed that subtotal medial meniscectomy in the ACL-deficient knee increased lateral tibial translation and internal rotation. In the meniscus-deficient state, ACL reconstruction did not restore lateral tibial translation or internal rotation. 15 Despite many reports that meniscus-deficient knees showed inferior stability after ACL reconstruction, no study has shown that MAT restored stability. In the present study, medial MAT resulted in significant improvement in the anterior drawer, Lachman, and pivot-shift tests, as well as STSD on Telos stress radiographs, at the 2-year follow-up in ACL-reconstructed knees. This represents evidence that instability, in addition to pain, should be considered when performing medial MAT in ACL-reconstructed knees.
Levy et al 7 reported that lateral meniscectomy in the ACL-deficient knee did not increase anterior translation. Musahl et al 11 showed that the lateral meniscus was more important than the medial meniscus for preventing anterior tibial translation during pivoting maneuvers. Shybut et al 16 demonstrated that tears of the lateral meniscus posterior root further reduce the stability of the ACL-deficient knee during rotational loading. In the present study, lateral MAT did not significantly improve the results of the pivot-shift test. However, the pivot-shift test results were fairly good preoperatively in the lateral MAT group. So, it is difficult to draw any conclusion concerning the effect of lateral MAT on pivot shift. Nonetheless, lateral MAT did improve the anterior drawer and Lachman tests, suggesting a role for lateral MAT in terms of anteroposterior stability.
Of note, the average time from ACL reconstruction (with meniscectomy) to MAT was 3 years in our lateral MAT group and 5 years in the medial MAT group. Our indications for MAT were unicompartmental pain and instability attributed to insufficiency of the unilateral meniscus. Although many factors may have contributed to the interval between ACL reconstruction and MAT, the discrepancy in the timing of MAT suggests that patients are unlikely to tolerate an ACL-reconstructed knee without a lateral meniscus.
In this study, after ACL reconstruction and total or nearly total meniscectomy of the meniscus, there was 6.5 mm of STSD in the medial MAT group versus only 2.3 mm in the lateral MAT group. Similarly, Grassi et al 3 reported residual anterior translation in patients with ACL reconstruction and partial medial meniscectomy. The present study has shown that medial MAT can restore preoperative anteroposterior instability.
This study had some limitations. First, it was a retrospective study and included a small sample, given the relatively uncommon and technically demanding procedure. Second, subjective physical examinations were used to evaluate stability, such as the anterior drawer, Lachman, and pivot-shift tests. Although the reliability of these tests has been demonstrated, 6 future studies may require data obtained via more accurate kinematic assessments. Third, this study investigated only the 2-year results of MAT in ACL-reconstructed knees. The long-term survival of MAT in ACL-reconstructed knees should be studied in the future. Fourth, many of the patients included in this study were referred to our institution after ACL reconstruction and meniscectomy were performed at another institution by several surgeons. Information on surgical technique (transtibial, accessory medial, outside-in) and graft choice was often unavailable. Fifth, all of the patients in the present study were male, and the generalizability of our data is limited.
In conclusion, medial MAT improved not only anteroposterior stability but also rotational stability in meniscus-deficient ACL-reconstructed knees. Lateral MAT yielded improvements in anterior drawer and Lachman tests but not in the pivot-shift test or STSD on Telos stress radiographs in meniscus-deficient ACL-reconstructed knees. Instability and pain are indications for MAT in meniscus-deficient ACL-reconstructed knees.
Footnotes
Submitted January 7, 2020; accepted May 7, 2020.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.