
Abstract
Background:
Muscle strain injury leads to a high risk of recurrent injury in sports and can cause long-term symptoms such as weakness and pain. Scar tissue formation after strain injuries has been described, yet what ultrastructural changes might occur in the chronic phase of this injury have not. It is also unknown if persistent symptoms and morphological abnormalities of the tissue can be mitigated by strength training.
Purpose:
To investigate if heavy resistance training improves symptoms and structural abnormalities after strain injuries.
Study Design:
Randomized controlled trial; Level of evidence, 1.
Methods:
A total of 30 participants with long-term weakness and/or pain after a strain injury of the thigh or calf muscles were randomized to eccentric heavy resistance training of the injured region or control exercises of the back and abdominal muscle. Isokinetic (hamstring) or isometric (calf) muscle strength was determined, muscle cross-sectional area measured, and pain and function evaluated. Scar tissue ultrastructure was determined from biopsy specimens taken from the injured area before and after the training intervention.
Results:
Heavy resistance training over 3 months improved pain and function, normalized muscle strength deficits, and increased muscle cross-sectional area in the previously injured region. No systematic effect of training was found upon pathologic infiltration of fat and blood vessels into the previously injured area. Control exercises had no effect on strength, cross-sectional area, or scar tissue but a positive effect on patient-related outcome measures, such as pain and functional scores.
Conclusion:
Short-term strength training can improve sequelae symptoms and optimize muscle function even many years after a strain injury, but it does not seem to influence the overall structural abnormalities of the area with scar tissue.
Registration:
NCT02152098 (ClinicalTrials.gov identifier).
Muscle strain injuries are one of the most common sports injuries, and the recurrence rate is substantial in competitive and amateur athletes.16,31,49 Previous studies have reported an extended repair process after injury,3,4 with the development of muscle atrophy4,55 and fibrosis.50,55 A direct identification of the scar tissue has, however, not been performed. Furthermore, some studies suggest that sports-active persons are left with persistent functional deficits, such as reduced muscle strength (especially of the eccentric component),10,52 muscle fatigue, and changes in the muscular activation after a hamstring strain injury.9,38 Whether these functional deficits can be restored has not been examined.
Muscle strain injuries occur predominantly at the myotendinous junction, 60 which is a highly organized structure connecting the cytoskeleton at the muscular side to the extracellular matrix on the connective tissue part.58,59 The myotendinous junction is configured to increase the contact area between the muscle and the connective tissue to significantly reduce the stress at the interface between the tissues. Incomplete repair at the myotendinous junction after a strain injury might demonstrate a weak spot and could partly explain the high proportion of reinjury at the same site as the index injury. Whether the specific architecture of the myotendinous junction is fully reestablished and functional after a strain injury is not understood and has never been examined in humans. Fibrotic scar formation as measured by magnetic resonance imaging (MRI) has been reported,51,55 but the actual composition of this scar and whether it is coupled to clinical symptoms remains unknown. 63 On a functional level, scar tissue displays altered mechanical properties as compared with intact tissue,12,13 including modified muscle in-series stiffness. 56 It is unknown if mechanical properties can be normalized by strength training.
Several structural impairments occur with experimental focal muscle damage, such as myofibrillar disruptions, Z-line streaming, and hypercontracted muscle fibers.11,14,35 These structural changes of the myofibers are short-term and restored in a span of weeks.14,39,40,47 In contrast, the remodeling of the connective tissue after this type of muscle damage requires a protracted time, 40 and injuries to connective tissue–rich structures are long lasting and structural restoration often incomplete.17,41 Heavy resistance training (HRT), particularly eccentric muscle contraction, has been shown to be effective in preventing first-time and recurrent hamstring strain injury,26,48 but the underlying mechanisms are not known. It has never been established that HRT induces positive tissue adaptations after a strain injury, especially in relation to scar tissue remodeling.
Our goal with this study was to investigate the effect of HRT on pain, muscle strength, and muscle cross-sectional area (CSA) in participants who experience chronic symptoms after a previous strain injury. Next, we aimed to characterize the scar tissue and register potential positive ultrastructural changes after HRT. Our hypotheses were as follows: (1) HRT would lead to reduced clinical symptoms, improved pain and function scores, and an increase in muscle CSA. (2) Scar tissue would be characterized by a disorganized structure of connective tissue, and HRT would lead to a local remodeling.
Methods
Study Design, Participants, and Intervention
This study investigates chronic muscle strain injuries. As it was registered with a separate but concurrent study,4,5 there was no specific a priori outcome. The present study was designed as a 2-arm randomized controlled trial using a computer-generated minimization randomization procedure for which the principal investigator (M.L.B.) was responsible. Several secondary outcomes were prespecified: magnetic resonance images determining muscle CSA, comparison of strength measurements between the injured and healthy (contralateral) muscle groups, and evaluation of structural tissue changes based on biopsy specimens from the injured muscle connective tissue interface before and after intervention. Minimization was based on muscle group and sex, and recruitment lasted from May 2014 to May 2016 (Figure 1). Amateur athletes were included when they fulfilled the inclusion criteria: a strain injury in the calf or thigh muscles at least 6 months previously, persistent pain, and/or functional deficits after injury (eg, weakness). An ultrasound scan showing a clear hyper- or hypoechoic area was an additional inclusion criterion (see Appendix Table A1, available in the online version of this article). All patients gave informed consent, and the study was approved by the local ethical committee (reference H-1-2014-005; approved March 21, 2014) and registered under ClinicalTrials.gov (NCT02152098). Participants were randomized to HRT or CORE training by the principal investigator.
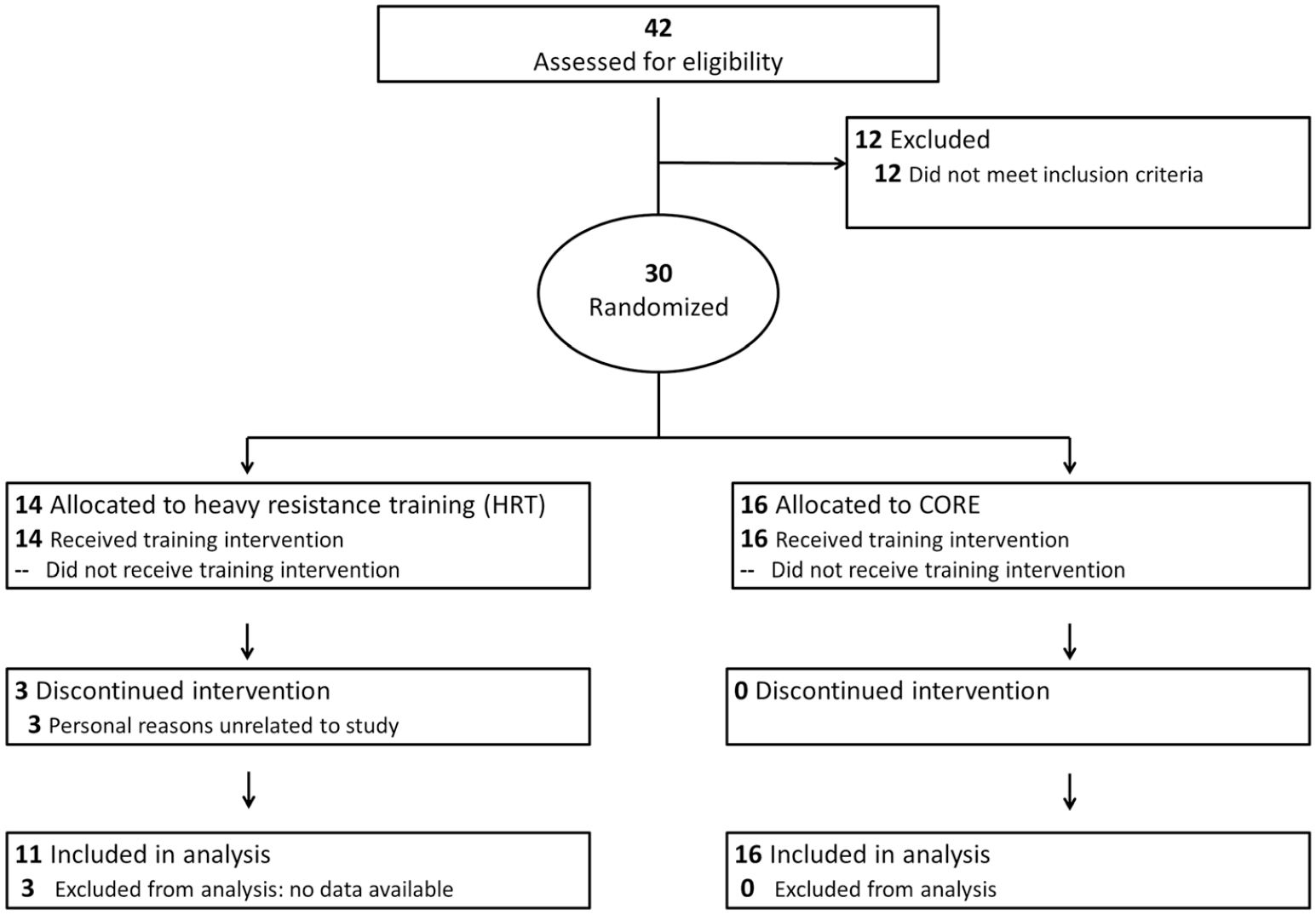
Flowchart of enrollment, participant allocation, and analysis. CORE, control exercises of the back and abdominal muscles.
Exercise Training Program
The HRT program focused on eccentric contractions with gradual increase in resistance and decrease in volume. The CORE training involved strengthening the back and abdominal muscles, omitting any exercises of the thigh or calf muscles. Table 1 gives a short overview of the exercises and progression, and the Appendix (available online) provides details of the different training programs.
Overview of Training Programs: HRT (Hamstrings and Calf) and CORE a
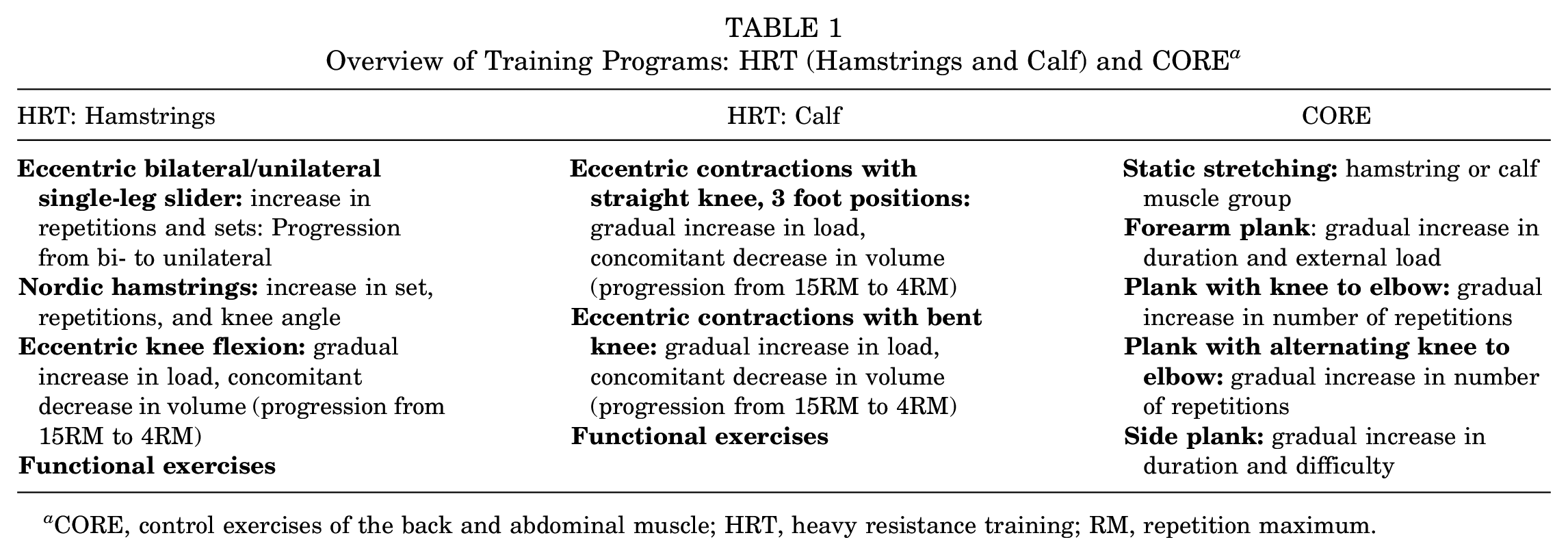
CORE, control exercises of the back and abdominal muscle; HRT, heavy resistance training; RM, repetition maximum.
MRI and Analysis
MRI of the injured thigh or calf was performed before and after intervention, and the second scan was obtained at least 48 hours after the final training bout. All scans were performed using a 1.5-T system (Ingenia dStream; Philips Healthcare), and all participants were scanned in the supine position using a 32-channel torso coil. Using Horos Software (Horos Project), a blinded investigator (M.H.H.) quantified muscle CSA by manual segmentation. It should be noted that muscle CSA was assessed in the involved muscle groups, not the noninvolved, owing to limited scanning time. The exact MRI protocol and details about image analysis are available in the Appendix (available online).
Tests of Muscle Function
All strength measurements were conducted before and after intervention and preceded by warm-up for 10 minutes on a Monark cycle ergometer at moderate intensity. Participants with an injury in the thigh muscles performed isokinetic strength testing using a KinCom dynamometer (Chattecx Corp). Participants were seated and reclined 10°, and their hips and thighs were firmly strapped to the seat of the dynamometer. The axis of rotation of the dynamometer lever arm was visually aligned with the lateral femoral condyle, and the lower leg was attached to the lever arm of the dynamometer 5 cm above the lateral malleolus. For each contraction mode, 2 preconditioning trials were performed, followed by 3 maximal contractions at an angular velocity of 60 deg/sec with a range of motion between 10° and 90° (0° indicating full knee extension). Recorded torques were corrected for the weight of the lower leg distal to the knee joint. The trial with the highest peak torque was used for data analysis. For statistical analysis, just the participants with a hamstring injury were included, given the low number of rectus femoris injuries.
Participants with a calf muscle injury performed isometric strength tests using the Good Strength device (Version 3.14 Bluetooth; Metitur Ltd), 7 as the KinCom dynamometer was not equipped to test calf muscles. Participants were seated with hips flexed at 90°, knees fixed at 0°, and ankle joints in a 90° position, and the force transducer was placed beneath the metatarsal bones. Three measurements were made at each time point, and the trial with the highest peak was used for data analysis. The passive force against the transducer was subtracted from the active isometric maximal voluntary contraction (MVC).
Additionally, participants performed a heel-rise test (MuscleLab; Ergotest Technology), which tests the ability of the calf muscles to repeatedly perform a unilateral heel rise in a given speed. For the heel-rise test, the MuscleLab system (Ergotest Technology) was used, and the participants were instructed to rise as high as possible with each heel and then lower it to the starting position. Concentric and eccentric phases each lasted 1 second (metronome guided). The distance was measured by a string attached to the participant’s heel and connected to a sensor. Participants were asked to perform as many heel rises as possible. The test was terminated when the participant was unable to raise the heel >5 cm at the correct pace.
Scar Tissue Sampling
Biopsy specimens from the scar tissue were taken under ultrasound guidance after identification of a clear hypo- or hyperechoic area. The medical doctors (J.L.O., M.H.-K.) responsible for biopsy sampling were blinded to the intervention groups. Samples were taken when pathological changes on the scan agreed with the site of the previous muscle strain injury where the participants felt pain or discomfort. After sterilization, the sample site was prepared with local anesthetics (lidocaine, 1%), and samples were taken with the Bard Magnum Biopsy Instrument (C.R. Bard, Inc) using a 14-g needle 45 under ultrasound guidance. One part of the biopsy specimen was immediately placed in 1 mL of buffered 10% formalin for histology, and a smaller part was fixed in 2% glutaraldehyde for electron microscopy. For detailed protocols, see the Appendix (available online).
Questionnaires to Assess Patient-Reported Outcome Measures
The questionnaire to assess subjective function scores, pain, and symptoms of the injured muscle (Hamstring Outcome Score) has been validated 18 and translated to Danish. It consists of 5 categories—symptoms, soreness, pain, function and activities, and quality of life/sports performance—and each category is scored separately. The total score is achieved by calculating the mean of the 5 categories in percentage of the maximal score. The questionnaire was modified for calf injuries to be specific to this region. 4 Participants were asked to complete the questionnaire before and after intervention.
Statistics
Two-way repeated measures analysis of variance (ANOVA) with post hoc Tukey tests was used to detect statistical differences between groups and time points. The ratio of the muscle CSA between the before-and-after time points was tested using 2-way ANOVA with the factors group and position (distal, middle, or proximal site). The MVC was tested as the ratio between the injured and healthy legs with 2-way repeated measures ANOVA with the factors group and time point. The differences between the injured and healthy legs were analyzed by paired t tests for each time point. The 5 items in the injury screening questionnaire were tested with 2-way repeated measures ANOVA with the factors group and time point. The difference between questionnaire scores for the injured and healthy legs was tested with the Wilcoxon signed-rank test for each time point. The level of significance was set at P < .05. Effect sizes are reported as Cohen d = (M1–M2)/s, where M1–M2 is the difference between the group means and s is the pooled standard deviation of the 2 groups. An effect size ≥0.2 to <0.5 is considered to have small clinical relevance; ≥0.5 to <0.8, medium clinical relevance, ≥0.8 to <1.3, large clinical relevance; and ≥1.3, very large. 57 As this article presents data from a substudy of a clinical trial investigating acute and chronic muscle strain injuries, sample size calculation was not performed for this study arm but targeted for the primary outcome of the acute study arm.
Results
Patient Characteristics
There were no differences in baseline characteristics between the intervention groups for sex composition (HRT, 73% male; CORE, 75% male; P = .99), age (HRT, 36 ± 11 years [mean ± SD]; CORE, 37 ± 10 years; P = .88), or injury duration (HRT, 43 ± 38 months; CORE, 44 ± 47 months; P = .95). All participants were injured during a sports activity ≥6 months before inclusion, and all cited chronic symptoms, the most common of which was pain in the affected region. Muscle weakness and high recurrence of strain injury during sports were frequent complaints. Participant characteristics are presented in detail in Appendix Table A2 (available online), including cause of the injury and the most common complaint at first medical examination before inclusion. There were 17 participants with hamstring injuries, 8 with calf injuries, and 2 with an injury in the rectus femoris. Data from rectus femoris injuries are included in the biopsy and patient-reported outcome measure analysis. Contraindications to biopsy sampling included proximity to a nerve (n = 6), multiple blood vessels in the area (n = 1), and allergic reaction to local anesthesia (n = 1). Two participants declined the postintervention biopsy for personal reasons, and none indicated any medical adverse effects.
Peak Strength and Function as a Result of the Intervention
The deficit in concentric hamstring MVC revealed an interaction between group and time point (P = .008). Post hoc tests showed that the MVC deficit improved in the HRT group with an increase by 23 percentage points (P = .002; Cohen d = 1.2), while there was no change in the CORE group, leading to a group difference after intervention (P = .03) (Figure 2A). Before the intervention, there was no group difference between the HRT and CORE group: concentric MVC was 17.5% lower in the injured as compared with the healthy leg in the HRT group (P = .055) and 18% lower in the injured leg in the CORE group (P = .008).
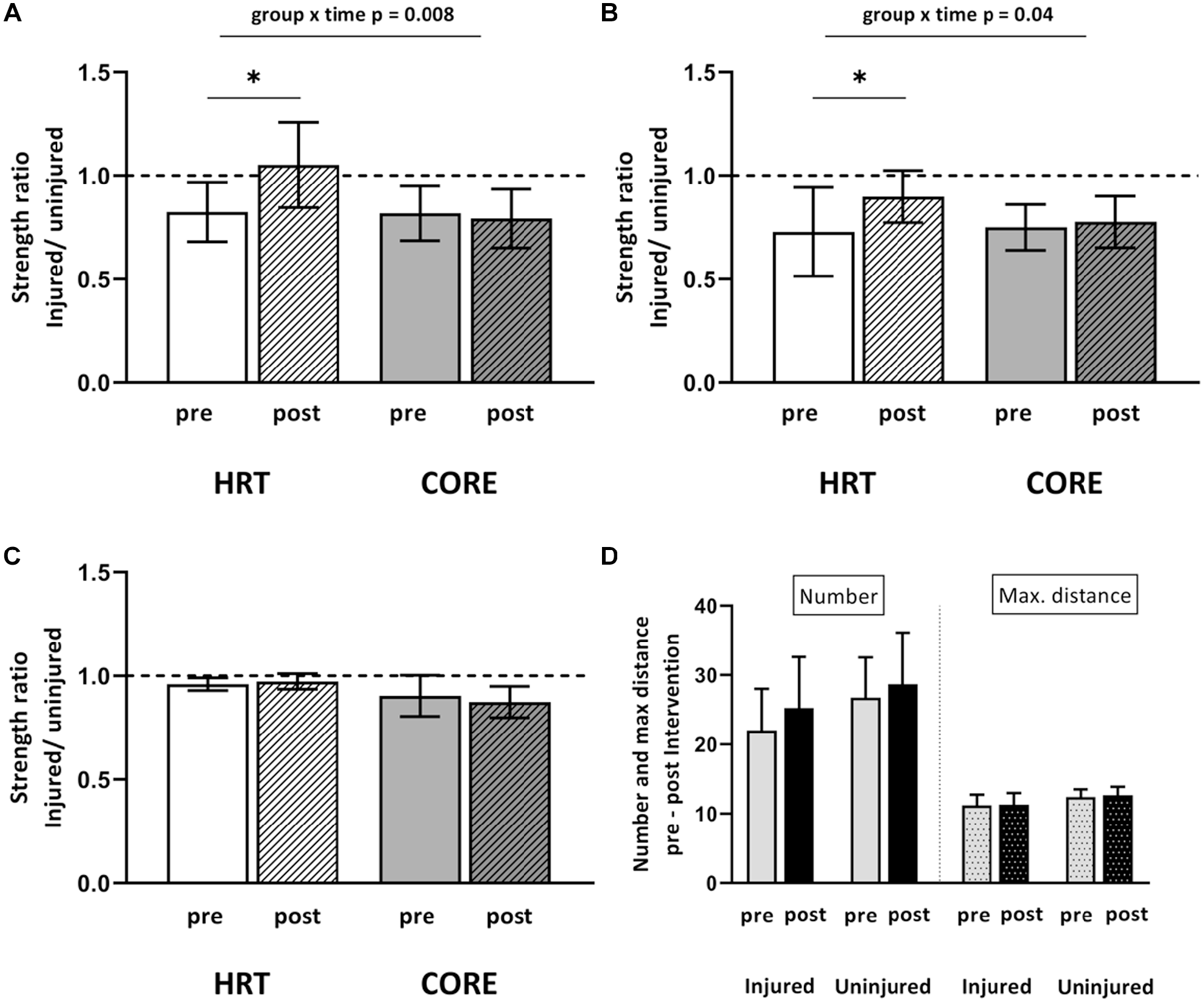
Hamstring isokinetic (A) concentric and (B) eccentric peak strength and (C) calf isometric peak strength, (D) as well as number and maximal distance of calf heel rises obtained before and after intervention (pre, post) in the HRT group (white bars) and CORE group (gray bars). (D) Data from both groups combined for number and maximal distance (in cm) of heel rises. (A-C) Data shown relative to the contralateral, healthy leg. Group × time interaction given with precise P values. *Significant increases in peak strength (P < .05). Data shown as mean ± SEM. CORE, control exercises of the back and abdominal muscle; HRT, heavy resistance training.
A similar pattern was observed for the deficit in eccentric hamstring MVC, with a group × time interaction (P = .04). Post hoc tests showed an increase in eccentric MVC after intervention in the HRT group by 17 percentage points (P = .001; Cohen d = 0.9), while there was no change in strength in the CORE group (P = .3) (Figure 2B). No group difference was observed at the start of the intervention between the groups, but there was a substantial torque deficit as compared with the healthy leg. Eccentric MVC was 27% lower in the injured as compared with healthy leg in the HRT group (P = .047) and 25% lower in the injured leg in the CORE group (P = .004).
Calf muscle strength was tested isometrically, and the deficit in isometric MVC between the injured and the healthy calf was not statistically different between the groups before or after intervention. The number and maximal distance of heel rises were not different in the injured as compared with the healthy calf either, and none of the parameters changed over time (Figure 2, C and D).
Muscle CSA
None of the hamstring muscles displayed interactions between position and group; therefore, main effects are reported in the following. For the hamstring muscles, there was a significant difference between the HRT and CORE groups after intervention in the size of the semitendinosus (P = .046). The CSA of the semitendinosus was increased by 7% after 3 months of HRT (P = .03; Cohen d = 0.6), while there was no change in CSA for the CORE group (Figure 3A). For the other 3 hamstring muscles, the CSA did not differ significantly between the groups. The biceps femoris caput brevis CSA increased significantly by 8% in the HRT group (P = .01; Cohen d = 0.7) and by 3% in CORE group (P = .04; Cohen d = 0.3) with no difference between the intervention groups (P = .3). There was no significant change in the semimembranosus CSA in either group and no significant effect on the CSA of the biceps femoris caput longum in either group. The position of the MRI was considered in the analysis, and the semimembranosus revealed a more pronounced increase at the proximal site as compared with the distal site in both groups (P = .02) with no difference between the intervention groups (P = .1).
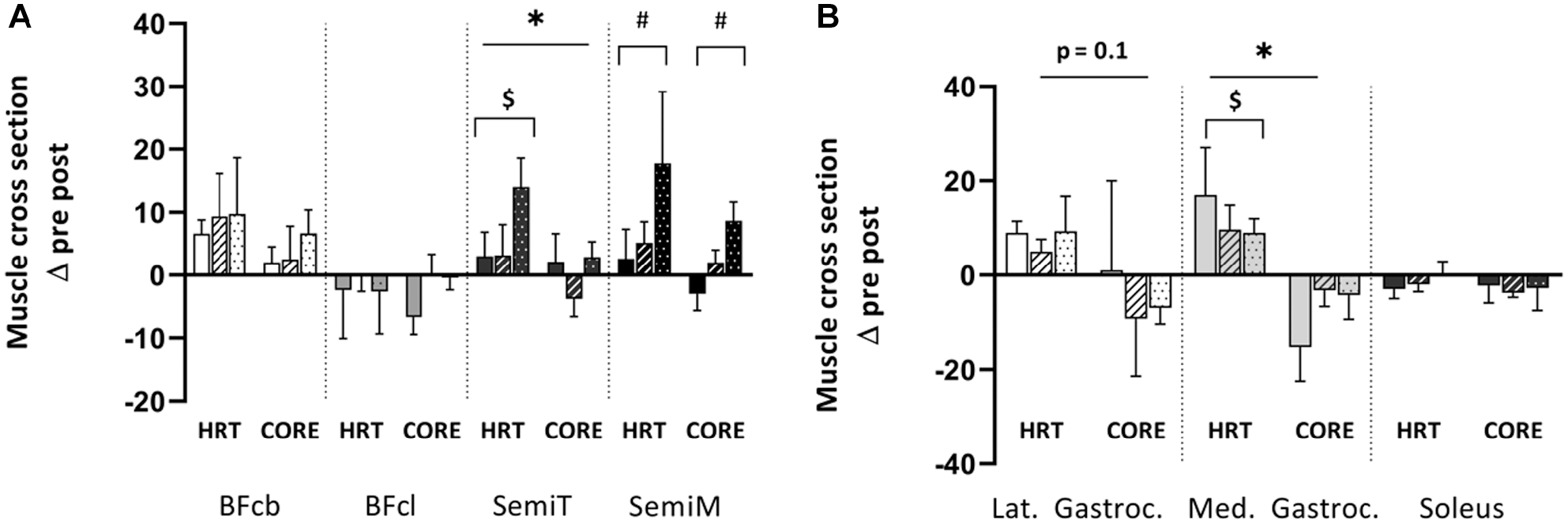
Muscle cross-sectional area in (A) hamstring and (B) calf muscles measured on magnetic resonance images obtained before and after intervention (pre, post) in the HRT and CORE groups. Cross sections were measured at 3 muscle positions: distal (bars without filling), middle (striated pattern), and proximal (dotted pattern). Data shown as changes relative to preintervention. *Significant group differences (P < .05). $Significant increase from premeasurement. #Significant increase in 1 specific muscle position vs others. Data shown as mean + SEM. BFcb, biceps femoris caput brevis; BFcl, biceps femoris caput longum; CORE, control exercises of the back and abdominal muscle; HRT, heavy resistance training; Lat Gastroc, lateral gastrocnemius; Med Gastroc, medial gastrocnemius; SemiM, semimembranosus; SemiT, semitendinosus.
The calf muscles did not show interactions between position and group either; therefore, main effects are reported as follows. HRT had a significant effect on the CSA of the calf muscles. The CSA of the medial gastrocnemius increased by 12% in the HRT group (P = .003; Cohen d = 1.1), whereas the CSA was decreased by 8% in the CORE group after the intervention (P = .06, Cohen d = 0.7; group difference, P = .001, Cohen d = 1.8) (Figure 3B). For the lateral gastrocnemius, there was a trend toward a difference between groups: the HRT group averaged an 8% increase in CSA (P = .08; Cohen d = 1.1) versus a 6% decrease (P = .07; Cohen d = 0.4) in the CORE group (group comparison: P = .094; Cohen d = 1). There was no major change in CSA of the soleus muscle in either group, and no effect of the position was detected.
Histological Characteristics of Biopsy Specimens
The most prevalent finding was intramuscular fat accumulation (Figure 4; Appendix Figures A3-A6, available online). Across time points and groups, the mean area of the scar tissue covered by adipocytes was 11.6%. Each participant had at least 1 biopsy specimen with obvious fatty infiltration, ranging from a minimum of 1.5% to a maximum of 63.2% of the total biopsy specimen area. In the HRT group, adipose tissue filled 6.1% of the total area before intervention versus 7.5% after intervention. In the CORE group, a mean 8.8% of the biopsy specimen area was composed of adipose tissue before intervention versus 25.4% after intervention (Figure 4A). Owing to variation in fat content among biopsy specimens, statistics on effect of group and time were avoided.
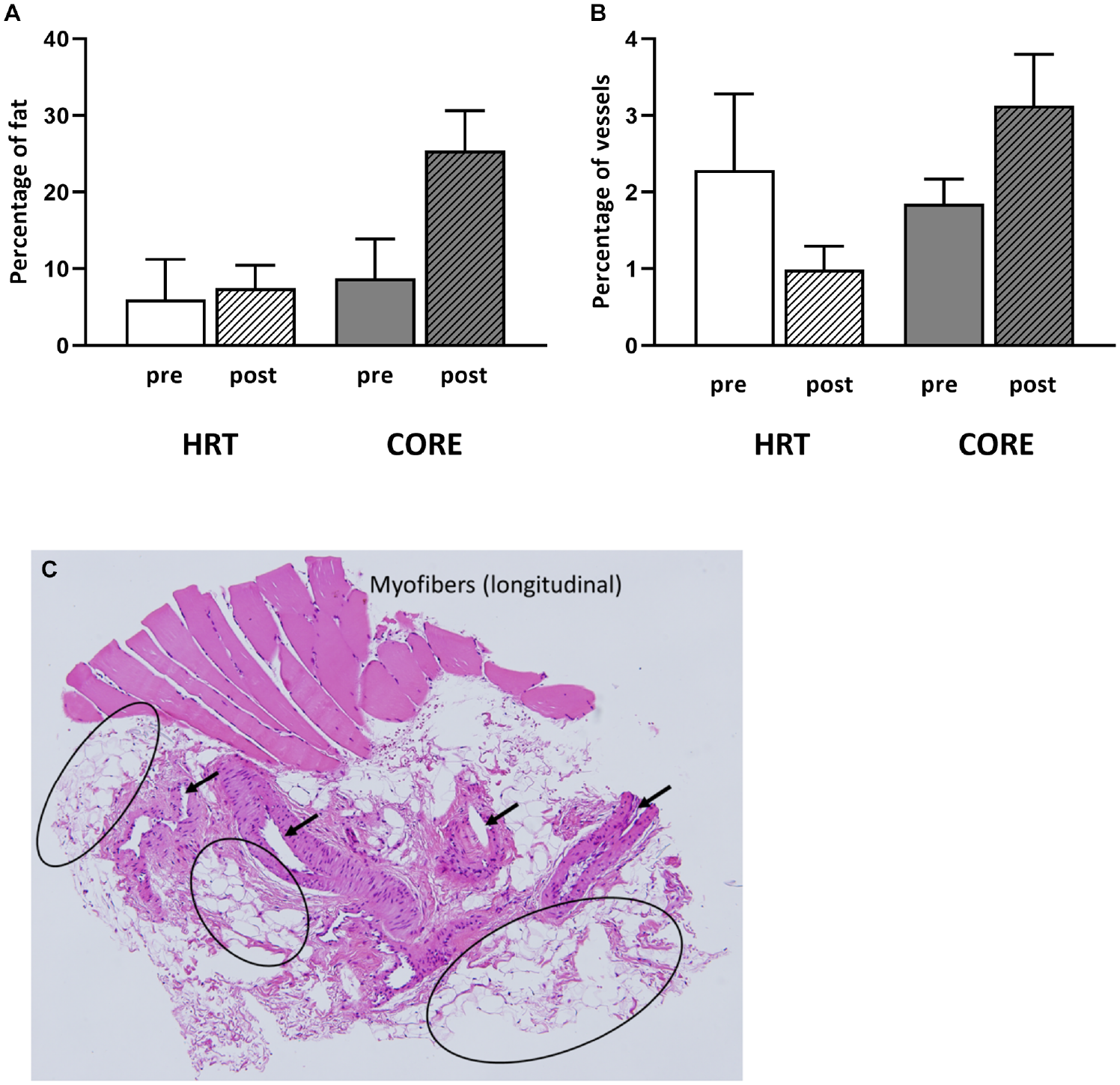
Quantification of (A) fat and (B) vessels in biopsy specimens obtained from participants in the HRT group (white bars) and CORE group (gray bars). Striated bars indicate measurements from postintervention (post) biopsy specimens. Data shown as mean + SEM; statistics not performed. (C) Representative hematoxylin and eosin image from scar biopsy specimen shows myofibers, adipocytes (circle), and large-diameter vessels (arrows). pre, preintervention.
In addition to adipocyte infiltration, there was an abundance of blood vessels, some with a very large diameter (Figure 4C; Appendix Figures A3 and A6, available online). We quantified a blood vessel area of 3.2% in the HRT group before intervention versus 0.99% after intervention. An average of 2.7% of the biopsy specimen was composed of blood vessels before intervention in the CORE group versus 2.9% after intervention (Figure 4B).
Ultrastructural Characteristics in the Biopsy Material
The most frequent observations were intramyofibrillar lipid droplets (Figure 5), disorganized hypercontracted sarcomeres (Figure 6), and granular areas devoid of sarcomeres (Appendix Figure A7, available online) within complete muscle fibers containing an intact sarcolemma and basement membrane (Figure 5, E and F; Figure 7). Sarcomere hypercontraction was a common finding (Figure 6); often, a faint pattern of condensed Z-lines was seen concomitant with lipid droplets (Figure 6, B, E, F). Subsarcolemmal mitochondria accumulation was another characteristic (Figure 7). Figure 6 (B, E, F; higher magnification) illustrates the transition between visible Z-line structures as well as myofibrillar components and hypercontracted sarcomeres.
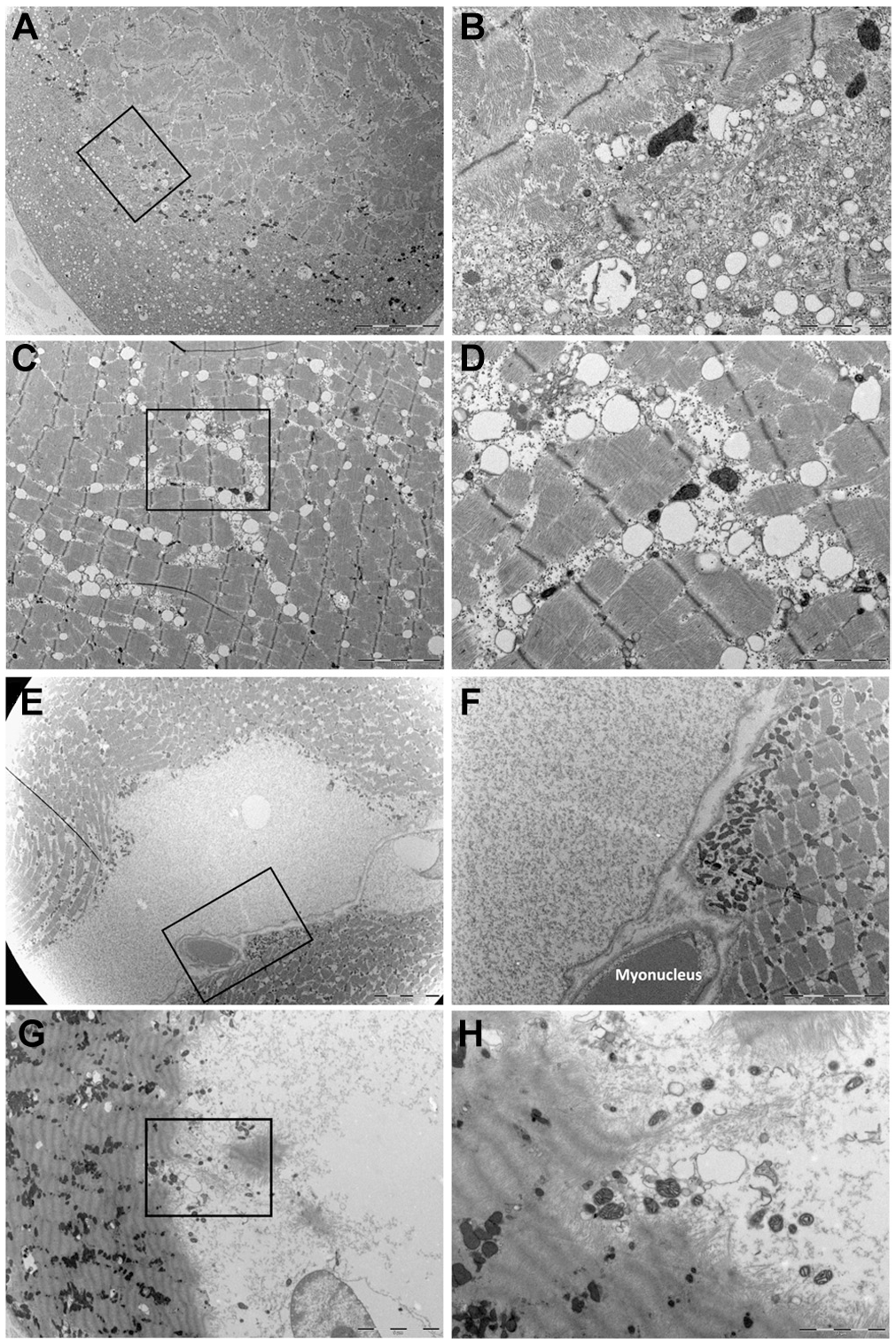
Presence of lipid droplets within myofibers in 3 participants. (A) Low magnification of sarcomere structure and disorganized sarcomere structure. (C) Lipid droplets adjacent to sarcomeres. (E) Two adjacent myofibers, both with granular areas devoid of sarcomeres. (G) Transition between sarcomeres with Z-lines present and hypercontracted sarcomeres with faint Z-lines. (B, D, F, H) Higher magnification of sections indicated by black box in panels A, C, E, and G.
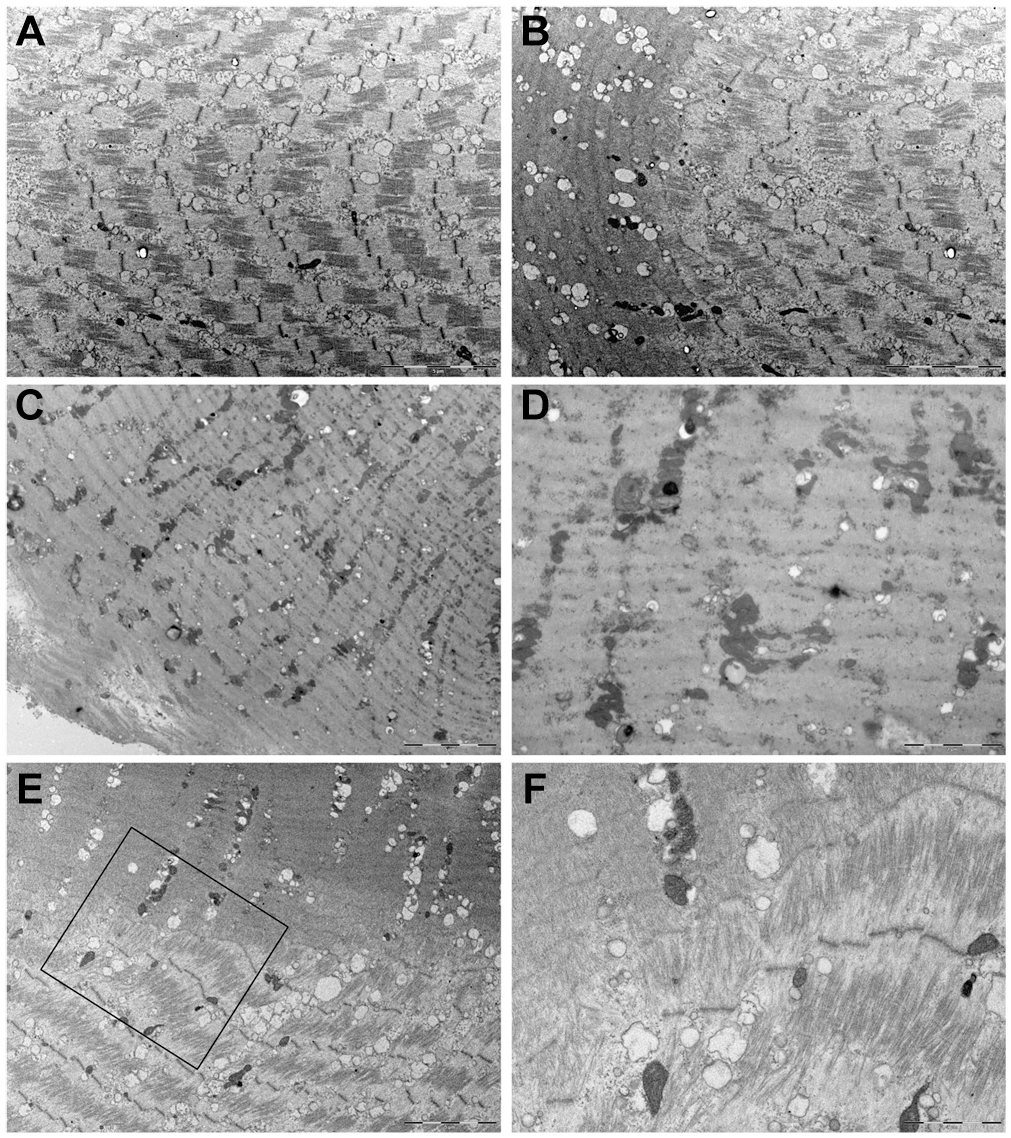
Sarcomere structure in 3 biopsy specimens. (A) Sarcomeres with extended I-bands in sarcomeres. (B) Transition between area with extended I-bands and hypercontracted sarcomeres with faint Z-lines. (C) Hypercontracted sarcomeres with faint Z-lines. (E) Transition between sarcomeres with Z-lines present and hypercontracted sarcomeres with faint Z-lines. (D, F) Higher magnification of electron micrographs shown in C and E. Magnified section shown in F indicated by black box in E.
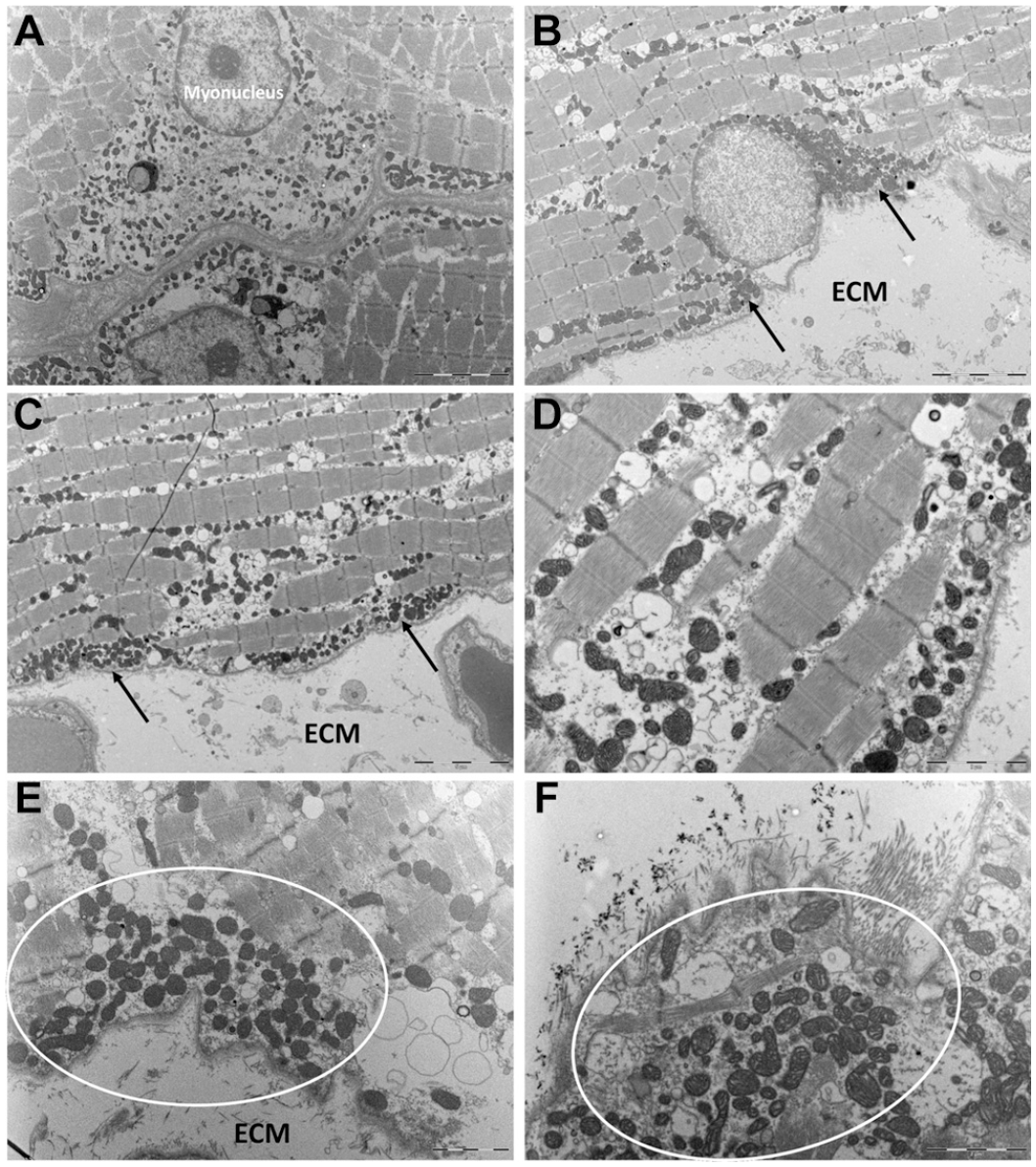
Accumulation of subsarcolemmal mitochondria. (A) Two adjacent myofibers with multiple mitochondria adjacent to sarcolemma and myonucleus. (B, C) Subsarcolemmal mitochondria (black arrows) and loosely packed extracellular matrix (ECM). (D) Higher magnification of image shown in panel C. Basement membrane appears intact. (E, F) Subsarcolemmal mitochondria indicated by white circle. Basement membrane appears intact.
When the extracellular matrix of the biopsy specimens was inspected, the lack of the normal tight, dense, and organized connective tissue became apparent. On the contrary, very few collagen fibrils appeared to be present in the extracellular matrix (Figure 7, B-D). The basal lamina of myofibers, however, appeared intact (Figure 5, E and F; Figure 7).
Patient-Reported Outcome Measures
Before the intervention, the injured leg scored poorer as compared with the healthy leg in both groups in each category. Although all items improved over time (Appendix Figure A2, available online), patients still scored the injured leg significantly poorer after intervention (data not shown). In the injured leg, the scores in the category symptoms improved from pre- to postintervention (time, P < .001), with no group difference. Soreness had a group × time interaction (P = .02), and post hoc tests showed an improvement in HRT (P < .001). Pain demonstrated a better score over time (P < .001), with no group difference. The same pattern was seen in function and daily living and the quality of life: both items improved over time (P < .001, P = .007, respectively) in the HRT and CORE groups.
Discussion
The motivation for the present study was to investigate a treatment option for chronic muscle strain injuries, which are among the most common types of sports injuries. Furthermore, we were interested in identifying scar tissue characteristics in the chronic state of strain injuries. Our primary aim was to examine the effect of HRT on pain, muscle strength, and muscle CSA in amateur athletes with chronic symptoms after a previous strain injury. The present study demonstrates that HRT improves pain and function in participants with long-term sequelae after a muscle strain injury. In addition, HRT can help normalize the concentric and eccentric muscle strength deficit and lead to greater muscle CSA in the injured region. However, HRT did not appear to alter the pathological infiltration of fat in the injured area. Taken together, this study indicates that short-term HRT can improve sequelae symptoms and muscle function, even many years after a muscle strain injury, but it does not significantly influence the structural abnormalities in the fibrotic muscle-tendon region.
Fatty Infiltration in Skeletal Muscle
For the first time, we have characterized the scar tissue directly in human strain-injured muscles. In contrast to our hypothesis proposing that we would discover extensive tight connective tissue in the fibrotic areas, the predominant finding was a substantial fatty infiltration in the intrafascicular space (Figure 4) and within myofibrils (Figure 5). Fatty degeneration after musculoskeletal injuries has been described almost exclusively after rotator cuff tears.24,25,27,29,42-44 One study reported fatty infiltration on MRI after hamstring strain injury 55 and 1 strictly in the rectus femoris. 20 We therefore postulate that strain and rotator cuff injuries share a common injury characteristic, as these injuries manifest a defect at the muscle–tendon/aponeurosis interface (strain injuries) or the tendon itself (rotator cuff), causing somewhat similar muscle pathology, such as muscle atrophy4,54 and fatty infiltration, as well as a high reinjury rate. 16
Fatty degeneration and atrophy do not regress after successful surgery for rotator cuff tears,24,25 but progression can be halted after surgical repair. 62 These findings indicate that once skeletal muscle is infiltrated by adipocytes, the process cannot be reversed, only discontinued. Whether this is the case for strain injuries is not known, but our data do not appear to show any notable fat regression by HRT (Figure 4). As mechanical stimuli are prerequisites to muscle and connective tissue homeostasis,1,6,8,23,32,34,37 we hypothesized that HRT might have a positive influence on scar tissue. However, the number of adipocytes and blood vessels seem to have remained more or less stable after intervention; therefore, we speculate that these data do not support our hypothesis that HRT could remodel the scar tissue. Muscle strain injuries are associated with a high risk of reinjury,16,28,31,49 which could reflect the permanent changes in the injured muscle and connective tissue (aponeurosis/tendon) as the present study proposes. The accumulation of intramuscular fat, the hypercontracted sarcomeres, the spaces without sarcomeric structure, and the sparse distribution of collagen fibrils in the extracellular matrix most likely contribute to a weakened muscle–connective tissue interface. A weakened interface might therefore not be able to sustain the high forces during explosive movements, which eventually contributes to reruptures at the site of the first injury. Since our study is the first to investigate the scar tissue composition after strain injuries and an intervention, it is clear that more research is required to allow for more definitive conclusions. One obvious yet unknown factor is the question of whether the scar tissue experiences similar load to the normal healthy tissue or whether the area is more or less unloaded even when subjected to specific exercises with progressively high loads. It remains speculative whether the high prevalence of recurrent injuries might be reduced by continuous HRT after a strain injury to strengthen the unaffected part of the muscle and muscle–connective tissue interface without directly normalizing the affected area (ie, the scar tissue). Further longitudinal studies are needed to examine the potential protective long-term effect of HRT on recurrent injuries.
Besides mechanical damage to tissues, the biochemical environment might have an additive effect on the pathology. We recently reported a significant upregulation of the key adipogenesis mediator peroxisome proliferator–activated receptor γ and the adipocytokine ANGPTL4 in cells derived from the injury exudate after strain injuries. 3 The exudate is present up to several months thereafter4,51 and has a persistent highly proinflammatory profile 3 ; consequently, cells in the exudate and factors released might contribute to pathological changes in the muscle. This indicates that acute events after injury eventually lead to chronic pathologic events that might not be reversible.
The observed fatty degeneration raises the question about the cell source of fatty accumulation/transition, especially in relation to potential treatment options in the future. Fibroadipogenic progenitors (FAPs) in skeletal muscle have been associated with the adoption of an adipogenic phenotype.2,33,46,61 So far, research on FAPs in vivo has been conducted in animal models in which injury was induced by toxic injections,15,33,36,61 rather than the more clinically relevant patient data. Patient samples from human rotator cuff, 19 vastus lateralis after anterior cruciate ligament tears, 21 and vastus medialis in patients with osteoarthritis reveal an increase in the number of FAPs concomitant with ectopic fatty accumulation in the muscles. Interestingly, the larger the tear size in rotator cuff patients, the higher the amount of FAPs and the fibro- and adipogenic potential of FAPs. 19 Although it is yet unknown whether FAPs are responsible for the fatty degeneration after strain injuries, it appears very likely that this cell source plays a role in ectopic fat accumulation. So far, it is not known which cascade of events causes the observed pathologic characteristics, such as sarcomeric disruptions and hypercontraction. Interestingly, a link between pathologic lipid accumulation and dysfunctional mitochondria was proposed in a rat muscle, 30 describing an accumulation of peripheral subsarcolemmal mitochondria, similar to our observations (Figure 7). In addition, a lower mitochondrial capacity to oxidize lipids concomitant with changes indicative of increased lipid droplet storage was noted. 30 Finally, almost all of the genes involved in the transport of free fatty acids into myofibers were reduced, and the synthesis of triglycerides from free fatty acids increased. 30
Functional and Structural Changes With Training
In this study, we show functional and structural long-term impairments of skeletal muscle after strain injuries as reported previously.4,5 The previous studies were, however, limited to a 6-month follow-up after injury. Strength training showed a clear effect on muscular tissue as participants randomized to the HRT group increased isokinetic MVC significantly after training. Concentric hamstring MVC recovered completely, but the eccentric MVC did not fully match the uninjured side. Since the HRT exercises predominantly involved eccentric contractions, the force deficit could indicate that the injured muscles experience long-term difficulties in exerting high forces in the lengthened state. This deficit might be the result of reduced neural activation of the injured area or a less optimal force transmission when the muscle-tendon unit is in the lengthened state, both coupled to the substantial fat accumulation. Likewise, whether the protective effect of eccentric HRT on recurrent strain injuries 48 relies on a training effect of motor unit recruitment, the enforcement of the connective tissue and/or changes to fascicles and their insertion into the aponeurosis remains unknown. However, our ultrastructural data do not suggest that there is any remodeling of the scar tissue. Our ultrastructural data show that the myofibers appear to be intact, which means that there is an undamaged basal lamina, suggesting that the myofibers per se are not disrupted (Figures 5 and 7). In the intramyofibrillar space, however, we detected large areas of hypercontracted sarcomeres and/or areas devoid of sarcomeric structure, which suggests quite substantial myofiber damage a long time after the strain injury.
For the calf injuries, we were unfortunately not able to measure dynamic concentric or eccentric strength, which is a clear limitation. Instead, isometric calf strength with an ankle degree of 90° was the only position that we could conduct a maximal calf muscle strength test, which did not detect any difference between the injured and the uninjured calf muscle. A previous study resulted in similar observations manifesting a significant isokinetic strength deficit after strain injuries at the same time when isometric maximal strength was not different in the injured as compared with the healthy leg. 4 Since there was a clear increase in CSA of the affected muscle (medial gastrocnemius) by 12% after 3 months of HRT, we are convinced that the training program was an effective stimulus of muscle growth and, hypothetically, isokinetic maximal strength.
Changes in Patient-Reported Outcome Measures After Training
Before and after intervention, the scores related to the injured leg were significantly worse than the healthy leg, indicating pain and soreness during movement, difficulty in performing specific tasks, and a significantly lower confidence in the injured leg. Both types of intervention improved the participants’ scores, but training was not sufficient to increase the scores to a level comparable with the healthy leg. The improvements of the CORE group are somewhat surprising, as only the HRT resulted in strength gains, but the CORE exercises might have translated into enhanced functional capacities and thereby increased confidence in the injured leg. Furthermore, HRT targeted specific muscle groups, which might have produced a hypoalgesic response as part of the well-described exercise-induced hypoalgesia, 53 and these findings indicate that the functional gains obtained with HRT were not reflected in the subjective response. The questionnaire outcome might therefore reveal a general response to any exercise intervention in relation to chronic pain. 22
Limitations
A limitation of this study is the lack of muscle CSA measures on the healthy leg, which was a function of available scanning time in the hospital. It was also not possible to quantify fat content on MRI. We did not take tissue samples from a healthy part of the muscle–connective tissue unit, to avoid any complications and further pain. The lack of isokinetic calf strength attributed to the lack of appropriate equipment is another limitation. The sample size is also smaller than that planned in the trial registration (NCT02152098), which included a group of patients with acute injury who formed the basis for the sample size calculation but were not part of the present study. For the present outcomes, no formal sample size could be determined a priori, although it should be noted that the robust effect sizes indicate that the results may be of clinical relevance despite the sample size. Last, the questionnaire was validated just for the hamstring muscle groups, and we modified it for the calf region following the same principles and wording as for the hamstring questionnaire.
Conclusion
We found substantial strength deficits in healthy amateur athletes who experienced chronic muscle strain injuries. HRT was well-tolerated and increased muscle strength and CSA in some muscles, while there was no similar change after CORE training. Intramuscular and myofibrillar fatty infiltration did not appear to change with training, and we speculate that the absence of a tight muscle–connective tissue interface led to focal unloading, which activated cellular processes associated with muscle pathology. Even though the structural changes did not seem to be reversed, strength training appeared an effective treatment option even many years after the injury.
Supplemental Material
sj-pdf-1-ajs-10.1177_03635465211026623 – Supplemental material for Chronic Sequelae After Muscle Strain Injuries: Influence of Heavy Resistance Training on Functional and Structural Characteristics in a Randomized Controlled Trial
Supplemental material, sj-pdf-1-ajs-10.1177_03635465211026623 for Chronic Sequelae After Muscle Strain Injuries: Influence of Heavy Resistance Training on Functional and Structural Characteristics in a Randomized Controlled Trial by Monika L. Bayer, Maren Hoegberget-Kalisz, Rene B. Svensson, Mikkel H. Hjortshoej, Jens L. Olesen, Janus D. Nybing, Mikael Boesen, S. Peter Magnusson and Michael Kjaer in The American Journal of Sports Medicine
Footnotes
Acknowledgements
The authors thank all the participants for their participation. The medical staff of the Institute of Sports Medicine Copenhagen, Bispebjerg Hospital, and the radiology department, Frederiksberg Hospital, are acknowledged for their assistance and contributions to this study.
Submitted November 12, 2020; accepted March 26, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: Funding was provided by AntiDoping Danmark, Bispebjerg Hospital Internal Research Funding, Gigtforeningen (R122-A3021), Kulturministeriet (TAKT2014-354), Lundbeckfonden (R198-2015-207), Novo Nordisk Fonden (12491), Region Hovedstaden (R139-A5061). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.