
Abstract
Background:
The relationship between the preoperative radiographic indices for femoroacetabular impingement syndrome (FAIS) and postoperative patient-reported outcome measure (PROM) scores continues to be under investigation, with inconsistent findings reported.
Purpose:
To apply a machine learning model to determine which preoperative radiographic indices, if any, among patients indicated for the arthroscopic correction of FAIS predict whether a patient will achieve the minimal clinically important difference (MCID) for 1- and 2-year PROM scores.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A total of 1735 consecutive patients undergoing primary hip arthroscopic surgery for FAIS were included from an institutional hip preservation registry. Patients underwent preoperative computed tomography of the hip, from which the following radiographic indices were calculated by a musculoskeletal radiologist: alpha angle, beta angle, sagittal center-edge angle, coronal center-edge angle, neck shaft angle, acetabular version angle, and femoral version angle. PROM scores were collected preoperatively, at 1 year postoperatively, and at 2 years postoperatively for the modified Harris Hip Score (mHHS), the Hip Outcome Score (HOS)–Activities of Daily Living (HOS-ADL) and –Sport Specific (HOS-SS), and the International Hip Outcome Tool (iHOT-33). Random forest models were created for each PROM at 1 and 2 years’ follow-up, with each PROM’s MCID used to establish clinical meaningfulness. Data inputted into the models included ethnicity, laterality, sex, age, body mass index, and radiographic indices. Comprehensive and separate models were built specifically to assess the association of the alpha angle, femoral version angle, coronal center-edge angle, McKibbin index, and hip impingement index with respect to each PROM.
Results:
As evidenced by poor area under the curves and P values >.05 for each model created, no combination of radiographic indices or isolated index (alpha angle, coronal center-edge angle, femoral version angle, McKibbin index, hip impingement index) was a significant predictor of a clinically meaningful improvement in scores on the mHHS, HOS-ADL, HOS-SS, or iHOT-33. The mean difference between 1- and 2-year PROM scores compared with preoperative values exceeded the respective MCIDs for the cohort.
Conclusion:
In patients appropriately indicated for FAIS corrective surgery, clinical improvements can be achieved, regardless of preoperative radiographic indices, such as the femoral version angle, coronal center-edge angle, and alpha angle. No specific radiographic parameter or combination of indices was found to be predictive of reaching the MCID for any of the 4 studied hip-specific PROMs at either 1 or 2 years’ follow-up.
Keywords
Femoroacetabular impingement syndrome (FAIS) represents a major cause of hip pain and limited range of motion in the young adult population.8,25 However, FAIS may be radiographically prevalent in both symptomatic and asymptomatic patients. In a cross-sectional study of 185 asymptomatic participants, FAIS was present in 53% of patients on plain radiographs. 7 However, in symptomatic patients, the prevalence approached 80%. 4 This contrast serves to illustrate that, despite our advances in the understanding of the complex causes for FAIS, radiographic and imaging tools may not fully capture the factors predictive of symptoms. As part of clinical practice, plain radiographs are used to confirm the presence of FAIS in symptomatic patients in conjunction with history and physical examination results. Specifically, alpha angles greater than 55° measured on anteroposterior, false profile, and Dunn lateral plain radiographic views confirm cam deformities of the femoral head.12,14 Despite the emergence and increasing ubiquity of hip arthroscopic surgery as a proven treatment modality to restore hip function, decrease pain, and improve patient-reported outcome measure (PROM) scores, the relationship between preoperative radiographic indices and outcomes in this complex pathophysiology remains elusive.
Nwachukwu et al 20 described the paradigmatic shift in hip preservation from radiographic and survivorship metrics to validated, patient-centered, clinically meaningful differences. In 707 patients undergoing hip arthroscopic surgery for FAIS, Lansdown et al 16 suggested that the preoperative anteroposterior alpha angle, preoperative false profile alpha angle, and postoperative false profile alpha angle are the strongest predictors of outcomes in anterolateral-based cam lesions. However, Briggs 5 described the need for more than 1 radiographic parameter and view to evaluate the joint, particularly in the context of mild dysplasia. Fabricant et al 9 evaluated 243 patients who underwent arthroscopic surgery for FAIS and found that less significant clinical improvement occurred in the setting of relative femoral retroversion (<5° femoral anteversion); moreover, no association was found between the McKibbin index and PROM scores. However, both Ferro et al 10 and Jackson et al 13 have demonstrated robust improvement on PROMs regardless of femoral version, suggesting that excessive femoral anteversion or retroversion should not be an absolute contraindication for the arthroscopic correction of FAIS. 1 Although these previous studies have established statistical significance in PROMs, this does not necessarily equate to clinical improvement. As such, reaching the minimal clinically important difference (MCID) for the respective PROM has become the accepted goal for a tangible clinical treatment target.6,11,17
Given the lack of clarity on the significance, if any, of the many available preoperative radiographic indices for FAIS, advanced modeling techniques may be ideally suited to analyze the intricacies of multiple variable parameters simultaneously to better characterize this elusive relationship. Machine learning, a subset of artificial intelligence, is the application of computational algorithms that can recognize patterns in data without explicit human instruction or supervision. In essence, machine learning is a technique that is capable of analyzing large sets of data, learning from historical data to make predictions about the future. First, real-world data sets are divided into “training sets” and “test sets.” The training sets are fed into machine learning models, which recognize subtle patterns in the data and iteratively improve. Then, the accuracy of the algorithm is assessed using a “test set,” for which outcomes are already known and can be compared with the output of the algorithm. With larger training sets and an increased number of training/testing repetitions, these algorithms can self-correct and reach higher levels of predictive accuracy. When given demographic, anthropometric, and radiographic indices for patients undergoing hip arthroscopic surgery for FAIS, the model may be able to determine whether a predictable relationship exists and, if so, which variables carry the most importance. Therefore, the purpose of the present study was to apply a machine learning model to determine which preoperative radiographic indices, if any, among patients indicated for the arthroscopic correction of FAIS predict whether a patient will achieve the MCID for 1- and 2-year PROM scores.
Methods
Patient Selection
Institutional review board approval for this study was obtained as part of an ongoing hip preservation registry analysis. A prospectively collected registry of demographic, biometric, and outcome data for all patients undergoing hip arthroscopic surgery for FAIS by 4 surgeons (D.H.N., A.S.R., B.T.K., B.U.N.) at a large tertiary care center between January 1, 2016, and December 31, 2019, was retrospectively reviewed. A total of 1735 consecutive patients indicated for hip arthroscopic surgery to correct FAIS were included for analysis. Overall, 106 patients included in the analysis underwent bilateral hip arthroscopic surgery. The radiographic signs of FAIS were corroborated with a history of symptoms for at least 3 months and physical findings, including diminished hip range of motion and a positive impingement test result. All patients underwent hip arthroscopic surgery only after previous nonoperative measures for a minimum of 6 weeks had failed. Nonoperative treatment methods included physical therapy, oral anti-inflammatory medication, and activity modification. Inclusion criteria were history, physical examination, and radiographic findings consistent with FAIS with a minimum of 2-year follow-up, no previous hip surgery, and no intraoperative psoas release. Exclusion criteria included acetabular dysplasia, moderate osteoarthritis (Tönnis grade >2), ipsilateral hip or knee surgery, revision surgical procedures, and labral reconstruction. Each patient underwent preoperative low-dose computed tomography (CT) of the operative hip alone, from which the following radiographic indices were calculated by institutional attending radiologists trained in musculoskeletal imaging: alpha angle; beta angle; sagittal center-edge angle; coronal center-edge angle; neck shaft angle; acetabular version angle at 1, 2, and 3 o’clock; and femoral version angle. The McKibbin index was calculated as the sum of the femoral version angle and acetabular version angle at 3 o’clock. 18 The hip impingement index was calculated by subtracting the alpha angle from the femoral version angle. All angles were analyzed as continuous variables.
Patients enrolled in the registry completed PROMs, with scores prospectively collected preoperatively and at 1- and 2-year follow-up. PROMs included the modified Harris Hip Score (mHHS), the Hip Outcome Score (HOS)–Activities of Daily Living (HOS-ADL) and –Sport Specific (HOS-SS), and the International Hip Outcome Tool (iHOT-33).
The mean age of the cohort was 31.1 ± 10.1 years. The mean body mass index of the cohort was 24.3 ± 4.0 kg/m2. The cohort was 49.8% female (864 female and 871 male) (Table 1).
Patient Characteristics a
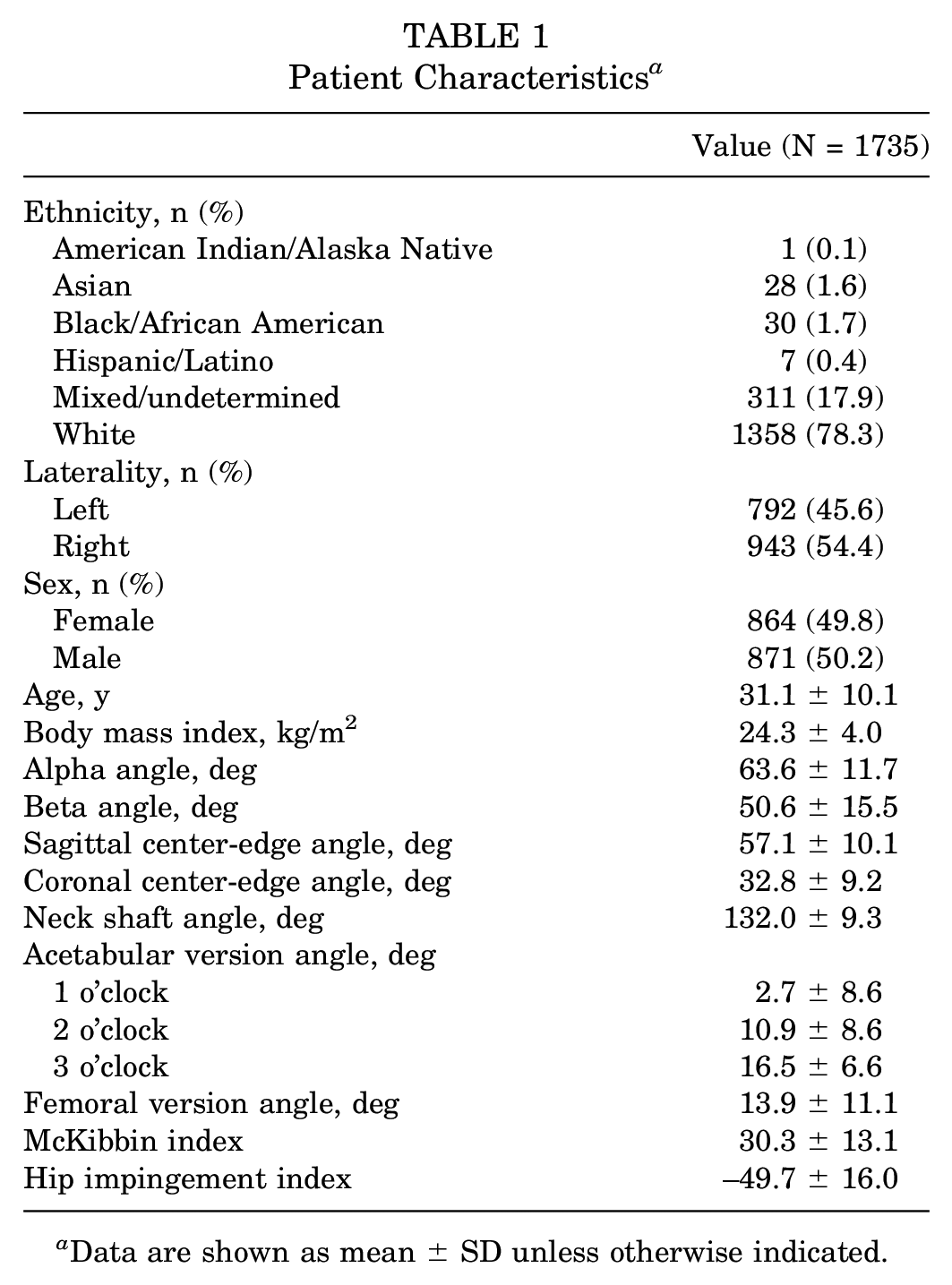
Data are shown as mean ± SD unless otherwise indicated.
Surgical Technique
Hip arthroscopic surgery was performed with the patient in the supine position. Interportal capsulotomy was performed to fully visualize and address the intra- and extra-articular sources of impingement, which were repaired before the end of the procedure. Labral refixation was performed if the tissue quality and tear pattern were amenable to repair and the labrum was not ossified (n = 1371; 79.0%). For stable tear patterns, labral debridement was performed (n = 364; 21.0%). For patients with irreparable labral tears, labral reconstruction was performed, and the patient was not included in the analysis. Femoral head-neck osteoplasty was performed in the peripheral compartment after the removal of traction and gentle hip flexion of 30° to 40° (n = 1353; 78.0%). The frequency of synovectomy performed was not recorded. Intraoperative fluoroscopy confirmed restoration of the offset (>9 mm) on the extended-neck lateral view, femoral head sphericity (alpha angle <50°), and proximal-distal correction from the physeal scar to the intertrochanteric line as assessed on 6 views (anteroposterior–internal rotation, anteroposterior-neutral, anteroposterior–external rotation, Dunn view–90° of hip flexion, Dunn view–45° of hip flexion, and frog leg lateral). 24 An intraoperative dynamic assessment of clearance with hip flexion and internal rotation was performed to confirm the improvement in range of motion.
Statistical Analysis
R statistical software version 3.5.2 (The R Foundation) was used for all data analyses. A power analysis was performed for each outcome measure of interest using the R package “pwr” version 1.2-2. The power analysis was performed using a 2-sided Student t test, power of 80%, significance of .05, and medium Cohen d effect size of 0.5. The minimum number of participants required per group was 64 patients with acceptable and nonacceptable clinical outcomes. Random forest models were created for each PROM using both the 1- and 2-year time points, with each PROM’s MCID used to establish clinical meaningfulness. Data inputted into the model included ethnicity, laterality, sex, age, body mass index, and the following angular measurements determined by a single musculoskeletal radiologist: alpha angle; beta angle; sagittal center-edge angle; coronal center-edge angle; neck shaft angle; acetabular version angle at 1, 2, and 3 o’clock; and femoral version angle. The area under the curve (AUC) of the receiver operating characteristic curve was calculated for each random forest model. Values of <0.7 were poor, 0.7-0.79 were fair, 0.8-0.89 were good, and >0.9 were excellent. 27 Both comprehensive and separate models were built using the following clinically determined independent variables decided by the senior author (B.U.N.): alpha angle, femoral version angle, coronal center-edge angle, McKibbin index, and hip impingement index (Figure 1). An alpha value of .05 was used to determine significance.
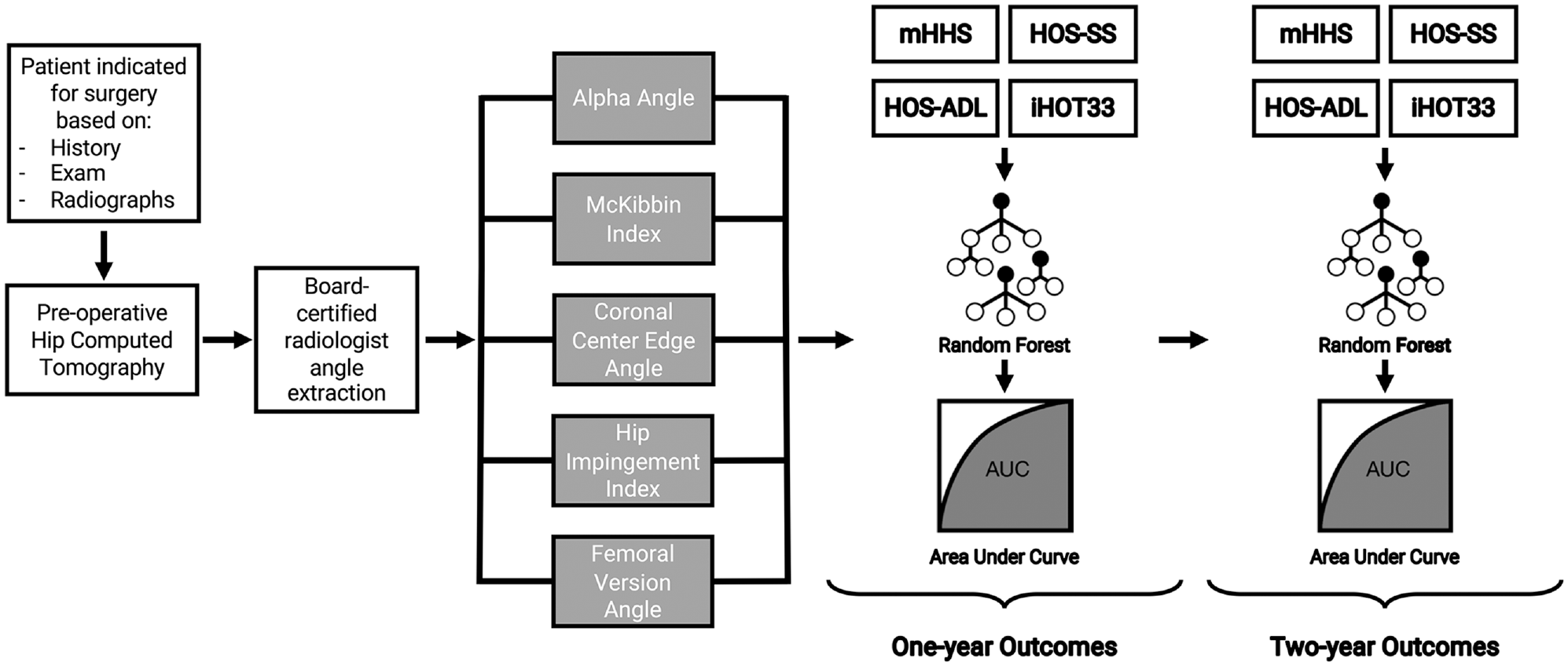
Schematic of the constructed machine learning models used to assess the relationship between critical radiographic indices and patient-reported outcome measure scores at 1 and 2 years. AUC, area under the curve; HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SS, Hip Outcome Score–Sport Specific; iHOT33, International Hip Outcome Tool; mHHS, modified Harris Hip Score.
Results
Outcome Data
Clinically meaningful outcomes were calculated using the MCID at both the 1- and the 2-year time points. The following MCID values for each PROM were used, as defined by Nwachukwu et al 22 using a distribution-based method: 9.1 for the mHHS, 9.8 for the HOS-ADL, 14.4 for the HOS-SS, and 14.6 for the iHOT-33. Figure 2 depicts the number of patients evaluated at 1 year and those who remained in the study to be evaluated at 2 years.
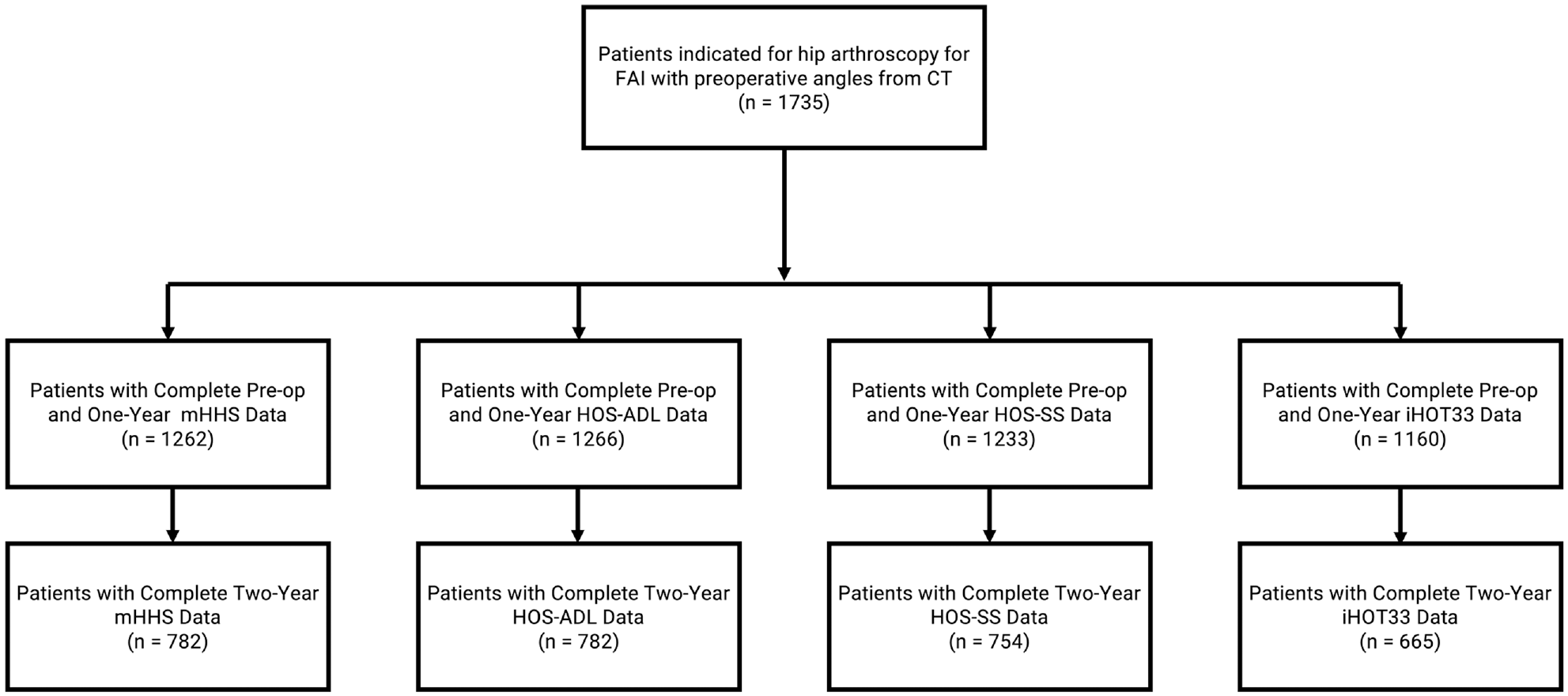
Summary of available patient data analyzed by the models. CT, computed tomography; FAI, femoroacetabular impingement; HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SS, Hip Outcome Score–Sport Specific; iHOT33, International Hip Outcome Tool; mHHS, modified Harris Hip Score; Pre-op, preoperative.
Modified Harris Hip Score
A total of 1679 (96.8%) patients completed the preoperative mHHS. Overall, 1262 (72.7%) patients completed the mHHS at 1 year after surgery, and 782 (45.1%) completed the mHHS at 2 years after surgery. Of these patients, 72.0% surpassed the MCID at 1-year follow-up, and 75.2% surpassed the MCID at 2-year follow-up.
For patients with 1-year mHHS scores, the mean preoperative mHHS score was 62.5 ± 13.1, and the mean 1-year mHHS score was 81.7 ± 16.1. The mean difference between 1-year and preoperative scores was 19.2 ± 17.5. For patients with 2-year mHHS scores, the mean preoperative mHHS score was 62.5 ± 12.5, and the mean 2-year mHHS score was 83.9 ± 15.6. The mean difference between 2-year and preoperative scores was 21.5 ± 17.7. The AUCs for the comprehensive multivariate model incorporating all radiographic angles for 1- and 2-year mHHS scores were 0.51 and 0.49, respectively, and reflected poor correlation between preoperative radiographic indices and mHHS scores. The alpha angle, coronal center-edge angle, femoral version angle, McKibbin index, and hip impingement index were not significant predictors of the mHHS score for each univariate model, as evidenced by the poor AUCs seen in Table 2.
Relationship Between Radiographic Indices and the mHHS Score at 1 and 2 Years’ Follow-up a
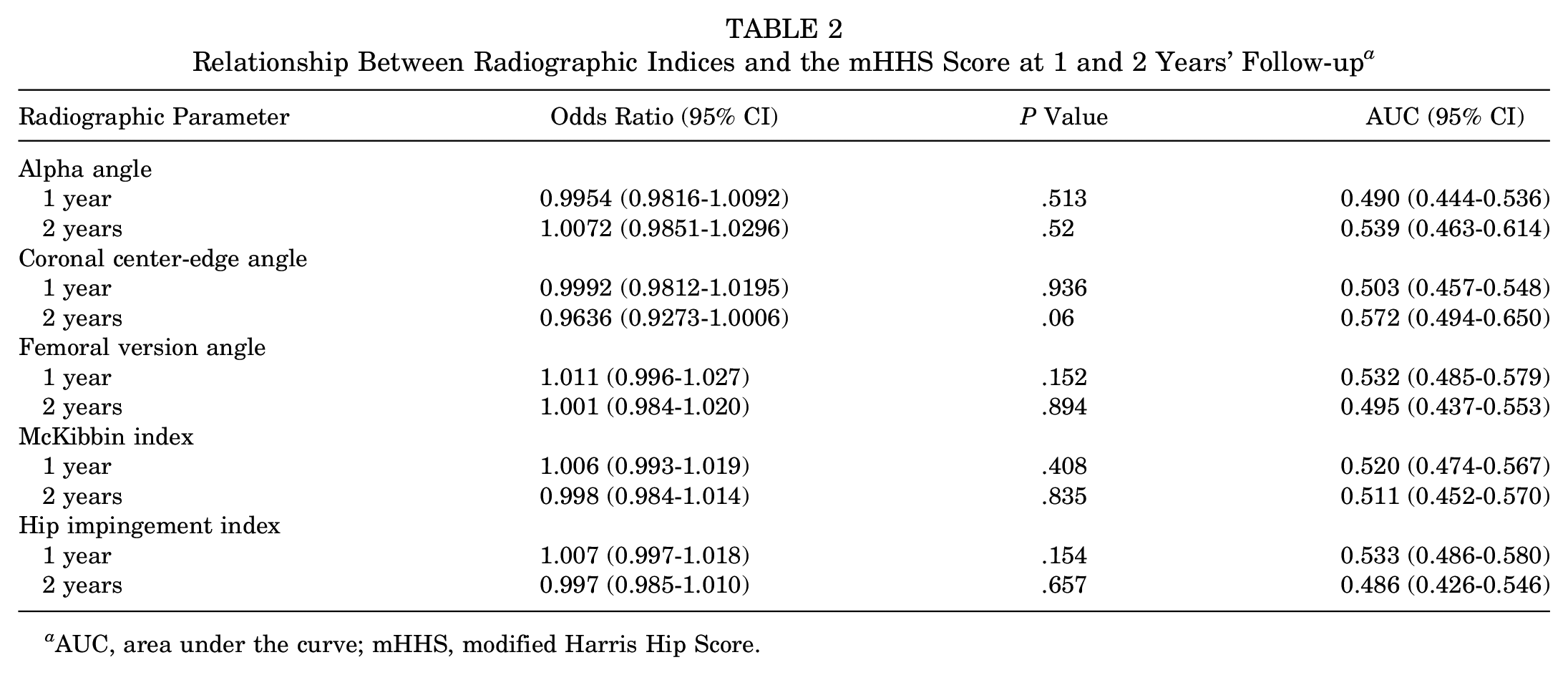
AUC, area under the curve; mHHS, modified Harris Hip Score.
Hip Outcome Score–Activities of Daily Living
A total of 1713 (98.7%) completed the preoperative HOS-ADL. Overall, 1266 (73.0%) patients completed the HOS-ADL at 1 year, and 782 (45.1%) completed it at 2 years. Of these, patients surpassed the MCID at 1- and 2-year follow-up at rates of 64.5% and 65.7%, respectively.
For patients with 1-year HOS-ADL scores, the mean preoperative HOS-ADL score was 72.2 ± 16.7, and the mean 1-year HOS-ADL score was 89.2 ± 14.1. The mean difference between 1-year and preoperative scores was 16.9 ± 17.3. For patients with 2-year HOS-ADL scores, the mean preoperative HOS-ADL score was 73.1 ± 16.3, and the mean 2-year HOS-ADL score was 90.2 ± 14.1. The mean difference between 2-year and preoperative scores was 17.1 ± 17.8. The AUCs for the comprehensive multivariate model incorporating all radiographic angles for 1- and 2-year HOS-ADL scores were 0.53 and 0.52, respectively, and reflected poor correlation between preoperative radiographic indices and HOS-ADL scores. The alpha angle, coronal center-edge angle, femoral version angle, McKibbin index, and hip impingement index were not significant predictors of the HOS-ADL score (Table 3).
Relationship Between Radiographic Indices and the HOS-ADL Score at 1 and 2 Years’ Follow-up a
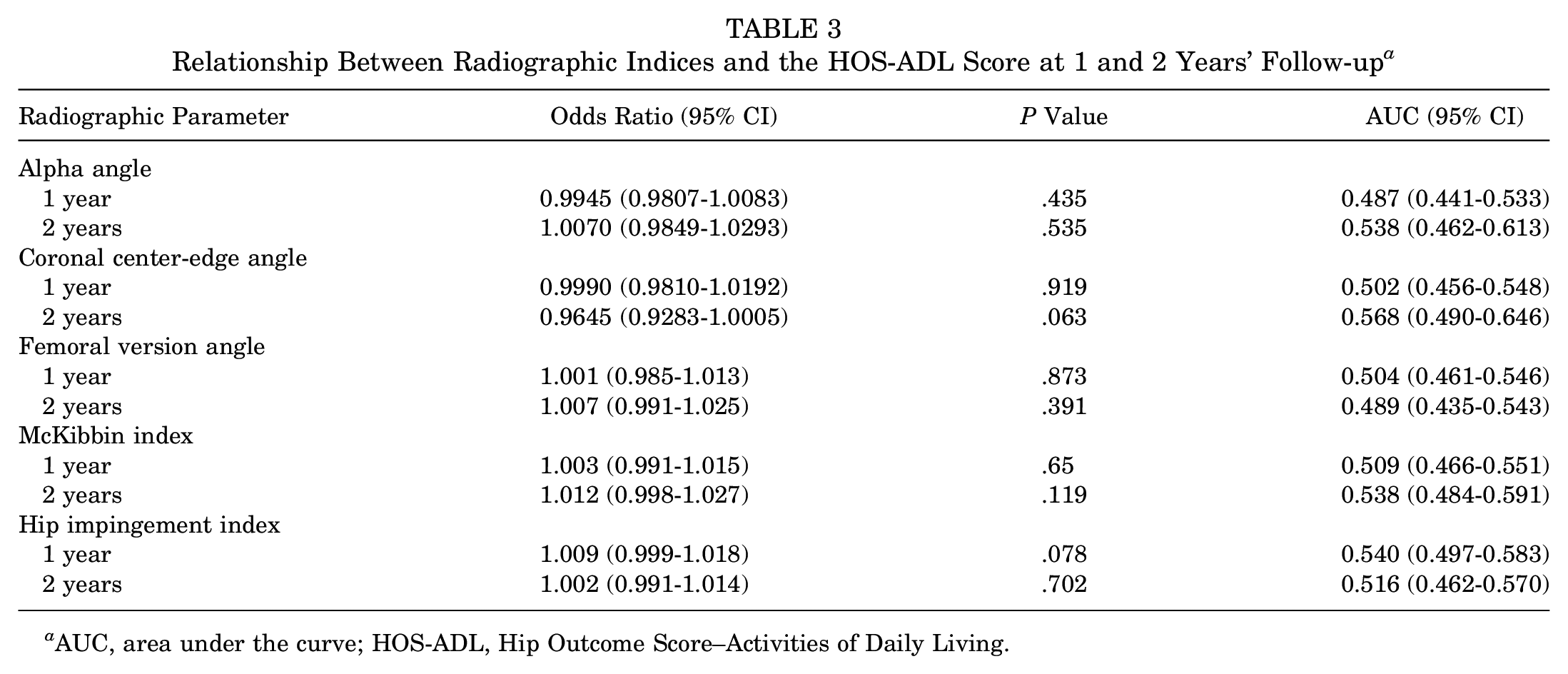
AUC, area under the curve; HOS-ADL, Hip Outcome Score–Activities of Daily Living.
Hip Outcome Score–Sport Specific
A total of 1675 (96.5%) completed the preoperative HOS-SS. Overall, 1233 (71.1%) completed the HOS-SS at 1 year, and 754 (43.5%) completed it at 2 years. Of these patients, 69.9% achieved the MCID at 1-year follow-up, and 74.7% achieved the MCID at 2-year follow-up.
For patients with 1-year HOS-SS scores, the mean preoperative HOS-SS score was 50.0 ± 23.7, and the mean 1-year HOS-SS score was 76.0 ± 26.3. The mean difference between 1-year and preoperative scores was 26.0 ± 29.5. For patients with 2-year HOS-SS scores, the mean preoperative HOS-SS score was 50.3 ± 23.5, and the mean 2-year HOS-SS score was 79.4 ± 24.7. The mean difference between 2-year and preoperative scores was 29.1 ± 29.5. The AUCs for the comprehensive multivariate model incorporating all radiographic angles for 1- and 2-year HOS-SS scores were 0.52 and 0.50, respectively, and reflected poor correlation between preoperative radiographic indices and HOS-SS scores. The alpha angle, coronal center-edge angle, femoral version angle, McKibbin index, and hip impingement index were not significant predictors of the HOS-SS score (Table 4).
Relationship Between Radiographic Indices and the HOS-SS Score at 1 and 2 Years’ Follow-up a
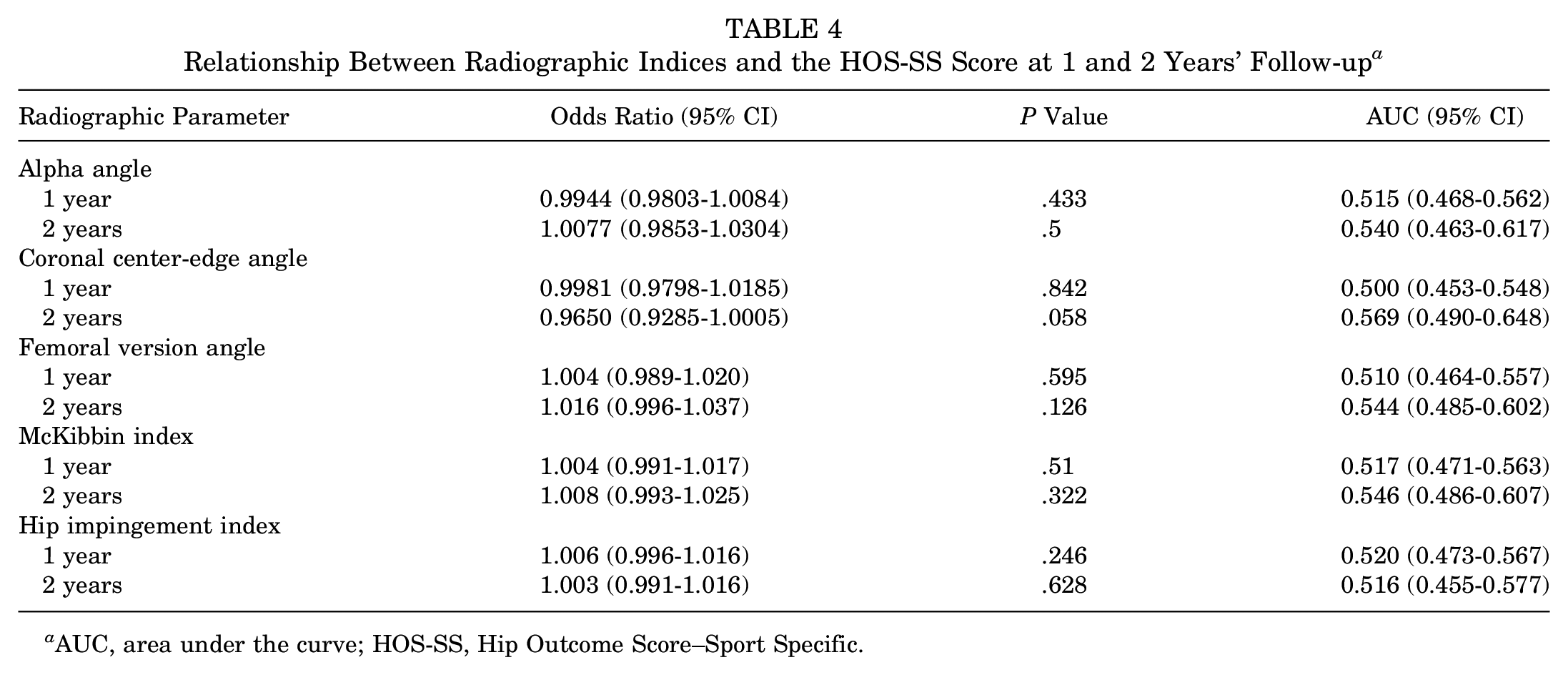
AUC, area under the curve; HOS-SS, Hip Outcome Score–Sport Specific.
International Hip Outcome Tool
A total of 1425 (82.1%) completed the preoperative iHOT-33. Overall, 1160 (66.9%) patients completed the iHOT-33 at 1 year, and 665 (38.3%) completed it at 2 years. Of these patients, 74.8% surpassed the MCID at 1 year, and 77.6% surpassed the MCID at 2 years.
For patients with 1-year iHOT-33 scores, the mean preoperative iHOT-33 score was 39.1 ± 17.1, and the mean 1-year iHOT-33 score was 71.8 ± 23.4. The mean difference between 1-year and preoperative scores was 32.7 ± 24.3. For patients with 2-year iHOT-33 scores, the mean preoperative iHOT-33 score was 39.5 ± 17.3, and the mean 2-year iHOT-33 score was 74.3 ± 24.5. The mean difference between 2-year and preoperative scores was 34.7 ± 24.5. The AUCs for the comprehensive multivariate model incorporating all radiographic angles for 1- and 2-year iHOT-33 scores were 0.56 and 0.54, respectively, and reflected poor correlation between preoperative radiographic indices and iHOT-33 scores. The alpha angle, femoral version angle, coronal center-edge angle, McKibbin index, and hip impingement index were not significant predictors of iHOT-33 scores (Table 5).
Relationship Between Radiographic Indices and the iHOT-33 Score at 1 and 2 Years’ Follow-up a
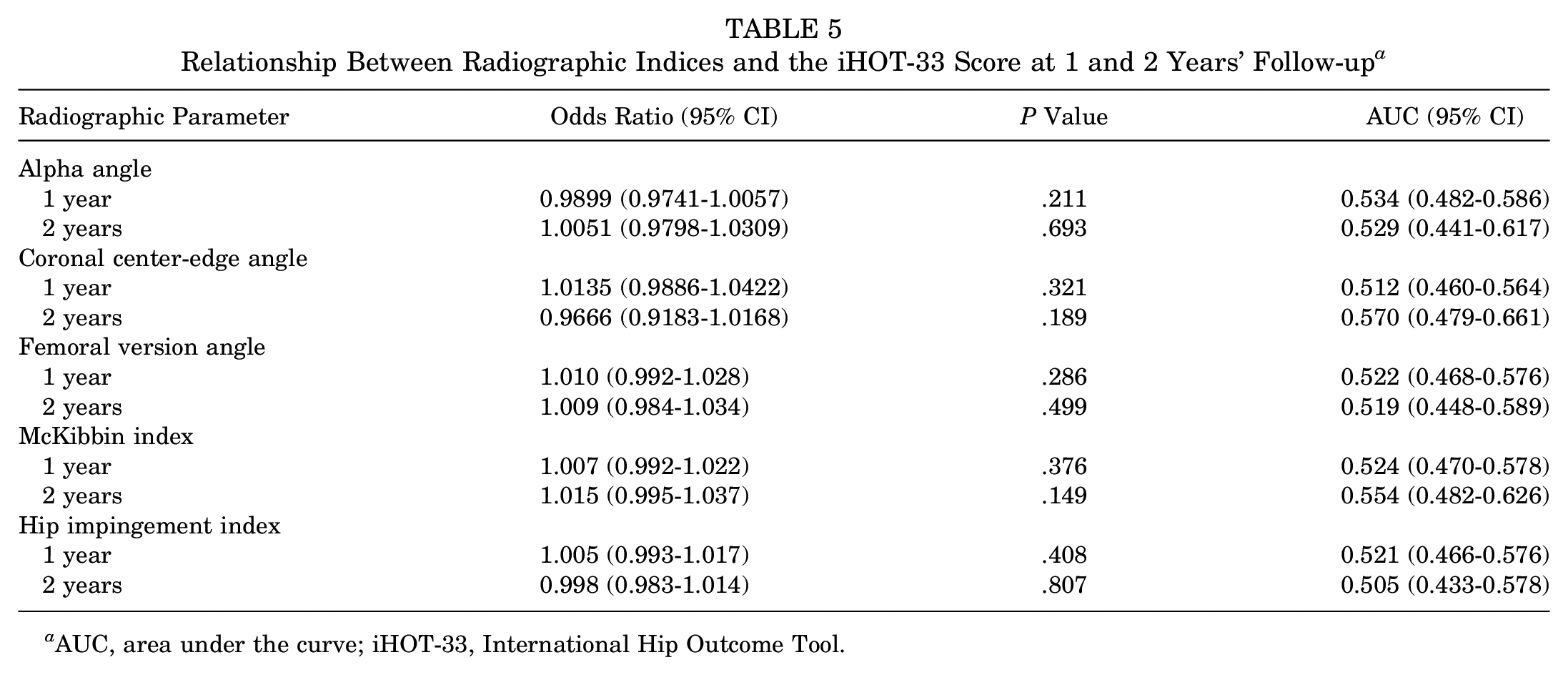
AUC, area under the curve; iHOT-33, International Hip Outcome Tool.
Discussion
The purpose of the present study was to apply a machine learning model to determine which preoperative radiographic indices, if any, among patients indicated for the arthroscopic correction of FAIS predict whether a patient will achieve the MCID for 1- and 2-year PROM scores. The secondary purpose was to evaluate if the alpha angle, femoral version angle, coronal center-edge angle, McKibbin index, and hip impingement index had similar associations with any of the 4 PROMs when isolated. In a series of 1735 patients indicated for primary hip arthroscopic surgery to correct FAIS, no apparent relationship existed between preoperative radiographic measurements and PROM scores at 1 and 2 years. In the overall cohort, the scores for all PROMs (mHHS, HOS-ADL, HOS-SS, and iHOT-33) improved by a clinically important degree as evidenced by a mean improvement beyond the MCID for each respective PROM. This suggests that, if surgical indications and techniques are sound for patients undergoing arthroscopic surgery for FAIS, the MCID for disease-specific PROMs is readily achievable at both 1 and 2 years postoperatively.
Previous research has not convincingly demonstrated a clear relationship between radiographic indices and PROMs, thus warranting an investigation. Several factors, such as femoral version, the McKibbin index, and center-edge angle, have been implicated as associative parameters that may predict a patient’s outcome. 9 However, identifying these key radiographic indices in isolation without context for all other available patient-related factors limits the applicability of the study. Moreover, treating these angular indices as continuous, instead of discrete, more appropriately accounts for the effects of these radiographic indices. A machine learning model, specifically the random forest model in this study, is uniquely advantageous in its capacity to learn from each of the 1735 patient cases to determine which data elements best predict achieving the MCID. Additionally, the model is capable of evaluating all radiographic indices as continuous variables. This study is the first to demonstrate that none of the studied radiographic indices, whether in isolation or in combination, predict surgical outcomes in terms of PROMs.
To our knowledge, only 2 previous reports have specifically evaluated the role of radiographic indices, such as femoral version and the McKibbin index, on any postoperative variable. Kelly et al 15 studied 56 hips and found that correction of the alpha angle improved internal rotation of the hip, although the magnitude of improvement was diminished in the patient cohort with relative retroversion. Fabricant et al, 9 however, analyzed 243 patients and found that, although patients with all degrees of femoral version achieved improvement, the least improvement was noted in patients with femoral retroversion. Moreover, no association between the McKibbin index and any PROMs was found, in concordance with the findings of our study. The influence of the coronal center-edge angle, hip dysplasia, and alpha angle has also been studied with a lack of conclusiveness. Beck et al 2 noted that patients with borderline dysplasia (coronal center-edge angle of 20°-25°) did not have significantly inferior outcomes after hip arthroscopic surgery. Similarly, for the preoperative alpha angle, there is an abundance of literature suggesting that this variable is not a significant predictor; however, one study by Lansdown et al 16 found that the preoperative alpha angle was predictive of postoperative scores. The latter study, however, was limited by a lack of analysis for a clinically meaningful improvement in outcomes. Although radiographs of patients in the current study did not possess the field of view to acquire spinopelvic parameters, future studies will evaluate the importance of the spinopelvic relationship using radiographic parameters.
Across the 1735 patients included in the present study, clinical improvement after FAIS surgery was found, regardless of the preoperative alpha angle, femoral version angle, and acetabular version angle. This study represents one of the largest studies to confirm that arthroscopic correction is possible, regardless of preoperative radiographic variables. Interestingly enough, the mean scores for all 4 PROMs continued to improve between 1 and 2 years, although the MCID had already been exceeded. This confirms previously reported findings in a case series of 719 patients that demonstrated that, for certain outcomes, absolute PROM scores continued to improve up to 2 years after hip arthroscopic surgery. 21 In practice, this study suggests that radiographic indices may be beneficial to identify the degree of pathoanatomy for surgical correction. However, counseling patients that they are at an increased risk for not achieving clinical improvement with appropriately indicated and well-executed surgery based on radiographic indices does not reflect the evidence presented in this study. It is important to keep in mind that a confounder in the current study is that included patients were indicated for arthroscopic surgery by hip preservation experts, and as such, radiographic parameters were already taken into account to a certain degree.
A rigorous method for measuring femoral version by comparing the difference between the posterior femoral condylar axis and the axis of the femoral neck was used in this study.3,19 This method generates a single independent variable that accounts for femoral torsion as well as neck version. However, deformities proximal to the neck (eg, head tilt) are unable to be accounted for, which may introduce further differences in version or rotational mechanics among patients. Future research may focus on quantifying such further deformities by defining the location of rotational morphology. Although assessing the accuracy of our measurement method is impossible in the absence of a globally accepted gold standard, the precision attained by musculoskeletal radiologists is known to be better than that achieved using similar magnetic resonance imaging techniques and has been validated with nearly perfect intraobserver correlation to confer generalizability of our results to practicing orthopaedic surgeons working with musculoskeletal radiologists. 3 One of the additional strengths of this study beyond the rigorous radiographic measurements using preoperative CT is the large, uniform patient sample and prospective registry data collection. This study represents the first in the sports literature to apply advanced machine learning techniques to radiographic data and investigate their effects on disease-specific patient-reported outcomes. While this study is not the first to employ machine learning for FAIS, our study accentuates the value of this methodology. Nwachukwu et al 20 analyzed several patient metrics using a binary logistic regression model for 1103 patients and identified anxiety/depression and preoperative hip injection as modifiable risk factors predictive of the inability to reach the MCID. The model from this study may be readily built upon the algorithm by Nwachukwu et al 20 to provide a comprehensive preoperative assessment, although radiographic parameters are unlikely to be driving contributors. However, the influence of radiographic parameters with preoperative injection status, anxiety, alpha angle, and the McKibbin index, among other permutations, is unknown and can only result in a strengthened model by more accurately representing the risk of not achieving the MCID in this complex pathoanatomy. Unlike non–machine learning models, our study is scalable and additive in that the accuracy improves with more patient data to strengthen the likelihood of a global consortium invested in studying outcomes after the arthroscopic correction of FAIS.
There are limitations to the present study. The relatively low follow-up rates for PROMs, particularly at 2 years postoperatively, approximating 45%, may have introduced significant bias for which we cannot account, thus limiting generalizability. However, increasing data surrounding PROMs in both the sports and arthroplasty literature have suggested little to no difference at 12 and 24 months postoperatively.23,26 Flores et al 11 found that the greatest improvements in PROMs after FAIS occurred in the first 3 months, reporting that the percentage of patients surpassing the MCID plateaued after 3 months for most scores. Although data were collected prospectively, the results were analyzed retrospectively, which may have led to selection bias. This potential was minimized with the rigorous inclusion and exclusion criteria. For situations with nonmodifiable variables, such as preoperative radiographic indices, large registries remain the greatest resource for analysis of observational data, and this registry represents one of the largest single-institution hip arthroscopic databases in the United States. Moreover, the database possesses the advantage of continuous radiographic measurements because of the study surgeons’ habit of performing preoperative CT for patients undergoing hip arthroscopic surgery. However, the CT version measurements made by the musculoskeletal radiologists may not be generalizable to others or to orthopaedic surgeons. Although the study question focused on the effect of preoperative radiographic parameters of patients who were already indicated for surgery, the strict surgical indications did not address all available patients who had hip pain, thus creating a spectrum bias. For example, the coronal center-edge angle may have been found to be a prognostic factor if indications were loosened to surgically treat the population with dysplasia. An additional limitation unaccounted for in the machine learning model was the degree of intraoperative correction, which could have been mitigated using postoperative CT to measure the change in indices. Despite this potential limitation in generalizability, the small number of surgeons performing the procedure served as an internal control for intraoperative variation. The McKibbin index used in the present study was a modification of the original index designed to evaluate infant hip stability, and it has not been specifically validated for use in FAIS. Future research could develop and validate a radiographic measure of combined version for use in FAIS.
Conclusion
Clinical improvements after arthroscopic FAIS surgery can be achieved, regardless of preoperative radiographic indices, such as the femoral version angle and alpha angle. No specific radiographic parameter or combination of indices was found to be predictive of reaching the MCID for any of the 4 studied PROMs at either 1 or 2 years’ follow-up.
Footnotes
Submitted March 26, 2020; accepted June 8, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was funded internally by the Cleveland Clinic. P.N.R. has received research support from FocusMotion and holds stock in Johnson & Johnson. D.H.N. has received consulting fees from Arthrex, Stryker, DePuy Synthes, and Biomet Orthopedics and education payments from Smith & Nephew and Gotham Surgical Solutions & Devices. A.S.R. has received consulting fees from Smith & Nephew, Medical Device Business Services, Arthrex, Linvatec, Heron Therapeutics, Medtronic, Moximed, and Stryker; has received royalties from ConforMIS and DePuy Orthopaedics; has received research support from Stryker, Arthrex, and DePuy Orthopaedics; and holds stock in ConforMIS and Enhatch. B.T.K. has received consulting fees from Arthrex and Smith & Nephew, has received royalties from Arthrex, has received financial or material support from Organicell, and holds stock in HS2. B.U.N. has received consulting fees from Stryker, Wright Medical Technology, and Zimmer Biomet and education payments from Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.