
Abstract
Background:
Limited evidence exists comparing short- and long-term patient-reported outcomes (PROs) and overall survival rates after hip arthroscopy for femoroacetabular impingement syndrome (FAIS).
Hypothesis:
Patients with high improvement (HI) versus low improvement (LI) at 1 year postoperatively would achieve higher PROs and better index procedure survival rates at 5-year follow-up.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Patients who underwent primary hip arthroscopy for FAIS between September 2012 and March 2014 with minimum 5-year outcome data were identified. Using the median 1-year change in modified Harris Hip Score (mHHS) as a threshold, HI and LI subcohorts were determined. Analysis of variance was used to compare PROs. Failure rates were determined using Kaplan-Meier and Cox proportional hazards model analyses. Regression analysis was used to identify factors associated with increasing 5-year change in mHHS and Nonarthritic Hip Score (NAHS).
Results:
Out of 108 eligible consecutive patients, 89 (82.4%) were included (mean [SD]: age, 43.3 [14.6] years; body mass index, 25.4 [4.5]). As compared with the LI group (n = 45), the HI group (n = 44) had a longer 5-year index surgery survival rate (mean ± SEM: 83.7 ± 3.3 months vs 68.5 ± 4.6 months; P = .012) and 5-year estimated survival rate (89% vs 71%). The HI group had a decreased risk of failure versus the LI group (hazard ratio, 0.15; P = .002). The HI group also had greater PROs than did the LI group at 1 year (mHHS: 94.8 ± 1.2 vs 72.6 ± 2.7, P < .001; NAHS: 94.0 ± 1.3 vs 75.6 ± 2.2, P < .001) and 5 years (mHHS: 86.9 ± 2.0 vs 77.6 ± 3.4, P = .017; NAHS: 92.6 ± 1.8 vs 82.7 ± 4.1, P = .020). As compared with the LI group, the HI group achieved higher rates of the Patient Acceptable Symptomatic State (PASS) and minimal clinically important difference (MCID) at 1 year (PASS: 95% vs 42%, P < .001; MCID: 100% vs 89%, P = .056) and 5 years (PASS: 77% vs 45%, P = .002; MCID: 86% vs 64%, P = .014). Linear regression demonstrated that being in the HI group (ΔmHHS, P = .041; ΔNAHS, P = .017) and decreasing body mass index (ΔmHHS, P = .055; ΔNAHS, P = .023) were associated with higher 5-year ΔPROs.
Conclusion:
Patients with FAIS and significant improvement in the first year after hip arthroscopy had superior 5-year outcomes versus patients with persistent symptom severity. Survival rates and PROs were significantly better in patients who achieved high early outcomes at the 1-year mark.
Femoroacetabular impingement syndrome (FAIS) is the result of pathological joint contact secondary to a combination of a deformed acetabulum abutting a deformed femoral head, vice versa, or both. Frequently, there is concomitant damage to the labrum and cartilage, resulting in a spectrum of FAIS symptoms.6,8,9,14 If left untreated, FAIS often progresses to degenerative joint disease and osteoarthritis, necessitating total hip arthroplasty (THA). 16
Hip arthroscopy has become a successful minimally invasive treatment for FAIS that allows for long-term joint preservation.5,6,9,10,12,16,20 As studies have shown, many factors have been associated with primary outcomes, including patient-specific and intraoperative prognostics, such as demographics, radiographic parameters, cam/pincer management, and chondrolabral injury management.16,21,22 While these studies assessing patient-reported outcomes (PROs) and clinical failure rates have demonstrated excellent overall results, patient selection and counseling in the setting of hip arthroscopy for FAIS remain challenging in clinical practice.5-7,9,11,21,22 Short- and long-term studies to date have mostly reported binary time points regarding pre- and postoperative outcomes after the index procedure. In multiple 2-year follow-up studies from preoperative baseline, various authors have demonstrated >85% high functional state achievement in large cohorts.1,2,23 Five- and 10-year data have echoed short-term trends regarding improvement; however, there has inevitably been a gradual decline in PROs and clinical survival rates to revision procedures regardless of various preoperative prognostic factors.6,7,9-11,16
When reviewing the literature, we found no current studies that have determined whether the degree of short-term improvement seen after hip arthroscopy for FAIS predicts long-term outcomes. From a patient counseling standpoint, the opportunity to discuss and anticipate likely long-term outcomes within the early postoperative period based on 1-year outcomes provides a unique advantage for orthopaedic surgeons. The purpose of this study was to assess whether high improvement (HI) versus low improvement (LI) 1 year after hip arthroscopy for FAIS predicts 5-year outcomes in regard to PROs and clinical failure rates. We hypothesized that the HI group would have a better survival rate to revision procedures and conversion to THA versus the LI group. We projected that the HI group would have better 5-year PROs than would the LI group. Finally, we believed that this difference would be statistically significant from a net score standpoint as well as clinically significant as assessed using 2 validated achievement thresholds: the minimal clinically important difference (MCID) and the Patient Acceptable Symptomatic State (PASS).
Methods
Patient Selection
Patients were identified from a clinical registry of those with FAIS who underwent hip arthroscopy between September 2012 and March 2014. All surgery was performed by the senior author of the current study (T.Y.). Patients in this study provided informed consent as outlined in the approved institutional review board protocol (i15-00058) for the current investigation. FAIS was diagnosed based on clinical symptoms and examination findings (Patrick test, anterior impingement test). Anteroposterior and 45° and 90° Dunn view radiographs in addition to magnetic resonance imaging or magnetic resonance arthrography were used to identify bony and chondrolabral pathology correlating with clinical signs, respectively.
The following composed our inclusion criteria for surgical indication as well as for the current study: lateral center-edge angle ≥40°, alpha angle ≥60°, and proximal focal acetabular retroversion (as indicated by the crossover sign), as well as chondrolabral lesions identified on radiographs, magnetic resonance imaging scans, and/or magnetic resonance arthrography. Patients undergoing surgery had at least 6 months of symptoms and a failed trial of nonoperative management, including activity modification, physical therapy, and nonsteroidal anti-inflammatory medications if tolerated. A diagnostic intra-articular injection was used to confirm the diagnosis of FAIS when the patient had atypical hip pain. A therapeutic cortisone injection was offered as well. The following composed our exclusion criteria: undergoing bilateral hip arthroscopy, a Tönnis grade >1, joint space narrowing ≤2 mm on any radiographic view, presence of hip dysplasia (center-edge angle <20°), age <15 years, rheumatological joint disease history, slipped capital femoral epiphysis history, previous hip procedures, undergoing a revision procedure within the first postoperative year after hip arthroscopy, and declining to participate in research.
Surgical Technique and Rehabilitation
Hip arthroscopy was performed using standard midanterior and anterolateral portal placement. A horizontal interportal capsulotomy was created. Shaving chondroplasty (Outerbridge grades I-III) and minimal abrasion arthroplasty (Outerbridge grade IV) were performed for appropriate chondral lesions. All labral tears involving the chondrolabral junction were repaired using suture anchors if amenable. Dynamic fluoroscopy was used to perform femoral and periacetabular osteochondroplasties for cam and pincer lesions, respectively. Standard capsular repair and portal closure were performed after a final irrigation and removal of debris. All patients received a postoperative hip brace limiting hyperextension and external rotation. Patients were flatfoot weightbearing with crutch assistance for the first 4 weeks, followed by a gradual increase in weightbearing and activity level. Standard postoperative deep vein thrombosis and heterotopic ossification chemoprophylaxis was employed.
Patient-Reported Outcomes
The PROs used for this study were the modified Harris Hip Score (mHHS) and the Nonarthritic Hip Score (NAHS). An MCID threshold of 8 points and a PASS threshold of 74 points were based on previously validated mHHS scores.4,13 All patients received baseline scores at the time of surgery and postoperative scores at the 1- and 5-year intervals. Conversion to a revision procedure after the 1-year follow-up was recorded as not meeting the MCID and PASS thresholds and regarded as clinical failure of the procedure. Additionally, clinical failure was defined as conversion to THA or an additional revision procedure. PROs were not recorded after clinical failure, as data would be assessing index and revision outcomes at that point.
Data Analysis
Median ΔmHHS (40.7 points) from baseline to 1 year was calculated for the cohort and used as the threshold partitioning 2 subcohorts. The HI group was defined as patients achieving higher than this threshold, while the LI group was defined as those achieving lower than this threshold at the 1-year time point. To allow for patients to achieve HI (ΔmHHS >40.7 points at 1-year outcome), patients with baseline mHHS >60 were excluded from this study. Continuous demographic variables were described using standard methods (mean and standard deviation), while categorical demographic variables were described using frequency and percentages. One-way analysis of variance (ANOVA) was used to compare age and body mass index (BMI), while categorical variables were compared using either the chi-square or the Fisher exact test depending on sample sizes. Kaplan-Meier analysis was performed to assess the mean survival time of each group with 95% CIs alongside 5-year survival rates and number at risk. Survival rates between groups were compared using Mantel-Cox log rank tests. A Cox proportional hazards model was performed to assess demographic data (age, sex, BMI), intraoperative data (labral repair, chondroplasty, cam resection, pincer resection), and group status (HI vs LI) to determine the hazard ratios with 95% CIs for significant predictors of risk to revision procedures or conversion to THA. Repeated-measures ANOVA was performed to assess whether a significant interaction existed across all time points for PROs across the entire cohort and using the HI-versus-LI group partition. If a significant interaction was found, a post hoc 1-way ANOVA was conducted at all 3 time points using HI versus LI as the between-patients factor. Last, a linear regression model was performed to assess predictability of baseline to 5-year ΔmHHS and ΔNAHS using the aforementioned demographic and intraoperative variables (as in the Cox model) and group status (HI vs LI). In the Cox model and linear regression, BMI was partitioned into weight class (normal weight, BMI <25.0; overweight, BMI = 25.0-30.0; obese weight, BMI >30). P values <.05 were considered significant. All continuous experimental variables were described as mean and standard error of the mean (SPSS version 25; IBM Corp).
Results
Clinical Outcomes
Out of 108 patients, 89 (82.4%) met the inclusion criteria for this study (mean [SD]: age, 43.3 [14.6] years; 67% female; BMI, 25.4 [4.5]) and had minimum 5-year follow-up (73.7 [12.5] months) (Table 1, Figure 1).
Patient and Intraoperative Characteristics a
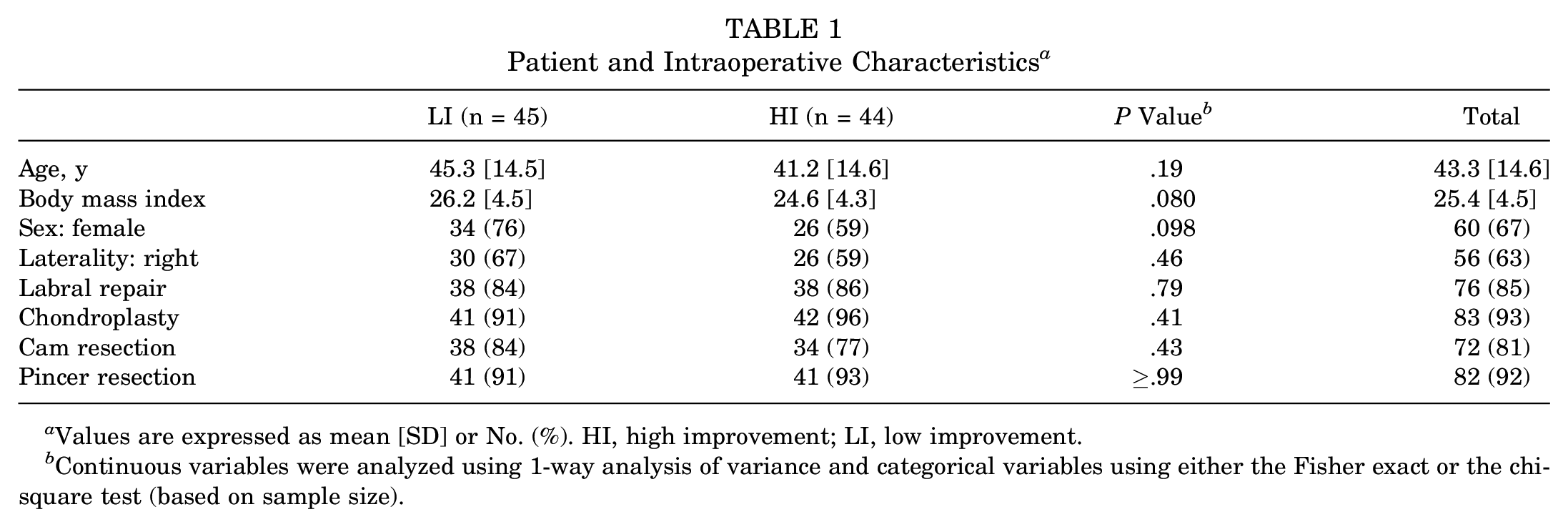
Values are expressed as mean [SD] or No. (%). HI, high improvement; LI, low improvement.
Continuous variables were analyzed using 1-way analysis of variance and categorical variables using either the Fisher exact or the chi-square test (based on sample size).
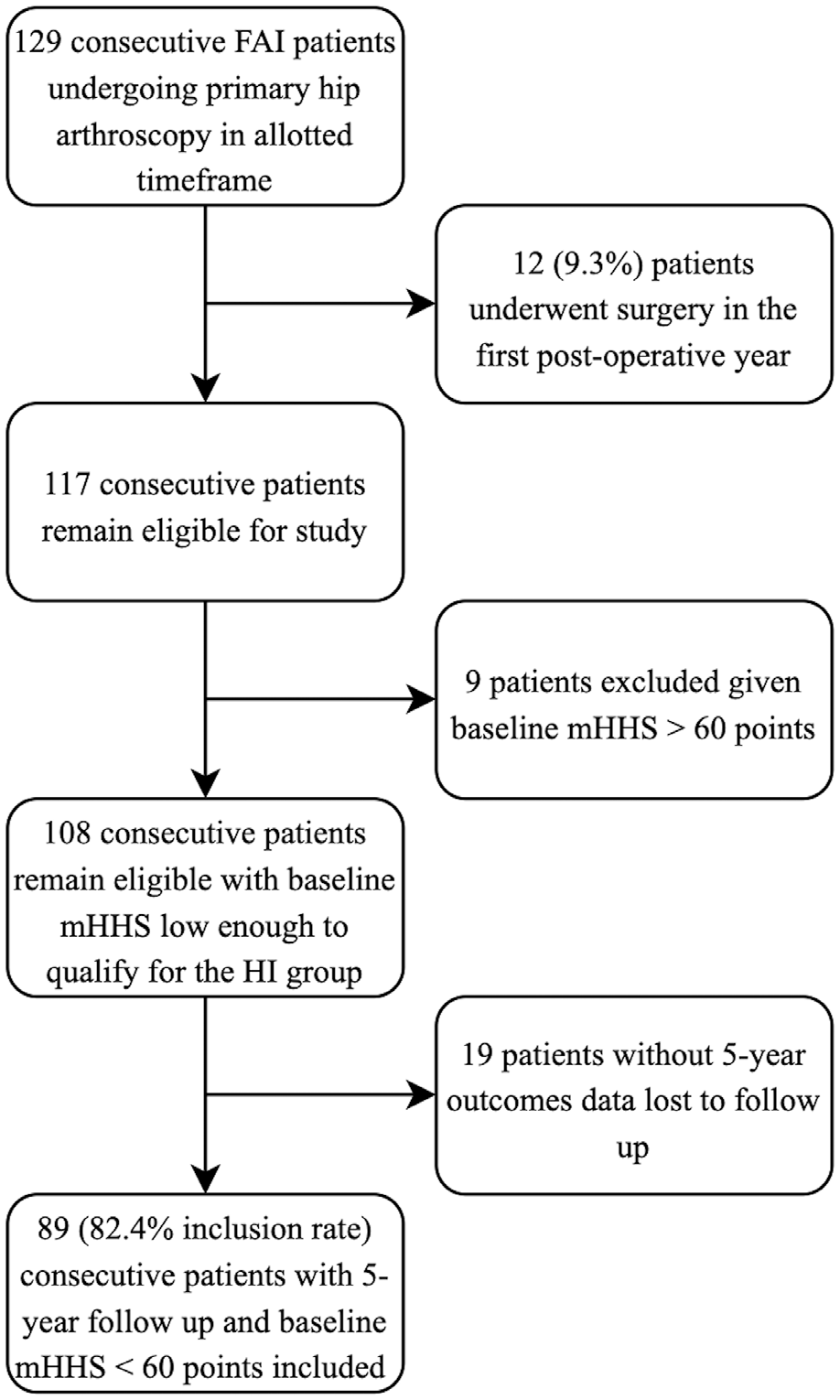
Flowchart indicating patients included in the current study out of total eligible consecutive cases of femoroacetabular impingement syndrome between September 2012 and March 2014. FAI, femoroacetabular impingement; HI, high improvement; mHHS, modified Harris Hip Score.
The HI group (n = 44; age, 41.2 [14.6] years; 59% female; BMI, 24.6 [4.3]; mean ± SEM: 1-year ΔmHHS, 50.5 ± 1.0) underwent a total of 6 revision procedures among 5 patients: 3 revision arthroscopies and 3 conversions to THA. The LI group (n = 45; age, 45.3 [14.5] years; 76% female; BMI, 26.2 [4.5]; 1-year ΔmHHS, 27.0 ± 1.9) underwent a total of 16 revision procedures among 14 patients: 12 revision arthroscopies and 4 conversions to THA. There was 1 mortality in the cohort due to unrelated medical comorbidities. The HI group had a longer survival time (83.7 ± 3.3 months) to the revision procedure than did the LI group (68.5 ± 4.6 months; P = .012). The 5-year survival rate to the revision procedure was 89% (number at risk, 38) in the HI group as compared with 71% (number at risk, 30) in the LI group. There was no difference in survival time to the conversion to THA between the HI group (87.1 ± 2.4 months; 5-year survival, 96%) and the LI group (84.3 ± 2.5 months; 5-year survival, 91%; P = .74) (Figure 2). A Cox proportional hazards model demonstrated labral repair (hazard ratio, 0.15; 95% CI, 0.04-0.50; P = .002) prevented the need for a revision procedure, in addition to being in the HI versus LI group (hazard ratio, 0.15; 95% CI, 0.05-0.52; P = .003).
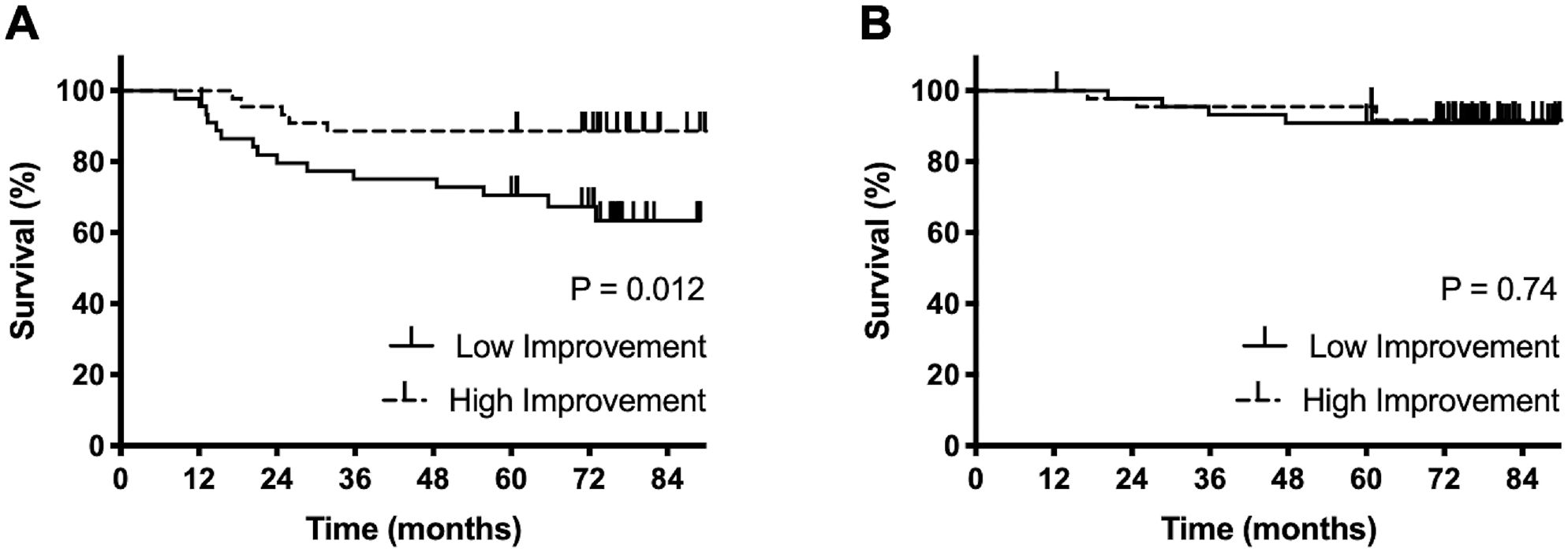
(A) Survival to initial revision procedure after hip arthroscopy in the low improvement (LI) versus high improvement (HI) groups. The HI group had a significantly lower conversion rate to revision procedures and a longer survival rate as compared with the LI group (P = .012). (B) Survival to total hip arthroplasty after hip arthroscopy in the LI and HI groups. There was no difference in survival time and conversion rate to total hip arthroplasty between the groups (P = .74). Kaplan-Meier analysis and Mantel-Cox log rank tests provided P values.
Modified Harris Hip Score
There was a significant increase in mHHS scores from baseline (43.8 ± 1.0) to 5 years (82.9 ± 1.9; P < .001) across the entire cohort. Being in the HI versus LI group demonstrated significant interaction in the repeated-measures ANOVA (P < .001). Post hoc 1-way ANOVA indicated that the HI group had significantly greater 1-year (94.8 ± 1.2 vs 72.6 ± 2.7; P < .001) and 5-year (86.9 ± 2.0 vs 77.6 ± 3.4; P = .017) mHHS outcomes than the LI group had. Baseline mHHS values between the LI and HI groups were not statistically different (P = .66) (Table 2, Figure 3). Linear regression analysis showed a significant correlation predicting 5-year ΔmHHS (r2 = 0.12; P = .018). Increasing weight class (beta, –5.4; 95% CI, –11.0 to 0.1; P = .055) trended predictive of lower 5-year ΔmHHS, while being in the HI versus LI group (beta, 8.0; 95% CI, 0.3-15.7; P = .041) was predictive of higher 5-year ΔmHHS.
Patient-Reported Outcome Comparisons a
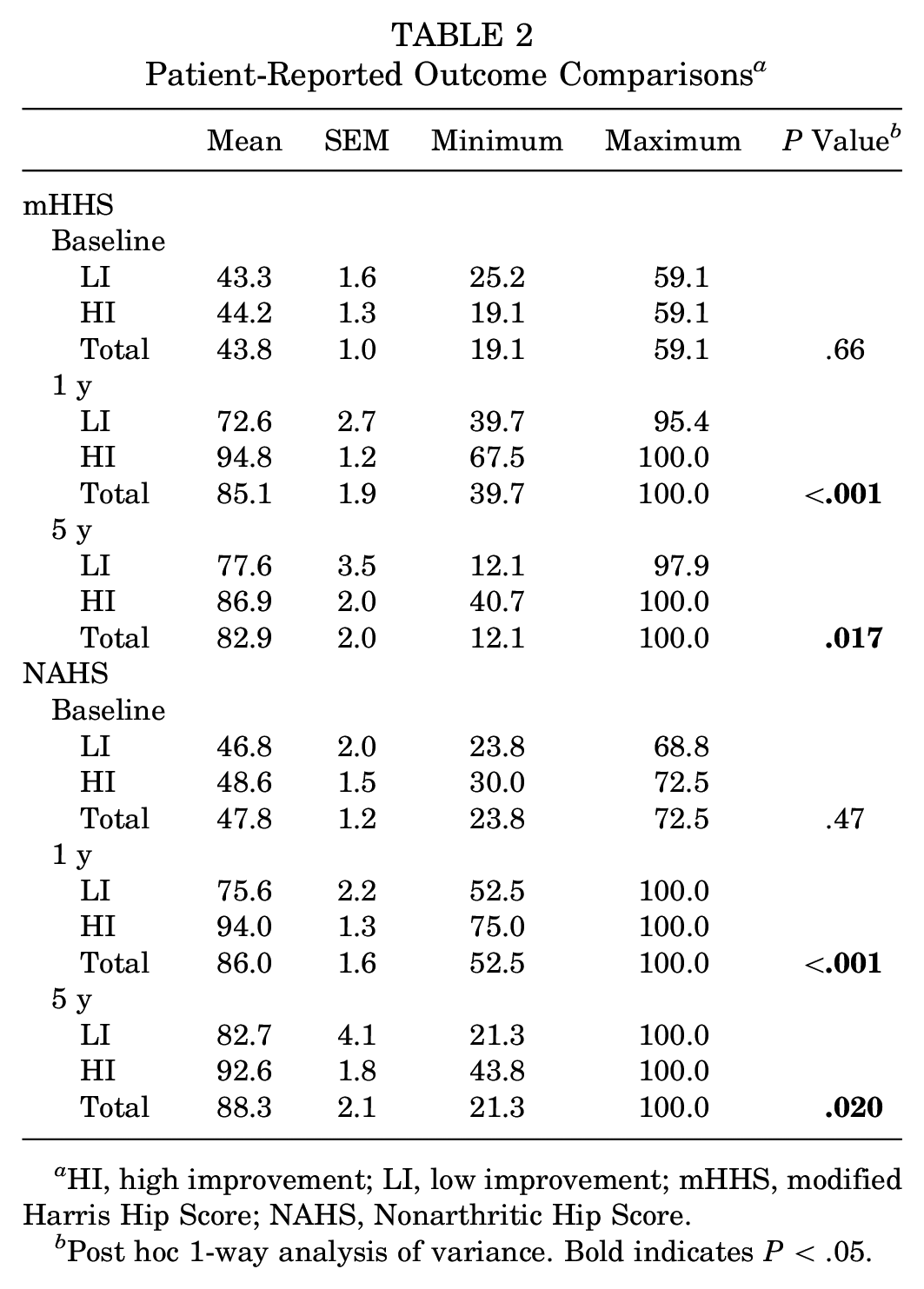
HI, high improvement; LI, low improvement; mHHS, modified Harris Hip Score; NAHS, Nonarthritic Hip Score.
Post hoc 1-way analysis of variance. Bold indicates P < .05.
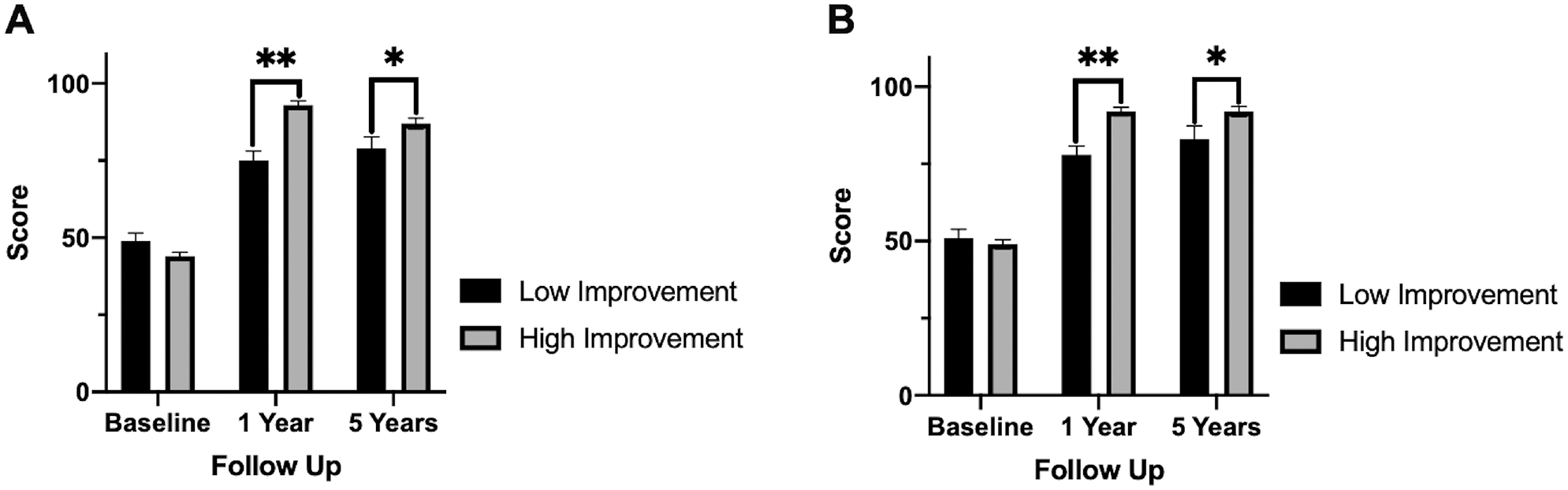
(A) The modified Harris Hip Score of the high improvement (HI) versus low improvement (LI) groups at baseline, 1 year, and 5 years. The HI versus LI group performed significantly better at the 1-year (P < .001) and 5-year (P = .017) time points. (B) Nonarthritic Hip Score of the HI versus LI groups at baseline, 1 year, and 5 years. The HI versus LI group performed significantly better at the 1-year (P < .001) and 5-year (P = .020) time points. Values are presented as mean ± SEM. *P < .05. **P < .001.
When compared with the LI group, the HI group achieved a higher PASS rate at 1 year (95% vs 42%; P < .001) and 5 years (77% vs 45%; P = .002). Last, the HI group achieved a trending higher MCID rate at 1 year (100% vs 89%; P = .056) and a significantly higher rate at 5 years (86% vs 64%; P = .014) (Figure 4).
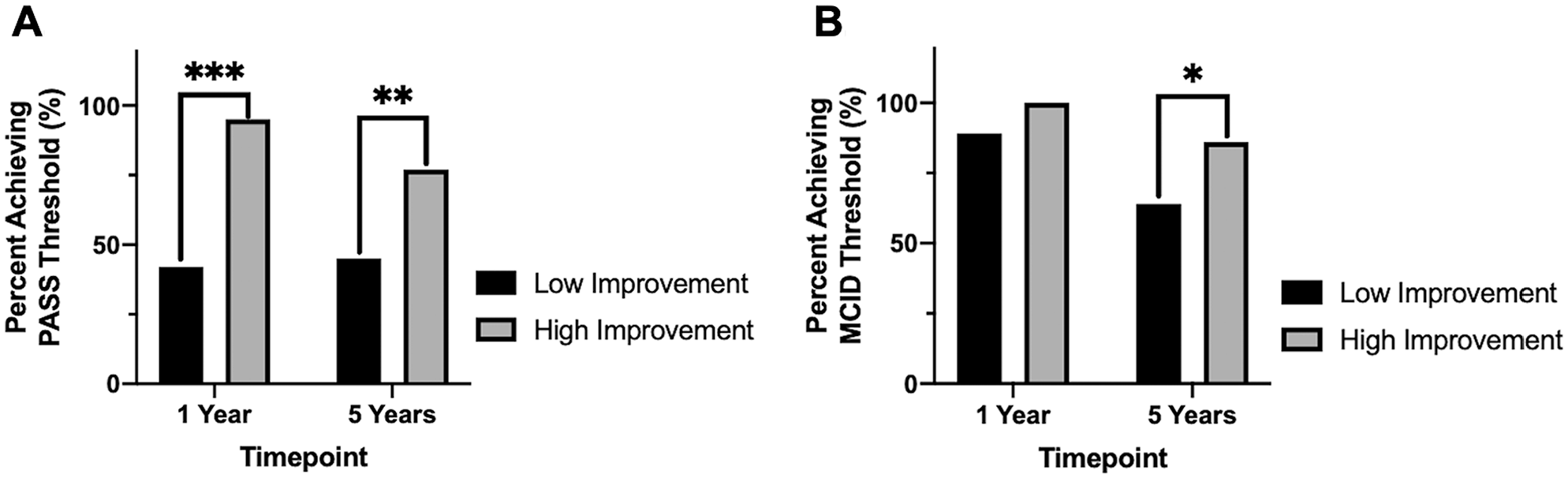
(A) Patient Acceptable Symptomatic State (PASS) rates achieved at 1- and 5-year outcomes. The high improvement group performed consistently better versus the low improvement group at 1-year (P < .001) and 5-year (P = .002) outcomes. (B) Minimal clinically important difference (MCID) rates achieved at 1- and 5-year outcomes. The high improvement group performed consistently better versus the low improvement group at 1 year (P = .056) and 5 years (P = .014). *P < .05. **P < .01. ***P < .001.
Nonarthritic Hip Score
There was a significant increase in NAHS from baseline (47.8 ± 1.2) to 5-year outcomes (88.3 ± 2.1) (P < .001) across the entire cohort. Being in the HI versus LI group demonstrated significant interaction in the repeated-measures ANOVA (P < .001). Post hoc 1-way ANOVA indicated that the HI group had significantly greater 1-year (94.0 ± 1.3 vs 75.6 ± 2.2; P < .001) and 5-year (92.6 ± 1.8 vs 82.7 ± 4.1; P = .020) NAHS outcomes as compared with the LI group (Table 2, Figure 3). Linear regression analysis showed a significant correlation predicting 5-year ΔNAHS (r2 = 0.15; P = .004). Increasing BMI (beta, −7.7; 95% CI, −14.2 to −1.1; P = .023) was predictive of lower 5-year ΔNAHS, while being in the HI versus LI group (beta, 11.1; 95% CI, 2.0-20.2; P = .017) was predictive of higher 5-year ΔNAHS.
Discussion
This study demonstrated that short-term outcomes after hip arthroscopy for FAIS predict long-term outcomes. Patients with significant improvement at the 1-year time point performed significantly better long-term as compared with patients unable to achieve significant symptomatic relief within the first postoperative year. This is clinically significant because hip arthroscopic surgeons can start predicting patient satisfaction after surgery by 1-year recovery time. If patients are not reporting a certain level of positive outcomes at 1 year postoperatively, they are not as likely to continue to improve and have sustained success.
Our results suggested that the HI group had a longer survival time to a revision procedure as well as a lower absolute conversion rate within the follow-up period as compared with the LI group. When assessed in a multivariate fashion, being in the HI versus LI group remained a positive predictor of long-term survival rates, while labral repair was found to be protective of conversion to a revision procedure. Furthermore, our analysis showed not only a statistically significant but also a clinically relevant improvement in 5-year PROs, as assessed using raw mHHS and NAHS scores as well as MCID and PASS achievement rates in the HI versus LI group. Our multivariate linear regression analysis demonstrated an increasing BMI was a negative predictor of ΔmHHS and ΔNAHS outcomes from baseline to 5 years, in addition to being in the LI versus HI group. Most important, our analysis provided a clinically relevant target threshold of the ΔmHHS (40 points) from baseline to 1 year, allowing for superior patient counseling at the 1-year follow-up visit rather than assessing this variable in a continuous fashion.
A variety of short-term studies have assessed outcomes after hip arthroscopy for FAIS using the 2-year follow-up time point.1,3,5,8,15,18,19 Nho et al 18 reported overall excellent outcomes in a high-volume study (n = 935) with regard to clinical failure rates. In contrast to the current study, Nho et al report an absolute conversion rate without a survival analysis and in an overall much younger cohort (mean age, 33 vs 43 years), making comparisons regarding clinical failure rates difficult. Regarding the ΔmHHS, the current study’s median ΔmHHS at 1 year (40) appears to be higher than their reported value (~22) at 2 years, which also suggests a discrepancy in analysis alongside cohort differences. 18 Interestingly, their multivariate analysis demonstrated that a lower preoperative symptom severity score in addition to the presence of chronic pain resulted in worse 2-year PROs. 18 Kunze et al 15 and Basques et al 1 probed the effects of preoperative symptom duration in similar large younger cohorts at the 2-year time point (Kunze: n = 1049 [mean age, 32 years]; Basques: n = 624 [mean age, 34 years]). After splitting their respective cohorts into variations of essentially early versus late hip arthroscopy for FAIS based on duration of symptoms, they showed that the groups with longer symptom duration had worse outcomes from a PRO standpoint as well as higher clinical failure rates (ie, progression to secondary procedures).1,15
The aforementioned cohorts appear to be different from ours, as evidenced by the older age in this study, which could predispose our cohort to undergoing a higher rate of revision procedures while still having a robust ΔmHHS 1-year outcome. 20 Regardless, the studies performed by Nho et al, 18 Basques et al, 1 and Kunze et al 15 highlight the importance of symptom severity and duration in affecting patient outcomes. As a corollary, our study showed that patient counseling and surgical decision making in the postoperative period may be predicted in part by symptom severity, as one would expect.
While comparisons are difficult, given the differences in cohort selection criteria, surgical techniques, data analysis, and overall patient populations studied, long-term studies inevitably quote higher clinical failure rates, while net change in PROs is variable. Menge et al 16 assessed 10-year outcomes in a large cohort (n = 154) and showed that labral repair was superior to debridement in the primary outcome of their study, as confirmed by our multivariate analysis. Contrary to the aforementioned short-term studies, an assessment of the survival analyses conducted in this 10-year study demonstrated comparable clinical failure rates with the current study at the 2- and 5-year time points. Regardless of this difference in survival rates, the ΔmHHS from the pre- to postoperative time points quoted by Menge et al (~20-30 points) is similar to the value quoted by short-term studies, which appears contradictory.
Domb et al 11 performed a study with a high inclusion rate (85%) that assessed 5-year trends after hip arthroscopy with labral base repairs. From pre- to postoperative values, the authors documented an ~20-point ΔmHHS, while clinical failure rates were slightly less than those of the current study and the Menge et al 16 study. However, Domb et al 11 studied a cohort that was one of the youngest (mean age, 29 years) and had a slightly lower BMI compared with that of the current study (23 vs 25). Chen et al 6 similarly quoted 5-year data from a younger cohort of athletes (mean age, 32 years; mean BMI, 23) with an ~20-point ΔmHHS from baseline to 5 years postoperatively. Given that our multivariate analysis reflected the deleterious effects of increasing BMI, discrepancies in absolute outcomes can be expected. Unique to the Chen et al 6 study, patient return to sports was also discussed, with the majority regaining some form of baseline activity level and with remarkably only 13.5% requiring secondary revision procedures in the follow-up period.
Five-year studies assessing major differences in not only intraoperative technique, such as microfracture, debridement versus labral repair, and joint space narrowing <2 mm, but also cohort makeup (ie, elderly) all have demonstrated similar trends in long-term outcomes.7,10,20-22 While these studies have cited a range of clinical failure rates, from <10% to >80% conversion, in addition to a range of ΔPROs from baseline to end-study outcomes, there do not seem to be evaluations in the literature regarding whether patients who do well early tend to progress in such fashion.
While useful in determining the efficacy of hip arthroscopy in joint preservation across various populations in the long term, these studies did not follow serial PRO values to trend symptom evolution in the postoperative period other than a binary pre- to postoperative PRO comparison. A strategy could be to compare short- and long-term studies systematically in an effort to evaluate common trends to counsel patients accordingly. Unfortunately, as evidenced from the present discussion, PRO- and survival-based outcomes seem to be too relative to the respective populations studied for successful cross-comparisons to occur. Furthermore, as the major aims of studies differ, there is additional inability to successfully extrapolate results from one study to another other than conclusions suggestive of positive or negative effects of various prognostics.
By providing a threshold with which short-term achievement suggests positive long-term outcomes, our results offer a new facet of patient counseling in the postoperative period. While it is clear that absolute ΔPRO values differ from cohort to cohort, our decision to use the median ΔmHHS at the 1-year mark allows the findings of this study to be generalizable to any cohort studied across other institutions by allowing them to choose their own median thresholds at the 1-year time point. As a result, our study could serve as a benchmark for future studies assessing risk to revision hip arthroscopy.
A significant limitation of our study secondary to the design is the exclusion of patients undergoing revision procedures within the first postoperative year. As a result, our study is applicable only to patients who successfully make it a year past the initial surgery date without having conversion to any other procedures. While this may decrease the generalizability of our study to the overall population with FAIS, it should be emphasized that just a minority of patients undergo secondary procedures within the first postoperative year. Additionally, our inclusion rate of 82.4%, while comparable with other studies, would inevitably lead to biases secondary to patients lost to follow-up. While our study employed the mHHS and NAHS metrics, the International Hip Outcome Tool–33 may be of more merit, although all the aforementioned PRO scales have been validated in the literature. 17 Additionally, the PROs demonstrated a slight decline in the HI group from 1- to 5-year outcomes, while they showed a slight increase in the LI group. Although net values in the HI versus LI group still support the superiority of 5-year outcomes in the HI group, this observation of intracohort trends must be noted. We applied the MCID and the PASS to 5-year outcomes even though the original validation studies were for 1-year outcomes, in effect creating a theoretical limitation. 4 Last, this study has biases and limitations inherent to any retrospective analysis, and although our cohort size is large, there is always a concern that the study may be underpowered.
In conclusion, patients with FAIS and high improvement in symptoms 1 year after undergoing hip arthroscopy had superior 5-year outcomes to patients with low improvement. Survival rates and PROs were significantly better long-term in patients who achieved an ΔmHHS above the median of the cohort at the 1-year time point. As such, providers should counsel patients accordingly during the 1-year follow-up period. While patients doing well early will likely continue to do so, patients without much symptom relief 1 year after surgery may not achieve similar improvements at 5-year follow-up.
Footnotes
Submitted May 1, 2020; accepted August 10, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: T.Y. has received consulting fees from Arthrex, speaking fees from Smith & Nephew, and hospitality payments from DePuy Orthopaedics. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.