
Abstract
Background:
Meniscal vascular supply is an important determinant of its healing potential. It has been reported that only the peripheral 30% of the meniscus is vascularized in cadavers aged 53 to 94 years; however, the vascularity in young patients, in whom meniscal repair is more often performed, is unknown.
Purpose:
The primary objective was to analyze and measure the microvascular anatomy of the meniscus in adult cadaveric specimens <35 years old. The secondary objective was to assess angiogenic potential by quantifying regional gene expression in a meniscal allograft cohort <45 years old.
Study Design:
Descriptive laboratory study.
Methods:
In part 1 of this study, 13 fresh-frozen cadaveric knees (age range, 22-34 years; mean, 28.5 years) underwent popliteal artery India ink injection and tissue clearing using a Spalteholz technique, followed by microvascular vascular measurement. In part 2, mRNA was isolated from 13 meniscal allografts (age range, 17-43 years; mean, 27.2 years), and expression of angiogenic genes, vascular endothelial growth factor (VEGF), and vascular endothelial growth factor receptor 1 (FLT1) was quantified using real-time polymerase chain reaction.
Results:
The maximal depth of vascular penetration into the periphery of the medial and lateral menisci ranged from 0% to 42% and 0% to 48%, respectively. There was variation in the degree of vascular penetration within the medial meniscus, with the posterior horn having a significantly smaller depth of penetration (median, 8.7%) than that of the anterior horn (median, 17.4%; P < .0001) or midbody (median, 17.5%; P = .0003). There were no differences in angiogenesis gene expression (VEGF/FLT1) based on circumferential or radial meniscal locations.
Conclusion:
The vascular supply of the medial and lateral menisci in specimens from adults <35 years of age extended farther than what was reported in specimens from older individuals; however, median values remained consistent. Gene expression of the angiogenic marker VEGF was low throughout all regions of uninjured menisci from young adults, which is consistent with reports in older specimens.
Clinical Relevance:
Improved understanding of meniscal vascular supply in young adults is critical to informing clinical treatment decisions.
It is well-established that the medial and lateral menisci play an integral role in the complex function of the knee joint. The menisci have several important functions that include load distribution and absorption, reduction of joint contact pressure, 34 knee stability, joint lubrication, 21 proprioception, 37 and increase of joint congruity.3,15,16,22 The role of the menisci in maintaining biomechanical knee stability is especially important in the setting of concurrent ligament injury, where the menisci act as secondary stabilizers to increased knee motion.2,35 Meniscal tears disrupt these functions, leading to altered knee homeostasis, which predisposes the knee to degenerative changes, instability, and chondral damage.
Treatment of meniscal tears aims to improve patient symptoms and restore normal anatomy and function whenever possible. Many variables are involved in deciding how to treat a meniscal tear: patient age and concurrent knee procedure (eg, anterior cruciate ligament reconstruction) as well as tear chronicity, location, type, and size. The vascular supply is believed to be one of the most critical factors in enabling meniscal repair. Studies have reported that tears within 2 mm of the meniscocapsular junction have the highest rates of healing after repair, while those >4 mm away from the meniscal rim have higher rates of failure.10,33 However, there are favorable clinical data reported for meniscal repairs performed outside this region, especially in younger patients.24,25,30
The vascularity of the menisci has been studied for nearly 100 years.13,18,32 At birth, the entire meniscus is vascular; however, the distribution of vascularity recedes toward the periphery during development.12,28 Arnoczky and Warren 5 were the first to provide a detailed description of the microvascularity of the human meniscus, reporting that only the peripheral 10% to 25% of the lateral meniscus and 10% to 30% of the medial meniscus were vascular. Their study indicated that the meniscal blood supply arises from the superior and inferior branches of the medial and lateral genicular arteries, which form a perimeniscal capillary plexus that sends radial branches into the peripheral meniscal stroma. A limitation of the Arnoczky and Warren study was that the authors reported on cadaveric knees that ranged in age from the 6th decade to the 10th. In addition, modern techniques allow for assessment of a tissue’s genetic makeup and innate angiogenic ability. While meniscal expression of vascular endothelial growth factor (VEGF) has been described in cadaveric specimens in their 8th and 9th decades, it has not been reported in young specimens.
It is unknown if the vascular supply of younger patients, in whom meniscal repair is more common, would have a more robust vascular supply. Thus, our main purpose was to analyze and measure the microvascular anatomy of the meniscus in adult cadaveric specimens <35 years old. Our secondary objective was to assess for angiogenesis gene expression in a meniscal allograft cohort <45 years old. We hypothesized that specimens <35 years of age would have greater depth of vascular penetration than that reported by Arnoczky and Warren. 5 We also hypothesized that meniscal allograft specimens <45 years of age would have higher levels of VEGF expression.
Methods
Microvascular Anatomy
Thirteen fresh-frozen cadaveric knees were obtained from commercial vendors and used for this study (n = 7 from Science Care, n = 4 from Innoved, n = 2 from United Tissue Network). Specimens were from donors ranging in age from 22 to 34 years old (mean, 28.5), with 9 men and 4 women. Ten were from White, 2 from Latino, and 1 from African American donors. All knees were inspected for previous meniscal injury via arthroscopy before inclusion. The vascular anatomy was evaluated in a technique similar to that of Arnoczky and Warren. 5 The popliteal artery was cannulated 10 cm proximal to the knee joint using a 14-gauge angiocatheter. The vessels branching from the popliteal artery were clamped 10 cm distal to the knee joint, and 120 mL of Higgins Black Magic India Ink (Chartpak Inc) was injected into the popliteal artery under manual pressure. The knees were then placed into full extension and frozen at −10°C for 3 days.
In 3 specimens, a band saw was used to section the frozen knee specimens into 5–mm thick coronal plane sections. The remaining 10 specimens were thawed, and the menisci were dissected en bloc, preserving the root attachments. The vascular synovial fringe (Figure 1) was measured with a Vernier caliper (reading error, 0.02 mm; Fowler High Precision). Next, all specimens were scrubbed clean under cold running water, fixed with 10% neutral-buffered formalin for 3 days, and transferred to 10% nitric acid for decalcification. Specimens were then dehydrated using 3 changes of ethanol (70%, 95%, 100%) for 2 days each and defatted in chloroform for 2 more days. Finally, specimens were cleared through a 24-hour incubation in Spalteholz solution (3:5 benzyl benzoate:methyl salicylate). In the 10 en bloc meniscal specimens, the medial and lateral menisci were divided into 3 radial locations according to the International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine (ISAKOS) classification 4 : anterior horn, midbody, and posterior horn. Menisci were cut into 3–mm thick cross sections, yielding 82 to 99 data points per meniscal radial location. A Vernier caliper (reading error, 0.05 mm) was used to measure the width of each meniscal segment from outer- to innermost substance, not including perimeniscal tissue. Vessel penetration was measured from outermost portion of the meniscus to the longest penetrating intrasubstance vessel visible. Measurements were made to the 0.1-mm level and recorded as a percentage of the width of the segment. Meniscal samples were photographed under illumination via an x-ray film light box using a high-resolution digital single lens reflex camera (Nikon).
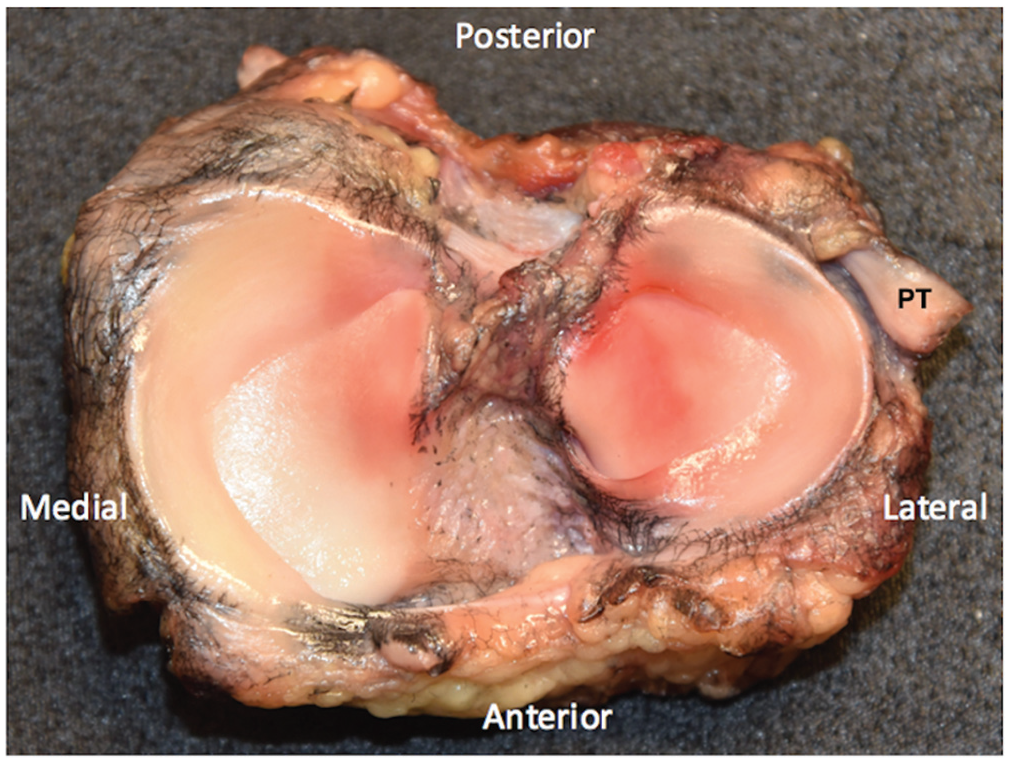
Gross meniscal specimen after injection with India ink and dissection (anterior and posterior cruciate ligaments have been removed). Note the vascular synovial fringe most prominent at the anterior and posterior horns. PT, popliteus tendon.
mRNA Isolation and Quantitative Real-time Polymerase Chain Reaction
Thirteen fresh-frozen meniscal allografts were obtained from commercial vendors (n = 6 from RTI Surgical Inc, n = 7 from JRF Ortho) from donors ranging in age from 17 to 43 years (mean, 27.2 years). Allografts were divided into 3 circumferential zones (0 to <3 mm, 3 to <5 mm, ≥5 mm) based on the ISAKOS classification of meniscal tears. 4 They were then subdivided into radial locations (anterior horn, midbody, posterior horn), again following the ISAKOS classification. Meniscal tissue from these regions was then homogenized in 1000 µL of TRIzol Reagent (15596026; Thermo Fisher) using the Ultra-Turrax IKA-T10 Basic. mRNA was isolated according to standard TRIzol user guidelines, and cDNA was reverse transcribed using qScript (48035; Quantabio). Quantitative real-time polymerase chain reaction was performed to measure intrinsic gene expression for the following genes: collagen 1 (COL1), collagen 2 (COL2), VEGF, and vascular endothelial growth factor receptor 1 (FLT1). COL1 and COL2 were chosen given their role in making collagen type I and type II, respectively. VEGF was used for its importance in promoting angiogenesis, and its receptor, FLT1, was chosen to understand if there may be a differential VEGF responsive element that could play a role in recovery after injury. Real-time polymerase chain reaction was performed using the perfeCTa SYBER Green Supermix (84018; Invitrogen) and 1 µg of cDNA mixed with the primers specific to COL1, COL2, VEGF, or FLT1 (Appendix Table A1, available in the online version of this article). Relative gene expression was calculated by first normalizing the genes of interest (COL1, COL2, VEGF, FLT1) to the structural RNA housekeeping gene 18s (ΔCT), which has been found to have the most stable expression in chondrocytes, to account for the potentially different number of cells within each sample.1,27 Fold change in gene expression was calculated using 2−ΔCT.
Statistical Analysis
Significance was determined using repeated measures analysis of variance and Tukey multiple-comparison test for multiple groups, with P < .05 considered significant (Prism 8; GraphPad). Outliers were determined in the vessel depth specimens using standard correction of 1.5 multiplied by the interquartile range added to or subtracted from the 75th percentile or 25th percentile, respectively.
Results
Microvascular Anatomy
A vascular synovial fringe extended over the femoral and tibial surfaces of the medial and lateral menisci; however, it did not contribute any vessels into the meniscal stroma (Figure 1). The extent of vascular synovial fringe varied by specimen but was most robust at the anterior horn. The vascular synovial fringe covered up to 100% of the femoral surface width and 50% of the tibial surface width of the anterior horns of medial and lateral menisci. The vascular synovial fringe overlying the posterior horn covered up to 40% of the femoral and tibial lateral meniscal surface width and 25% of the femoral and tibial medial meniscal surface width. The vascular synovial fringe extended 1 to 2 mm on both meniscal surfaces in the region of medial and lateral meniscal midbody. There was an absence of synovial fringe in the region of the popliteal hiatus.
After the specimens were cleared in the Spalteholz solution, a rich perimeniscal capillary plexus was identified (Figure 2). Radial branches from this capillary plexus penetrated the substance of the medial and lateral menisci (Figures 3 and 4).
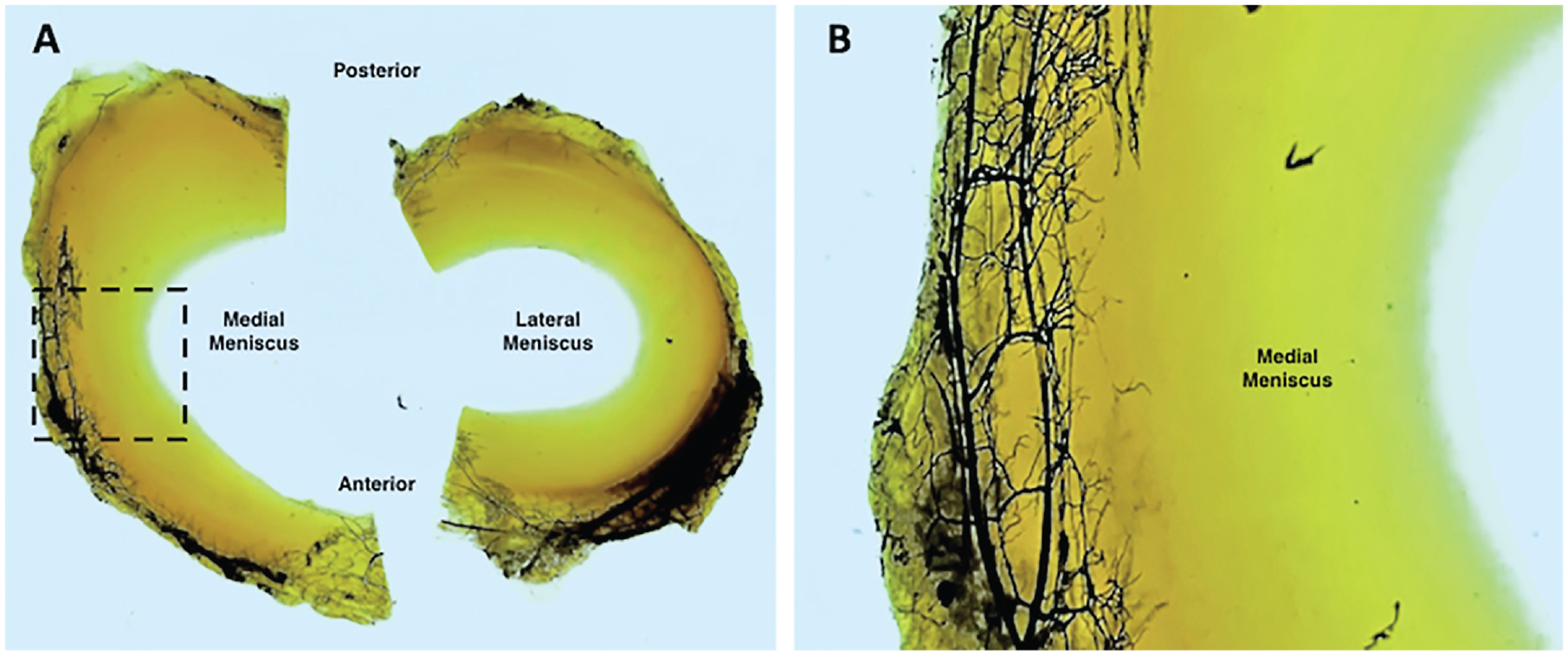
(A) Medial and lateral menisci after clearing in Spalteholz solution with the tibial bone block removed. (B) Close-up view of the medial meniscus demonstrates the rich perimeniscal capillary plexus.
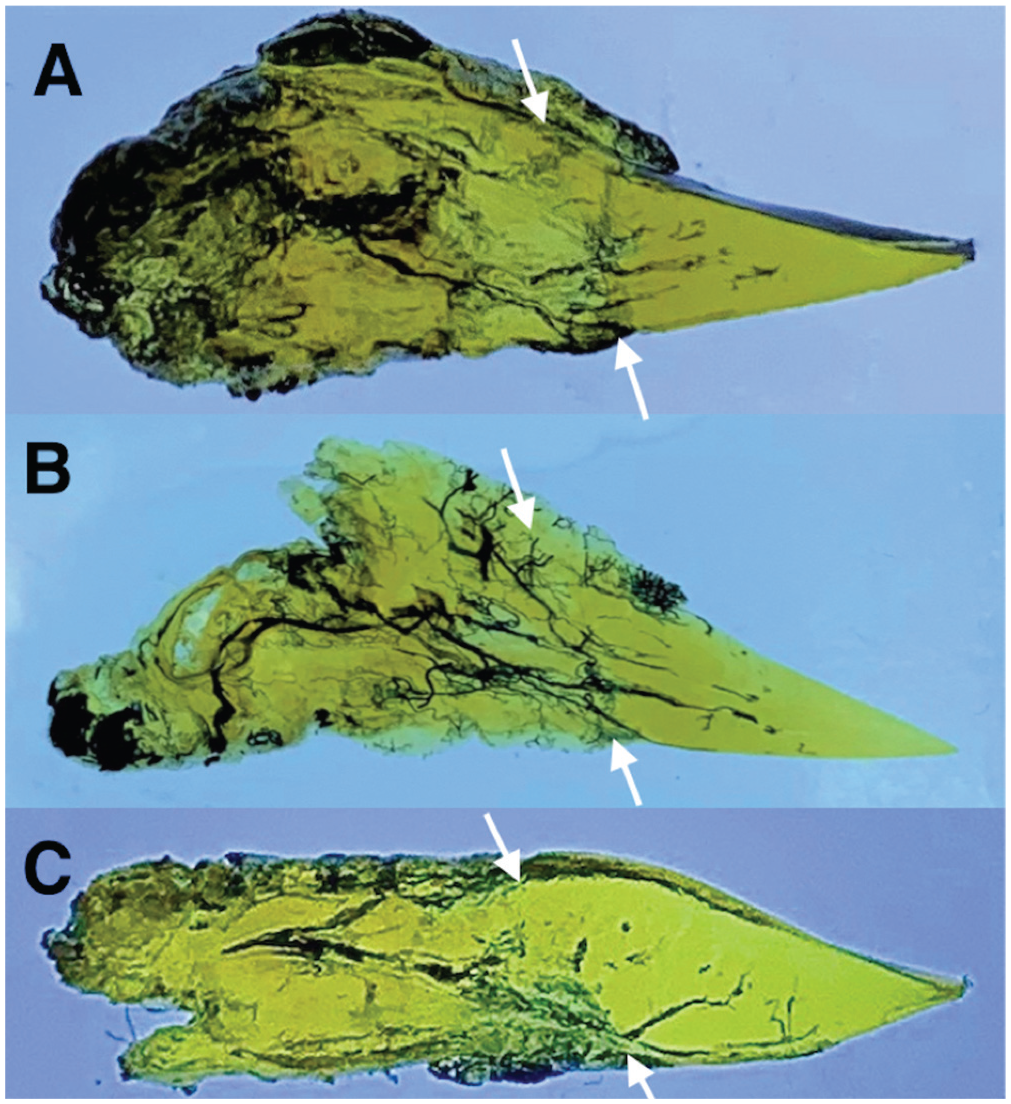
Cross-sectional 3-mm cut of the meniscus demonstrates rich perimeniscal vascularity and radial vessel penetration into the (A) lateral anterior horn, (B) medial midbody, and (C) lateral posterior horn. Arrows indicate the meniscocapsular junction.
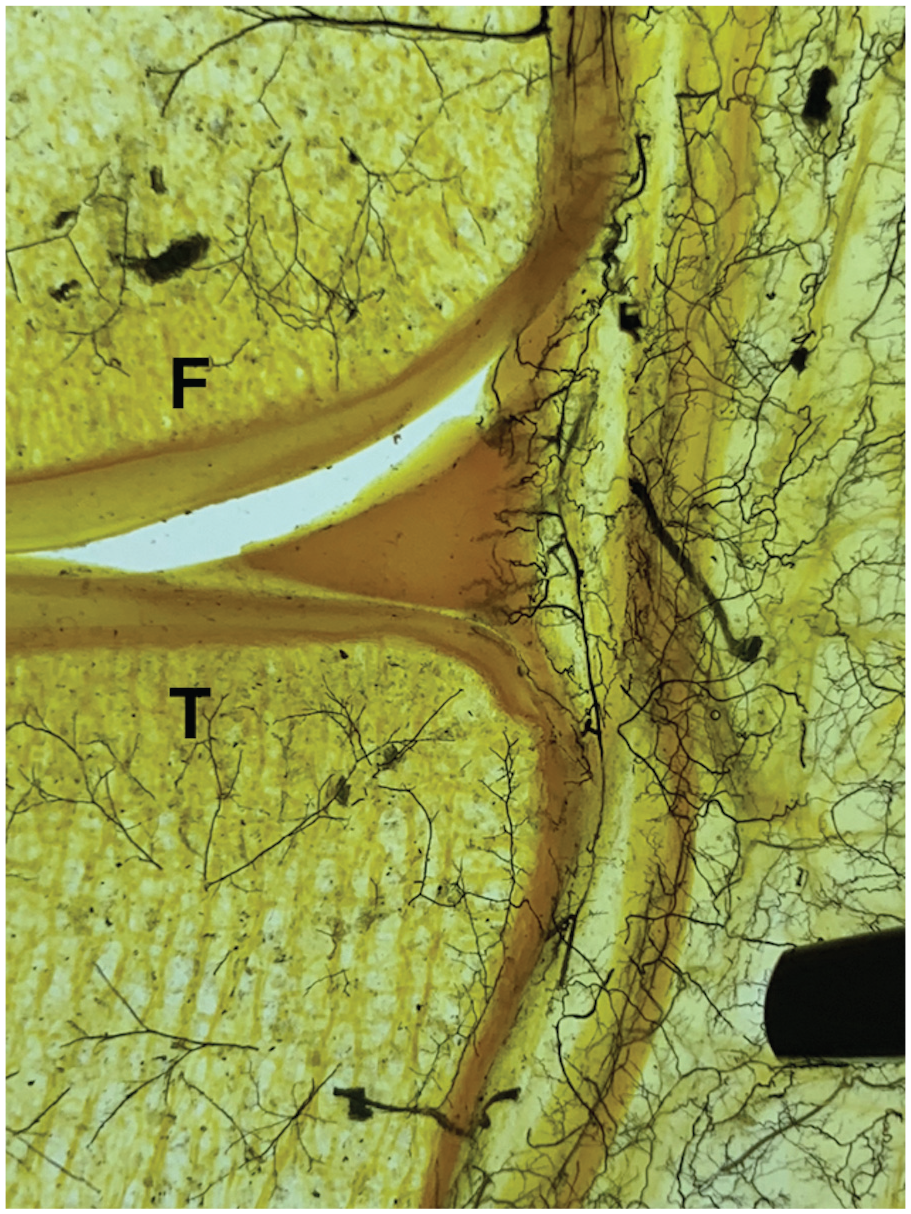
Coronal view of the lateral compartment. Radial vessels penetrate from the perimeniscal capillary plexus into the peripheral lateral meniscus. F, femur; T, tibia.
Measurement of the depth of meniscal vascular penetration is reported in Figure 5. There was a wide range of vascular penetration across all meniscal samples, including many with no penetration. The degree of vascular penetration into the periphery of the medial meniscus ranged from 0% to 42%. The posterior horn of the medial meniscus exhibited the least depth of penetration (median, 8.7%), which was significant in comparison with that of the anterior horn (median, 17.4%; P < .0001) and midbody (median, 17.5%; P = .0003) of the medial meniscus. The degree of vascular penetration into the periphery of the lateral meniscus ranged from 0% to 48%. There were no significant differences in the depth of vascular penetration among the different radial locations within the lateral meniscus (median: anterior horn, 13.5%; midbody, 13.3%; posterior horn, 13.2%). Also, there was no correlation between the depth of vascular penetration and sex or race.
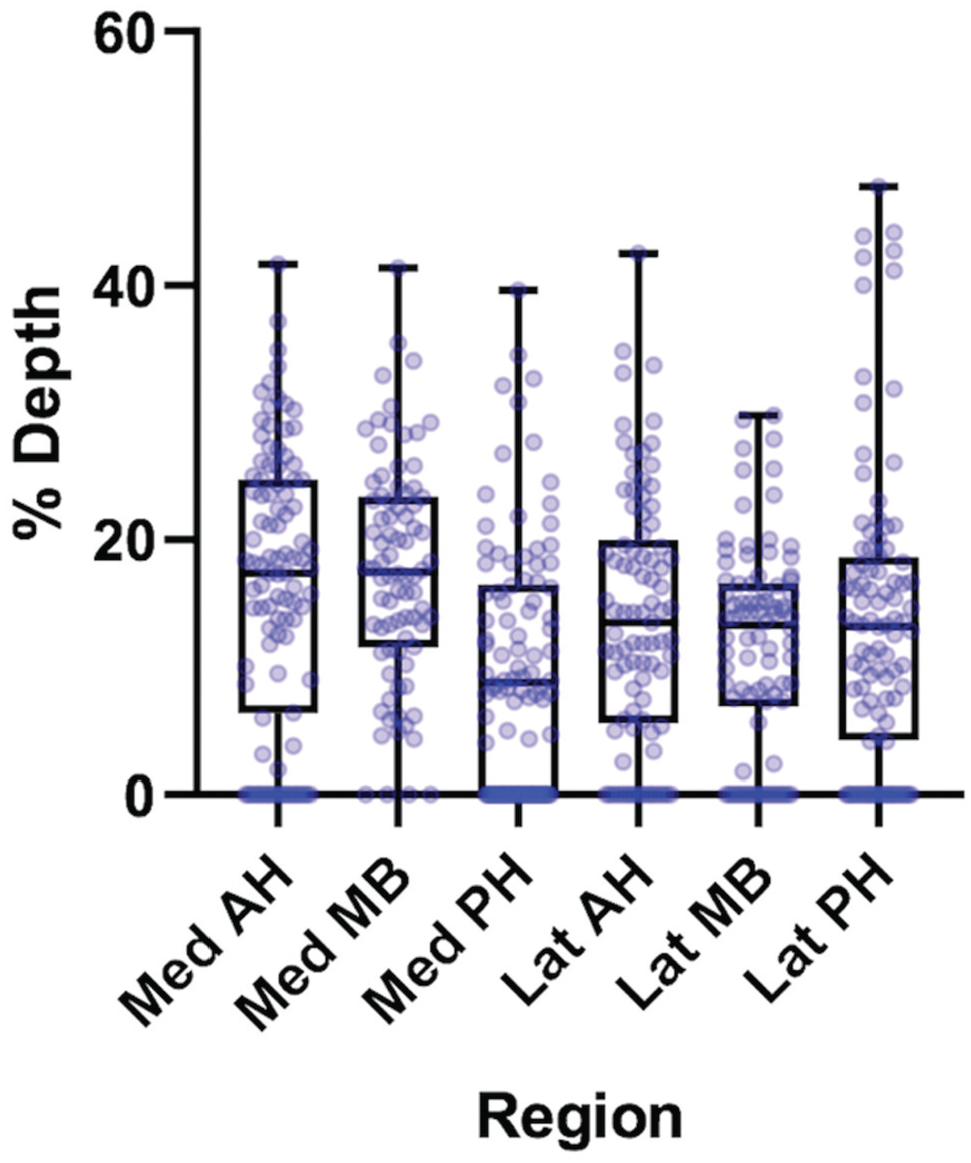
Depth of vascular penetration by meniscal radial location. Each dot represents 1 value, with 82 to 99 data points per radial location. The box represents the 25th to 75th percentiles, with the median noted by the center line inside the box. Whiskers extend from the minimum to maximum values. Darker clusters represent a larger number of specimens. Note that the dark lines clustered at 0% represent multiple segments that did not demonstrate any vessel penetration. Correlation of measured millimeter depth of vascular penetration for the 25th to 75th percentiles is as follows: Med AH, 0.93-2.42; Med MB, 2.03-3.11; Med PH, 0.65-1.87; Lat AH, 0.93-1.85; Lat MB, 0.74-2.42; Lat PH, 0.76-2.05. AH, anterior horn; Lat, lateral; Med, medial; MB, midbody; PH, posterior horn.
Quantitative Real-Time Polymerase Chain Reaction
VEGF and FLT1 gene expression was low in all radial and circumferential zones of the medial and lateral menisci. The anterior horn, midbody, and posterior horns of the medial and lateral menisci did not reveal significant differences in gene expression among circumferential zones (0 to <3 mm, 3 to <5 mm, or ≥5 mm) as determined by repeated-measures analysis of variance (COL1, P = .4121; COL2, P = .3772; VEGF, P = .2490; FLT1, P = .1918). Samples from each radial location within the medial and lateral menisci were then combined, and gene expression was again compared for each circumferential zone. Again, no significance was found between any circumferential zones of the meniscus for any gene (COL1, P = .0744; COL2, P = .2393; VEGF, P = .6738; FLT1, P = .1140) (Figure 6).
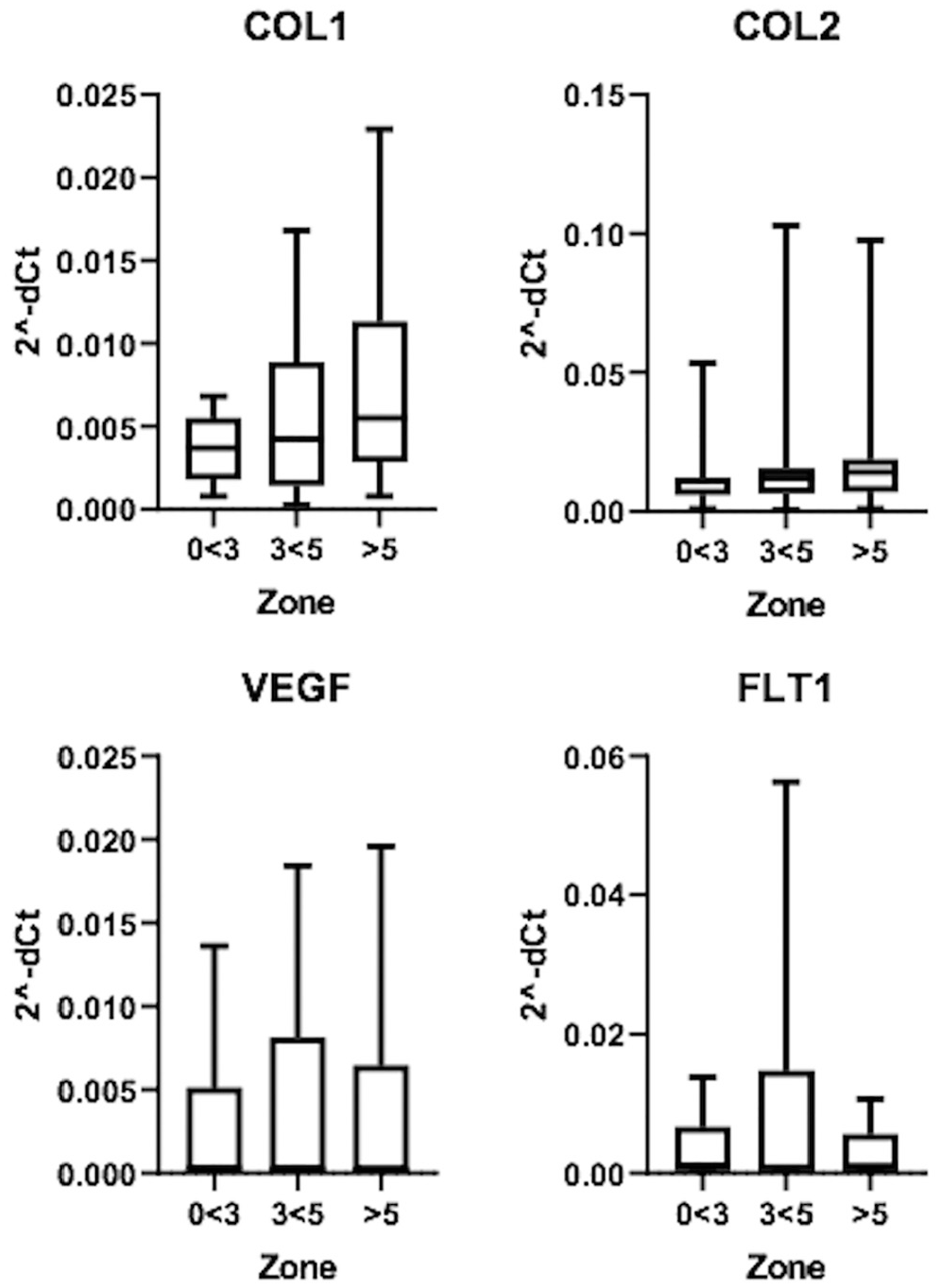
Gene expression patterns from each circumferential zone (0 to <3 mm, 3 to <5 mm, and >5 mm) of the meniscus as determined by polymerase chain reaction. Boxes represent 25th to 75th percentiles, with the median values noted by a line inside the boxes, and whiskers range from the 5th to 95th percentiles. The expression pattern is represented as relative to an internal housekeeping gene (18S) for each specimen. No significant findings were found between any zones for any gene. COL1 and COL2, collagen 1 and 2; FLT1, vascular endothelial growth factor receptor 1; VEGF, vascular endothelial growth factor.
Discussion
The main finding of this study was that the maximal depth of vascular penetration into the periphery of the medial and lateral menisci in cadaveric specimens with an average age of 28.5 years ranged from 0% to 42% and 0% to 48%, respectively. There was variation in the degree of vascular penetration within the medial meniscus, with the posterior horn having a significantly smaller depth of penetration (median, 8.7%) than that of the anterior horn (median, 17.4%) or midbody (median, 17.5%). There were no significant differences in the degree of vascular penetration within radial zones of the lateral meniscus. Angiogenesis gene expression (VEGF/FLT1) showed no significant differences, with low gene expression throughout all circumferential meniscal zones in an allograft cohort with an average age of 27.2 years.
The degree of vascular penetration (medial meniscus: range, 0%-42%; lateral meniscus: range, 0%-48%) in these specimens with an average age of 28.5 years exceeds what was previously published by Arnoczky and Warren 5 ; however, the median values of vascular depth within different radial locations of the menisci are consistent with that work. Arnoczky and Warren’s classic article on the microvascular anatomy of the human menisci described a perimeniscal capillary plexus supplying the peripheral 10% to 30% of the medial meniscus and 10% to 25% of the lateral meniscus. This provided an anatomic foundation to approach meniscal repair and is the origin of the “red-red,”“red-white,” and “white-white” terminology depicting the perceived appearance of blood supply within the meniscus.
The similarity in meniscal vascular penetration between the young specimens in this study (age range, 22-34 years) and Arnoczky and Warren’s 5 older specimens (age range, 53-94 years) is consistent with clinical findings of age-independent meniscal healing. Meniscal vascular supply is an important consideration when determining treatment of meniscal tears. Several clinical studies and systematic reviews have reported on the efficacy of meniscal repair, especially in the red-white zone of the meniscus. Although measures to validate meniscal healing have varied (magnetic resonance imaging, patient-reported outcome measures, repeat arthroscopy), these studies found acceptable clinical healing rates.7,11,25,30 The greatest identified positive predictor of healing is a narrow peripheral meniscal rim (range, 0-2 mm). 33 With respect to the effects of age on the meniscus, biomechanical and biochemical studies have shown that tensile properties and collagen content are not age-dependent in meniscal allografts <45 years of age. 9 Furthermore, several clinical studies have indicated that meniscal repair can be equally as effective in patients >40 years old as compared with younger cohorts.14,29,36
An advantage of this study was that it provided a thorough quantitative assessment of vascular penetration, with up to 99 vascular measurements per meniscal radial location. A significantly smaller depth of vascular penetration into the posterior horn of the medial meniscus was found in comparison with that into the anterior horn and midbody. This relative lack of vascularity in combination with a number of other factors (increased weightbearing load, role as a secondary stabilizer to anterior tibial translation) may in part be responsible for the high prevalence of degenerative tears in this location. These measurements also provide clinical relevance and can assist with decision making at the time of arthroscopy. The majority of meniscal vascular penetration occurred within the peripheral 2 mm; however, it extended farthest in the midbody, with 75th-percentile vascular penetration measuring 3.11 mm in the medial meniscus and 2.42 mm in the lateral.
In addition to the extrinsic blood supply, the intrinsic ability of the meniscus to produce a healing response is critical to meniscal repair. In this study, gene expression for the angiogenic markers VEGF and FLT1 did not differ according to the radial or circumferential location of the meniscus. These results are consistent with those of Lu et al, 20 who found a lack of VEGF mRNA expression in the uninjured central and peripheral zones of menisci aged 69 to 78 years. Injury to the meniscus, however, resulted in increased VEGF expression that was most pronounced in the peripheral zone of the meniscus. The ability for the meniscus to upregulate angiogenic growth factors has been supported in animal models, where increased VEGF expression has been seen after meniscal injury in rabbits.8,31
These studies highlight the dynamic response to injury and intrinsic regenerative potential of meniscal tissue, which may be as or more important than extrinsic blood supply in meniscus healing. Animal and human studies have shown that this intrinsic healing potential is more robust in the peripheral zone than the central zone. In a rabbit model, Kobayashi et al 19 demonstrated improved healing after transplantation of peripheral meniscus into an avascular central meniscal defect. Osawa et al 26 showed a higher supply of vascular-derived stem cells (CD-34, CD-146) in the peripheral zone of fetal and adult menisci in comparison with that in the central zone. The contribution of vascular synovial tissue to meniscal healing is also well-documented. Arnoczky and Warren 6 showed healing of avascular meniscal tears when connected to the peripheral synovium in dogs, and Nakagawa et al 23 showed that transplantation of synovial mesenchymal stem cells into avascular meniscal tears improved healing in pigs. Clinically, Henning et al 17 demonstrated improved healing rates in meniscal tears with peripheral rims up to 5 mm after parameniscal synovial abrasion.
The findings of this study provide weak support of our hypothesis that vascularity in young specimens extends beyond the peripheral 25% to 30% of the meniscus. While vascularity penetrated up to 42% and 48% of the medial and lateral meniscal width, respectively, median values were within the range proposed in Arnoczky and Warren’s work. 5 With reports indicating strong clinical healing rates in relatively avascular meniscal tears, these findings suggest that the intrinsic nature of meniscal tissue may be more important to healing than is its extrinsic vascularity. Further investigation should focus on the in vivo meniscal environment and build on currently published work to study how meniscal injury stimulates a healing cascade of stem cells, growth factors, and cytokines; the role of synovial fluid; and the potential differences in healing response based on meniscal location as well as patient age.
A limitation of this study was that only 13 cadavers were used for India ink staining, given the difficulty of procuring specimens <35 years old. Additionally, this was an ex vivo study, which limited our ability to make conclusions about the dynamic interplay required in meniscal regeneration and healing.
Conclusion
The vascular supply of the medial and lateral menisci in specimens from young adults <35 years of age extended farther than what was reported in specimens from older individuals; however, median values remained consistent. Gene expression of the angiogenic marker VEGF was low throughout all regions of uninjured menisci from young adults, which is consistent with reports in older specimens.
Supplemental Material
DS_10.1177_0363546520961555 – Supplemental material for Microvascular Anatomy and Intrinsic Gene Expression of Menisci From Young Adults
Supplemental material, DS_10.1177_0363546520961555 for Microvascular Anatomy and Intrinsic Gene Expression of Menisci From Young Adults by Matthew D. Crawford, Justin E. Hellwinkel, Zachary Aman, Ramesses Akamefula, J. Thomas Singleton, Chelsea Bahney and Robert F. LaPrade in The American Journal of Sports Medicine
Footnotes
Acknowledgements
The authors thank Dr Steven Arnoczky for his review of and recommendations for this article.
Submitted May 1, 2020; accepted June 18, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: R.F.L. has received royalties from Arthrex and Smith & Nephew; is a paid consultant for Arthrex, Ossur, and Smith & Nephew; and receives research support from Arthrex, Linvatec, Ossur, and Smith & Nephew. M.D.C. has received food and beverage from Lilly USA LLC, Sanofi-Aventis US LLC, SI-Bone Inc, Stryker Corp, Allergen Inc, Amgen Inc, Bioventus LLC, DePuy Synthes Sales Inc, Ferring Pharmaceuticals Inc, Haylard Health Inc, Horizon Pharma PLC, and Vertical Pharmaceuticals LLC. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.