
Abstract
Background:
The lateral femoral notch sign (LNS) is a bony impression on the lateral femoral condyle correlated with anterior cruciate ligament (ACL) injury. Its presence is associated with lateral meniscal injury and higher cartilage degradation on the lateral femoral condyle.
Purpose/Hypothesis:
The purpose was to investigate the effect of the presence and magnitude of LNS on rotatory instability. The hypothesis was that a positive LNS is correlated with a high-grade pivot shift (PS).
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A total of 90 consecutive patients with complete ACL tears between 2013 and 2017 underwent intraoperative kinematic evaluation with the surgical navigation system and were included in the present study. The same surgeon performed a standardized PS under anesthesia. The PS was quantified through the acceleration of the lateral compartment during tibial reduction (PS ACC) and the internal-external rotation (PS IE). Presence and depth of LNS were evaluated on sagittal magnetic resonance images (1.5-T).
Results:
In 47 patients, the LNS was absent; in 33, the LNS depth was between 1 mm and 2 mm; and in 10 patients, it was deeper than 2 mm. Patients with a notch deeper than 2 mm showed increased PS ACC and PS IE compared with the group without the LNS. However, no significant differences were present between the group with a notch between 1 and 2 mm and the patients without LNS. Receiver operating characteristic curve analysis showed that 2 mm was the most predictive cutoff value to identify the “high-grade rotatory instability” group, with an accuracy of 77.8% and 74.4% and a specificity of 95.5% and 93.9% referred to the PS ACC and PS IE, respectively.
Conclusion:
The presence of a lateral LNS deeper than 2 mm could be used for the preoperative identification of patients with a high risk of increased rotatory instability.
The lateral femoral notch sign (LNS) is a bony impression on the lateral femoral condyle that can be seen on conventional lateral radiographs or magnetic resonance imaging (MRI) in approximately 6% to 25% of the patients who experience an anterior cruciate ligament (ACL) injury.8,11
The LNS was initially described by Losee et al 20 in 1978. The authors did not classify the depression in terms of size or depth, but they suggest the presence of “pathological notches” in cases of fissured or eroded cartilage at its bottom. The authors also believed that the LNS was the result of chronic subluxation and repetitive impingement of the posterolateral margin of the tibia against the lateral femoral condyle, with a progressive deepening of this bony impression. However, subsequent studies have proved the presence of the LNS due to ACL injuries, primarily if the trauma occurs with a pivot mechanism.3,8,10,33 Recently, the LNS has also been correlated with an increased incidence of lateral meniscal injury8,16 and higher cartilage degradation on the lateral femoral condyle, even after an uneventful ACL reconstruction (ACLR). 1 On the practical side, its presence is useful to increase suspicion of an ACL injury in the acute setting when physical examination of the knee is not possible because of knee pain and swelling. 10
Once ACL injury is confirmed, it is crucial to quantify the knee instability: the pivot-shift (PS) test is a complex and multiplanar clinical examination that is predictive of osteoarthritis, failure to return to sports, and low clinical scores.12,35 Unfortunately, the PS is more complex and difficult to perform and assess when compared with other uniplanar clinical examinations; therefore, different devices have been developed, such as electromagnetic sensors,27,40 accelerometers,2,15,25 and the surgical navigation system, which is considered the gold standard, for intraoperative kinematic evaluation.13,42 Given that the preoperative laxity influences the results of the ACLR, 21 it is crucial to identify the subset of high-risk patients before surgery to set the patient’s expectations and possibly to plan additional surgical procedures such as lateral extra-articular tenodesis (LET).
It is also known that physiological and morphological bone variations, especially on the lateral side of the knee, have been associated with high-grade PS and increased risk of ACL revision.26,30,31,39 Considering this background, the present study aimed to investigate the effect of the presence and magnitude of LNS on rotatory laxity. The hypothesis of the study was that a positive LNS will be correlated with higher rotatory laxity during the PS maneuver assessed with the surgical navigation system.
Abbreviations used in this article are shown in Table 1.
List of Abbreviations
Methods
Ethics
All the enrolled patients signed informed consent forms to undergo the surgical procedure, and the institutional review board (IRB) of Istituto Ortopedicco Rizzoli (Bologna, Italy) approved the research study (IRB approval: 0013202, April 19, 2013).
Patient Characteristics
In total, 97 consecutive patients who underwent navigated ACLR by a single senior surgeon (S.Z.) between 2013 and 2017 were screened for eligibility. All the patients underwent an MRI scan (1.5-T) preoperatively; image acquisition was performed at the same institution, using the same protocol, with the patient in a supine position. Inclusion criteria for the navigated ACLR were age 16 to 50 years; complete, traumatic, and unilateral ACL injury; no concomitant posterior cruciate ligament, posterolateral corner, lateral collateral ligament, or medial collateral ligament lesion; no previous knee surgery; and absence of mild to severe knee osteoarthritis (Kellgren-Lawrence score III-IV). For the present study, patients with low-quality MRI images, presence of impaction fracture on the lateral tibial plateau, and incomplete kinematic data were excluded.
Testing Protocol
To evaluate joint laxity, the authors opted for a surgical navigation system (BLU-IGS; Orthokey) equipped with software dedicated to intraoperative kinematic acquisitions (KLEE; Orthokey) (Figure 1). Once the anatomic bony landmarks were identified, the same senior orthopaedic surgeon, with an experience of more than 200 navigated ACLRs, 7 performed the PS test under anesthesia following a standardized maneuver.9,29 The examination protocol was performed by utilizing the method developed by Martelli et al.22,23 The PS test was quantified, according to the literature, 28 through 2 different parameters: the posterior acceleration of the lateral tibial compartment during tibial reduction (PS ACC) and the internal-external rotation (PS IE).

Setting of the surgical navigation system for intraoperative kinematic assessment.
The reliability of all laxity tests performed at maximum force has been evaluated in previous studies.17,22,23 To avoid bias in the acquisition of the quantitative results, the whole set of tests and reconstructions was blind tested. Data were captured offline with a specially developed MATLAB interface (The MathWorks Inc).
Notch Sign Measurement
The sagittal MRI images were evaluated by a single observer (P.A.) who was blinded to the patients’ kinematic data. The presence and depth of LNS were evaluated by using the method previously described by Warren et al 41 (Figure 2), employing the software DICOM viewer Osirix Lite 7.0.3 (Pixmeo). The LNS was identified on MRI sagittal images, and the slice with the deepest notch was used for the analysis. According to Lodewijks et al, 16 patients were first divided into 2 groups: patients without LNS, the “no LNS” group; and patients with a positive LNS (>1 mm), the “LNS” group. Further categorization was made within the LNS group based on the depth of LNS, and patients were divided into the “LNS between 1 and 2 mm” group and “LNS >2 mm” groups.10,16 To assess the inter-rater reliability, one of the authors (G.D.F) performed the same measurement on 25 MRI scans randomly chosen from those included in the study.
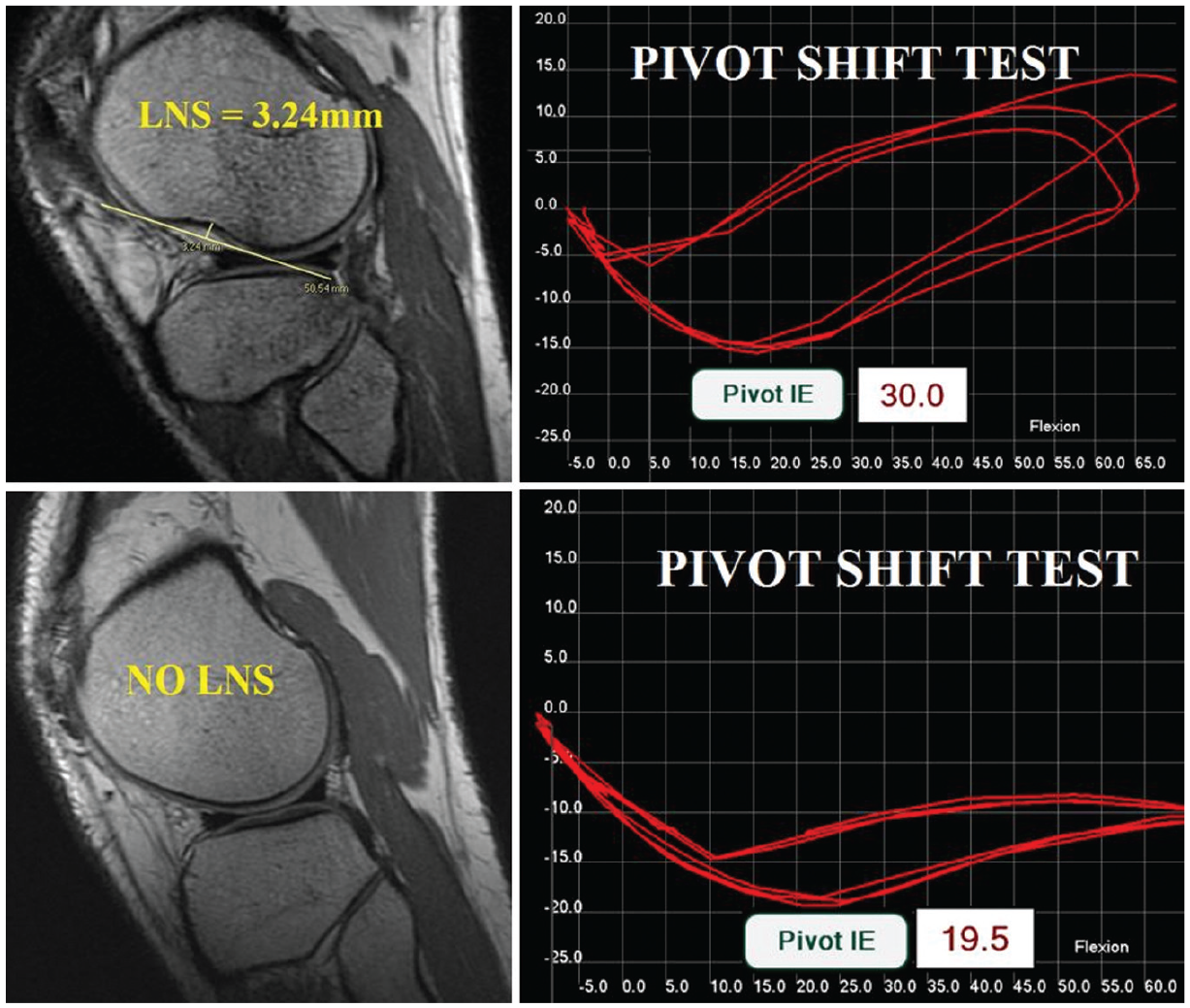
Presence of LNS evaluated through a magnetic resonance imaging scan of 2 patients (left). Quantitative evaluation of the PS IE performed through the surgical navigation system for the same patients (right). Note the increased PS IE in the patient with a notch deeper than 2 mm, when compared with the patients without the LNS (NO LNS). LNS, lateral notch sign; PS IE, pivot-shift internal-external rotation.
Statistical Analysis
The evaluation of the LNS was performed separately by 2 operators (P.A. and G.D.F). The intraclass correlation coefficient (ICC 2,1) was calculated to verify the agreement between the measurements. The normal distribution of the kinematic data was verified using the Shapiro-Wilk test. Normally distributed continuous variables were presented as mean and standard deviation, while categorical variables were presented as a percentage of the total. The 1-way analysis of variance was performed to assess the between-group differences of continuous variables, while the t test with Dunn-Sidak post hoc correction for multiple comparisons was used to compare the groups with each other. Differences between the groups were considered statistically significant if P < .05. A receiver operating characteristic (ROC) curve analysis was performed to determine the most predictive LNS cutoff value. Sensitivity, specificity, positive predictive value, negative predictive value, accuracy, and Youden Index were computed for multiple LNS cutoff values and used to determine the best one. Patients with values of PS ACC or PS IE above the 75th percentile were considered “high rotatory instability” patients. Moreover, the 75th percentile value of either the PS ACC or the PS IE parameters were used as cutoff input for the ROC analysis, aiming to identify patients with a “high-grade rotatory laxity.” A post hoc power analysis was performed using G*Power 3.1.9.4 (Franz Paul) to ensure the statistical power given the sample size of the present study. Based on the results of the t test with P value correction regarding the posterior acceleration of the tibial lateral compartment, a power of 0.80 was calculated. A further analysis was conducted to evaluate possible confounding variables in the group distribution. The parameters evaluated were sex, presence of medial meniscal tear, presence of lateral meniscal tear, and presence of tibial slope greater than 9°, which has been reported to influence the magnitude of PS. 31 All the statistical analyses were performed in MATLAB.
Results
From the 97 patients of the initial cohort, 2 patients had poor-quality MRI scans, 2 had incomplete kinematic data, and 3 had a posterolateral tibial plateau impaction fracture and were therefore excluded, leaving 90 patients (78 men, 12 women) with a mean age of 26 ± 8 years (range, 16-48 years) for the final analysis.
A total of 43 patients (48%) had a positive LNS. Among these, 33 (37%) showed an LNS between 1 mm and 2 mm, and 10 (11%) showed an LNS deeper than 2 mm.
The analysis of the confounding variables resulted in no statistically significant differences based on sex, presence of medial/lateral meniscal tears, and presence of tibial slope greater than 9°. 31
Patients with a positive LNS had higher PS ACC compared with patients without LNS, while PS IE was not significant (Table 2).
Evaluation of the Dynamic Knee Laxity Through the Pivot Shift Test Performed With the Surgical Navigation System a
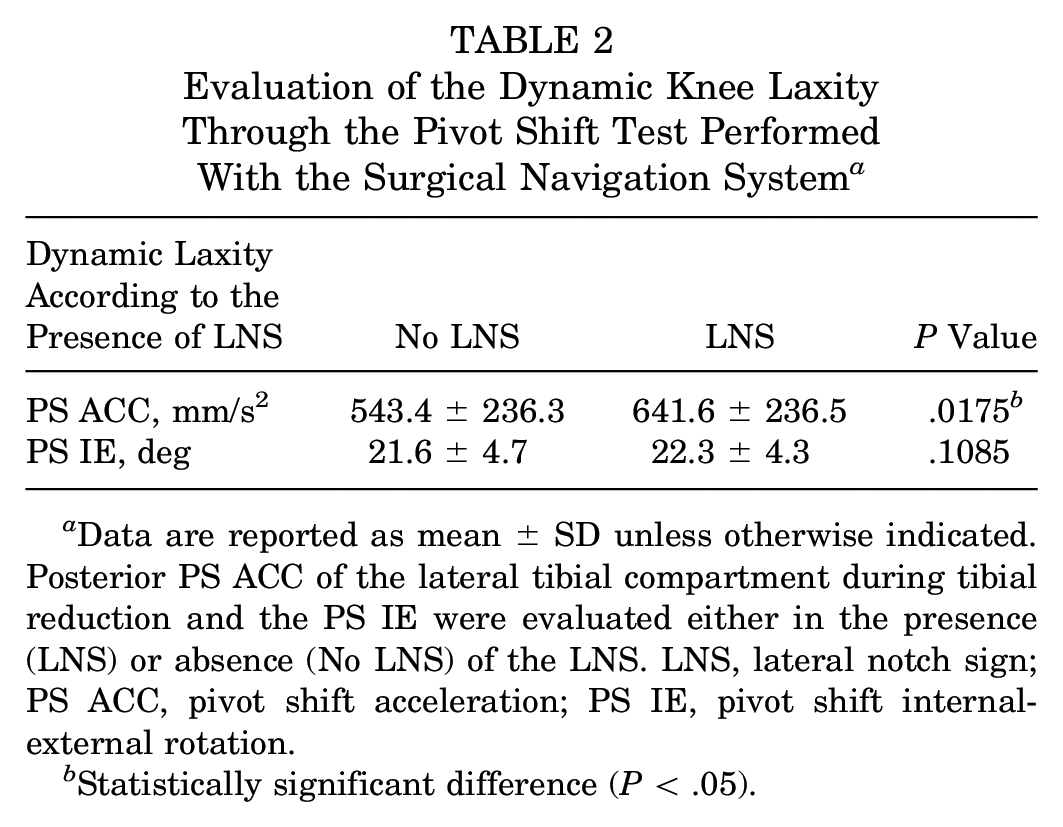
Data are reported as mean ± SD unless otherwise indicated. Posterior PS ACC of the lateral tibial compartment during tibial reduction and the PS IE were evaluated either in the presence (LNS) or absence (No LNS) of the LNS. LNS, lateral notch sign; PS ACC, pivot shift acceleration; PS IE, pivot shift internal-external rotation.
Statistically significant difference (P < .05).
When further stratifying the LNS according to its depth, patients with a notch deeper than 2 mm showed larger PS ACC and PS IE compared with the group without the LNS. However, no significant differences were present within the group with a notch between and 1 and 2 mm and the patients without LNS regarding both parameters (Table 3).
Evaluation of the Dynamic Knee Laxity Through the PS Test Performed With the Surgical Navigation System a
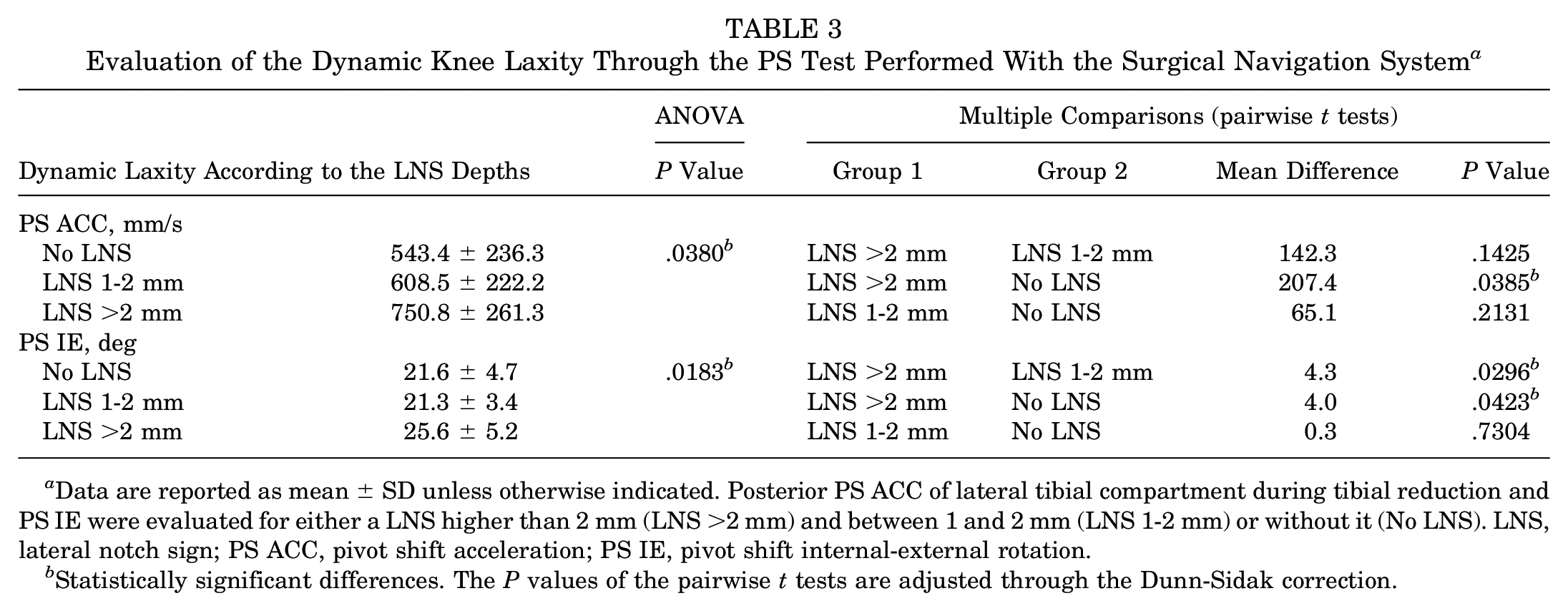
Data are reported as mean ± SD unless otherwise indicated. Posterior PS ACC of lateral tibial compartment during tibial reduction and PS IE were evaluated for either a LNS higher than 2 mm (LNS >2 mm) and between 1 and 2 mm (LNS 1-2 mm) or without it (No LNS). LNS, lateral notch sign; PS ACC, pivot shift acceleration; PS IE, pivot shift internal-external rotation.
Statistically significant differences. The P values of the pairwise t tests are adjusted through the Dunn-Sidak correction.
The ROC curve analysis showed that 2 mm was the most predictive cutoff value to identify the “high-grade rotatory instability” group, with an accuracy of 77.8% and 74.4% and a specificity of 95.5% and 93.9% referred to the PS ACC and PS IE, respectively (Table 4).
ROC Curve Analysis to Determine the Most Predictive LNS Cutoff Value a
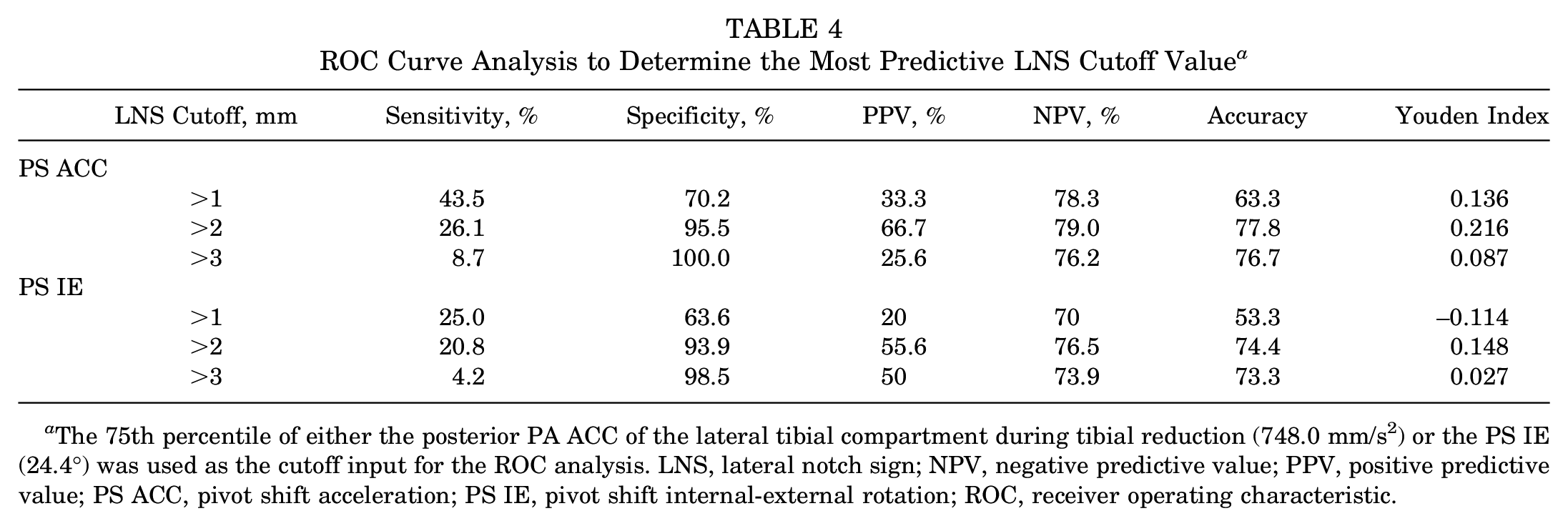
The 75th percentile of either the posterior PA ACC of the lateral tibial compartment during tibial reduction (748.0 mm/s2) or the PS IE (24.4°) was used as the cutoff input for the ROC analysis. LNS, lateral notch sign; NPV, negative predictive value; PPV, positive predictive value; PS ACC, pivot shift acceleration; PS IE, pivot shift internal-external rotation; ROC, receiver operating characteristic.
Finally, the evaluation of the LNS performed by the 2 operators resulted in an ICC of 0.90, thus showing an excellent agreement.
Discussion
The main finding of the present study was that a radiological sign, the deep LNS, was strongly correlated with increased rotatory laxity in patients with ACL injuries.
These findings are in contrast with those reported by Kanakamedala et al 11 who also investigated the effect of the LNS on PS with inconsistent results. There are several differences between the 2 studies that could explain the different conclusions. First, in the former study, the number of cases analyzed with MRI was 64 cases reporting 6 notches deeper than 2 mm, while in the latter, we included 90 cases of which 10 had a deep LNS. It is, therefore, possible that we were able to identify significant differences thanks to a larger cohort of patients and a higher number with deep notches. Also, the PS was quantified with different tools: Kanakamedala et al used the triaxial accelerometer and tablet-based image analysis software, while in this study, the biomechanical analysis was performed with the surgical navigation system. The latter tool is considered the gold standard for intraoperative biomechanical quantification because it can overcome the buffering effect of the skin. 14 Finally, they chose a different analysis setting, performing a direct correlation between the notch depth and the amount of laxity. As already observed, only the patients with a notch deeper than 2 mm had increased laxity; therefore, an analysis without this data stratification could not give the same results.
The ROC curve analysis showed that 2 mm was the most predictive cutoff value for identifying the patients with “high-grade rotatory instability.” In particular, this cutoff value showed a very high specificity, suggesting that the presence of deep LNS should raise suspicion for increased laxity. However, the low sensitivity highlights that this test could not be used as a “screening” during the workup of patients with ACL injuries, probably because other factors need to be taken into account and could be responsible for increased instability even though the LNS is absent.
The PS is a multifactorial phenomenon, and different bone morphological variations as well as soft tissue lesions, such as lateral meniscal tears,7,18,19 influence its magnitude. Many studies have focused on the effect of physiological osseous variations such as a steep lateral tibial plateau slope 31 and increased femoral condyle ratio. 30 However, little is known about how pathological bone lesions, such as the Segond fracture, which may entail a complex pattern of instability, affect the PS. While the Segond fracture has been widely studied with in vitro and in vivo studies because of the connection between this osseous fragment and the anterolateral ligament,5,24,28,32,34 the LNS has not been extensively investigated yet. The association between the LNS and increased rotatory instability is not easy to interpret and could be explained by different hypotheses. First, since it is known that ligaments fail by a progressive and sequential mechanism of collagen fibril failure, it is conceivable that there could be differences in the patterns of ACL injury, such as during injuries involving multiple ligaments, referred to as high- and low-energy. A low-grade injury could result in a somewhat isolated ACL tear, while a high-grade injury may involve ACL tear, a consequent bony impression on the lateral femoral condyle, and involvement of secondary rotatory stabilizers (see Figure 3).
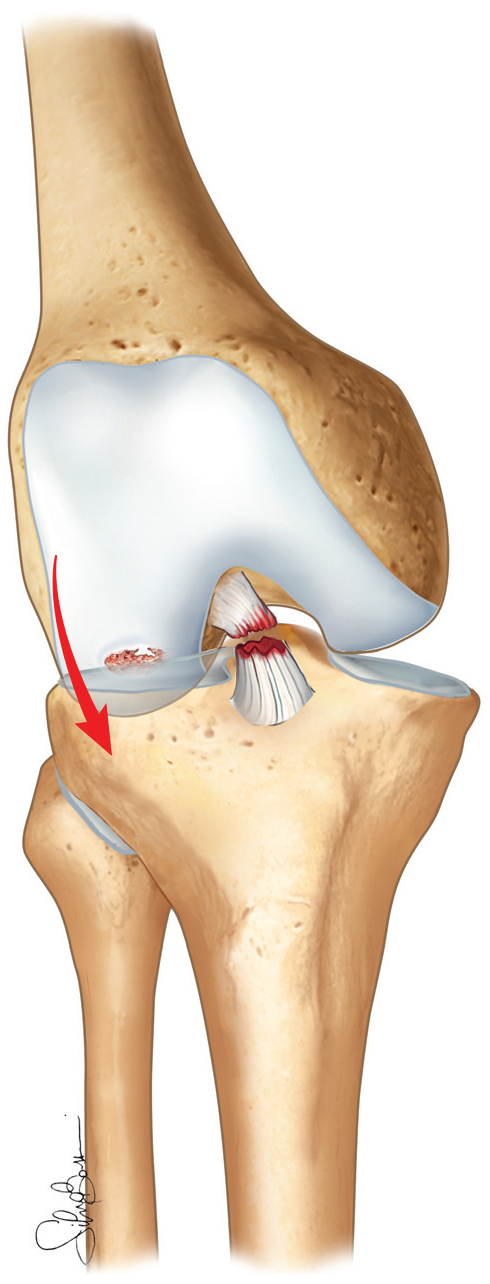
Anatomic drawing representing the impaction responsible for the LNS during an ACL injury. ACL, anterior cruciate ligament; LNS, lateral notch sign.
Moreover, the injury mechanism responsible for the LNS could be directly associated with tears of the anterolateral capsule: in fact, in the series by Losee et al, 20 stretching of the anterolateral capsule “comparable to the one seen in recurrent dislocation of the shoulder” was reported. Finally, it is also likely that the LNS could directly impair the knee kinematics with a mechanism of bone engagement, as already hypothesized by Galway and MacIntosh 4 ; the contour and depth of the notch may also play a contributory role. In fact, Losee et al described cases of PS performed under direct vision during open ACLR where the posterolateral tibial rim struck directly with the LNS. However, this mechanism has not yet been investigated or described with recent methodologies.
It is essential to underline that the results of our study could be easily translated into the clinical setting because the assessment of the LNS was performed using MRI scans that are mandatory when managing patients with an ACL injury. Moreover, like other authors have previously reported, these measurements present an almost perfect interobserver reliability.11,16
The possibility of identifying at least some of the patients who are at high risk of increased laxity would be useful to set patients’ expectations and possibly modify the surgical planning so as to reduce the risk of failure. In a recent consensus paper, the role of the LNS on anterolateral instability has been reconsidered, and it was included as a secondary criterion for the decision to perform an additional LET. 36 Moreover, in a large cohort of high-risk patients, Getgood et al 6 demonstrated that the addition of a LET to the intra-articular ACLR reduced the incidence of persistent rotatory instability from 40% to 25% and the incidence of graft failure from 11% to 4%. In a similar cohort of patients, Sonnery-Cottet et al 37 reported a reduction in risk of graft failure of 2.5 times with the LET procedure compared with B-PT-B grafts, and of 3.1 times with quadrupled hamstring graft. Moreover, the same authors published a series with 92 patients treated with combined ACLR and LET that showed excellent clinical results in terms of PS reduction and Tegner activity, reporting just 1 graft failure at 2 years of follow-up. 38 Interestingly, 21 patients included in that study were treated with LET because of LNS deeper than 2 mm.
This study presents several limitations. First, due to the incidence of 11% of a deep LNS, we identified only 10 cases on 90 MRI scans. Therefore, studies with a larger sample size are needed to confirm the results reported by our investigation. Moreover, we analyzed the depth of the LNS on sagittal MRI images: since it is conceivable that other parameters such as the position and the 3-dimensional morphology of the notch could play a role in the PS genesis, other investigations could help to determine if these factors could have an effect on the magnitude of PS. Finally, we proposed different theories about the genesis of increased rotatory laxity in this complex pattern of injury and we speculated about possible treatment strategies; however, it is not demonstrated that if the “bone engagement mechanism” is prevalent, even additional extra-articular procedures could restore nearly normal knee kinematics.
Conclusion
The LNS is a reliable radiological sign that can be used to identify patients with a high risk of increased rotatory instability. This finding could be useful in the clinical setting to set patients’ expectations and to better define the surgical planning.
Footnotes
Acknowledgements
The authors thank Silvia Bassini for the images and graphical support.
Submitted May 9, 2020; accepted September 23, 2020.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.