
Abstract
Background:
Relatively little is known about the true incidence of posterior shoulder instability in the United States.
Purpose/Hypothesis:
The purpose of this study was to characterize the incidence of posterior shoulder instability in the US military population and to examine which characteristics place these patients at highest risk. We hypothesized that the rate of posterior instability in this cohort of patients would be higher than previously reported.
Study Design:
Descriptive epidemiology study.
Methods:
All initial cases of posterior shoulder dislocation and subluxation in the Defense Medical Epidemiology Database were screened between 2016 and 2018 using the relevant International Classification of Diseases–Tenth Revision-Clinical Modification codes. Incidences were calculated, and multivariate Poisson regression was used to calculate adjusted rate ratios for the effects of sex, race, age, military service branch, rank, and year.
Results:
The overall unadjusted incidence was 0.032 per 1000 person-years for posterior dislocations, 0.064 per 1000 person-years for posterior subluxations, and 0.096 per 1000 person-years for all cases of posterior shoulder instability. The total incidence of all shoulder instability was 1.84 per 1000 person-years, with posterior shoulder instability accounting for 5.2% of total cases. For posterior subluxation, significant differences between groups were found in the unadjusted and adjusted rate ratio (ARR) for sex (ARR, 3.31; 95% CI, 1.85-5.93 for men), race (ARR, 0.458; 95% CI, 0.294-0.714 for Black servicemembers and ARR, 0.632; 95% CI, 0.421-0.948 for servicemembers of other race), age (ARR, 3.69; 95% CI, 1.56-8.70 for patients aged 30-34 years), and military service branch (ARR, 0.663; 95% CI, 0.460-0.955 for Air Force servicemembers). For posterior shoulder dislocations, a significant difference was found only between men and women (ARR, 4.55; 95% CI, 1.85-11.2 for men).
Conclusion:
The incidence of posterior shoulder instability among US military personnel is higher than previously reported in the general US population, with a majority of cases due to subluxation. This increased incidence is likely reflective of a young and highly active population along with improvements in awareness and diagnosis of posterior instability in recent years.
To date, relatively little is known about the true incidence of posterior shoulder instability in the United States.2,12,13,16 Initial population-based studies from the United Kingdom suggested that the incidence of posterior dislocation could be as low as 0.006 to 0.011 per 1000 person-years among the general population.12,13 However, these studies did not include specific information regarding instances of posterior subluxation versus dislocation.12,13 Population-based studies from the United States have reported similarly low numbers, with 1 Minnesota-based investigation showing a posterior shoulder instability rate of 0.046 per 1000 person-years, 28% of which were dislocations. 16
As noted by Owens et al, 9 general population-based estimates of both anterior and posterior shoulder instability may underestimate the true incidence in a young, physically active population, as this group represents the largest at-risk segment of the population. Indeed, 1 study of US military cadets found posterior shoulder instability incidence to be as high as 4.28 per 1000 person-years. 7 This represents a nearly 100-fold increase in incidence compared with that in other US-based general population studies, suggesting that posterior shoulder instability may be more common in a highly active population. Furthermore, among the US military population, nearly 10% of total shoulder instability events have been noted to be posterior in nature. 10
The US military population represents a closed system of highly active individuals who perform a rigorous battery of training exercises and recreational sports. This type of training as it relates to upper extremity injuries has been thoroughly described.5,11 To date, the incidence of posterior shoulder instability has not been determined in this population. Furthermore, with the mandated transition to the 10th revision of the International Classification of Diseases Clinical Modification (ICD-10 CM) in the United States in 2015, both directionality and instability type (subluxation vs dislocation) are now specified within US military databases. The purpose of this study was to characterize the incidence of posterior shoulder instability in the US military population and to examine which characteristics place these patients at highest risk. We hypothesized that the rate of posterior instability in this cohort of patients would be higher than previously reported.
Methods
Data Source
The Defense Medical Epidemiology Database (DMED) was screened between January 2016 and December 2018 in this study. This database captures health care services provided to active component servicemembers at both military treatment facilities and civilian-contracted facilities, all within a closed health care system, both local and abroad. It contains information on servicemember characteristics, ICD-10-Clinical Modification codes, military-specific data, and the total number of active component servicemembers for each year. This database is ideal for epidemiological studies, and its utility in studying orthopaedic injuries has been previously demonstrated.6,9,14,15 The years selected in this study represent all of the available and completely documented years after the conversion to ICD-10 that contain information on directionality and shoulder instability type (subluxation vs dislocation).
Case Selection
We selected all cases containing ICD-10 codes S43.021A-023A (posterior subluxation of humerus, initial encounter; right, left, and unspecified) and S43.024A-026A (posterior dislocation of humerus, initial encounter; right, left, and unspecified) for patients who sought medical attention for the above-listed codes. Only initial encounters were selected in order to reduce confounding from patients with recurrent instability as well as duplicate encounters for the same patient. The total number of shoulder instability cases was summed (S43.00-03), and the percentage of cases attributed to posterior instability was calculated. Information on servicemember sex, race, age, service branch, and rank were obtained for each patient. Race was divided into White, Black, and “other” categories. Age was classified as <20, 20-24, 25-29, 30-34, 35-39, and ≥40 years. Service branch was defined as Air Force, Army, Marines, or Navy. Rank was classified as E1-E4 (junior enlisted), E5-E9 (senior enlisted), O1-O3 (company grade officer), and O4-O9 (field grade/general officer). The total number of active component servicemembers was screened by each of these variables as well. One exposure year for a servicemember was defined as 1 year of active duty service in the US Armed Forces.
Statistical Analysis
Incidences and unadjusted rate ratios of posterior shoulder subluxation and dislocation per 1000 person-years were calculated for each of the demographic and military-specific categories. A multivariate Poisson regression was then performed to calculate adjusted rate ratios while controlling for sex, age, race, military service, and rank. Furthermore, 95% CIs were calculated for all rate ratios. P < .05 was considered significant (SPSS Statistics Version 26.0; IBM Corporation).
Results
Over the 3-year course of the study period, there were 124 posterior dislocations and 248 posterior subluxations among a population of 3,868,007 person-years. The overall unadjusted incidence was 0.032 per 1000 person-years for posterior dislocations, 0.064 per 1000 person-years for posterior subluxations, and 0.096 per 1000 person-years for all cases of posterior shoulder instability. The total incidence of all shoulder instability was 1.84 per 1000 person-years over this time period, and posterior shoulder instability accounted for 5.2% of all cases of shoulder instability.
For posterior subluxation, significant differences between groups were found in the unadjusted and adjusted rate ratios for sex, race, age, service, and year (Table 1). The incidence was 0.073 per 1000 person-years for men compared with 0.019 for women, giving an adjusted rate ratio of 3.31 (95% CI, 1.85-5.93) for men. Race was also a significant factor. Specifically, shoulder subluxation occurred at a rate of 0.075 for White servicemembers compared with 0.033 for Black servicemembers and 0.049 for servicemembers of other race; adjusted rate ratios were 0.458 (95% CI, 0.294-0.714) for Black servicemembers and 0.632 (95% CI, 0.421-0.948) for servicemembers of other race. All age groups (Table 1) except for the ≥40-year group had significantly increased risk of subluxation compared with the <20-year group, and the 30- to 34-year group had the highest adjusted rate ratio (3.69; 95% CI, 1.56-8.70). The branch of military service was also significant, with servicemembers in the Navy experiencing posterior subluxation at a rate of 0.075 and Air Force servicemembers at a rate of 0.052. This gave an adjusted rate ratio of 0.663 (95% CI, 0.460-0.955) for Air Force servicemembers compared with Navy servicemembers. Finally, the incidences were different for different calendar years. The incidence rate was 0.076 in 2017 compared with 0.054 in 2018, giving an adjusted rate ratio of 1.41 (95% CI, 1.04-1.92). The differences in adjusted rate ratios between 2016 and 2018 or between any military ranks were not significant.
Unadjusted and Adjusted Rates and Rate Ratios of Posterior Shoulder Subluxations Among US Armed Forces Servicemembers Between 2016 and 2018 a
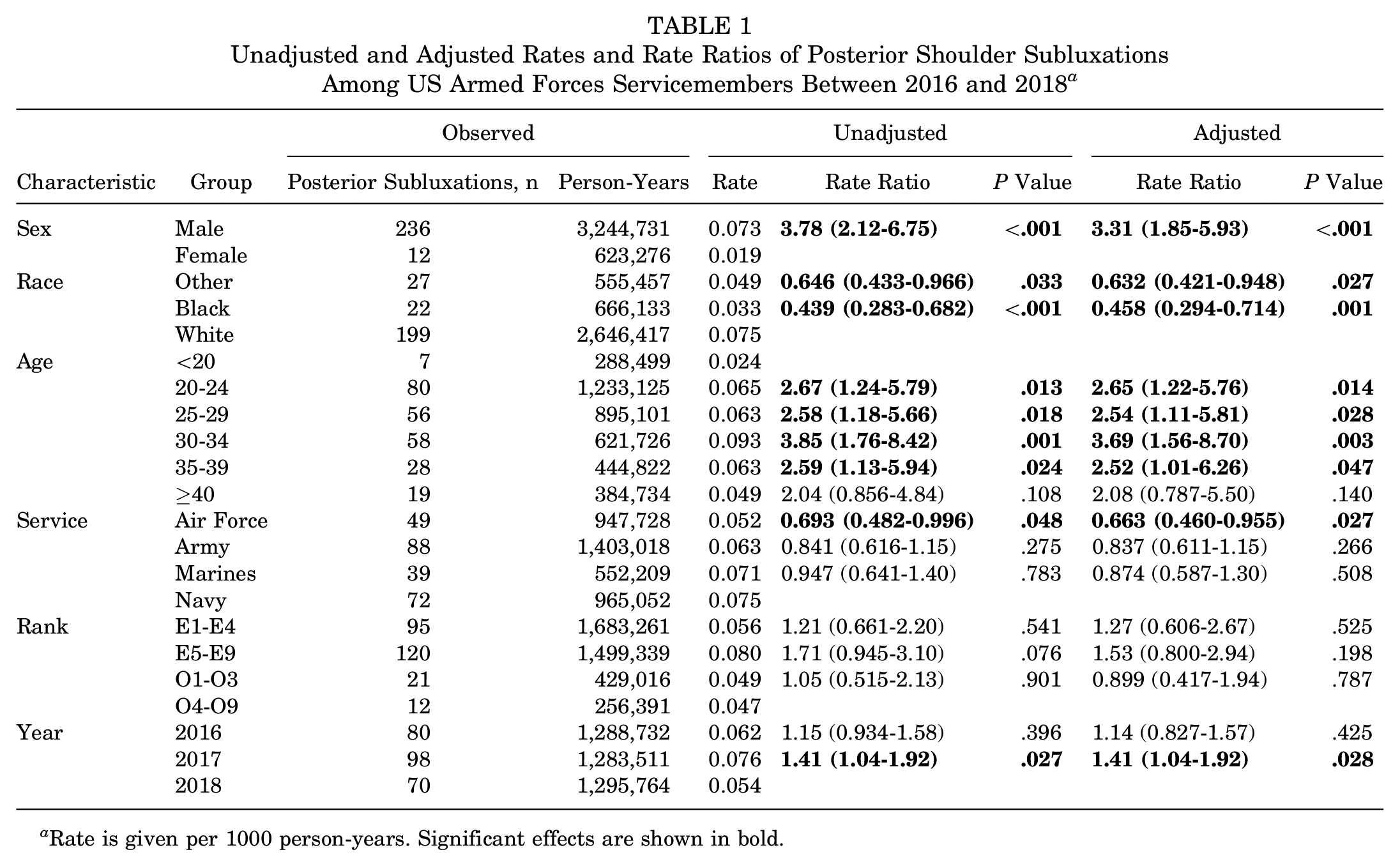
Rate is given per 1000 person-years. Significant effects are shown in bold.
For posterior shoulder dislocations, a significant difference between groups was found only for men versus women (Table 2). Dislocations occurred at a rate of 0.037 for men compared with 0.008 for women. This gives an unadjusted rate ratio of 4.57 (95% CI, 1.87-11.2). The adjusted rate ratio was almost identical (4.55; 95% CI, 1.85-11.2), as no other variables had significant effects.
Unadjusted and Adjusted Rates and Rate Ratios of Posterior Shoulder Dislocations Among US Armed Forces Servicemembers Between 2016 and 2018 a
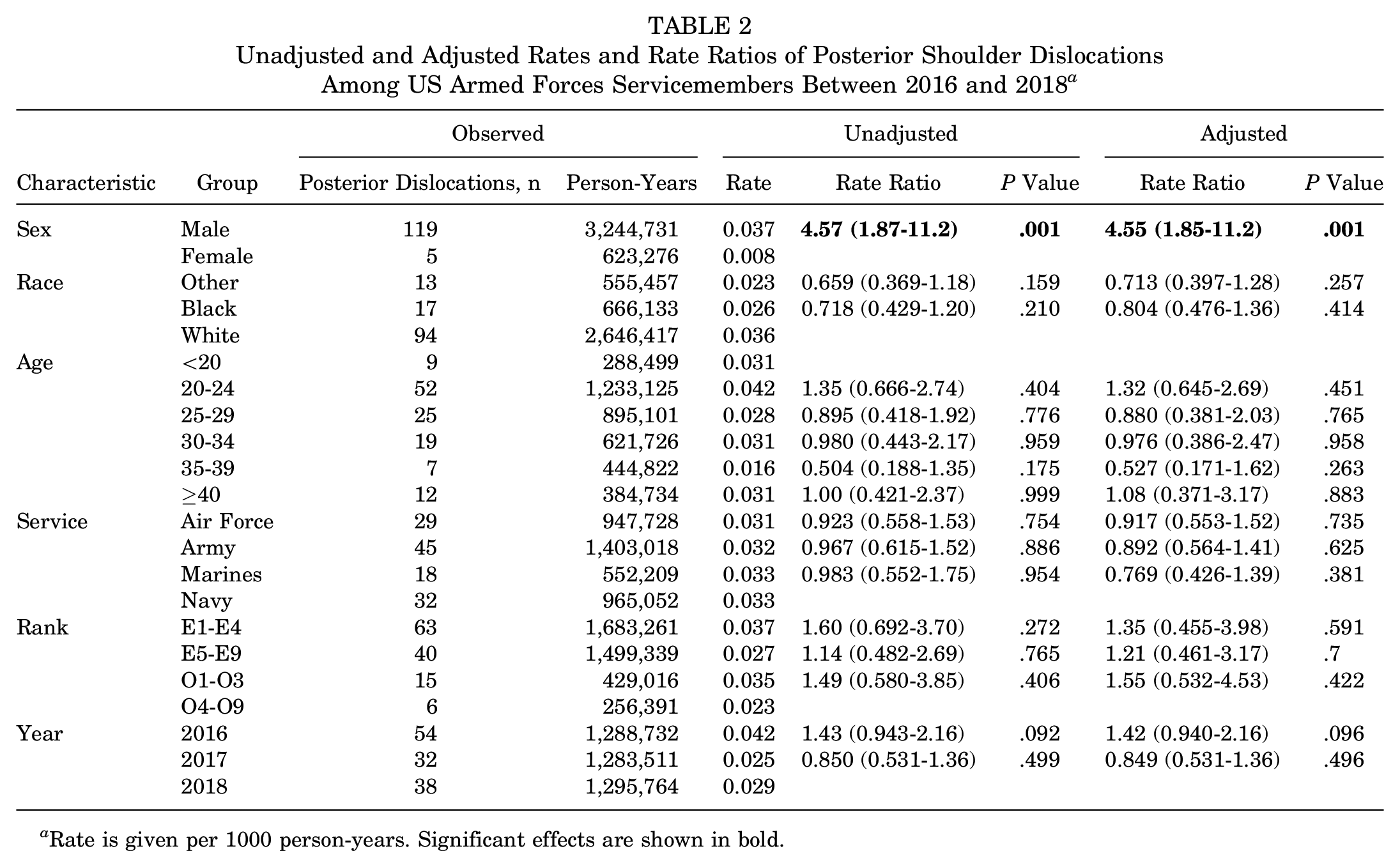
Rate is given per 1000 person-years. Significant effects are shown in bold.
Discussion
The purpose of this study was to characterize the incidence of posterior shoulder instability in the US military population and to examine which demographic characteristics place these patients at highest risk. In keeping with what is currently known about posterior instability, we hypothesized that posterior instability in this cohort of patients would be more common than previously reported, with a larger proportion of patients with subluxations. We also hypothesized that younger, more active male participants would be at highest risk for posterior instability.
Although shoulder instability is well studied in the literature, posterior shoulder instability is typically regarded as a rare clinical entity.2,9 Posterior instability is noted to account for <10% of all shoulder instability cases, with acute traumatic posterior dislocation occurring at rates as low as 0.01 per 1000 person-years. 2 In this population of US military personnel, posterior instability accounted for 5.2% of all cases of shoulder instability. This study represents the first known study to use the DMED to determine the incidence of posterior shoulder instability among US military servicemembers, in addition to differentiating between dislocation and subluxation. In comparison, Woodmass et al 16 sought to better characterize the rate of posterior shoulder instability in the general population over a 22-year period. An incidence of 0.046 per 1000 person-years was reported, with posterior instability being more common in male participants (0.0886/1000 person-years), particularly those aged 14 to 19 years (0.32/1000 person-years). 16 Our investigation found a 2-fold increase in incidence compared with that in this general population, with posterior instability occurring at a rate of 0.096 per 1000 person-years. This 2-fold increased rate was likely attributable to the increased activity level of military personnel compared with the general population.
The US military represents a highly active patient population that draws similarities to other at-risk populations, such as heavy manual laborers. Other studies of military cadets have largely focused on athletes and may not be generalizable to civilian populations.7,8 Lanzi et al 7 used the Cadet Illness and Injury Tracking System over a 6-year period to determine the rate of instability among recreational and varsity athletes within the US Military Academy. A very high rate of injury was found in this group. Specifically, the authors reported an overall rate of 4.28 per 1000 person-years, nearly 100 times the rate quoted previously. 7 Wrestlers had the highest injury rate (34.15 per 1000 person-years). 7 Although Lanzi et al investigated a unique cohort of trainees that may be incompatible with the general population, their study did demonstrate that posterior instability may be more common than traditionally believed, particularly as cadets experience a significant number of athletic exposures compared with other members of the military, especially in the form of contact sports. Our study expands on this knowledge by investigating all US military servicemembers, who serve as a more generalizable patient population of highly active individuals than do cadets alone. Although US military servicemembers are often called on to perform strenuous activities as part of their daily training and job duties, the population studied here is more likely to represent a general active population, in which the dedicated high-level athletic exposures seen in the cadet population are absent. 8 More specifically, these strenuous activities include lifting heavy objects overhead, upper body strengthening in the form of push-ups and pull-ups, climbing, crawling, and negotiating physical obstacles along with difficult terrain. 3 As such, we believe this population is most comparable with heavy manual laborers in the general US population.
A crucial finding of the current study was that posterior instability did not always present as frank dislocation, with subluxations being the more common initial presentation. This is the first study, to our knowledge, which used the specific ICD-10 codes for dislocation and subluxation to separate these clinical entities. In our cohort, posterior subluxation occurred in approximately a 2:1 ratio to dislocation (0.064/1000 person-years compared with 0.032/1000 person-years for dislocation). It follows that subluxation may be an underrecognized phenomenon in the early presentation of posterior instability and that physicians must maintain a high suspicion in at-risk populations like the one studied here.
In addition to overall incidence, risk factors for posterior instability were examined. When sex was evaluated as an independent risk factor for posterior instability, our finding of male predominance was consistent with previous work.2,9,11,12,16 Interestingly, male sex was the only statistically significant characteristic with an increased risk of posterior dislocation. Dislocations occurred at a rate of 0.037 for men compared with 0.008 for women. A similar result was found for subluxation, with the incidence of 0.073 per 1000 person-years for men compared with 0.019 for women, giving an adjusted rate ratio of 3.31 (95% CI, 1.85-5.93). Lanzi et al 7 found similar results, reporting that male participants were more likely to sustain instability events compared with female participants (4.67 vs 2.04 per 1000 person-years, respectively).
Another risk factor for posterior subluxation in the current study was age. All age groups younger than the ≥40-year group had a significantly increased risk of subluxation, with the 30- to 34-year age group having the highest adjusted rate ratio at 3.69. This is consistent with that reported in other studies that identified age <40 years as an independent risk factor for posterior instability. 2
Several other risk factors were investigated in the present study. As was shown with previous studies of shoulder instability within the military, White servicemembers experienced posterior subluxation at a rate greater than that of servicemembers of other race or Black servicemembers. 9 Servicemembers in the Navy, Army, or Marines also had a significantly greater risk of subluxation compared with those in the Air Force (adjusted rate ratio, 0.663). This effect of servicemembership may reflect differing types of activity. Further examination of the modifiable and nonmodifiable occupational risk factors associated with military service branch is warranted. Finally, although we observed no clear trend among incidence of posterior subluxation and dislocation over time, we did find that the incidence of posterior subluxation decreased from 2017 to 2018. Although further data are required to clearly delineate a trend, this decrease could represent an increased familiarity with the newer ICD-10 coding system and subsequent use of alternative codes.
Limitations
This study is not without limitations. As with any database study, the overall quality of the data depends on the completeness, validity, consistency, timeliness, and accuracy of the patient records. 4 This is particularly true for the diagnosis of posterior instability, which is often confused with multidirectional instability, an increasingly recognized phenomenon. 1 Unfortunately, because the DMED database does not allow the screening of patient radiographs or advanced imaging, we were unable to support the diagnosis of posterior instability radiographically or further comment on the pathoanatomic bony and soft tissue injuries observed in these patients, which represents an intrinsic weakness of this study. Furthermore, because this database does not allow for following patients over time, we were unable to follow the ICD-10 coding over time to further support the initial diagnosis. Although errors such as injury miscoding may occur, this method is consistent with that used in previously reported shoulder epidemiology studies, as military personnel have routine access to advanced musculoskeletal care. 9 Furthermore, this study is the first to our knowledge to investigate the specific ICD-10 codes for dislocation and subluxation, adding valuable information to the epidemiological study of posterior shoulder instability. Another limitation of this study is that by including only the first occurrence of injury, our data may not have captured cases that were initially classified as “shoulder strain.” However, this filter was intentionally used to remove multiple instances in the same patient, which would overinflate the true incidence. We can make no definitive statement on recurrent injuries because our study was designed to capture acute instability and was limited to 1 injury per servicemember. Despite the limitations noted, the ambulatory care data contained within the DMED provide many advantages over similar civilian systems. Patient data are collected for all visits in the population of interest (eg, US servicemembers on active duty) with use of standardized inpatient and ambulatory care data records throughout military treatment facilities. 4
Conclusion
The incidence of posterior shoulder instability among US military personnel is higher than previously reported in the general US population, with a majority of cases due to subluxation. This increased incidence is likely reflective of a young and highly active population along with improvements in awareness and diagnosis of posterior instability in recent years.
Footnotes
Submitted April 22, 2020; accepted August 18, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.F.D. has received education payments from Medical Device Business Services and hospitality payments from Zimmer Biomet outside the submitted work. S.L.B. has received hospitality payments from Stryker Corporation and Zimmer Biomet. B.D.O. has received consulting fees from DePuy Orthopaedics, Linvatec, Medical Device Business Services, and Musculoskeletal Transplant Foundation; royalties from Linvatec Corporation; and honoraria from Vericel. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.