
Abstract
Background:
Glenoid bone loss (GBL) has been implicated as a risk factor for failure of arthroscopic anterior glenohumeral instability repair. Although certain amounts of GBL are associated with higher recurrence rates, there are limited studies on successes versus failures in these cohorts.
Purpose:
To compare the outcomes of arthroscopic Bankart repair in patients with and without GBL to determine a threshold percentage of GBL that predicts success.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
All consecutive patients who underwent arthroscopic Bankart repair for anterior shoulder instability between 2004 and 2013 were prospectively enrolled. Patients with ≤25% GBL were included. Patients with no GBL were grouped and compared with those having 5% to 25% GBL. Outcomes included Single Assessment Numerical Evaluation, Western Ontario Shoulder Index, and American Shoulder and Elbow Surgeons scores, with evidence of recurrent instability. Patients with and without GBL were statistically compared with respect to outcomes and recurrence rates.
Results:
Of 434 eligible patients, the cases of 405 (45 female, 360 male; mean age, 27.5 years [range, 18-47 years]) were followed for a mean 61 months (range, 48-96 months). There were 189 (46.6%) with no GBL and 216 (53.3%) with GBL; the mean GBL of the latter cohort was 15% (range, 5%-25%). The mean duration of instability symptoms was 7.9 months (range, 1-21 months) and was significantly longer in the GBL group (P < .05). The mean recurrence rate was 14.8%, which was significantly greater in patients presenting with GBL versus those with none (48/216 [22.2%] vs 12/189 [6.3%]; P < .01). Within the GBL group, GBL ≥15%, duration of symptoms >5 months, and younger age (<20 years) were independent risk factors for failure (P < .01). Patients with any GBL had >4-times greater odds of recurrence after arthroscopic stabilization (odds ratio, 4.21; 95% CI, 2.16-8.21). Moreover, patients presenting for arthroscopic Bankart repair with GBL ≥15% had nearly 3-times greater odds of recurrent instability.
Conclusion:
GBL ≥15% in an active patient population portends to increased odds of recurrent instability events and inferior clinical outcomes after arthroscopic Bankart repair. Furthermore, nonmodifiable risk factors, such as age (<20 years) and duration of symptoms before presentation (>5 months), significantly affect risk of recurrence and should be key factors when counseling patients on risk of failure and determining the ideal procedure for the individual patient.
Glenoid bone loss (GBL) is often present in patients with glenohumeral instability.10,15,16,21 Osseous glenoid abnormalities have been reported in 87% of shoulders with chronic anterior instability and in 22% of shoulders after first-time dislocations.10,21 Many authors have noted significant GBL as a contraindication for soft tissue repair alone, with 1 study finding GBL to be the most common risk factor causing recurrent instability after surgical repair. 22
While it is clear that GBL is a risk factor for failed arthroscopic instability repair, there is no consensus when additional bony augmentation is necessary. Burkhart and De Beer 8 described the arthroscopic finding of the “inverted pear” glenoid and stated that bony augmentation is necessary because of the glenoid’s decreased depth and arc length. Boileau et al 6 reported that GBL >25% was significantly associated with failure in 131 patients overall, with a 75% failure rate in a subset of patients undergoing Bankart repair. Authors have similarly noted arthroscopic repair to be insufficient for unstable shoulders with bone loss >25% to 30%, as well as in a prospective series of patients with attritional GBL.4,14,15 More recently, Shin et al 19 found 17.3% bone loss to be the critical value of anterior GBL in 169 cases, noting that 43% of patients above this value experienced surgical failure, in contrast to 3.7% of patients below this cutoff. Shaha et al 18 defined a “subcritical” level of bone loss, finding that >13.5% led to clinically significant poor outcome scores in an active population of 72 patients. Biomechanical investigations have found recurrent glenohumeral instability to increase with glenoid defects after Bankart repair, 12 with 19% bone loss leading to significantly reduced force required for dislocation. 24 In addition to quantifying the bone loss, determining whether a Hill-Sachs lesion was “on track” relative to GBL has been shown to be helpful in determining glenohumeral stability.17,23 As a result, GBL amount remains a well-known but fluid factor associated with recurrent anterior shoulder instability.
The purpose of this study was to compare the outcomes of arthroscopic instability repair surgery in a large and prospectively collected cohort of patients with and without GBL. Ultimately, we sought to (1) determine if there is a threshold percentage of GBL that predicts success of arthroscopic stabilization and (2) identify preoperative risk factors for postoperative failure. We hypothesized that patients who presented with symptom duration >6 months and were <20 years old with GBL >17% would have inferior outcomes when compared with those classified as having no bone loss.
Methods
Participant Enrollment
Approval for this study was obtained from the institutional review board of Naval Medical Center San Diego before patient enrollment. We prospectively enrolled all consecutive patients at an active duty military installation who underwent arthroscopic repair of recurrent anterior shoulder instability between 2004 and 2013 performed by the senior author (M.T.P.). Patients were excluded from the present study if they had an epileptic or neurologic disorder, humeral avulsion of glenohumeral ligament (HAGL), acute glenoid fracture, or GBL >25% or had undergone any previous stabilization procedures. Descriptive variables and instability-specific factors were documented, such as age at initial dislocation, total duration of instability symptoms, number of instability events, and need for manual reduction.
Diagnostic Imaging
All patients underwent preoperative imaging, including radiographs, computed tomography scans with 3-dimensional reconstructions of the glenoid using digital subtraction of the humeral head, and magnetic resonance arthrogram, and their findings were corroborated and recorded by the senior author and 1 sports medicine–trained fellow (M.T.P., A.S.B.) (Figure 1). Magnetic resonance arthrogram was used to determine the extent of labral tears as well as any other concomitant injuries. Any GBL present was measured using the best-fit circle technique to calculate the percentage of missing glenoid relative to the surface area of the glenoid on the en face axial 3-dimensional computed tomography reconstruction view,5,7,20 and patients with <5% GBL were classified into the no-GBL group (Figure 2).
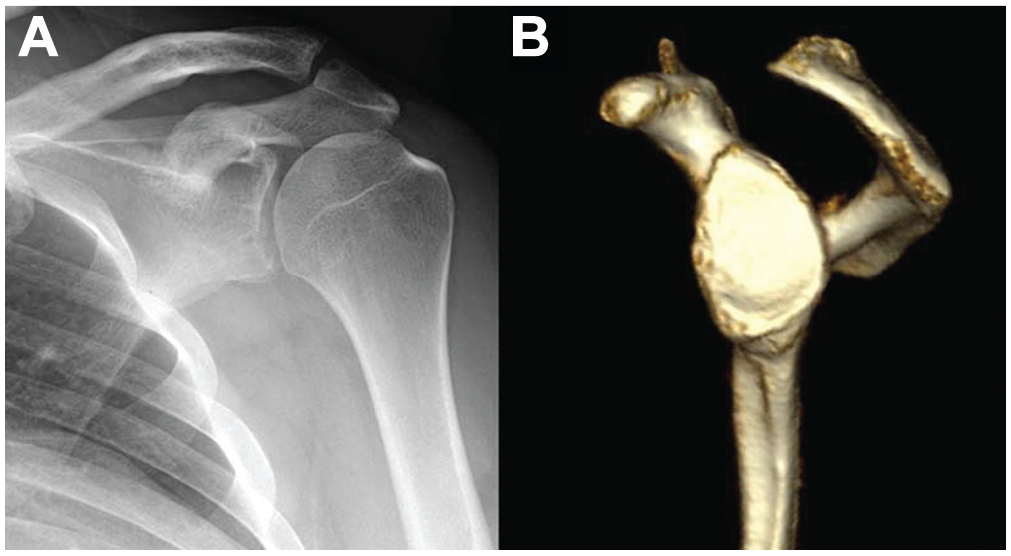
(A) Grashey (anteroposterior oblique) view radiograph of a left shoulder demonstrates loss of anteroinferior glenoid bone contour, which indicates the presence of glenoid bone loss. (B) Three-dimensional computed tomography scan of the same patient’s left shoulder confirms appreciable glenoid bone loss in the anteroinferior quadrant of the glenoid.
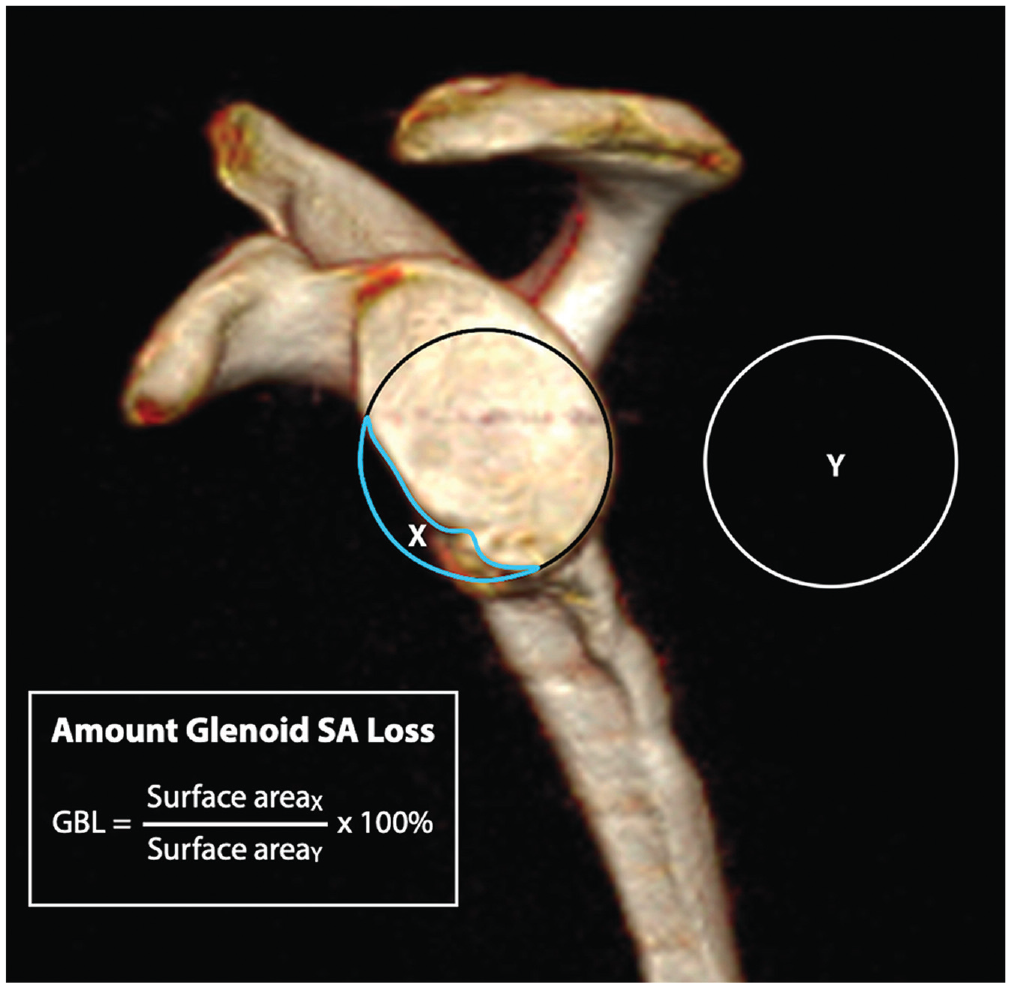
Glenoid bone loss (GBL) measurement using the best-fit circle technique to calculate the percentage of missing glenoid relative to the surface area (SA) of the glenoid.
Operative Technique
Primary arthroscopic anterior shoulder stabilization began with the patient in the lateral decubitus position. The lateral and axial traction allowed for lower suture anchor placement on the anteroinferior aspect of the glenoid, as the surgeon had increased visualization and working room within the glenohumeral joint. All patients were treated with extensive labral and glenoid bone debridement as well as an arthroscopic Bankart repair using a minimum of 3 suture anchors (mean, 4.5 anchors).
Portals were placed at the posterolateral, midglenoid, and anterosuperior rotator interval portal positions. The anterosuperior portal was used to assess the exact location and extent of the labral tear, as it provided optimal visualization of the anteroinferior aspect of the glenoid and labrum. The Bankart repair was then performed through a posterolateral (7 o’clock) portal 4 cm lateral to the posterolateral corner of the acromion to facilitate anchor placement and improve anchor trajectory. Anchor placement began at the 6-o’clock position on the glenoid and proceeded superiorly. The anchors were positioned 1 to 2 mm medial to the apex of the glenoid rim and were evenly spaced to span the entirety of the labral tear (Figure 3A). Sutures were shuttled with the use of a SutureLasso device (Arthrex Inc) and placed with an anterior-superior shift of the anterior-inferior glenohumeral ligament to provide adequate capsular tightening to further stabilize the glenohumeral joint (Figure 3B). Postoperatively, patients underwent a standardized rehabilitation protocol that has been described and used in military patients after anterior arthroscopic shoulder stabilization. 14 This protocol consisted of strict use of a sling for 6 weeks with emphasis on passive and progressive range of motion exercises under the guidance of a physical therapist. Graduated motion protocols allowed for early limitations of external rotation to 30°, forward flexion to 120°, and abduction to 90°, with aims of full passive range of motion by week 6. All range of motion restrictions were stopped after week 6, with initial strengthening exercises permitted by week 9 and return to full activities and impact sports 6 months after surgery.
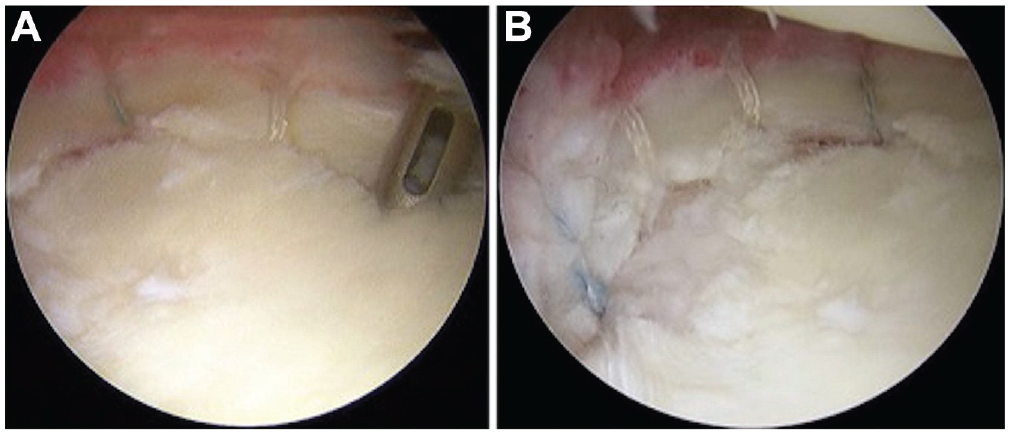
(A) Knotless anchors are positioned 1 to 2 mm medial to the glenoid rim at the anteroinferior aspect of a patient’s right glenoid. (B) Knotless anchors are evenly spaced to span the entirety of the labral tear.
Assessment of Shoulder Function and Instability
Shoulder instability and overall function were assessed pre- and postoperatively for both patient groups according to the American Shoulder and Elbow Score (ASES), Single Assessment Numerical Evaluation (SANE), and Western Ontario Shoulder Index (WOSI) and statistically compared. Failure was defined as recurrence of dislocation, subluxation, or both.
Paired t tests were performed to compare pre- and postoperative ASES, SANE, and WOSI scores overall as well as between the GBL and non-GBL patient groups. P values <.05 were assumed to be significant. Logistical regression analysis was performed to determine the threshold GBL that is predictive of recurrence. The regression analysis was performed on all patients, which was then utilized to identify a break point threshold of recurrence. This yielded a mean (± error) of the breakpoint that was analyzed statistically. Once the breakpoint was identified, an analysis of variance test was performed above and below the GBL threshold and statistically compared between and within groups. Analysis was conducted using the statistical program language R (Version 3.3.3, R Development Core Team).
Results
Patient Characteristics
From 2004 to 2013, a total of 562 consecutive patients presented to the senior author (M.T.P.) with recurrent anterior shoulder instability for arthroscopic shoulder stabilization. From this initial cohort, 157 patients were excluded on the basis of having previous shoulder stabilization surgery (46 patients), presenting with a concomitant HAGL lesion (12), having GBL >25% (68) or an acute glenoid fracture (2), or being lost to follow-up (29). In this large cohort that presented for primary shoulder arthroscopic stabilization, no concomitant procedures were performed (remplissage, superior labrum anterior and posterior repair, HAGL repair, etc). Thus, 405 patients—45 women (11.1%) and 360 men (89.9%) with a mean age of 27.5 years (range, 18-47 years)—met the inclusion criteria and were prospectively enrolled, and their cases were followed for a mean 61 months (range, 48-96 months) after arthroscopic stabilization. Overall 189 (46.6%) patients had no GBL, and 216 (53.3%) had GBL ≥5%. The mean amount of bone loss in the GBL cohort was 15.0% (range, 5%-25%). Across both patient groups, the mean age at initial dislocation was 24.3 years (range, 18-46 years), and the mean duration of instability symptoms was 7.9 months (range, 1-21 months), the latter of which was significantly greater in the GBL group (P < .05) (Table 1). Moreover, patients in the GBL cohort had more extensive labral tears, a higher frequency of glenolabral articular disruption lesions, and larger Hill-Sachs lesions (P < .01). Of the GBL cohort, 70 of 216 (32.4%) patients had GBL <15%, and 8 of those 70 patients (11.4%) reported recurrent instability. The remaining 146 patients (67.6%) within the GBL cohort had GBL >15%, and treatment for 40 of those 146 patients (27.4%) failed because of recurrence. Patients with GBL >15% had a Hill-Sachs lesion incidence of 89%, as compared with those with <15% GBL having an incidence of 61%.
Patient Characteristics a (N = 405)
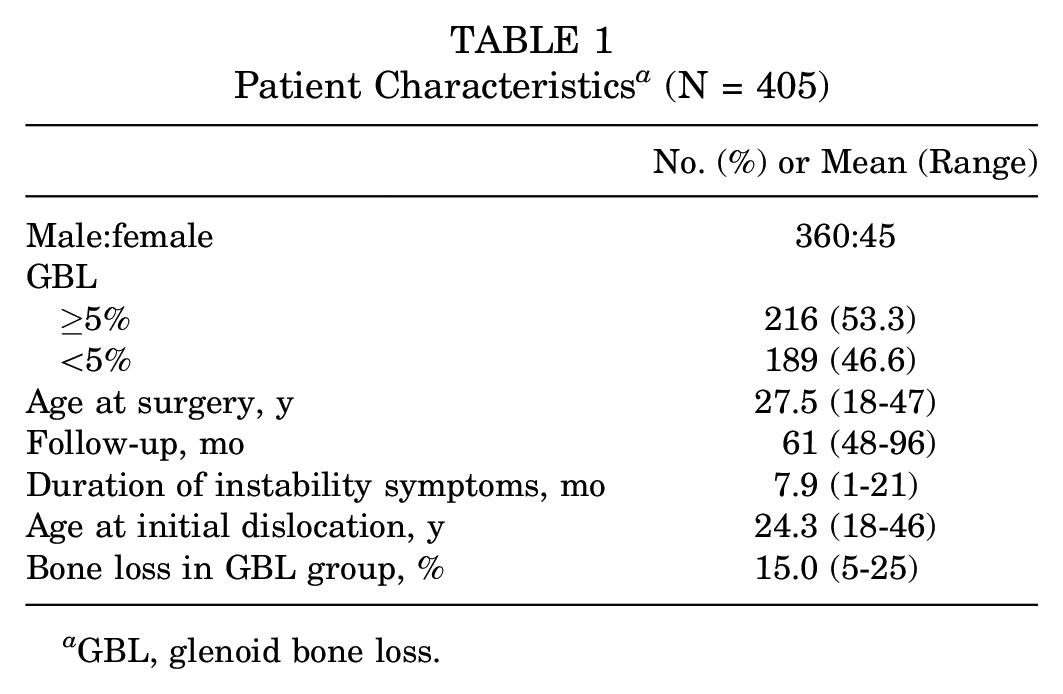
GBL, glenoid bone loss.
Risk Factors for Repair Failure
At a mean follow-up of 61 months, there was an overall failure rate of 14.8% for arthroscopic stabilization, as 40 of 405 patients (9.9%) reported experiencing recurrent frank dislocation and 20 of 405 (4.9%) reported recurrent subluxation or generalized anterior instability symptoms. Failure rates of arthroscopic stabilization were significantly greater in patients with any GBL as compared with those with no GBL (22.2% [48/216] vs 6.3% [12/189], P < .01). It was found that patients presenting with any amount of GBL incurred a 4-times greater odds of recurrent instability after arthroscopic Bankart repair (odds ratio, 4.21; 95% CI, 2.16-8.21). Moreover, statistical analysis revealed that patients with GBL ≥15% had nearly 3-times greater odds of recurrence after arthroscopic Bankart repair (odds ratio, 2.92; 95% CI, 1.29-6.65). Within the GBL patient group, GBL >15%, duration of symptoms >5 months, and younger age (<20 years) were identified as independent risk factors for failure of arthroscopic stabilization (Table 2).
Subgroup Analysis of All Failures in the GBL Group by Independent Risk Factor a (n = 48)
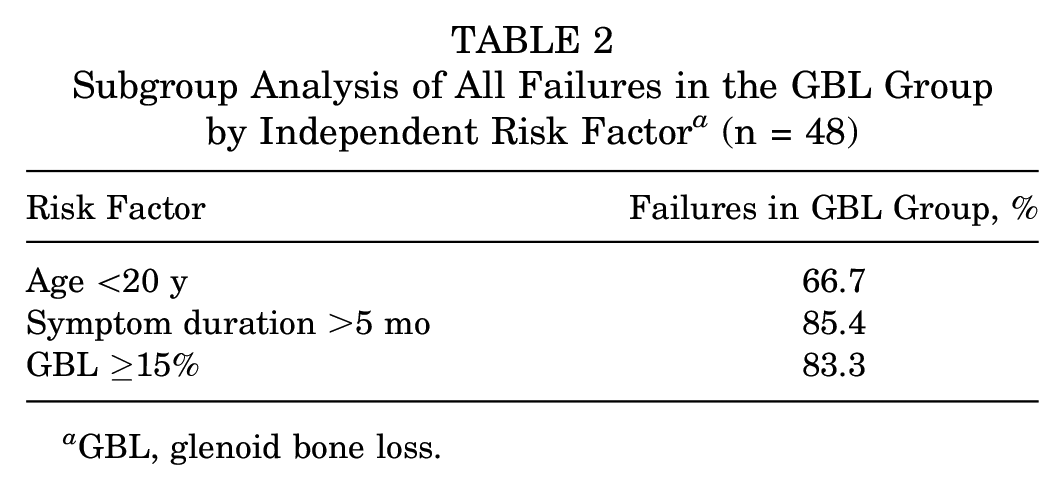
GBL, glenoid bone loss.
Postoperative Patient Outcomes
Postoperative outcome scores after anterior arthroscopic stabilization demonstrated significant improvements overall for both patient cohorts. Mean ASES scores improved from 40 to 92 (P < .001), mean SANE scores from 44 to 91 (P < .01), and mean WOSI scores from 1300 to 310 (P < .001). After identification of 15% GBL as the critical threshold for failure, postoperative outcomes were compared between patients with ≥15% bone loss and patients with <15% bone loss. Those with ≥15% GBL demonstrated significantly worse outcomes than those with <15% GBL (P < .01). The postoperative outcome scores of these groups can be seen in Table 3.
Mean Postoperative Outcomes and Failure Rates of Patients Above and Below the Critical Bone Loss Threshold (15% GBL) a
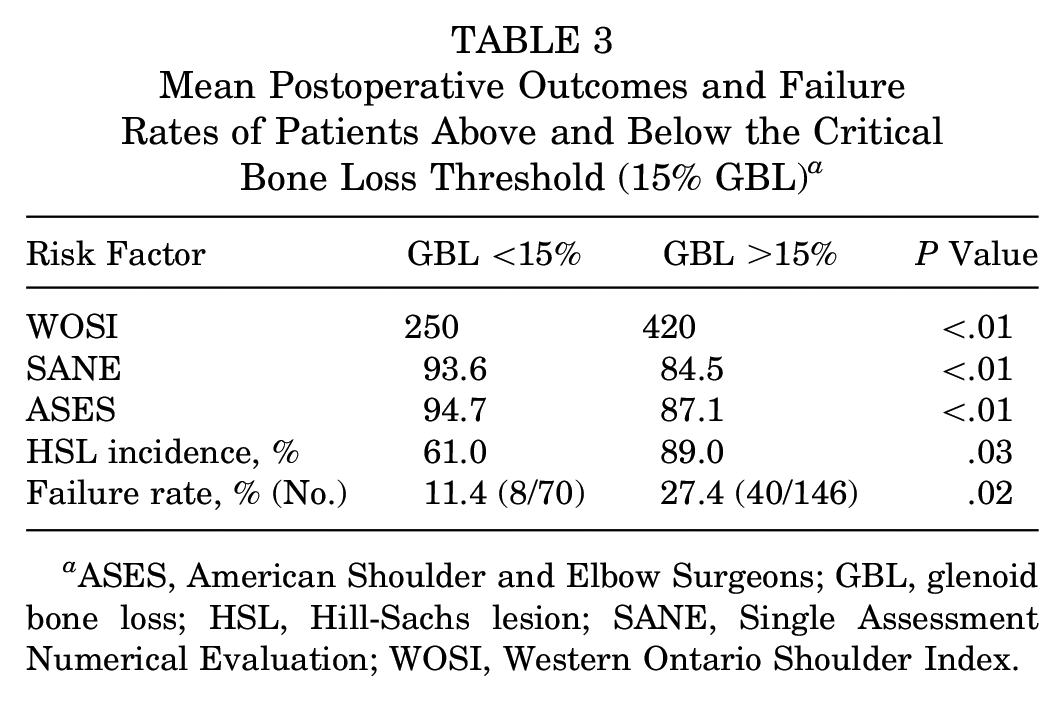
ASES, American Shoulder and Elbow Surgeons; GBL, glenoid bone loss; HSL, Hill-Sachs lesion; SANE, Single Assessment Numerical Evaluation; WOSI, Western Ontario Shoulder Index.
Discussion
The most important finding of the present study was the identification of factors that predispose one to a significantly greater risk of recurrent anterior instability and inferior clinical outcomes after arthroscopic Bankart repair. These independent risk factor included GBL ≥15.0%, duration of instability symptoms >5 months, and younger patient age (<20 years). These findings corroborate our hypothesis that duration of instability events, patient age <20 years, and critical amount of GBL are associated with recurrent anterior shoulder instability. Recognition of even small amounts of bone loss is paramount in a thorough evaluation of the shoulder to adequately treat complex anterior shoulder instability. At 5-year follow-up, this study shows significantly increased risk of recurrent anterior shoulder instability after arthroscopic Bankart repair in patients with GBL, especially in those with ≥15% bone loss. In addition, patients identified with any amount of bone loss demonstrated an increased risk of recurrence when compared with those without bone loss.
Furthermore, patients who sustained an initial injury >5 months before surgical intervention and patients aged <20 years were at higher risk for recurrence after undergoing an arthroscopic Bankart repair. These findings have immense implications in surgical decision making when choosing the correct procedure for the patient at risk for failure; they also serve as a tool for counseling patients, aiding their understanding of their pathology and the likelihood of recurrence based on nonmodifiable risk factors (age <20 years, duration of symptoms, and extent of bone loss).
Itoi et al 12 and Lo et al 13 pioneered the concept of critical bone loss and the risk of recurrence for soft tissue–only repairs. 23 Burkhart’s original description of the “inverted pear” was associated with minimum 25% anteroinferior GBL and the recommendation for a bony augmented procedure. 9 Furthermore, in a biomechanical cadaveric study, Itoi et al demonstrated that capsular restraints, when adequately repaired, can provide sufficient stabilizing forces to the shoulder to prevent recurrent instability when bone loss was <21%. A newer concept of the glenoid track was generated by Yamamoto et al, 23 stating that a significant Hill-Sachs lesion that is in line with corresponding anterior bone loss can engage and place a patient at further risk for instability and recurrence after isolated soft tissue repair. This was clinically validated and found to be more accurate than the evaluation of GBL alone. 17 Nevertheless, GBL remains an important component of patients with recurrent anterior instability, as it is a primary driver in determining soft tissue versus bone augmentation anterior shoulder stabilization procedures. 6 This study demonstrates that even a small percentage of bone loss portends worse outcomes and risk of recurrent instability. Although 15% GBL amounts to only 4.35 mm of bone loss in the average glenoid, the current study demonstrates that this level of bone loss is significant enough to directly affect recurrence and clinical outcomes. 11
The findings of this study, with a 14.8% risk of recurrence, demonstrate slightly higher risk of recurrence when compared with historical controls after arthroscopic Bankart repair, with previous failure rates averaging 10%. 2 However, the critical threshold of 15% GBL puts patients at a significantly increased risk of recurrence versus those without bone loss (22.2% vs 6.3; P < .01). Also, the Instability Shoulder Index Score has allowed for the identification of specific risk factors, as well as a quantitative preoperative analysis, to stratify risk of failure before an arthroscopic Bankart repair. 3 Similar to the Instability Shoulder Index Score, the findings of the present study demonstrate that patient age <20 years is an independent factor for risk of recurrent shoulder instability after arthroscopic stabilization. Interestingly, this study was the first to quantify the duration of preoperative symptoms that portends worse outcomes and increased risk of experiencing recurrent instability events. Patients often delay presentation; therefore, it is important to identify the exact amount of time that symptoms of instability have been present, as it directly affects risk of recurrence if patients choose to undergo an arthroscopic Bankart repair. On the basis of our findings, in the presence of bone loss ≥15% and a history of >5 months of instability or younger age, the patient should undergo a bony augmentation procedure or additional soft tissue stabilization or at least be thoroughly counseled on the increased risk of recurrence if choosing to have an arthroscopic Bankart repair.
Defining critical bone loss and how it correlates with patient-reported outcome measures remains a topic of controversy. Shaha et al 18 redefined the amount of “critical bone loss” in the active population to be 13.5%, where they found a significant decrease in WOSI scores and unacceptable outcomes with this specific threshold. In fact, even in high-level athletes with <13.5% bone loss, arthroscopic Bankart stabilization is a reliable procedure with excellent outcomes. 9 This study corroborates these findings with significant differences in WOSI, ASES, and SANE outcome scores for patients with ≥15% bone loss when compared with those with less.
In a large cohort of active duty military patients, selection bias may be present, as the majority of patients are evaluated per their occupational requirements, which are physically demanding and require the daily use of their shoulders. We attempted to reduce these limitations by collecting data from consecutive patients. Additionally, although we have a mean midterm follow-up of 5 years, it is possible that failure rates and satisfaction after these procedures can change. However, Ahmed et al 1 demonstrated that among patients whose arthroscopic Bankart procedures fail, >55% do so within 1 year; furthermore, >90% of failures that are attributed to recurrent instability occur within the first 5 years. Based on the time frame of patient enrollment, the concept of on- and off-track bone loss had not been well-defined and was not prospectively collected for these patients. Additionally, although we could have chosen a slightly higher or lower break point, we thought that 15% GBL was consistent with previous literature and offered a clinically meaningful difference from 0% to 15% and >15%; furthermore, a 1% difference between 14% and 15% is not relevant nor measurable. Despite these limitations, this study corroborates findings that even minimal bone loss (15%) portends worse outcomes. Furthermore, it gives credence to the value of determining the patient’s age at first instability event and duration of symptoms before surgery, as these may directly affect clinical outcomes and one’s risk of recurrent instability.
Conclusion
This study demonstrates that GBL ≥15% in an active patient population portends increased risk of recurrent instability events and inferior clinical outcomes after arthroscopic Bankart repair. Furthermore, nonmodifiable risk factors, such as age (<20 years) and duration of symptoms before presentation (>5 months), significantly affect risk of recurrence and should be key factors when patients are counseled on risk of failure and the ideal procedure is determined for the individual patient.
Footnotes
Submitted December 18, 2019; accepted June 3, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.T.P. has received royalties and consulting fees from Arthrex and holds patent numbers 9226743, 20150164498, 20150150594, and 20110040339. T.J.D. has received education payments from Smith & Nephew. A.S.B. has received hospitality payments from Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.