
Abstract
Background:
Posterior glenohumeral instability is an increasingly recognized cause of shoulder instability, but little is known about the incidence or effect of posterior glenoid bone loss.
Purpose:
To determine the incidence, characteristics, and failure rate of posterior glenoid deficiency in shoulders undergoing isolated arthroscopic posterior shoulder stabilization.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
All patients undergoing isolated posterior labral repair and glenoid-based capsulorrhaphy with suture anchors between 2008 and 2016 at a single institution were identified. Posterior bone deficiency was calculated per the best-fit circle method along the inferior two-thirds of the glenoid by 2 independent observers. Patients were divided into 2 groups: minimal (0%-13.5%) and moderate (>13.5%) posterior bone loss. The primary outcome was reoperation for any reason. The secondary outcomes were military separation and placement on permanent restricted duty attributed to the operative shoulder.
Results:
A total of 66 shoulders met the inclusion criteria, with 10 going on to reoperation after a median follow-up of 16 months (range, 14-144 months). Of the total shoulders, 86% (57/66) had ≤13.5% bone loss and 14% (9/66) had >13.5%. Patients with moderate posterior glenoid bone loss had significantly greater retroversion (−11.5° vs −4.3°; P = .01). Clinical failure requiring reoperation was seen in 10.5% of patients in the minimal bone deficiency group and 44.4% in the moderate group (P = .024). There was no difference between groups in rate of military separation or restricted duty. Patients with moderate posterior glenoid bone deficiency were more likely to be experiencing instability instead of pain on initial presentation (P < .001), were more likely to have a positive Jerk test result (P = .05), and had increased glenoid retroversion (P = .01).
Conclusion:
In shoulders with moderate glenoid bone deficiency (>13.5%) and increased glenoid retroversion, posterior capsulolabral repair alone may result in higher reoperation rates than in shoulders without bone deficiency.
Posterior shoulder instability is an increasingly recognized cause of shoulder instability in young athletes, representing between 2% and 18% of shoulder instability cases.1,8,22,27,31,34 More recent studies have reported posterior instability rates as high as 24% in a military population. 13 Options for treatment include arthroscopic or open capsulolabral repair and posterior bone augmentation. Of these options, arthroscopic glenoid-based posterior capsulolabral repair with suture anchors is most common and has failure rates between 6% and 12%.9,19 The factors influencing failure after arthroscopic posterior stabilization have been incompletely evaluated.
Anterior glenoid bone loss significantly affects successful arthroscopic capsuloligamentous repair and has been associated with recurrent instability rates as high as 67%. 11 More recent studies have demonstrated significantly higher rates of recurrent instability and associated lower patient-reported outcomes after arthroscopic anterior stabilization in patients with >13.5% bone loss.14,33 Biomechanical studies have demonstrated that posterior glenoid bone loss (pGBL) is associated with increased posterior humeral translation in cadaveric models; however, the clinical success of arthroscopic posterior stabilization in the setting of pGBL has not been well-described. 10 Furthermore, the effect of an increasing amount of combined glenoid retroversion with pGBL on the success of these repairs has not been well-described. Intuitively, it would appear that pGBL and glenoid retroversion would be associated with failure of arthroscopic posterior stabilization, although there remains a paucity of literature focused on the incidence or effect of pGBL and morphology in shoulders after arthroscopic posterior labral repair.4,11,36
The purpose of this study was to determine the clinical and morphologic factors that contribute to the failure of surgery in shoulders undergoing isolated arthroscopic posterior shoulder stabilization. We hypothesized that pGBL >13.5% would be associated with increased glenoid retroversion and higher rates of failure of arthroscopic stabilization.
Methods
Design and Setting
We initiated a retrospective cohort study in a young, physically active population at high risk for posterior shoulder instability to identify risk factors for instability after isolated arthroscopic posterior glenoid-based capsulolabral repair. After institutional review board approval, we identified all cases of isolated posterior labral stabilization from 2008 to 2016. Patients were included if they were >18 years old with complete preoperative magnetic resonance imaging (MRI) demonstrating an isolated posterior labral tear. Additionally, patients were included if they underwent a first-time isolated glenoid-based posterior-only capsulolabral repair with suture anchors. All procedures were performed arthroscopically: with the patient in either the lateral position or the beach-chair position. The patient position selected for arthroscopic posterior labral repair was based on the treating surgeon’s preference. The median number of anchors used was 3 (range, 3-4). The glenoid was divided into posterior and anterior hemispheres; the posterior hemisphere was defined as the 12- to 6-o’clock position on the left shoulder and the 6- to 12-o’clock position on the right shoulder. Patients with anchor placement in the posterior hemisphere were classified as having undergone a posterior labral repair, and all patients had at least 1 of their anchors placed in the posteroinferior quadrant and a minimum of 3 anchors total. Shoulders were excluded from the study if they had any anchors placed in the anterior hemisphere, if they underwent posterior glenoid bone augmentation, if this was revision surgery, or if they underwent concomitant surgical procedures (eg, rotator cuff repair, distal clavicle excision, or superior labrum anterior to posterior [SLAP] repair). Patients with voluntary dislocations, multidirectional instability, or <12-month follow-up were excluded. We initially identified 167 patients; however, 98 failed to meet inclusion criteria, and an additional 3 lacked appropriate follow-up and were excluded from the study, leaving us with 66 patients.
Preoperative documentation was evaluated to determine chronicity of symptoms, whether the patient’s primary complaint was pain or instability, and whether a patient had a specific traumatic event leading to presentation. All patients undergoing surgery reported posterior instability or pain, with physical examination findings and MRI consistent with posterior shoulder instability. The presence of a positive Kim test, Jerk test, and posterior load shift was assessed for all patients. The indication for surgery was made at the discretion of the treating surgeon.
Recurrence and Failure
The primary outcome of interest was failed arthroscopic posterior stabilization requiring revision stabilization. Medical records were reviewed with the Armed Forces Health Longitudinal Technology Application to determine shoulders that sustained a reinjury or reoperation. No patients were lost to follow-up.
Failure of arthroscopic posterior shoulder stabilization was defined as reoperation for any reason. Additionally, patients were followed for their ability to return to full activity without restriction and/or revision stabilization at a minimum 1-year follow-up. All patients in the present study were active military servicemembers, representing a unique population in which to evaluate posterior instability because their everyday activities of push-ups, pull-ups, and lifting place repetitive stress on the posterior shoulder. Servicemembers who were unable to participate and complete these minimum requirements but were able to complete their assigned job tasks were involuntarily placed on a medical profile or permanent restricted duty. Furthermore, service members who remained unable to perform physical activities and could not complete their assigned military tasks were medically retired from the military. These performance variables were compared on the basis of posterior glenoid bone deficiency. Patients who were unable to return to full unrestricted duty (ie, those with permanent profile or medical separation) were deemed clinical failures.
Glenoid Measurement and Imaging
MRI was performed with a 1.5- or 3.0-T imaging magnet (Intera; Philips Medical Systems), with a phased array surface coil (Synergy Flex-M; Philips Medical Systems). In all shoulders, the sagittal image was aligned perpendicular to the plane of the scapular spine for assessment of the glenoid.
Posterior bone deficiency was calculated for each patient by using an adaptation of the perfect circle model originally described by Suguya et al. 35 Using the T2-weighted axial slice, we identified the T2-weighted sagittal slice that most closely corresponded with the lateral subchondral bone of the glenoid (Figure 1). In cases with substantial posterior bone deficiency, the lateral subchondral bone in the anterior and central aspects of the glenoid was preferentially used. The best-fit circle was placed along the inferior two-thirds of the glenoid, aligned with the anterior and inferior edge to assess pGBL. Calculations were based on the preoperative MRI. We then used a free form drawing tool to determine the posterior bone deficiency, which was the area between the posterior aspect of the circle and the posterior aspect of the glenoid 5 (Figure 2). The area of posterior bone deficiency was divided by the total area of the circle to determine the percentage of glenoid bone loss. These measurements were completed by 2 independent observers (J.W. and K.N.). Intra- and interobserver reliabilities were calculated (intraobserver was based on 2 calculations performed 1 month apart). On the basis of previous anterior instability studies that demonstrated a clinical significance of 13.5% bone loss,14,19,33 we used 13.5% pGBL as our threshold for defining minimal versus moderate bone loss.
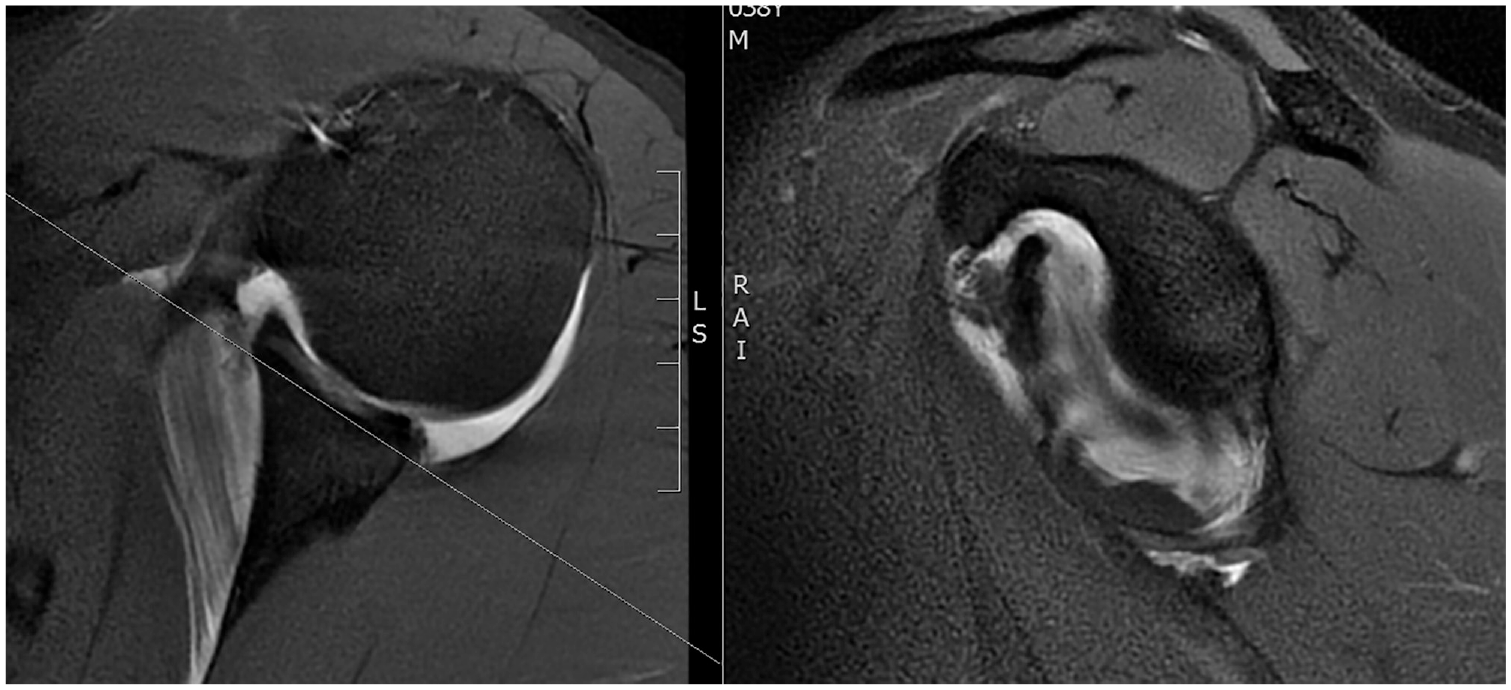
Magnetic resonance imaging demonstrating how an appropriate sagittal cut for a bone deficiency measurement was determined.
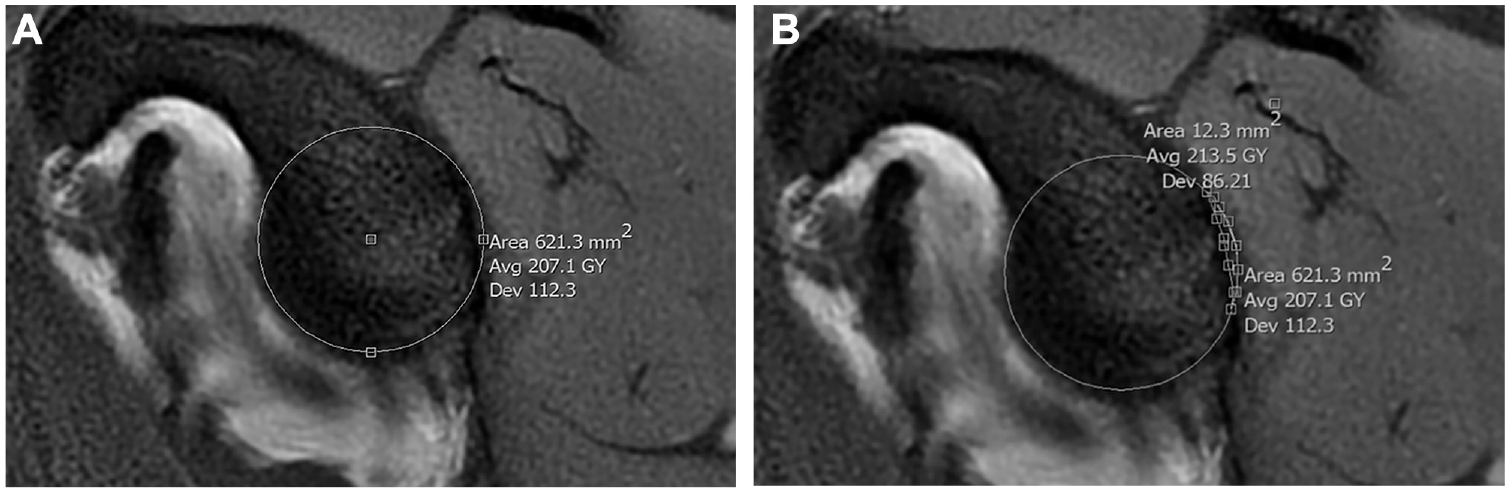
Example of how bone deficiency measurements were made: (A) the perfect circle based on the anterior inferior glenoid and (B) bone loss measured as the posterior glenoid that does not fill the circle.
Glenoid version was measured on the axial MRI slices at the midglenoid point (Figure 3). Glenoid version was measured by creating a straight line that bisected the glenoid fossa and the vertebral edge of the scapula (line A). A second line was drawn perpendicular to the first line at the site where it bisected the glenoid fossa (line B). A third line was drawn across the face of the glenoid, from the anterior glenoid rim to the posterior glenoid rim (line B′). The angle between lines B and B′ was then measured. Retroversion was expressed as a negative integer and anteversion as a positive one. 15

Our method for calculating glenoid retroversion. Version is 1.4° of anteversion in this example.
Statistical Analysis
Descriptive statistics were calculated with the mean and standard deviation or median and interquartile range for continuous variables. For categorical variables, frequencies and proportions were calculated; 95% CIs were also calculated, where appropriate. Our primary outcome was reoperation for any reason. Secondary outcomes included return to full duty, medical separation, and being placed on permanent limited duty. These outcomes were all compared on the basis of bone deficiency and retroversion. Ordinal data were compared with a chi-square test or Fisher exact test, and nominal data were compared with a t test or Mann-Whitney test, as appropriate. Calculations were performed with SPSS (version 25; IBM Corp.).
Results
A total of 66 shoulders in 66 patients met inclusion criteria for primary arthroscopic stabilization of posterior instability with glenoid-based capsulorrhaphy with suture anchors; 43 patients underwent surgery in the lateral position and 23 in the beach-chair position. The mean age was 27 years (range, 18-52 years), and the median follow-up was 26 months (range, 14-144 months). We divided patients into 2 groups defined by the amount of bone loss: minimal (≤13.5%) and moderate (>13.5%). The median time from presentation to surgery was 3.8 months (range, 1-22 months) and was not different between the groups. There were no differences between the groups on the basis of follow-up time, age, or sex (Table 1). Patient characteristics—including contact athlete status, chronicity of injury, primary complaint, number of instability events, age, and sex—were gathered for all patients and compared between groups.
Cohort Characteristics
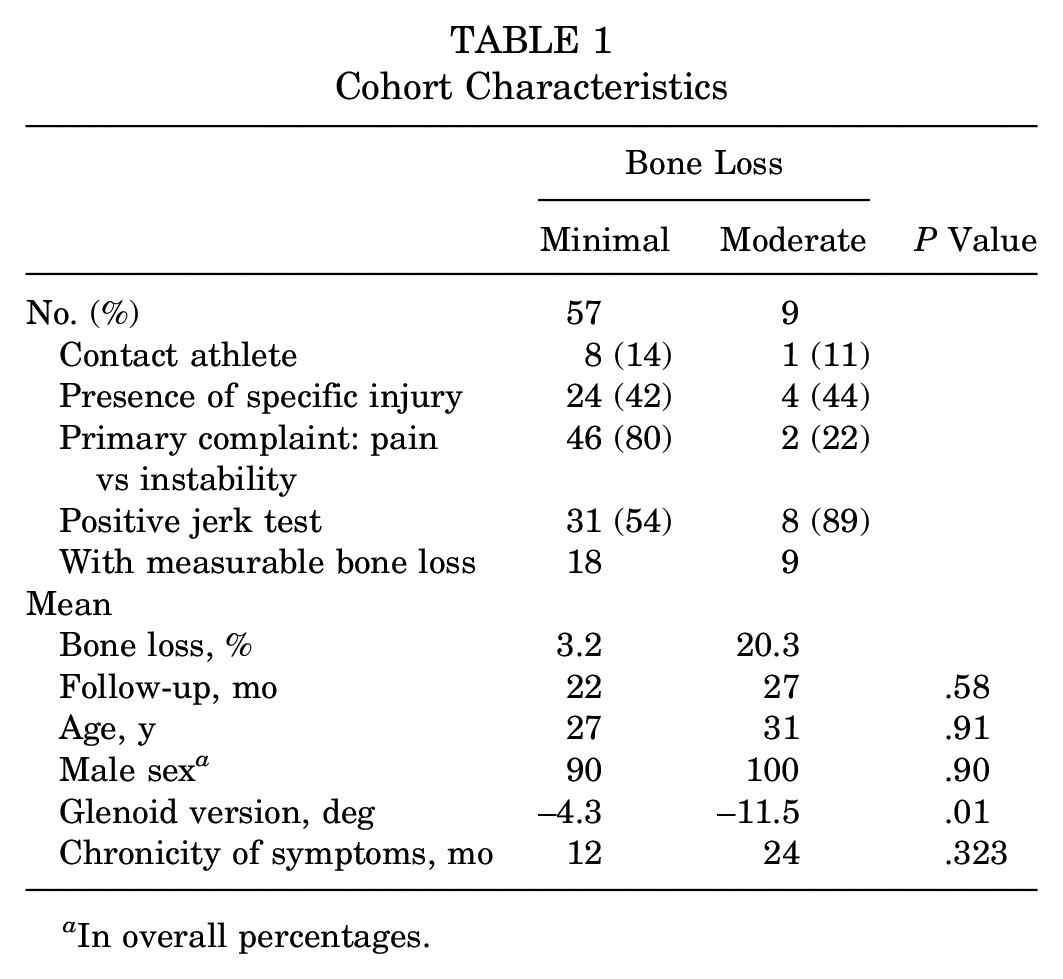
In overall percentages.
Morphology
The mean pGBL was 5.5%, and the glenoid version was −5.3° of retroversion. Overall, 86% of shoulders (57/66) had minimal measurable bone loss (37 had no bone loss), while 14% (9) demonstrated moderate bone loss. The calculated intra- and interobserver reliability for bone loss demonstrated interclass correlation coefficients of 0.96 and 0.86, respectively. The mean retroversion measurements were −4.3° (range, –17.2° to 5.2°) and −11.5° (range, –31° to 2.8°) in the minimal and moderate bone loss groups (P = .01).
Clinical Outcomes
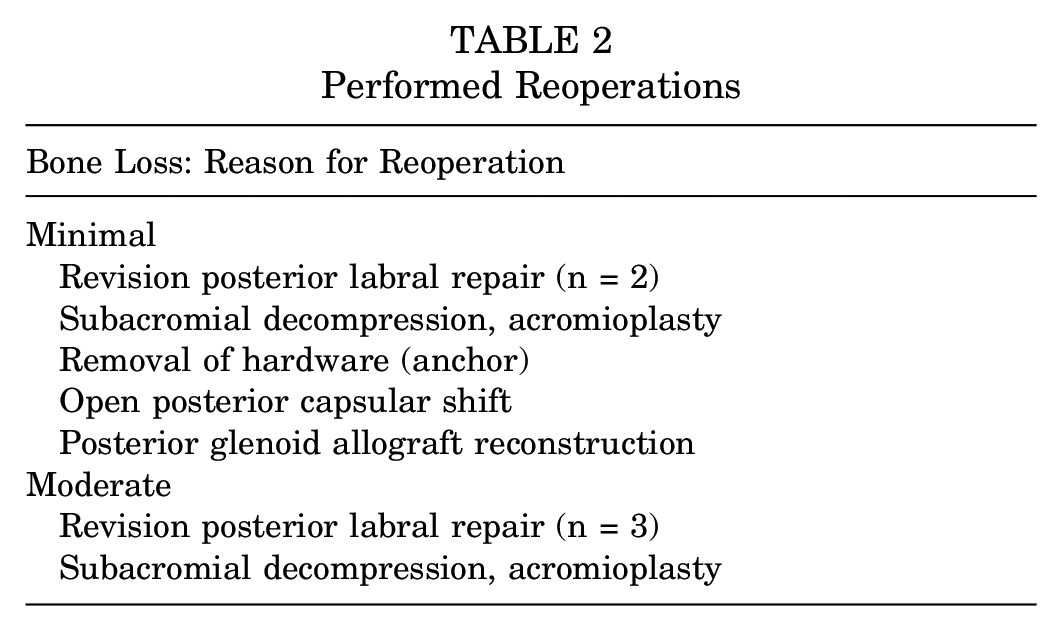
Overall, 10 (15.1%) of 66 patients required reoperation after primary stabilization, including 7 revision stabilization procedures. The other 3 procedures consisted of 2 subacromial decompressions and removal of a prominent labral anchor. When stratified by revision stabilization procedures alone, reoperations rates were 4 times higher in the moderate bone loss group (3/9; 33.3%) than the minimal bone loss group (4/57; 7.1%; P = .017). The performed reoperations for each group are listed in Table 2.
Performed Reoperations
There was no statistically significant difference in the rate of permanent restricted military duty (minimal bone loss, 26.4%; moderate bone loss, 55.6%; P = .117) and the rate of medical separation (minimal bone loss, 11.3%; moderate bone loss, 33.3%; P = .115) (Table 3). All patients who returned to full duty were able to complete their full fitness test to include push-ups. Nineteen patients were unable to return to full duty: 4 for subjective feelings of instability, 10 for pain, and 5 undocumented.
Military Activity Function
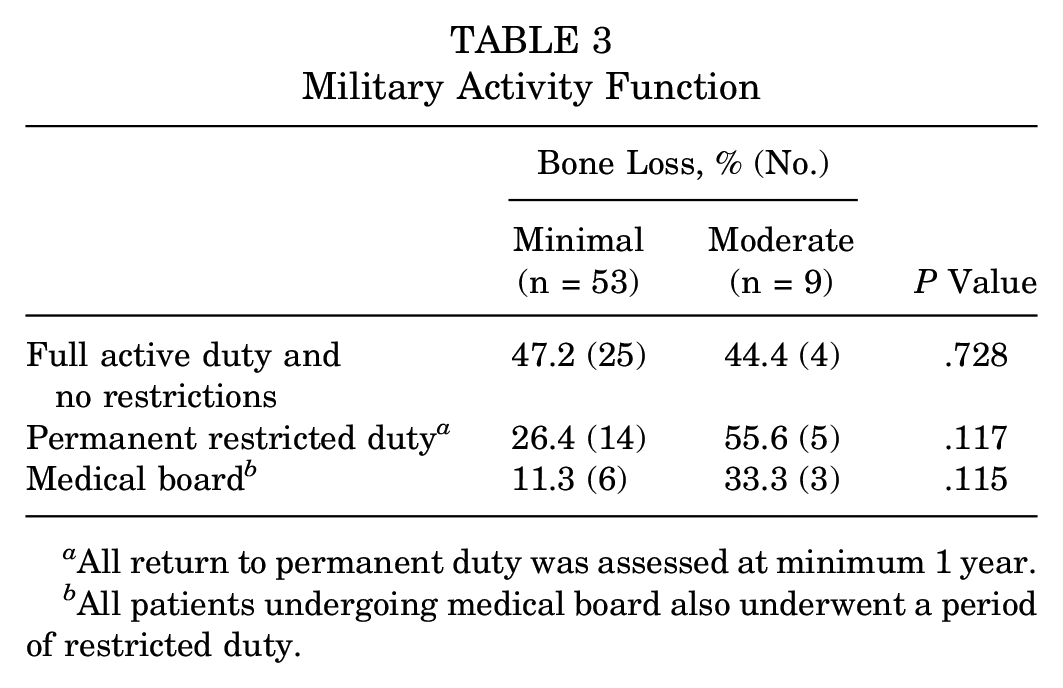
All return to permanent duty was assessed at minimum 1 year.
All patients undergoing medical board also underwent a period of restricted duty.
The primary preoperative symptom of pain was reported in 46 of 57 (80.7%) and 2 of 9 (22.2%) patients with minimal and moderate bone loss, respectively (P < .001). The remainder of patients reported a primary preoperative symptom of instability, with the majority of the moderate bone loss group (7/9; 77.8%) endorsing instability as the primary preoperative symptom. Additionally, clinical instability was more readily elicited by means of a positive Jerk test in patients with moderate bone loss (88.9 vs 54.3%; P = .05). There was no difference between the minimal and moderate bone loss groups with regard to duration of symptoms (mean 12 vs 24 months; P = .323), percentage of contact athletes (14% vs 11.1%; P = .81), or the presence of a specific initial injury rather than insidious onset (42.1% vs 44.4%; P = .89).
At the final postoperative follow-up, shoulders with minimal bone loss were significantly less likely to exhibit pain than those with moderate bone loss (18/57 [31.6%] vs 8/9 [88.9%]; P = .002) (Table 4). There was no difference in recurrent instability between minimal (6/57; 10.5%) and moderate (0%) bone loss groups (P = .585).
Clinical and Radiographic Differences a
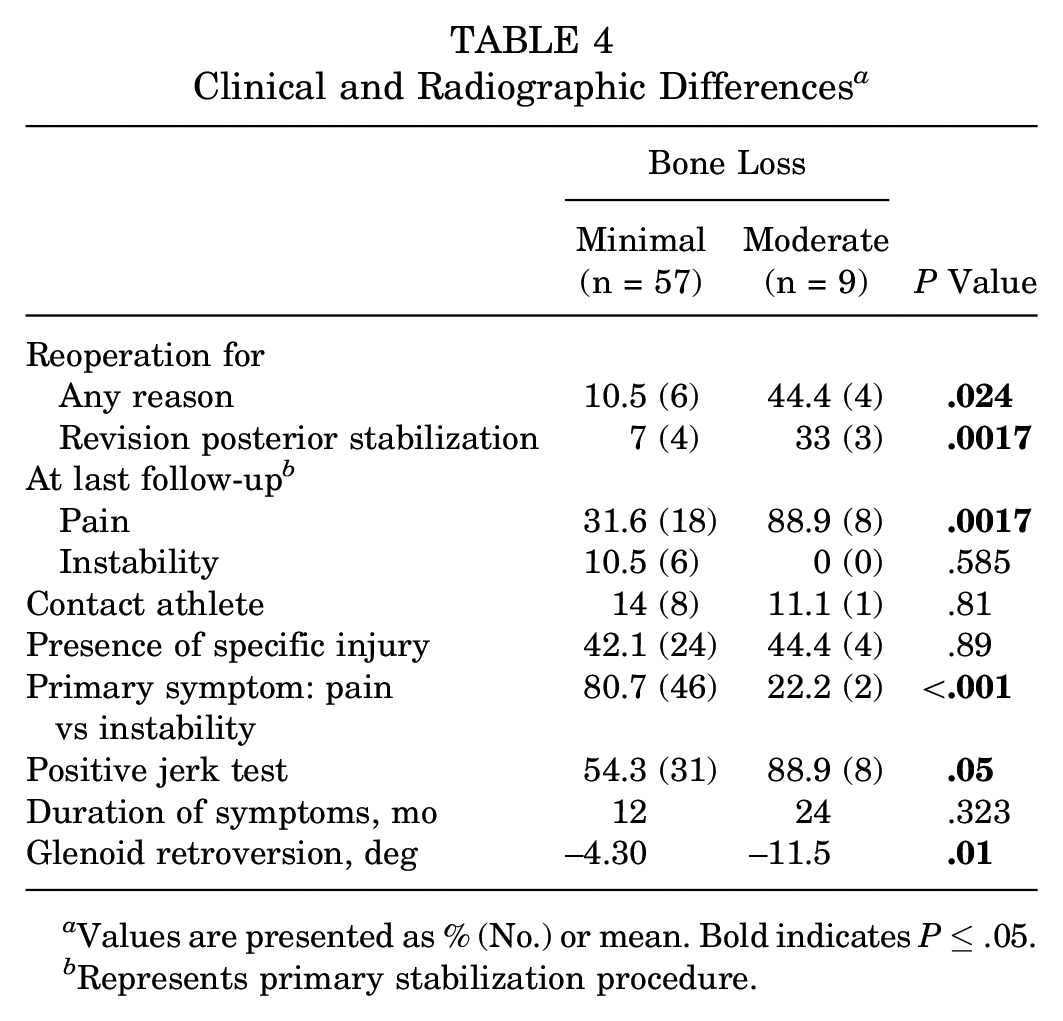
Values are presented as % (No.) or mean. Bold indicates P≤ .05.
Represents primary stabilization procedure.
Discussion
The purpose of this study was to determine the clinical and morphological factors that contribute to failure in shoulders undergoing isolated arthroscopic posterior labral repair for unidirectional posterior instability. We demonstrated that 14% of shoulders had >13.5% bone loss and these shoulders were >4 times more likely to require revision surgery for stabilization as compared with shoulders with ≤13.5% bone loss.
An important finding from this study is the association between glenoid retroversion and pGBL. This study showed an association between glenoid retroversion in combination with pGBL and failure of arthroscopic posterior stabilization. It is possible that shoulders with glenoid retroversion could be at increased risk for accelerated and/or increased pGBL in the setting of posterior instability owing to the increased frequency or incidence of instability events. This association, as well as the less robust posterior capsulolabral tissue, could contribute to higher failure rates in patients with chronic recurrent posterior shoulder instability. Additionally, this information may be important for future studies investigating the timing of surgical stabilization (immediate or chronic) and the role of bone augmentation or soft tissue capsulolabral repair.
Most previous studies did not examine the combination of glenoid retroversion with posterior bone loss in the setting of posterior capsulolabral repair. Studies comparing patients with posterior glenoid instability with either healthy controls or those with anterior instability have demonstrated increased levels of retroversion in patients with posterior instability.17,28,29 Gottschalk et al 16 examined 28 patients undergoing posterior shoulder stabilization and found that patients with glenoid retroversion >16° were more likely to have contralateral symptoms, but there was no increase in postsurgical recurrent instability. Mauro et al 23 examined the glenoid morphology of 118 athletes with unidirectional posterior instability and found that increased glenoid width, but not glenoid retroversion, was associated with improved pain and American Shoulder and Elbow Surgeons scores postoperatively. This study did not specifically address the potential for posterior bone loss.
Arthroscopic posterior capsulolabral repair has demonstrated successful clinical outcomes with a failure rate of 2% to 8% in military and civilian populations2,7,9,30,32; however, these studies did not evaluate glenoid morphology. Hines et al 19 recently reported the prevalence of pGBL in the setting of arthroscopic posterior shoulder stabilization. In their study, 78% (25/32) of shoulders had ≤13.5% bone loss, while 22% (7/32) had >13.5%. The authors indicated no significant differences between pGBL and reoperation rates. In contradistinction, we found a 33% revision stabilization rate in those with pGBL >13.5% as compared with 7% in those with ≤13.5%. It is possible that the chronicity of posterior shoulder instability (24 months) and the combined glenoid retroversion with pGBL may contribute to the higher revision rate in the present study.
Our study suggests that posterior glenoid deficiency, defined as combined glenoid retroversion and pGBL, may be a risk factor for failure of arthroscopic capsulolabral repairs in patients undergoing posterior shoulder stabilization. These results are consistent with similar studies done examining bone loss in anterior shoulder instability.6,11,35 The thinner and less robust posterior capsulolabral tissue likely places a greater emphasis on osseous morphology for stability of the glenohumeral joint.3,12 Furthermore, Owens et al 26 found that shoulders with soft tissue–only labral repairs remained unstable if the posterior bone loss was >20%. Therefore, deficiency of the posterior glenoid not only affects shoulder stability but may also predict potentially adverse outcomes after capsulolabral repair.
Our secondary goal was to examine whether clinical outcomes were affected by increased glenoid bone loss. As compared with patients with minimal bone loss, patients with moderate bone loss were more likely to report instability at their preoperative exam and pain at their final postoperative follow-up (88.9% vs 31.6%). However, there were no differences between bone loss groups when their subjective instability was compared at final follow-up (0% vs 10.5%). The ability to return to full military duty was used to define clinical success postoperatively and means that patients were able to perform a minimum set of push-ups in 2 minutes: 39 for men and 17 for women. Placement on permanent restricted duty denotes inability to return to preinjury level of function and, therefore, clinical failure. Hines et al 19 reported that, among 43 patients, 88% were able to return to duty without limitations; however, patients with moderate bone loss were significantly less likely to return to duty (86% vs 92%). Overall return to duty was lower in our cohort (69.4%). Additionally, we found a lower rate of return to duty among patients with >13.5% bone loss (44.4% vs 73.6%); however, unlike Hines et al, we could not conclude that this difference was statistically significant, likely because of an underpowered design. These findings suggest that patients with moderate posterior bone deficiency may not recover from a soft tissue stabilization procedure to the same level as their counterparts who have minimal bone deficiency and thus are more likely to require permanent restricted duty.
There are several limitations with this study. First, pGBL represents a spectrum of diseases ranging from small amounts of pGBL to developmentally acquired glenoid hypoplasia. pGBL was originally thought to be a relatively infrequent finding, but recent studies suggested that it may be present in as many as 20% of shoulders. 21 Based on the current classification system of minimal, moderate, and severe glenoid hypoplasia, our cohort did not contain any shoulders classified as moderate or severe glenoid hypoplasia. 18 However, we likely did include shoulders with minimal hypoplasia, as it is recognized that there is substantial overlap in shoulders with acquired pGBL and glenoid hypoplasia. 21 The effect that this may have on patient symptoms and surgical outcomes is still not well-understood.
Another notable limitation of this study is the methodology to determine pGBL. The morphologic pattern of pGBL is not well-defined, and there are few studies defining the optimal method to measure pGBL. The present method was selected on the basis of previous studies using this method, to make comparison possible. Additionally, we used preoperative MRI to measure glenoid bone loss rather than computed tomography (CT). While 3-dimensional CT remains the modality of choice for determination of glenoid bone loss, MRI has demonstrated consistent assessment of bone loss, with strong correlation to CT results.20,25,31 A sports medicine fellowship-trained orthopaedic surgeon performed all surgery; however, the capsulolabral repairs were not standardized, and differences in technique among surgeons may result in a performance bias. More important, our patient cohort included primarily active duty servicemembers, whose unique physical demands may not be generalized to the general public. Additionally, while we found increased pain among patients with >13.5% bone loss, validated patient-reported outcome measures would provide a better indication of clinical outcomes. There are other factors that contribute to instability and patient outcomes that were not considered in this study, including humeral bone defects. Multiple studies have shown that engagement of reverse Hill-Sachs lesions can affect shoulder stability and patient outcomes.24,26 Last, while our study did not yield statistically significant differences in return to full duty, there was a >2-fold increase in permanent restricted duty among patients with moderate bone loss. Patients with moderate bone loss were also nearly 3 times as likely to undergo medical retirement from the military. These differences indicate clinical significance between minimal and moderate bone loss, and our cohort likely lacked power to demonstrate a statistically significant difference. Despite these limitations, this study represents the largest series published examining the effect of posterior bone loss on arthroscopic posterior labral repair.
Conclusion
Posterior glenoid bone deficiency represents an underrecognized and underreported component of posterior shoulder instability. Among our patients with posterior glenohumeral instability, 13.6% had glenoid bone loss >13.5% and a mean glenoid retroversion of 11.5°. Contrary to previous studies, our study demonstrated higher rates of reoperation and poorer clinical outcomes in patients with moderate bone loss as compared with patients with minimal pGBL. Furthermore, moderate pGBL may lead to worse functional outcomes, as seen by increased rates of restricted duty placement. This study is the first to report that patients with increased pGBL have increased glenoid retroversion. Additionally, these patients were more likely to have a positive jerk test result on initial presentation and were more likely to report instability as a presenting concern. The prevalence and effect of pGBL remains underreported in the literature; therefore, future studies should focus on the effect of pGBL to better elucidate what constitutes significant bone loss.
Footnotes
Submitted October 17, 2019; accepted May 22, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: D.C. has received education and hospitality payments from Zimmer Biomet Holdings and education payments from Supreme Orthopedic Systems. J.F.D. has received education payments from Supreme Orthopedic System. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.