
Abstract
Background:
How to improve rotator cuff healing remains a challenge. Little is known about the effect of the parasympathetic transmitter acetylcholine (ACh) and the acetylcholinesterase inhibitor pyridostigmine (PYR), both of which have anti-inflammatory properties, in the healing process of rotator cuff injury.
Hypothesis:
ACh and PYR could enhance bone-tendon interface healing in a murine model of rotator cuff repair.
Study Design:
Controlled laboratory study.
Methods:
A total of 160 C57BL/6 mice underwent unilateral rotator cuff repair surgery. Fibrin gel (FG) was used as a drug carrier. The mice were randomly assigned to 4 groups with 40 mice per group: FG group (received FG alone), 10-5 M ACh group (received FG containing 10-5 M ACh), 10-6 M ACh group (received FG containing 10-6 M ACh), and PYR group (received FG containing 25 µg of PYR). Ten mice in each group were euthanized at 2, 4, 8, and 12 weeks postoperatively. Histologic, immunohistochemical, and biomechanical evaluations were performed for analysis.
Results:
Histologically, fibrocartilage-like tissue was shown at the repaired site. The proteoglycan content of the 10-5 M ACh group was significantly increased compared with the FG group at 4 weeks. M2 macrophages were identified at the repaired site for all groups at 2 and 4 weeks. At 8 weeks, M2 macrophages withdrew back to the tendon in the FG group, but a number of M2 macrophages were retained at the repaired sites in the ACh and PYR groups. Biomechanically, failure load and stiffness of the ACh and PYR groups were significantly higher than those of the FG group at 4 weeks. The stiffness of the ACh and PYR groups was significantly increased compared with the FG group at 8 weeks (P < .001 for all). At 12 weeks, most of the healing properties of the ACh and PYR groups were not significantly different compared with the FG group.
Conclusion:
ACh and PYR enhanced the early stage of bone-tendon insertion healing after rotator cuff repair.
Clinical Relevance:
These findings imply that ACh and PYR could serve as potential therapeutic strategies for rotator cuff healing.
The rotator cuff plays an important role in maintaining stability as well as facilitating movements of the shoulder. The bone-tendon interface (BTI) of the rotator cuff consists of bone, mineralized fibrocartilage, unmineralized fibrocartilage, and tendon. 4 This unique hierarchical structure is well-adapted to dissipate stress concentration and mediate load transmission between bone and tendon. 4 Once a rotator cuff is torn, shoulder pain and dysfunction will ensue. 45 Surgical repairs are often required to reattach the torn tendon to its bony insertion. However, one study reported that the retear rate was as high as 94% after rotator cuff repair. 15 In another study, fibrovascular tissue was found at the repaired site instead of at the newly regenerated fibrocartilaginous interface. 27 Promotion of BTI healing, especially regeneration of the fibrocartilage layer, is an unmet need in sports medicine. Bioactive factors, stem cells, and engineered scaffolds have been widely investigated to enhance BTI healing. Promising results have been demonstrated in many preclinical experimental studies.8,9,23,27,29,46 However, much work is needed before these applications can be used in clinical practice.
Recently, investigation has turned to the parasympathetic nervous system, which has not normally been a topic in musculoskeletal research. Of the classic parasympathetic neurotransmitters, acetylcholine (ACh) has been proven to play a crucial role in nonneural tissue regulation and inflammation control.1,36,41 Cartilage and tendon have been considered nonneural tissues. However, ACh and its receptors (AChRs) have been identified in tenocytes and chondrocytes.5,10,11,14,17,21 Moreover, ACh and AChRs have been identified in osteoblasts and osteoclasts.2,13,20,26,31 All of these studies have indicated that ACh plays a potential regulatory role in bone, tendon, and cartilage. Acetylcholinesterase (AChE) is the crucial enzyme to rapidly hydrolyze ACh, thus terminating the biological effects of ACh. The AChE inhibitor (AChEI) pyridostigmine (PYR) has been reported to attenuate the inflammatory response.6,41 Optimal inflammatory response has been reported to facilitate the healing process of rotator cuff.19,27 Moreover, M2 macrophages have shown an indispensable role in the regulation of inflammation and tissue repair. 7
Because rotator cuff healing occurs between the interface of bone and tendon, ACh and PYR may have an important effect on BTI healing. However, to date, the role of ACh and PYR in the healing process of the rotator cuff has not been studied. We hypothesized that ACh and PYR could promote rotator cuff healing. In this study, a mouse model of rotator cuff repair was used to evaluate the effect of ACh and PYR treatments via histology, immunohistochemistry, and biomechanical testing.
Methods
Study Design
A total of 160 C57BL/6 mice (12 weeks old) were enrolled for the supraspinatus tendon repair model. The use of animals and all procedures for this study were approved by our animal ethics committee (No. 201703222). Mice were randomly assigned to 1 of 4 groups with 40 mice per group: fibrin gel (FG) group (control), 10-5 M ACh group, 10-6 M ACh group, and PYR group. A total of 10 mice were sacrificed in each group at 2, 4, 8, and 12 weeks postoperatively. At each time point, 7 animals per group were used for biomechanical testing, and 3 animals were used for histologic and immunohistochemical evaluation (Figure 1).
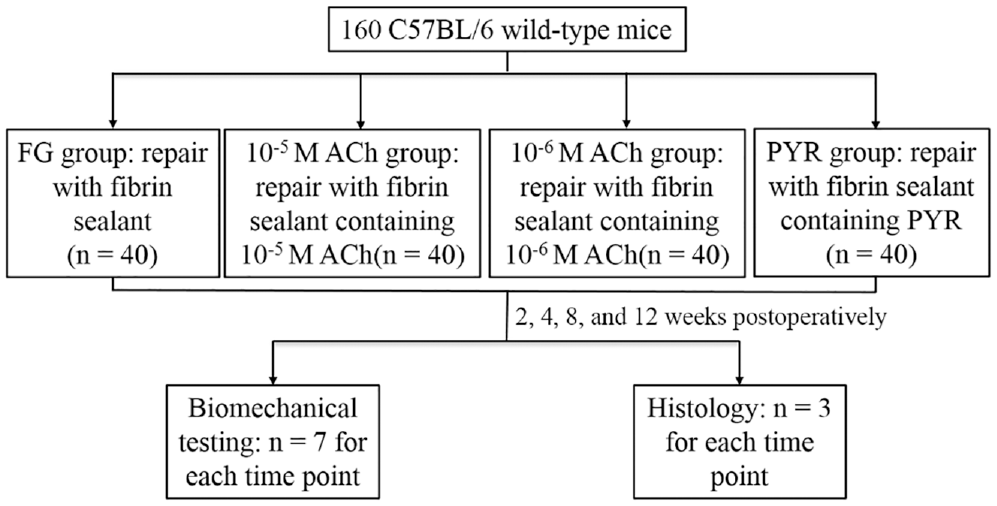
Flowchart depicting study design including experimental groups, number of animals in each group, time points for sacrifice, and outcome assessments. ACh, acetylcholine; FG, fibrin gel; PYR, pyridostigmine.
Preparation of Fibrin Sealant Carrier for Rotator Cuff Repair
Fibrinogen solution (Sigma-Aldrich) and thrombin solution (Sigma-Aldrich) were prepared per the manufacturer’s manual. ACh and PYR were then added to the thrombin solution. Both the fibrinogen and thrombin solutions were sterilized using a 0.22-µm syringe filter (Millex; Sigma). We used 10 µL of fibrinogen solution and 2 µL of thrombin solution to fabricate each fibrin sealant, or fibrin gel. Thus, 4 types of fibrin sealant were fabricated: fibrin sealant alone and fibrin sealant containing 10-5 M ACh, 10-6 M ACh, or 25 µg of PYR.
Surgical Procedure
All mice were anesthetized using an intraperitoneal injection of pentobarbital sodium, 0.3%, and were positioned in a right lateral decubitus position. The left shoulder was shaved and prepared for surgery. All procedures were performed under sterile technique using a surgical microscope. An incision was made on the lateral side of the left shoulder. The deltoid muscle was identified and minimally dissected to expose the supraspinatus tendon.3,24 A customized retractor was put under the acromion to improve visualization. After the supraspinatus tendon was fixed using No. 6-0 PDS suture (Ethicon) in a figure-of-8 pattern, the supraspinatus tendon was sharply dissected at the bony insertion site. Any remaining fibrocartilage at the insertion site was carefully removed. A bone tunnel was created transversely within the humeral head, avoiding damage to the infraspinatus and subscapularis tendon. The PDS suture was then passed through the bone tunnel.
At this point, the animals were assigned to 4 groups: FG group (FG alone), 10-5 M ACh group (fibrin sealant containing 10-5 M ACh), 10-6 M ACh group (fibrin sealant containing 10-6 M ACh), and PYR group (fibrin sealant containing 25 µg of PYR). After the fibrin sealant was placed between the supraspinatus tendon and bone, 2 square knots were made to bring the supraspinatus tendon back to its bony insertion site. 3 The skin was closed using No. 4-0 Ethibond suture (Ethicon). All mice were allowed free cage activity after surgery.
Histologic and Immunohistochemical Evaluation
At 2, 4, 8, and 12 weeks postoperatively, mice were euthanized. A total of 3 specimens at each timepoint from each group were allocated for histologic and immunohistochemical analysis. The supraspinatus tendon-humerus complex was carefully harvested under the surgical microscope. Once dissected, the specimens were immediately fixed using neutral paraformaldehyde, 10%, for 24 hours and decalcified in neutral ethylenediaminetetraacetate, 10%; dehydrated using a serial of graded ethanol; and embedded in paraffin. The paraffin blocks were serially sectioned with 5-µm thickness in the coronal plane.
The dewaxed tissue sections were stained with standard hematoxylin and eosin (H&E) and toluidine blue O/fast green per the manufacturer’s instructions. For immunohistochemistry staining, dewaxed tissue sections were preincubated using H2O2, 3%, to block endogenous peroxidase. The primary antibody against M2 macrophage (CD206, ab64693; Abcam) was incubated overnight at 4°C. Then, the tissue sections were incubated using an anti-rabbit secondary antibody conjugated with horseradish peroxidase (ab7090; Abcam) for 30 minutes at room temperature. Thereafter, a DAB (3,3′diaminobenzidine) substrate kit (ab64238; Abcam) was used, followed by counterstaining of nuclei with hematoxylin. All digital images were taken using an Olympus CX31 microscope under the same condition. H&E staining was used for the histologic description of the repaired tendon-bone insertion. Semiquantification analyses of the regenerated fibrocartilage were performed based on the toluidine blue O/fast green staining. 28
Biomechanical Testing
At each timepoint, 7 mice from each group were biomechanically tested. The supraspinatus muscle-tendon-humerus complex was carefully isolated from surrounding tissue under a surgical microscope. After the supraspinatus muscle was scraped from the tendon, the suture material used to fix the tendon was removed. The humerus was mounted, and the supraspinatus tendon was placed in a custom grip using sandpaper and ethyl cyanoacrylate. The specimens were transferred to a materials testing system and loaded to failure at a rate of 1 mm/min. 24 Failure load was obtained from the recorded load-to-failure data, and the stiffness was calculated from the linear portion of the load-deformation curve. All samples were kept moist using saline, 0.9%, during testing.
Statistical Analysis
All quantitative data are shown as mean ± SD with 95% CI. A 2-way analysis of variance with Tukey post hoc test was used to analyze the differences among the 4 groups using GraphPad Prism software (Version 8.0.1). The significance level was set at P < .05.
Results
We noted no side effects of ACh and PYR in the 3 treatment groups after surgery, and none of the mice had postsurgical complications. No gross failures or gap formations were observed at the supraspinatus tendon–humeral head repair site in any of the specimens.
Histologic Analysis
The H&E and toluidine blue O/fast green staining showed no gap formations at the repaired supraspinatus tendon–humeral head site at 2, 4, 8, and 12 weeks postoperatively for all groups (Figures 2 and 3).
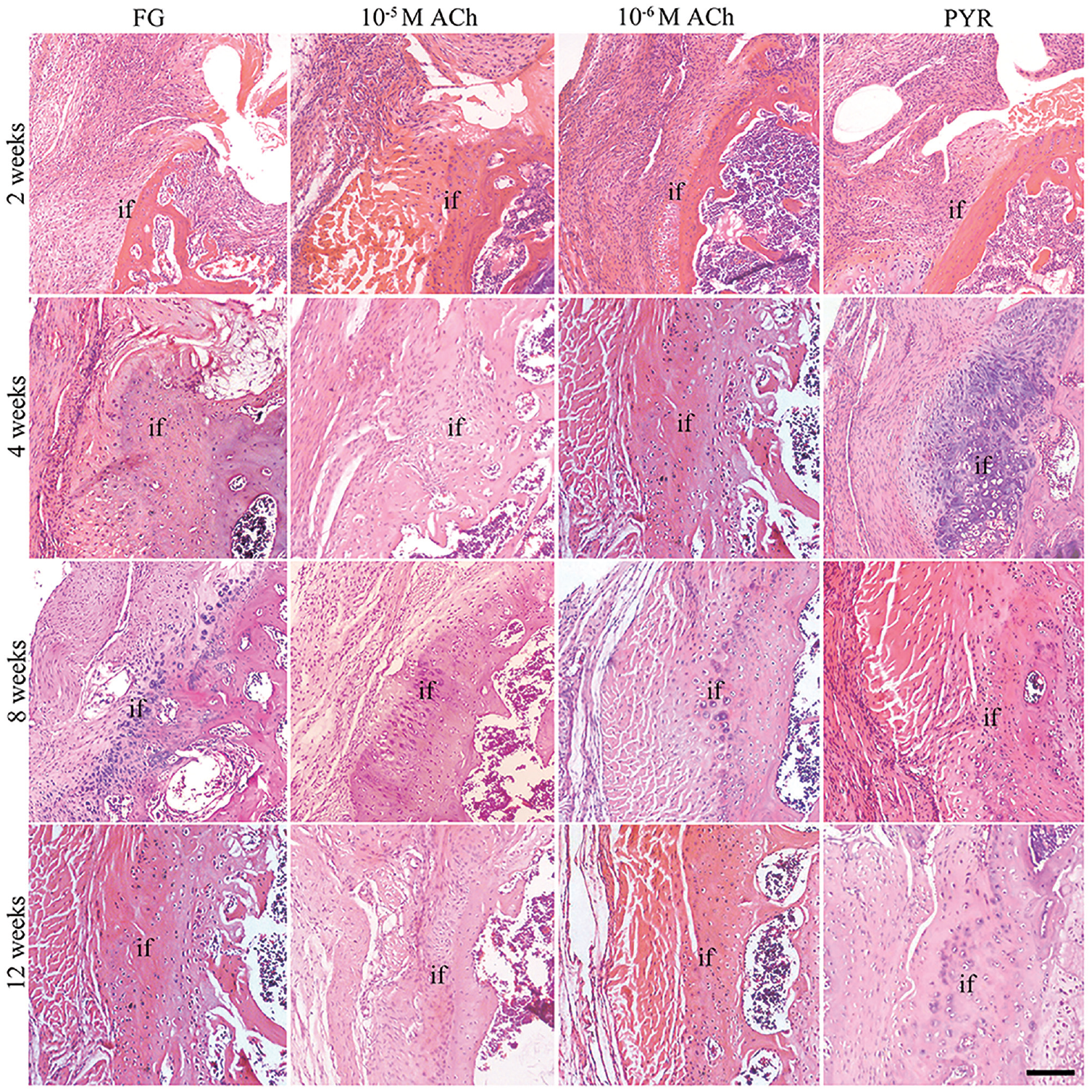
Representative hematoxylin and eosin staining of coronal sections of the supraspinatus tendon–humeral head insertion at postoperative 2, 4, 8, and 12 weeks in the 4 groups. ACh, acetylcholine; FG, fibrin gel; if, interface; PYR, pyridostigmine. Scale bar = 100 µm.
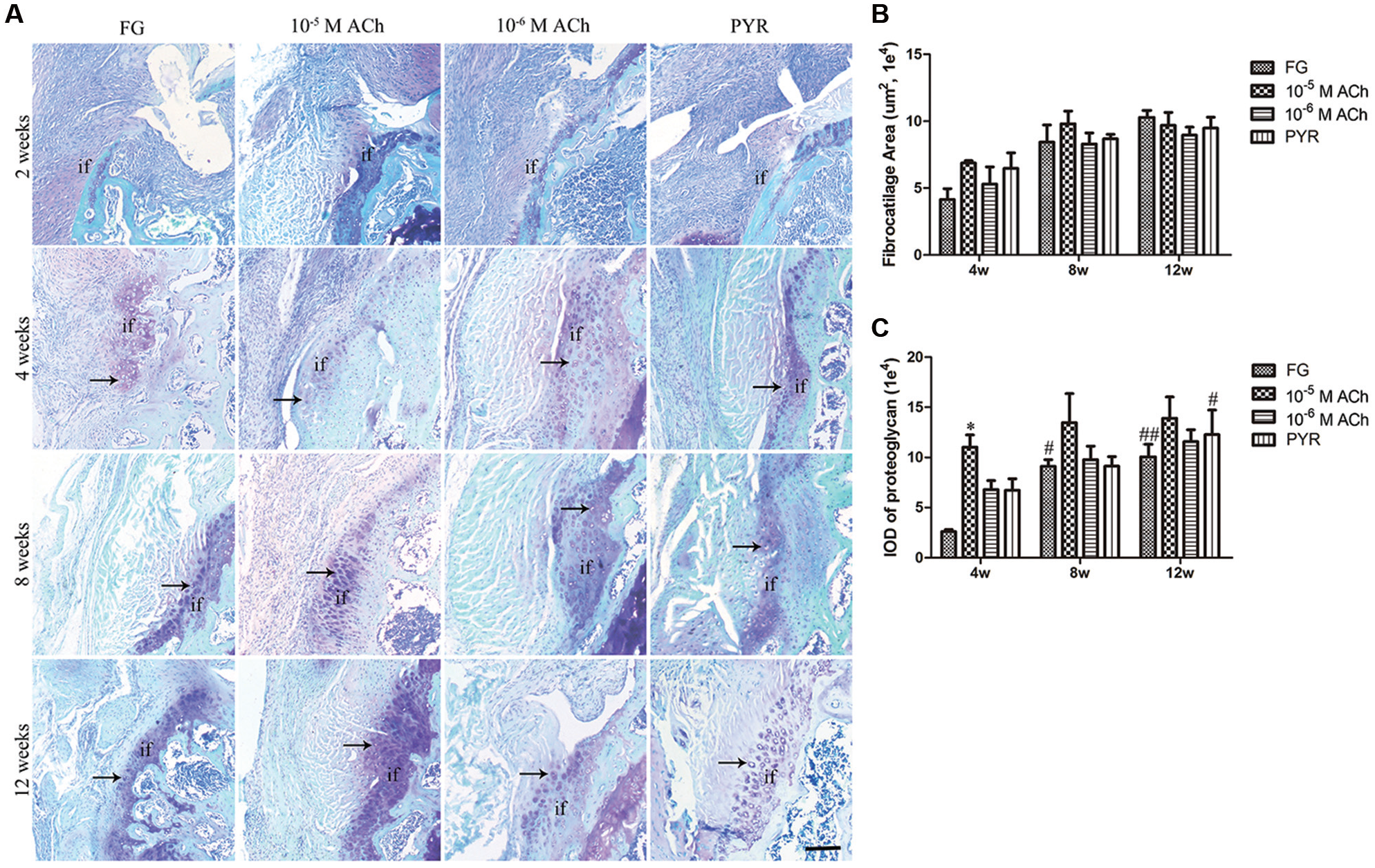
(A) Representative toluidine blue O/fast green staining of coronal sections of the supraspinatus tendon–humeral head insertion at postoperative 2, 4, 8, and 12 weeks for the 4 groups. Comparison of (B) the area of regenerated fibrocartilage-like tissue and (C) integrated optical density (IOD) of the proteoglycan among the 4 groups at different time points. Data are shown as mean ± SD. *P < .05 compared with the FG group at 4 weeks. #P < .05 and ##P < .01 compared with the same group at 4 weeks. Black arrows denote the fibrochondrocyte-like cells at the repaired insertion. ACh, acetylcholine; FG, fibrin gel; if, interface; PYR, pyridostigmine. Scale bar = 100 µm.
At 2 weeks, fibrovascular tissue was shown at the repaired site in all groups (Figure 2). At 4 weeks, regenerated fibrocartilage-like tissue connected the supraspinatus tendon and humeral head. The hypertrophic chondrocyte-like cells were embedded in the characteristic matrix enriched with proteoglycans (Figure 3A). However, these chondrocyte-like cells were not well organized in any specific pattern. Although remodeling of the regenerated fibrocartilage-like tissue had occurred at 8 and 12 weeks, the organized insertion zone with unmineralized and mineralized fibrocartilage was not achieved compared with the native enthesis (Appendix Figure A1, available in the online version of this article). Quantitively, although the area of the regenerated fibrocartilage zone increased along with the healing time for all 4 groups, no significant differences were seen among the groups (Figure 3B). At 4 weeks, the integrated optical density (IOD) of proteoglycan at the repaired BTI in the 10-5 M ACh group was significantly higher than that in the FG group (P = .045) (Figure 3C). The IOD of proteoglycan in the FG group at 8 and 12 weeks was significantly higher compared with that at 4 weeks (P = .019 and P = .008, respectively) (Figure 3C). The IOD of proteoglycan in the PYR group at 12 weeks was significantly increased compared with that at 4 weeks (P = .046) (Figure 3C).
Immunohistochemical Evaluation
The spatial and temporal changes of the M2 macrophages at different time points postoperatively for all groups are shown in Figure 4. At 2 weeks and 4 weeks postoperatively, M2 macrophages were observed at the repaired insertion for all groups. Compared with 2 weeks, the percentage of the M2 macrophage–positive area was decreased at 4 weeks for the FG group. At 8 weeks, the M2 macrophages had withdrawn back to the tendon in the FG group, while many M2 macrophages remained at the repaired site for the ACh and PYR groups. At 12 weeks, few M2 macrophages were seen at the repaired site for all groups.
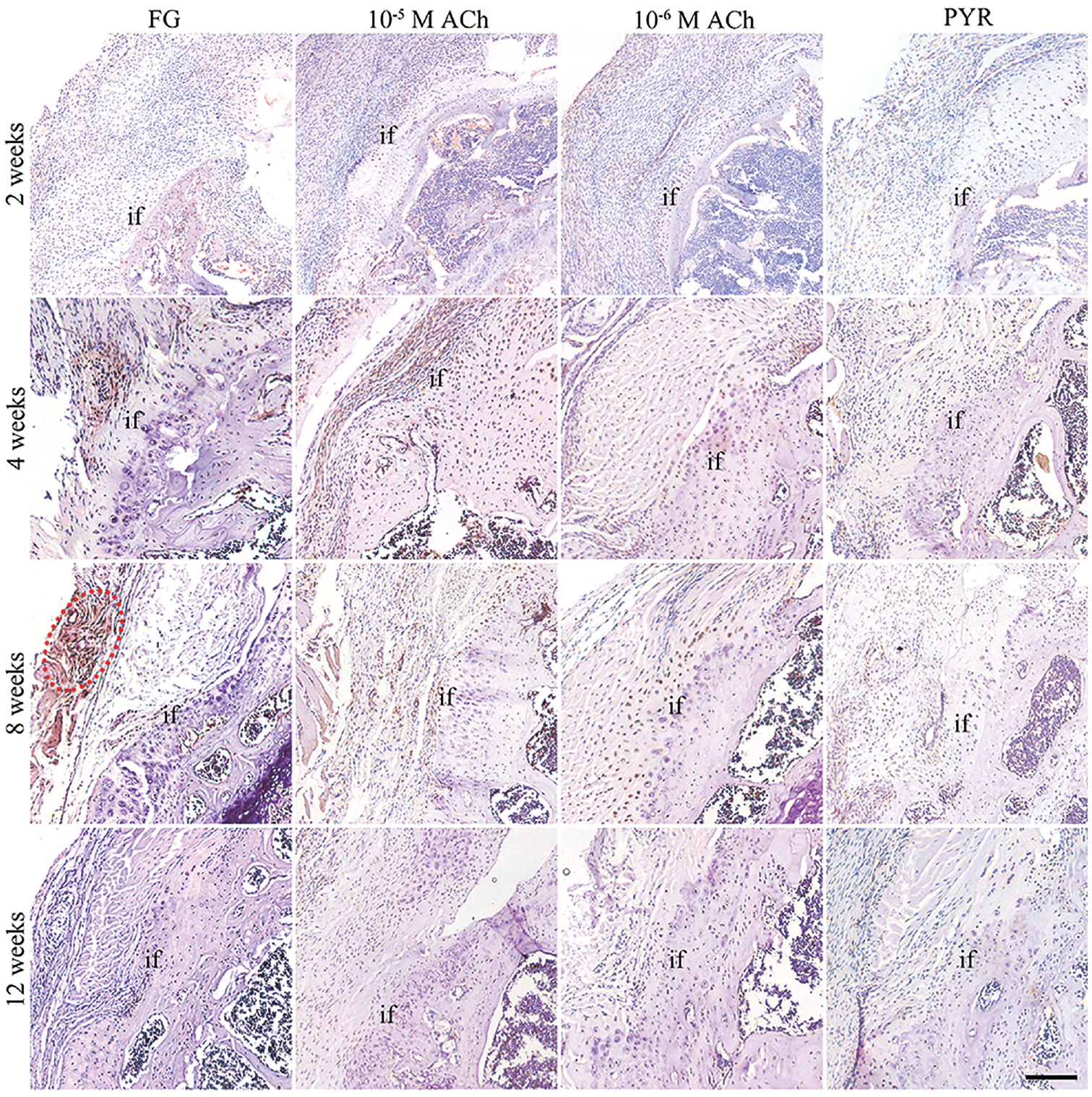
Representative immunohistochemistry of the coronal sections of the supraspinatus tendon–humeral head insertion at postoperative 2, 4, 8, and 12 weeks for the 4 groups. Red circle denotes that the M2 macrophage withdrew back to the tendon. ACh, acetylcholine; FG, fibrin gel; if, interface; PYR, pyridostigmine. Scale bar = 100 µm.
Biomechanical Testing
At 2 weeks, the mean failure load was 1.79 ± 0.60 N (95% CI, 1.23-2.35 N) in the FG group, 2.07 ± 0.74 N (95% CI, 1.38-2.75 N) in the 10-5 M ACh group, 1.70 ± 0.64 N (95% CI, 1.11-2.29 N) in the 10-6 M ACh group, and 1.79 ± 0.54 N (95% CI, 1.30-2.29 N) in the PYR group. No significant differences were seen among the 4 groups at 2 weeks (P > .05 for all). At 4 weeks, the mean failure loads for the 10-5 M ACh group (3.90 ± 0.76 N; 95% CI, 3.20-4.61 N), the 10-6 M ACh group (3.84 ± 0.75 N; 95% CI, 3.14-4.53 N), and the PYR group (4.08 ± 0.90 N; 95% CI, 3.25-4.92 N) were significantly higher than that of the FG group (2.46 ± 0.74 N; 95% CI, 1.77-3.15 N) (P = .017, P = .021, and P = .015, respectively) (Figure 5). At 8 and 12 weeks, no significant differences were observed among the 4 groups. In the FG group and the 10-6 M ACh group, the failure load at 8 and 12 weeks was significantly higher compared with 4 weeks (P < .001 for all). In the 10-5 M ACh group, the failure load at 12 weeks was significantly higher than that at 4 weeks (P = .009). No significant differences were noted among the different time points for the PYR group. All the specimens failed at the bone-tendon reattachment site.
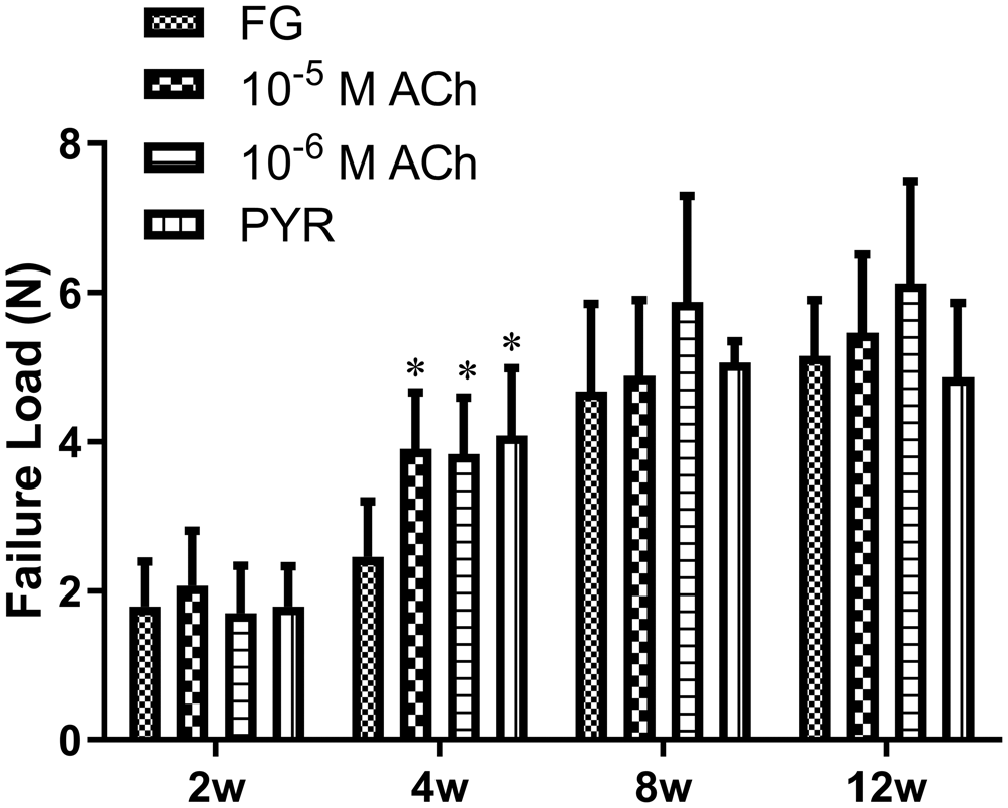
Comparison of the failure load for the 4 groups at different time points. Data are shown as mean ± SD. *P < .05 compared with the FG group at 4 weeks. ACh, acetylcholine; FG, fibrin gel; PYR, pyridostigmine.
The changing trend of stiffness in the 4 groups was quite similar to the trend for failure load (Figure 6). At 2 weeks, the stiffness was 1.85 ± 0.35 N/mm (95% CI, 1.53-2.18 N/mm) in the FG group, 1.92 ± 0.23 N/mm (95% CI, 1.71-2.14 N/mm) in the 10-5 M ACh group, 1.67 ± 0.49 N/mm (95% CI, 1.22-2.12 N/mm) in the 10-6 M ACh group, and 1.89 ± 0.67 N/mm (95% CI, 1.27-2.50 N/mm) in the PYR group. No significant differences were seen among the 4 groups at 2 weeks (P > .05 for all). At 4 weeks, the stiffness was 4.46 ± 0.87 N/mm (95% CI, 3.66-5.26 N/mm) in the 10-5 M ACh group, 4.12 ± 1.14 N/mm (95% CI, 3.07-5.17 N/mm) in the 10-6 M ACh group, and 4.75 ± 1.84 N/mm (95% CI, 3.05-6.45 N/mm) in the PYR group, all of which were significantly higher than that of the FG group (2.33 ± 1.14 N/mm; 95% CI, 1.28-3.38 N/mm) (P = .003, P = .017, and P < .001, respectively). At 8 weeks, the stiffness was 6.56 ± 0.77 N/mm (95% CI, 5.85-7.27 N/mm) in the 10-5 M ACh group, 6.02 ± 1.29 N/mm (95% CI, 4.83-7.21 N/mm) in the 10-6 M ACh group, and 6.74 ± 1.12 N/mm (95% CI, 5.70-7.77 N/mm) in the PYR group, all of which were significantly higher than that of the FG group (3.63 ± 1.27 N/mm; 95% CI, 2.46-4.81 N/mm) (P < .001 for all). At 12 weeks, no significant differences were observed among the 4 groups. For the FG group, the stiffness at 12 weeks was significantly higher compared with that at 4 and 8 weeks (P < .05 for all). Both the 10-5 M ACh group and the 10-6 M ACh group had significantly higher stiffness at 8 weeks compared with 4 weeks (P < .05 for all). The stiffness of the 10-6 M ACh group was significantly higher at 8 and 12 weeks than at 4 weeks (P < .05 for all).
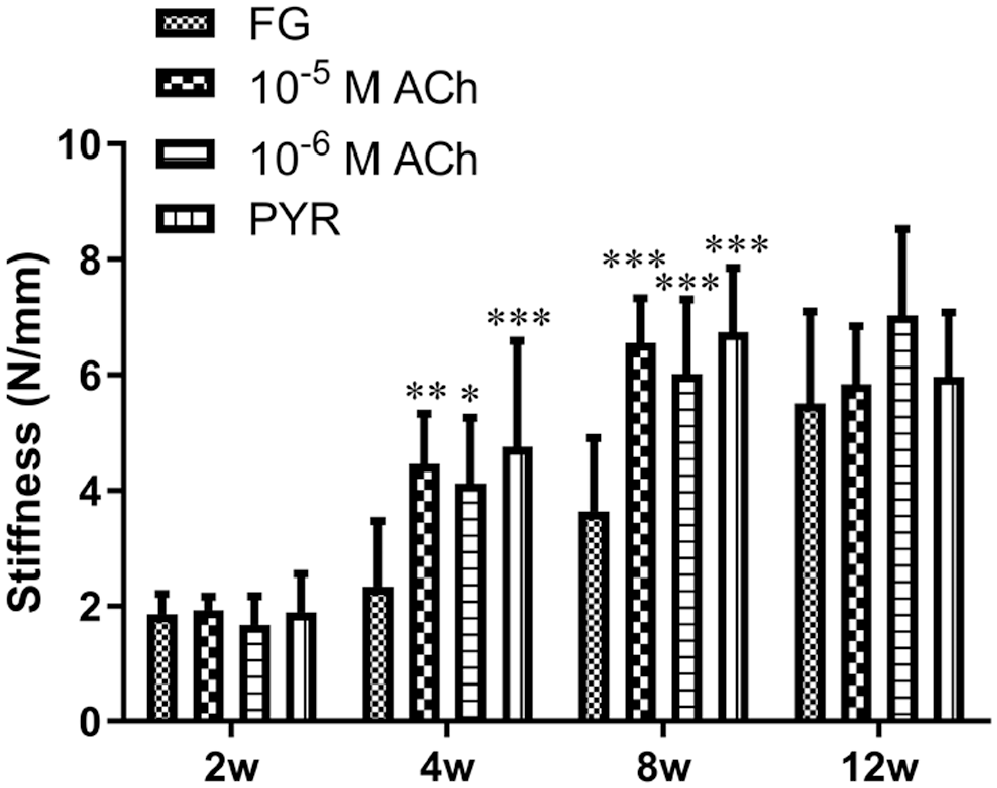
Comparison of stiffness for the 4 groups at different time points. Data are shown as mean ± SD. *P < .05, **P < .01, and ***P < .001 compared with the FG group at 4 weeks. ACh, acetylcholine; FG, fibrin gel; if, interface; PYR, pyridostigmine.
The specific data for failure load and stiffness are summarized in Appendix Table A1 (available online).
Discussion
In the current study, we investigated the effects of ACh and PYR on BTI healing in a murine model of rotator cuff repair. The principal findings showed that ACh and PYR could improve the biomechanical properties of the repaired rotator cuff at 4 and 8 weeks postoperatively; however, the effects of ACh and PYR faded at 12 weeks, which indicated that ACh and PYR could enhance only the early stage of rotator cuff healing.
For decades, orthopaedic surgeons and researchers have been dedicated to improving rotator cuff healing. Surgical techniques and tissue engineering have been well developed; however, the clinical outcomes remain unsatisfactory. One crucial reason is that the native, well-organized fibrocartilage zone is absent at the repaired BTI. Approaches including stem cells, bioactive factors, scaffolds, and other biophysical therapies have been used to promote the regeneration of fibrocartilage.8,23,40,44,46 However, the parasympathetic nervous system and its major neurotransmitter ACh have not been studied in this field.
It is well acknowledged that ACh is synthesized, stored, and released by the cholinergic neurons. 42 However, many studies have reported that ACh, as well as its receptors, have been identified in nonneural tissues and cells. Romano et al 35 found that the nicotinic receptor α7 (α7nAChR) gene was present in the tendon during early development. Later, Danielson et al 11 showed that tenocyte expressed the choline acetyltransferase and M2 AChR. Moreover, it has been reported that ACh could promote the proliferation of tenocytes. 14 Chondrocytes and bone have also been shown to express AChRs.17,21 All of these studies have indicated that ACh and AChRs play an important regulatory role in maintaining the homeostasis of tendon, cartilage, and bone. According to research investigating the biological effects of different concentrations of ACh in vitro, the effective concentration was 10-5 M ACh and 10-6 M ACh.6,12,14,30,41 Therefore, we examined these 2 concentrations in our study. The results showed that the IOD of proteoglycan was significantly increased only in the 10-5 M ACh group compared with the FG group at 4 weeks (Figure 3C). Teng et al 37 reported that nicotine could prevent cartilage degradation and aggrecan loss in osteoarthritis through the activation of α7nAChR. ACh might activate α7nAChR, resulting in the increase of proteoglycan. With respect to failure load and ultimate stress, all 3 treatment groups (ie, the 10-5 M ACh, 10-6 M ACh, and PYR groups) had significantly higher results compared with the FG group at 4 weeks (Figure 5). Furthermore, the 3 treatment groups had significantly improved stiffness compared with the FG group at both 4 and 8 weeks (Figure 6). These findings indicate that 10-5 M ACh, 10-6 M ACh, and PYR could promote rotator cuff healing, whereas 10-5 M ACh had superior performance on the synthesis of proteoglycan.
In this study, we found that ACh and PYR showed different effects on the healing process of rotator cuff. ACh and PYR significantly improved the mechanical properties of tendons at 4 weeks, but this effect had decreased at 8 weeks and faded at 12 weeks. One possible reason was that we delivered ACh and PYR only once during the surgery. At 4 weeks after surgery, FG was not found at the repair site, which indicated that ACh and PYR in the FG had been totally released. At 8 weeks and 12 weeks after surgery, the ACh concentration might be very low at the repair site, which would affect the healing process. Whether higher doses or multiple doses would have maintained the effects at 8 weeks and 12 weeks needs further study. The second possible reason for different effects of ACh and PYR might be that ACh expedites the early process of healing but does not change long-term outcomes. However, one study reported that nicotine had a deleterious effect on bone-tendon healing at early stages (10 and 28 days), 16 which seems contradictory to our results. In the study by Galatz et al, 16 the maximum force of the nicotine group was significantly higher compared with the control group at 56 days after surgery. Meanwhile, the stiffness and maximum stress of the nicotine group were similar to those of the control group. 16 The authors explained this difference by increases in collagen crosslinking caused by advanced glycation end products. However, the nicotine level they used has been shown to delay bone fracture healing. This dose could be too high for rotator cuff healing. The different dose and the activation of muscarinic AChRs and nicotinic AChRs caused by ACh might explain the contradictory results.
The underlying mechanism whereby ACh and PYR enhanced rotator cuff healing remains unclear. One presumable explanation is the “cholinergic anti-inflammation pathway.”6,41 Macrophages are key regulators of inflammation, tissue repair, and regeneration.7,43 Generally, macrophages can be classified into 2 subpopulations according to their polarization status: classically activated M1 macrophages and alternatively activated M2 macrophages. M1 macrophages are mainly involved in the acute inflammation phase of tissue healing. M2 macrophages are associated with anti-inflammation, tissue remodeling, and healing. 7 Borovikova et al 6 reported that ACh reduced the release of proinflammatory cytokines tumor necrosis factor and interleukin 6 but not the anti-inflammatory cytokine interleukin 10 in lipopolysaccharide-stimulated M1 macrophage. 6 Administration of AChEI could also suppress the inflammation that is attributable to the accumulation of ACh.18,33,34 Wang et al 41 proved that α7nAChR was essential for this anti-inflammatory response. Moreover, activation of α7nAChR protected the M2 macrophages from apoptosis. 25 In the current study, we found that M2 macrophages appeared at the repaired insertion site at 4 weeks in all 4 groups (Figure 4). At 8 weeks postoperatively, M2 macrophages withdrew back to the tendon in the FG group. In contrast, M2 macrophages were still identified at the repaired site in the ACh and PYR groups at 8 weeks. A possible explanation is that a low concentration of ACh might remain at the repair site after ACh and PYR treatment. The retention of M2 macrophages at the repaired insertion site might have enhanced tissue modeling and repair, resulting in the significantly improved biomechanical properties in the ACh and PYR groups compared with the FG group at the early healing stages. At 12 weeks, M2 macrophages were not found at the repaired insertion site. At the same time, no differences were found among the 4 groups with respect to failure load, ultimate stress, and stiffness. This might be ascribed to the fact that ACh and PYR in the FG had already been released and the environment at the repaired insertion site had returned the same state among the 4 groups.
There are some limitations to this current study. First, we investigated only 2 ACh doses, and the sample size was low. Although many in vitro studies have shown that 10-5 M and 10-6 M ACh have biological effects, the in vivo environment is much more complicated. Optimized doses or delivery systems need to be further studied. Second, we observed the effect of ACh and PYR on M2 macrophages at the repair site, and specific mechanisms, such as the role of ACh receptors in the healing process, were not determined. Other underlying mechanisms as well as the role of ACh in healthy tendon still need to be explored. Third, we did not include a control group that did not receive FG. The use of FG has not been found to affect the tendon repair strength in vitro 39 or improve rotator cuff healing in vivo. 38 Many published papers have used FG as a control condition.22,32,40 Moreover, further study is needed regarding how the addition of FG at the repair site in a research investigation translates to a clinical application. Fourth, the histologic evaluation showed that the native enthesis with 4 zones was not regenerated, although ACh and PYR significantly improved the biomechanical properties. This implies that regeneration of the native enthesis might require more than application of ACh or PYR only at the time of surgery.
Conclusion
This study is the first to investigate the effects of ACh and PYR on the healing process of the rotator cuff in a mouse model. ACh and PYR could enhance the early stage of bone-tendon insertion healing after rotator cuff repair.
Supplemental Material
sj-pdf-1-ajs-10.1177_0363546520988680 – Supplemental material for The Enhancement Effect of Acetylcholine and Pyridostigmine on Bone-Tendon Interface Healing in a Murine Rotator Cuff Model
Supplemental material, sj-pdf-1-ajs-10.1177_0363546520988680 for The Enhancement Effect of Acetylcholine and Pyridostigmine on Bone-Tendon Interface Healing in a Murine Rotator Cuff Model by Zhanwen Wang, Yang Chen, Han Xiao, Shengcan Li, Tao Zhang, Jianzhong Hu, Hongbin Lu and Hui Xie in The American Journal of Sports Medicine
Footnotes
Submitted September 30, 2019; accepted October 14, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by the National Natural Science Foundation of China (No. 81730068), the Youth Project of Natural Science Foundation of Hunan Province, China (No. 2018JJ3814), and the Fundamental Research Funds for the Central Universities of Central South University (2017zzts214). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.