
Abstract
Background:
The pivot-shift test is used to assess for rotatory knee laxity in the anterior cruciate ligament (ACL)-deficient knee and ACL-reconstructed knee; however, the pivot shift uses a subjective grading system that is limited by variability between examiners. Consequently, quantified pivot shift (QPS) test software (PIVOT iPad application) has been developed and validated to measure the magnitude of rotatory knee laxity during the positive pivot-shift test.
Purpose:
To employ intraoperative QPS (iQPS) to assess for differences in residual rotatory knee laxity after ACL reconstruction (ACLR) versus ACLR augmented with lateral extra-articular tenodesis (ACLR + LET), and to employ iQPS to determine if ACLR and/or ACLR + LET result in overconstrained knee kinematics when compared with the contralateral knee.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
iQPS was performed in 20 patients by a single surgeon on both the operative and contralateral knees before ACLR. ACLR was augmented with a LET if the lateral compartment tibial translation measured during QPS was greater than or equal to double the amount of lateral tibial compartment translation measured for the contralateral knee. After each reconstruction (ACLR or ACLR + LET), iQPS measurements were performed. iQPS data were compared with the preoperative QPS measurements of the operative and contralateral knees. Postoperative iQPS data were compared with both the preoperative QPS measurements of the operative and contralateral knees with paired samples t tests. Categorical variables were compared using the Fisher exact test.
Results:
The mean age in the cohort was 17.3 years (range, 15-24 years). There were no significant differences between the groups in terms of the proportion of male patients (ACLR: 5 male, 5 female vs ACLR + LET: 4 male, 6 female) or age (ACLR: 17.7 ± 3.3 years; 95% CI, 15.4-24.0 vs ACLR + LET: 16.8 ± 2.8 years, 95% CI, 14.8-22.0; P = .999). There were no significant differences between the groups with respect to preoperative QPS performed during examination under anesthesia (ACLR: 4.7 ± 2.0 mm; 95% CI, 3.3-6.1 vs ACLR + LET: 3.6 ± 1.8 mm; 95% CI, 2.3-4.9; P = .2). Both ACLR and ACLR + LET resulted in significant decreases in rotatory knee laxity when compared with preoperative QPS measurements (ACLR: –3.4 ± 1.7 mm; 95% CI, −4.6 to −2.2; P < .001: ACLR + LET: –2.6 ± 1.9 mm; 95% CI, −3.9 to −1.3; P < .002). Moreover, when compared with isolated ACLR, ACLR + LET did not result in a significantly smaller magnitude of change in iQPS between the pre- and postoperative states (P = .3).
Conclusion:
Both ACLR and ACLR + LET resulted in significant decreases in rotatory knee laxity. The augmentation of ACLR with LET did not change the constraint of the knee with respect to lateral compartment translation as measured during iQPS.
Keywords
Injuries to the anterior cruciate ligament (ACL) result in both anterior tibial translation and rotatory knee laxity, and persistent rotatory knee instability is oftentimes a multifactorial phenomenon that has been implicated in diminished clinical outcomes after ACL reconstruction (ACLR).4,20 In particular, injuries to the anterolateral complex may predispose patients to persistent rotatory knee instability even in the setting of successful anatomic single-bundle (SB) ACLR.31,36 Consequently, a series of lateral extra-articular augmentation procedures (ie, anterolateral ligament reconstruction, and lateral extra-articular tenodesis [LET]) have been described to ameliorate persistent rotatory knee laxity and protect the intra-articular ACL graft during remodeling and healing.1,8,9,38 While a recent clinical study demonstrated that the addition of LET to hamstring tendon autograft ACLR may result in significant reductions in graft rupture and persistent rotatory knee laxity, there is a relative paucity of information demonstrating that augmentation of ACLR with LET definitively affects clinical outcomes. 14 In fact, those advocating one technique over another have done so based upon the results of biomechanical studies, which are fraught with limitations.2,7,12,30 Moreover, concerns persist regarding the possibility that LET may overconstrain native knee kinematics, which may significantly reduce internal rotatory movement relative to the native knee joint and contribute to the development of premature osteoarthritis.12,33,36 To date, there have only been limited descriptions of methods for assessing the time-zero, in vivo effect, if any, of particular surgical interventions on rotatory knee laxity. Furthermore, these methods can be difficult and/or invasive to implement in routine clinical practice.21,29,40
The pivot-shift test is a dynamic assessment of the rotational laxity observed in the setting of an ACL rupture. While the grade of the pivot-shift test has been associated with clinical instability symptoms, considerable variations in interobserver reliability have been reported, and the diagnostic accuracy of the test remains somewhat limited. Authors have observed a pooled sensitivity and specificity of 24% and 98%, respectively, in a meta-analysis of 28 studies pertaining to clinical tests used to detect ACL insufficiency.6,33 In light of these limitations, multiple modalities have been developed to quantify the “feel” of the pivot shift. The PIVOT iPad application is one such innovation, and this modality has been validated as a means to determine the amount of lateral compartment tibial translation and shown to be highly accurate and reliable between single and multiple examiners.17,31 Using the contralateral knee as an internal control, the quantified pivot shift (QPS) can be performed in an office setting as part of both pre- and postoperative assessments as well as during an examination under anesthesia (EUA). 25 Recently, the QPS has been modified using sterilized materials to perform as an intraoperative QPS (iQPS), affording the opportunity for the examiner to obtain a time-zero, in vivo measurement of rotatory knee laxity either before or after commonly performed surgical procedures. It is entirely possible that these data may facilitate comparative studies, the results of which could clarify the indications for LET based on the residual amount of rotatory knee laxity present after ACLR.
Therefore, the purposes of this study were to report on the use of iQPS using the PIVOT iPad application to (1) determine if ACLR and/or ACLR + LET result in overconstrained knee kinematics when compared with the contralateral knee; and (2) assess for differences in residual rotatory knee laxity after ACLR versus ACLR + LET. It was hypothesized that neither procedure would lead to significantly overconstrained knee kinematics when compared with the uninjured, contralateral knee. It was further hypothesized that ACLR + LET would result in a greater reduction in rotatory knee laxity when compared with ACLR in isolation.
Methods
Institutional review board approval was obtained before the commencement of this investigation. During EUA, QPS was performed on both the operative and the nonoperative knees before ACLR by the senior surgeon (V.M.). Three yellow three-quarter-inch markers were attached to the skin overlying bony landmarks: (1) lateral epicondyle, (2) Gerdy tubercle, and (3) 3 cm posterior to Gerdy tubercle. The PIVOT iPAD application was employed to measure lateral compartment translation during the pivot-shift test. Briefly, this application uses a frame-by-frame analysis to measure the translation of the tibial markers relative to the femoral markers, which is used to construct a reduction curve and provide a precise measurement of lateral compartment tibial translation (Figure 1). Previous studies have demonstrated this modality to be highly accurate, strongly correlated with 3-dimensional (3-D) osseous motion through the pivot-shift maneuver, and reliable between examinations and across multiple examiners.3,17,31
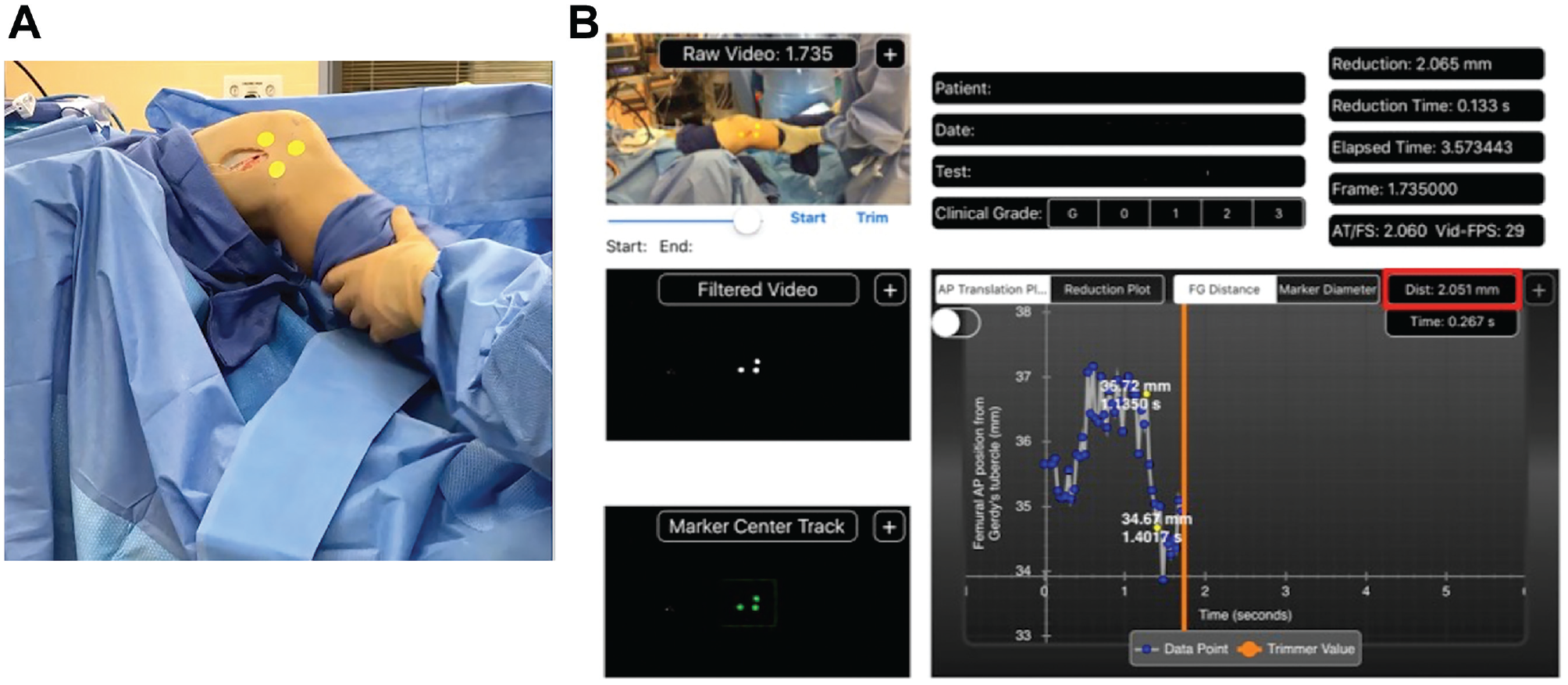
(A) QPS testing setup intraoperative QPS testing setup (right knee) with sterilized skin markers once again placed on 3 predetermined anatomic reference points, and (B) iPad PIVOT interface. A frame-by-frame analysis is performed to measure the translation of the tibial markers relative to the femoral markers, which is used to construct a reduction curve and provide a precise measurement of lateral compartment tibial translation. The x-axis represents the anteroposterior distance (mm) of the femur to Gerdy tubercle, and the y-axis represents time (s). QPS, quantitative pivot shift.
To assess feasibility of performing iQPS under sterile conditions, the senior author (V.M.) performed 10 anatomic ACLRs using either a bone–patellar tendon–bone (n = 8) autograft or an all–soft tissue quadriceps tendon autograft (n = 2) among patients aged 15 to 24 years with isolated, complete ACL injuries. Patients with multiligamentous knee injuries were excluded from the analysis. All femoral tunnels were independently drilled via a medial portal through the anatomic center of ACL. All bone–patellar tendon–bone grafts were secured on the femur with either a fixed-loop suspensory button or interference screw and an on the tibia with an interference screw, whereas quadriceps tendon grafts were secured with a fixed-loop suspensory button on the femur and an interference screw in the tibia. All meniscal repairs were performed in an all-inside fashion. After completion of each ACLR, iQPS was performed using sterilized yellow three-quarter-inch markers applied on the predetermined points as previously described. Lateral compartment translations during the pivot-shift test were again measured and recorded (Figure 1).
Ten ACLRs were then performed by the same senior surgeon with either bone–patellar tendon–bone (n = 7) or quadriceps tendon autografts (n = 3) in a comparably aged cohort of patients aged 15 to 24 years and subsequently augmented with a LET. Once again, only patients with isolated, complete ACL injuries were included, while patients with multiligamentous knee injuries were excluded from the study. However, this time, the decision to augment the ACLR with LET was made after EUA and iQPS measurements of both the operative and contralateral knees were obtained. An ACLR was augmented with LET if the lateral compartment translation of the operative knee was greater than or equal to twice the lateral compartment translation of the uninjured, contralateral knee according to the iQPS. The rationale of this decision making was based upon the facts that (1) greater magnitudes of lateral tibial translation as measured during the QPS most likely occur on a continuum (partial vs complete ACL injuries) and (2) lateral tibial translation in the setting of failed primary ACLR have recently been observed to be twice that measured in primary ACL injuries. 23 Additionally, the contralateral, uninjured knee was used to obtain a baseline measurement of lateral compartment translation given that patient-specific variations in osseous morphologies have previously been observed to be associated with higher grades of rotatory knee laxity.23,34,35 The LET was performed as a modified Lemaire procedure. A 6-cm curvilinear incision was made slightly posterior to the lateral epicondyle of the distal femur. The Gerdy tubercle was identified by direct palpation, and a 1 cm–wide and 8 cm–long strip of the central one-third of the iliotibial band (ITB) was harvested proximally such that the distal insertion was left intact on the Gerdy tubercle. The free end of the ITB was whipstitched. The fibular collateral ligament (FCL) was then identified and the free strip of ITB was passed deep to the FCL ligament in a distal-to-proximal fashion. The lateral femoral supracondylar area was then identified by direct palpation proximal to the lateral head of the gastrocnemius. The periosteum was dissected off of the distal femur, and the ITB strip was held under tension and fixed to the “over-the-top” position on the lateral femoral condyle, proximal and posterior to the FCL, with a metal staple with the knee held in 60° of flexion and neutral rotation (Figure 2). 28 During fixation, care was taken to avoid putting undue tension on the ITB graft whipstitch ends given the fact that previous biomechanical studies have suggested that tension >20 N may overconstrain knee kinematics. 13
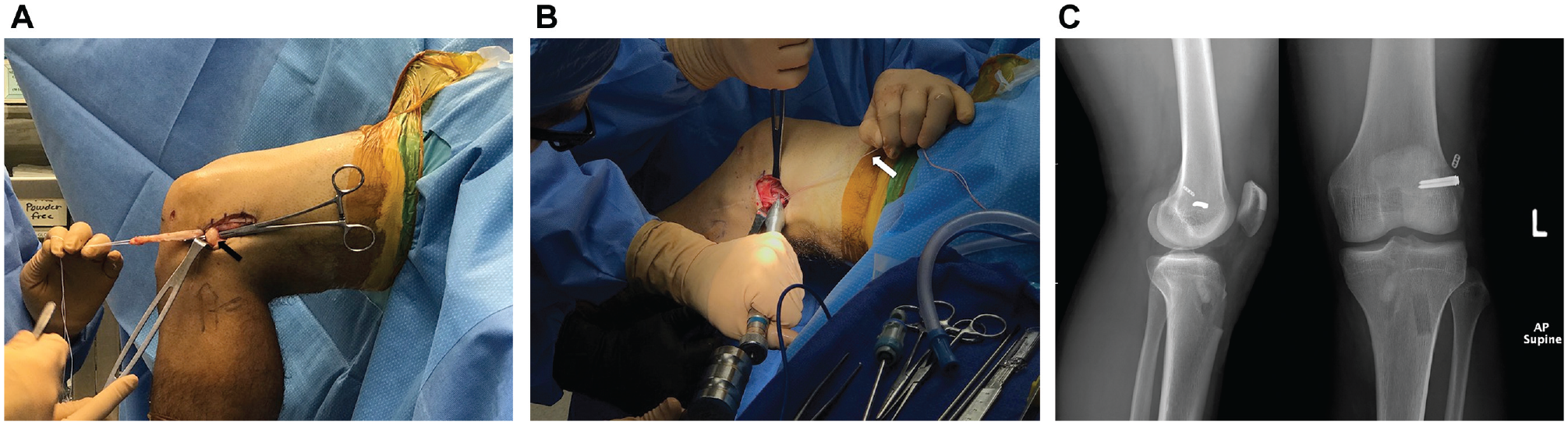
Intraoperative photograph demonstrating lateral extra-articular tenodesis technique. (A) The central 10 mm of the ITB has been incised, truncated proximally, and whipstitched in preparation for shutting under the fibular collateral ligament (black arrow). (B) The ITB is fixed to the distal femur in the vicinity of the Kaplan fibers with the knee flexed to 60°, in neutral rotation, and with manual tension pulled on the whipstitch (white arrow.) (C) Postoperative anteroposterior (AP) and lateral radiographs demonstrate staple fixation of the ITB to the distal femur. ITB, iliotibial band.
The ITB graft was then sutured back on itself and the ITB was left open to avoid overtightening the lateral retinaculum. 39 In select cases, ACL tears were found in conjunction with meniscal pathology, which were either debrided or repaired with an all-inside repair technique at the discretion of the senior surgeon. Data were analyzed using SPSS software Version 23 (IBM Corporation). The groups were examined for differences in sex, age, and the presence of concomitant meniscal pathology using Fisher exact tests and t test (Table 1). Independent, between-group (ACLR vs ACLR + LET) comparisons using t tests were performed on the contralateral knee QPS, preoperative QPS, postoperative QPS, the QPS difference preoperatively to postoperatively, and the QPS difference postoperatively to the contralateral knee (Table 2). An additional within-group test using the paired t test was performed to examine the ability to restore the postoperative QPS to similar levels to the contralateral knee. A sample size estimate was performed using QPS data established from a database of 178 previously performed ACLRs at our institution. 24 It was assumed that ACLR would restore the QPS to the level of the contralateral knee, and therefore an effect size of 1.2 was calculated using QPS measurements from this data set. Thus, it was determined that 8 patients in each group would be required to achieve 80% power with an effect size of 1.2 and an alpha level of .05 in detecting significant differences in rotatory knee laxity between groups.
Patient Characteristics for Groups Undergoing ACL and ACLR With LET a
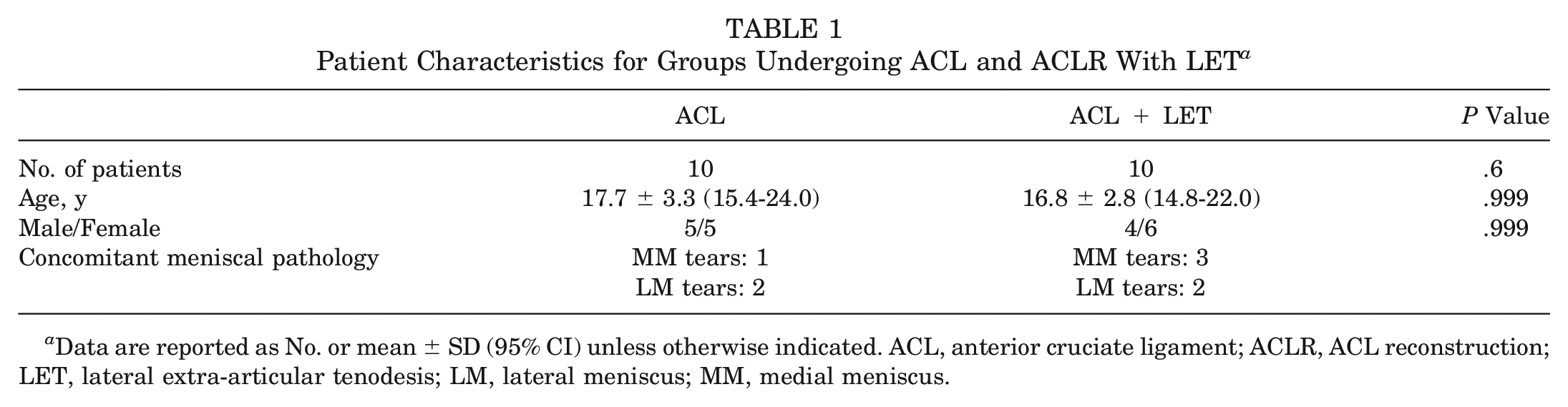
Data are reported as No. or mean ± SD (95% CI) unless otherwise indicated. ACL, anterior cruciate ligament; ACLR, ACL reconstruction; LET, lateral extra-articular tenodesis; LM, lateral meniscus; MM, medial meniscus.
Comparison of Measurements of iQPS Between Groups a
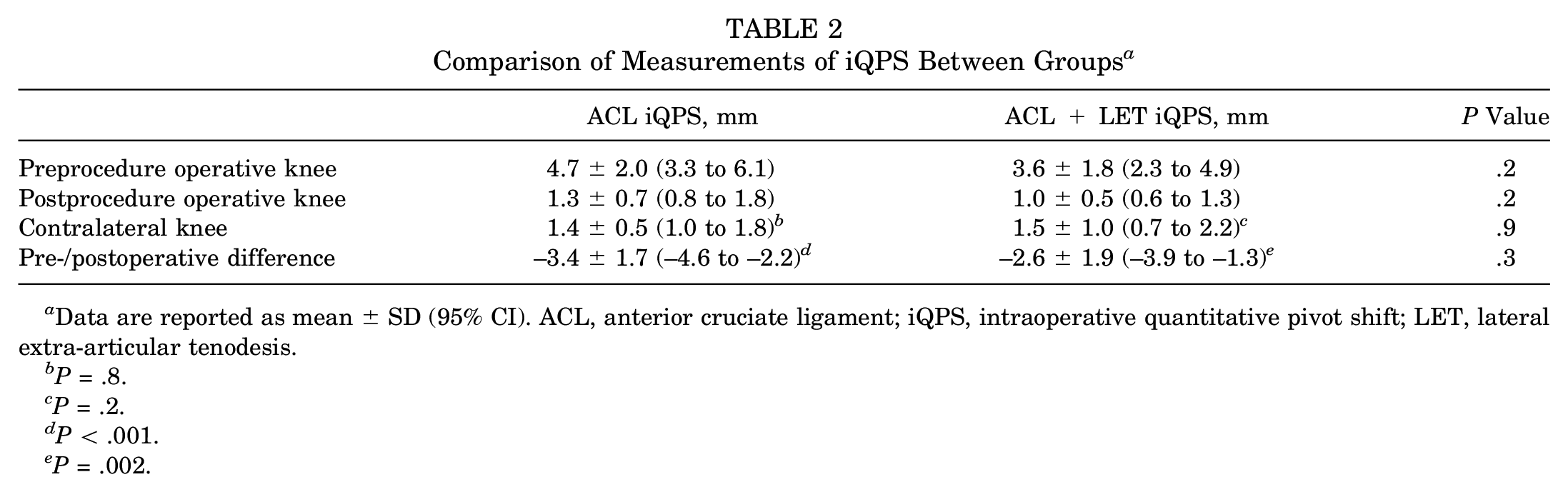
Data are reported as mean ± SD (95% CI). ACL, anterior cruciate ligament; iQPS, intraoperative quantitative pivot shift; LET, lateral extra-articular tenodesis.
P = .8.
P = .2.
P < .001.
P = .002.
Results
The mean age in the cohort was 17.3 years (range, 15-24 years). There were no significant differences between groups in terms of the proportion of male patients to female patients. Of the 10 ACLRs, concomitant meniscal pathology was identified in 3 patients (1 medial meniscal tear, 2 lateral meniscal tears.) No cases of meniscus root injuries were observed within the cohort. In 2 cases, ACLR was performed in conjunction with a meniscal repair, whereas 1 case involved a partial meniscectomy. Of the 10 ACLR + LET procedures, concomitant meniscal pathology was identified in 5 individuals (3 medial meniscal tears, 2 lateral meniscal tears). In 3 cases, ACLR + LET was performed in conjunction with a meniscal repair, whereas 2 cases involved partial meniscectomy (Table 1).
With respect to the QPS of the contralateral knees between the ACLR and ACLR + LET groups, there were no significant differences in QPS measurements. There were no significant differences between groups with respect to preoperative QPS performed during EUA (Table 2).
Both ACLR and ACLR + LET resulted in significant decreases in lateral compartment translation when compared with preoperative QPS measurements. The addition of LET to ACLR did not result in a significant difference in the magnitude of change in iQPS between the pre- and postoperative states when compared with isolated ACLR. Furthermore, there were no significant differences in lateral compartment translation between the postoperative knees and contralateral knees, suggesting that neither ACLR nor ACLR + LET resulted in overconstrained kinematics (Table 2).
Discussion
The principle finding of the present study was that in comparison with isolated ACLR, the augmentation of ACLR with LET did not significantly affect lateral compartment translation when compared with the contralateral knee. Both ACLR and ACLR + LET were effective in restoring native knee rotatory knee stability relative to the uninjured, contralateral knee. The augmentation of ACLR with LET did not overconstrain rotatory knee motion during the pivot-shift maneuver. Moreover, the augmentation of ACLR with LET did not significantly reduce lateral compartment translation during pivot-shift testing when compared with ACLR performed in isolation. The use of iQPS was feasible and useful in precisely quantifying the amount of lateral compartment tibial translation during the pivot-shift test. The application of this technology in an intraoperative setting represents a substantial innovation in the study of both rotatory knee laxity and the surgical procedures currently employed to treat this complex pathology.
There is conflicting clinical and biomechanical evidence regarding the potential for LET to overconstrain knee kinematics, and these concerns must be balanced against the possibility that LET may have a protective effect on ACLR. Several authors have raised concerns that these procedures may increase the likelihood of secondary injuries to associated structures and/or hasten the progression of osteoarthritis.12,34 However, several other reports, including 1 retrospective review of 140 patients with 25 years’ follow-up and a prospective trial involving 54 patients at 10 to 13 years’ follow-up after combined LET and ACLR did not observe significantly higher rates of osteoarthritis and/or untoward clinical outcomes.10,27 Moreover, a recently published randomized controlled trial comparing hamstring autograft ACLR to ACLR + LET demonstrated significantly reduced rates of graft failure among those patients undergoing ACLR + LET, substantiating the notion that LET may diminish stress across the graft and improve clinical outcomes. 14 These results would seem to corroborate the fact that the addition of LET to ACLR may diminish composite forces across the graft by as much as 43%. 9
Conversely, several biomechanical reports have raised concerns about the possibility of LET resulting in overconstrained knee kinematics. One recent systematic review 37 of 10 studies examining the effects of LET on anterior tibial translation and/or rotation concluded that LET procedures overconstrained the ACL-deficient knee relative to the native state. In fact, 7 of 8 studies reporting on the effects of LET on tibial rotation observed significant reductions in the magnitude of tibial internal rotation at knee flexion angles between 0° and 90°. 37 However, it is important to acknowledge that 12 different LET procedures were examined in this analysis, and it can be argued that this magnitude of heterogeneity in the surgical procedures included for review precludes any definitive statement on the effect of LET on ACL-deficient knee kinematics. Additionally, a separate biomechanical study investigating the effects of both tibial rotation and the magnitude of tension applied to the graft at the time of fixation had significant effects of residual tibial rotation, as a LET (MacIntosh procedure) performed on a free-hanging tibia with 80 N of tension applied to the graft overconstrained the ACL-deficient knee, whereas LET performed on a tibia fixed in neutral rotation with 20 N of tension applied to the graft did not overconstrain the ACL-deficient knee. 18 Thus, caution must be exercised when pooling results of dissimilar biomechanical studies performed using variable testing parameters, all of which can readily obscure efforts to determine the superiority of one procedure over another. The limitations of the available biomechanical reports underscore the importance of innovations to better understand the time-zero, in vivo effects of these surgical reconstructions in the ACL-deficient knee.
With specific regard to the modified Lemaire procedure, concerns persist regarding the potential for producing overconstrained knee kinematics in the setting of isolated ACL injury based on a previous biomechanical study. 16 Conversely, the current study of in vivo ACL-deficient knee kinematics suggests that the addition of a LET (modified Lemaire procedure) does not overconstrain the knee, as no significant differences between the operative and contralateral knees were observed. These findings appear to corroborate the results of another recent biomechanical study of the Lemaire procedure with the graft fixed with 20 N of tension in neutral rotation that did not observe overconstrained knee kinematics throughout a range of knee flexion angles (0°, 30°, or 60°). 19
The indications for augmenting ACLR with LET remain poorly defined and have largely been based upon imprecise assessments of rotatory knee laxity and/or the identification of patients who may be at risk for graft retear. In the current study, we were unable to detect a difference in either the final amount of rotatory laxity or the change in the magnitude of pre- and postoperative lateral compartment tibial translation between groups. With respect to the baseline QPS measurements between the ACLR and ACLR + LET groups, there were no significant differences in preoperative lateral tibial compartment translations. The decision to augment ACLR with LET was predicated upon the amount of lateral compartment translation during QPS compared with that of the contralateral, uninjured knee. In this way, the contralateral, uninjured knee served as an internal control used to identify “looser,” injured knees. In the absence of significant differences in the presence (or absence) of concomitant injuries, the use of the contralateral, uninjured knee to determine which cases were augmented with LET limited the potential for the confounding effects of variations in other important determinants of knee laxity such as osseous morphology and generalized ligamentous laxity. These data do not necessarily contradict the results of a biomechanical study comparing the amount rotatory knee laxity after anatomic ACLR versus ACLR + LET in the setting of an isolated ACL tear combined with a simulated anterolateral capsule injury. 15 In fact, in the absence of an anterolateral capsule injury, no differences in rotatory knee laxity after ACLR or ACLR + LET were observed. That being said, the injury to the anterolateral capsule in that study involved the removal of a 2-cm slip of anterolateral capsule, which does not reproduce the characteristics of the injury pattern typically observed in vivo. Moreover, the current study did not specifically characterize injuries to the anterolateral complex based upon magnetic resonance imaging, as has been previously described.
A limited amount of literature exists on in vivo, time-zero assessments of the effect of ACLR on rotatory knee instability, with a substantial focus on the application of this technology on the study of the kinematics properties of SB and double-bundle (DB) ACLR. 11 In 1 study, 15 patients with isolated ACL tears undergoing anatomic DB ACLR were tested intraoperatively using a computer navigation system that involved the use of 2 reference frames fixed to the proximal and distal tibia by way of bicortical pins. 21 A stepwise assessment of rotatory knee laxity was conducted after reconstruction of the posterolateral and anteromedial bundles, and the authors observed that the addition of separate bundles improved the laxity parameters in the ACL-deficient knee. 21 In a separate prospective study, 40 100 patients undergoing ACL were assessed during EUA with an invasive, navigation system involving fixation pins in the femur and tibia. The authors found that patients with greater posterior tibia reduction (PTR) during the pivot-shift test performed at the time of EUA were more likely to have a positive pivot shift at 2 years postoperatively. While both studies employed a navigation apparatus to precisely quantify the degree of rotatory knee laxity, an invasive approach was taken in each investigation, involving rigid fixation of sensors to the femur and/or tibia. Presumably, the addition of a separate, invasive aspect of the procedure could create logistical issues pertaining to obtaining patients’ consent in addition to the morbidity associated with the rigid fixation of the testing apparatuses to bone. Moreover, the second study specifically measured the degree of PTR rather than lateral compartment rotation of the tibia during the pivot-shift test, which may very well underestimate the magnitude of rotatory knee instability as manifested by a positive pivot shift-test result. This is similar to another recently published study reporting on the utility of a noninvasive testing setup that was able to reliably detect PTR when compared with the more invasive technique involving sensors fixed to the femur and/or tibia. 26 The current investigation involved the noninvasive measurement of lateral compartment rotation of the tibia, thereby providing a more practical and accurate means for precisely quantifying rotatory knee instability during various stages of surgical reconstruction.
This study has several limitations. All iQPS measurements were performed by a single examiner, which precludes a determination of interobserver reliability. Previous reports have demonstrated this modality to be both accurate and reliable in quantifying the pivot shift. However, we acknowledge there are aspects of performing the test, such as the subtle motions of the stickers on the skin and variations in the position in which the iPad is held during data collection, that may diminish the accuracy of the testing. 31 It should also be acknowledged that QPS is a 2-dimensional (2-D) approximation of a 3-D movement, and a previous report has demonstrated that 3-D osseous movement increased 2.7 to 3.5 times per unit measured by the 2-D QPS measurement. 3 Thus, the QPS and iQPS are best considered as approximations of osseous movement throughout the pivot-shift maneuver, and this fact has the potential to obscure efforts to associate iQPS measurements with a clinical examination, as 6 to 7 mm of lateral tibial translation are required to achieve a grade 1 pivot. 5 We also acknowledge the novelty of the PIVOT iPad application and the fact that this technology is not readily available to all institutions. Both of these points limit the external validity of our results, but it should be pointed out that the PIVOT iPad application has been used across multiple international centers currently participating in the PIVOT (Prospective International Validation of Outcome Technology) Trial, suggesting the potential for this innovation to be incorporated into routine clinical practice in a variety of centers. 23 Moreover, as has been previously demonstrated, the PIVOT iPad application is highly reliable between multiple examinations and across multiple examiners (κ > 0.9). 31 The effects of concomitant pathology on the presence of residual rotatory knee laxity after ACLR cannot be overlooked, as medial and lateral meniscal tears as well as anterolateral capsule injuries have been associated with increased magnitudes of rotatory knee instability in a separate study utilizing the PIVOT iPAD application.31,32 While normative data derived from a larger database of QPS data obtained from over 150 individuals were used to estimate the sample size necessary to demonstrate a difference between the ACLR and ACLR + LET groups, we acknowledge that our study was not powered to detect for differences between specific patterns of injury (ie, combined ACL and medial and/or lateral meniscal tears). This may limit conclusions based upon comparisons of groups with varying patterns of injury, as has recently been demonstrated among a cohort of 354 patients with different injury patterns (isolated partial vs complete ACL tears and combined injuries). 23 In addition, variations in patients’ underlying osseous morphology and generalized ligamentous laxity have been shown to contribute to the magnitude of rotatory knee instability in the ACL-deficient knee.22,34-36 However, it should be noted that there were no significant differences in the magnitudes of preoperative rotatory knee laxity between groups, and the iQPS measurements may perhaps represent a summation of a constellation of factors affecting rotatory knee laxity. In fact, among larger groups of patients, future studies incorporating iQPS data should be pursued to either refute or corroborate previously observed relationships between various injury patterns.
Conclusion
The augmentation of ACLR with LET did not result in overconstrained knee kinematics. Both ACLR and ACLR + LET resulted in significant decreases in rotatory knee instability. However, when compared with isolated ACLR, the addition of LET to ACLR did not result in a significant decrease in time zero, rotatory knee laxity. The utility of combining a LET with ACLR remains unclear and future research is necessary to refine the indications for LET in patients determined to be at risk for residual rotatory knee instability and/or variations in injury pattern.
Footnotes
Acknowledgements
The authors thank Adam Popchak, PT, PhD, SCS, for his assistance with the statistical analysis of this investigation’s data.
Submitted January 12, 2020; accepted July 30, 2020.
Presented at the AOSSM annual meeting, Boston, Massachusetts, July 2019.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.J.S. has received education and hospitality payments from Arthrex, Smith & Nephew, and Stryker; and education payments from MedInc of Texas and Wright Medical Technology. R.T. has an educational grant from Johnson & Johnson. D.d.S. has received education payments from Smith & Nephew and Mid-Atlantic Surgical Systems and a grant from Arthrex. V.M. is a paid consultant of Smith & Nephew and holds a patent for pivot shift software. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.