
Abstract
Background:
Medial patellofemoral ligament (MPFL) reconstruction is one of the main treatments for lateral patellar translation. Based on intraoperative true lateral radiographs, the accepted methods for femoral MPFL tunnel location are potentially inaccurate. Direct assessment of anatomic characteristics during surgery through palpation of the anatomic landmarks involving the saddle sulcus might help eliminate tunnel malposition.
Hypothesis:
The saddle sulcus is a reliable osseous landmark where the MPFL attaches for tunnel placement.
Study Design:
Descriptive laboratory study.
Methods:
A total of 9 fresh-frozen unpaired human cadaveric knees were dissected; MPFL insertion point and relative osseous structures were marked. Three-dimensional images and transformed true lateral radiographs were obtained for analysis; 3 previously reported radiographic reference points for MPFL femoral tunnel placement were determined on all images and compared with the anatomic insertion.
Results:
A saddle sulcus consistently existed where the MPFL was attached, located at 11.7 ± 5.9 mm from the apex of the adductor tubercle (AT) to the medial epicondyle (ME), 62.8% of the average distance between the apexes of the AT and ME, and 5.6 ± 2.8 mm perpendicular-posterior to the border connecting the AT and ME. The reported radiographic reference points were located at average distances of 6.2 ± 3.2 mm (Schöttle method), 5.9 ± 2.3 mm (Redfern method), and 7.3 ± 6.6 mm (Fujino method) from the saddle sulcus center on the true lateral radiographs.
Conclusion:
The saddle sulcus was a reliable landmark where the MPFL was anatomically attached, located approximately 12 mm from the AT to the ME (approximately 60% along a line from the AT to the ME) and 6 mm perpendicular-posterior to the border connecting the apexes of the AT and ME. Additionally, the saddle sulcus position presented variability on the femoral aspect of different knees. All of the average direct distances from the sulcus to the reference radiographic points exceeded 5 mm, and tunnel localizations on a true lateral radiograph were inaccurate.
Clinical Relevance:
This study demonstrates the potential precise position of the saddle sulcus, according to the ME and AT, as a reliable anatomic landmark for MPFL femoral tunnel location. Radiographic reference points were not accurate during MPFL reconstruction. Direct palpation of the landmarks might be effective for femoral MPFL tunnel placement.
Keywords
The MPFL is the main passive restraint to lateral patellar translation.6,7 Partial or complete rupture of the ligament has been shown to occur in >85% of primary patellar dislocations,14,26 potentially leading to recurrent instability and even complete fixed dislocation after nonoperative treatment.23,30 To functionally restore normal patellar tracking in the trochlear groove, prevent further lateral luxation, and treat chondral damage and relieve pain, MPFL reconstruction is used as a routine procedure for patients in whom nonoperative measures fail.
Anatomic MPFL reconstruction is crucial to reestablish graft isometry and function, predominantly on the femoral tunnel placement.24,30 Numerous gross and radiographic studies on femoral MPFL insertion and tunnel positioning have provided guidance for MPFL reconstruction5,9,19,22,24; however, 47% of major postoperative complications result from technical problems, and 67% of young patients who experience recurrent lateral patellar dislocation, patellofemoral arthrosis, or pain are found to have nonanatomic femoral ligament position. 17
Intraoperative true lateral radiographs have indicated that accepted methods for femoral MPFL tunnel location are inaccurate; the inaccuracy persists with a true lateral knee imaging, which is challenging to obtain.3,30 Radiology simply provides an approximate position during MPFL reconstruction, possibly exceeding a nonnegligible threshold of 5 mm away from the anatomic insertion.13,21 Discovering the saddle sulcus where the MPFL attaches,4,30 via direct assessment during surgery through palpation of the anatomic landmarks, might help eliminate malpositioning of MPFL anatomic tunnel fixation. To our knowledge, the precise position and determination of the saddle sulcus are still unknown.
Therefore, the purposes of this study are (1) to determine the anatomic insertion of the MPFL and the saddle sulcus; (2) to quantify the position of the anatomic saddle sulcus based on the surrounding osseous landmarks, thus providing guidance for femoral tunnel placement; and (3) to compare the position of the saddle sulcus with 3 previously reported radiographic localization techniques. The hypothesis is that the saddle sulcus is a reliable osseous landmark where the MPFL attaches for tunnel placement.
Methods
Specimen Preparation
A total of 9 fresh-frozen unpaired human cadaveric knees (donated for medical research from a tissue bank, purchased by our institution; 5 men and 4 women; aged 70-82 years, 5 right and 4 left) were used for the study; the samples had no evidence of meniscal or ligamentous defects or any severe traumatic or degenerative changes. The specimens were kept frozen at −20°C and were thawed overnight at room temperature before use. The medial side of the knee was dissected on all specimens to identify the medial collateral ligament, MPFL, AT, ME, and MGT (Figures 1 and 2; Table 1). A 2-mm stainless steel sphere was embedded into the center of the MPFL, namely the middle of the saddle sulcus, if any; the apexes of the AT, ME, and MGT were pinned with colored pushpins for better recognition (Figure 2).
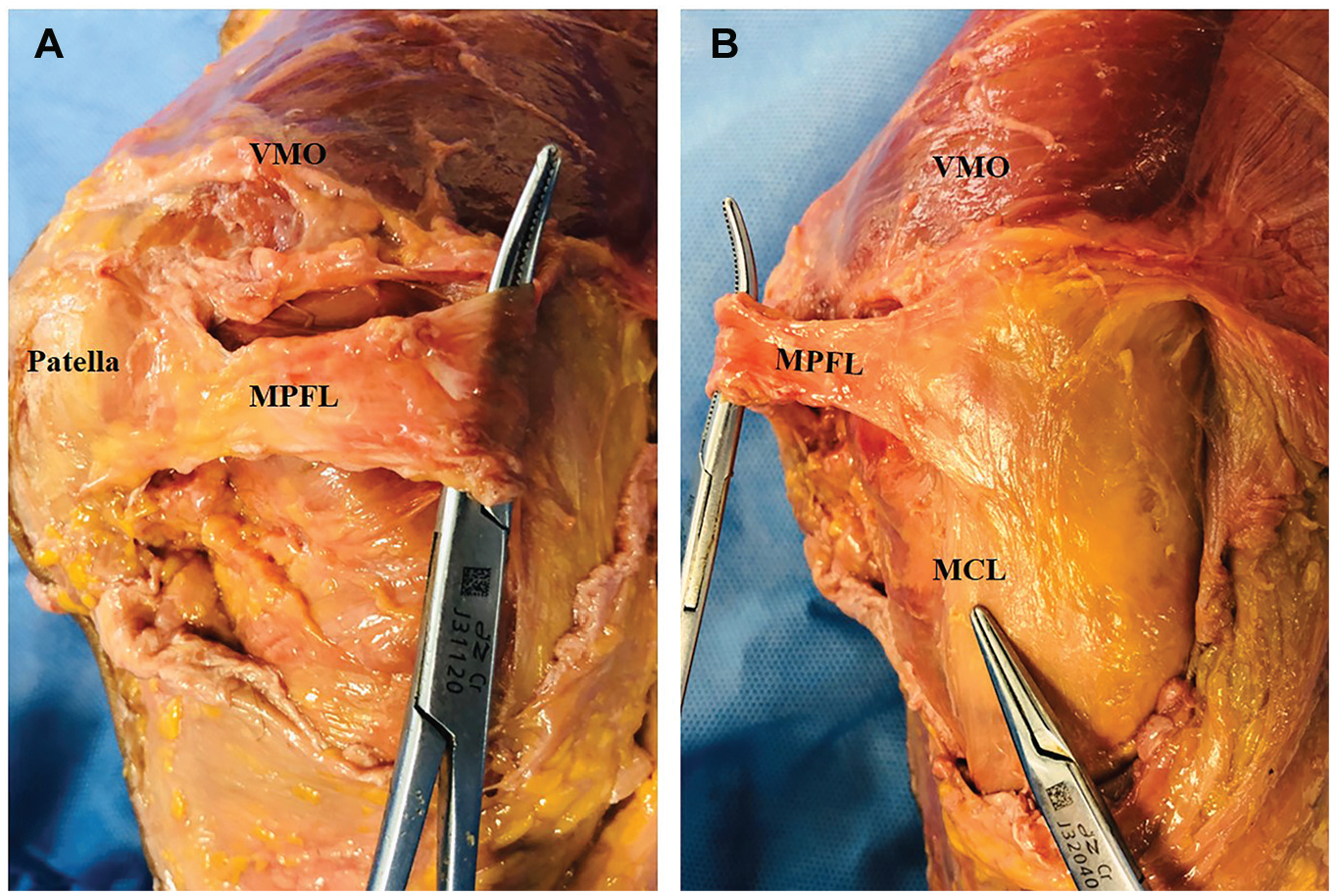
Cadaveric dissection of a right knee demonstrating the MPFL (A) patellar insertion and (B) femoral insertion.
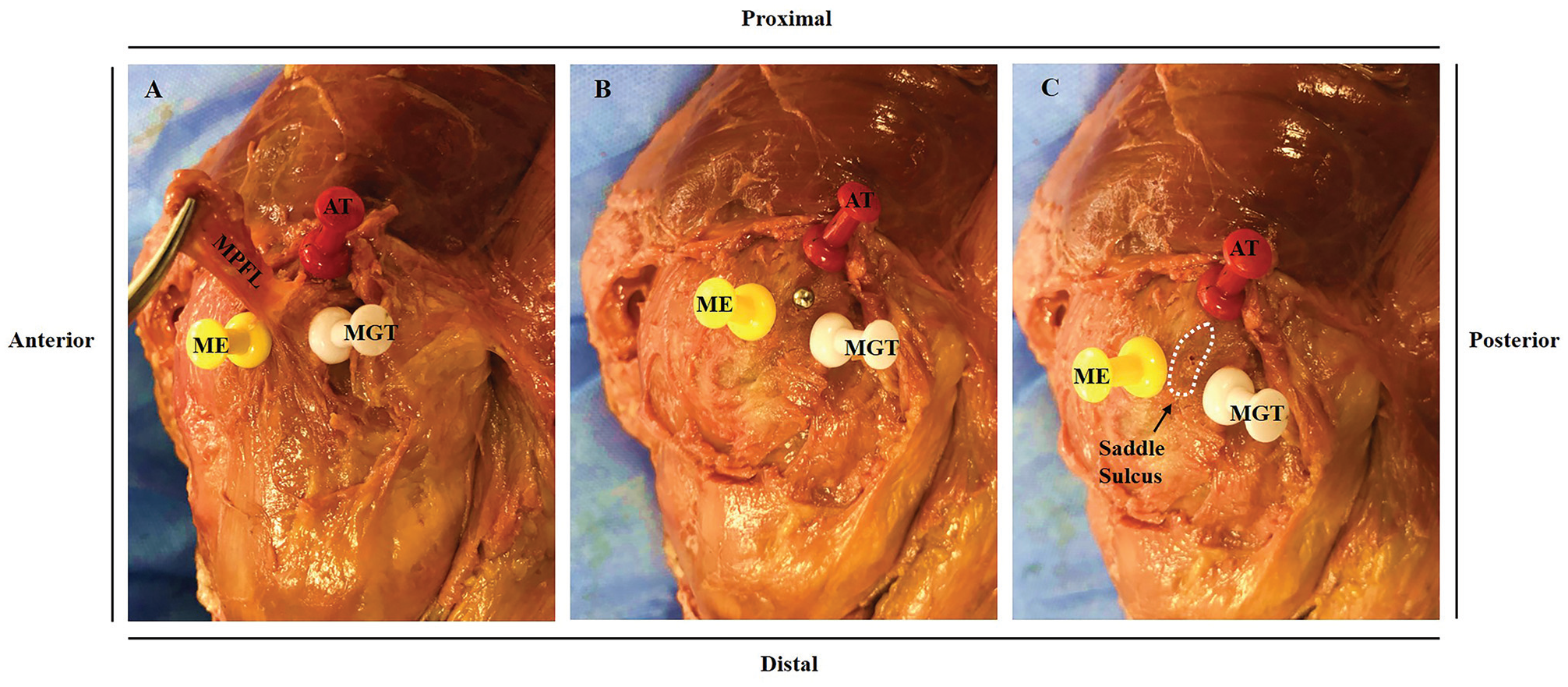
Cadaveric dissection of a right knee demonstrating pertinent soft tissue and osseous anatomic features, with the apexes of the AT, ME, and MGT (pinned). (A) The MPFL was elevated to better delineate the femoral insertion. (B) The MPFL was dissected and its center was pinned with a 2-mm stainless steel sphere. (C) The white dotted circle marks the MPFL femoral attachment, located in an osseous saddle-shaped sulcus.
Abbreviations Used
Image Collection and Measurements
Computed tomography (CT) scans (SOMATOM Definition AS+; Siemens) of the knee joints (thickness, 0.6 mm; resolution, 512 × 512 pixels) were obtained for measurements after the anatomic landmarks were determined on the specimens and marked with pins. The images were then imported into 3-dimensional (3D) modeling software (Mimics Research 21.0; Materialise NV) to reconstruct surface models of the femur with preembedded pins in order to delineate the osseous structures and saddle sulcus. Direct distances along the center of the saddle sulcus and the apexes of the related structures were measured from 3D images by 2 independent observers (J.C. and K.H.). The perpendicular distance from the center of the saddle sulcus to the margin (connecting the apexes of the AT and ME) and the direct distance from the projected point to the AT were measured subsequently (Figure 3). Upon comparison of the accuracy of 3D models oriented from CT scan versus optical scan, the mean ± SD observational error was 0.2 ± 0.31 mm. 10 The femur was rotated until the medial and lateral femoral condyles fully coincided to create a true lateral view, with the software set in transparent mode. Additionally, our preliminary study indicated that the deviation of the distances measured directly on the specimen with clearance from soft tissues and the transformed true lateral radiographs was within ±1 mm precision, irrespective of the measurement error.
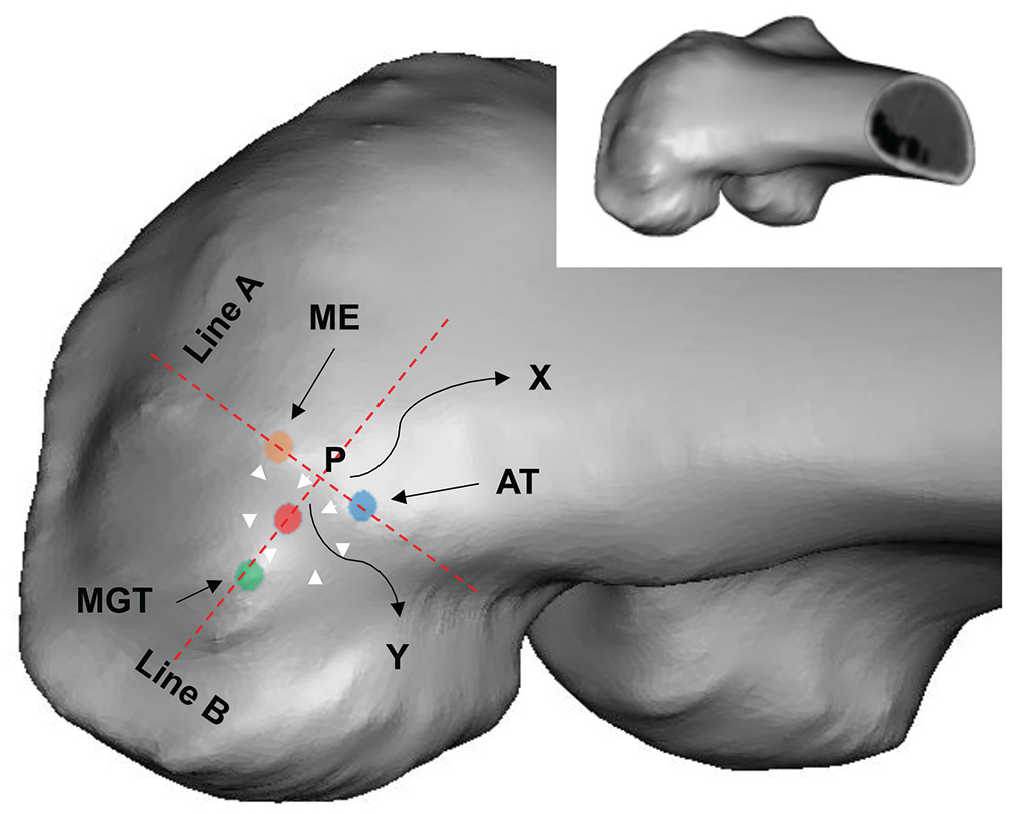
Medial region of the 3-dimensionally reconstructed right knee with marking of the saddle sulcus center and apexes of the adductor tubercle (AT, blue dot), medial epicondye (ME, orange dot), and medial gastrocnemius tubercle (MGT, green dot). The oblong area delineated by white arrowheads, the center of which is marked with a red dot, is the saddle sulcus. The perpendicular distance (Y) along line B from the center of the saddle sulcus to line A crossing the apexes of the AT and ME, and the distance (X) from the projected point (P) to the AT, were measured using dedicated software. The small image of the femur from the oblique posterior femoral view shows the alignment of the specimen.
Previously reported radiographic reference points of femoral MPFL insertion were marked using the radiographic reference lines: the Schöttle et al 22 point (1.3 mm anterior to the distal posterior cortex and 2.5 mm distal to the posterior origin of the medial femoral condyle), Redfern et al 19 point (0.5 mm anterior to the posterior cortex extension and 3 mm proximal to the apex where it meets the Blumensaat line), and Fujino et al 9 point (approximately 10 mm distal to the adductor tubercle) (Figure 4). The shortest straight-line distances were measured between the center of the saddle sulcus and these reported radiographic reference points on each specimen.
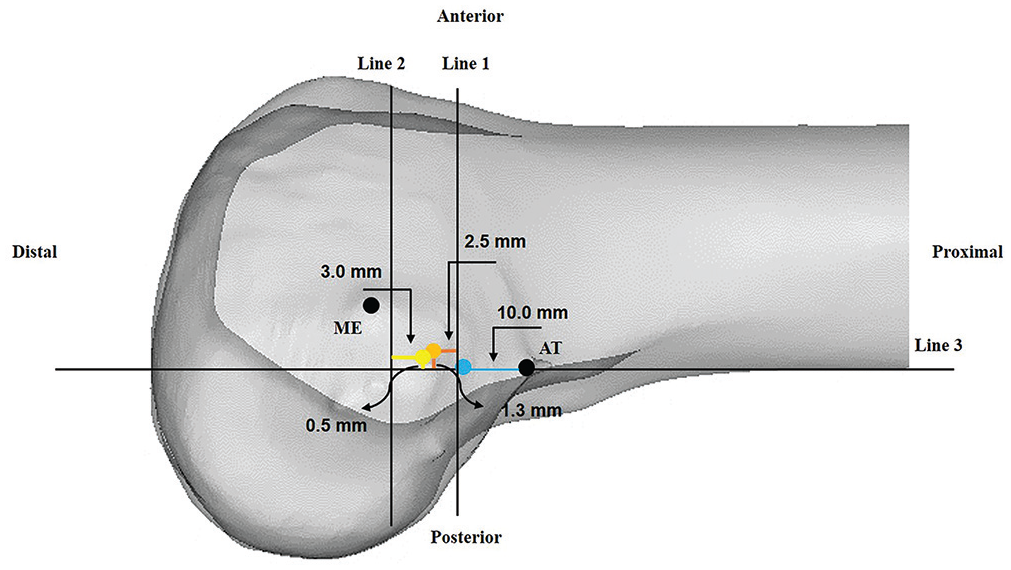
Radiographic reference points for positioning of the femoral tunnel during MPFL reconstruction, according to Schöttle et al 22 (orange dot) (1.3 mm anterior to the distal posterior cortex and 2.5 mm distal to the posterior origin of the medial femoral condyle), Redfern et al 19 (yellow dot) (0.5 mm anterior to the posterior cortex extension and 3 mm proximal to the apex where it meets the Blumensaat line), and Fujino et al 9 (blue dot) (approximately 10 mm distal to the adductor tubercle). Line 1 intersects the contact point of the medial condyle and the posterior cortex; line 2 intersects the most posterior point of the Blumensaat line; line 3 extends distally along the posterior femoral cortex.
Results
Macroscopic Findings
On all specimens, a palpable broad and oblong osseous saddle sulcus, posterior to the ME and distal to the AT, was detected where the MPFL was attached (Figure 2). The saddle sulcus was consistently located posterodistal to the margin crossing the apexes of the ME and AT; among all specimens, 3 saddle sulcus centers lay outside the triangular space between the apexes of the AT, ME, and MGT, exceeding the margin between the apexes of the ME and MGT. With the medial collateral ligament adjoining the MPFL on the medial femoral aspect, the sulcus was deepened by the posterior border of the soft tissue. When the surrounding soft tissue was dissected and cleared, the sulcus was no more than a shallow depression. Along the course of the adductor muscle tendon, the AT on the femur could be easily located. The ME was then palpated anterodistal to the AT; the MGT was more difficult to palpate because of its larger relative tendon insertion and variable existence. With the clearly and easily identified landmarks of the ME and AT, palpation of MGT could further confirm the positioning of the saddle sulcus.
Radiographic Measurements
The mean distances between the saddle sulcus and osseous landmarks on the femoral medial aspect based on the true lateral radiographs are listed in Table 2. The saddle sulcus center was closer to the ME on average than the AT, and the distances were 9.8 ± 2.3 mm and 16.3 ± 6.7 mm, respectively. The saddle sulcus lay on 1 side of the border connecting the apexes of ME and AT with variability (Figure 5). On the basis of the apexes of the ME and AT, the saddle sulcus was determined to be 11.7 ± 5.9 mm (X), 62.8% of the average distances between the ME and AT, and 5.6 ± 2.8 mm (Y) (Figures 3 and 5). The interclass correlation coefficient was 0.95, indicating a high interrater reliability.
Distance Between Saddle Sulcus and Osseous Landmarks on True Lateral Radiographs a
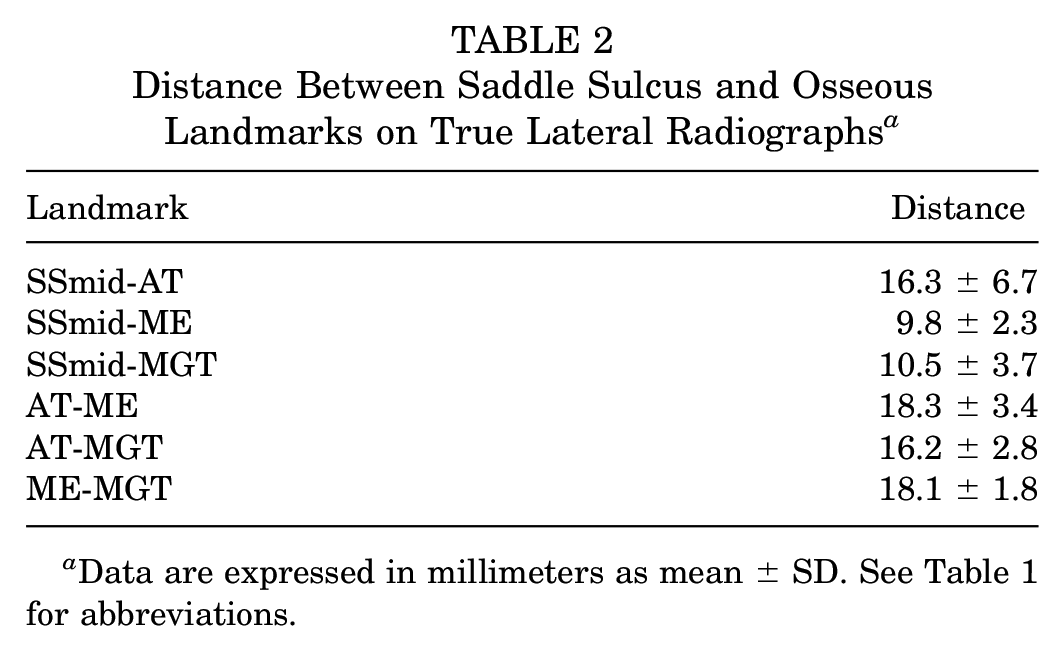
Data are expressed in millimeters as mean ± SD. See Table 1 for abbreviations.
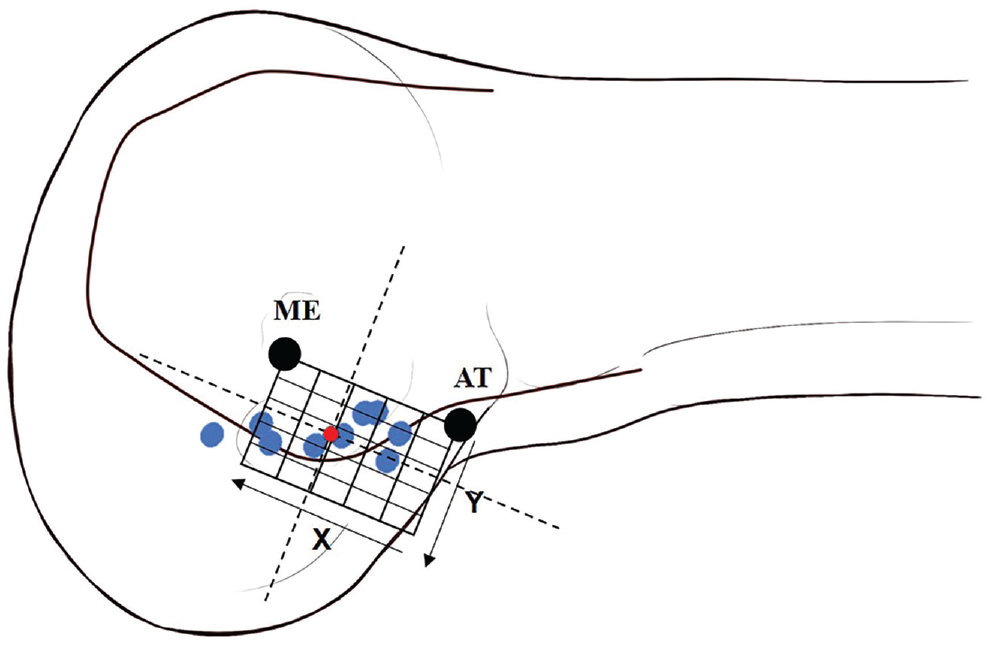
Each blue point shows the relative position of the center of the saddle sulcus between the apexes of the ME and AT on the true lateral radiograph outline, with the X-Y coordinates defined in Figure 3. The positions of the ME and AT were determined by the mean distance measured on all specimens. The black dotted perpendicular lines were drawn to present the average position of the sulcus saddle (red dot).
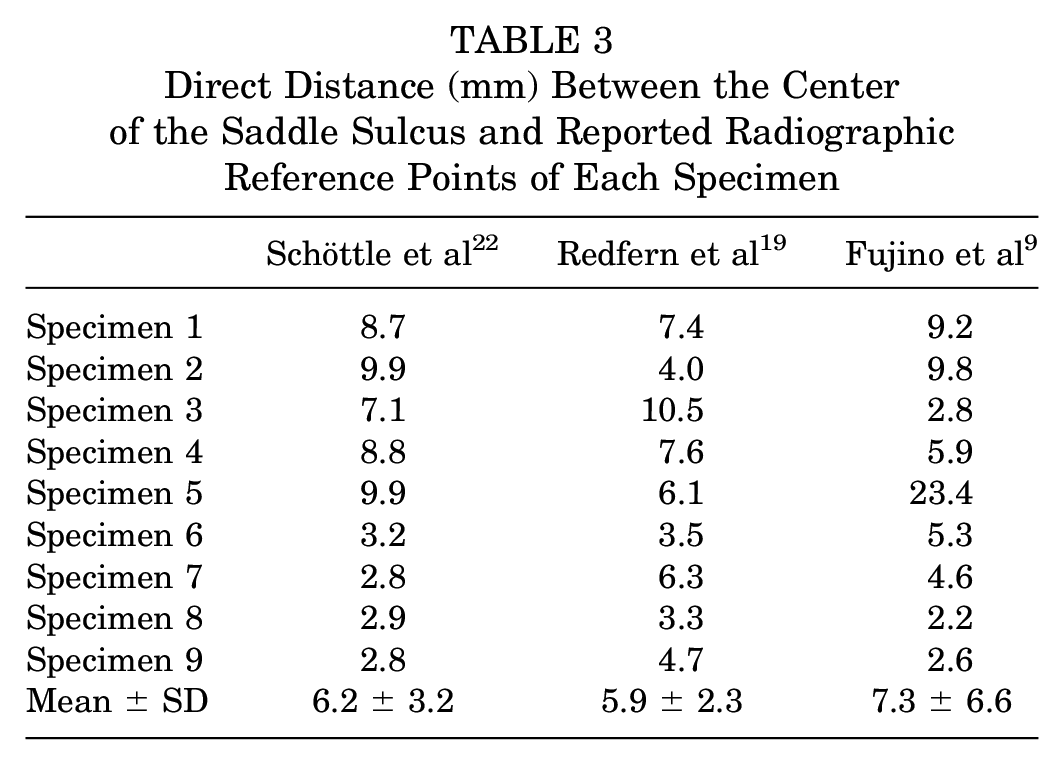
The reported radiographic reference points were located at a mean distance of 6.2 ± 3.2 mm (Schöttle et al 22 ), 5.9 ± 2.3 mm (Redfern et al 19 ), and 7.3 ± 6.6 mm (Fujino et al 9 ) from the saddle sulcus center on the true lateral radiographs (Table 3). The radiographic points were basically located anteroproximal to the sulcus center.
Direct Distance (mm) Between the Center of the Saddle Sulcus and Reported Radiographic Reference Points of Each Specimen
Discussion
The most important finding of our study was that the saddle sulcus was a reliable landmark where the MPFL was anatomically attached, located at approximately 12 mm from the AT to the ME and 6 mm perpendicular-posterior to the border connecting the apexes of the AT and the ME. All of the mean direct distances from the sulcus to the reported reference radiographic points exceeded 5 mm, a reported small malposition resulting in dramatic increase in patellofemoral pressure and alteration of graft isometry.8,24 To our knowledge, this is the first study to quantify the anatomic landmark (saddle sulcus), which was mentioned and described in several previous studies4,29,30 without further examination.
In our study, the performed anatomic dissections confirmed the presence of a saddle sulcus where the MPFL was consistently attached, and its location coincided with previously reported sites 30 : namely, distal to the AT, anterior to the MGT, and posterior to the ME and medial collateral ligament femoral insertion. A recent meta-analysis 1 reported that the femoral MPFL insertion was reliably surrounded by the triangular space of 3 osseous landmarks on the femoral medial aspect, namely the AT, MGT, and ME. However, in our study, the saddle sulcus was not consistently inside the triangle; 3 of 9 specimens presented a variation of the anatomic location where the center of the saddle sulcus was outside the border connecting the apexes of the ME and the MGT. Correspondingly, the MPFL attachment presented variability on the femoral aspect (Figure 5). The underlying nonconformity might originate from the patient-specific anatomic properties of the MPFL insertion, potential variability of the ME location, 12 and the broad, flat shape of the ME apex, 9 suggesting that using the fixed-location radiographic reference points on different knees might not ensure a precise tunnel positioning. Thus, more focus should be placed on the anatomic characteristics of the medial femoral aspect while using intraoperative imaging for confirmation as a response to the variability of MPFL attachment. Moreover, consistent with the previous studies,4,30 the osseous landmarks involving the ME, AT, MGT, and saddle sulcus were palpable in each specimen upon careful dissection of the MPFL. The palpation of these osseous landmarks through an approximately 2-cm skin incision could be realized after sufficient release and exposure, which was believed to be an accurate and feasible intraoperative technique in a previous study. 29
The current study also presented a detailed anatomic localization concerning the saddle sulcus, based on the apexes of the landmarks and associated average measured distances of the AT and ME (18.3 mm), a value that was similar to the distances reported by LaPrade et al 15 (proximal 12.6 mm and posterior 8.3 mm; namely, approximately 15.0 mm of direct distance). We found that the saddle sulcus was located at approximately 12 mm from the apex of the AT to the ME and 6 mm perpendicular-posterior to the border connecting the apexes of AT and ME. Considering the potential variability of the landmarks leading to the deviation of the distances of these two apexes, approximately 60% along a line from the AT to the ME, would aid in further determination of the final tunnel position.
Several previous cadaveric studies illustrated the MPFL femoral attachment in detail, according to surrounding osseous structures. LaPrade et al 15 found that the MPFL center was located 10.6 mm proximal and 8.8 mm posterior to the ME and 1.9 mm anterior and 3.8 mm distal to the AT. Philippot et al 18 reported the center to be positioned 10.7 mm posterior and proximal to the ME and 11.2 mm anterior and distal to the AT. Reported quantified anatomic localization methods require a coordinate generated by the outlines of the femur and tibia, which is difficult for an inexperienced surgeon to precisely determine intraoperatively via a small incision, or even by intraoperative radiographs, let alone the tunnel positioning on this tiny area. However, our procedure used the osseous landmarks alone to create a coordinate to locate the anatomic position, which required approximately 1 to 2 minutes to find the precise and effective location. 29 Considering the anterior and posterior medial femoral condyle width to be 100%, Nomura et al 16 and Stephen et al 24 identified that the femoral MPFL insertion was located around 60% from the anterior margin of the medial femoral condyle in normal cadaveric knees. However, trochlear dysplasia, one of the predominant risk factors for patellar instability, 2 either with a spur or a cliff, would potentially change the proportion of the MPFL insertion site on the whole medial condyle diameter and significantly affect patellofemoral kinematics. 27 Clinical confirmation was therefore required for the 60% rationale, while our location method should not be affected by the femoral trochlear variation. Moreover, the midpoint localization of the AT and ME showed less accurate tunnel positioning and ignored individual variability in most cases. 29
Radiographic landmarks, along with anatomic location, have gained popularity since Schöttle et al 22 first proposed a localization method based on true lateral radiographs. Similarly, reference lines have been used for several other reference points,5,9,19,24,28,30 involving the posterior femoral cortex extension line, the line intersecting the contact point of the medial condyle and the posterior cortex, the long axis of the femur, the Blumensaat line, and associated intersecting lines. However, radiographic points in the literature differ dramatically, indicating the potentially inaccurate tunnel positioning, even on a true lateral radiograph with inherent room for error. 30 Our study also found >5 mm distance from the anatomic femoral placement for all 3 identified radiographic reference points, consistent with the results of the 4.1-mm deviation reported by Ziegler et al. 30 Likewise, Sanchis-Alfonso et al 20 reported only 36.7% and 25.5% overlapping of the anatomic tunnel area using the Schöttle et al 22 and Stephen et al 24 methods, respectively. Sanchis-Alfonso et al 21 further confirmed the failure of fluoroscopy-guided positioning, especially in female patients with severe trochlear dysplasia. Izadpanah et al 13 reported the inaccuracy of tunnel positioning using intraoperative radiographs for patients with severe dysplasia. Although Herschel et al 11 argued against the accuracy of the visual-palpatory procedure for MPFL tunnel placement and used routine fluoroscopic guidance, they defined a “correct zone” as an anatomic position by the radiological reference lines, and their tunnel placement by palpation was an approximation, slightly posterior to the midpoint of the AT and ME. Therefore, the effectiveness of palpation might have been underestimated.
We acknowledge several limitations of the current study. First, the limited specimen number might not represent the full scope of the anatomic variability in the entire population with patellar instability. Further epidemiologic “big data” research is required. Second, specimens of old age with degenerative changes might have altered morphologic features of the medial aspect of the femur. However, knees with severe degenerative changes were not used. Third, we used the reconstructed 3D knees and transformed true lateral radiographs, which might result in bias. Fourth, the evolving understanding of the medial patellar complex shows that in addition to the MPFL, other ligament such as the MQTFL, MPTL, and MPML might also help to medially stabilize the patella. 25 However, only MPFL reconstruction was included for consideration to treat patellar instability in our study.
Conclusion
The saddle sulcus was a reliable landmark to show where the MPFL was anatomically attached, located at approximately 12 mm from the AT to the ME (approximately 60% along a line from the AT to the ME) and 6 mm perpendicular-posterior to the border connecting the apexes of the AT and the ME. Additionally, the saddle sulcus position presented variability on the femoral aspect of different knees. All of the average direct distances from the sulcus to the reference radiographic points exceeded 5 mm, and tunnel localizations on a true lateral radiograph were inaccurate.
Footnotes
Submitted May 8, 2020; accepted August 18, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: The work was funded by the National Key Research and Development Program of China, 2018YFC1106200, 2018YFC1106202; the Western Medicine Guidance Project of Science and Technology Commission of Shanghai Municipality, Grant No. 17411966400; the Key Disease Joint Tackling Project of Xuhui District, Shanghai, Grant No. XHLHGG201802; and the National Natural Science Foundation of China, Grant No. 81871753. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.