
Abstract
Background:
Superior capsule reconstruction (SCR) has been shown to improve shoulder function and reduce pain in patients with isolated irreparable supraspinatus tendon tears. However, the effects of SCR on biomechanics in a shoulder with an extensive posterosuperior rotator cuff tear pattern remain unknown.
Purpose/Hypothesis:
The purpose was to (1) establish a dynamic robotic shoulder model, (2) assess the influence of rotator cuff tear patterns, and (3) assess the effects of SCR on superior humeral head translation after a posterosuperior rotator cuff tear. It was hypothesized that a posterosuperior rotator cuff tear would increase superior humeral head translation when compared with the intact and supraspinatus tendon–deficient state and that SCR would reduce superior humeral head translation in shoulders with massive rotator cuff tears involving the supraspinatus and infraspinatus tendons.
Study Design:
Controlled laboratory study.
Methods:
Twelve fresh-frozen cadaveric shoulders were tested using a robotic arm. Kinematic testing was performed in 4 conditions: (1) intact, (2) simulated irreparable supraspinatus tendon tear, (3) simulated irreparable supra- and infraspinatus tendon tear, and (4) SCR using a 3 mm–thick dermal allograft (DA). Kinematic testing consisted of static 40-N superior force tests at 0°, 30°, 60°, and 90° of abduction and dynamic flexion, abduction, and scaption motions. In each test, the superior translation of the humeral head was reported.
Results:
In static testing, SCR significantly reduced humeral superior translation compared with rotator cuff tear at all abduction angles. SCR restored the superior stability back to native at 60° and 90° of abduction, but the humeral head remained significantly and superiorly translated at neutral position and at 30° of abduction. The results of dynamic testing showed a significantly increased superior translation in the injured state at lower elevation angles, which diminished at higher elevation, becoming nonsignificant at elevation >75°. SCR reduced the magnitude of superior translation across all elevation angles, but translation remained significantly different from the intact state up to 60° of elevation.
Conclusion:
Massive posterosuperior rotator cuff tears increased superior glenohumeral translation when compared with the intact and supraspinatus tendon–insufficient rotator cuff states. SCR using a 3-mm DA partially restored the superior stability of the glenohumeral joint even in the presence of a simulated massive posterosuperior rotator cuff tear in a static and dynamic robotic shoulder model.
Clinical Relevance:
The biomechanical performance concerning glenohumeral stability after SCR in shoulders with large posterosuperior rotator cuff tears is unclear and may affect clinical outcomes in daily practice.
Keywords
Massive, irreparable rotator cuff tears are challenging to treat, especially in a young and athletic patient population. 11 Various treatment options ranging in invasiveness include debridement, partial versus complete repair, tendon transfers, and joint replacement.3,5,10,16,34,38,39 Mihata et al 21 presented the reconstruction of the superior capsule (SCR) by using an autologous fascia lata graft for isolated irreparable supraspinatus tendon tears as an alternative procedure. Improved clinical outcomes, marked by high rate of return to work and sports, have been recorded in short- and midterm trials.18-21
Furthermore, several biomechanical studies have shown that SCR prevents superior migration of the humeral head in the presence of isolated supraspinatus tears.8,17,22,25,26 By maintaining the humeral head in its native position, SCR allows the remaining rotator cuff muscle groups and the deltoid muscle to compensate for the lack of the supraspinatus during early abduction and forward elevation, improving overall joint function. 3 SCR has also been shown to prevent bony impingement between the greater tuberosity and acromion. 24
SCR has been modified to use acellular human dermal allografts (DA) to decrease donor-site morbidity and expedite the procedure. 30 Preliminary results have shown significant improvements in clinical outcome scores and in the incorporation of cells at short-term follow-up.1,2,4,11,12 However, there is inconsistency in the clinical outcomes of Mihata et al,18-21 which may be due to varying biomechanical properties among different graft choices. Further, the widening indication for SCR to treat posterosuperior rotator cuff tears with irreparable supra- and infraspinatus tendons has not been biomechanically validated.
To date, all biomechanical studies on SCR have been limited to static evaluation of joint forces on specific angles of abduction/forward elevation.8,17,22,25,26 Therefore, the purpose of this study was to (1) establish and report a dynamic robotic shoulder model for forward elevation, abduction, and scaption movements; (2) compare the changes in superior humeral head translation between the intact joint, supraspinatus-deficient shoulder, and the subsequent supra- and infraspinatus-deficient shoulder; and (3) evaluate the effect of SCR using a DA on humeral head translation for the posterosuperior rotator cuff–deficient shoulder (supra- and infraspinatus tendons cut). The 3 hypotheses (H) of this study are as follows: (H1) an isolated supraspinatus tendon tear would lead to superior migration of the humeral head; (H2) a posterosuperior rotator cuff tear would further increase superior migration of the humeral head; and (H3) SCR would restore the native humeral head positioning, even after a massive rotator cuff tear involving both the supra- and infraspinatus tendons.
Methods
Specimen Preparation
Twelve male fresh-frozen cadaveric shoulders (mean age, 56.3 years; range, 51-62 years) were tested in this study. All specimens were donated to a tissue bank for the purpose of medical research and then purchased by our institution. Specimens were excluded if any history of injury, surgery, osteoporosis, osteoarthritis, or degenerative joint disease was detected. Before dissection, an arthroscopic evaluation was performed by an experienced sports medicine fellow (L.L.) to exclude any specimens with evidence of capsule, rotator cuff, or major labral pathology. Skin, subcutaneous tissue, and muscle tissue were dissected to the level of the rotator cuff, carefully leaving all tendons and underlying capsular structures intact. The inferior aspect of the scapula was potted in polymethyl methacrylate (PMMA; Fricke Dental) just inferior to the glenoid, allowing for unrestricted movement of the humerus. The shaft of the humerus was also potted in PMMA in a half-cylindrical mold, with the long axis of the humerus central and parallel to the long axis of the half-cylinder mold. The rotator cuff muscles (supraspinatus, infraspinatus, teres minor, and subscapularis) and the deltoid muscle were all reflected, leaving their tendinous insertions on the humerus intact.
Biomechanical Testing
Before potting the specimens, a joint coordinate frame was established using a coordinate measuring machine (Romer Absolute Arm; Hexagon Manufacturing Intelligence) in accordance with the methodology established by SimVITRO labVIEW software (Cleveland Clinic). 40 To estimate the joint center, the humerus was rigidly clamped and the scapula was left free to rotate. A small hole was drilled with a K-wire into the trigonum scapulae to create a repeatably measurable point on the scapula. This point was digitized 20 times in different shoulder positions, covering the entire range of motion of the joint, and a best-fit sphere was fitted to these points to establish the joint center, which was used as the origin of the joint coordinate frame. The lateral axis was defined along the line connecting the joint center with the trigonum scapulae. The anterior axis was defined as mutually perpendicular to the lateral axis and the axis passing through the joint center and a point collected on the inferior angle of the scapula. The superior axis was defined as mutually perpendicular to the anterior and lateral axes.
After completion of specimen preparation, the humerus was secured to a custom-designed fixture on the end effector of the 6 degrees of freedom robotic arm (KR 60-3; KUKA Robotics), equipped with a 6-axis universal force/torque sensor (ATI Industrial Automation). The scapula was rigidly fixed to another custom-designed fixture on a steel pedestal. No. 2 suture (No. 2 FiberWire; Arthrex) was used to stitch each tendon (supraspinatus, infraspinatus, teres minor, subscapularis, and deltoid) with a Krackow stitch from medial to lateral. A pulley and weight system allowed the muscle tendons to be loaded along their respective anatomic force vectors (Figure 1). The specimen was then set to neutral rotation, setting the position of the glenohumeral joint to 0.8° of elevation, 3.1° of plane of elevation, and 14.1° of external rotation, as reported in vivo. 15
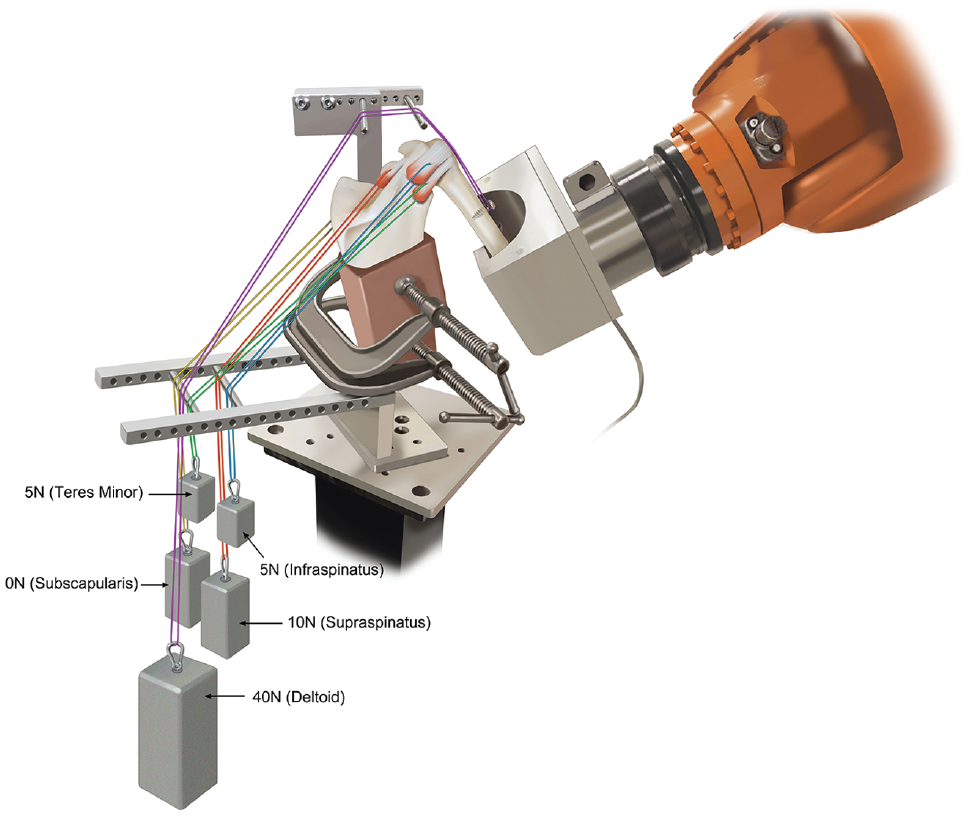
Biomechanical setup with the humerus secured to a custom-designed fixture on the end effector of the 6 degrees of freedom robotic arm. The scapula was rigidly fixed to another custom-designed fixture on a steel pedestal. A pulley and weight system allowed the muscle tendons to be loaded along their respective anatomic force vectors.
Shoulder Kinematics
Four static tests and 3 dynamic tests were performed in a randomized order to evaluate glenohumeral joint kinematics. The total duration of the 7 tests was 10 minutes. The 4 static tests consisted of a 40-N superior force applied to the joint at neutral position and at 30°, 60°, and 90° of humerothoracic abduction. Humeral head translation was recorded throughout all tests, and superior humeral head translation was the reported outcome measure for all tests.
The 3 dynamic tests were (1) abduction, (2) scapular plane elevation (scaption), and (3) flexion. In these tests, the glenohumeral joint angles were prescribed according to an in vivo model, established by Ludewig et al, 15 from a neutral position to 120° of humerothoracic elevation, while the joint forces were minimized by the robot, allowing the simulated muscle forces to naturally stabilize the joint.
Experimental Conditions
Each specimen was tested in 4 consecutive states: (1) native, (2) isolated supraspinatus tear, (3) combined supra- and infraspinatus (posterosuperior) tear, and (4) SCR with a 3 mm–thick acellularized DA (ArthroFLEX; Arthrex), as recently described by Lacheta and Millett. 11 The weight on each muscle was adapted from a previously reported protocol. 17 In the native state, the weights were distributed as follows: supraspinatus, 10 N; infraspinatus, 5 N; teres minor, 5 N; subscapularis, 10 N; deltoid 40 N. In the isolated supraspinatus tear state, the supraspinatus and underlying capsule were sharply incised. The combined supra- and infraspinatus tear state was created by sharply resecting the infraspinatus tendon and its underlying capsule. The SCR using the acellularized DA was performed as previously described, 30 and this state was tested with identical muscle weight distribution to the combined supra- and infraspinatus tear state. The specimens were sprayed with saline solution between each state to avoid tissue desiccation. All states are shown in Figure 2.
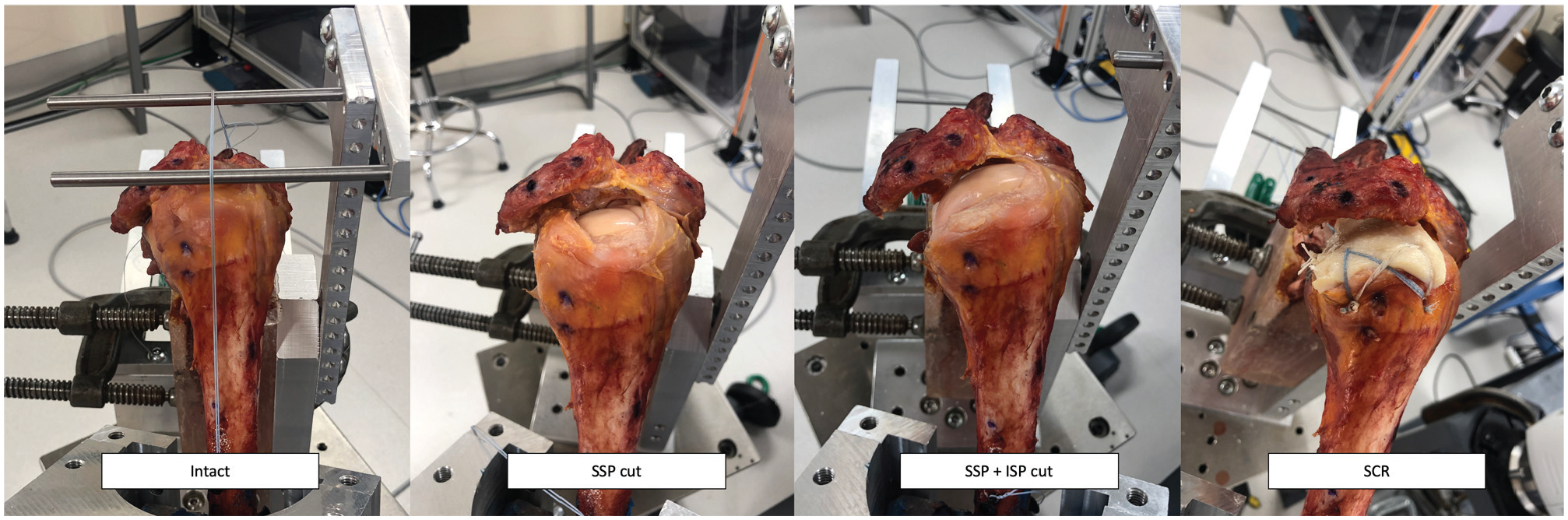
Four consecutive states: (1) native, intact (2) isolated SSP tear, (3) SSP+ISP tear, and (4) SCR with a 3 mm–thick acellularized DA. DA, dermal allograft; ISP, infraspinatus; SCR, superior capsule reconstruction; SSP, supraspinatus.
Statistical Analysis
For the static tests, to match the repeated-measures experimental design, random-intercepts linear mixed effects models were used to compare the superior translation of the humerus at neutral abduction and at 30°, 60°, and 90° of abduction among native, supraspinatus cut, supraspinatus and infraspinatus cut, and SCR states. Estimated marginal means were reported and the Tukey method 37 was used to make all pairwise comparisons among the 4 states. Residual diagnostics were inspected to ensure model fit and that assumptions were met. All hypothesis tests were 2-tailed, and P values < .05 were deemed statistically significant. The statistical software R Version 3.5.0 was used for all plots and analyses (R Core Team).9,14,16
For dynamic tests, statistical parametric mapping (SPM) was used to analyze the superior translation of the humeral head in the dynamic tests. SPM provides a statistical means to compare 2 or multiple trajectories that change in time or space. 35 This novel method is based on a different theoretical framework compared with the commonly used analysis of variance (ANOVA) and can provide important insights into locations where the 2 trajectories become significantly different. 29 A typically used ANOVA is unable to detect the differences between trajectories unless a pointwise comparison, followed by P value corrections, is performed. Such an approach may lead to considerable statistical power loss. Alternatively, calculating 1 value (eg, average) from a trajectory to perform ANOVA might be prone to bias in kinematic data. 29 Thus, SPM was used in the current study for the statistical analysis to compare each experimental state to the native state.
Results
Superior Translation During Static Testing
In static testing, the supraspinatus cut and the supra- and infraspinatus cut states showed a significant increase in superior translation compared with the native state at all degrees of abduction (all P < .001). Supra- and infraspinatus cut increased superior translation significantly when compared with the supraspinatus cut only at neutral position and at 60° of abduction (P = .03 and P = .02). SCR significantly decreased superior translation when compared with the supra- and infraspinatus cut in all degrees of abduction (all P < .05) and when compared with the supraspinatus cut at neutral position and at 60° of abduction (all P < .001). When compared with the native state, SCR showed a significant increase in translation compared with the native state at 0° and 30° of abduction (P < .001), but it was not significantly different from the native state at 60° and 90° of abduction (P > .05). The greatest superior translation of the humeral head was found in the supra- and infraspinatus-deficient state at all degrees of abduction, followed by the superior translation in the supraspinatus-deficient state (Figure 3).
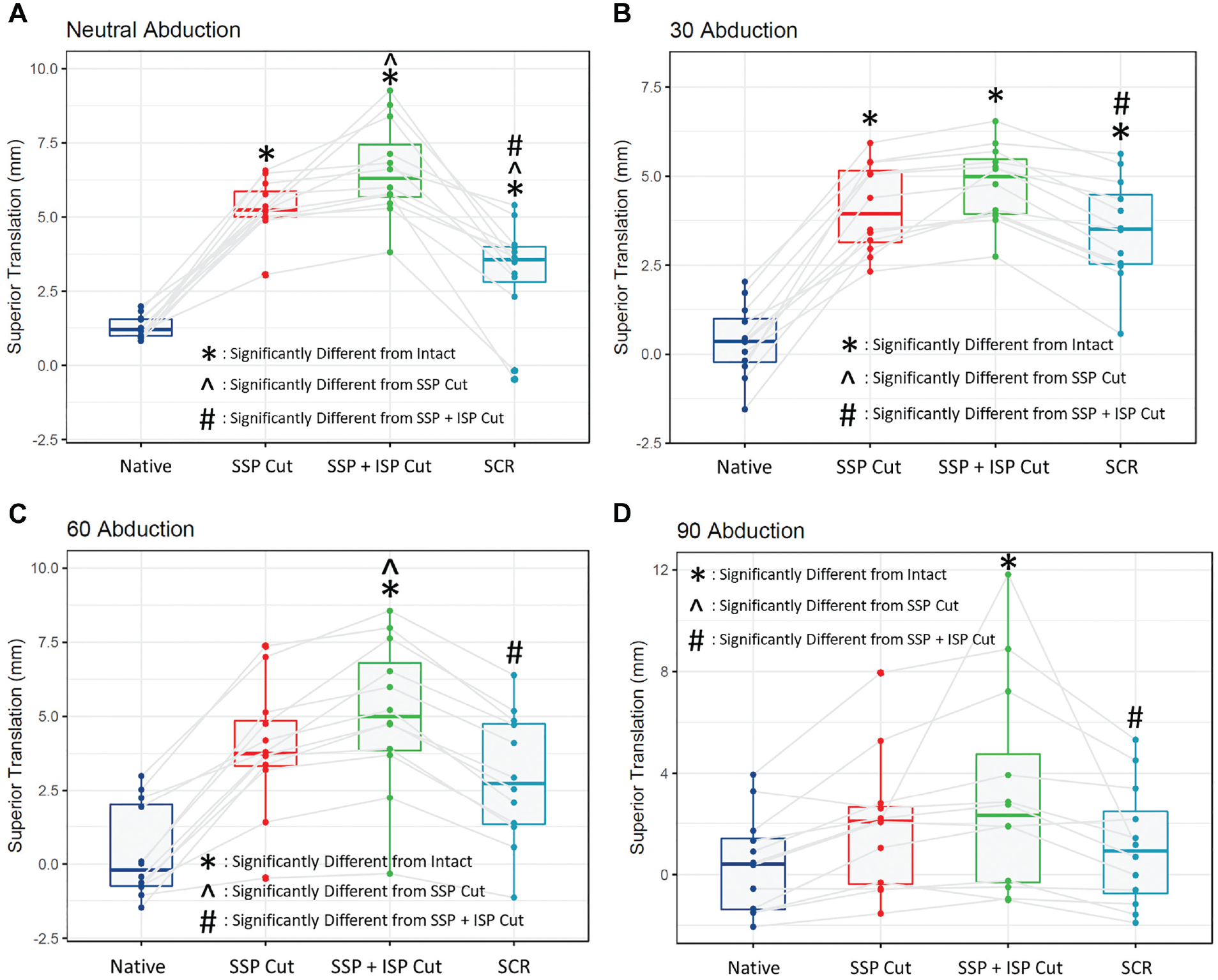
(A) Superior translation of the humeral head at 0° of abduction. (B) Superior translation of the humeral head at 30° of abduction. (C) Superior translation of the humeral head at 60° of abduction. (D) Superior translation of the humeral head at 90° of abduction. ISP, infraspinatus; SCR, superior capsular reconstruction; SSP, supraspinatus.
The results of dynamic testing are shown in Figures 4, 5, and 6. Zero mm of superior translation denotes the position of the humeral head in the neutral shoulder position in the intact state.
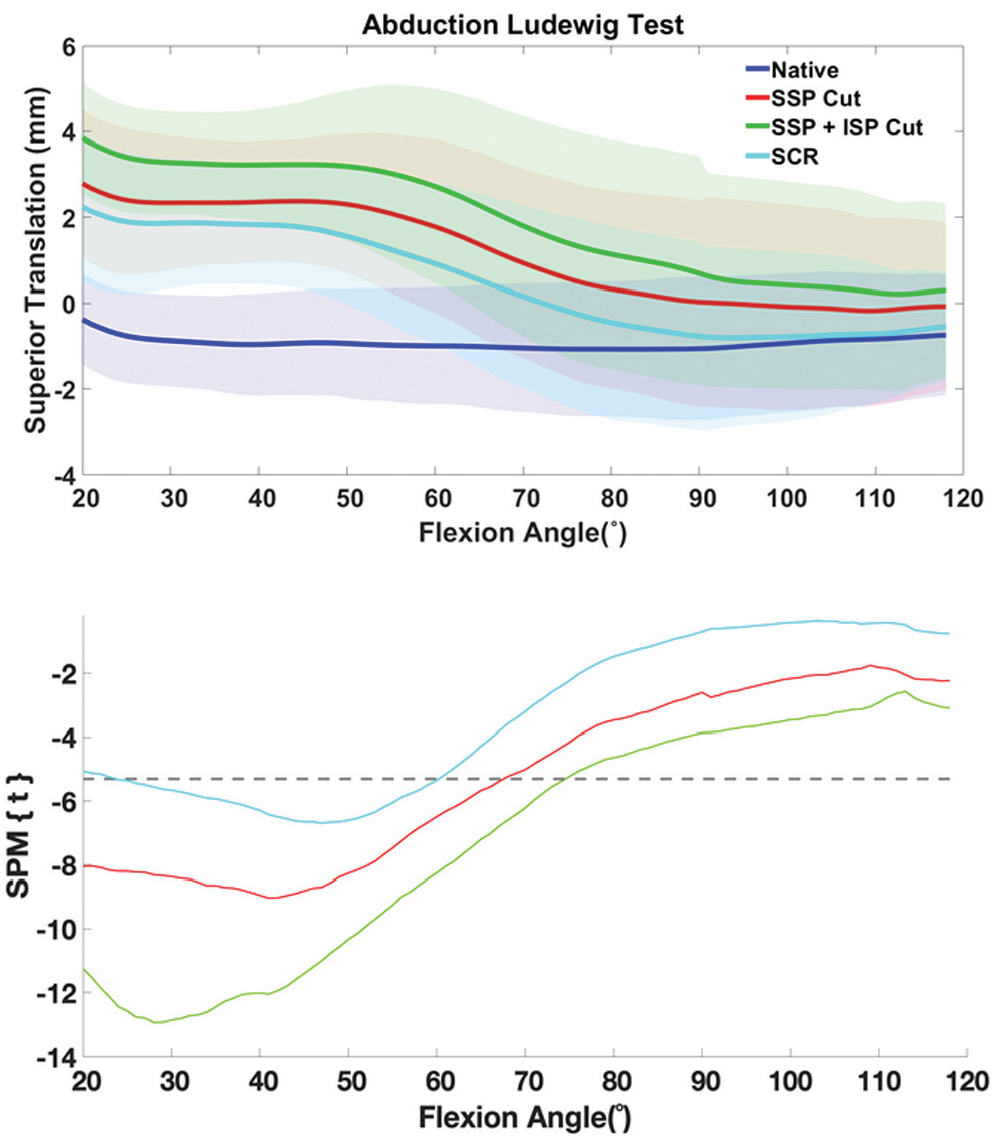
Superior humeral head translation as a function of elevation angle during the abduction test. The top graph shows the magnitude of superior humeral head translation (in mm), with shading indicating the magnitude of variability. The bottom graph shows the result of the SPM analysis (t value). For each state, a t value under the grey dotted line indicates a significant difference from the intact state, while a value above the dotted line indicates no significant difference from the intact state. ISP, infraspinatus; SCR, superior capsular reconstruction; SPM, statistical parametric mapping; SSP, supraspinatus.
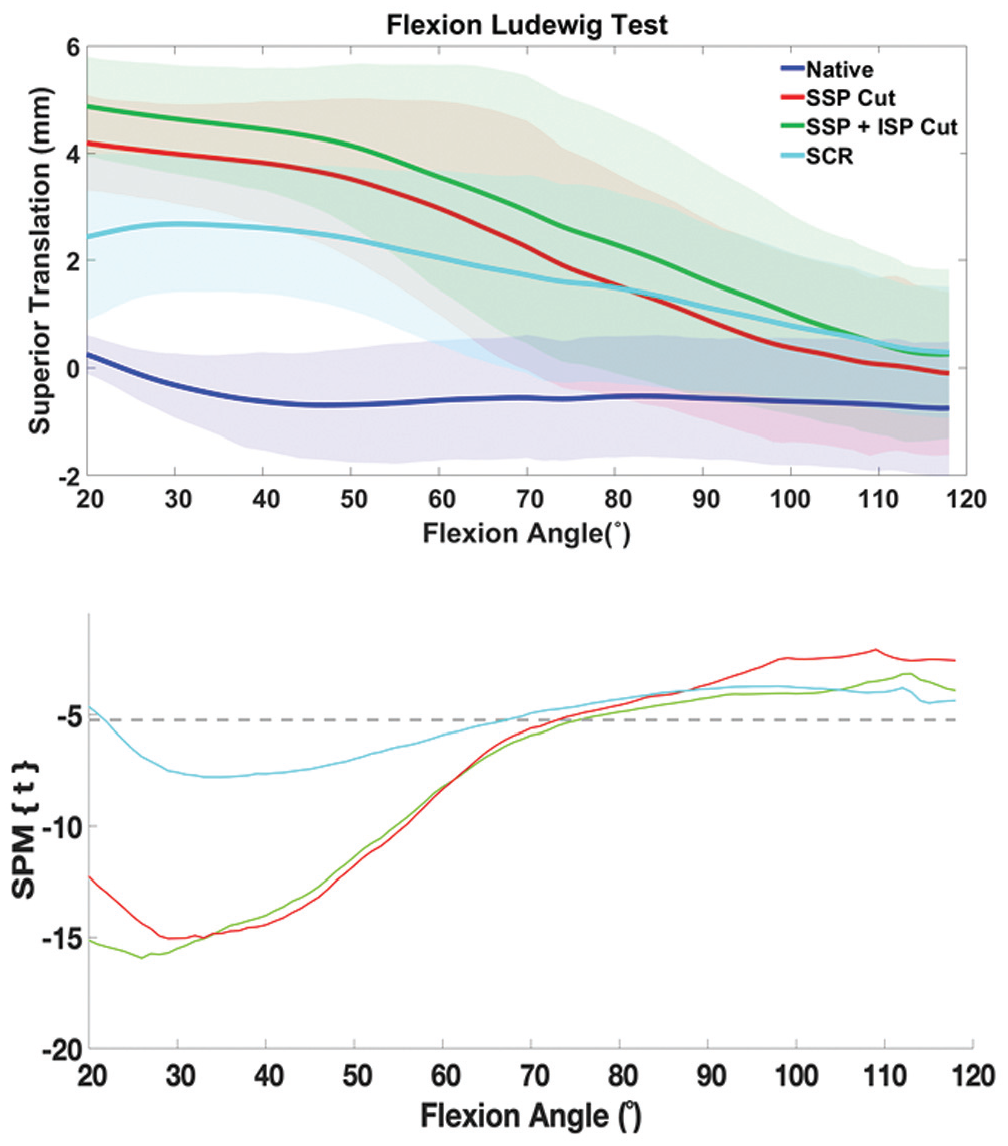
Superior humeral head translation as a function of elevation angle during the flexion test. The top graph shows the magnitude of superior humeral head translation (in mm), with shading indicating the magnitude of variability. The bottom graph shows the result of the SPM analysis (t value). For each state, a t value under the grey dotted line indicates a significant difference from the intact state, while a value above the dotted line indicates no significant difference from the intact state. ISP, infraspinatus; SCR, superior capsular reconstruction; SPM, statistical parametric mapping; SSP, supraspinatus.
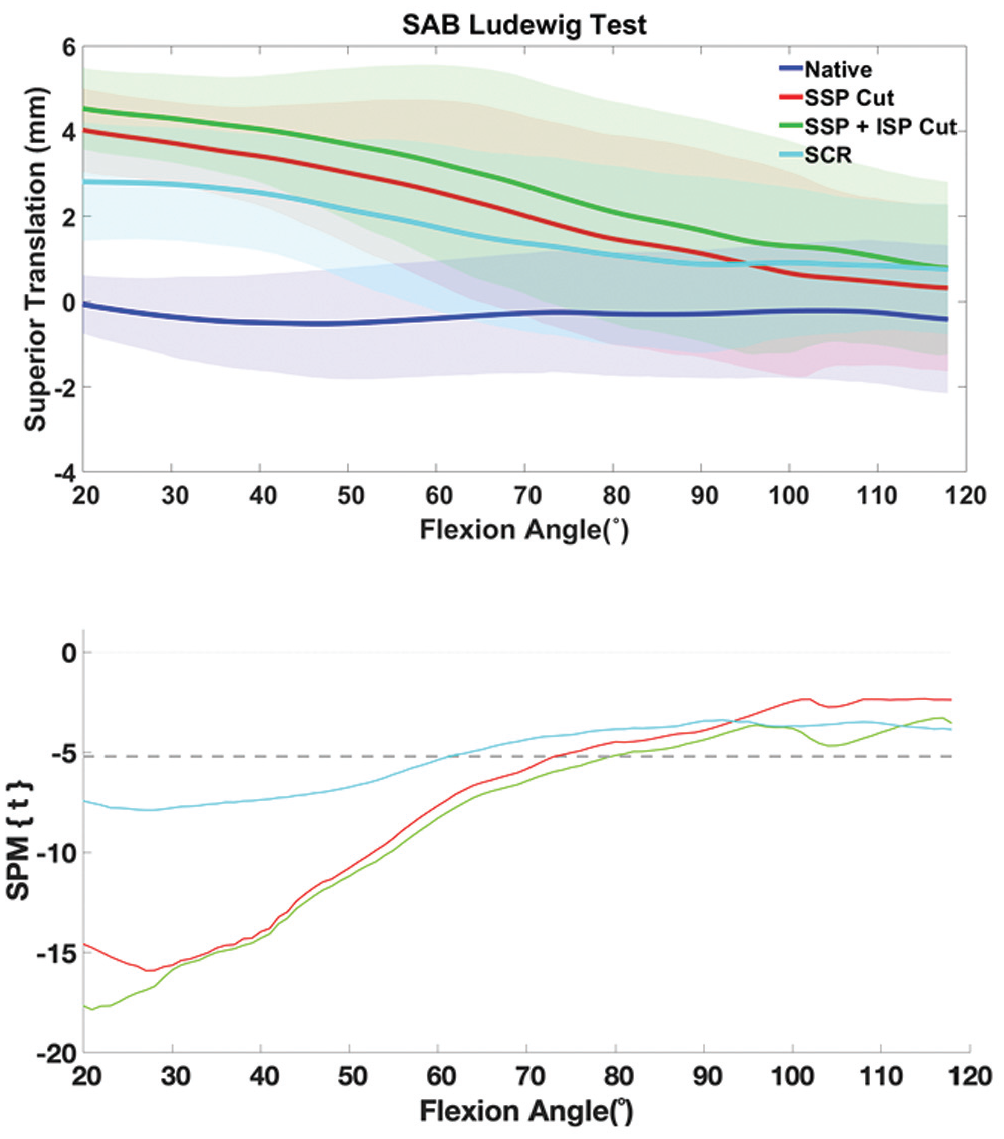
Superior humeral head translation as a function of elevation angle during the scapular plane abduction (SAB) test. The top graph shows the magnitude of superior humeral head translation (in mm), with shading indicating the magnitude of variability. The bottom graph shows the result of the SPM analysis (t value). For each state, a t value under the grey dotted line indicates a significant difference from the intact state, while a value above the dotted line indicates no significant difference from the intact state. ISP, infraspinatus; SCR, superior capsular reconstruction; SPM, statistical parametric mapping; SSP, supraspinatus.
Dynamic testing results showed significantly increased superior translation in the supra- and infraspinatus cut state compared with the native state at lower elevation angles, which diminished at higher elevation, becoming nonsignificant in all tests at elevation >75°. SCR reduced the magnitude of superior translation across all elevation angles compared with the cut states, but it remained significantly different from the intact state up to 60° of elevation.
Discussion
The main finding of this study is that a posterosuperior rotator cuff tear pattern significantly increased superior glenohumeral translation when compared with the native and supraspinatus insufficient states in a robotic shoulder model in abduction, flexion, and scaption motions. Further, while SCR for posterosuperior rotator cuff patterns improved superior stability when compared with the superior- and posterosuperior rotator cuff deficient state, superior translation remained significantly increased when compared with the native state at <60° of abduction. These findings partially confirm the initial hypotheses. Although greater structural deficits in the rotator cuff lead to increased glenohumeral instability (H1 and H2 confirmed), SCR restored stability in higher degrees of abduction. However, SCR was unable to restore native stability at <60° of abduction (H3 partially confirmed).
This study aimed to establish an accurate, dynamic shoulder model with the ability to simulate different rotator cuff tear patterns and further evaluate the influence of surgical techniques on glenohumeral stability. A dynamic test setup can better mimic active, in vivo motions compared with a static test setup, an advantage that has been previously recognized and utilized in knee-related research.6,7,28,32 Recent dynamic cadaveric knee studies have focused on the evaluation of knee-motion patterns with the help of a dynamic robotic test setup, as seen in investigations by Rasmussen et al, 32 Nitri et al, 28 and Geeslin et al.6,7 However, there is a lack of reports utilizing dynamic shoulder models. In this study, to mimic in vivo conditions, multiplanar humeral in vivo motions measured by Ludewig et al 15 were implemented to the current robotic model in the planes of flexion, abduction, and scaption. To prove the accuracy of the data generated by this dynamic model, static testing was performed simultaneously. The results of dynamic testing are consistent with those of static testing, showing a significantly increased superior translation in the supra- and infraspinatus cut state compared with the native state at lower elevation angles, which diminished at higher elevation, becoming nonsignificant in all tests at elevation >75°.
The results of the current study are consistent with previously published biomechanical studies by Mihata et al17,25,26 on the behavior of SCR in a static test setup, with a significantly increased superior translation of the humeral head after superior rotator cuff transection, which was completely to partially restored with SCR using an auto- or allograft.
Another important contribution to previous literature is the additional glenohumeral instability that was observed when creating a posteriorly extending massive rotator cuff tear. Ishihara et al 8 and Mihata et al22,25 have previously shown that the superior rotator cuff and the superior shoulder capsule play an important role in passive stability of the glenohumeral joint. A tear in the superior capsule at the greater tuberosity, which may be observed in articular-sided partial rotator cuff tears, increases anterior and inferior translation. 8 A defect in the superior capsule, seen in transmural superior rotator cuff tears, increases glenohumeral translations in all directions in a static biomechanical evaluation. 8 The current study confirmed the biomechanical role of the superior capsule and the superior rotator cuff during early abduction at lower angles.25,26 Also, this study demonstrated that a posteriorly extending tear, including both the supra- and infraspinatus tendons, significantly increased glenohumeral instability in static and dynamic testing when compared with the supraspinatus-deficient state alone. This additional instability needs to be respected when encountered surgically, as increasing tear sizes may lead to larger forces applied to the reconstruction/graft when addressing technically irreparable rotator cuff tears.
Mihata et al17,23,25 have demonstrated that SCR using a fascia lata autograft or a human DA can restore native glenohumeral kinematics in simulated superior rotator cuff tears (supraspinatus cut only) in biomechanical studies. These findings were reflected by excellent clinical outcomes and the increased acromiohumeral distance observed in several clinical investigations.18-20 Convincing results have led to the indication for SCR in even massive posterosuperior rotator cuff tears. Short-term results have confirmed an improvement in clinical outcomes in these cases.4,11 However, compared with initial reports for SCR in isolated superior rotator cuff tear patterns, improvements in clinical outcomes are diminished and the gain in acromiohumeral distance is reduced. As graft choice (fascia lata vs human DA), 17 graft thickness, 23 graft tension, 23 graft fixation,31,33 and capsular continuity 25 have been identified to be important factors for glenohumeral stability after SCR, the influence of rotator cuff tear size on glenohumeral stability has remained unknown. In the current study, in the setting of a massive posterosuperior rotator cuff tear, SCR led to a significant decrease in superior translation when compared with the supra- and infraspinatus insufficient states. However, this decrease in superior translation was unable to restore the biomechanical stability to that of the intact rotator cuff state. This suggests that posterosuperior rotator cuff tear seems to have exceeded the “critical size” that SCR alone is able to restore in terms of superior stability in this static and dynamic shoulder model.
While previous studies have indicated that the spacer 13 or biologic tuberoplasty effect 27 may be beneficial to recenter the humeral head (decrease superior translation), especially at higher degrees of abduction, this study has proven that rotator cuff tear size is a negative biomechanical predictor for glenohumeral stability during abduction, flexion, and scaption motion at lower flexion angles. SCR significantly improved glenohumeral stability when compared with the rotator cuff insufficient states, but it only partially restored native glenohumeral stability after large, posterosuperior rotator cuff tears. This factor has to be taken into account when performing SCR in patients whose rotator cuff tears exceed superior rotator cuff tears. Partial repair of the infraspinatus and subscapularis tendons may be performed, when possible, to reduce the posterosuperior gap and strengthen the function of SCR on passive glenohumeral stability.
Limitations
While this study revealed interesting and novel findings, there are limitations. First, muscle loading was static rather than dynamic during testing. Second, other previously described factors influencing glenohumeral stability after SCR (graft tension, graft thickness, etc) were not evaluated in this study. Third, the inherent limitation of cadaveric models in that healing is not considered. However, SCR was performed as routinely done in everyday clinical practice.11,30 Despite these limitations, this study provides valuable information to clinicians treating technically irreparable rotator cuff tears.
Conclusion
Massive posterosuperior rotator cuff tears biomechanically increased humeral superior translation when compared with the intact and supraspinatus tendon–insufficient rotator cuff states. SCR using a 3–mm DA partially restored the superior stability of the glenohumeral joint even in the presence of a simulated massive posterosuperior rotator cuff tear in a static and dynamic robotic shoulder model.
Footnotes
Submitted July 23, 2020; accepted January 19, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: P.J.M. has received royalties from Arthrex and Medbridge; research support from Arthrex, Ossur, Siemens, and Smith & Nephew; consulting fees from Arthrex; hospitality payments from Merz Pharmaceuticals GMBH, Arthrosurface Incorporated, Gemini Mountain Medical LLC, Stryker Corporation, and Sanofi-Aventis; and holds stock in VuMedi. M.T.P. has received royalties and consulting fees from Arthrex; and consulting fees from Joint Restoration Foundation (Allosource). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.