
Abstract
Background:
Controversy exists regarding the surgical treatment of recurrent patellar dislocation (RPD) with an increased femoral anteversion angle (FAA). Medial patellofemoral ligament reconstruction (MPFL-R) either alone or combined with derotational distal femoral osteotomy (DDFO) results in favorable clinical outcomes.
Purpose:
To compare the clinical outcomes of MPFL-R versus MPFL-R with DDFO in treating RPD with increased FAA (>30°).
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Between January 2014 and December 2017, 126 patients (135 knees) with RPD and increased FAA (>30°) were surgically treated using MPFL-R with or without DDFO and eligible for this retrospective study. These patients were allocated into 2 groups based on whether an additional DDFO was performed: the DDFO group (MPFL-R + DDFO with or without tibial tubercle transfer; n = 66) and the control group (MPFL-R with or without tibial tubercle transfer; n = 69). Pre- and postoperative patellar stability was measured using stress radiography. Patellar maltracking (J-sign) and patient-reported outcomes (Kujala, International Knee Documentation Committee, Lysholm, and Tegner scores) were evaluated and compared between the 2 groups. Subgroup analysis was performed by stratifying the results in terms of the severity of preoperative patellar maltracking (low-grade vs high-grade J-sign).
Results:
A total of 135 knees (126 patients) with a mean follow-up time of 3.7 ± 1.2 years were evaluated in the present study. The rates of postoperative MPFL residual graft laxity and residual J-sign were significantly lower in the DDFO group than in the control group (6% vs 19%, P = .028; 33% vs 54%, P = .018). The DDFO group had significantly higher Kujala (82.3 vs 76.7; P = .001) and Lysholm (83.7 vs 77.7; P = .034) scores than the control group had postoperatively. For patients with a preoperative high-grade J-sign, further subgroup analysis demonstrated that the DDFO group had a significantly lower rate of MPFL residual graft laxity than the control group had (18% vs 57%; P = .029).
Conclusion:
In this retrospective study, treatment of RPD with increased femoral anteversion using MPFL-R with DDFO yielded more favorable subjective and objective outcomes than did MPFL-R without DDFO, and this circumstance was more remarkable when the patients had a preoperative high-grade J-sign.
Keywords
Recurrent patellar dislocation (RPD) is a multifactorial disease,5,10,24 and increased femoral anteversion angle (FAA) has been recognized as a predisposing factor.5,8,17,19,25 If left untreated, the increased FAA may result in a persistent lateralizing force vector exerted on the patella, which might increase stress on the reconstructed medial patellofemoral ligament (MPFL) and ultimately lead to patellar redislocation.15,16
Currently, it remains unclear how to address RPD with increased FAA. Several studies have analyzed the influence of excessive femoral anteversion on clinical outcomes and found that those with an FAA >30° are prone to have worse patient-reported outcomes.11,33 Furthermore, some authors have suggested that an uncorrected increased FAA is a contributing factor to MPFL reconstruction (MPFL-R) failure.13,16,21 For this reason, derotational distal femoral osteotomy (DDFO) has been suggested as an alternative treatment for RPD with increased FAA, and favorable short-term clinical outcomes have been reported after this procedure. ‡
On the other hand, another argument holds that although various skeletal deformities exist, including increased FAA, the reconstructed MPFL has the potential to counteract adverse effects, yielding favorable clinical outcomes.1,9,18 Sappey-Marinier et al 22 reported a satisfactory clinical outcome of 211 patients who underwent isolated MPFL-R regardless of bony deformities. Recently, another study supported the view that the isolated MPFL-R could be effective in treating RPD with bony risk factors, including increased FAA. 1
To date, there is a lack of studies comparing clinical outcomes of MPFL-R with or without combined DDFO in treating RPD with increased FAA, although such information may help surgeons in decision making when encountering patients with RPD and increased FAA.
Therefore, the purpose of this study was to compare the clinical outcomes of MPFL-R versus MPFL-R with DDFO in treating RPD with increased FAA (>30°). It was hypothesized that the MPFL-R with DDFO would lead to better postoperative patellar stability and patient-reported outcomes than would MPFL-R without DDFO.
Methods
A total of 434 patients (454 knees) with a diagnosis of RPD were treated at our institution between January 2014 and December 2017. Patients with increased FAA (>30°) were enrolled in this study. All included patients underwent MPFL-R, and 2 combined procedures (DDFO or tibial tubercle transfer) were performed in selected patients. Between 2014 and 2015, patients with increased FAA were routinely treated using MPFL-R alone or with tibial tubercle transfer. After 2015, the DDFO procedure was performed in the treatment of such patients, and increased FAA (>30°) with a positive J-sign were the indications for DDFO in our department. An Elmslie-Trillat medialization osteotomy was performed in patients with a tibial tubercle-trochlear groove (TT-TG) distance ≥20 mm. Patients were allocated into 2 groups based on whether a DDFO was performed: patients undergoing MPFL-R with DDFO were allocated into the DDFO group (n = 66), and patients undergoing MPFL-R without DDFO were allocated into the control group (n = 69) (Figure 1). The inclusion and exclusion criteria are presented in Table 1. This study was approved by our institutional ethics board and complied with the patients’ consent.
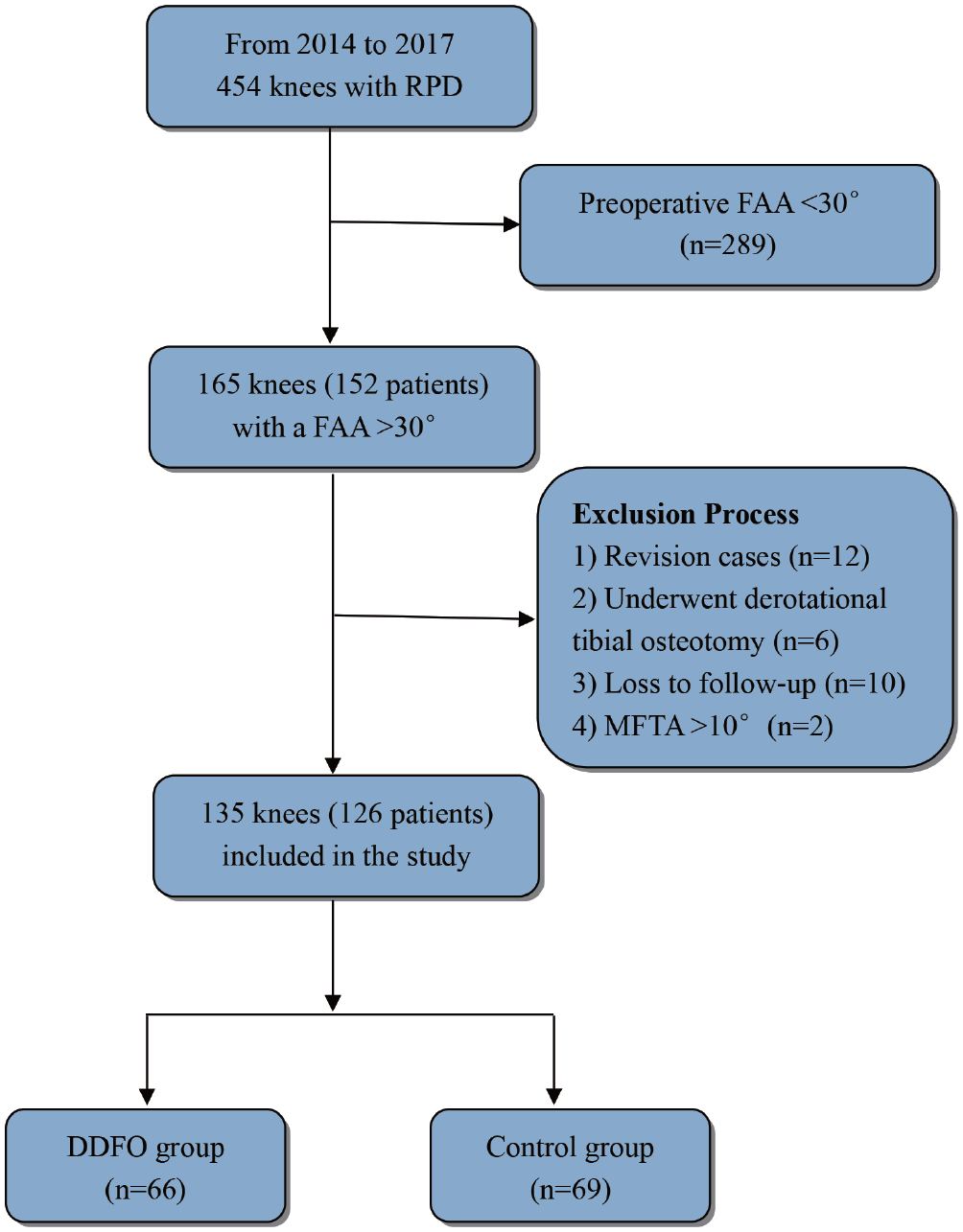
Flowchart of the patient selection. DDFO, derotational distal femoral osteotomy; FAA, femoral anteversion angle; MFTA, mechanical femorotibial angle; RPD, recurrent patellar dislocation.
Inclusion and Exclusion Criteria a
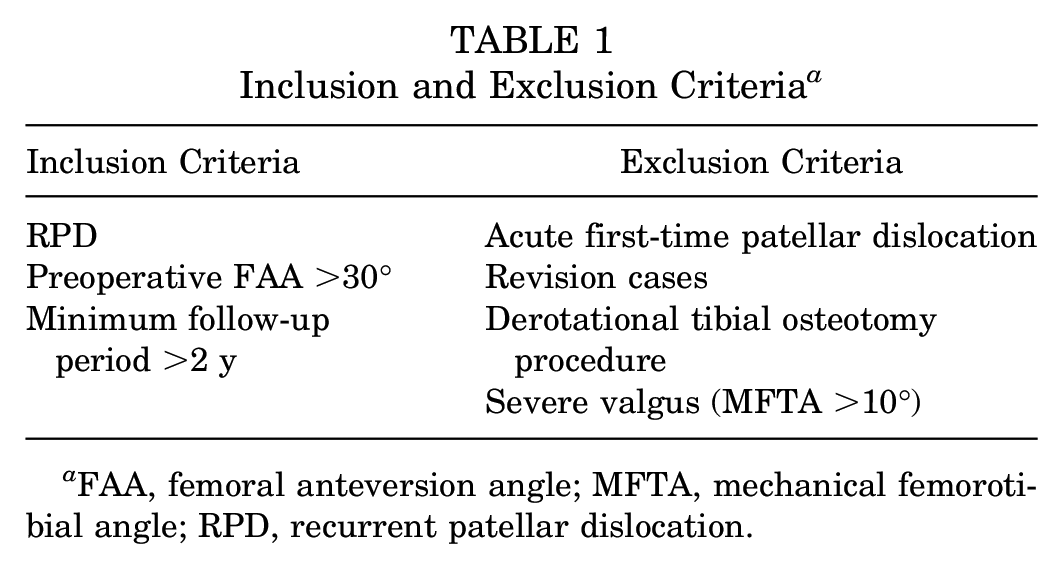
FAA, femoral anteversion angle; MFTA, mechanical femorotibial angle; RPD, recurrent patellar dislocation.
Radiological Parameter Measurements
Computed tomography (CT) scans were performed for all patients preoperatively (Toshiba Medical Systems). The Digital Imaging and Communications in Medicine data from the hip-knee-ankle CT scan were reconstructed into 3-dimensional models using Mimics Research 20.0 (Materialise) to detect rotational deformities of the lower extremity according to a method described previously. 31 The FAA was defined as the angle formed between the axis of the femoral head-neck and distal femur, and the external tibial torsion angle was assessed by measuring the rotational angle of the proximal tibia relative to the distal tibia. The present study showed an interobserver agreement of 0.9° for femoral anteversion and 0.7° for external tibial torsion angle.
The Caton-Deschamps Index was used to measure patellar height. 23 Trochlear dysplasia was detected on the true lateral view of the knee and classified according to the Dejour classification system; 5 severe trochlear dysplasia was defined as type B or D. 31 All patients were examined using axial CT for the measurement of the TT-TG distance according to the method described by Camp et al. 3 To detect the presence of valgus/varus deformity, the femorotibial angle was measured on the whole-leg standing anteroposterior radiograph. All these radiological parameters were measured by 2 independent examiners (H.Z., Z.J.Z.) who were blinded to the treatment groups.
Surgical Techniques
Derotational Distal Femur Osteotomy
DDFO was performed according to a method described previously. 31 A standardized lateral subvastus approach at the distal femur was used. A self-designed osteotomy goniometer was employed to determine the rotation angle of the osteotomy, which was marked using 2 Kirschner wires (Youke). The osteotomy was performed using an oscillating saw, and Steinmann nails (Youke) were placed proximally and distally to the osteotomy to control the torsion angle from an axial view. The preoperatively planned FAA was 10°, and the maximum correction angle was 40°. The distal femur was rotated to a predetermined angle using Steinmann nails and fixated using a Tomofix distal femoral plate (DePuy Synthes) (Figure 2).
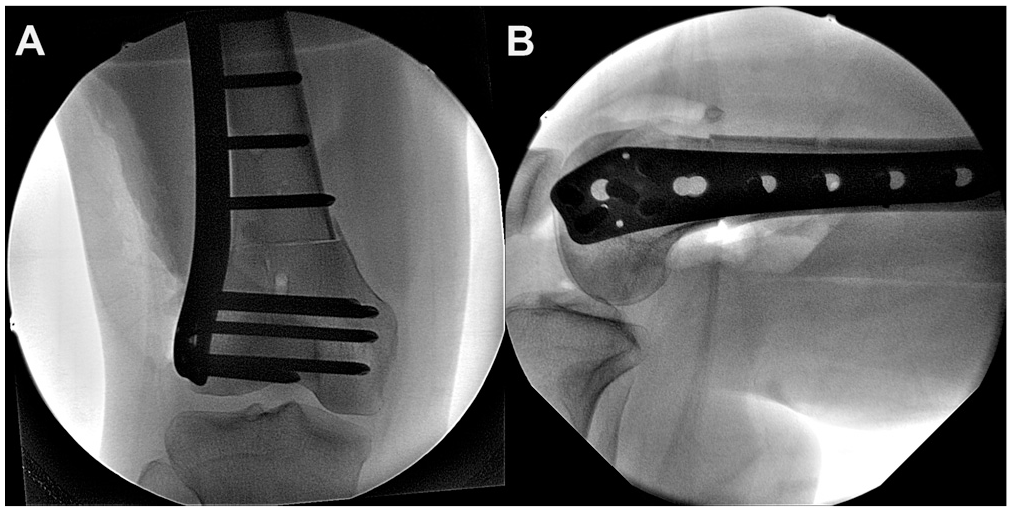
Derotational distal femoral osteotomy fixed using Tomofix distal femoral plate (DePuy Synthes) in the right leg. (A) Anteroposterior view. (B) Lateral view.
Other Procedures
The MPFL was reconstructed using the semitendinosus tendon autograft under intraoperative fluoroscopy according to the method described by Schöttle et al. 23 Elmslie-Trillat medialization osteotomy was performed in patients with TT-TG distance ≥20 mm to normalize the TT-TG to 10 to 12 mm. In addition, tibial tubercle distalization osteotomy was performed in patients with patella alta (Caton-Deschamps Index ≥1.2) to decrease the patellar height to 1.0.
Postoperative Rehabilitation
A protective knee brace without limitation of range of motion was applied during the first 4 weeks after surgery. A crutch providing protective weightbearing was also used during this period, and partial weightbearing (<10 kg) for the first 4 weeks was allowed, followed by full weightbearing. Flexion increased slowly each week as tolerated. The isometric quadriceps muscle training started immediately after surgery for all patients.
Patient-Reported Outcome and Patellar Maltracking (J-sign) Assessment
The Tegner score, Kujala score, Lysholm score, and International Knee Documentation Committee score were assessed preoperatively and at the final follow-up. The preoperative J-sign was graded according to a method described previously 31 : grade 1, >1 quadrant of patellar motion; grade 2, >2 quadrants of patellar motion; and grade 3, complete patellofemoral dislocation. In the present study, a grade 3 J-sign was categorized as a high-grade J-sign, and a grade 0/1/2 J-sign was categorized as a low-grade J-sign. The postoperative J-sign was assessed again to identify patients with a residual J-sign. The interobserver and intraobserver weighted kappa values were 0.81 and 0.83, respectively, for the J-sign classification.
Stress Fluoroscopy Assessment
Patellar Medial Laxity Index
Axial stress fluoroscopy was used to assess the patellar medial laxity index with the knee flexed at 30° (all knees in the DDFO group and 52 knees in the control group).28,31 First, a stress-free radiograph of the patellofemoral joint was obtained. Second, maximum manual pressure was applied to the medial side of the patella, displacing it laterally, to obtain the maximum lateral stress radiograph. The patellar medial laxity index was calculated using these 2 radiographs according to the method described in Figure 3. The interobserver and intraobserver kappa values were 0.91 and 0.93, respectively. If the patellar medial laxity index exceeded 50%, MPFL residual graft laxity was considered for the reconstructed ligament.
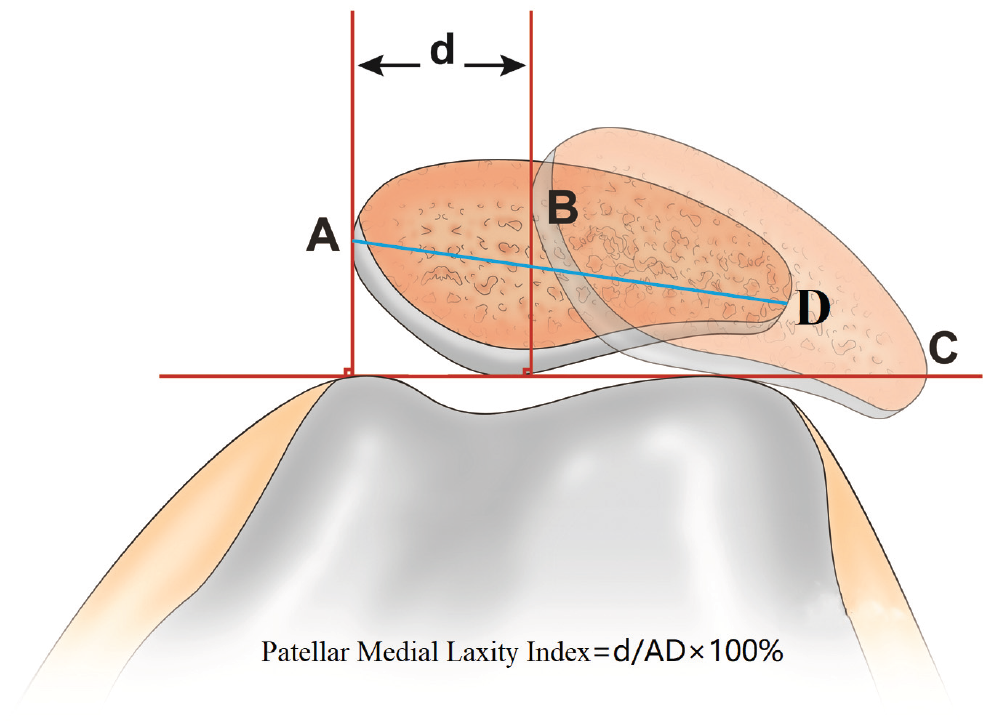
Measurement of the patellar medial laxity index. A line is drawn tangent to the femoral trochlea, and 2 perpendicular lines are drawn through the medial border of the patella in the nonstress radiograph (left, A) and stress radiograph (right, B). C represents the lateral border of the patella in the stress radiograph. The distance d is the maximum lateral shift distance relative to the nonstress status, AD represents the medial-lateral width of the patella, and the ratio of d/AD× 100% is the patellar medial laxity index.
Statistical Analyses
Statistical analyses were performed using the SPSS Version 20.0 software package (IBM Corp). The Pearson chi-square test or Fisher exact test was used to compare categorical variables. For comparisons of continuous variables, the Student t test or Mann-Whitney U test was used. First, a comparison of clinical outcomes was performed between the DDFO group and the control group. Second, given the adverse effect of a high-grade J-sign on clinical outcome,31,32 subgroup analysis was conducted by stratifying the results according to the severity of preoperative patellar maltracking (low-grade vs high-grade J-sign). A priori power analysis was performed based on the postoperative Kujala score between the DDFO group and the control group; it was determined that a sample size of 38 for each group was adequate to detect this difference with a power of 0.95 and an α = .01.
Results
A total of 135 knees (126 patients) with a mean follow-up time of 3.7 ± 1.2 years (range, 2.0-6.0 years) were included in the present study. Characteristics of the groups are presented in Table 2.
Characteristics of the DDFO Group and Control Group a
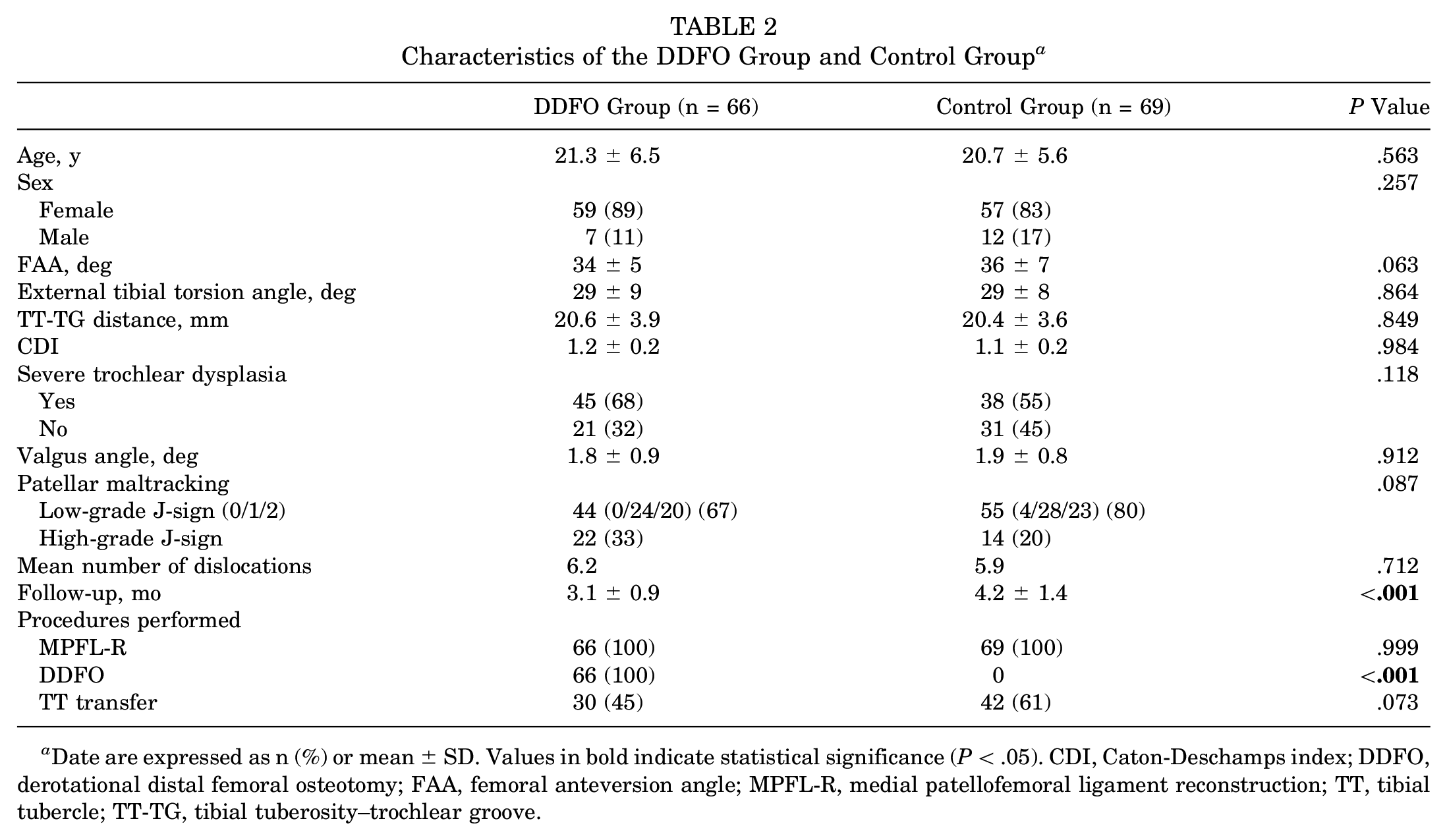
Date are expressed as n (%) or mean ± SD. Values in bold indicate statistical significance (P < .05). CDI, Caton-Deschamps index; DDFO, derotational distal femoral osteotomy; FAA, femoral anteversion angle; MPFL-R, medial patellofemoral ligament reconstruction; TT, tibial tubercle; TT-TG, tibial tuberosity–trochlear groove.
The postoperative patellar medial laxity index was significantly higher in the control group than in the DDFO group (33% vs 23%; P = .001). Moreover, 19% of the patients in the control group showed MPFL residual graft laxity, which was significantly higher than that in the DDFO group (6%) (Table 3). All patient-reported outcomes improved significantly in both groups at the final follow-up, and the DDFO group had significantly higher postoperative Kujala scores and Lysholm scores than did the control group (Table 3).
Comparison of Clinical Outcomes Between the DDFO Group and the Control Group a
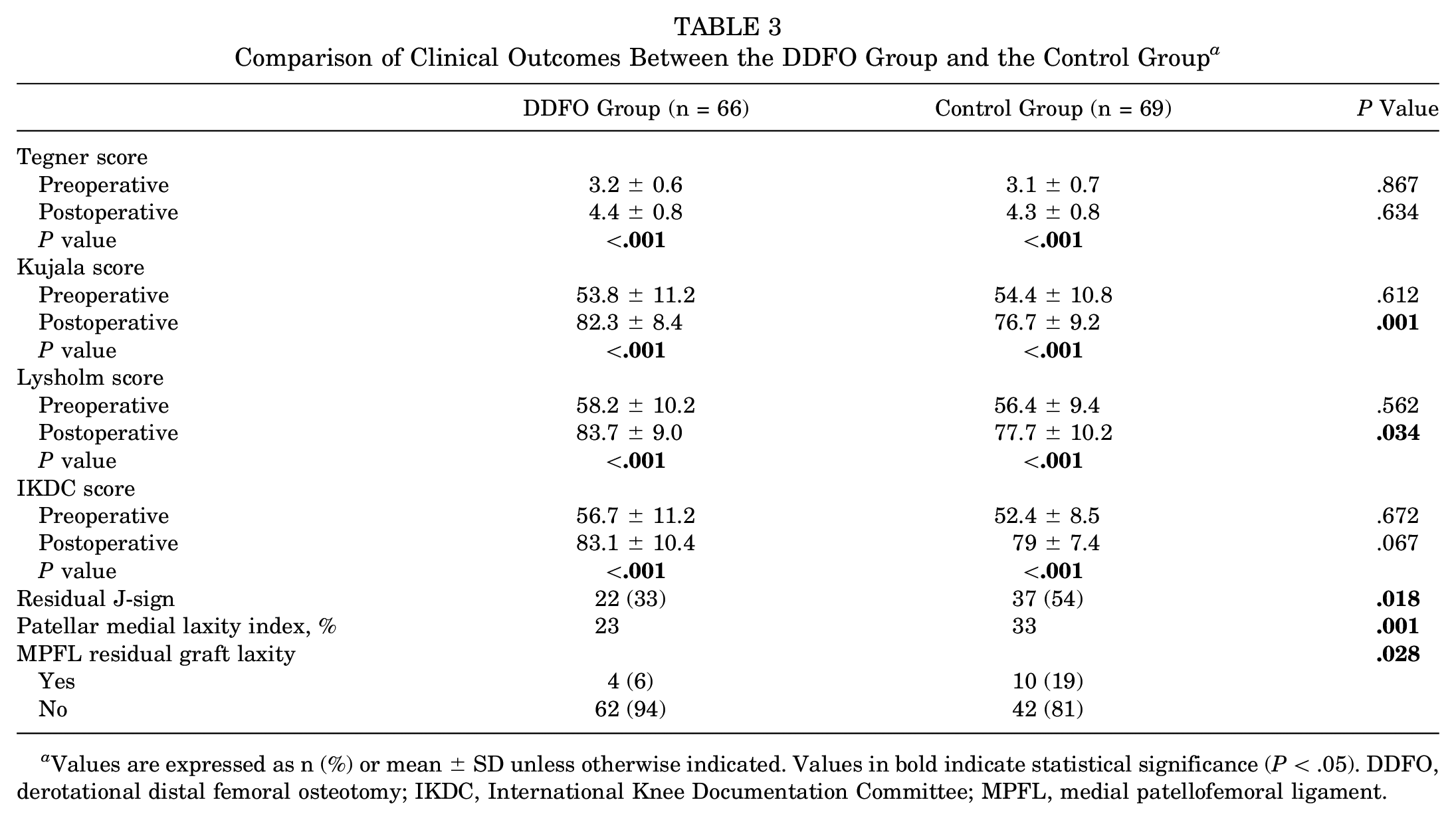
Values are expressed as n (%) or mean ± SD unless otherwise indicated. Values in bold indicate statistical significance (P < .05). DDFO, derotational distal femoral osteotomy; IKDC, International Knee Documentation Committee; MPFL, medial patellofemoral ligament.
Further subgroup analysis by the severity of patellar maltracking revealed that among patients with a high-grade J-sign, the DDFO group had a significantly lower rate of MPFL residual graft laxity than did the control group (18% vs 57%; P = .029). No significant difference between these 2 groups in the rate of MPFL residual graft laxity was found for patients with a low-grade J-sign (0% vs 5%; P = .212) (Table 4).
Subgroup Analysis of Clinical Outcomes by the Severity of Patellar Maltracking a
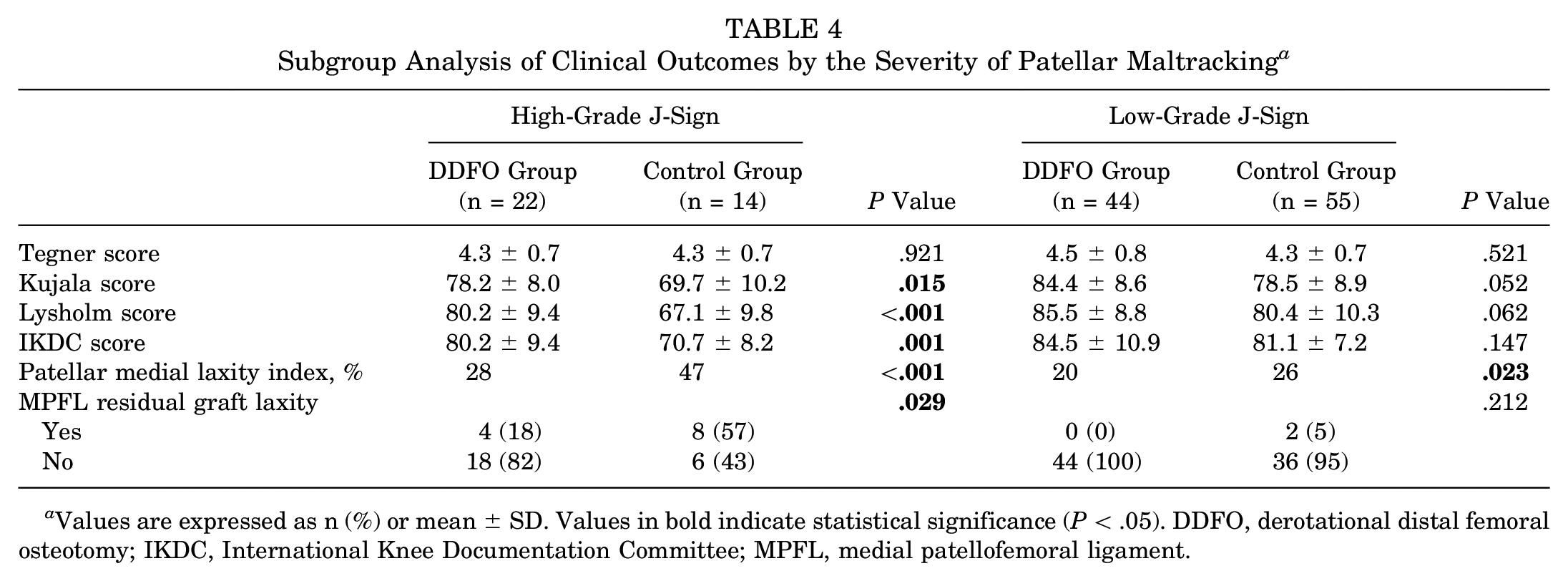
Values are expressed as n (%) or mean ± SD. Values in bold indicate statistical significance (P < .05). DDFO, derotational distal femoral osteotomy; IKDC, International Knee Documentation Committee; MPFL, medial patellofemoral ligament.
The association between residual J-sign and MPFL residual graft laxity was preliminarily analyzed, demonstrating that patients with MPFL residual graft laxity (n = 14) had a significantly higher rate of residual J-sign than did those who had normal patellar stability (100% vs 43%; P < .001).
No patients in either group experienced subjective patellar redislocation or other major complications, such as delayed union or nonunion, during the follow-up period.
Discussion
The most important finding of this study was that patients who underwent MPFL-R with DDFO had better subjective and objective outcomes than did those who underwent MPFL-R without DDFO in the treatment of RPD with increased femoral anteversion. Furthermore, this circumstance was more remarkable when the patients had a preoperative high-grade J-sign.
The optimal treatment for RPD with increased FAA remains controversial. Some authors believe that the reconstructed MPFL is so strong that it is sufficient to treat patients with an increased FAA; therefore, the isolated MPFL-R is becoming increasingly popular among surgeons because the procedure is less invasive. Erickson et al 9 reported a significant improvement in outcome scores with a low redislocation rate (1.1%) after isolated MPFL-R, regardless of the FAA. Similarly, in the study by Blanke et al, 1 isolated MPFL-R resulted in superior clinical outcomes and patellofemoral stability, irrespective of the value of the FAA.
In contrast, other authors have deemed that combined MPFL-R and DDFO should be performed in patients with an increased FAA, and the rationality of DDFO in treating these patients has been investigated. Recent biomechanical research found that the isolated MPFL-R was insufficient to address patients with an increased FAA. 16 Franciozi et al 11 found that an FAA >30° was associated with an inferior outcome in patients with RPD when treated using MPFL-R with tibial tubercle transfer. This was in line with a recent study by Zhang et al, 33 and the authors speculated that patients with an excessive FAA (>30°) were potential candidates for DDFO. Therefore, the MPFL-R with DDFO might be a more suitable procedure than isolated MPFL-R for these patients.
Several studies have reported the clinical outcomes of the DDFO in treating patients with RPD.12,14,20,30,31 Nelitz et al 20 performed a combined DDFO and MPFL-R in 12 patients with RPD and increased FAA (>25°), which resulted in a favorable clinical outcome and good patient satisfaction. In the study by Frings et al, 12 16 patients underwent DDFO to correct the increased FAA, and significant improvements of knee function and activity level were achieved. Similarly, Zhang et al 31 performed DDFO and combined procedures in 47 patients with an FAA >30°, and no patellar redislocation was noted during the follow-up. To date, no comparative study has been conducted to investigate whether patients with an increased FAA could benefit from the combined MPFL-L and DDFO. The present study, for the first time, made a direct comparison between different treatments and found that patients who underwent combined MPFL-L and DDFO showed a lower rate of MPFL residual laxity and better patient-reported outcomes than did those who underwent MPFL-R without DDFO, which clearly demonstrated the advantage of DDFO over non-DDFO procedures in treating RPD with increased FAA. The uncorrected increased FAA might produce a persistent overlateralizing force vector on the patella after MPFL-R and even lead to graft laxity failure,15,16 which might partially explain the observed difference about the MPFL residual graft laxity between these 2 groups. Therefore, it would be rational to perform DDFO to neutralize the force vector produced by femoral torsion, protect the MPFL-R, and prevent iatrogenic patella squinting.13,15,16,21,27
Another confusing issue confronting surgeons is to what extent the increased FAA needs to be addressed. 16 A recent study by Zhang et al 33 reported that patients with a higher FAA (>30°) had worse patellar stability and lower patient-reported outcomes than did those who had an FAA <30°. The authors recommended that patients with an excessive FAA (>30°) are potential candidates for DDFO. In another study, 32 patients with a high-grade J-sign had significantly inferior subjective and objective outcomes than did patients with a low-grade J-sign, indicating that a high-grade J-sign should be considered a surgical indication for DDFO.
Motivated by these findings, the present study was conducted with the aim of directly comparing and analyzing the merits of these 2 entirely different surgical procedures (MPFL-R vs MPFL-R + DDFO), which were performed in different periods but with the same indication. The results were consistent with those of previous studies,31-33 showing that in the treatment of RPD with increased FAA (>30°) and concurrent high-grade J-sign, MPFL-R alone or with tibial tubercle transfer yielded high rates of MPFL residual graft laxity and residual patellar maltracking.
Another interesting finding of this study was that for patients with an increased FAA (>30°) and concurrent low-grade J-sign, the control group and DDFO group had similar subjective and objective outcomes. Thus, not all of the patients with an increased FAA (>30°) needed the aggressive DDFO procedure: indeed, patients with a low-grade J-sign can be successfully treated using MPFL-R alone or with tibial tubercle transfer, and adding DDFO is indicated only for patients with a high-grade J-sign.
Bearing in mind the concepts of femoral torsional deformity and patellar maltracking, we believe that cases with concurrent excessive FAA and a high-grade J-sign pose a challenging scenario in the RPD spectrum, as described previously and also observed in the present study. 31 On the basis of our findings, we believe that FAA and patellar tracking should be identified and that their severity should be surgically corrected using more extensive procedures, such as DDFO, rather than using MPFL-R alone or with tibial tubercle transfer.
The clinical relevance of the present study is as follows: (1) accurate assessment of the severity of FAA and patellar maltracking is vital to surgical decision making for patients with RPD; (2) adding DDFO should be considered for patients with an increased FAA (>30°) and concurrent high-grade J-sign; (3) MPFL-R alone or with tibial tubercle transfer is sufficient when treating patients with an increased FAA and concurrent low-grade J-sign; (4) these results may provide additional information for counseling patients on MPFL residual graft laxity and risk of redislocation after MPFL-R.
There are several limitations to this study. First, the subjective nature of the J-sign grading should be regarded as the main limitation. Both the examiner’s interpretation and the quadriceps contraction force might affect the final grading of patellar maltracking. Second, MPFL residual graft laxity was assessed using stress fluoroscopy, which made it less likely to be popular with surgeons. Third, the mean follow-up time in the DDFO group was significantly shorter than that in the control group (3.1 vs 4.2 years), which might reduce the comparability of the results between the 2 groups. Fourth, the present study was retrospective in nature and not randomized.
Conclusion
In this retrospective study, the treatment of RPD with increased femoral anteversion using MPFL-R combined with DDFO yielded more favorable subjective and objective outcomes than did MPFL-R without DDFO, and this circumstance was more remarkable when the patients had a preoperative high-grade J-sign.
Footnotes
Submitted May 2, 2020; accepted August 10, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by Beijing Natural Science Foundation (L192051), Beijing Municipal Science & Technology Commission (No. Z181100001718106), and Capital Health Development Research Project (2020-1-2071). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.