
Abstract
Background:
Although a variety of pathologic conditions associated with osteochondritis dissecans (OCD) have been reported, the pathological progression has remained unclear.
Hypothesis:
Separation of the immature epiphyseal cartilage is an early event in OCD, and osteonecrosis in the articular fragment is a late event.
Study Design:
Case Series; Level of evidence, 4.
Methods:
The participants were 26 boys (mean age, 13.8 years; mean skeletal age score for the elbow, 24.6 points) with capitellar OCD who underwent osteochondral autograft transplantation. A total of 28 cylindrical osteochondral plugs, including the articular fragment, an intermediate layer, and proximal epiphyseal bone, were harvested from the central area of the capitellum and were examined histologically. The articular fragments of OCD were independently assessed by 5 observers and divided into 4 pathological variations: IA, nearly normal-cartilaginous; IB, deteriorated-cartilaginous; IIA, cartilage-ossifying; and IIB, cartilage-osteonecrotic. The reliability of assessment and the correlation of the pathological variations with the clinical data were examined.
Results:
The reliability of the assessment among 5 observers was almost perfect (Cohen kappa value = 0.91). OCD variations of IA, IB, IIA, and IIB were evident in 5, 10, 5, and 6 patients, respectively. OCD-I (cartilaginous) and OCD-II (osteochondral) corresponded significantly to radiographic stage I (radiolucency or slight calcification with open physis) and stage II (delayed ossification or bony fragment), respectively (Cohen kappa value = 0.79; percentage agreement = 81%). The pathological OCD variations were significantly correlated with the clinical data, including the period from symptom onset to surgery, patient age, and the skeletal age score (P < .01, in each).
Conclusion:
The present study has revealed that the pathological variations correspond to the progression of OCD, thus proving our hypothesis. OCD-IA was shown to be an early lesion caused by separation of the immature epiphyseal cartilage. OCD-IB appeared to result from ossification arrest over a prolonged period from the onset of OCD-IA, whereas OCD-IIA showed delayed ossification in the epiphyseal cartilage where vascularization from the surrounding bone had been established. Osteonecrosis in OCD-IIB was shown to be a late pathological event caused by disruption of the vascular supply to OCD-IIA.
Osteochondritis dissecans (OCD) of the elbow is a localized disorder of the articular cartilage and subchondral bone that commonly arises in young athletes.22,26 Many authors have advocated that an accepted cause of OCD is either acute or repetitive microtrauma applied to the immature epiphysis during sports, making the lesions unstable. ‖ On the other hand, several reports suggested a link between OCD and hereditary familial factors.28,31,33
A variety of pathologic conditions associated with OCD have been reported, such as chondral injury,2,3,17,19,39 cartilage degeneration,12,15,42 ossification defects,1,2,3 osteochondral fractures,9,41 nonunion, 42 and avascular necrosis.16,21,24,27,40,41 However, the natural pathological progression of OCD has remained unclear; for example, it remains controversial whether osteonecrosis is an early5,16,20,41 or late4,17 event.
Radiography, ultrasound, and magnetic resonance imaging have revealed that OCD shows natural progression through several stages: I, localized subchondral bone flattening of the epiphysis before growth plate closure; IIA, delayed ossification over the flattened bone; and IIB, fragmentation and displacement of the fragment.23,36,37,38 We hypothesized that incomplete separation of the immature epiphyseal cartilage is an early event in OCD, and osteonecrosis in the articular fragment is a late event. The aim of this study was to clarify the pathological progression of OCD.
Methods
This study of a case series was approved by our institutional review board.
Participants and Preoperative Clinical Data
A total of 123 elbows in 123 patients aged under 20 years were diagnosed to have OCD of the capitellum at a single institute (Izumi Orthopaedic Hospital) between July 2015 and December 2019. Thirty-four patients who were assessed to have a stable OCD were treated nonoperatively, and 9 of the 34 patients underwent surgery after failed nonoperative treatment of more than 90 days. A total of 81 patients who were assessed to have an unstable OCD lesion underwent surgery within 90 days after the initial presentation. The remaining 8 patients visited our outpatient clinic only a few times and did not undergo any surgery or nonoperative treatment for more than 90 days. Overall, 90 patients with OCD of the capitellum underwent surgery during the study period. We performed arthroscopic removal of the lesion for 39 elbows, and osteochondral autograft transplantation (OAT) was performed for 51 elbows that had a large OCD lesion more than 12 mm in width, principally. 22 Of these 51 elbows, 26 met the inclusion criteria: (1) the detachment of the articular fragment from the capitellum was not complete but partial; and (2) both the articular fragment and the underlying bone were simultaneously harvested from the center of the capitellum using a cylindrical chisel of the OAT system. The remaining 25 elbows were excluded from the analysis because of complete detachment (2 elbows) or separate harvest (23 elbows).
The participants in the present study were 26 boys with an average age at surgery of 13.8 years (range, 10.6-16.7 years). The mean skeletal age score for the elbow using the Sauvegrain method (0-27 points system)7,30 was 24.6 points (range, 16-27 points). The capitellar growth plate was open in 3 elbows, and 10 elbows were assessed as fully mature with a score of 27 points. The mean age at onset of lateral elbow pain was 12.0 years (range, 10.4-13.6 years), and the mean period from the onset of pain to surgery was 1.8 years (range, 0.2-4.5 years).
All patients had belonged to sports clubs and played competitive games. The preoperative sport was baseball in 22 cases (11 pitchers, 7 catchers, and 12 fielders, including 8 overlaps), tennis in 2 cases, badminton in 1 case, and shot put in 1 case.
On the anteroposterior radiograph of the elbow at 45° of flexion, the capitellar OCD lesions were assessed as the following radiographic OCD stages: I, radiolucency or slight calcification with open physis23,36; II, delayed ossification or bony fragment23,36; and III, normal or bony union of the delayed ossified fragment with the surrounding bone. The stages of the lateral area (lateral wall side) and central area (articular side) in each capitellum were assessed, respectively, because the central area was the target of the OAT.
Five patients who preoperatively had nonoperative treatment with a mean of 14.4 months (range, 3-33 months) initially had radiographic stage I in both lateral and central areas. During the observation period, the central area remained at stage I in 4 cases (Figure 1, B, D, and F) and progressed to stage II in 1 case (Figure 1H), although the lateral area progressed to stage II in 2 cases (Figure 1, D and H) and stage III in 2 cases (Figure 1F and Table 1). Overall, the preoperative radiographic stage of the central area of the capitellum was I in 14 cases and II in 12 cases, and that of the lateral area was I in 2, II in 18, and III in 6 cases.
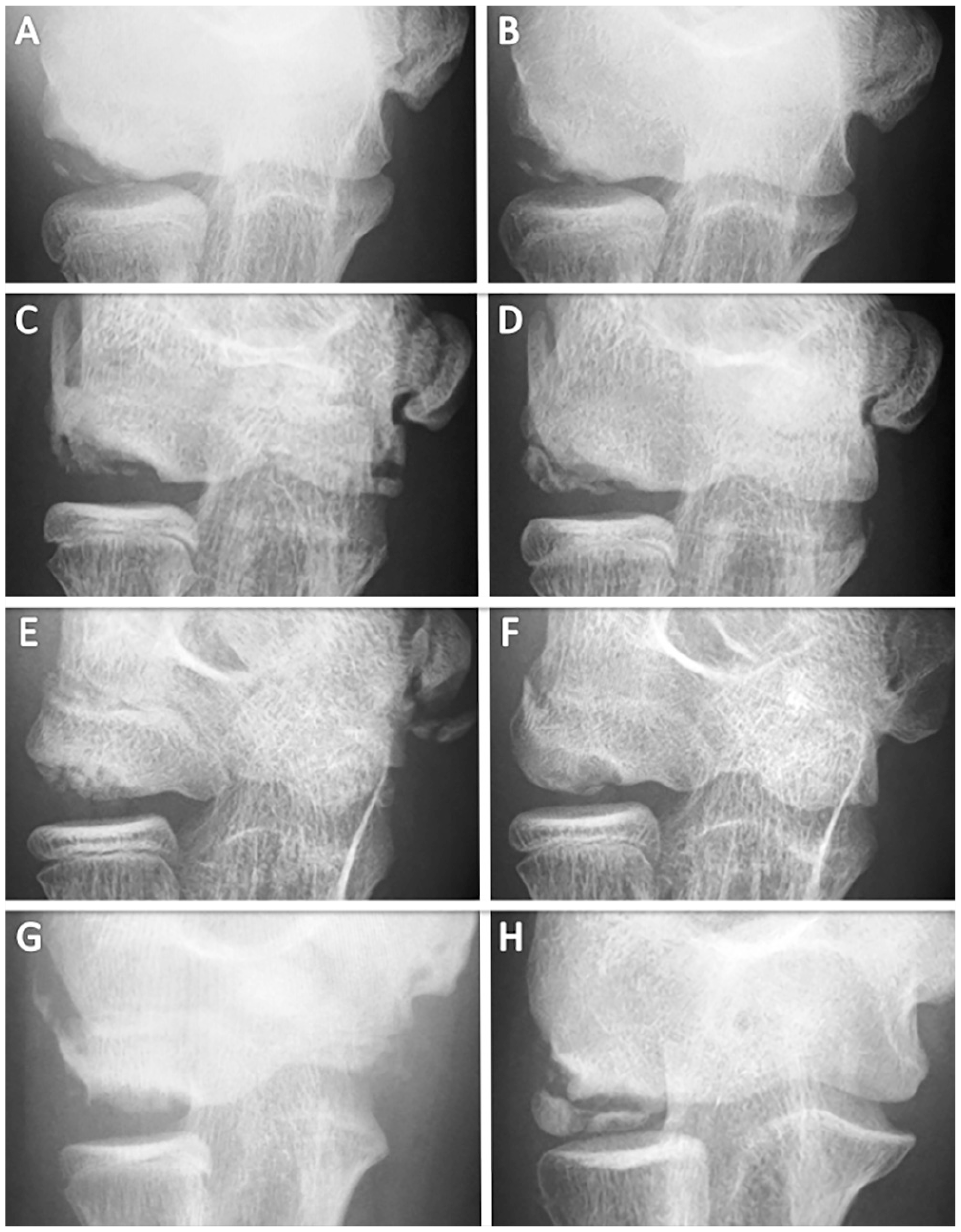
Anteroposterior radiographs of the elbow at 45° of flexion showing changes of the capitellar OCD. Radiographs at (A, C, E, G) initial presentation and (B) after an observation period of 3 months, (D) 4 months, (F) 9 months, and (H) 33 months. (A, B) No significant change of radiographic OCD stage I (radiolucency or slight calcification with open physis). (C, D) Change from stage I to stage II (delayed ossification or bony fragment) in the lateral area of the capitellum and no change of stage I in the central area. (E, F) Change from stage I to stage III (bony union) of the lateral area of the capitellum and no change of stage I of the central area. (G, H) Change from stage I to stage II of the lateral and central areas of the capitellum. OCD, osteochondritis dissecans.
Changes of Radiographic Stage in 5 Cases With Preoperative Observation a
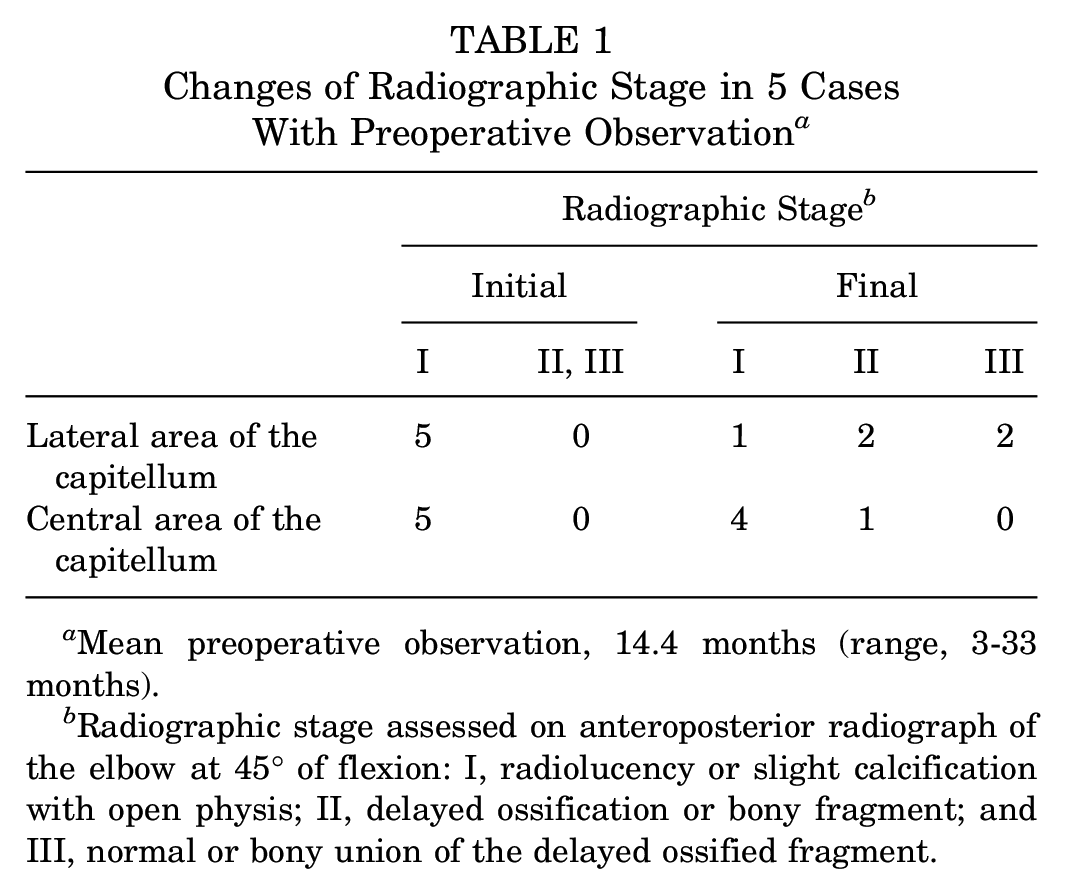
Mean preoperative observation, 14.4 months (range, 3-33 months).
Radiographic stage assessed on anteroposterior radiograph of the elbow at 45° of flexion: I, radiolucency or slight calcification with open physis; II, delayed ossification or bony fragment; and III, normal or bony union of the delayed ossified fragment.
Surgical Procedure
All 26 patients had a partially detached articular fragment from its normal site at the capitellum, and 4 patients additionally had completely detached fragments. Intraoperative assessment of the capitellar OCD showed that the International Cartilage Repair Society (ICRS)–OCD grade of instability was I in 1 patient, II in 5 patients, III in 9 patients, and IV in 11 patients.
All patients underwent open OAT. The number of grafted plugs was 1 in 24 cases and 2 in 2 cases. With use of a cylindrical chisel of 7 mm in diameter, 28 cylindrical osteochondral plugs, including the articular fragment, an intermediate layer, and the underlying proximal epiphyseal bone, were harvested from the central area of the capitellum (Figure 2). The capitellar bone component of 8 plugs was reused intraoperatively as a graft material and not used for histological examination.
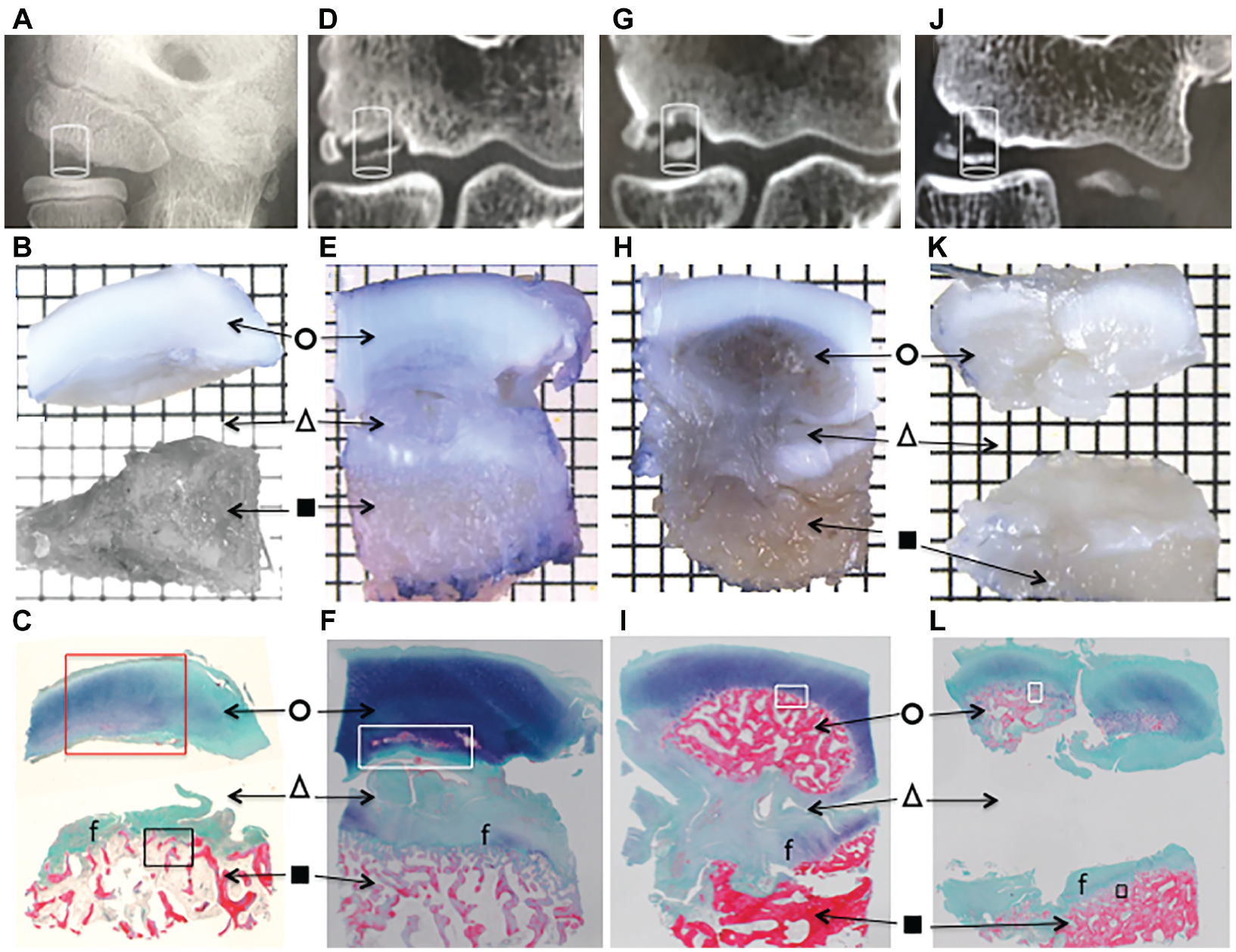
Radiographs, osteochondral plugs, and histological photographs of the capitellar OCD of (A-C) a 10.6-year-old boy, (D-F) a 14.8-year-old boy, (G-I) a 14.2-year-old boy, and (J-L) a 16.7-year-old boy. (A, D, G, J) Cylinder on the anteroposterior radiographs of the elbow at 45° of flexion indicating the osteochondral plug to be harvested from the central area showing radiographic OCD (A, D) stage I and (G, J) stage II. (B, E, H, K) Harvested cylindrical osteochondral plugs sectioned longitudinally in half. (C, F, I, L) Histological photographs with Elastica-Masson staining. The osteochondral plugs are composed of the articular fragment (○), an intermediate layer (△), and proximal epiphyseal bone (▪). Articular fragments are divided into 4 variations: (C) OCD-IA, nearly normal-cartilaginous; (F) OCD-IB, deteriorated-cartilaginous; (I) OCD-IIA, cartilage-ossifying; and (L) OCD-IIB, cartilage-osteonecrotic. Separation beneath the articular fragment is (C, L) complete, (F) incomplete by half or more, and (I) less than half. The proximal epiphyseal bone is covered by fibrocartilage (f). OCD, osteochondritis dissecans.
Histological Examination
Twenty osteochondral plugs and 8 articular fragments were fixed immediately with 10% formalin, decalcified, sectioned longitudinally in half, and embedded in paraffin. The tissues were then sectioned at a thickness of 5 µm, and subjected to hematoxylin and eosin and Elastica-Masson staining (Figure 2), followed by a light microscopy examination by an experienced pathologist who was blinded to the clinical data.
On the basis of the pathological images and reports, the first author (M. Takahara) divided 28 articular fragments into the following characteristic variations. The articular fragments were grossly divided into 2 types based on the absence or presence of a bony component: OCD-I (cartilaginous) and OCD-II (osteochondral). OCD-I (cartilaginous) articular fragments were subdivided into 2 types: OCD-IA, nearly normal-cartilaginous with or without slight calcification in the epiphyseal cartilage (Figures 2C and 3); and OCD-IB, deteriorated-cartilaginous with degradation or degeneration in the epiphyseal cartilage, such as local chondrolysis and excessive calcification (Figures 2F and 4). OCD-II (osteochondral) articular fragments were subdivided into 2 types: OCD-IIA, cartilage-ossifying with endochondral ossification at the cartilage-bone interface (Figures 2I and 5); and OCD-IIB, cartilage-osteonecrotic with empty lacunae of the bone matrix and deterioration of the bone matrix and marrow (Figures 2L and 6).
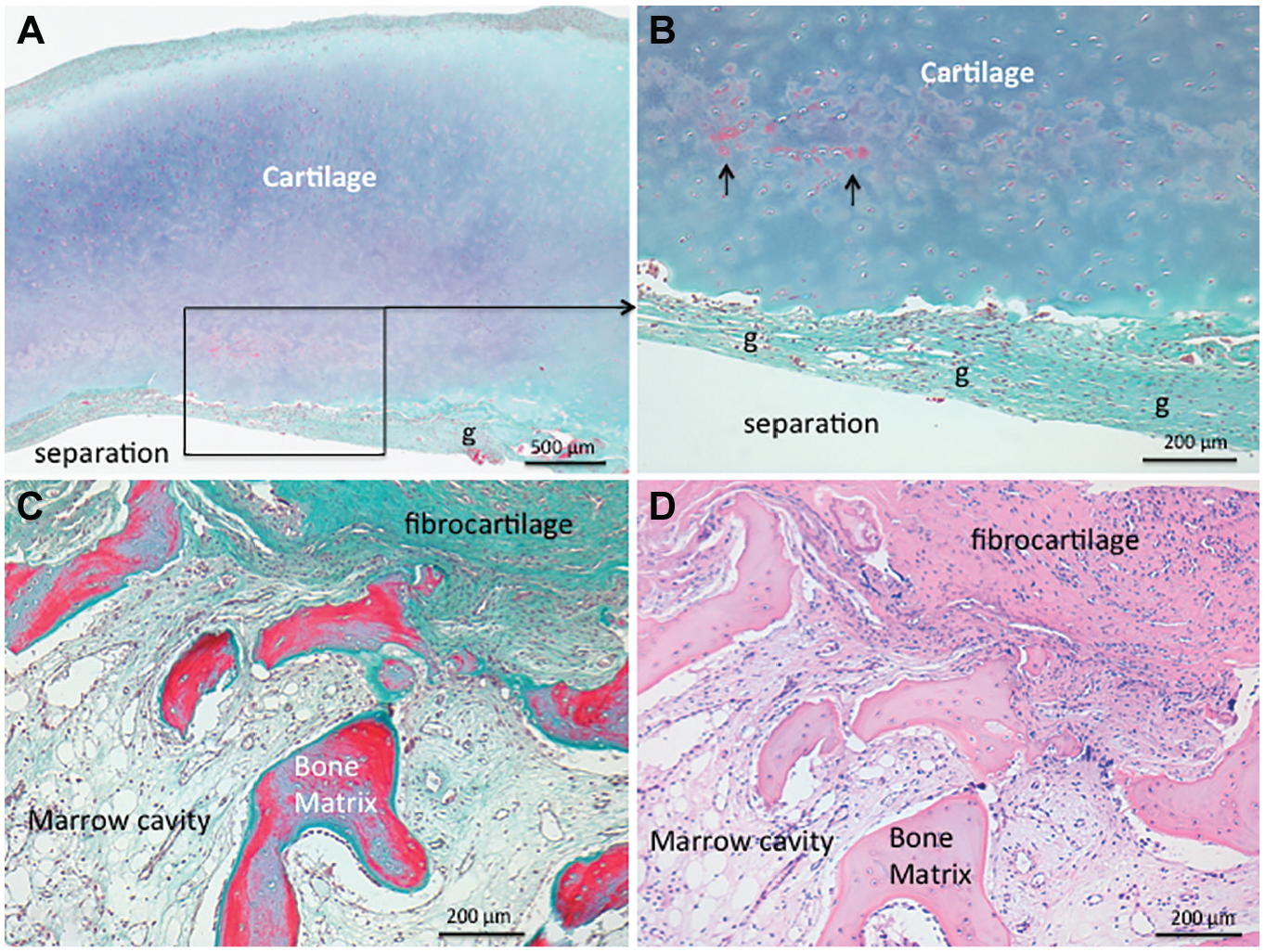
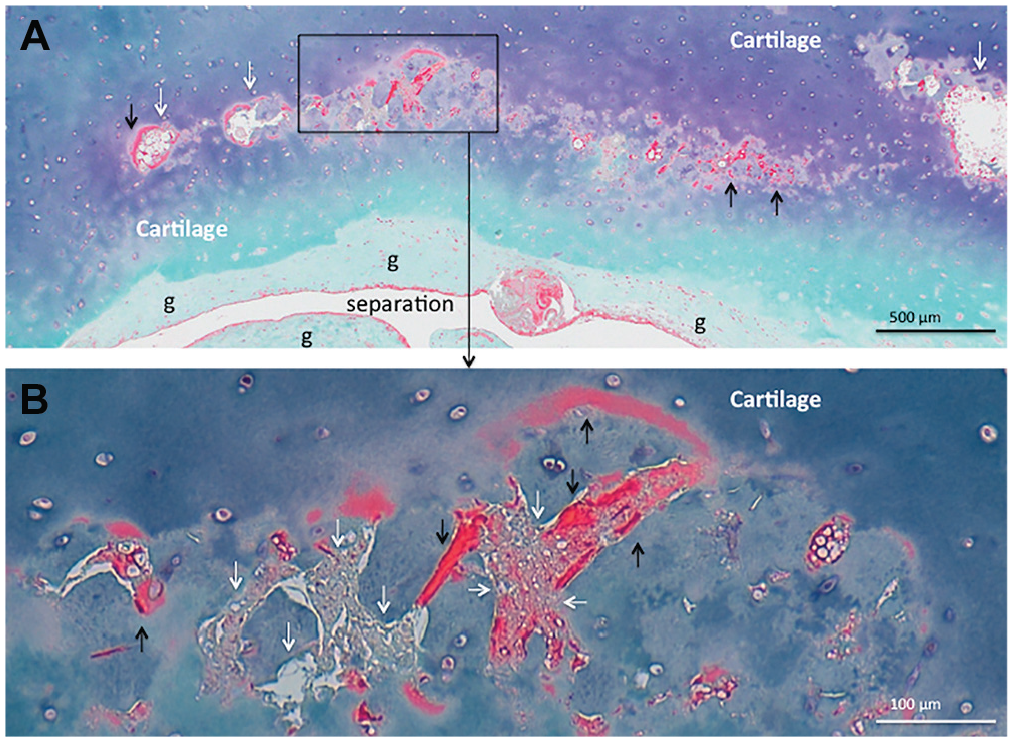
(A) High-magnification image of the area surrounded by the red square in the histological photograph (Figure 2C) with Elastica-Masson staining of a specimen harvested from a 10.6-year-old boy. (A, B) OCD-IA, nearly normal-cartilaginous, articular fragment with slight calcification (black arrows) is not followed by ossification. Separation is complete beneath the articular fragment covered by granulation tissue (g). (C) High-magnification image of the area surrounded by the black square (Figure 2C) showing proximal epiphyseal bone and overlying fibrocartilage. The bone is living. Bone matrix is stained red. (D) Histological photograph of the same area with hematoxylin and eosin staining showing living bone.
(A) High-magnification image of the area surrounded by the white square in the histological photograph (Figure 2F) with Elastica-Masson staining of a specimen harvested from a 14.8-year-old boy. (A, B) OCD-IB, deteriorated-cartilaginous, articular fragment has chondrolysis (white arrows) and excessive calcification (black arrows) where endochondral ossification has not followed. There is separation and granulation tissue (g) in the intermediate layer.

High-magnification image of the area surrounded by the white square of the histological photograph (Figure 2I) with Elastica-Masson staining of a specimen harvested from a 14.2-year-old boy. OCD-IIA articular fragment is composed of cartilage and ossifying subchondral bone with osteocytes (white arrows), osteoblasts, osteoclasts, and endochondral ossification at the cartilage-bone interface. Bone matrix is stained red.
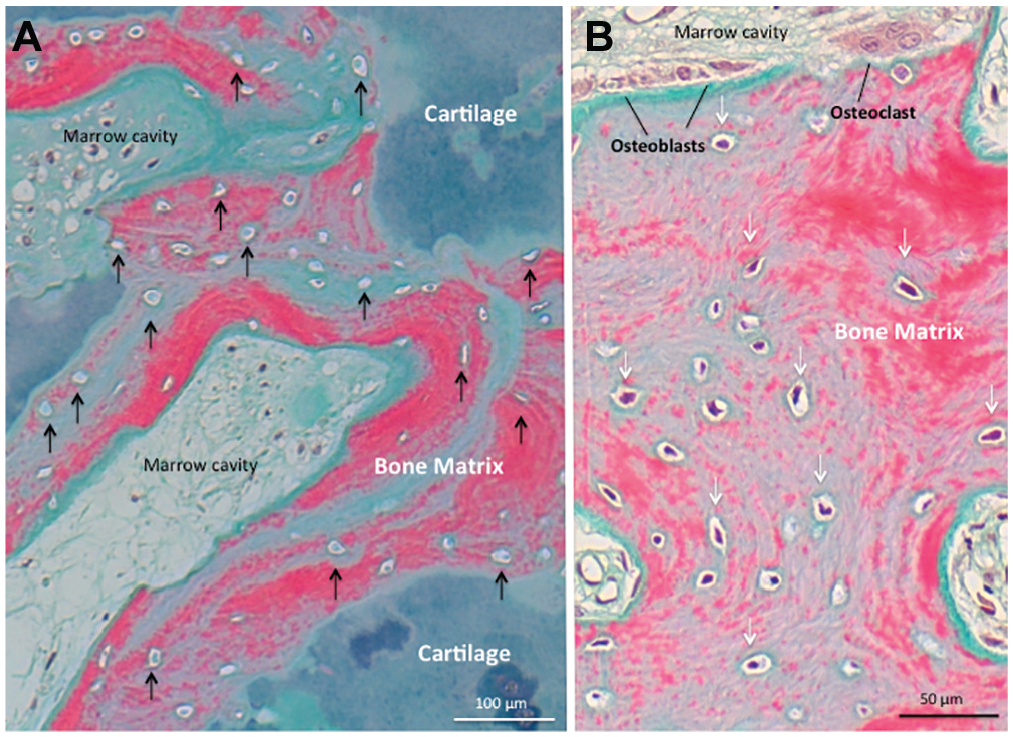
(A) High-magnification image of the area surrounded by the white square in the histological photograph (Figure 2L) with Elastica-Masson staining of a specimen harvested from a 16.7-year-old boy. OCD-IIB articular fragment is composed of cartilage and subchondral bone with many empty lacunae (black arrows) in the bone matrix (stained red) and decreased number of cells in the marrow cavity. (B) High-magnification image of the area surrounded by the black square in the histological photograph (Figure 2L) with Elastica-Masson staining showing normal viability of the proximal epiphyseal bone, including osteocytes (white arrows) in the bone matrix (stained red) and osteoclasts, osteoblasts, and marrow cells in the marrow cavity.
Four co-authors, who were blinded to the clinical data and pathological reports, independently assessed the pathological images of 28 articular fragments and divided them into the 4 variations according to the above-mentioned characteristics. All 5 observers, including 4 sports doctors (M. Takahara, M.M., T.U., and M.H.) and 1 musculoskeletal oncologist (D.T.), had experience with histological studies on cartilage and bone.
Data Analysis
To examine the reliability of assessment among the 5 observers, Cohen kappa values and percentage agreements were calculated. Kappa values were classified with values of 0.81-1.00 indicating almost perfect agreement, 0.61-0.80 indicating substantial agreement, 0.41-0.60 indicating moderate agreement, 0.21-0.40 indicating fair agreement, and 0-0.20 indicating slight agreement. 18 For articular fragments assigned different variations, the final variation adopted was that suggested by the majority of observers.
To address the pathological progression of OCD, we examined the correlation between the pathological variations and the clinical data, including the period from symptom onset to surgery, patient age, and the skeletal age score for the elbow, by Spearman rank correlation. Differences in the clinical data between 2 groups and among the 4 pathological variations were analyzed by Mann-Whitney U test and Kruskal-Wallis test followed by Bonferroni correction, respectively.
To examine the correspondence between pathological variation and radiographic stage, Cohen kappa values and the percentage agreements were calculated. To investigate the effect of the underlying separation, we compared the relationship between the articular fragment and the underlying separation, and the differences between 2 groups were analyzed by the Fisher exact test. All statistical analyses were performed using EZR 13 Version R-3.6.1 and significance was set at P≤ .05.
Results
Part 1: Articular Fragment
For 22 (79%) articular fragments, there was total agreement on the assessment among the 5 observers. For the remaining 6 (21%) articular fragments, the assessment was the same among 4 of the observers. The interobserver reliability was considered to be almost perfect, with a mean Cohen kappa value of 0.91 (range, 0.81-1.00) and a mean percentage agreement of 91% (range, 82%-100%). The final assessment of the 28 articular fragments was OCD-IA in 5 patients, OCD-IB in 11 patients, OCD-IIA in 6 patients, and OCD-IIB in 6 patients. Among the 26 patients, 5 had OCD-IA, 10 had OCD-IB, 5 had OCD-IIA, and 6 had OCD-IIA.
Part 2: Intermediate Layer Between the Articular Fragment and the Proximal Epiphyseal Bone
None of the specimens showed an osseous connection between the articular fragment and the proximal epiphyseal bone. There were various degrees of separation and fibrocartilage connection between them (Figure 2, C, F, I, L): complete separation without connection (complete separation) in 14 specimens; incomplete separation by half or more (separation ≥ connection) in 4 specimens; incomplete connection by more than half (connection > separation) in 5 specimens; fibrocartilage connection without separation (complete connection) in 3 specimens, and unknown in 2 specimens.
Part 3: Proximal Epiphyseal Bone
The viability of the proximal epiphyseal bone appeared to be normal in all 20 specimens examined, and its surface was covered by the fibrocartilage (Figure 2, C, F, I, L). Active ossification was observed at the interface of the fibrocartilage and bone.
Clinical Data and Pathological Variations
Table 2 shows the differences in the clinical data between pathological OCD-I and OCD-II. Patients with OCD-I, compared with those with OCD-II, were younger (13.3 years vs 14.5 years; P = .040) with a significantly lower skeletal age score (23.3 points vs 26.3 points; P = .013) and had a significantly shorter time from symptom onset to surgery (1.4 years vs 2.4 years; P = .032). OCD-I and OCD-II significantly corresponded to radiographic stage I (radiolucency or slight calcification with open physis) and stage II (delayed ossification or bony fragment), respectively (P < .01; substantial agreement with a Cohen kappa value of 0.79 and the percentage agreement of 81%).
Clinical Data for Pathological OCD-I and II a
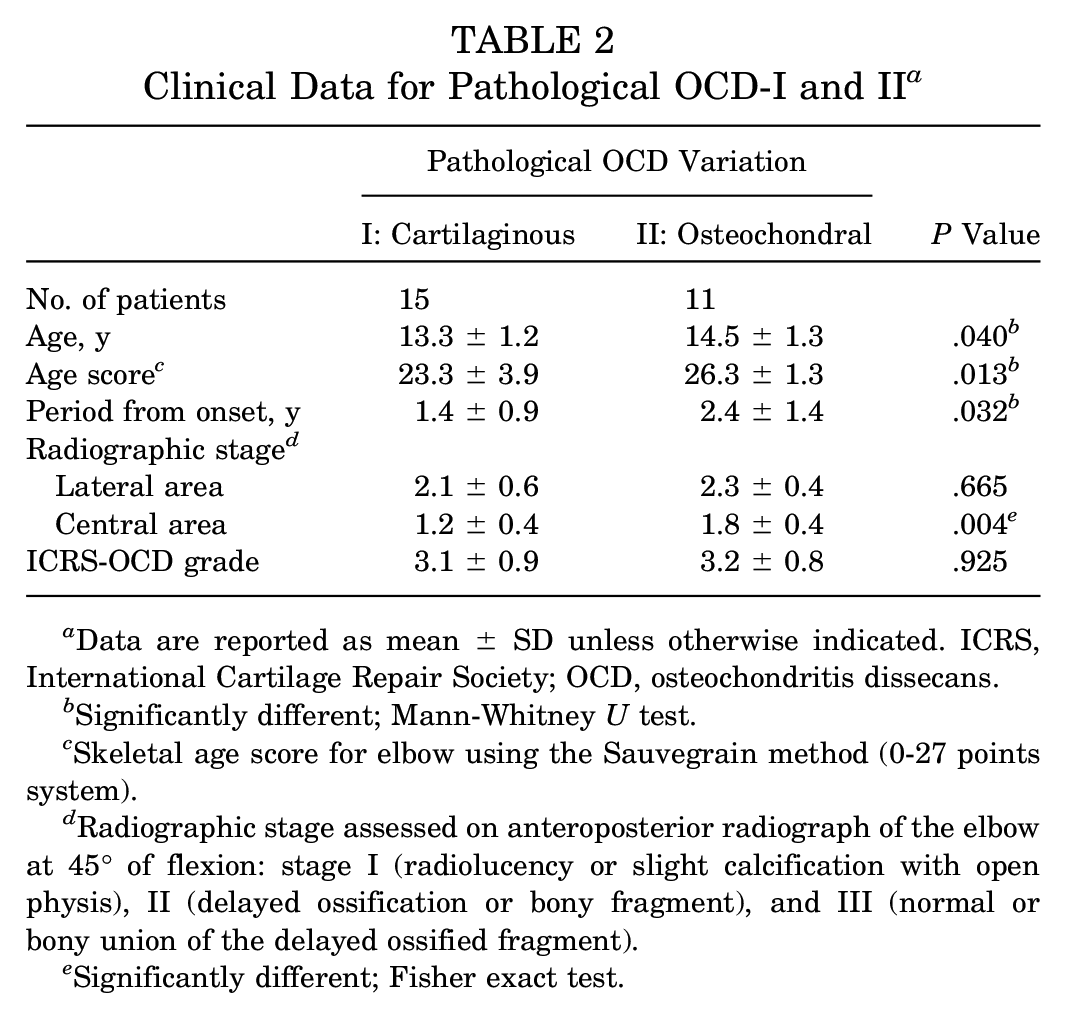
Data are reported as mean ± SD unless otherwise indicated. ICRS, International Cartilage Repair Society; OCD, osteochondritis dissecans.
Significantly different; Mann-Whitney U test.
Skeletal age score for elbow using the Sauvegrain method (0-27 points system).
Radiographic stage assessed on anteroposterior radiograph of the elbow at 45° of flexion: stage I (radiolucency or slight calcification with open physis), II (delayed ossification or bony fragment), and III (normal or bony union of the delayed ossified fragment).
Significantly different; Fisher exact test.
Figure 7 and Table 3 show significant correlations between the pathological variations and the following clinical data: the period from symptom onset to surgery (P < .01), patient age (P < .01), and the skeletal age score for the elbow (P < .001). The skeletal age score of patients with OCD-IA, compared with that of patients with OCD-IIB, was significantly lower (Bonferroni correction, P = .033). In contrast, there were no significant differences in the age at symptom onset or ICRS grade between patients with OCD-I and OCD-II, or among those with OCD-IA, OCD-IB, OCD-IIA, and OCD-IIB.
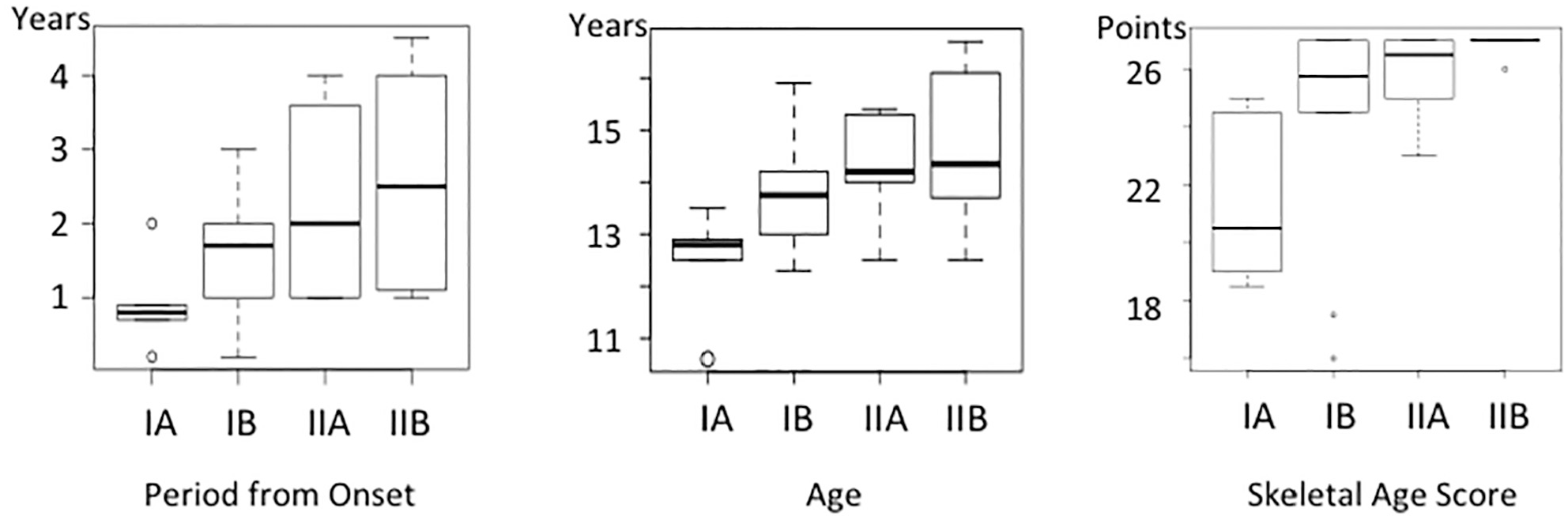
Correlations between pathological variations and clinical data: the period from symptom onset to surgery, patient age, and the skeletal age score for the elbow. OCD-IA, nearly normal-cartilaginous; IB, deteriorated-cartilaginous; IIA, cartilage-ossifying; IIB, cartilage-osteonecrotic.
Clinical Data for Pathological OCD-IA, IB, IIA, and IIB a
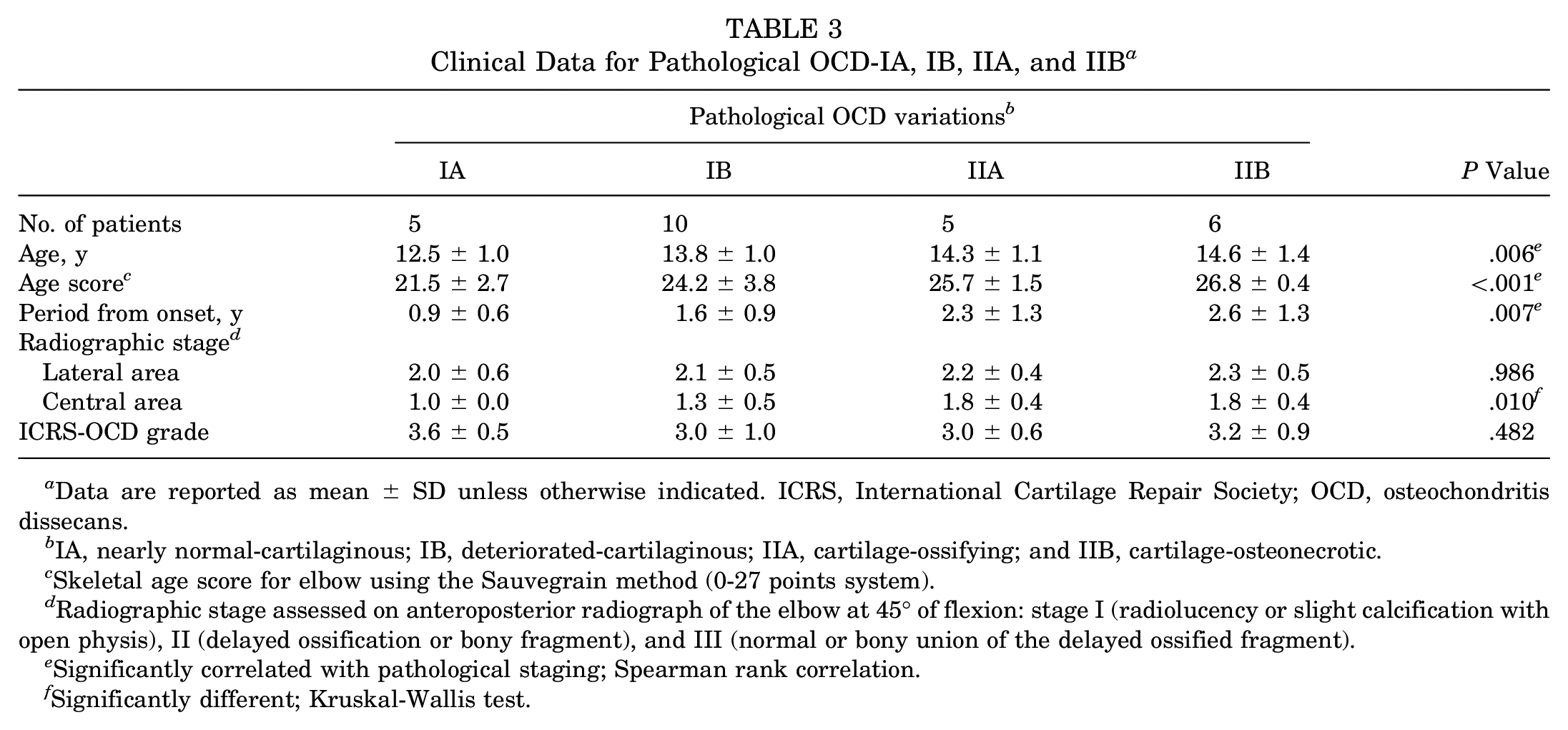
Data are reported as mean ± SD unless otherwise indicated. ICRS, International Cartilage Repair Society; OCD, osteochondritis dissecans.
IA, nearly normal-cartilaginous; IB, deteriorated-cartilaginous; IIA, cartilage-ossifying; and IIB, cartilage-osteonecrotic.
Skeletal age score for elbow using the Sauvegrain method (0-27 points system).
Radiographic stage assessed on anteroposterior radiograph of the elbow at 45° of flexion: stage I (radiolucency or slight calcification with open physis), II (delayed ossification or bony fragment), and III (normal or bony union of the delayed ossified fragment).
Significantly correlated with pathological staging; Spearman rank correlation.
Significantly different; Kruskal-Wallis test.
Articular Fragment and Intermediate Layer
Figure 8 shows the proportions of the various degrees of separation beneath the articular fragments. The fibrocartilage connection was dominant (complete connection or connection > separation) in 20% of OCD-IA, 9.1% of IB, 100% of IIA, and 33.3% of IIB. OCD-IIA, compared with OCD-I and IIB, was associated with a significantly dominant fibrocartilage connection (100% compared with 18.2%; P < .01).
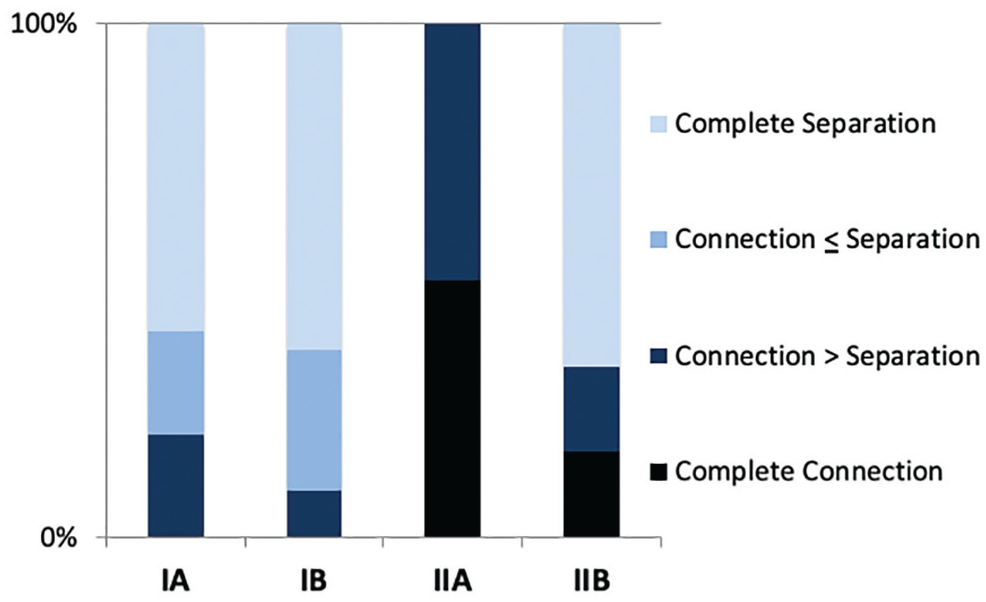
Separation and connection beneath articular fragment. Complete separation: complete separation without connection. Separation ≥ connection: incomplete separation by half or more. Connection > separation: connection by more than half. Complete connection: fibrocartilage connection without separation. OCD-IA, nearly normal-cartilaginous; IB, deteriorated-cartilaginous; IIA, cartilage-ossifying; IIB, cartilage-osteonecrotic.
Discussion
We confirmed the various pathological conditions in the articular fragments of OCD demonstrated in previous studies, ¶ including excessive calcification, cartilage deterioration, ossification defects, delayed ossification, un-united fragment, and osteonecrosis. In contrast, the proximal epiphyseal bone had none of these pathological conditions. The intermediate unstable layer showed various degrees of separation, and fibrocartilage covered the surface of the proximal epiphyseal bone, as commonly seen in previous studies.9,16,17,41,42 It is generally accepted that separation is a crucial pathological condition for the appearance of an articular fragment,2,3,17,19,39,41,42 and that fibrocartilage formation is a common reaction to exposure of the proximal epiphyseal bone.
We divided the articular fragments of OCD into 4 variations: IA, nearly normal-cartilaginous; IB, deteriorated-catilaginous; IIA, cartilage-ossifying; and IIB, cartilage-osteonecrotic. The interobserver reliability of our pathological assessments was considered to be almost perfect, and the pathological variations were significantly correlated with the clinical data, including the period from symptom onset to surgery, patient age, and the skeletal age score for the elbow. These results indicated that the pathological variations corresponded to the progression of OCD, thus proving our hypothesis that separation of the immature epiphyseal cartilage is an early event in OCD, and osteonecrosis in the articular fragment is a late event.
Fairbank 9 suggested that the typical OCD lesion was a fracture. Histological studies17,42 supported that separation may be an early event, although there were no clinical correlations. Experimental results showed that OCD can arise as a sequel of cartilage fracture in the immature epiphysis.19,39 On the basis of clinical correlations, our study clinically demonstrated that the pathological progression of OCD begins with separation beneath the immature epiphyseal cartilage.
The immature epiphysis is composed of the articular cartilage, the epiphyseal cartilage, the secondary ossification center (epiphyseal bone), and the physis (growth plate). 29 An experimental study on the mechanical failures of the physis in immature animals demonstrated that compression forces produced fractures in the zone of provisional calcification and metaphysis, and shear forces caused fractures in the proliferative and hypertrophic zones. 25 The epiphyseal bone forms as a result of the endochondral ossification within the epiphyseal cartilage (Figure 9, 0). 29 Experimental studies on the mechanical properties of the growing epiphysis demonstrated the weakness in the cartilage-bone interface, relative to the articular cartilage and epiphyseal bone, 14 and indicated that the adolescent tissue had a significant reduction in the fracture toughness of its cartilage-bone interface compared with that of the immature or mature tissues. 10 These experimental findings led us to hypothesize that microtrauma on the adolescent capitellum during sports can cause fracture-separation beneath the epiphyseal cartilage (Figure 9, Onset), followed by fibrocartilage formation over the exposed bone surface, leading to OCD-IA (Figure 9, IA).
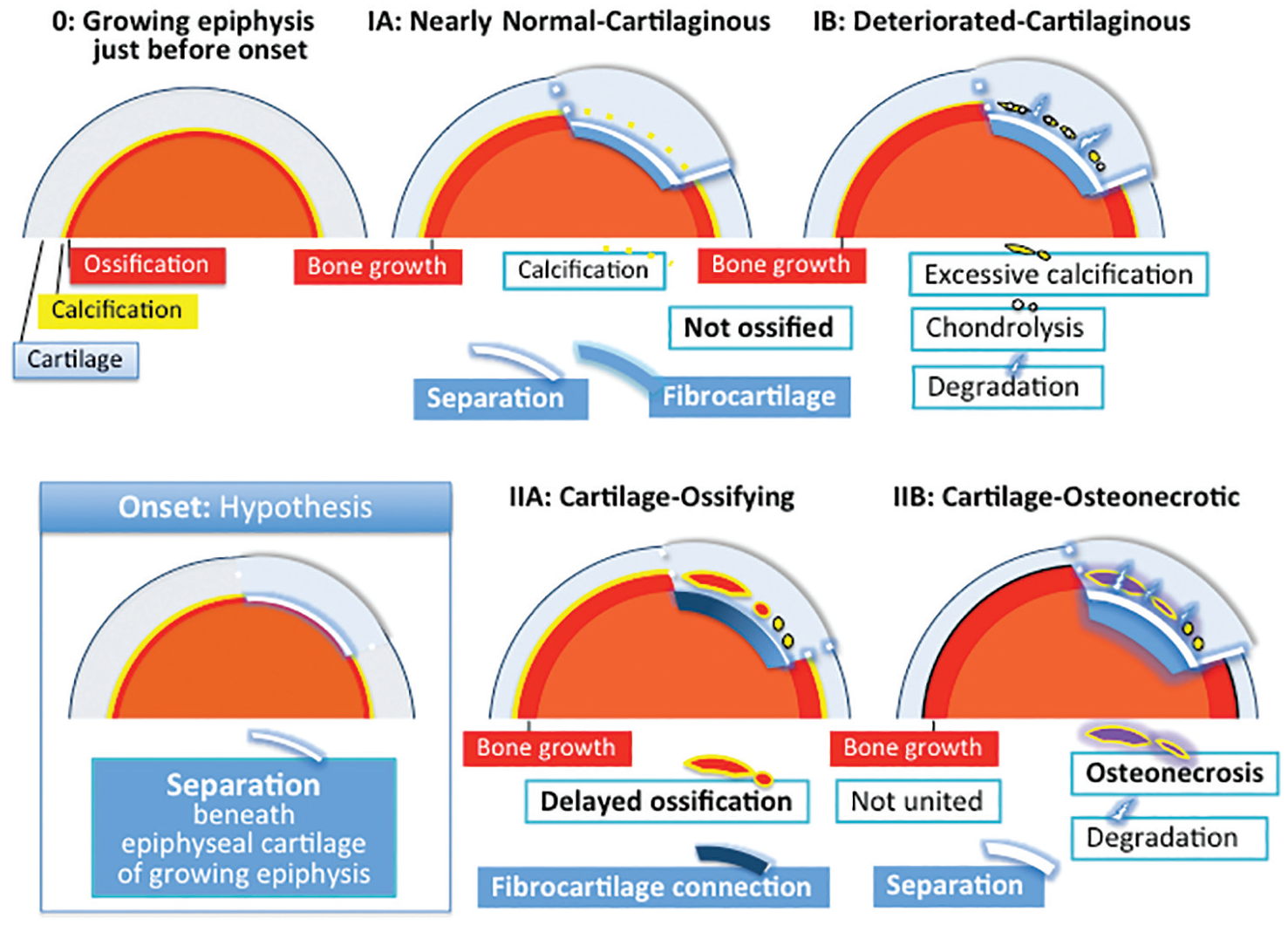
Pathological progression of osteochondritis dissecans (OCD) of the elbow in surgically treated cases. (O) Growing epiphysis just before onset. The epiphysis is composed of cartilage (gray) and a secondary ossification center (orange). Cartilage calcification (yellow) is followed by endochondral ossification (red) at the cartilage-bone interface, which is responsible for the circumferential bone growth. (IA, IB) OCD-I, cartilaginous, articular fragments over separation (space) have not ossified, and are subdivided into OCD-IA, nearly normal-cartilaginous with or without slight calcification (yellow dots); and OCD-IB, deteriorated-cartilaginous, with excessive calcification (yellow particles), chondrolysis, and degradation. (IIA, IIB) OCD-II, osteochondral, articular fragments are composed of cartilage and subchondral bone, the bone being irregular and immature. OCD-II articular fragments are subdivided into OCD-IIA, with endochondral ossification; and OCD-IIB, including osteonecrosis. (IIA) Delayed-ossified bone (red surrounded by yellow) is associated with the fibrocartilage connection (dark blue) to the proximal epiphyseal bone. (IIB) Osteonecrotic bone (purple surrounded by yellow) is characterized by separation (space) and degradation. (Onset) Hypothesis of onset of OCD. Separation (space) beneath the epiphyseal cartilage of the growing epiphysis, followed by fibrocartilage formation over the exposed bone surface, leading to OCD-IA. During the period from onset to surgery, the circumferential bone growth (red) appears, excluding the separated surface covered by fibrocartilage (blue).
The present clinical data showed that OCD-IA (nearly normal-cartilaginous) was followed by OCD-IB (deteriorated-cartilaginous), characterized by deterioration in the epiphyseal cartilage, not followed by endochondral ossification. These findings indicated that OCD-IB resulted from ossification arrest for a prolonged period after onset of OCD-IA, while growth of the surrounding epiphyseal bone occurred as a result of endochondral ossification (Figure 9, IB).
OCD-IIA (cartilage-ossifying) articular fragments included immature and ossifying subchondral bone. The ossification appeared to be delayed relative to the growth of the surrounding epiphyseal bone. Delayed ossification in OCD has often been demonstrated by radiography (Figure 1, D, F, H).23,34-36 It is generally considered that in OCD-IIA, the subchondral bone formed in the epiphyseal cartilage where the vascularization from the surrounding bone had been established. This was supported by the fact that OCD-IIA was associated with a significantly dominant fibrocartilage connection to the proximal bone (Figures 2I and 9, IIA).
The necrotic subchondral bone in OCD-IIB was not fully mature, although the skeletal age score for elbows showed almost full maturity. These results indicated that osteonecrosis in OCD-IIB appeared in the subchondral bone during delayed ossification. In the present pathological progression, OCD-IIB (cartilage-osteonecrotic) followed OCD-IIA (cartilage-ossifying) and was the last variation. It was concluded that the osteonecrosis in OCD-IIB was the last pathological event caused by disruption of the vascular supply to OCD-IIA (Figures 2L, 8, and 9, IIB).
There were several limitations to this study. First, the observers who assessed the articular fragments included no residents or doctors inexperienced in histological study. Second, intraobserver reliability was not examined because the sample size was small. Third, the lateral area of the capitellum was not examined, while the central area of the capitellum was examined in each case. In the lateral area of the capitellar OCD, radiography often demonstrated delayed ossification over the flattened bone and bone union, as shown in previous studies.23,36,38 We could not histologically examine the healing process. Therefore, the pathological progression of OCD described in the present study cannot be applied for all lesions, but only unstable lesions that have partially detached from the normal site at the capitellum and that result in the need for surgery.
We conclude that the pathological progression of OCD begins with separation beneath the immature epiphyseal cartilage, followed by ossification arrest or delay, and that osteonecrosis is a last event (see Figures 2 and 9).
Footnotes
Acknowledgements
The authors sincerely thank Nobuaki Tamahashi, MD, PhD (Director, Surgical Pathology Japan, Inc, Sendai, Japan), for examining the pathological conditions of OCD. They also thank Tadanobu Nemoto, MD (Chief Director, Izumi Orthopaedic Hospital, Sendai, Japan), for his support.
Submitted April 18, 2020; accepted August 10, 2020.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.