
Abstract

The authors appreciate the letter to the editor and all the insightful points it raised.
First, it should be pointed out that the authors had an error on the inclusions criteria. The prospectively collected database utilized to search these patients regularly collects lateral center-edge angle (LCEA), anterior center-edge angle (ACEA), and Tönnis angle and so they were utilized to find our cohort. The true inclusion criteria for this study were LCEA <25°
Although LCEA solely measures lateral acetabular coverage, and fails to account for the global morphology of the acetabulum, it is commonly used in isolation to define dysplasia in the literature. Pereira et al 23 demonstrated that while using only the LCEA to define borderline or mild dysplasia, 20% to 39% of hips categorized as normal were actually mildly dysplastic using other radiographic measurements (Tönnis angle, depth/width ratio, and acetabular head index). This highlights the potential importance of including several radiographic parameters while categorizing hip dysplasia (Table 1) and supports the findings of our study as well.
LCEAs in “Mild” or “Borderline” Dysplasia a
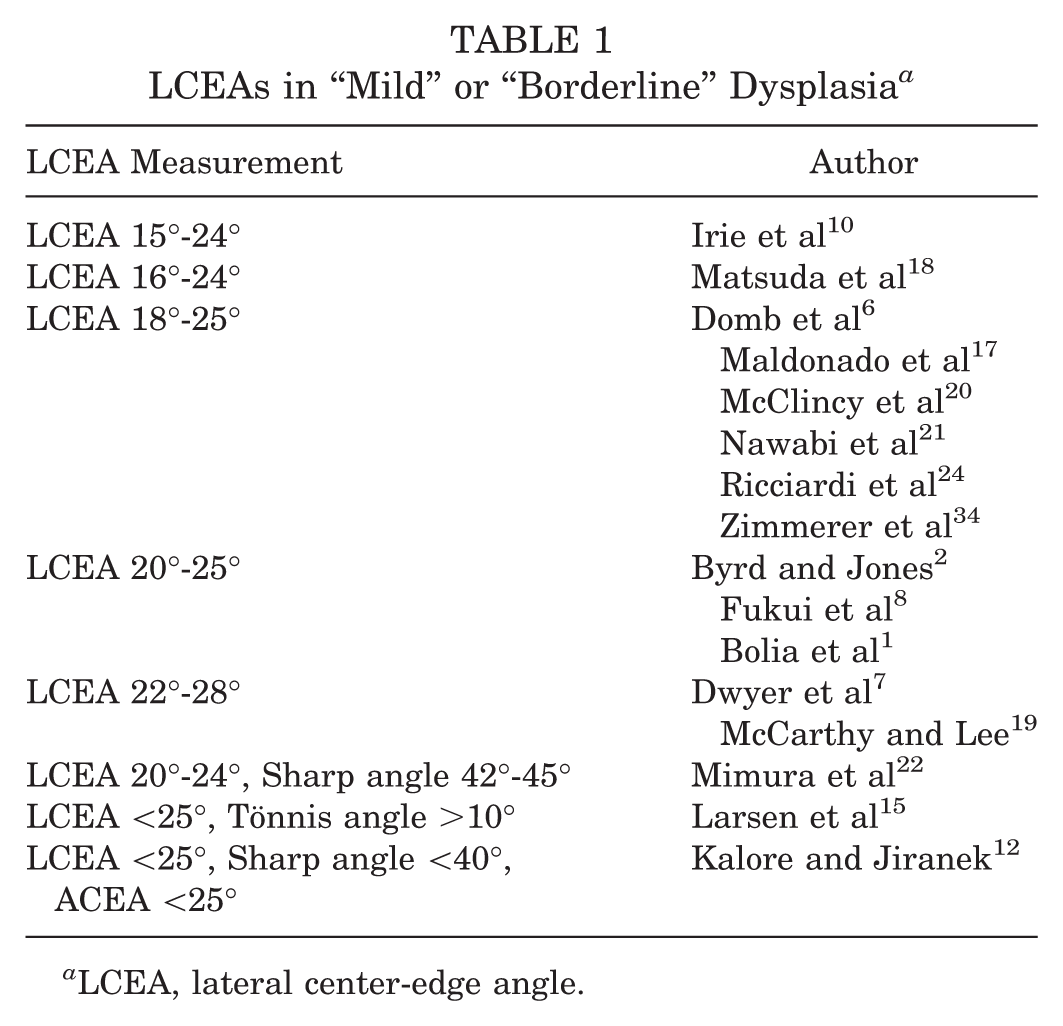
LCEA, lateral center-edge angle.
Furthermore, studies analyzing associations between different radiographic parameters have found they are often not correlated.6,18,25 McClincy et al 20 evaluated 98 patients with borderline dysplasia as defined by a LCEA of 18° to 25° and found the ACEA was abnormal in 45% of patients, femoro-epiphyseal acetabular roof (FEAR) index was abnormal in 34% of patients, and anterior wall index (AWI) was abnormal in 30% of patients. 20 The findings in this study demonstrate radiographic indicators of borderline dysplasia are often independent of each other. This is precisely why in our study the means of the various parameters were not in the dysplastic range.
Defining dysplasia with one measure (lateral coverage with LCEA), in our view, is very over-simplified and fails to take into account other features of borderline hips such as anterior and posterior acetabular coverage, rotational alignment of the femur and acetabulum, and proximal femoral morphology. 26 All of these morphologic features, in addition to patient demographics, ligamentous laxity, and spine issues, should be considered during the evaluation of the dysplastic hip. The authors agree that in borderline cases looking at multiple parameters can be helpful in making the final decision whether hip arthroscopy is reasonable or if the patient is better served with an osteotomy. As this study demonstrated, the Tönnis angle is a measure that is of clinical significance. The commentary’s remarks considering anterior and posterior wall coverage make sense from a biomechanical standpoint; however, no clinical study has demonstrated improved outcomes when AWI and posterior wall index (PWI) are solely considered. On the other hand, when used together with a handful of other radiographic indicators, or “clusters” of indicators (FEAR index, LCEA, Tönnis angle, Alpha angle, and femoral neck angle), there may be a correlation, but it is undetermined the extent to which inclusion of AWI and/or PWI alone play in improved outcome measures. 34
Despite this observation, most studies use only LCEA as a measure of dysplasia (Table 1). Wiberg, in his original article, concluded hips with a LCEA <20° were dysplastic while hips with a LCEA >25° were normal. 32 Hips with a LCEA between 20° and 25° were concluded to be indeterminate. This indeterminate zone is what we term “mild” or “borderline” dysplasia, which are often synonymously used in the literature.3,4,8,14 Specific criteria as to what LCEAs fall within the terminology of “mild” or “borderline” dysplasia differ according to author. Measurements vary from as low as 16° to as high as 28° (Table 1). Rarely are other radiographic parameters considered when defining borderline or mild hip dysplasia (Table 2).
Radiographic Indicators of Acetabular Morphology a
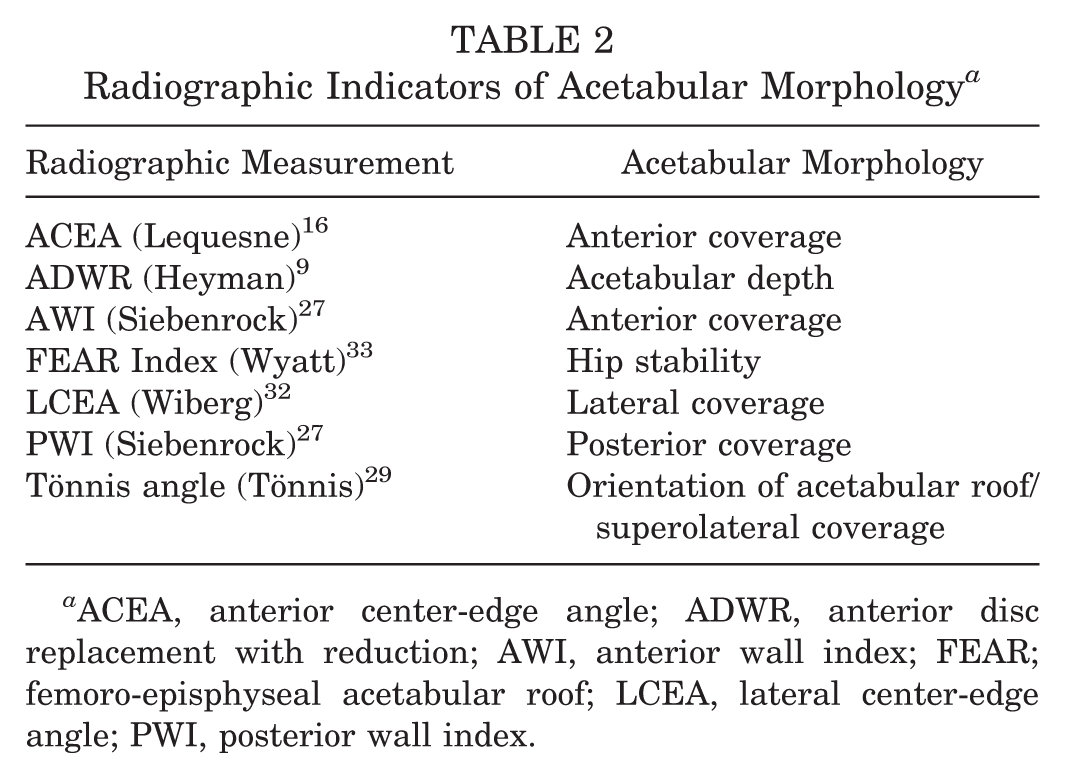
ACEA, anterior center-edge angle; ADWR, anterior disc replacement with reduction; AWI, anterior wall index; FEAR; femoro-episphyseal acetabular roof; LCEA, lateral center-edge angle; PWI, posterior wall index.
To the point of the commentary about utilizing 2-dimensional (2-D) radiographic parameters to evaluate hips, regardless of the measure (ACEA, Tönnis, PDI, ADI, FEAR, etc), it is important to critically assess the technical adequacy of patient radiographs. Several studies have demonstrated that pelvic tilt/rotation, together with errors in imaging technique, have been shown to effect the accuracy of these measurements.13,25,28 In the setting of the pitfalls of 2-D radiographic evaluation of dysplasia, an ongoing matter of study has been the utility of 3-dimensional imaging techniques (computed tomography [CT], magnetic resonance imaging [MRI]) in borderline hip dysplasia.5,15 The optimal method for using CT/MRI in this setting is still a matter of debate as we continue to establish normative data with regard to normal controls, and evaluate the most efficient and reproducible method.11,15,30,31
Footnotes
Submitted November 9, 2020; accepted November 12, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.G.D. has received consulting fees from Arthrex and Pacira; royalties from Arthrex and DJD LLC; and education payments from Medwest Associates. D.E.H. has received education payments from Arthrex, Smith & Nephew, and Goode Surgical Inc; and personal fees from Arthrex. A.J.K has received research support from Aesculap/B.Braun, Ceterix, Exacteh, Gemini Medical, and Histogenics; consulting fees from JRF Ortho and Vericel; speaking fees from Arthrex; and royalties from Arthrex; he is a board or committee member for the Musculoskeletal Transplant Foundation and has stock/stock options in Responsive Arthroscopy. B.A.L. has received research support from Arthrex, Biomet, Smith & Nephew, and Stryker; educational support from Linvatec; consulting fees from Arthrex; speaking fees from Arthrex and Smith & Nephew; and royatlies from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.