
Abstract
Background:
Adverse effects of graft extrusion after meniscal allograft transplantation (MAT) are difficult to assess and can be determined only in the long term using a simple radiograph. Recently, subchondral bone marrow lesions (BMLs) detected on magnetic resonance imaging (MRI) scans have been used to evaluate the outcomes or prognoses of various knee surgeries. However, whether subchondral BMLs on MRI scans reflect the effects of allograft extrusion remains unclear.
Hypothesis:
Subchondral BML in the lateral compartment of the knee joint on postoperative MRI scans would be associated with graft extrusion after lateral MAT.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
Overall, 170 patients with lateral MAT between 2008 and 2013 were classified into extrusion (≥3 mm) and nonextrusion (<3 mm) groups based on findings on MRI scans obtained 3 to 6 months postoperatively. Subchondral BMLs in the lateral compartment were evaluated on the latest MRI scans. To exclude any bone marrow signal changes other than those caused by allograft extrusion, the latest MRI scans were compared with those obtained 3 to 6 months postoperatively. Only subchondral BMLs that occurred after that time point were counted. The association between allograft extrusion and subchondral BML was assessed using chi-square analysis. Logistic regression analysis was performed to control other related factors, including age, sex, body mass index, time from previous meniscectomy, alignment, and cartilage status at the time of MAT. Clinical outcomes according to subchondral BML were evaluated using the Lysholm score.
Results:
Of the 170 patients, 20 (11.8%) had subchondral BML on the latest MRI scans at a mean 53.6 ± 31.2 months postoperatively, with 14 and 6 patients in the extrusion and nonextrusion groups, respectively. Chi-square analysis showed a significant association between allograft extrusion and subchondral BMLs (P = .025). Logistic regression analysis showed that extrusion and age were significant factors associated with subchondral BML (P = .011 and .004, respectively). However, no differences were observed in the Lysholm scores in accordance with the subchondral BML (P = .248).
Conclusion:
Subchondral BMLs on postoperative MRI scans were associated with graft extrusion after lateral MAT. However, there was no difference in clinical outcomes according to subchondral BML.
With the establishment of the biomechanical role of menisci, meniscal allograft transplantation (MAT) has received growing attention as a viable treatment for meniscus-deficient knees. Its efficacy in relieving pain and improving knee function is well-supported by numerous previous studies.29,43,47 However, graft extrusion has been consistently reported as a potential complication after MAT.32,41,46 Although biomechanical disadvantages are expected, clinical implications of MAT extrusion have not been fully elucidated.
There are some differences between extrusion of the native meniscus and that of an allograft. Extrusion of the allograft has been observed more often in magnetic resonance imaging (MRI) analyses than has that of the normal meniscus.7,46 Allograft extrusion beyond the articular margin has been reported in up to 25% to 75% of patients.15,21,27,30-32,40 While extrusion of the native meniscus is associated with meniscal tear or underlying degeneration of the joint,5,44 conflicting outcomes have been reported regarding MAT extrusion. Short- to midterm follow-up studies have shown no significant differences in clinical outcomes according to MAT extrusion.15,31 However, a long-term observational study with a minimum 8-year follow-up period revealed that MAT extrusion had an adverse effect on radiologic outcomes measured using joint space width. 33 The effect of MAT extrusion on the joint has not been investigated using more sensitive methods, other than simple radiography.
Recently, the presence of subchondral bone marrow lesions (BMLs) on MRI scans was used to evaluate the outcome or prognosis of various knee surgeries.6,14,17,24,36,37 Furthermore, previous studies have proved that subchondral BML was associated with progression of osteoarthritis or functional outcomes from it.11,19 For MAT, a single study focused on preoperative BML affecting clinical outcomes. 42 There has been no other study to date regarding subchondral BML as a postoperative change in MAT. Therefore, the objective of this study was to analyze the effects of graft extrusion after lateral MAT on the postoperative occurrence of subchondral BML. We hypothesized that subchondral BML in the lateral compartment of the knee joint would be associated with allograft extrusion on postoperative MRI.
Methods
Patient Selection
A total of 204 consecutive patients who underwent lateral MAT between January 2008 and December 2013 were retrospectively reviewed following approval from the institutional review board of Asan Medical Center. Physically active patients who reported persistent localized joint line pain after subtotal or total meniscectomy underwent the index surgery.16,35 Previous or concurrent procedures were applied to correct severe malalignment or instability of the joint. A minimum preserved joint space of 2 mm was confirmed on the Rosenberg view before MAT, 22 and the cartilage status was double-checked intraoperatively using the International Cartilage Repair Society (ICRS) scale. 25 ICRS grade 3 or less and localized grade 4 defects confined to the area covered by the meniscus were considered acceptable indications for MAT. Postoperative radiologic evaluation included MRI (Achieva 3T; Philips Healthcare) performed during the first postoperative year and every 2 or 3 years thereafter. The Lysholm scoring system was used for clinical evaluation at every follow-up with a 1- or 2-year interval.
Patients were included if they (1) underwent primary lateral MAT; (2) were evaluated using MRI scans at least 1 year postoperatively, which were necessary to detect subchondral BML and allograft extrusion; (3) did not show tear of the allograft that could lead to bone marrow signal changes in itself; and (4) did not have a history of trauma or vigorous sports activity that could cause acute bone marrow edema at the time of MRI examination. Accordingly, 4 patients with revision MAT, 20 patients without available MRI scans, and 10 patients with allograft tear were excluded, and 170 remaining patients were enrolled.
Surgical Technique and Rehabilitation
All transplantations were performed by 1 senior surgeon (S.-I.B.). The keyhole technique was applied for lateral MAT. 20 Fresh-frozen allografts were used in all cases, and their size was determined based on methods described by Pollard et al. 39 Lateral MAT started with an arthroscopic examination, after which the remaining host menisci were resected. Preparation of the tibial slot for the bone bridge of the lateral meniscus was followed by the introduction of the allograft through anterior mini-arthrotomy. Once the optimal position of the allograft was confirmed, it was repaired using the traditional inside-out method with 10 to 12 vertical No. 2-0 nonabsorbable sutures (Orthotech). The anterior part of the allograft was sutured to the anterior capsule under direct visualization. Rehabilitation was initiated using quadriceps sets, straight leg raises, and calf pumps immediately after surgery. Postoperative range of motion achieved full extension within 1 week, 90° of flexion within 4 weeks, and 120° of flexion at 6 to 8 weeks. Toe-touch weightbearing was allowed during the first 2 weeks and was gradually advanced to full weightbearing at 6 to 8 weeks postoperatively. Patients were advised to participate only in low-impact sports activities and light labor because of concerns regarding the deterioration of the meniscal transplants.
Allograft Extrusion and Subchondral BML on Postoperative MRI Scans
Allograft extrusion and subchondral BML were always evaluated using 3.0-T superconducting MRI. Extrusion was measured on MRI scans obtained 3 to 6 months postoperatively by drawing 2 vertical lines joining the outer edges of the tibial plateau surface and the meniscus (Figure 1). The coronal image showing maximal extrusion was chosen after confirming its location on the matched sagittal image. On the basis of the maximal amount of extrusion, patients were categorized into extrusion (≥3 mm) and nonextrusion (<3 mm) groups, as in most previous related studies in the literature.4,7,15,30-32,48
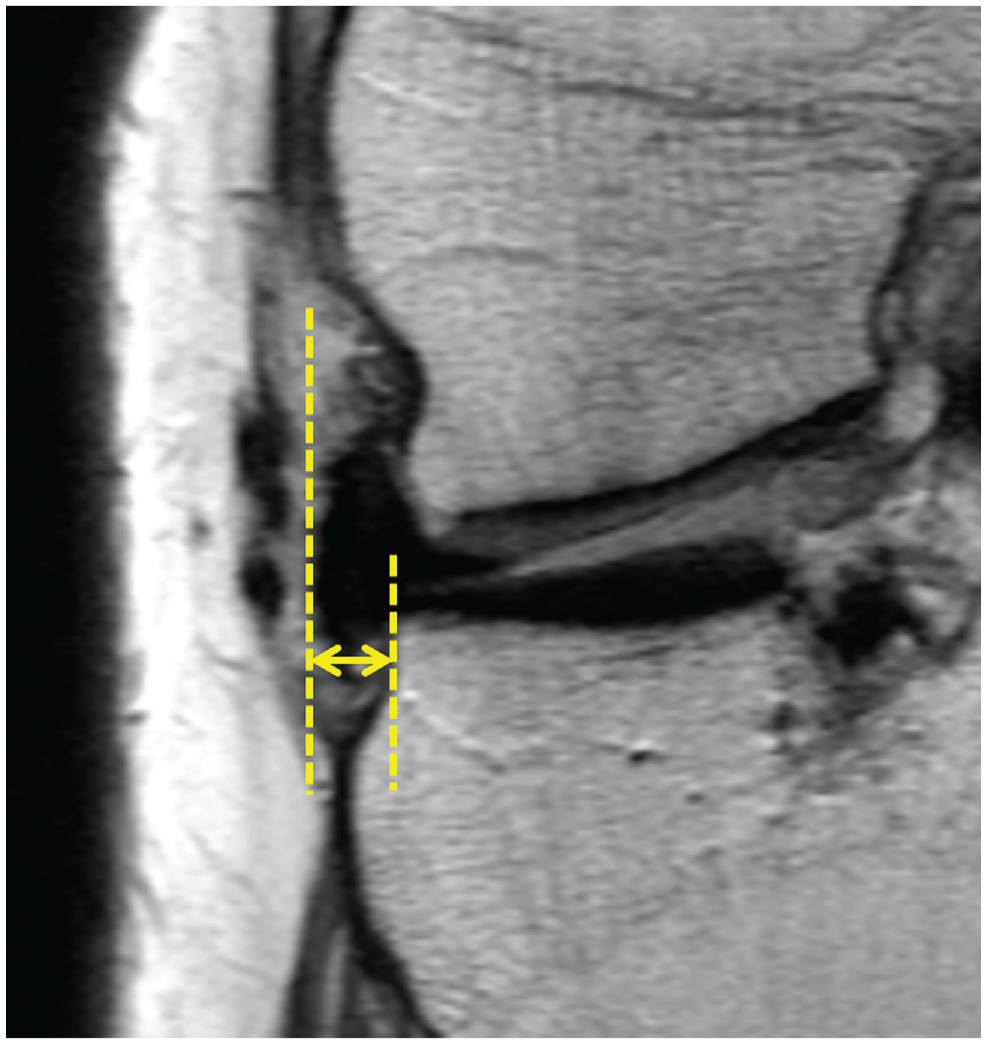
Extrusion was defined as the distance between 2 vertical lines touching the outer edge of the tibial plateau surface and the meniscal outer edge.
For subchondral BML, only changes that occurred after MAT were counted. Thus, the latest MRI scans were compared with those obtained 3 to 6 months postoperatively so that BML that already existed before or just after MAT could be ruled out. Subchondral cysts were distinguished based on the definition of the Whole-Organ Magnetic Resonance Imaging Score system, 38 which was a focus of markedly increased signal in the subchondral bone without evidence of internal trabecular marrow tissue.
Two orthopaedic surgeons (S.-I.B. and J.-H.S.) evaluated the presence of allograft extrusion (≥3 mm) and subchondral BML independently. The interrater reliability of both parameters was assessed using Cohen kappa: <0.20, 0.21 to 0.40, 0.41 to 0.60, 0.61 to 0.80, and >0.80 showed poor, fair, moderate, good, and very good agreement levels, respectively. 3
Statistical Analysis
The association between allograft extrusion and subchondral BML was assessed using chi-square analysis. Thereafter, logistic regression analysis was performed to control other related factors including age, sex, body mass index, time from previous meniscectomy, alignment, and cartilage status at the time of MAT. For alignment, valgus and varus mechanical alignment were defined as positive and negative, respectively. The status of the femoral and tibial articular cartilage in each compartment was evaluated intraoperatively using the ICRS grading system. The cartilage status was classified into low ICRS (grade 0, 1, or 2) on both the femoral and tibial sides, high ICRS (grade 3 or 4) on either the femoral or tibial side, and high ICRS (grade 3 or 4) on both the femoral and tibial sides. 26 Clinical outcomes according to subchondral BML were evaluated using the Lysholm score and analyzed using the t test or Mann-Whitney U test. All statistical analyses were performed using IBM SPSS Statistics software (version 19.0; IBM Corp), with P < .05 considered statistically significant.
Results
Of the 170 patients with primary lateral MAT, there were 95 male and 75 female patients, with a mean age of 33.6 ± 10.2 years (range, 15-57 years). The mean follow-up duration was 53.6 ± 31.2 months (range, 12-124 months). The preoperative Lysholm score was 62.8 ± 15.3, which improved to 90.8 ± 7.3 at the final evaluation. The mean Tegner activity levels were 4.0 ± 1.1 and 4.5 ± 1.1 before surgery and at the latest follow-up, respectively. Characteristics of the study population for allograft extrusion are summarized in Table 1. The interrater reliability using Cohen kappa was 0.83 (95% CI, 0.74-0.91) for allograft extrusion and 0.82 (95% CI, 0.72-0.89) for subchondral BML, both indicating very good agreement levels.
Descriptive Data for Allograft Extrusion a
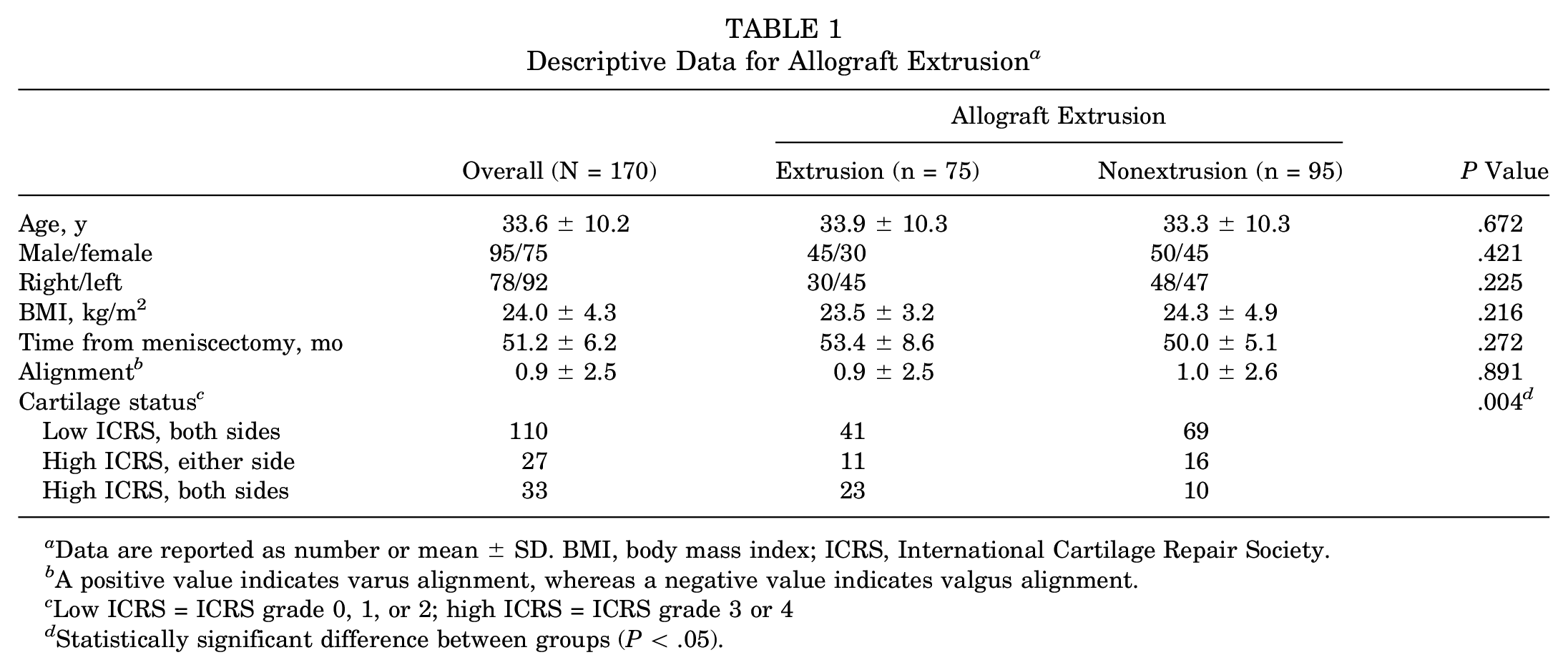
Data are reported as number or mean ± SD. BMI, body mass index; ICRS, International Cartilage Repair Society.
A positive value indicates varus alignment, whereas a negative value indicates valgus alignment.
Low ICRS = ICRS grade 0, 1, or 2; high ICRS = ICRS grade 3 or 4
Statistically significant difference between groups (P < .05).
Subchondral BML According to Allograft Extrusion
Subchondral BMLs were noted on the latest MRI scans in 20 patients (11.8%): 9 patients had subchondral BML on the tibial side, 8 on the femoral side, and 3 on both sides. Fourteen out of 75 patients (18.7%) in the extrusion group showed subchondral BMLs, whereas 6 out of 95 patients (6.3%) in the nonextrusion group showed them (P = .025, chi-square test). The logistic regression analysis including other covariates showed that extrusion and age were significant factors associated with subchondral BML (P = .011 and .004, respectively) (Table 2 and Figure 2).
Logistic Regression Analysis of Related Factors Associated With Subchondral BML a
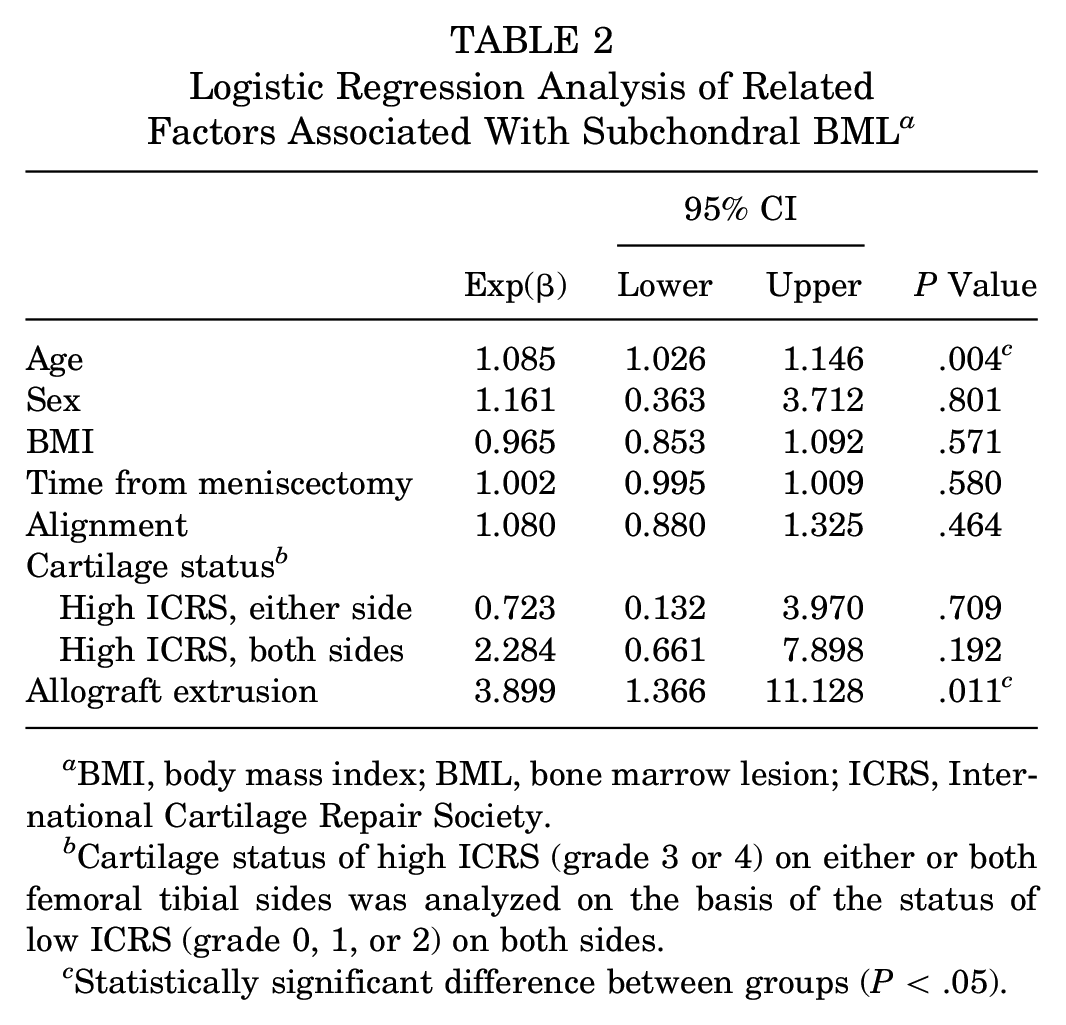
BMI, body mass index; BML, bone marrow lesion; ICRS, International Cartilage Repair Society.
Cartilage status of high ICRS (grade 3 or 4) on either or both femoral tibial sides was analyzed on the basis of the status of low ICRS (grade 0, 1, or 2) on both sides.
Statistically significant difference between groups (P < .05).
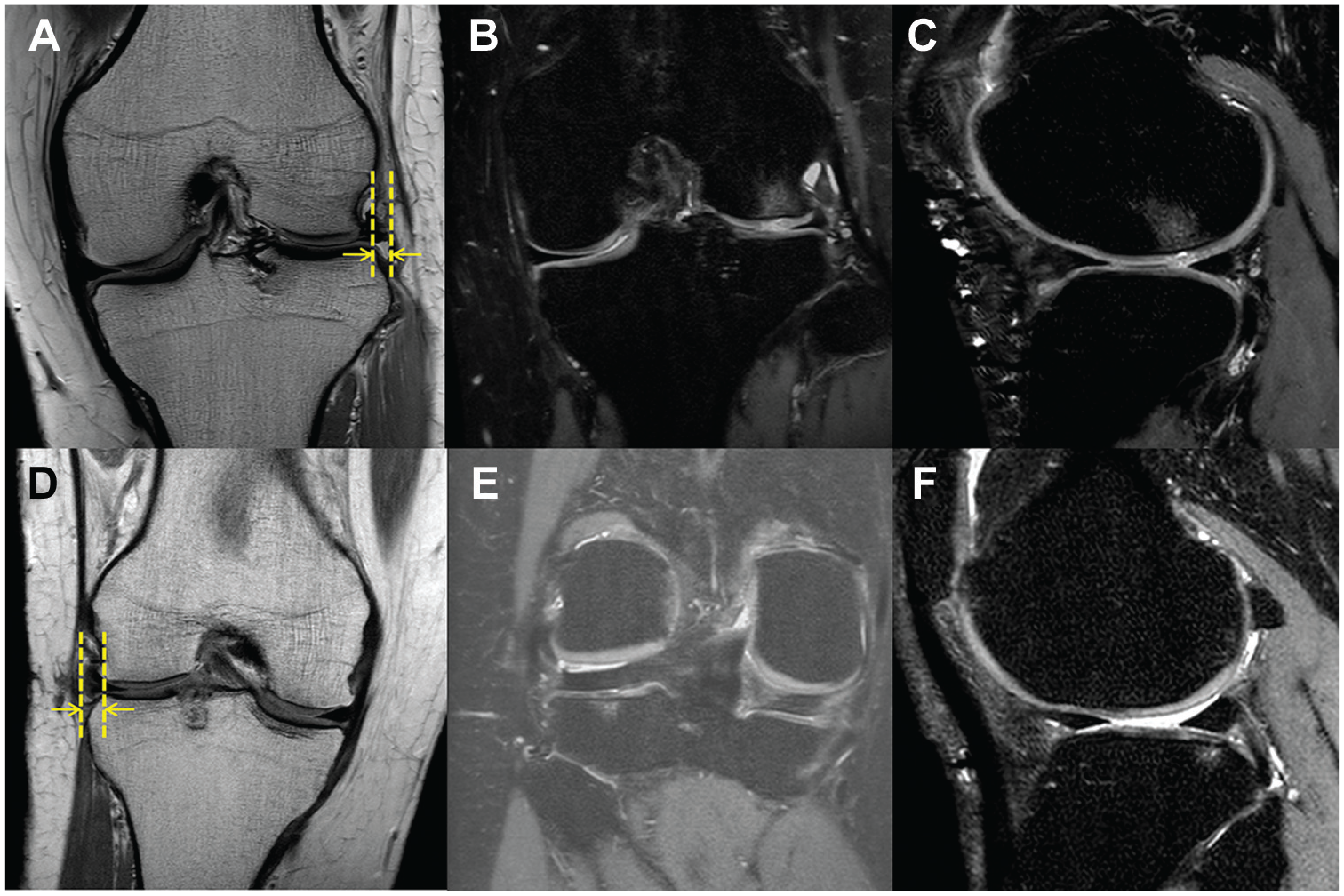
(A) Magnetic resonance imaging (MRI) scan of a 38-year-old man at 6 months after surgery showing allograft extrusion of 3.58 mm. (B) Coronal and (C) sagittal MRI scans of the same patient at 58 months postoperatively showing subchondral bone marrow lesion (BML) in the lateral femoral condyle. (D) MRI scan of a 35-year-old woman at 6 months after surgery showing allograft extrusion of 3.44 mm. (E) Coronal and (F) sagittal MRI scans of the same patient at 64 months postoperatively showing subchondral BML in the lateral tibial plateau. Vertical lines indicate the outer edge of the tibial plateau surface and the lateral meniscus and arrows indicate the amount of extrusion.
Comparison According to Subchondral BML
Comparison according to subchondral BML showed significant differences in age and cartilage status (P = .004 and .003, respectively). No differences were found in the other variables. The mean Lysholm score improved from 65.6 ± 15.6 preoperatively to 89.0 ± 7.4 at the final follow-up in patients with subchondral BML and from 63.9 ± 15.7 to 91.1 ± 7.3 in patients without subchondral BML. No differences were seen in the preoperative and final Lysholm scores according to the subchondral BML (P = .591 and .248, respectively). The preoperative and final Tegner activity levels were also not different for the subchondral BML (P = .893 and .821, respectively) (Table 3).
Comparison According to Subchondral BML a
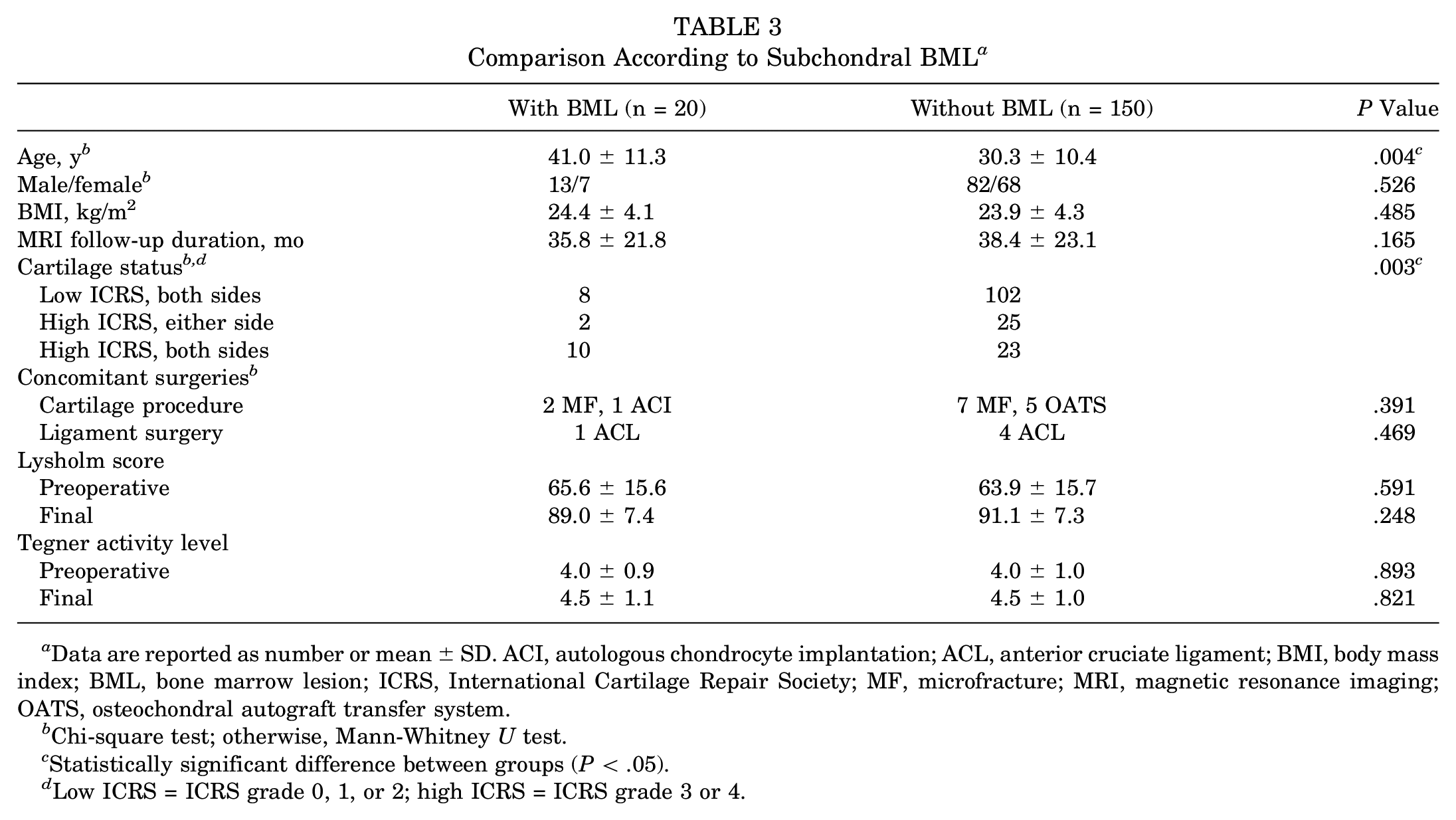
Data are reported as number or mean ± SD. ACI, autologous chondrocyte implantation; ACL, anterior cruciate ligament; BMI, body mass index; BML, bone marrow lesion; ICRS, International Cartilage Repair Society; MF, microfracture; MRI, magnetic resonance imaging; OATS, osteochondral autograft transfer system.
Chi-square test; otherwise, Mann-Whitney U test.
Statistically significant difference between groups (P < .05).
Low ICRS = ICRS grade 0, 1, or 2; high ICRS = ICRS grade 3 or 4.
Discussion
The present study found that graft extrusion after lateral MAT was associated with the postoperative occurrence of subchondral BML. The logistic regression analysis performed to control for other related factors revealed that extrusion and age were significant factors for subchondral BML. No difference was seen in the postoperative Lysholm scores according to subchondral BML.
Extrusion of MAT was considered different from that of the native meniscus. The latter was associated with the degeneration of articular cartilage and the meniscus itself.1,13 On the other hand, some authors have found various factors other than joint degeneration contributing to allograft extrusion after MAT, such as graft size, 46 position of the graft,2,8 osteophytes, 18 or cartilage wear on the tibial side. 28 However, regardless of the site of extrusion, similar biomechanical disadvantages are expected. Pathologic extrusion of the native meniscus was reported to cause excessive load transmission. 44 For MAT extrusion, an abnormal position of the allograft and incongruity of the femoral condyle were found to be related to it.10,45
There have been numerous studies regarding the effects of MAT extrusion. To the best of our knowledge, only 1 long-term follow-up study verified the disadvantageous effects of MAT extrusion, 33 whereas others reported no difference in the outcomes of MAT for the extrusion. 31 The present study confirmed the results of the previous long-term study and showed that the adverse effects occurred earlier than during the long-term period.
Subchondral BML has been used to evaluate the outcomes of various knee surgeries. Regarding anterior cruciate ligament reconstruction, the development of osteoarthritis or cartilage degeneration was associated with subchondral BML.14,19 Some studies also demonstrated a correlation between clinical outcomes and subchondral BML, whereas others reported no significant association.6,14,24 Previous studies about autologous chondrocyte implantation showed conflicting results concerning a correlation between subchondral BML and clinical outcomes.9,12,36,37 For MAT, Saltzman et al 42 first focused on subchondral BML and demonstrated that preoperative subchondral BML in the tibia was associated with clinical scores after isolated MAT.
In the present study, only postoperative change of subchondral BML was included to assess the effect of MAT extrusion. Thus, the latest MRI scans were compared with those obtained 3 to 6 months postoperatively. In this way, bone marrow signal changes related to the keyhole technique for lateral MAT or BMLs that already existed before MAT could be distinguished. This study also excluded medial MAT because it was often performed concurrently with anterior cruciate ligament reconstruction, which would have been a confounding factor for subchondral BML.
Clinical outcomes measured using the Lysholm scores showed no difference according to subchondral BML. This was consistent with the findings of Lee et al, 33 who reported no difference in clinical outcomes for MAT extrusion. As they said, clinical scores do not reflect the progressive outcome or prognosis of surgery but only reflect the current outcome. Saltzman et al 42 found that the preoperative BML size was correlated with worse postoperative pain measure and activity ratings. Preoperative BML may represent underlying cartilage degeneration or the degree of osteoarthritis, which might have been attributed to the correlation between preoperative BML and clinical outcomes. When confined to postoperative bone marrow changes, the present study found patient age to be a significant factor for subchondral BML. This also supported the notion that subchondral BML reflected degeneration of the joint.
There were several limitations in this study. First, the quantitative analysis could not be performed on postoperative subchondral BML. As mentioned above, the present study focused only on marrow signal changes after MAT, which was why the quantification of subchondral BML was hardly feasible. However, previous studies have considered subchondral BML as present or not present.22,42 Considering that the purpose of the present study was to verify the association between MAT extrusion and subchondral BML, the binary determination was enough for the analyses. Second, MAT extrusion was only determined at a single point. Although studies have reported that extrusion did not progress over time during the short- 32 and midterm period, 23 long-term follow-up results of the extrusion were not evaluated. Third, MRI was performed with patients in the supine position, and MAT extrusion might be undetected without weightbearing. However, the study participants were categorized into the extrusion and nonextrusion groups based on a cutoff extrusion of 3 mm, which has been applied widely in the previous literature using nonweightbearing MRI to evaluate meniscal or allograft extrusion.5,15,33,34 Fourth, other risk factors for BML are undetected, in spite of our effort to include a comprehensive set of related factors in the logistic regression analysis regarding BML. This might be the reason why some knee joints without extrusion still developed BMLs. Fifth, to clarify the effect of MAT extrusion on BML, the interval between the onset of graft extrusion and BML should be considered; however, such analysis was not possible because both extrusion and subchondral BMLs were to be identified using MRI, which could not be prescribed so often in practice.
Conclusion
Subchondral BMLs on postoperative MRI scans were associated with graft extrusion after lateral MAT. However, there was no difference in clinical outcomes according to subchondral BML.
Footnotes
Submitted January 16, 2020; accepted June 18, 2020.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.