
Abstract
Background:
Research has demonstrated that female athletes are more likely to report their sports-related concussion (SRC) symptoms compared with male athletes; however, it is unknown if these reporting behaviors correspond to immediate removal from activity in sex-comparable sports.
Purpose:
To compare the incidence of high school student-athletes removed and not removed from activity after SRC in sex-comparable sports in Michigan.
Study Design:
Descriptive epidemiology study.
Methods:
Participants included student-athletes diagnosed with SRC participating in Michigan High School Athletic Association–sponsored athletic activities (22 sex-comparable sports) between 2016 and 2019. All SRCs were recorded in the association’s Head Injury Reporting System (HIRS) by certified athletic trainers, administrators, or coaches. Removal from activity indicated that the student-athlete was removed from play at the time of an injury event. If the student-athlete reported that his or her suspected injury event occurred earlier during activity or if symptom onset was delayed, “not removed from activity” was entered into the HIRS. Incidence proportions were calculated by dividing SRCs not removed by total SRCs in each sport. Risk ratios were calculated by dividing the incidence proportions of girls not removed by boys not removed in each sport.
Results:
A total of 4418 (2773 female, 1645 male) SRCs were reported, with the most occurring in female soccer players (n = 1023). Overall, 515 girls and 243 boys were not removed from activity, resulting in incidences of 0.19 (95% CI, 0.17-0.20) and 0.15 (95% CI, 0.13-0.17), respectively. Across all sports, girls were 1.26 (95% CI, 1.09-1.45) times as likely to not be removed from activity compared with boys. Of the sports with the most SRCs—soccer, basketball, baseball/softball, and lacrosse—girls had 1.37 (95% CI, 1.09-1.72), 1.15 (95% CI, 0.89-1.47), 1.19 (95% CI, 0.77-1.84), and 1.35 (95% CI, 0.94-1.95) times the risk of not being removed, respectively.
Conclusion:
Girls were at greater risk of not being removed from activity compared with boys in sex-comparable sports. Results from this study should be incorporated into SRC education in Michigan and potentially elsewhere to inform affiliated personnel of potential sex differences and protect female student-athletes from further harm.
Sports-related concussions (SRCs) account for up to 10% of sports injuries each year, and an estimated 1.1 to 1.9 million occur annually in the pediatric population in the United States.7,18 An SRC results in a variety of clinical signs, symptoms, and impairments in neurological function that typically follow a sequential course to resolution. 32 Most SRCs in children and adolescents resolve within 1 month; however, resuming play before complete recovery may place an athlete at significant risk for serious neurological damage or future health implications. 22 In the short term, potential risks include sustaining a subsequent SRC,19-21 prolonged recovery,1,2,15 and second-impact syndrome. 3 In the long term, evidence has suggested a decline in health-related quality of life.33,39
As SRC awareness has increased, timely reporting and immediate removal from play have become focal points of proper injury management. In 2009, Washington was the first state to pass legislation (ie, the Lystedt law) addressing the timely management of SRC. 4 Since that time, all 50 states and the District of Columbia have established SRC legislation. In addition to state laws, consensus and position statements from numerous medical organizations, including the American Academy of Pediatrics, American Medical Society for Sports Medicine, National Athletic Trainers’ Association, and the Concussion in Sport Group, have all called for the same guiding principles when an SRC is suspected: immediate removal from play, no same-day return to play, and clearance by a medical professional before returning to play.6,22,23,32
There is still limited research addressing whether athletic communities are adhering to the principles, specifically if athletes are being immediately removed from play after a suspected SRC. One reason for this dearth of evidence is that removal from play is a complex process involving recognition of a potential SRC and the decision to act on that knowledge by various parties (eg, athlete, coach, medical professional). Outside of this complicated set of behaviors, lack of removal from play may also be the result of a delayed onset in symptoms 36 and not the fault of the injured athlete or other stakeholders. In the pediatric population, Howell et al 24 found that 227 of 516 (44%) patients diagnosed with an SRC at a sports medicine clinic reported that they continued to play after their injury. Aside from that study, most of the current evidence addresses the outcomes of immediate versus delayed removal from play rather than the frequency of continued play. Elbin et al 15 examined 35 high school athletes who were immediately removed and 34 who experienced delayed removal and found that those who continued playing exhibited greater symptoms and demonstrated protracted recovery. Asken et al 2 also examined the timing of removal and found that collegiate athletes with delayed removal from play missed 5 more days on average and were 2.2 times more likely to experience prolonged recovery than were athletes who were immediately removed. However, none of these studies examined population differences, particularly based on sex.
Previous research has repeatedly demonstrated that female athletes are more likely to sustain an SRC than are male athletes in sex-comparable sports.5,8,26,27,35 In a recent study examining SRC incidence and trends in high school athletes, SRC rates were >2 times higher in girls than boys among sex-comparable sports. 26 Potential reasons associated with this sex difference include neck musculature, cerebral blood flow, hormonal regulation, and SRC reporting/disclosure.10,16,40,41 While research has demonstrated that female athletes are more likely to report their SRC symptoms compared with male athletes,4,13 it is unknown if these reporting behaviors correspond with immediate removal from activity in sex-comparable sports. Zynda et al 42 examined a population of 87 youth soccer players and found that girls were 5 times more likely to continue playing after a suspected SRC compared with boys. However, previous research has been limited by small sample size, and no research has been done to examine sex differences in other sex-comparable sports. Therefore, the purpose of this study was to compare the incidence of high school student-athletes removed and not removed from activity after SRC in sex-comparable sports in the state of Michigan. We hypothesized that boys would be removed from activity more than would girls in sex-comparable sports.
Methods
The institutional review board of record approved this study as exempt because of deidentified data.
Research Design, Schools, and Participants
This was a descriptive epidemiology study using data obtained from the Michigan High School Athletic Association (MHSAA) Head Injury Reporting System (HIRS). The MHSAA HIRS was established in the 2015-2016 school year to provide data on the frequency and severity of head injuries incurred during interscholastic athletic events. Current MHSAA SRC protocol requires all participating high schools in the state of Michigan (2015-2016, n = 755 high schools; 2016-2017, n = 751; 2017-2018, n = 750; 2018-2019, n = 747) to enter data in the HIRS; however, individual high schools set their own deadlines for reporting student-athlete and SRC data. There are 28 sports sanctioned by the MHSAA: male baseball, male and female basketball, male and female bowling, female competitive cheerleading, male and female cross-country, male 11- and 8-player football, male and female golf, female gymnastics, male ice hockey, male and female lacrosse, male and female skiing, male and female soccer, female softball, male and female swimming and diving, male and female tennis, male and female track and field, female volleyball, and male wrestling.
To date, there are 15,676 SRC cases recorded in the HIRS (male, 66.7%, n = 10,451; female, 33.3%, n = 5225). Data for this study were collected between the 2016-2017 and 2018-2019 academic years and included 9th through 12th grade student-athletes participating in the following 22 sex-comparable sports: male baseball/female softball, male and female basketball, male and female bowling, male and female cross-country, male and female golf, male and female lacrosse, male and female skiing, male and female soccer, male and female swimming and diving, male and female tennis, and male and female track and field. Data from the 2015-2016 school year were excluded from analysis because the variable “removed from activity” was not introduced into the HIRS until the 2016-2017 school year.
Data Reporting and Definitions
Operational Definition of SRC
The MHSAA Concussion Protocol and HIRS defined an SRC as an injury that (1) occurred during participation in an MHSAA-sanctioned sport that provided a postseason tournament; (2) occurred during an in-season practice, scrimmage, or game (including preseason); and (3) required the student-athlete to be withheld from activity after exhibiting signs, symptoms, or behaviors consistent with an SRC (eg, loss of consciousness, headache, dizziness, confusion, or balance problems). All SRCs were recorded in the HIRS if they met these criteria. Cases that occurred outside of MHSAA-sanctioned events (ie, gymnasium class, at home) were not included. All SRCs were recorded in the HIRS by certified athletic trainers, administrators, or coaches, as MHSAA member schools vary with respect to medical personnel available. All SRCs had to be diagnosed by one of the following health care professionals: medical doctor (MD), doctor of osteopathic medicine (DO), physician assistant (PA), or nurse practitioner (NP).
Definition of Removal From Activity
Removal from activity indicated the student-athlete was removed from play (game, scrimmage, or practice) at the time of a suspected injury event. If the student-athlete reported that his or her suspected injury event occurred earlier during activity or if symptoms did not arise until after activity ended, “not removed from activity” was entered into the HIRS. Lack of removal does not indicate mismanagement at the time of the event but that the injury was not reported to any school personnel, whether the result of a decision made by the athlete or a lack of symptoms at that time. Although delayed symptom onset may have been a reason for nondisclosure and nonremoval, a mechanism of injury was present (ie, direct impact to head, neck, or chest or whiplash) that eventually led to an SRC diagnosis by one of the aforementioned providers. Symptoms may not present until 24 to 48 hours after the suspected SRC in the pediatric population. 36
Procedures
Data collection procedures have been previously described in other studies.5,11 The MHSAA Concussion Protocol requires school personnel to submit an online initial and subsequent follow-up report for each SRC. In addition to the SRC information, data recorders were required to submit total student-athlete participation per sport as well as descriptive (ie, sex, grade, level, sport) data. The SRC injury event included date of injury, game or practice, time of injury during game or practice, type of protective equipment worn, cause of the injury (ie, person-to-person contact, person-to-object contact), surface type, initial examiner, and removal from play decision. Each student-athlete had a 7-digit identification number to ensure the data remained anonymous. If a student-athlete incurred a second SRC in either the same sport or a different sport, each SRC was recorded as a separate injury. Athletic trainers were the primary data recorders for the HIRS; however, if an athletic trainer was not employed by a high school, coaches and school officials were required to record data in the HIRS.
MHSAA staff members monitored the information entered into the HIRS daily to identify any errors. If an error or anomaly was identified, the MHSAA staff contacted schools requesting edits. The MHSAA also required high schools to report if they did not have an SRC to be entered into the HIRS. The MHSAA deemed SRC data collection complete when no less than 99% of all injury reports were received. Only MHSAA staff members were authorized to edit SRC reports once submitted.
Statistical Analysis
Descriptive statistics were reported as frequencies with percentages. Incidence proportions (IPs) were calculated by dividing the number of SRCs of athletes not removed by the total number of SRCs in each sport. Risk ratios (RRs) were used to compare the risk of not being removed from activity between female and male athletes in sex-comparable sports. The RRs were calculated by dividing the IP of girls not removed by boys not removed in each sport. 28 All RRs with a confidence interval (CI) that overlapped 1.00 did not meet clinical significance, and the differences were considered minimal. Sex-comparable sports with a frequency of SRC cases <50 are reported in Table 3 but are not described in the Results section. Statistical analyses were performed using IBM SPSS Statistics Version 25.0 (IBM Corp).
Results
The total number of SRCs and whether those athletes were removed from activity between 2016 and 2019 are represented in Figure 1. A total of 4418 (2773 female, 1645 male) SRCs were reported across sex-comparable sports, with the most occurring in female soccer (n = 1023), female basketball (n = 1010), and male soccer (n = 578). Table 1 presents the characteristics of student-athletes throughout the 3 athletic seasons, and Table 2 presents the frequency of SRCs in athletes removed and not removed from activity by sport.
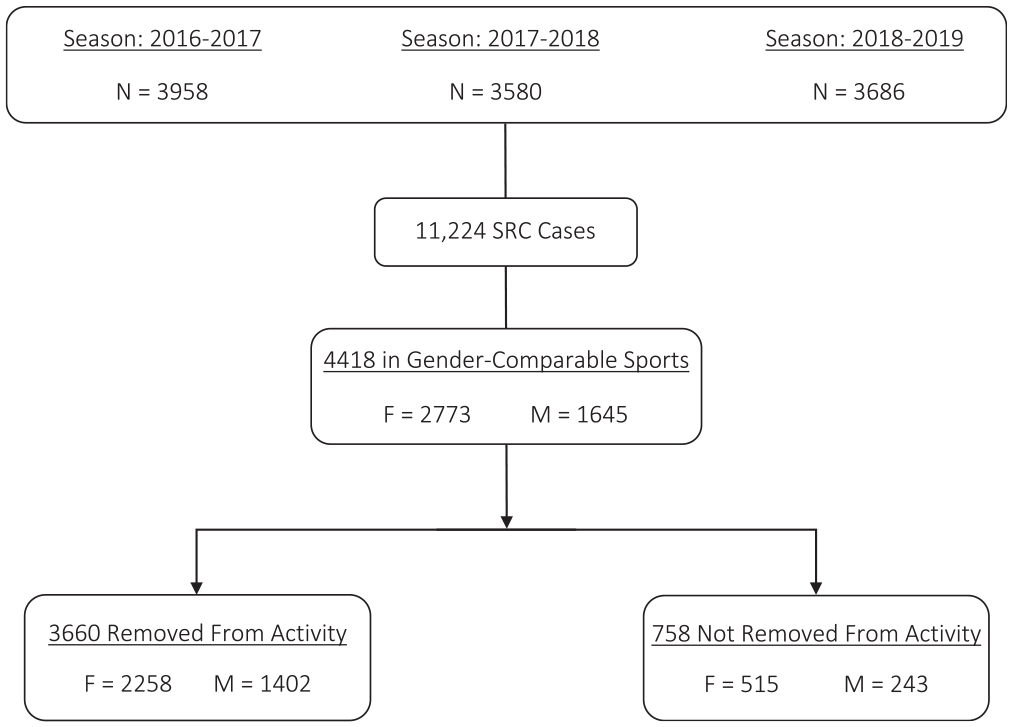
Sports-related concussion (SRC) cases recorded in the Head Injury Reporting System during the 2016-2017, 2017-2018, and 2018-2019 athletic seasons. F, female; M, male.
Characteristics of Student-Athletes in the HIRS in Sex-Comparable Sports Between the 2016-2017 and 2018-2019 Seasons a

HIRS, Head Injury Reporting System; SRC, sports-related concussion.
Frequencies of SRCs in Sex-Comparable Sports in Athletes Removed and Not Removed From Activity Between the 2016-2017 and 2018-2019 Seasons a
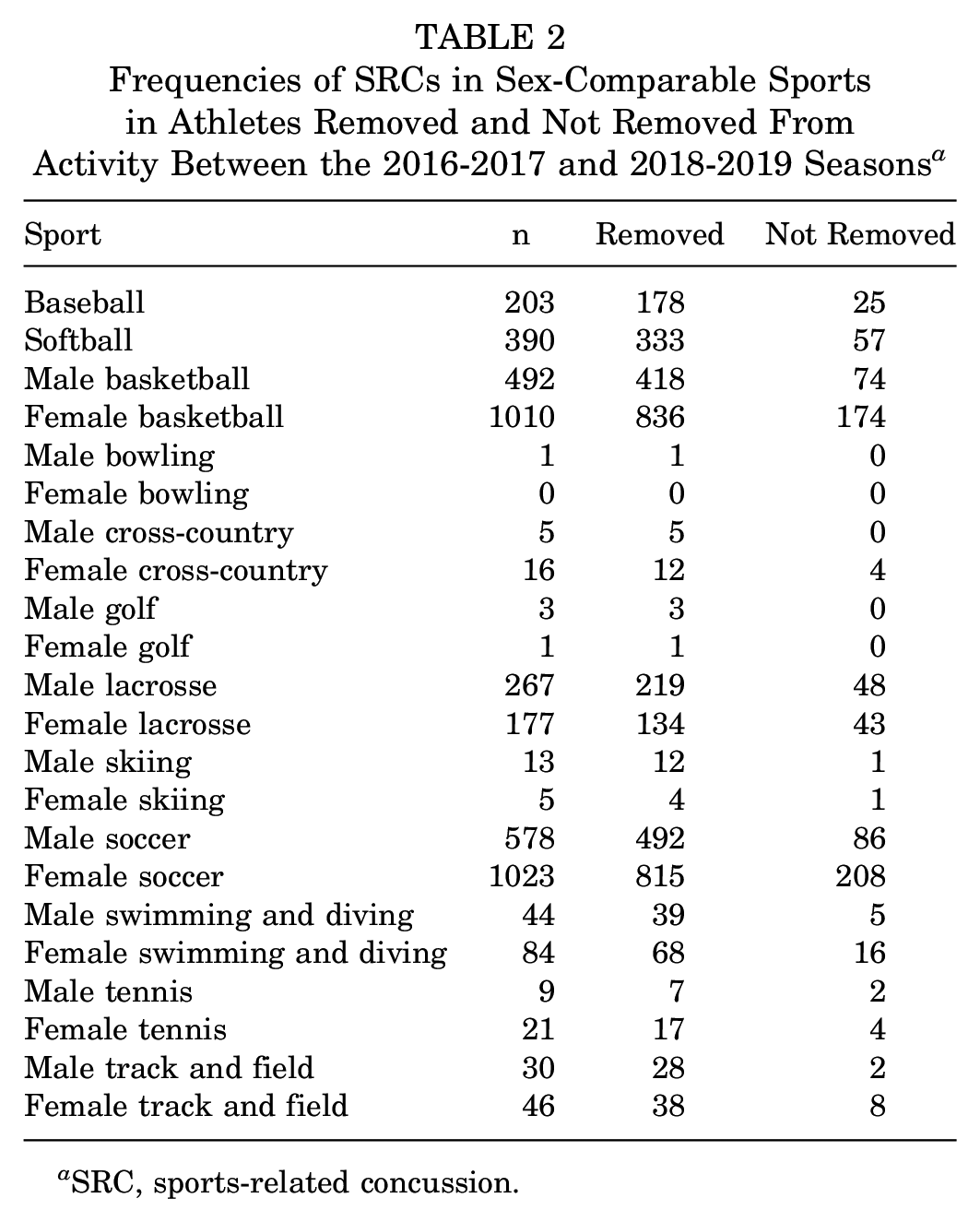
SRC, sports-related concussion.
Overall, 758 of 4418 high school student-athletes were not removed from activity, resulting in an IP of 0.17 (95% CI, 0.16-0.18). A total of 515 (68%) girls and 243 (32%) boys were not removed from activity, resulting in IPs of 0.19 (95% CI, 0.17-0.20) and 0.15 (95% CI, 0.13-0.17), respectively. Across all sports, girls were 1.26 (95% CI, 1.09-1.45) times as likely to not be removed from activity compared with boys.
Sports-Specific Analyses
Sex-comparable sports with ≥50 SRCs are described in more detail below, while all sports are presented in Table 3.
RRs for Student-Athletes Not Removed From Activity Between the 2016-2017 and 2018-2019 Seasons a
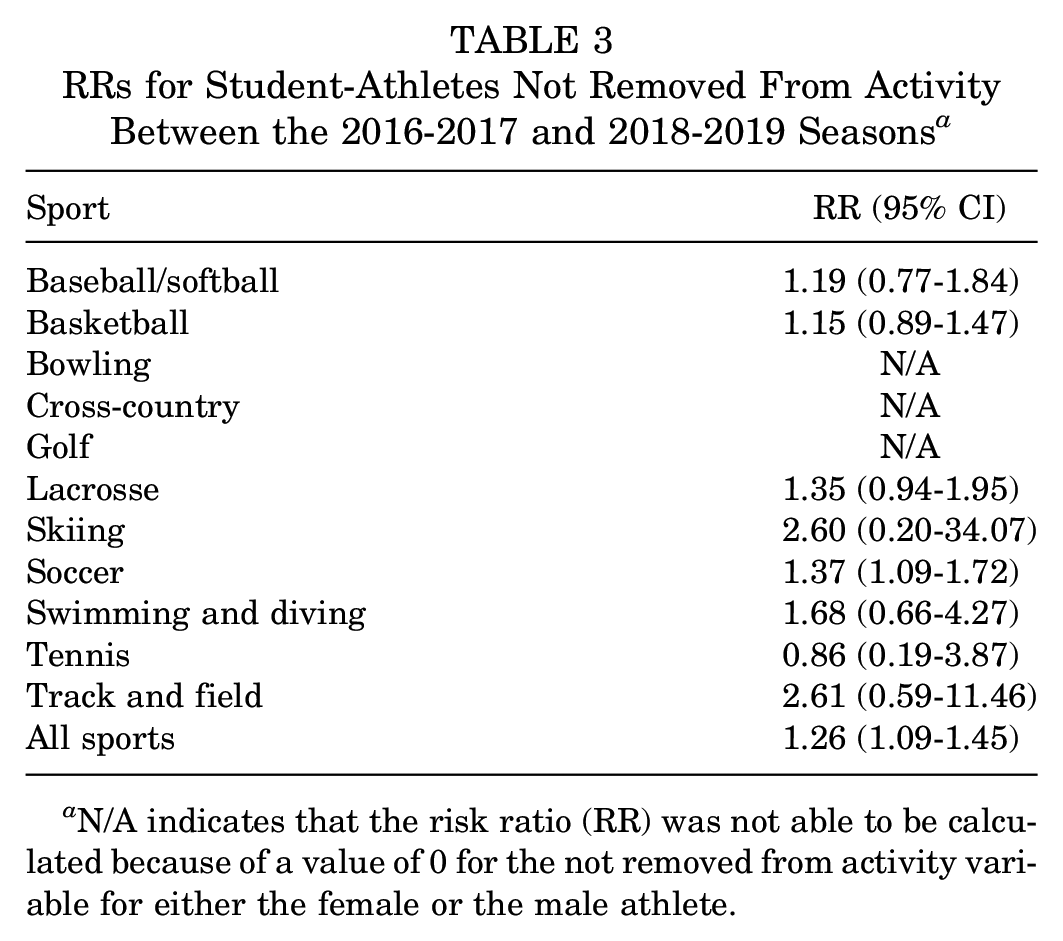
N/A indicates that the risk ratio (RR) was not able to be calculated because of a value of 0 for the not removed from activity variable for either the female or the male athlete.
Baseball/Softball
A total of 593 SRCs (not removed, 82; removed, 511) were reported in baseball and softball, with more occurring in girls (Table 2). The IP of not being removed from activity was 0.15 (95% CI, 0.11-0.18) in girls and 0.12 (95% CI, 0.08-0.17) in boys. The risk of not being removed from activity was greater in female than male athletes (RR, 1.19 [95% CI, 0.77-1.84]).
Basketball
A total of 1502 SRCs (not removed, 248; removed, 1254) were reported in male and female basketball, with more than double the number occurring in girls (Table 2). The IP of not being removed from activity was 0.17 (95% CI, 0.15-0.20) in girls and 0.15 (95% CI, 0.12-0.18) in boys. The risk of not being removed from activity was greater in female than male athletes (RR, 1.15 [95% CI, 0.89-1.47]).
Lacrosse
A total of 444 SRCs (not removed, 91; removed, 353) were reported in male and female lacrosse, with more occurring in boys (Table 2). The IP of not being removed from activity was 0.24 (95% CI, 0.18-0.30) in girls and 0.18 (95% CI, 0.13-0.23) in boys. The risk of not being removed from activity was greater in female than male athletes (RR, 1.35 [95% CI, 0.94-1.95]).
Soccer
A total of 1601 SRCs (not removed, 294; removed, 1307) were reported in male and female soccer, with almost double the number occurring in girls (Table 2). The IP of not being removed from activity was 0.20 (95% CI, 0.18-0.23) in girls and 0.15 (95% CI, 0.12-0.18) in boys. The risk of not being removed from activity was greater in female than male athletes (RR, 1.37 [95% CI, 1.09-1.72]).
Swimming and Diving
A total of 128 SRCs (not removed, 21; removed, 107) were reported in male and female swimming and diving, with nearly double occurring in girls (Table 2). The IP of not being removed from activity was 0.19 (95% CI, 0.11-0.27) in girls and 0.11 (95% CI, 0.02-0.21) in boys. The risk of not being removed from activity was greater in female than male athletes (RR, 1.68 [95% CI, 0.66-4.27]).
Track and Field
A total of 76 SRCs (not removed, 10; removed, 66) were reported in male and female track and field, with the majority occurring in girls (Table 2). The IP of not being removed from activity was 0.17 (95% CI, 0.06-0.28) in girls and 0.07 (95% CI, –0.02 to 0.16) in boys. The risk of not being removed from activity was greater in female than male athletes (RR, 2.61 [95% CI, 0.59-11.46]).
Discussion
The purpose of the current study was to compare the incidence of high school athletes removed and those not removed from activity after SRC in sex-comparable sports. The results of this study suggest that, across all sports, girls are at a greater risk of not being removed from activity compared with boys after SRC. In addition, in every individual sex-comparable sport except tennis, girls were at a greater risk of not being removed from activity compared with boys after SRC. However, soccer was the only individual sport to demonstrate clinically significant CIs.
Little research has examined removal from activity in sex-comparable high school sports. The current study found that female high school athletes were less likely to be removed from activity compared with male athletes, although this lack of removal may not have always been the result of nondisclosure. These results were similar to those of Zynda and colleagues, 42 who reported that 51.7% of high school female soccer players continued to play the same day as their injury. Furthermore, high school female soccer players in that sample were 5 times more likely to continue to play after SRC compared with male players. 42 As soccer was the only individual sport with a clinically significant CI in the present study, taken together, the results from these studies may indicate that sex differences in removal from play are most prominent in soccer. In several other studies examining removal from play, no sex differences were found; however, these did not focus on sex-comparable sports.1,2,15,24 A majority of epidemiology research has suggested that high school girls have a higher incidence of SRC than do boys, and this is consistent in research that focuses on sex-comparable sports.5,18,31,35,38 This higher SRC incidence in sex-comparable sports and the emerging data on continued play in girls are cause for concern.
Disclosure of SRC to a person of authority (ie, athletic trainer, coach, parent) involves a complex set of behaviors that have been shown to be influenced by sex.29,30,34,40 Based on existing evidence, it is widely accepted that high school girls are more likely to disclose SRC compared with boys. For example, Wallace and colleagues 40 reported that high school girls were more knowledgeable of SRC symptoms and were 4 to 11 times more likely to report symptoms to an authoritative figure compared with high school boys. Similarly, Miyashita et al 34 reported that female high school athletes were more likely to report a concussive incident especially if they had received a form of SRC education. The greater presence of positive disclosure behaviors in high school girls should suggest that female athletes are less likely to continue to play after SRC, especially when taking into consideration that adolescent boys and girls appear to have delayed symptom onset similarly. 36 However, the current study revealed that girls are at a greater risk of continuing to play after SRC, suggesting that there may be contextual factors, such as access to health care and the nature of the sport, inhibiting the immediate disclosure of SRC in high school female athletes.
It has been reported that girls are more comfortable seeking medical attention and are more satisfied with medical services when the practitioner is of the same sex.12,14 Drummond and colleagues 14 found that female collegiate athletes were more comfortable reporting and receiving medical attention for upper body injuries and psychological issues from same-sex athletic trainers. Furthermore, a national study conducted in 2009 reported that men are more likely to be employed as an athletic trainer in the secondary school setting than are women. 25 Therefore, it is possible that the high school girls may be more at risk of nonremoval in sex-comparable sports regardless of their SRC disclosure behaviors because they are uncomfortable reporting their SRC to a male athletic trainer.
The sex of athletic trainers may be a factor in an athlete’s continuing to play after SRC, but the nature of sex-comparable sports and how that may affect the decision to remove oneself from play after injury may play an even larger role. As previously stated, high school girls are historically more likely to remove themselves from play immediately after the presentation of SRC symptoms because of positive disclosure behaviors.13,40 However, behaviors such as intention to report are driven by deliberative decisional processes and often are overridden during situations of high arousal and emotion (eg, sports competition) by reactive and associative processes.17,29 Participating in risk behaviors in sport (ie, play through pain and win-at-all-cost mentalities) is often rooted in traditional views of masculinity, and it is not uncommon for athletes of both sexes to conform to masculine roles during competition. Kroshus et al 29 found that male and female collegiate athletes conform to these masculine roles similarly, and those who value winning may view playing through injury as more intrinsically motivating. This is supported by previous literature documenting that athletes did not report SRC because they did not want their coach or teammates to think they were weak, did not want to lose playing time, and did not want to let their team down.9,37,40 Given that the current study examined sex-comparable sports, an argument can be made that the potential for direct comparisons between the success of male and female teams may promote a greater conformity to masculine roles in girls. This may lead to the promotion of risk behaviors over their usual positive reporting behaviors in high-intensity athletic situations, resulting in greater female nonremoval.
This study has limitations that should be considered when interpreting the findings. While the risk ratio was greater for girls in all individual sports except tennis, the CIs did not meet clinical significance in any sport except for soccer; therefore, the differences were considered minimal. In addition, it is unknown which cases included in our results came from high schools that did not have licensed health care professionals available at sponsored athletic events. Nonmedical personnel may lack the training necessary to appropriately recognize SRCs, which could have affected decisions regarding timely removal from play. Delayed symptom onset, which may occur after SRC in the pediatric population, 36 may have contributed to differences in reporting and removal from play as well. This results in 2 potential populations within the “not removed” group: those who did not have symptoms at the time of their injury and those who did but were not removed. While the sample size was large overall, it was limited to high school student-athletes in Michigan, the complexity of the SRCs was unknown, and some sports (eg, soccer, basketball) were overrepresented. As such, the results may not be generalizable to other levels of participation and all sex-comparable sports.
Conclusion
This is the only study, to date, examining sex differences in removal from activity after SRC across sex-comparable sports. The results from this study revealed that girls are at greater risk of not being removed from activity after an SRC compared with boys across all sex-comparable sports in the state of Michigan. However, soccer was the only individual sport to demonstrate a clinically significant CI, which should be considered when interpreting the findings. These findings do not reflect those in previous literature stating that girls are more likely to report their SRC, which highlights the need for further research in this area. Future studies should examine each individual sex-comparable sport to determine if these findings persist and why girls are at greater risk of not being removed, as the reasons currently are unknown and complex. The results from this study should be incorporated into SRC education in Michigan in an effort to inform affiliated personnel of potential sex differences and protect female student-athletes from further harm.
Footnotes
Submitted September 16, 2020; accepted March 10, 2021.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. This project was supported by the Michigan High School Athletic Association (MHSAA). The content of this report is solely the responsibility of the authors and does not necessarily reflect the views of the MHSAA. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.