
Abstract
Background:
Although minimal clinically important difference (MCID), Patient Acceptable Symptom State (PASS), and substantial clinical benefit (SCB) have been defined for hip-specific legacy patient-reported outcome measures, these metrics have not been defined for the Patient-Reported Outcomes Measurement Information System (PROMIS) instruments for patients undergoing hip arthroscopy.
Purpose:
To define the MCID, PASS, and SCB thresholds for the PROMIS Physical Function (PF) computerized adaptive test (CAT) and PROMIS Pain Interference (PI) instruments in patients undergoing hip arthroscopy for femoroacetabular impingement syndrome (FAIS).
Study Design:
Cohort study (Diagnosis); Level of evidence, 2.
Methods:
Patients undergoing primary hip arthroscopy between August 2018 and January 2019 for the treatment of FAIS were retrospectively analyzed. Patients were administered the PROMIS-PF, PROMIS-PI, Hip Outcome Score (HOS)–Activities of Daily Living, HOS–Sports Subscale, modified Harris Hip Score, and International Hip Outcome Tool–12 preoperatively and at 1 year postoperatively. MCID was calculated using the distribution method, whereas PASS and SCB were calculated using an anchor-based method. Patients achieving clinically significant outcomes (CSOs) were compared with those who did not achieve CSOs via chi-square and independent-samples t tests, and a multivariate logistic regression was conducted to determine predictors of CSO achievement.
Results:
124 patients with a mean age of 32.7 ± 12.3 years were included in the analysis. The threshold scores required to achieve MCID, PASS, and SCB, respectively, were as follows: PROMIS-PI (–3.1, 53.7, 51.9) and PROMIS-PF (3.3, 47.0, 49.9). Patients achieved any MCID, PASS, and SCB for PROMIS scores at a rate of 89.0%, 71.8%, and 62.1%, respectively, compared with 87.1%, 76.6%, and 71.8% for legacy patient-reported outcome measurements. For PROMIS-PF, higher preoperative PROMIS-PF score was a positive predictor of CSO achievement, and patients achieving SCB were significantly younger (30.3 ± 12 vs 35.6 ± 12 years; P = .017) with significantly lower body mass index (BMI) (24.7 ± 6.4 vs 27.9 ± 7; P = .009). Preoperative chronic pain and history of orthopaedic surgery were negative predictors of PROMIS-PI CSO achievement, whereas higher (worse) preoperative PROMIS-PI scores were a positive predictor.
Conclusion:
Our study defined the MCID, PASS, and SCB for the PROMIS-PF CAT and PROMIS-PI CAT at 1 year postoperatively. Patients with higher preoperative PROMIS scores, younger age, and lower BMI were more likely to achieve CSO, whereas preoperative chronic pain and history of orthopaedic surgery were negative predictors of CSO achievement.
The Patient-Reported Outcomes Measurement Information System (PROMIS) has been used increasingly within orthopaedic research since it was developed in 2004 by the National Institutes of Health. PROMIS functions with integrated item response theory with computerized adaptive testing (CAT) to provide a single, generalizable, and validated patient-reported outcome measure (PROM) while attempting to negate floor or ceiling effects with fewer individual questions when compared with legacy PROMs.9,11,15,17,40 Previous studies have used PROMIS for evaluating patients with meniscal surgery, rotator cuff tears, shoulder arthritis, shoulder instability, and anterior cruciate ligament tears.2,3,14,19,20 However, there is a relative paucity of literature applying PROMIS to patients who have undergone hip arthroscopy for femoroacetabular impingement syndrome (FAIS).28,30,32,34,35
Minimal clinically important difference (MCID), Patient Acceptable Symptom State (PASS), and substantial clinical benefit (SCB) are relatively new metrics of determining whether patients achieve clinically significant outcomes (CSOs) after interventions. 7 MCID serves as an important measure that goes beyond statistically significant differences between groups and establishes the smallest difference that a patient would describe as beneficial, whereas SCB can be considered the upper bound and ideal target for CSO.30,34 Furthermore, PASS can be interpreted as an intermediate outcome that is also acceptable to the patient. 5 Although these values have been defined for the modified Harris Hip Score (mHHS), the Hip Outcome Score (HOS), the International Hip Outcome Tool–2 (iHOT-12),32-34 and the visual analog scale (VAS) for pain 5 in the setting of FAIS, these values for PROMIS at the 1-year postoperative setting remain unknown. Although the PROMIS does not have hip-specific questions, the PROMIS Physical Function (PF) scale is the default scale applied to patients with hip and other lower extremity conditions. Little is known about whether this delineation is appropriate. The PROMIS Pain Interference (PI) instrument may also be appropriate for evaluating patients with FAIS. This instrument measures the consequences of pain and may include the extent to which pain hinders engagement with social, cognitive, emotional, physical, and recreational activities. 1 PROMIS PI also incorporates items regarding sleep and overall enjoyment in life. The PI form is universal rather than injury specific.
The purpose of this study was to define the MCID, PASS, and SCB thresholds for the PROMIS-PF and PROMIS-PI CAT instruments in patients undergoing hip arthroscopy for FAIS. We hypothesized that higher preoperative physical function, lower body mass index (BMI), and younger age would positively predict CSO achievement, whereas preoperative chronic pain or a history of orthopaedic surgery would negatively predict CSO achievement.
Methods
Patient Selection
After approval was obtained from our institutional review board, data were prospectively collected on all patients undergoing hip arthroscopy for the treatment of FAIS by a single, fellowship-trained and board-certified orthopaedic surgeon (S.J.N.). Data were retrospectively analyzed in a clinical repository for patients undergoing primary hip arthroscopy for the treatment of FAIS between August 2018 and January 2019. Inclusion criteria consisted of clinical and radiographic diagnosis of symptomatic FAIS, failure of nonoperative management (including physical therapy, activity modification, oral anti-inflammatory drugs, and/or intra-articular cortisone injection), and surgical treatment with hip arthroscopy for FAIS. 18 Only patients completing at least 1 preoperative outcome measure and a 1-year postoperative outcome measure were included. Exclusion criteria consisted of history of bilateral hip surgery, hip arthroscopy for an indication other than FAIS, signs of osteoarthritis (Tönnis grade >1), hip dysplasia (lateral center-edge angle <20°), a history of pediatric hip disorders (eg, slipped capital femoral epiphysis, hip dysplasia, Perthes disease), and concomitant gluteus medius or minimus repair.
Functional Outcome Evaluation
Preoperatively, demographic data were collected from all patients, including sex, age, operative extremity, BMI, sports participation, past orthopaedic surgery, preoperative chronic pain, and medical comorbidities. All patients completed preoperative and 1-year legacy hip-specific PROMs including the HOS–Activities of Daily Living subscale (HOS-ADL), 27 the HOS–Sports Subscale (HOS-SS), the mHHS, 10 and iHOT-12. 31 Patients also completed the CAT version of PROMIS-PF and PROMIS-PI 25 via the Outcome Based Electronic Research Database (Universal Research Solutions). 15 For PROMIS CAT, the measures are scored on a T-score metric where a score of 50 represents the average of the general population of the United States and 10 represents the standard deviation. A higher PROMIS-PI score represents greater (worse) pain, whereas a higher PROMIS-PF score represents greater (better) function.
The MCID for 1-year PROMIS-PF, PROMIS-PI, HOS-ADL, HOS-SS, mHHS, and iHOT-12 was determined by calculating the ½ SD of each preoperative outcome score in the study patients, as described in the literature.12,21,24
The PASS for PROMIS-PF, PROMIS-PI, HOS-ADL, HOS-SS, mHHS, and iHOT-12 was calculated using an anchor-based method. 29 At 1-year follow-up, patients were asked the following question: “Taking into account all the activities you have during your daily life, your level of pain, and also your functional impairment, do you consider that your current state is satisfactory?” Choices available were “yes” and “no.” Patients answering “yes” were considered to have achieved PASS whereas patients answering “no” were not. Receiver operating characteristic (ROC) curve analysis was used to determine threshold scores based on the Youden J value, which seeks to optimize sensitivity and specificity, with an area under the ROC curve (AUC) of 0.70 or higher being considered clinically useful.22,26 The ROC curve analysis is provided in Appendix A1 (available in the online version of this article).
SCB for the PROMs was also calculated using an anchor-based method. At 1-year follow-up, patients were asked the following question: “Since your surgery, has there been any change in your daily functioning and nonsporting activities related to your treated hip?” Choices available are shown in Figure 1. Patients responding with either “A very great deal better,”“A great deal better,” or “A good deal better” were classified as the “much improved group,” and patients responding with either “Almost the same, hardly any better,”“No change,” or “Almost the same, hardly any worse” were classified as the “no change group.” The ROC curve analysis is provided in Appendix A2 (available online).
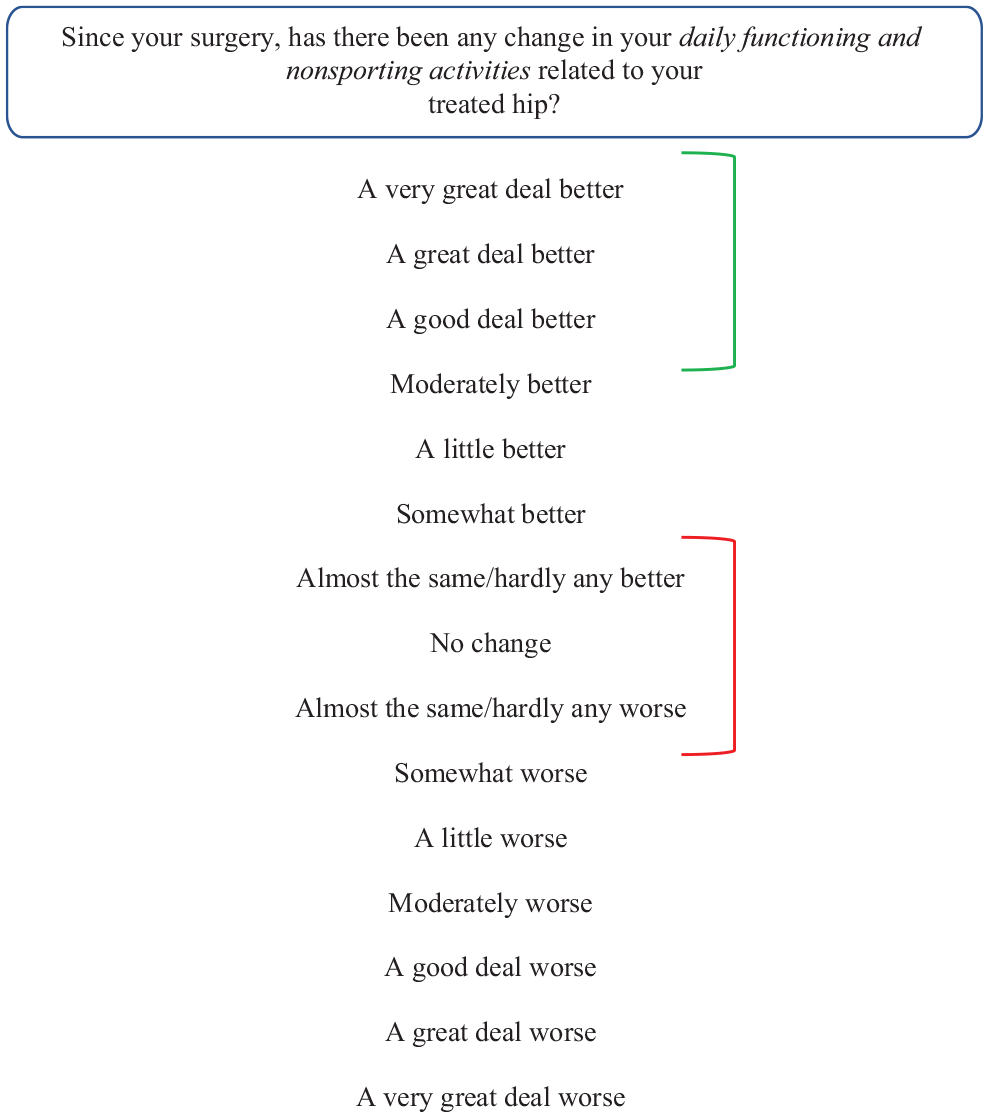
Anchor question overview for substantial clinical benefit. Patients responding with either “A very great deal better,”“A great deal better,” or “A good deal better” were classified as the “much improved group,” and patients responding with either “Almost the same/hardly any better,”“No change,”“or Almost the same/hardly any worse” were classified as the “no change group.”
Statistical Analysis
Descriptive statistics for all continuous variables were reported as means with standard deviations, and frequency statistics were reported for all noncontinuous variables. Paired-samples t tests were used to compare preoperative and 1-year postoperative PROMs. For the legacy PROMs, any percentage of patients ≥15% of the study population achieving the maximum or minimum score was deemed as a significant ceiling or floor effect. 38 For PROMIS, any percentage ≥15% of the study population in the top or bottom 5th percentile was deemed as significant ceiling or floor effect.3,28 A ROC curve analysis was performed to identify preoperative threshold values on the PROMIS instruments that predicted postoperative achievement of CSOs. To compare patients achieving CSOs with patients who did not achieve CSOs, chi-square tests for categorical variables and independent-samples t tests for continuous variables were performed. Variables with a significant difference (P≤ .05) and P values <.20 were used to construct a multivariate logistic regression. Statistical significance for all analyses was set at α≤ .05. All statistical analysis was performed using SPSS (Version 26; SPSS Inc).
Results
Demographics
A total of 124 patients completed preoperative and 1-year PROMs and were included in the study, with a mean ± SD age and BMI of 32.7 ± 12.3 years and 26.2 ± 6.9, respectively (Figure 2). The majority of patients were female (73.4%), and 56.5% of patients underwent surgery on their right hip. All patients underwent primary labral repair, acetabuloplasty, debridement, synovectomy, femoral osteochondroplasty, and capsular closure. All cartilage defects discovered at the time of surgery were debrided. No concomitant procedures such as microfracture or trochanteric bursectomy were performed in this cohort.
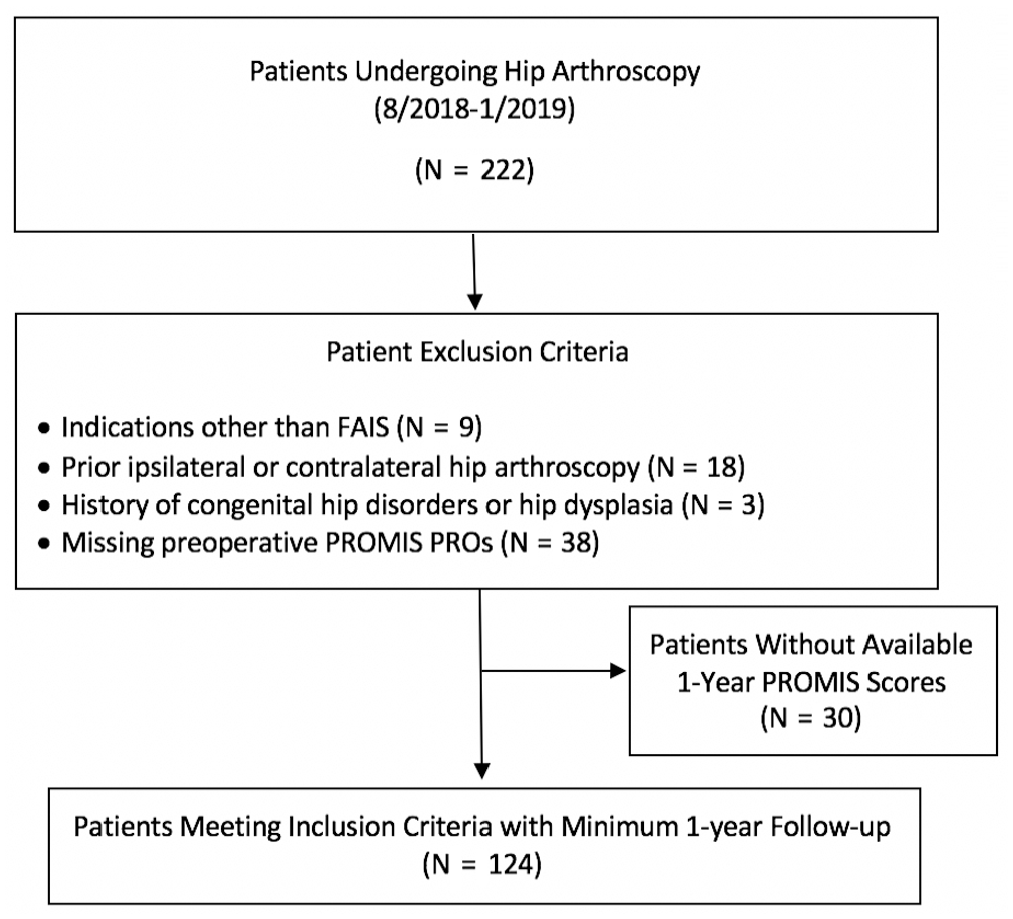
Flowchart indicating the number of patients excluded and lost to follow-up and patients meeting the inclusion criteria who were included in the final analysis. FAIS, femoroacetabular impingement syndrome; PRO, patient-reported outcome; PROMIS, Patient-Reported Outcomes Measurement Information System.
Clinical Outcomes Analysis
Comparisons of preoperative and minimum 1-year postoperative patient-reported outcomes are summarized in Figure 3. There were statistically significant improvements in PROMIS-PF (40.4 ± 6.5 vs 51.2.1 ± 10.9; P≤ .001), HOS-ADL (62.4 ± 17.0 vs 88.4 ± 13.1; P < .0001), HOS-SS (40.0 ± 20.7 vs 79.6 ± 22.9; P < .0001), mHHS (60.2 ± 15.0 vs 85.0 ± 15.8; P < .0001), iHOT-12 (31.9 ± 18.0 vs 62.3 ± 33.5; P < .0001), PROMIS-PI (61.6 ± 6.2 vs 50.6 ± 9.2; P < .001), and VAS pain score (55.0 ± 18.7 vs 17.8 ± 19.6; P < .001) at 1 year after surgery. A ceiling effect was observed for HOS-ADL and mHHS, with 16.1% and 19.3% of patients achieving the maximum scores, respectively. No floor effect was observed for any measure.
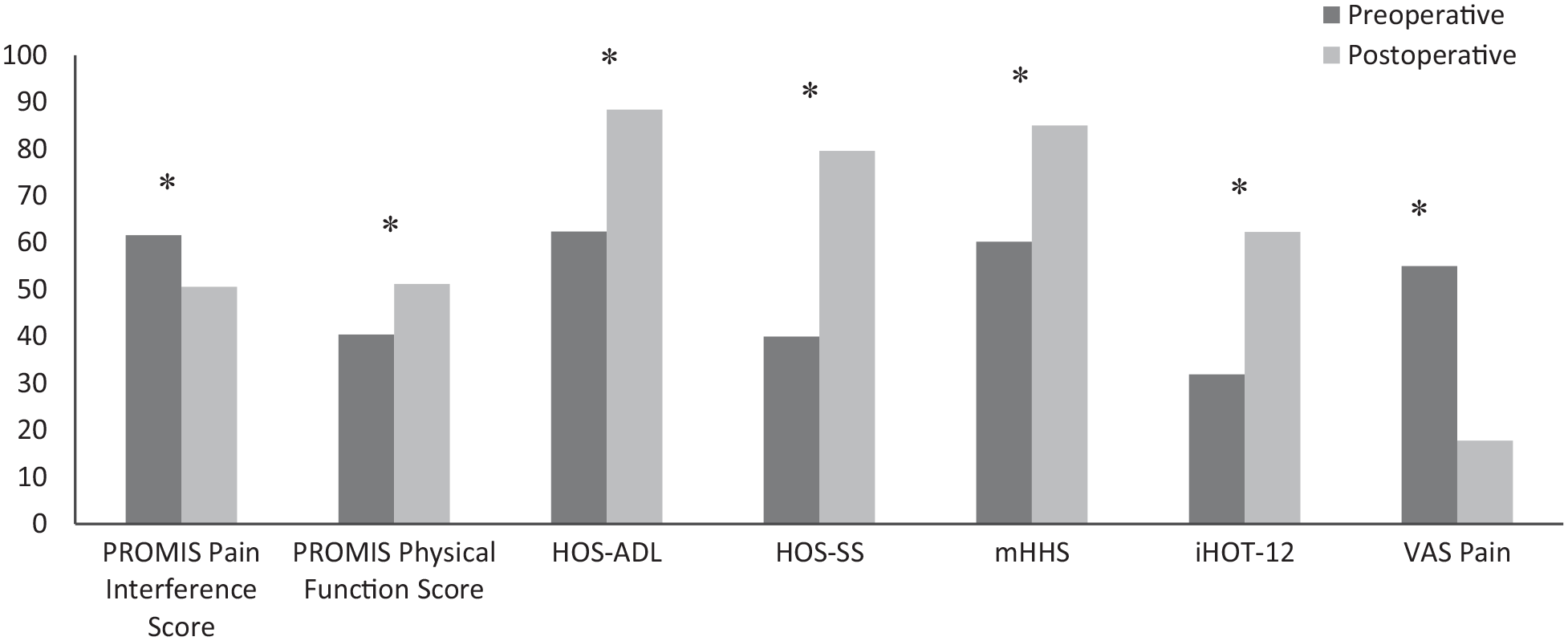
Comparison of preoperative and 1-year postoperative patient-reported outcome measures. *Significant improvements. iHOT-12, International Hip Outcome Tool–12; HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SS, Hip Outcome Score–Sports Subscale; mHHS, modified Harris Hip Score; PROMIS, Patient-Reported Outcomes Measurement Information System; VAS, visual analog scale.
MCID, PASS, and SCB
The PROMIS-PF, PROMIS-PI, HOS-ADL, HOS-SS, mHHS, and iHOT-12 threshold scores for achieving MCID, PASS, and SCB at 1 year after surgery are summarized in Table 1. The percentage of patients achieving meaningful clinical outcomes is provided Table 2.
MCID, PASS, and SCB Thresholds a
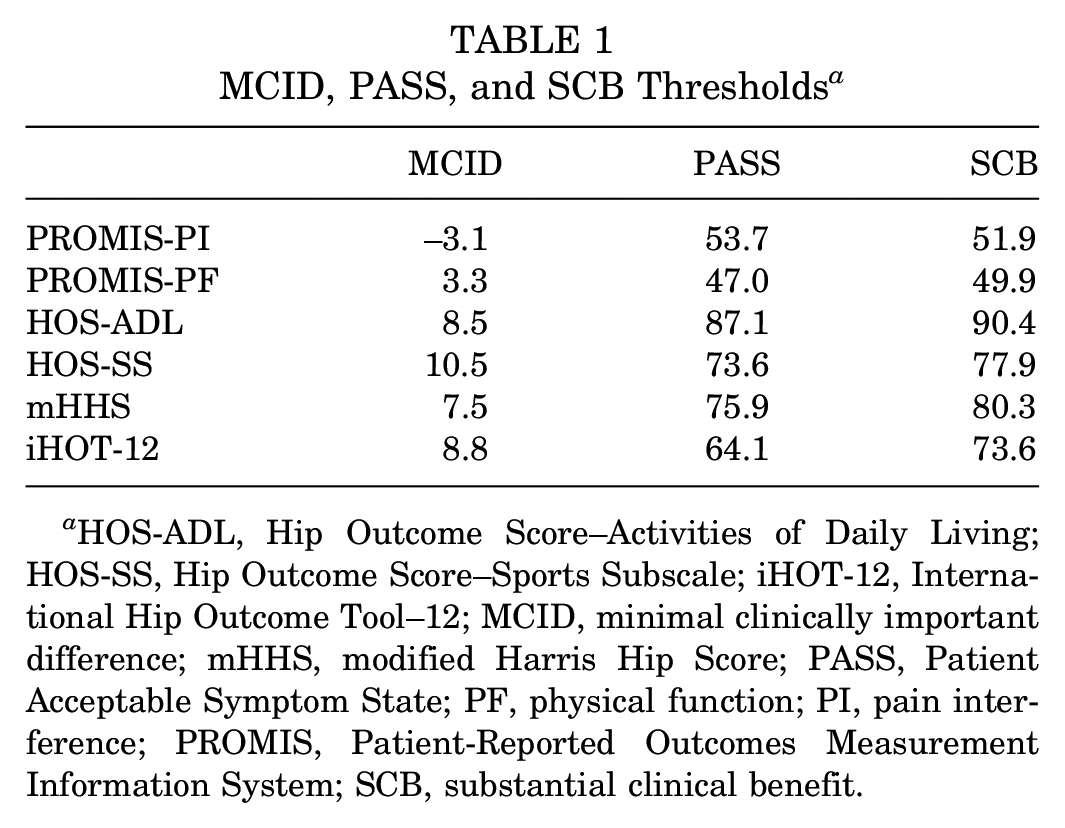
HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SS, Hip Outcome Score–Sports Subscale; iHOT-12, International Hip Outcome Tool–12; MCID, minimal clinically important difference; mHHS, modified Harris Hip Score; PASS, Patient Acceptable Symptom State; PF, physical function; PI, pain interference; PROMIS, Patient-Reported Outcomes Measurement Information System; SCB, substantial clinical benefit.
Percentage of Patients Achieving MCID, PASS, and SCB Thresholds a
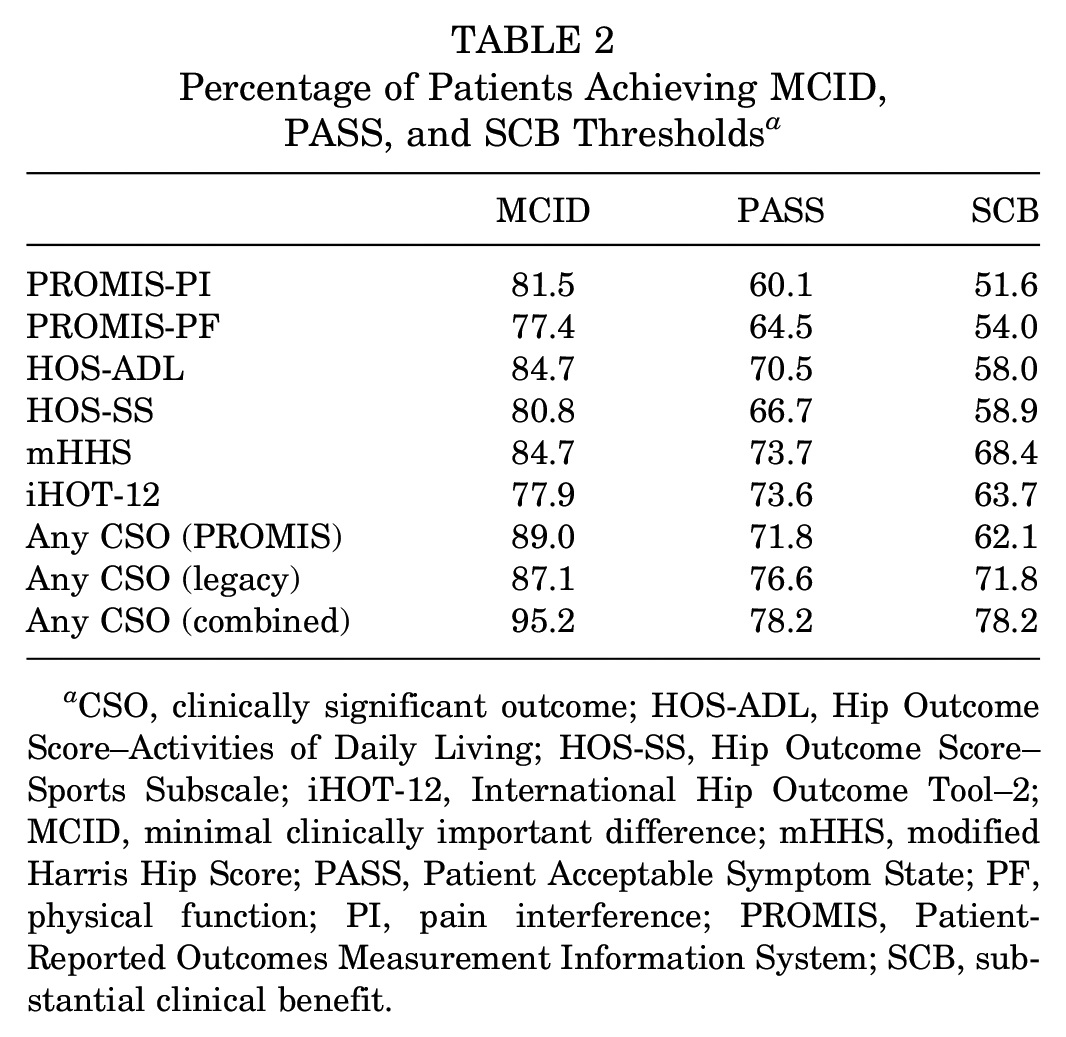
CSO, clinically significant outcome; HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SS, Hip Outcome Score–Sports Subscale; iHOT-12, International Hip Outcome Tool–2; MCID, minimal clinically important difference; mHHS, modified Harris Hip Score; PASS, Patient Acceptable Symptom State; PF, physical function; PI, pain interference; PROMIS, Patient-Reported Outcomes Measurement Information System; SCB, substantial clinical benefit.
Predictors of CSOs
For PROMIS-PF, the ROC curve analysis identified that preoperative scores >40.1 predicted achievement of PASS (AUC, 0.710; 95% CI, 0.61-0.81). For PROMIS-PI, a preoperative score >59.0 predicted achievement of the MCID (AUC, 0.761; 95% CI, 0.64-0.88).
Comparisons of patients who did and did not achieve MCID, PASS, and SCB on PROMIS-PF are shown in Table 3, and results of the multivariate binary logistic regressions are provided in Table 4. No significant differences were seen in any demographic or clinical variables for patients achieving MCID (P > .05). For PASS, patients achieving this CSO had significantly higher preoperative PROMIS-PF scores, and they tended to be younger on average. On multivariate analysis, higher preoperative PROMIS-PF scores remained significant. Patients achieving SCB were significantly younger, had significantly lower BMIs, and had significantly higher preoperative PROMIS-PF scores. Higher preoperative PROMIS-PF scores were a significant predictor of SCB achievement on multivariate analysis.
Comparison of Patients Who Achieved and Did Not Achieve CSOs for PROMIS-PF a
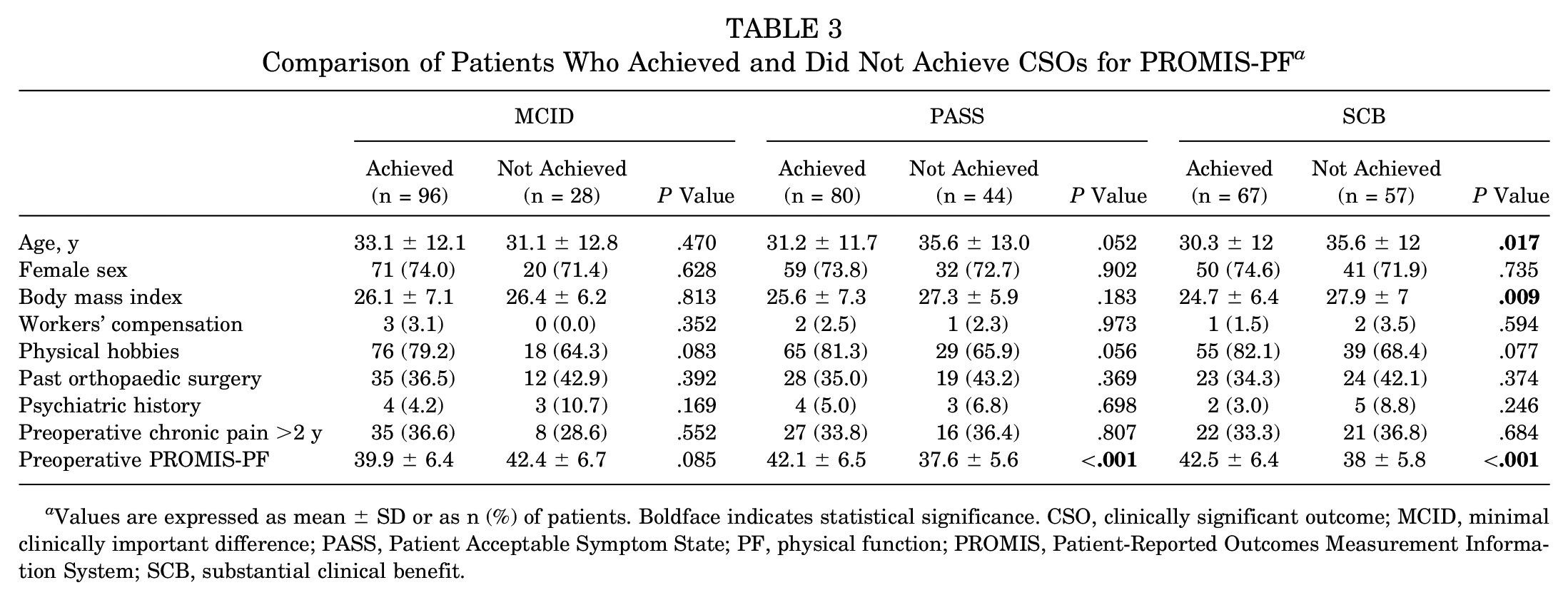
Values are expressed as mean ± SD or as n (%) of patients. Boldface indicates statistical significance. CSO, clinically significant outcome; MCID, minimal clinically important difference; PASS, Patient Acceptable Symptom State; PF, physical function; PROMIS, Patient-Reported Outcomes Measurement Information System; SCB, substantial clinical benefit.
Multivariate Binary Logistic Regression Results of Predictors for CSO Achievement a
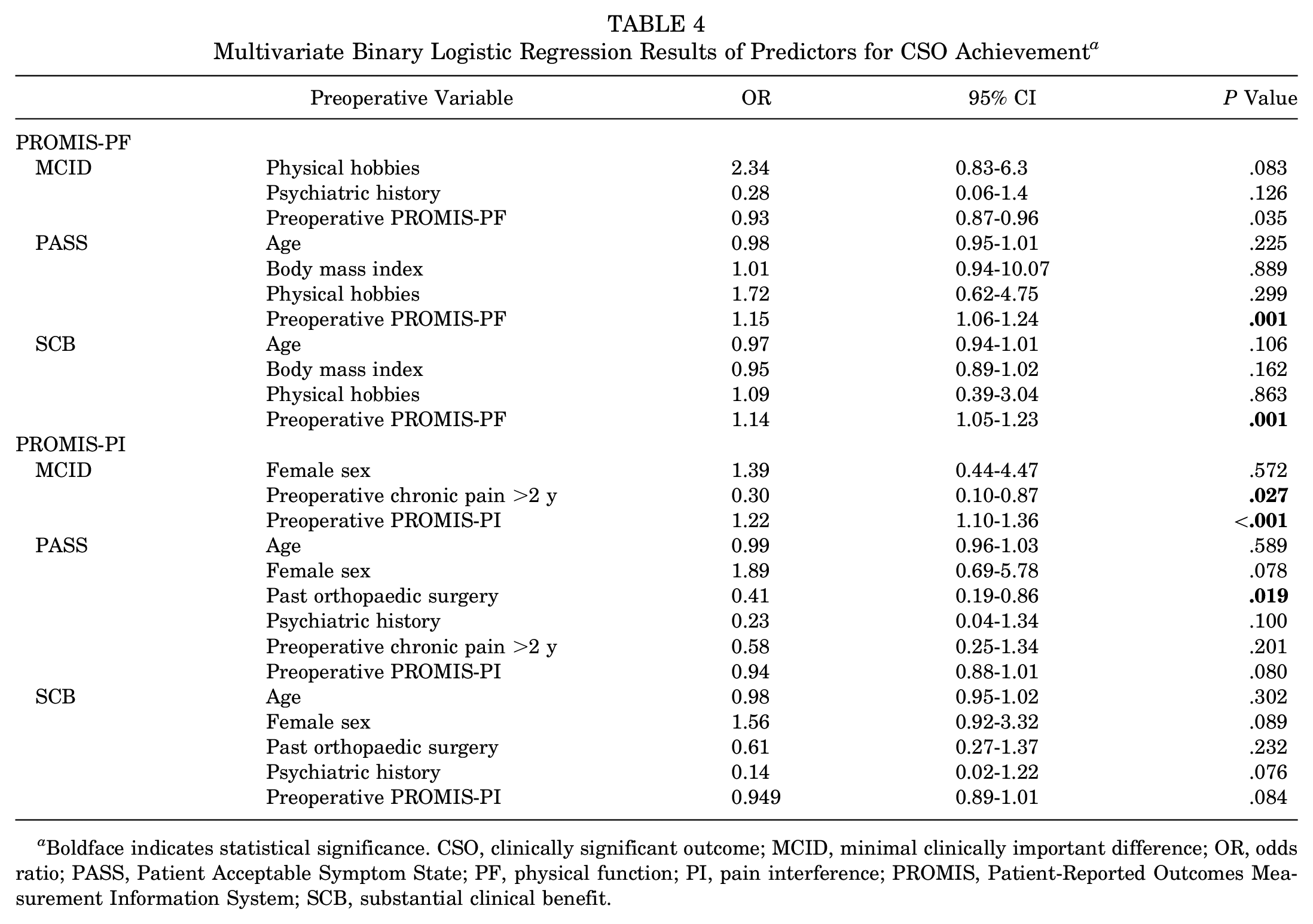
Boldface indicates statistical significance. CSO, clinically significant outcome; MCID, minimal clinically important difference; OR, odds ratio; PASS, Patient Acceptable Symptom State; PF, physical function; PI, pain interference; PROMIS, Patient-Reported Outcomes Measurement Information System; SCB, substantial clinical benefit.
Results of the comparisons between patients who did and did not achieve MCID, PASS, and SCB for PROMIS-PI are shown in Table 5, and results of the multivariate binary logistic regressions are provided in Table 4. Patients achieving MCID had higher (worse) preoperative PROMIS-PI scores and a lower percentage of patients had chronic pain (>2 years) preoperatively. Preoperative chronic pain was a negative predictor of MCID achievement, whereas higher (worse) preoperative PROMIS-PI scores were a positive predictor on multivariate analysis. A lower percentage of patients achieving PASS had a history of past orthopaedic surgery than those who did not achieve PASS, and history of past orthopaedic surgery remained a significant negative predictor of PASS achievement in multivariate regression. For SCB, the following trended toward significance: there was a lower percentage of past orthopaedic surgery and psychiatric history in those patients who achieved SCB compared with those who did not.
Comparison of Patients Who Achieved and Did Not Achieve CSOs for PROMIS-PI a
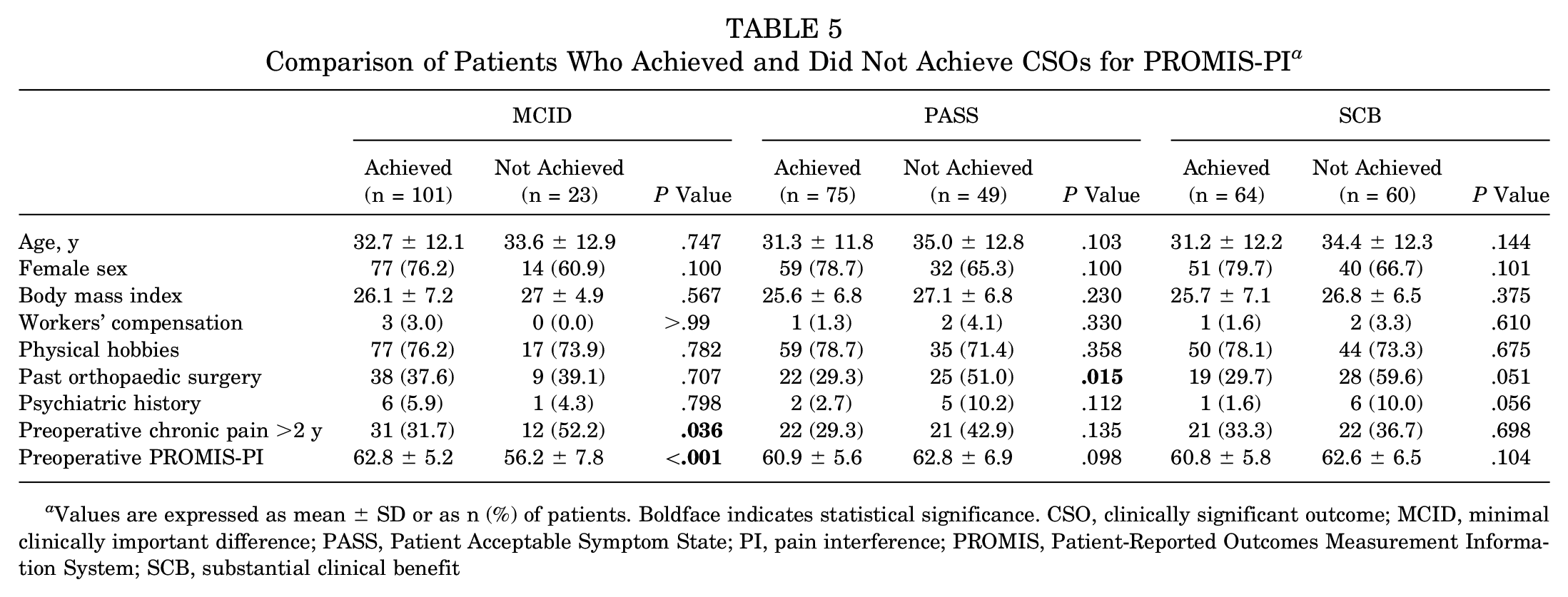
Values are expressed as mean ± SD or as n (%) of patients. Boldface indicates statistical significance. CSO, clinically significant outcome; MCID, minimal clinically important difference; PASS, Patient Acceptable Symptom State; PI, pain interference; PROMIS, Patient-Reported Outcomes Measurement Information System; SCB, substantial clinical benefit
Discussion
In the present study, we defined the MCID, PASS, and SCB for the PROMIS PF and PI CAT for patients 1 year after hip arthroscopy for FAIS. The threshold scores required to achieve MCID, PASS, and SCB, respectively, were as follows: PROMIS-PI (–3.1, 53.7, 51.9); PROMIS-PF (3.3, 47.0, 49.9); HOS-ADL (8.5, 87.1, 90.4); HOS-SS (10.5, 73.6, 77.9); mHHS (7.5, 75.9, 80.3); and iHOT-12 (8.8, 64.1, 73.6). With regard to any legacy PROMs, 87.1%, 76.6%, and 71.8% reached MCID, PASS, and SCB, respectively, at 1 year after surgery. When using either PROMIS-PF or PROMIS-PI, 89.0%, 71.8%, and 62.1% of the cohort reached MCID, PASS, and SCB, respectively. Patients more likely to achieve CSO as evaluated by PROMIS-PF were those with younger age, lower BMI, and higher (better) preoperative PROMIS-PF score. Patients were more likely to achieve CSO via PROMIS-PI if they had higher (worse) preoperative score, shorter history of preoperative pain, and less history of previous orthopaedic surgery. The MCID, PASS, and SCB of the legacy PROMs in this study were in agreement with previous literature on this topic. 29
PROMIS scores are being increasingly used in the medical and orthopaedic field to attempt to negate the floor and ceiling effects of more traditional legacy PROMs. The PROMIS questionnaires were developed to be adaptive, giving patients questions more relevant to their disease state and tailoring the line of questioning based on previous responses. 36 For instance, when a legacy PROM such as the HOS-SS is used, patients who do not participate in rigorous athletic activities will already be at a disadvantage, giving a ceiling to the maximum score they can achieve and potentially skewing results based on the patient population being treated. PROMIS scores attempt to negate this effect. PROMIS has been validated for a number of orthopaedic and other conditions with respect to its ability to outperform legacy PROMs.6,8,23 Our study showed that more patients reached MCID via PROMIS metrics than legacy PROMs (89% vs 87.1%); however, patients achieved PASS (71.8% vs 76.6%) and SCB (62.1% vs 71.8%) at lower rates with PROMIS. This may indicate that PROMIS metrics are less responsive than legacy PROMs. Additionally, it is possible that patients had not yet reached maximal improvement at 1 year after surgery. Nwachukwu et al 29 showed that the greatest proportion of patients achieved MCID, PASS, and SCB at 2 years postoperatively when using legacy PROMs.
PROMIS has been evaluated in other areas of medicine for its validity compared with extremity-specific PROMs. Suriani et al 37 correlated the PROMIS Global-10 with legacy shoulder PROMs including the American Shoulder and Elbow Surgeons (ASES) score, Single Assessment Numeric Evaluation (SANE), and Western Ontario Shoulder Instability Index (WOSI) in the assessment of 175 patients with shoulder instability. The PROMIS Global-10 was developed to be a comprehensive instrument for the evaluation of mental and physical health. Despite this, Suriani et al showed that this instrument correlated with only the ASES, having poor correlation with the SANE and WOSI, leading the authors to conclude that the PROMIS Global-10 was unreliable in assessing patients with shoulder instability. In a population of patients with rotator cuff disease, Beckmann et al 6 showed that the PROMIS-PF CAT compared well with the ASES score and Simple Shoulder Test (SST) and required fewer questions to complete, decreasing the burden on patients. The PROMIS-PF CAT also had improved reliability over the ASES score and a lower rate of floor effect compared with the SST. 6 Brodke et al 8 reported that the PROMIS-PF CAT outperformed the Oswestry Disability Index Version 2.0 and 36-Item Short Form Health Survey Physical Function Domain in patients with spinal conditions who had back or leg pain.
With regard to patients undergoing hip arthroscopy, Childs et al 13 recently demonstrated that the PROMIS-PF CAT and PROMIS-PI correlated well with legacy PROMs such as VAS, HOS-ADL, HOS-SS, and mHHS up to 3 months postoperatively. The authors found that the PROMIS-PF performed better, having high correlation with legacy PROMs, whereas the PROMIS-PI had only a moderate correlation. Our study sheds some light on this by demonstrating that a history of pain had a correlation with a lower rate of CSOs via the PROMIS-PI score. This indicates that the patients’ lack of improvement may be influenced to a degree by their previous pain and not as much as by the state of their hip. Another study comparing PROMIS metrics with legacy PROMs found that although PROMIS scores did correlate, PROMIS had a lower effect size and was less responsive. Nwachukwu et al 35 retrospectively assessed 96 patients with 6-month follow-up after arthroscopic FAIS treatment who were evaluated via both PROMIS and legacy PROMs. The investigators found that the PROMIS-PF had excellent correlation with HOS-SS, very good correlation with HOS-ADL, and good correlation with iHOT-12. No floor was observed for any measure. However, the iHOT-12 was more responsive than PROMIS-PI, PROMIS-PF, HOS-ADL, and HOS-SS. The PROMIS-PF was overall the least responsive when compared with legacy PROMs. Although PROMIS was less responsive than hip-specific legacy PROMs, Nwachukwu et al 35 demonstrated that the Cohen d values for PROMIS-PF and PROMIS-PI were 0.94 and 0.96, respectively, when comparing preoperative and 6-month scores. A Cohen d≥ 0.8 is considered large and visible to the naked eye. 39 Therefore, PROMIS outcome measures are suitable to detect change in patients undergoing hip arthroscopy. Although PROMIS may correlate with hip-specific metrics, it is not as responsive, which may limit its ability to replace legacy metrics in their present form.
Given that PROMIS scores should be used as an adjunct to legacy hip PROMs, it is important to understand risk factors that may correlate with better or worse PROMIS scores. The present study demonstrated that younger patients, those with lower BMI, and those with higher preoperative PROMIS-PF scores were more likely to achieve CSOs as evaluated by multivariate regression. With regard to PROMIS-PI, higher (worse) preoperative score as well as chronic preoperative pain for >2 years and history of orthopaedic surgery correlated with inability to achieve CSO. These results are in agreement with the findings reported by Basques et al, 4 who demonstrated that patients with symptoms for >2 years before hip arthroscopy had worse outcomes and were less likely to achieve CSO. The current study is the first to look at a large cohort of patients undergoing hip arthroscopy for the treatment of FAIS to define the MCID, PASS, and SCB of PROMIS scores. Through better understanding of the true clinical improvement in these metrics, patient-reported outcomes data can be collected in a quicker and more reliable fashion. Further work is needed in this area to see how the defined values change with time, as has been demonstrated with regard to the legacy PROMs. 13
Limitations
The present study is not without limitations. The major limitation in this study is the limited follow-up of 1 year postoperatively. Although we can support the use of PROMIS and how it correlates with legacy PROMs over a 1-year period, we are unable to predict further outcomes. Additionally, PROMIS-PF does not contain hip-specific questions, and therefore patients with concomitant orthopaedic problems may experience a loss of function that affects scores. However, our outcome collection software instructs patients to complete the surveys with regard to their operative hip. The majority of our patients were female, which may not be representative of other practices. However, male and female patients have been shown to achieve clinically significant outcomes at similar rates after hip arthroscopy. 16 Next, this was a single-surgeon series and all surgeries were performed by a high-volume hip arthroscopist, which may limit generalization. Last, this study may be limited by its sample size as well as its nonrandomized, retrospective study design.
Conclusion
Our study defined the MCID, PASS, and SCB for the PROMIS-PF and PROMIS-PI CAT. Clinically significant outcomes were achieved via PROMIS at a rate comparable with but slightly less than legacy hip PROMs. In addition, patients with higher preoperative PROMIS scores, younger age, and lower BMIs were more likely to achieve CSO, whereas preoperative chronic pain and history of orthopaedic surgery were negative predictors of CSO achievement. Although PROMIS may correlate with hip-specific metrics, it is not as responsive, which may limit its ability to replace legacy metrics in their present form.
Supplemental Material
sj-pdf-1-ajs-10.1177_03635465211015687 – Supplemental material for Defining Clinically Significant Improvement on the Patient-Reported Outcomes Measurement Information System Test at 1-Year Follow-up for Patients Undergoing Hip Arthroscopy for the Treatment of Femoroacetabular Impingement Syndrome
Supplemental material, sj-pdf-1-ajs-10.1177_03635465211015687 for Defining Clinically Significant Improvement on the Patient-Reported Outcomes Measurement Information System Test at 1-Year Follow-up for Patients Undergoing Hip Arthroscopy for the Treatment of Femoroacetabular Impingement Syndrome by Blake M. Bodendorfer, Steven F. DeFroda, Ian M. Clapp, Alexander Newhouse, Benedict U. Nwachukwu and Shane J. Nho in The American Journal of Sports Medicine
Footnotes
Submitted September 15, 2020; accepted February 11, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.F.D. has received education support from Medical Device Business Services and Zimmer Biomet Holdings. B.U.N. has received royalties from Remote Health; grants from Arthrex; education support from Arthrex, Smith & Nephew, and Medwest Associates; and hospitality payments from Stryker, Wright Medical, Zimmer Biomet, and Medical Device Business Services. S.J.N. has received research support from Allosource, Arthrex Inc, Athletico, DJ Orthopaedics, Linvatec, Miomed, Smith & Nephew, and Stryker; IP royalties and consulting fees from Ossur; consulting fees from Stryker; and education support from Elite Orthopedics. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.