
Abstract
Background:
The variable anatomy and controversy of the anterolateral ligament (ALL) reflect the complex relationship among the anterolateral knee structures.
Purpose/Hypothesis:
The purpose was to quantify the microstructural and mechanical properties of the ALL as compared with the anterolateral capsule (ALC) and lateral collateral ligament (LCL). The primary hypotheses were that (1) there is no difference in these properties between the ALL and ALC and (2) the LCL has significantly different properties from the ALL and ALC.
Study Design:
Descriptive laboratory study.
Methods:
The LCL, ALL, and ALC were harvested from 25 cadaveric knees. Mechanical testing and microstructural analyses were performed using quantitative polarized light imaging. The average degree of linear polarization (AVG DoLP; mean strength of collagen alignment) and standard deviation of the angle of polarization (STD AoP; degree of variation in collagen angle orientation) were calculated.
Results:
Linear region moduli were not different between the ALC and ALL (3.75 vs 3.66 MPa, respectively; P > .99). AVG DoLP values were not different between the ALC and ALL in the linear region (0.10 vs 0.10; P > .99). Similarly, STD AoP values were not different between the ALC and ALL (24.2 vs 21.7; P > .99). The LCL had larger modulus, larger AVG DoLP, and smaller STD AoP values than the ALL and ALC. Of 25 knee specimens, 3 were observed to have a distinct ALL, which exhibited larger modulus, larger AVG DoLP, and smaller STD AoP values as compared with nondistinct ALL samples.
Conclusion:
There were no differences in the mechanical and microstructural properties between the ALL and ALC. The ALC and ALL exhibited comparably weak and disperse collagen alignment. However, when a distinct ALL was present, the properties were suggestive of a ligamentous structure.
Clinical Relevance:
The properties of the ALL are similar to those of a ligament only when a distinct ALL is present, but otherwise, for the majority of specimens, ALL properties are closer to those of the capsule. Variability in the ligamentous structure of the ALL suggests that it may be more important in some patients than others and reconstruction may be considered in selective patients. Further study is needed to better understand its selective role and optimal indications for reconstruction.
The anterolateral ligament (ALL) of the knee has recently gained attention for its contribution to rotational stability. Segond 39 described an avulsion fracture of the proximal anterolateral tibia associated with a band of tissue that tensioned during tibial internal rotation. Since then, several eponyms have been coined for similar anterolateral knee tissue structures.3,20,23,49 More recently, studies have linked the ALL to the Segond fracture and reported characteristics of a distinct ligamentous structure.5-8,17,34,50
The ALL runs from the lateral femoral epicondyle (LFE) to the proximal anterolateral tibia in an oblique direction, but the origin is debated. 34 Anatomic studies of the ALL have shown conflicting results, with a reported prevalence between 0% and 100%.8,12,38,45,50,51 Histological examination of the ALL has shown ligamentous and capsular organization.5,11,15 There is a complex relationship among the other anterolateral knee structures, such as the iliotibial band, Kaplan fibers, and anterolateral capsule (ALC), but the structure-function relationship is unknown.27,31 Biomechanical studies have shown that the ALL plays a role in rotational stability but not necessarily along its longitudinal axis.1,14 Clinical outcomes for combined anterior cruciate ligament (ACL) and ALL reconstructions have demonstrated favorable results, but long-term studies are lacking.9,22,44,47
There is an intricate relationship among the anterolateral knee structures, which contributes to the controversy surrounding the ALL. Defining the functional and microstructural anatomy of the anterolateral knee could advance our understanding behind the variance and significance of the ALL. Previous studies used a novel approach to assess the microstructural and mechanical properties of the cruciate ligaments using quantitative polarized light imaging (QPLI).41,53 The purpose of this study was to quantify the microstructural and mechanical properties of the ALL as compared with the ALC and lateral collateral ligament (LCL). We tested the primary hypotheses that (1) there is no difference in these properties between the ALL and ALC and (2) the LCL has significantly different properties from the ALL and ALC.
Methods
Study Design
Fresh-frozen human cadaveric knees were obtained from Restore Life USA and handled in accordance with the School of Medicine body donation policy. Institutional review board approval was waived given the cadaveric study design and lack of identifiable donor data. Inclusion criteria consisted of cadavers <60 years of age with no history of knee trauma, surgery, or instability.
Dissection Technique
In total, 25 knee specimens (9 male knees including 4 bilateral specimens and 1 unilateral specimen, and 16 female knees including 5 bilateral specimens and 6 unilateral specimens) were dissected to harvest the tissues of interest: LCL, ALC, and ALL. The mean age of donors was 45.6 years (SD, 6.4 years; range, 35-59 years), and the mean body mass index was 26.5 (SD, 8.4).
The dissection approach followed previously described techniques for the ALL.8,31 All dissections were performed by the lead author (R.M.P.), and any discrepancies were reviewed by the senior author (R.H.B.). A rectangular window was centered over the lateral knee, and skin and subcutaneous fat were removed to expose the extensor mechanism, iliotibial band, Gerdy tubercle, fibular head, and LFE. The iliotibial band was cut transversely 6 to 10 cm proximal to the LFE and reflected distally over the tibial insertion by cutting the Kaplan fibers (attachments to the lateral intermuscular septum and lateral retinaculum). A manual internal rotation torque was placed on the tibia to allow identification of an anterolateral structure (ie, ALL) that showed a distinct ligamentous structure and was oriented from around the LFE to midway between the Gerdy tubercle and the fibular head. A robust ligament-like tissue had to be present for this to be labeled a distinct ALL. If the tissue was only a capsular thickening, it was labeled a nondistinct ALL. The LCL was visible more posteriorly with manually applied varus stress.
Three tissue samples (LCL, ALL, and ALC) were harvested from each cadaveric knee (Figure 1). The ALL was taken as a quadrilateral piece of tissue starting posterior (mean distance, 11.0 mm; SD, 4.2) and proximal (mean, 9.5 mm; SD, 5.2) to the LFE, anterior to the fibular head (distal/posterior), and ending anteriorly at the lateral border of the Gerdy tubercle, as most studies agree on this definition. 34 The mean distance distal to the joint line was 14.2 mm (SD, 8.0). Care was taken to harvest only tissue superficial to the LCL. The identified area included the anatomic path of the ALL, with landmarks that have been described previously.1,14 Using these landmarks, this piece of tissue was taken as the ALL regardless of whether it was distinctly ligamentous or not. Next, the ALC was taken as a quadrilateral piece of tissue starting from the anterior border of the ALL to the patella, similar to the procedure of Smeets et al. 43 The mean dimensions of the ALC along the proximal, posterior, distal, and anterior margins were 20.8 mm (SD, 7.5), 44.2 mm (SD, 16.6), 18.4 mm (SD, 4.3), and 39.9 mm (SD, 9.2), respectively. Finally, the LCL was dissected from its insertions on the LFE and fibular head. Tissues were kept hydrated with phosphate-buffered saline (PBS) during all stages of the study, including dissection, sample preparation, and mechanical testing. Tissues were kept frozen overnight after dissection and thawed the next day for sample preparation.
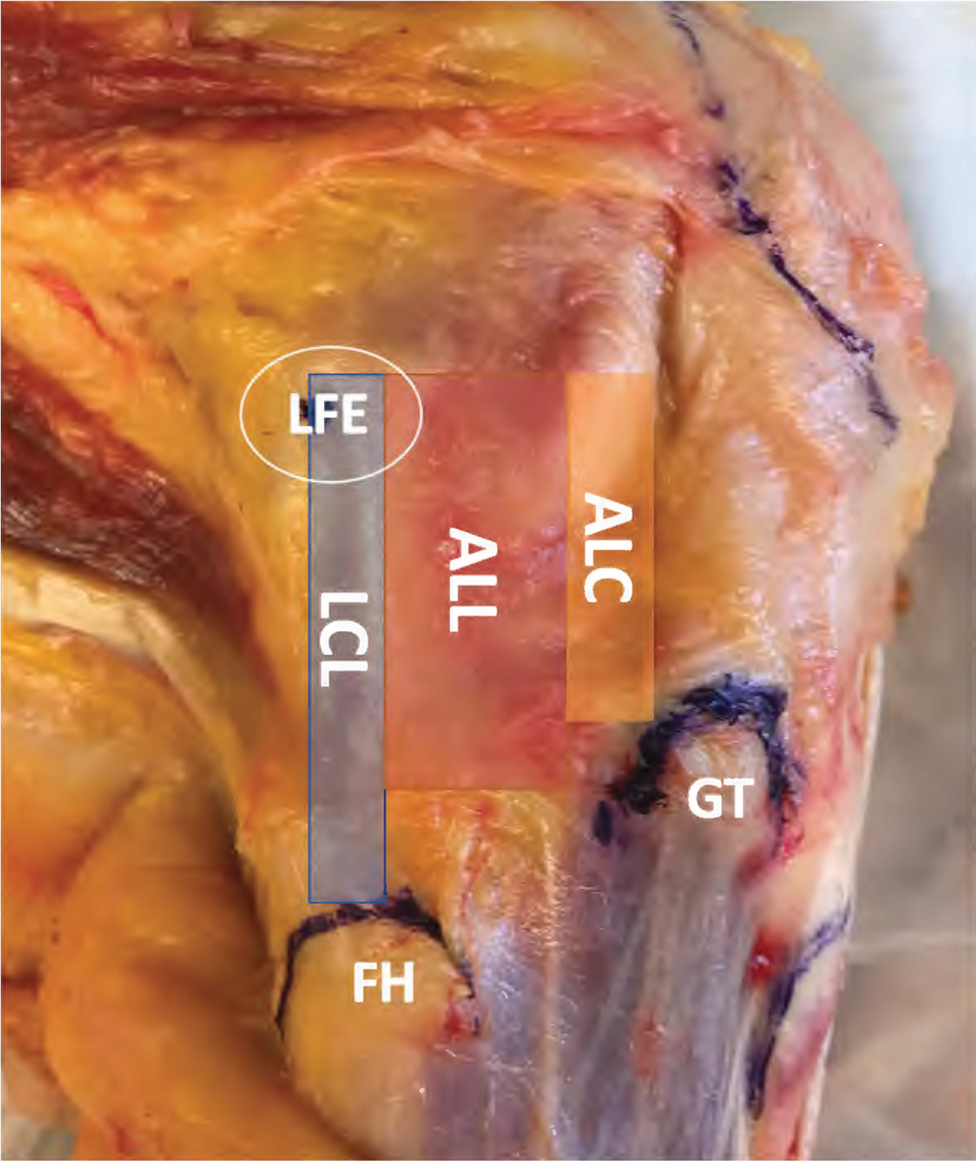
A cadaveric dissection of the anterolateral knee showing the landmarks for harvesting and tissues tested: lateral collateral ligament (LCL), anterolateral ligament (ALL), anterolateral capsule (ALC), lateral femoral epicondyle (LFE), fibular head (FH), Gerdy tubercle (GT).
Sample Preparation
Each tissue sample was attached to a freezing-stage sliding microtome (Leitz 1400; Leica) using embedding medium. Once a layer of tissue was sectioned, it was thawed, turned over, and frozen again to allow proportionate sectioning of the inner and outer surfaces. Thus, there was a total of 3 freeze-thaw cycles per specimen, similar to past studies.41,53 The microtome was used to level off both sides of the sample surface, leaving an approximately 1 mm–thick tissue slice with the help of a 1-mm thickness gauge. A noncontact laser-scanning system (Keyence) was used to measure sample cross-sectional area. The ends of each sample were then glued to sandpaper using cyanoacrylate to facilitate secure tissue gripping during mechanical testing. Small aluminum beads (diameter, 0.8 mm) were glued using cyanoacrylate to the sample surface in a grid pattern for strain measurement.
Mechanical Testing
Testing was performed as previously described for the ACL and posterior cruciate ligament (PCL).41,53 Samples were placed in a PBS bath and loaded in a tensile testing machine (Test Resources) integrated with a custom-built QPLI system to quantify fiber alignment during testing. 29 The QPLI system consists of a linear backlight (Dolan-Jenner), linear polarizing sheet, and quarter-wave plate retarder (Edmund Optics) to generate circularly polarized light, as well as a high-resolution custom division-of-focal-plane polarization imaging camera. Samples were preconditioned for 10 cycles to 3% strain, subjected to a stress-relaxation hold at 5% strain for 5 minutes, and then ramped to failure at a quasi-static rate of 0.1% per second from a preload of 0.1 N to ensure that the toe region was obtained. The polarization imaging camera acquired video throughout testing to enable calculation of collagen fiber alignment in static and dynamic loading scenarios.
The stress-relaxation portion of the testing measured viscoelastic tissue properties and was conducted and analyzed similar to previous studies.4,53 Peak and equilibrium points of the stress-relaxation curve corresponded to the maximum value immediately following the ramp and steady-state values at the end of the relaxation test, respectively. Normalized data (ie, time-dependent values divided by the peak values) were calculated for stress, average degree of linear polarization (AVG DoLP), and standard deviation of the angle of polarization (STD AoP). These values were interpolated at regular intervals on a log time scale to track the time-dependent changes throughout the relaxation period.
Videos were analyzed to quantify the DoLP and AoP. DoLP indicates how much of the circularly polarized light becomes linearly polarized after passing through the tissue, and it represents the relative strength of collagen fiber alignment within a given pixel. AoP indicates the average direction of linear polarization and represents the average direction of collagen fiber alignment for a given pixel. For a given region of interest within each tissue sample, AVG DoLP and STD AoP values were computed to provide parameter values that represent the strength of collagen alignment and the variation in orientation angle, respectively.
Data Analysis
An a priori power analysis was performed to determine the sample size. Previous studies that utilized the QPLI technique to study the ACL and PCL performed power analyses that demonstrated a sample size of 14 cadaveric knees.41,53 However, the ALL is considerably weaker and has variability. 42 Therefore, we used data from a study on hip ligaments, which are capsular redundancies and are 2 to 3 times weaker than the strongest ligaments. 19 We assumed that the standard deviation of the mechanical properties of a capsular tissue would be different than a ligamentous tissue. Using the mechanical data from hip ligaments, we calculated an effect size of 0.833. The alpha was set at .05 with a power of 0.8, which yielded a sample size of 24, and we chose this larger number as a conservative estimate.
A custom analysis program (Matlab, version R2018a) was used to optically track the surface beads and calculate 2-dimensional Lagrangian strain using tensor algebra. Stress was calculated as force divided by initial cross-sectional area. Using the least squares method, a bilinear curve fit was applied to the stress-strain data to quantify the modulus in the toe and linear regions, as well as the stress and strain values corresponding to the transition point of the bilinear fit. A Matlab program was used to quantify the collagen alignment throughout testing using QPLI and to create fiber alignment maps. During the stress-relaxation portion of the test, peak and equilibrium values were taken as the values immediately after the initial ramp (peak) and before the return to zero strain (equilibrium). Percentage change values were then computed between the peak and equilibrium values. Data were determined to be nonnormally distributed, so nonparametric statistical analyses were utilized. We used Prism (GraphPad Software, version 8.4.3) for statistical analyses. Statistically significant differences for each parameter were detected using Kruskal-Wallis tests with Dunn tests for multiple comparisons to elucidate differences among the ALL, ALC, and LCL. Differences between the ALL and distinct ALL were detected using a nonparametric t test (Mann-Whitney). Statistical significance was set at P < .05.
For abbreviations used in the article, see Table 1.
Abbreviations
Results
Of 25 knee specimens, 3 (12%) were observed to have a distinct ligamentous structure in the region of the ALL (Figure 2A) as compared with a majority of donor knees that exhibited a nondistinct anatomic appearance (Figure 2B). Distinct ALLs appeared as a ligamentous structure arising from the LFE and attaching between the anterior aspect of the fibular head and posterior margin of the Gerdy tubercle.
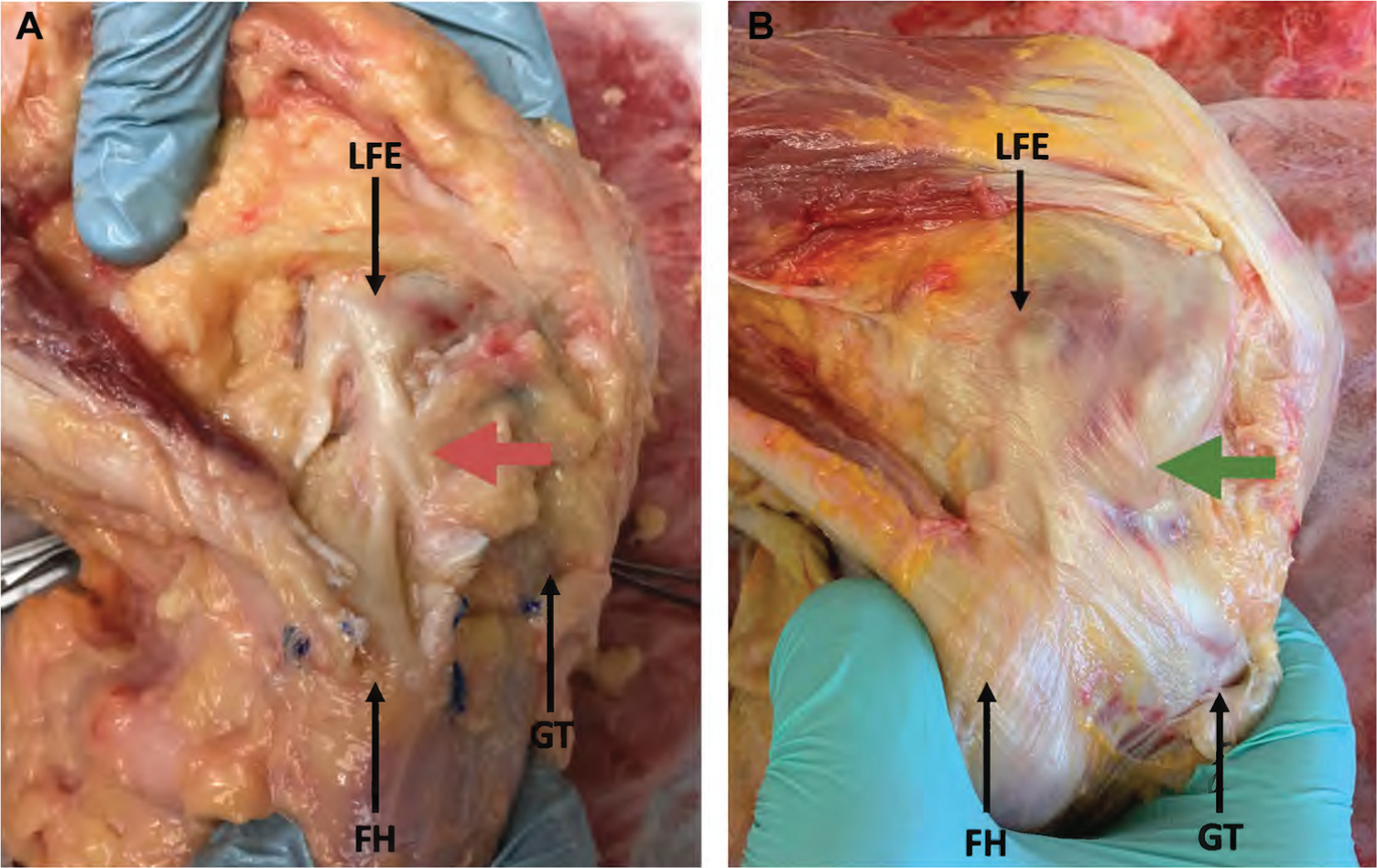
Anatomic dissection of the anterolateral knee in specimens with a (A) distinct ALL (red arrow) and (B) nondistinct ALL (green arrow). Both specimens are flexed at the knee and internally rotated at the tibia. ALL, anterolateral ligament; FH, fibular head; GT, Gerdy tubercle; LFE, lateral femoral epicondyle.
Table 2 shows a summary of the mechanical, microstructural, and viscoelastic data. Mechanical test results demonstrated no difference in elastic moduli between the ALC and ALL in the toe region (P > .99) and linear region (P > .99). However, the LCL showed larger elastic moduli than the ALC and ALL in the toe (P < .001) and linear (P < .001) regions of the stress-strain curves (Figure 3). For the stress and strain data in the transition region, see Appendix Figure A1 (available in the online version of this article).
Summary of Statistical Results a
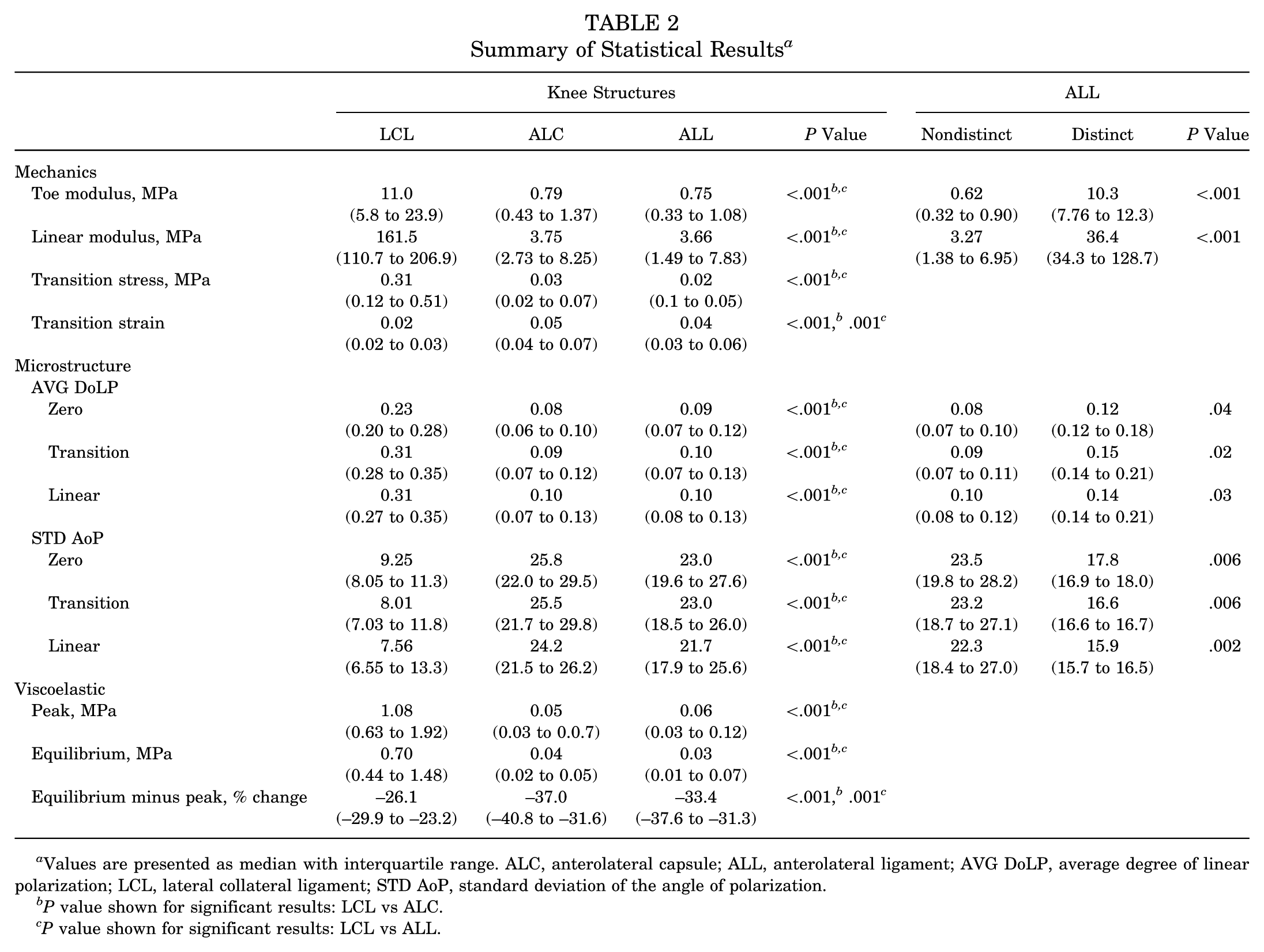
Values are presented as median with interquartile range. ALC, anterolateral capsule; ALL, anterolateral ligament; AVG DoLP, average degree of linear polarization; LCL, lateral collateral ligament; STD AoP, standard deviation of the angle of polarization.
P value shown for significant results: LCL vs ALC.
P value shown for significant results: LCL vs ALL.
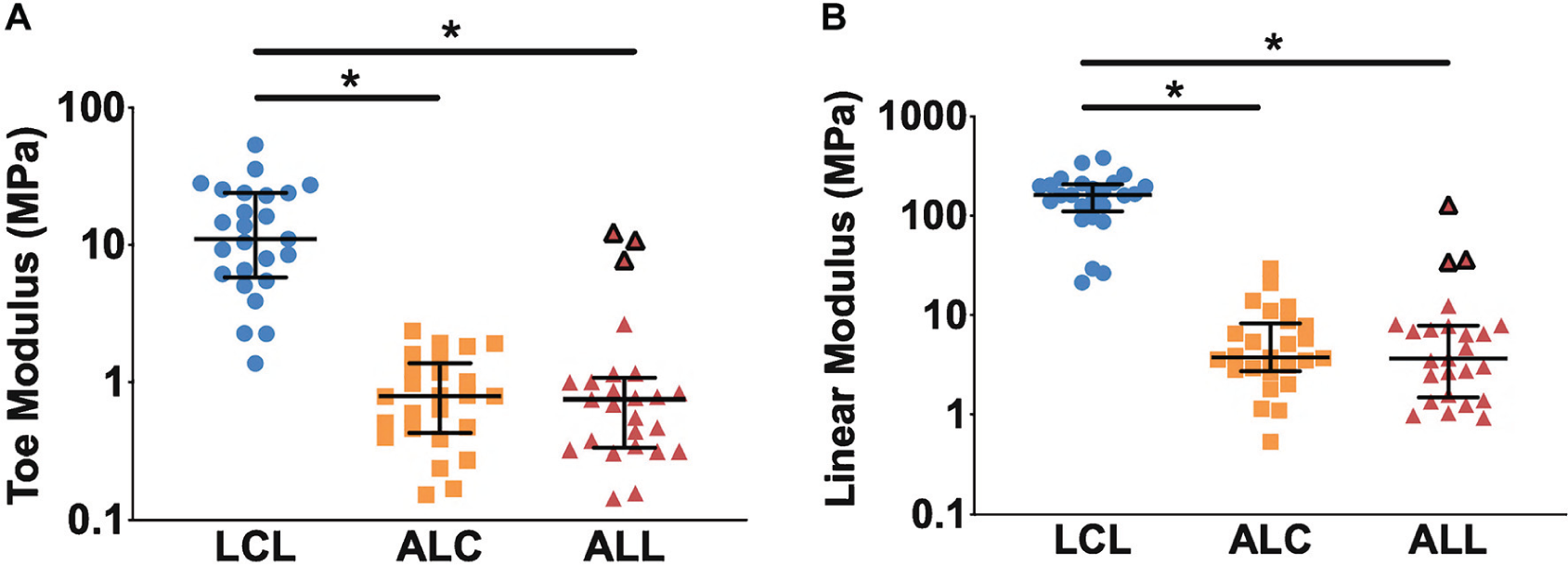
The (A) toe and (B) linear moduli of elasticity for the LCL, ALC, and ALL. Distinct ALL samples are outlined in black. Note that the graph scale is log 10. *P < .05. Values are presented as median and interquartile range. ALC, anterolateral capsule; ALL, anterolateral ligament; LCL, lateral collateral ligament.
Microstructural analysis during quasi-static ramp to failure was used to quantify collagen fiber organization and dynamic changes during tissue loading (Figure 4). There were no differences in AVG DoLP (Figure 5A) values between the ALC and ALL at zero, transition, and linear strain levels (all P > .99). There were no differences in STD AoP (Figure 5B) values between the ALL and ALC at zero, transition, and linear strain levels (all P > .99). The LCL demonstrated larger DoLP values (ie, stronger collagen fiber alignment) than the ALL and ALC at zero (P < .001), transition (P < .001), and linear (P < .001) strain. The LCL also demonstrated smaller STD AoP values (ie, less variation in collagen orientation) than the ALL and ALC at zero (P < .001), transition (P < .001), and linear (P < .001) strain.
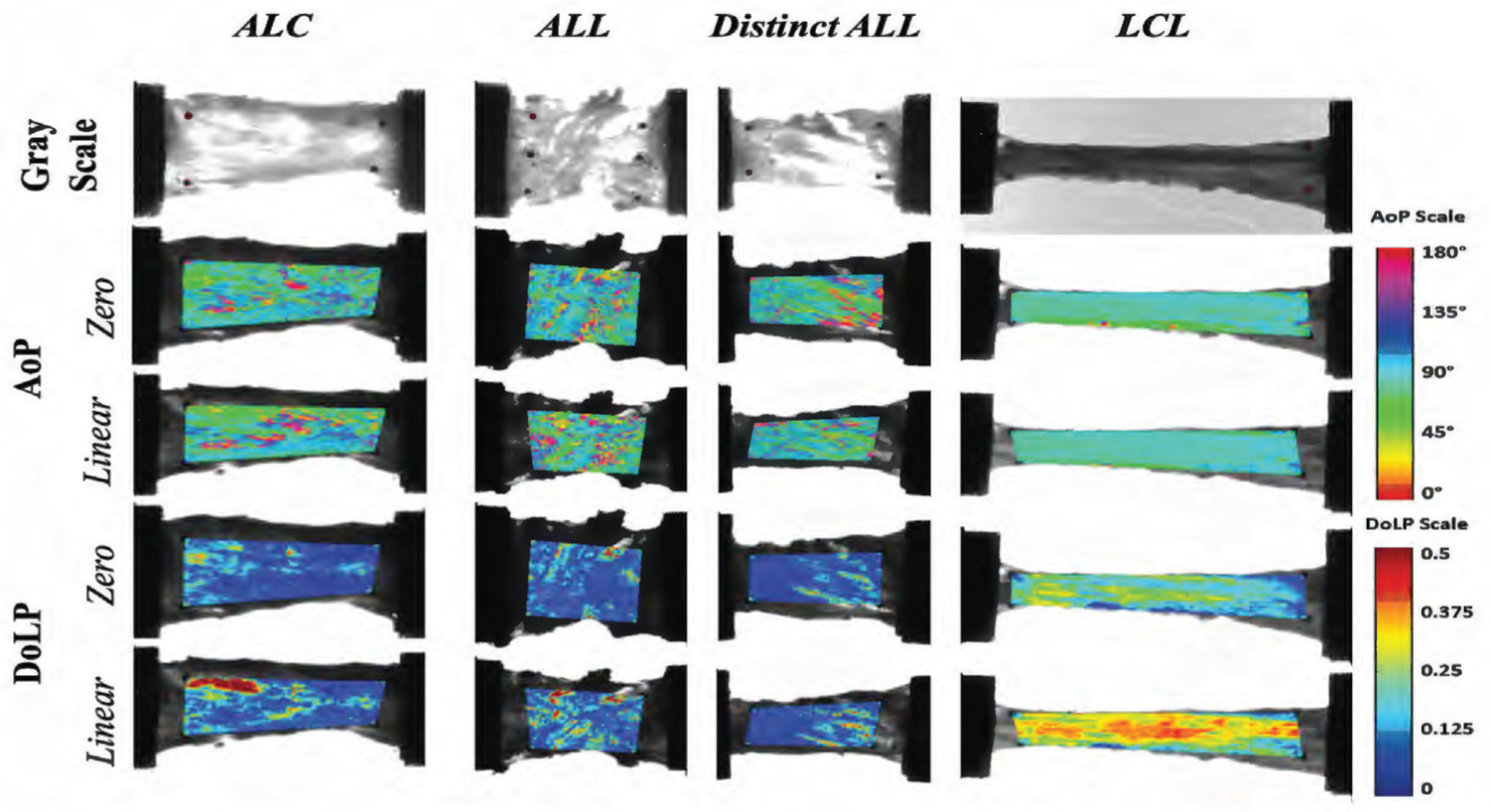
Representative images of each tissue type. Examples are in grayscale at zero strain and AoP and DoLP at zero strain and in the linear portion of the ramp to failure. For AoP images, a more uniform color means that collagen is more aligned; for DoLP, the more nonblue space means that collagen has a higher degree of polarization. ALC, anterolateral capsule; ALL, anterolateral ligament; AoP, angle of polarization; DoLP, degree of linear polarization; LCL, lateral collateral ligament.
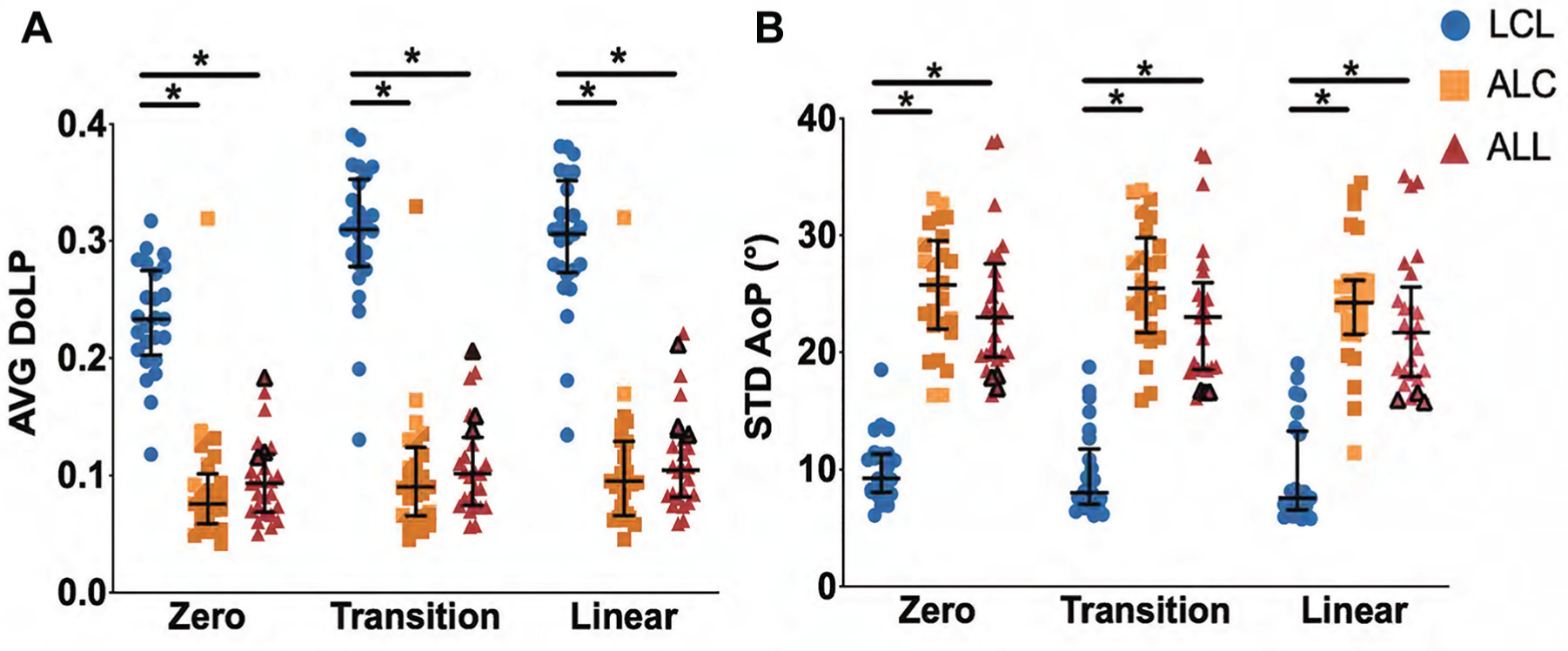
Microstructural analysis showing (A) AVG DoLP and (B) STD AoP at the zero, transition, and linear points of the quasi-static ramp to failure for the LCL, ALC, and ALL. Distinct ALL samples are outlined in black. *P < .05. Values are presented as median and interquartile range. ALC, anterolateral capsule; ALL, anterolateral ligament; AVG AoP, average angle of polarization; STD DoLP, standard deviation degree of linear polarization; LCL, lateral collateral ligament.
Viscoelastic properties were measured during the stress-relaxation portion of testing. LCL samples exhibited significantly larger stress values at the peak and equilibrium points as compared with the ALC (P < .001) and ALL (P < .001) (Figure 6A). The ALC (P < .001) and ALL (P = .001) exhibited significantly decreased percentage change in stress as compared with the LCL. In terms of time-dependent stress relaxation, the ALL and ALC values decreased more quickly than the LCL from the very beginning of the relaxation period (Figure 6B). Overall, the rate of change in AVG DoLP (Figure 6C) and STD AoP (Figure 6D) was minimal at ~0% to 3% as compared with the change seen in stress. However, at later time points, the AVG DoLP and STD AoP were significantly different among the 3 tissue types. The ALL showed stable collagen fiber alignment with relatively little change in AVG DoLP and STD AoP. However, there was a time-dependent increase for both parameters in the LCL and decrease in the ALC at later time points.
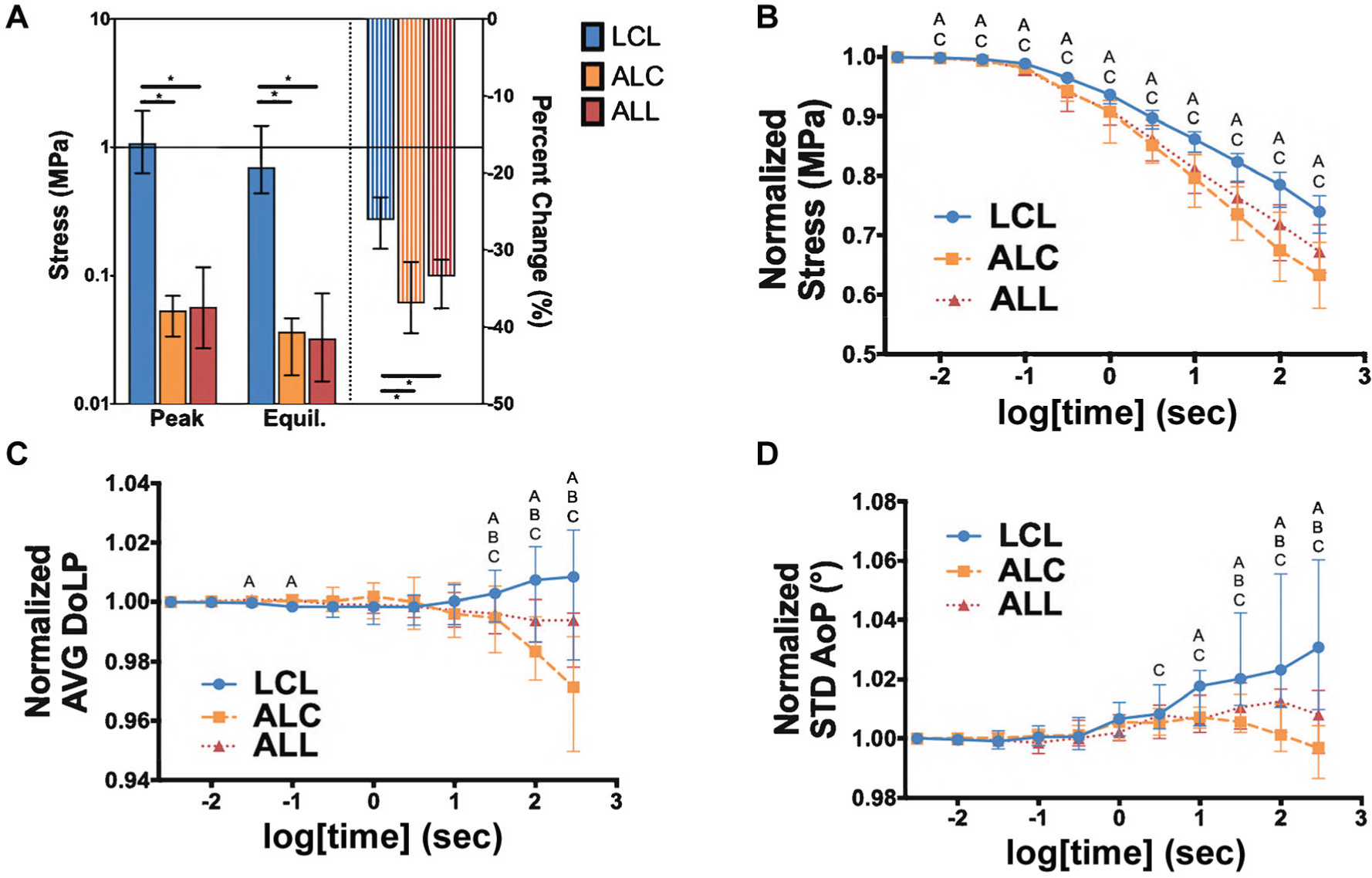
During stress-relaxation, (A) the LCL exhibited significantly higher peak and equilibrium stresses than the ALC and ALL. The ALC and ALL showed significantly more total relaxation than the LCL and (B) smaller normalized stress values during the relaxation phase. All 3 samples had significantly different normalized (C) AVG DoLP and (D) STD AoP at later time points during the relaxation phase. (A) *P < .05. Values are presented as median and interquartile range. (B-D) Values are presented as a normalized ratio to the peak value. A = significant difference between ALL vs LCL, B = ALL vs ALC, and C = LCL vs ACL. ALC, anterolateral capsule; ALL, anterolateral ligament; AVG DoLP, average degree of linear polarization; LCL, lateral collateral ligament; STD AoP, standard deviation angle of polarization.
Knee specimens with a distinct ALL showed different mechanical and microstructural properties as compared with knees with a nondistinct ALL (Figure 7). Distinct ALL samples had significantly larger toe (P < .001) and linear elastic (P < .001) moduli as compared with nondistinct ALL samples. They showed larger AVG DoLP values at zero (P = .04), transition (P = .02), and linear (P = .03) strain levels. They also showed smaller STD AoP values at zero (P = .006), transition (P = .006), and linear (P = .002) strain levels. These 3 distinct ALL tissues were found to cluster near the LCL data points in the correlation between mechanical and microstructural properties (see Appendix Figure A2, available online).

Distinct ALL samples showed significantly larger (A) toe and (B) linear moduli of elasticity, (C) larger AVG DoLP, and (D) lower STD AoP as compared with nondistinct ALL samples. (A, B) Note that the graph scale is log 10. *P < .05. Values are presented as median and interquartile range. ALL, anterolateral ligament; AVG DoLP, average degree of linear polarization; STD AoP, standard deviation angle of polarization.
Discussion
The mechanical and microstructural properties of the ALL and ALC were not different from each other but were significantly different from the LCL, confirming our primary and secondary hypotheses. When a distinct ALL was present, however, the mechanical and microstructural properties were more similar to a ligament. Further research should more precisely define the prevalence of distinct ALLs in the population and the implications of their presence.
Multiple studies have reported conflicting data supporting ligamentous and nonligamentous properties of the ALL based on anatomic, biomechanical, and radiographic investigations. ‡ Our technique examined the material properties of the anterolateral knee tissues at a microstructural level. Our data suggest that the collagen fiber orientation and mechanical properties of the ALL are more similar to the ALC than the LCL. Results were consistent in mechanical parameters (eg, tensile modulus) and microstructural parameters (eg, strength and variation of collagen alignment). These findings are in contrast to a previous cadaveric study that showed comparable histological and ultrastructural properties between the medial collateral ligament (MCL) and ALL, with both tissues exhibiting different properties as compared with capsular tissue. 36 Of note, this previous study included tissues from 8 donors, with an average age of 62 years, while our study included a much larger sample size and excluded tissue from older donors. Differences between the MCL and the LCL could also partially explain these contrasting results; the MCL has not been evaluated using our technique to confirm but could be completed in the future. The LCL was chosen as a representative ligament for the current study to better understand the complex interrelationship among all connective tissues of the anterolateral knee.
The mechanical properties of the ALL are conflicting in the literature. The linear modulus of the ALL has been reported as 174 MPa 42 and 1.20 MPa 54 ; our specimens had a median value of 3.66 MPa. Both studies42,54 used a dissection technique similar to ours. 8 However, Zens et al 54 left the ALL natively attached to its insertion and origin but excised all other tissue before testing. Interestingly, they found a similar modulus to that of the present study, while Smeets et al 42 harvested and tested the ALL similar to our study but found a much higher modulus. Our technique involved microtoming the sample to 1-mm thickness, which may partially explain this difference, even though it was corrected for cross-sectional area. The reported LCL modulus (289 MPa) 42 was also higher than what we found (162 MPa). In a subsequent study, the same group added a mechanical investigation of the ALC and inferior glenohumeral ligament (IGHL). 43 While the linear modulus for the ALC (62 MPa) was one-third that of the ALL (174 MPa), it is higher than our calculated ALC linear modulus (3.75 MPa). All 3 aforementioned studies42,43,54 had smaller sample sizes and older specimens, which could also contribute to differences. Guenther et al 14 mechanically tested anterolateral knee tissues and concluded that the ALC (analogous to what we called ALL) acts as a sheet of fibrous tissue; forces were observed to transmit perpendicular to the longitudinal axis of the tissue, suggesting that the ALL does not function like a ligament. It is important to note that they tested the structures in situ using the principle of superposition while we harvested tissue. The authors noted that 2 of 7 samples had a macroscopic thickening of the capsule in the anatomic region of the ALL, but they did not specifically describe the presence or absence of a distinct ALL in the anatomic region of the ALL. It is also unclear whether these 2 samples behaved differently than those without a thickening.
The IGHL has been likened to the ALL given its appearance and location in proximity to the glenohumeral joint capsule. The IGHL is widely known to play a crucial role as a static restraint within the shoulder. 2 Smeets et al 43 found that the mechanical tensile properties between the ALL and IGHL were similar, while those of the ALC was significantly lower. Histologic findings was also similar between the ALL and IGHL, with parallel collagen bundles with elastin, while the capsule had random collagen orientation. Interestingly, our stress-relaxation data found that the overall collagen alignment (AVG DoLP) and orientation (STD AoP) of the ALL stayed constant through a 300-second hold at 5% strain, in contrast to the LCL and ALC. It is plausible that the elastin fibers in the ALL have a role in this property. Our study differed in that we found no difference between the ALL and ALC, but it is unknown whether a distinct ALL would be more similar to the IGHL. This warrants further investigation, as the elastin fibers are thought to explain the function of the IGHL in stabilizing a highly unconstrained joint such as the shoulder. 48
Previous studies have reported variable prevalence or identification of the ALL in cadaveric dissections, ranging from 0% to 100%.8,12,38,45,50,51 Several studies have noted a thickening within the ALC but no distinct anatomic structure in anatomic dissections and MRI studies.11,21,30 In the current study, a distinct or nondistinct ALL was determined by the presence or absence of a ligamentous structure in the appropriate anatomic location. An internal tibial torque was applied to a flexed knee as described previously to identify the structure. 8 A previous study utilized an inside-out approach to identify and palpate the ALL from intra- and extra-articular windows for ease of identification. 25 We were able to identify all 3 distinct ALL samples without having to palpate inside out. Furthermore, this approach is used to dissect out any tissue that is not tensioned with internal rotation. We harvested a quadrilateral piece of ALL tissue, as our technique utilizes sectioning samples and requires a small size of tissue for testing. A distinct ALL running from the LFE to the midpoint between the fibular head and Gerdy tubercle was observed in 3 of 25 specimens. Other specimens had no appreciable ligamentous structure or had a nonligamentous capsular thickening as previously described. 35 Furthermore, a macroscopically observed distinct ALL corresponded with significantly more ligamentous-type mechanical and microstructural characteristics. While the distinct ALL group consisted of only 3 samples, the results were consistent across these 3 samples and were significantly different from data corresponding to the nondistinct ALL samples. Conversely, other studies have identified a distinct structure running in the anatomic area of the ALL in all specimens and confirmed tissue suggestive of a ligament through histology.15,36,50 However, our method of testing evaluated these tissues under load as compared with static histological assessment. A similar polarization imaging technique was used to study collagen fiber alignment in ligaments and tendons in several previous studies.29,41,53
The presence of a distinct ALL in 3 of our specimens suggests that there is variability in the thickness or “ligamentous” quality of the ALL region throughout the population. In a cadaveric study, Kent et al 26 found interspecimen variability in the ALL based on biomechanical properties. The authors also found that the ALL engaged in half of ACL-intact knees. In ACL-deficient knees, the ALL typically engaged with excessive anterior tibial translation, but this result varied among specimens. Noyes et al 32 tested the ALL and iliotibial band’s role in rotational stability in ACL-intact and ACL-deficient knees. This study concluded that the ALL and iliotibial band are secondary anterolateral constraints, but the authors noted significant variation in rotational stability among specimens with the same injury patterns. In conjunction with our data, these studies suggest that the indication for ALL reconstruction (ALL-R) and lateral extra-articular tenodesis (LET) procedures may be patient specific.
The clinical significance of a ligamentous ALL in the context of knee stability, risk of ACL tear, or failure after ACL reconstruction is unknown. Our study suggests that a small percentage of the population (12%) has a distinct ALL with function and structure representative of a ligament-like tissue. How the presence or absence of a native ligamentous ALL affects the risk for initial ACL injury, let alone subsequent reinjury after ACL reconstruction, is unknown. Furthermore, performing an ALL-R on a knee with a native capsular ALL could overconstrain the knee. Choosing between ALL-R and LET is also up for debate, as the anatomic line of constraint is presumably different between them. While the use of ALL-R or LET should likely be patient specific, the criteria to make that determination are unknown. Determining whether the ALL is ligamentous in an uninjured knee, let alone an injured knee, is limited by current techniques and imaging modalities, similar to the variability found in anatomic studies. 34 Further study is needed to establish better methods for determining the nature of the ALL in the native knee of injured and uninjured patients.
There are several limitations to this study. Sectioning the tissues to approximately 1-mm thickness with a freezing-stage microtome could lead to sampling error. Theoretically, the ALL could reside in a layer of the harvested quadrilateral tissue, and sectioning could miss this. Our technique requires thinning of the tissue to allow polarized light to shine through. We counteracted this by sectioning both sides of the tissue as described in the methods to ensure uniform sectioning. Furthermore, the average thickness of the ALL is 1 to 3 mm, which presumes that we would not have sectioned through the entirety of its thickness.8,15,50 While it is possible that sample preparation and the testing environment could affect overall stress-strain results, the current study used consistent methods validated from previously published studies, which are unlikely to confound the results.41,53 The tissues in this study were not evaluated in situ or in vivo. This study aimed to quantify the properties of tissues in the anterolateral knee using mechanical and microstructural analysis. Importantly, the goal of this study was to elucidate the material properties of the structures in the anterolateral knee but not to replicate the exact orientation of in vivo loading, as might be done in a clinical or macroscopic evaluation. The determination of distinct versus nondistinct ALLs was a subjective assessment, although our approach was systematic and our data suggest that the distinction was accurate. The inclusion of bilateral knee specimens could alter the estimated prevalence of distinct ligamentous ALLs. Anecdotally, 1 of the distinct ALLs in our study had a matched contralateral knee without a distinct ALL, while the other 2 distinct ALLs came from matched bilateral knees. The current study was not originally designed or powered to compare distinct versus nondistinct ALLs, and this comparison deserves further investigation. Finally, to analyze the microscopic structure, tissues were sectioned with a freezing-stage microtome to permit transmission of circularly polarized light. However, other similar studies of musculoskeletal connective tissues have not shown significant changes in properties when subjected to a limited number of freeze-thaw cycles.13,24,40
This study showed that there were no differences in the mechanical and microstructural properties between the ALL and ALC, while the LCL demonstrated different properties. The ALC and ALL showed weaker and more disperse collagen alignment as compared with the LCL. However, when a distinct ALL was present, there was stronger collagen alignment and larger modulus values suggestive of a ligamentous structure. Interperson variability in the anatomic, microstructural, and mechanical properties of the ALL is likely, suggesting that the ALL may have a selective role in the context of ACL injury, reconstruction, and rerupture.
Footnotes
Submitted April 1, 2020; accepted August 10, 2020.
Presented at the annual meeting of the AOSSM, July 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported in part by a grant from the Mid-America Orthopaedic Association. R.H.B. has received consulting fees from Sanofi-Aventis and education payments from Arthrex and Elite Orthopedics. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.