
Abstract
Background:
Mandated sports safety policies that incorporate evidence-based best practices have been shown to mitigate the risk of mortality and morbidity in sports. In 2017, a review of the state-level implementation of health and safety policies within high schools was released.
Purpose:
To provide an update on the assessment of the implementation of health and safety policies pertaining to the leading causes of death and catastrophic injuries in sports within high school athletics in the United States.
Study Design:
Cross-sectional study.
Methods:
A rubric composed of 5 equally weighted sections for sudden cardiac arrest, traumatic head injuries, exertional heatstroke, appropriate health care coverage, and emergency preparedness was utilized to assess an individual state’s policies. State high school athletic/activities association (SHSAA) policies, enacted legislation, and Department of Education policies were extensively reviewed for all 50 states and the District of Columbia between academic year (AY) 2016-2017 (AY16/17) and 2019-2020 (AY19/20). To meet the specific rubric criteria and be awarded credit, policies needed to be mandated by all SHSAA member schools. Weighted scores were tabulated to calculate an aggregate score with a minimum of 0 and a maximum of 100.
Results:
A total of 38 states had increased their rubric scores since AY16/17, with a mean increase of 5.57 ± 6.41 points. In AY19/20, scores ranged from 30.80 to 85.00 points compared with 23.00 to 78.75 points in AY16/17. Policies related to exertional heatstroke had the greatest change in scores (AY16/17 mean, 6.62 points; AY19/20 mean, 8.90 points; Δ = 2.28 points [11.40%]), followed by emergency preparedness (AY16/17 mean, 8.41 points; AY19/20 mean, 10.29 points; Δ = 1.88 points [9.40%]).
Conclusion:
A longitudinal review of state high school sports safety policies showed progress since AY16/17. A wide range in scores indicates that continued advocacy for the development and implementation of policies at the high school level is warranted.
Keywords
Approximately 8 million student-athletes participate in sanctioned high school athletics annually within the United States, 1 and while sports participation has numerous positive health benefits, catastrophic injuries and fatalities do occur. Evidence has suggested that sudden cardiac arrest, traumatic head injuries, exertional heatstroke, and exertional collapse associated with sickle cell trait account for >90% of all catastrophic injuries and deaths in sports and physical activity. 7 While it may not be possible to eliminate all risks of mortality and morbidity related to sports participation, there are numerous strategies that can be taken to optimize emergency preparedness and mitigate said risks. 9
Mandating policies that require the utilization of evidence-based best practices specific to the prevention and management of the leading causes of sports-related sudden death have been shown to mitigate morbidity and mortality.2,16-18 Previous literature has shown that estimated preseason exertional heat illness rates were 55% lower in states that mandated evidence-based heat acclimatization policies compared with states that did not. 18 Similarly, work by Cooper et al 13 found a 35% to 100% reduction in exertional heat illness incidence rates after the implementation of a heat policy that included both heat acclimatization and environment-based activity modification guidelines in the state of Georgia. Furthermore, Drezner et al 15 showed that 89% of athletes who sustained sudden cardiac arrest survived when resuscitation was applied, an automated external defibrillator (AED) was on site, and the organization had established an emergency action plan, highlighting the importance of these components.
Mandates from state high school athletic/activities associations (SHSAAs) and state laws within the United States have been cited as facilitators to implement or improve emergency action plans,26,27 and state mandates have been associated with improved adoption of these policies at the local level.28,29 Despite strong evidence showing the relationship between evidence-based best practice policies and a reduction in morbidity and mortality, a majority of US high schools lack the appropriate policies for the health and safety of student-athletes.21,28,29
It is important to note that the creation and implementation of health and safety policies for preventing and managing the leading causes of death in sports at the high school level are left to the individual states and their respective governing bodies; this is in contrast to settings such as intercollegiate athletics, where the respective governing body (eg, National Collegiate Athletic Association) establishes nationwide mandates by which all member institutions must abide. In 2017, a document was released outlining the current status of required health and safety policies within high school athletics in the United States. 3 The findings indicated that while all states required some type of health and safety policies, there was a lack of compliance overall with evidence-based health and safety policies (range, 23.00%-78.85%). 3
Before the release of the 2017 document on the state-level implementation of health and safety policies, 3 the extent to which individual states had mandated health and safety policies in place was unknown. As previous literature 3 has provided a static assessment of state-level health and safety policies, which does not allow for an understanding of how policies change over time, further work in this area must continue. Therefore, the purpose of this study was to provide an update on the graded assessment of the implementation of health and safety policies relating to the leading causes of sudden death and catastrophic injuries in sports at the high school level. We hypothesized that >50% of states in the United States would make positive changes (ie, improve their required policies) from the original study.
Methods
Study Design
This study used a descriptive observational design that was derived from a previous study published in 2017. 3 The purpose of the current study was to describe the contemporary landscape of state-required health and safety policies and to identify any changes (improvements or regression) from the 2017 study. The health and safety policies specific to the prevention and management of the leading causes of sudden death and catastrophic injuries in sports and emergency preparedness were quantified for the 50 states and the District of Columbia over the following time period: between academic year (AY) 2016-2017 (AY16/17) and 2019-2020 (AY19/20). The evaluation of health and safety policies was performed by assessing required policies from the SHSAA, state legislation (eg, Department of Education, Department of Public Health), or both the SHSAA and state legislation.
Health and safety policies required by the SHSAA are mandated for all member schools, whereas those required through legislation are often mandated for all high schools within each respective state, regardless of association membership. State high school health and safety policies are thoroughly reviewed once a year (detailed below). Only policies that are required or mandated to be followed by all SHSAA member schools and that are publicly available online were included. If a policy was recommended or encouraged, the state was not credited with having the policy in place, as there is an implication that individual member schools are left to decide whether to implement the practice. Because human participants were not directly involved in this study, the institutional review board at the University of Connecticut deemed that this study was exempt from needing to be reviewed.
Rubric
The rubric for this study was previously developed 15 and comprised 5 specific areas associated with the leading causes of sports-related death and catastrophic injuries: (1) exertional heatstroke, (2) traumatic head injuries, (3) sudden cardiac arrest, (4) appropriate health care coverage, and (5) emergency preparedness. 7 Importantly, there were an estimated 56, 64, and 62 sports-related catastrophic injuries in high school athletics in AY16/17, AY17/18, and AY18/19, respectively, accounting for, on average, 74.57% of all catastrophic injuries in collegiate and high school athletics combined. 19 At the time of this publication, the National Center for Catastrophic Sport Injury Research had not released data on catastrophic injuries for AY19/20. Additional information on the rubric development process can be found in the original study. 3 In brief, the rubric was developed utilizing current position statements, consensus statements, and interassociation task force recommendations4-6,8-12,14,20 for each of the 5 rubric components. Each of the 5 areas of the rubric was weighted equally (ie, 20 points) for a total aggregate score of 100 and a minimum score of 0. A blank rubric with section and item scores can be found in Appendix A (available online).
Data Collection Procedures
For each review period between AY16/17 and AY19/20, a 3-tier process was used to review the publicly available state health and safety policies. For the purpose of this study, only publicly available policies were accessed and analyzed, as the accessibility of the information to stakeholders (eg, high schools, parents, and health care professionals) is imperative to the successful implementation of such policies. The first tier (tier 1) included a team of research assistants who independently reviewed all 50 states’ plus the District of Columbia’s health and safety policies in the fall of 2018 and 2019. The second tier (tier 2) included an independent audit of the tier 1 findings by senior research assistants. The final tier (tier 3) included 3 researchers (S.E.S.M., C.M.E., W.M.A.) who independently reviewed the policies implemented at the state level. After an independent review, the tier 3 researchers met to compare their findings. As 3 researchers participated in the full independent review, any policy score with a discrepancy was discussed, and the ultimate decision was derived from a two-thirds vote. If the research team was notified of recent changes, updates, or the need to re-review the state-required policies, a second review was conducted. The second review period consisted of the tier 3 researchers independently reviewing the policies in question and meeting to compare the findings. Discrepancies were discussed, and the ultimate decision was derived from a two-thirds vote. The 3-tier system allowed for the confirmation of the accessibility of the policies, ensuring that all policies, regardless of their location on publicly accessible websites, were identified and included in the analysis.
Data Analyses
Grading for each state’s rubric was conducted to obtain an aggregate score, with a maximum of 100. Each state was ranked from 1 (representing the greatest number of health and safety policies required) to 51 (representing the lowest number of health and safety policies required). To identify changes between AY16/17 and AY19/20, we calculated the change in scores for the total score (state AY19/20 total points – state AY16/17 total points) and section scores (AY19/20 section total points – AY16/17 section total points). The mean, median, standard deviation, and interquartile range (IQR) are presented for the AY16/17 original scores and AY19/20 current scores. The change in scores (Δ) is presented as a difference in points within each state, with the mean and standard deviation shown for the change between AY16/17 and AY19/20 as well as the relative change (AY19/20 score / AY16/17 change). Further, the relative percentage change was calculated—(AY19/20 score / AY16/17 score) * 100—to depict an individual state’s improvement for overall health and safety policies.
Results
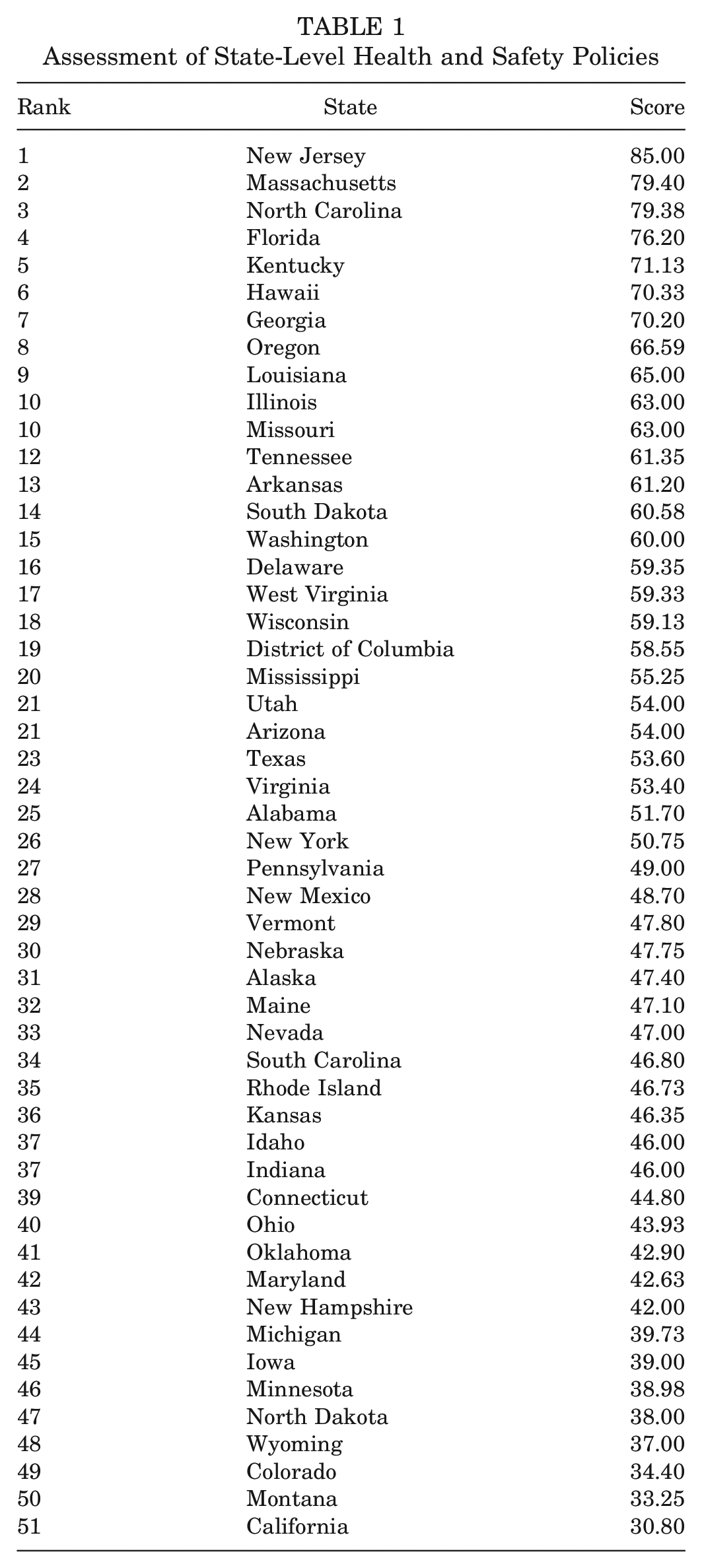
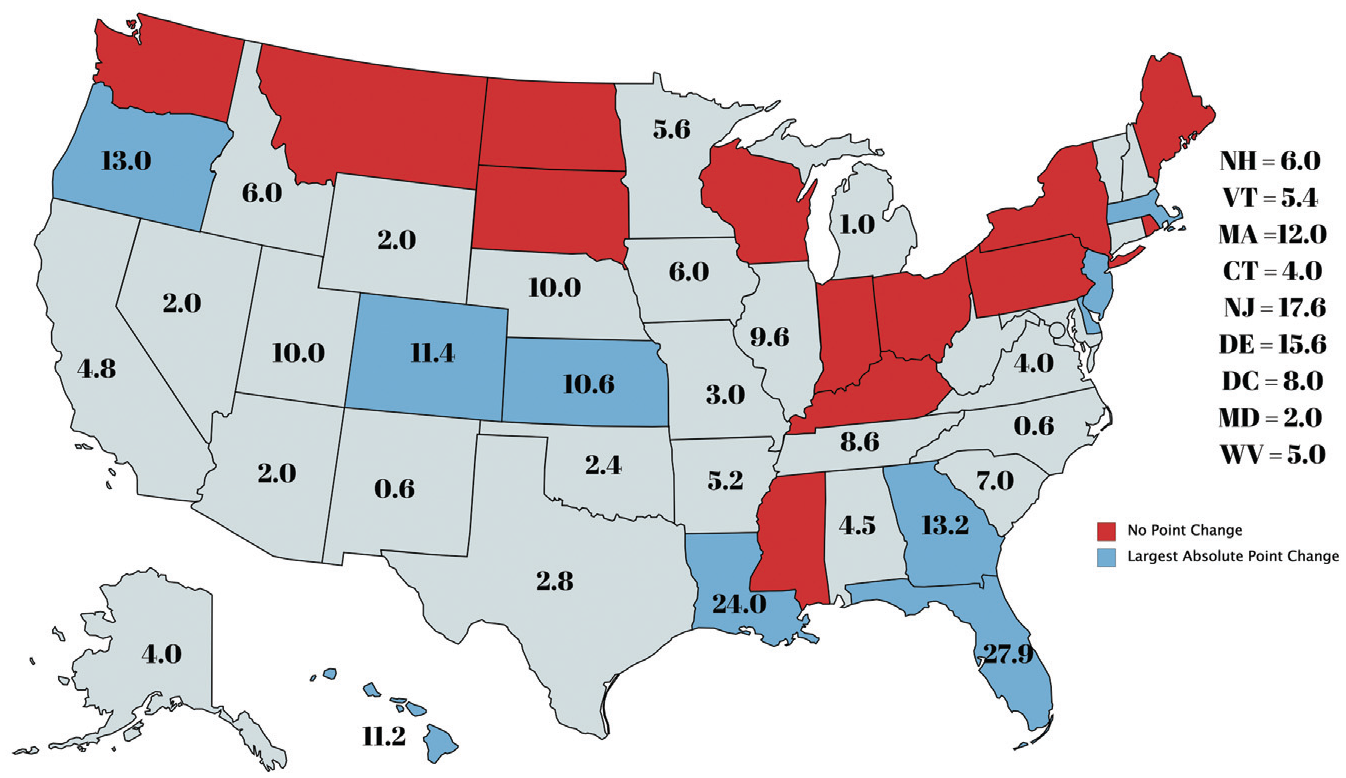
The updated assessment of all 50 states’ plus the District of Columbia’s health and safety policies is presented in Table 1. In AY19/20, the median was 50.75 points (IQR, 45.40-60.89 points), and the mean was 53.24 ± 12.63 points. On average, states improved 5.57 ± 6.41 points between AY16/17 and AY19/20. The range in AY16/17 was 23.00 to 78.75 points, and in AY19/20, the range was 30.80 to 85.00 points. The states with the greatest amount of positive change (eg, implemented new or revised existing health and safety policies) between AY16/17 and AY19/20 were Florida (27.95 points), Louisiana (24.00 points), New Jersey (17.97 points), Delaware (15.62 points), and Georgia (13.22 points) (see Appendix B, available online). Of the 38 states that had improvement in their overall scores, the mean point change was 7.6 ± 6.2, and the mean relative change was 17%. When normalizing to relative change, the states with the greatest relative change were Louisiana (relative Δ = 1.59), Florida (relative Δ = 1.58), Colorado (relative Δ = 1.50), Delaware (relative Δ = 1.36), and Kansas (relative Δ = 1.30). There were 13 states (Indiana, Kentucky, New York, Maine, Mississippi, Montana, North Dakota, Ohio, Pennsylvania, Rhode Island, South Dakota, Washington, Wisconsin) that did not make any changes related to the evaluated health and safety policies on the rubric between AY16/17 and AY19/20. After the publication of the AY16/17 findings, the research team was notified of an incorrectly awarded policy for New York (athletic trainer licensure within the appropriate health care coverage section of the rubric) and therefore removed points (5 points) from New York to correct the current policy requirement. Figure 1 highlights the 10 states that had the greatest absolute point increase and the 13 states that made no changes between AY16/17 and AY19/20.
Assessment of State-Level Health and Safety Policies
Absolute point change.
Of 20 points possible for each of the 5 topic areas, sudden cardiac arrest had the highest implementation rate (mean, 12.72 ± 4.38 points), followed by appropriate health care coverage (mean, 12.45 ± 3.79 points), emergency preparedness (mean, 10.29 ± 4.03 points), exertional heatstroke (mean, 8.89 ± 5.46 points), and traumatic head injuries (mean, 8.88 ± 2.72 points) (see Appendix B). On average, the scores in each of the 5 topic areas increased 0.86 points or 4.32%. The topic area from the rubric with the greatest change between AY16/17 and AY19/20 was exertional heatstroke (AY16/17 mean, 6.62 points; AY19/20 mean, 8.90 points; mean Δ, 2.28 points [11.4%]”), followed by emergency preparedness (AY16/17 mean, 8.41 points; AY19/20 mean, 10.29 points; mean Δ, 1.88 points [9.40%]) (see Appendix B). Figure 2 illustrates rubric category point increases between AY16/17 and AY19/20 for all states that had a total increase of ≥10 points.
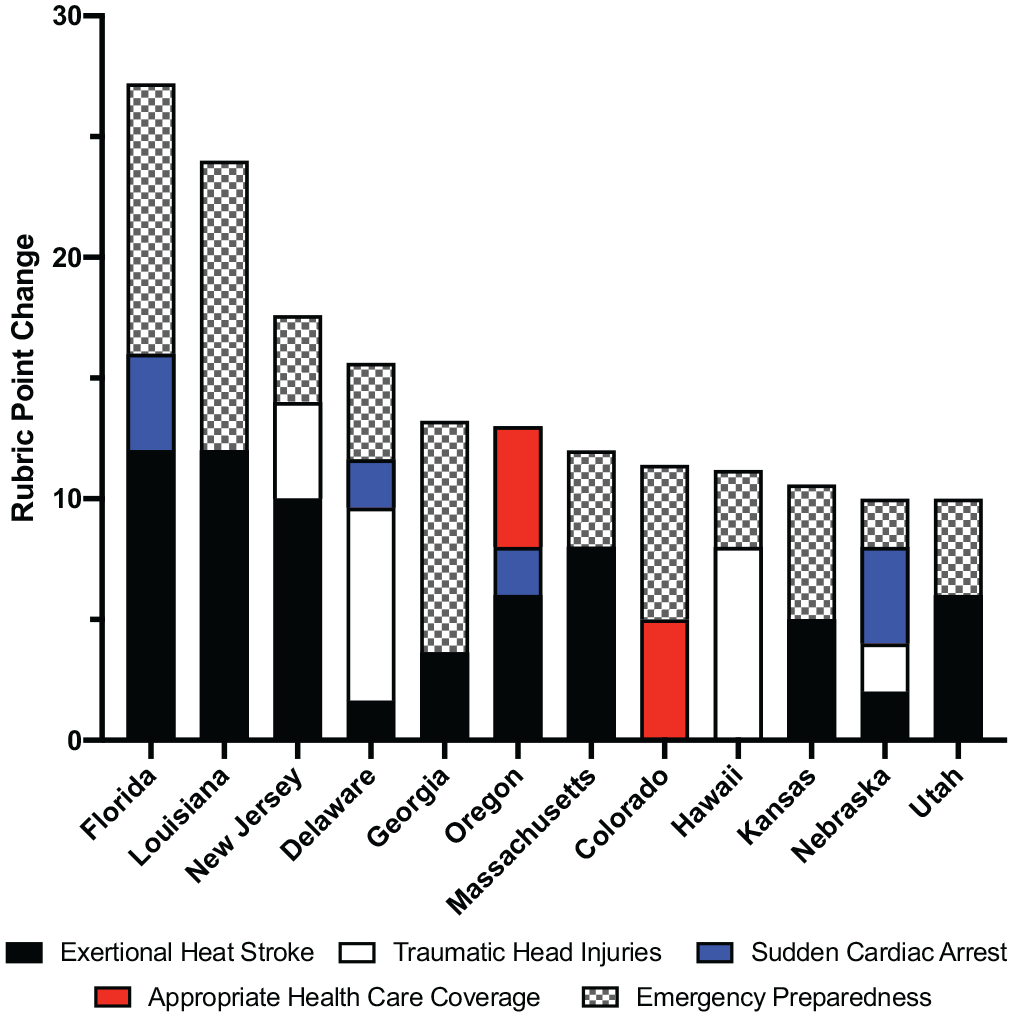
Rubric category point increases between AY16/17 and AY19/20 for all states that had a total increase of ≥10 points.
Discussion
The implementation of health and safety policies surrounding the prevention and management of the leading causes of death and catastrophic injuries at the state level is associated with improved patient outcomes.13,16,18 Despite this, an AY16/17 study on state-level requirements of these policies provided evidence that states failed to fully implement these life-saving guidelines. 3 The purpose of this study was to provide an update to the AY16/17 document on the state-level implementation of health and safety policies for the proper management of the leading causes of death and catastrophic injuries within high school athletics. 3 A review of health and safety policies for AY19/20 showed that 38 states have made improvements in the implementation of policies when compared with the health and safety policies that were in effect for AY16/17. While there are several states that have not made policy changes that were reflected on the rubric, the increase in overall median (4.5 points) and mean (5.59 points) scores is encouraging. Similar to the AY16/17 review, there is still a large degree of variability in mandated policies for each state, which is obvious in the large range (30.80-85.00 points) of states’ scores.
It is important to note that the original mean and median scores from AY16/17 included the 5-point error that was allotted to New York. This error was corrected, but the original mean and median scores are slightly inflated because of that. If the points awarded to New York had been removed from the AY16/17 review, the mean would have been 47.57% (–0.10), the median would have been 47.10% (–0.00), and the standard deviation would have been 11.18% (–0.04); this would have demonstrated a 5.67-point increase between AY16/17 and AY19/20. Despite this, the policy review indicates a 5.57-point increase in overall mean scores between AY16/17 and AY19/20. This finding is encouraging, as it appears that those in leadership positions within state organizations and state legislators may be more cognizant of the need for health and safety policies, thus enacting change. A theoretical consideration for this change may be explained by the Lewin model of change. 25 In this model, change may be able to be explained by 3 progressive stages: stage 1, unfreezing (eg, challenging the status quo); stage 2, change (eg, implementation of new strategies to achieve change); and stage 3, refreezing (eg, sustaining the changes over time). Although impossible to measure in this study, it is possible that the AY16/17 document initiated stage 1, thus accounting for the positive changes (ie, stage 2) identified in the current review.
States that made changes to their health and safety policies utilized SHSAA or legislative mandates to modify or implement sports safety policies. Both Florida and Louisiana, which had the largest changes in health and safety policy scores, achieved changes via legislative avenues. Access to data and expertise have been cited as barriers to the adoption of evidence-based policies related to sports health and safety as well as injury prevention. 24 It is difficult for us to assert, with any certainty, the factors leading to these changes; however, we would be remiss if we did not offer some plausible hypotheses leading to improved policies. First, key advocates in the state from several different backgrounds (eg, health care professionals, parents, legislators, board members) identified the need for improved standards and relentlessly championed the efforts for change. Second, the key advocates, along with policy makers, developed draft policies for governing bodies to review, making it easier for executive directors, legislators, and board members, among others, to consider the policy. Third, in 2018, the Team Up for Sports Safety (TUFSS) initiative was launched to address these barriers. TUFSS meetings are held with key stakeholders from each state (eg, state legislators, SHSAA administrators, health care professionals, high school administrators), in addition to experts on topics related to sudden death in sports and policy change, to develop strategies to implement policies at the state level.
The policy topics discussed at the TUFSS meetings are decided by stakeholders in each state and are dictated by current perceived needs. For example, New Jersey stakeholders decided to discuss exertional heat illness prevention, exertional heat illness management, traumatic head injuries, and strength and conditioning session regulations, as they recognized a gap in their preexisting policies on these topics. Each TUFSS meeting is different, as each state’s stakeholders perceive different topics to be important. Although the purpose of this project was not to identify the effect of the TUFSS initiative on policy change, we would be remiss to mention that the states with the greatest changes in health and safety policy scores (Florida, Louisiana, New Jersey, Delaware, Georgia) were involved with the TUFSS initiative between AY16/17 and AY19/20. It is possible that the TUFSS meetings helped propel change in these states, with previous literature supporting the utilization of education and fostering collaborative relationships as factors that are associated with successful policy implementation. 23 However, we note that this is purely speculation, as there is no evidence suggesting that the meetings held in relation to the TUFSS initiative were the primary and/or sole driving force leading to positive changes. Each state has different catalysts for implementing health and safety policy changes, which can include student-athlete death, empirical data, and proactivity. 22 While the factor that propelled change in different states varied, shared leadership and communication were the fundamental factors that allowed for the successful adoption of health and safety policies. 22
While overall scores associated with state-level mandated health and safety policies increased in the current study, the categories of greatest improvement on the rubric were exertional heatstroke and emergency preparedness. Both of these categories include policies that have zero or low cost associated with implementation, heat acclimatization, and emergency action plans. Previous research has shown perceived financial constraints to be a barrier to requiring state-level health and safety policies for high school athletics.23,24 This finding is mirrored when researching barriers at the local high school level, with athletic trainers and athletic directors identifying perceived financial constraints as a common barrier to the implementation of comprehensive health and safety policies.26,27 Because unfunded mandates have been reported as an organizational barrier to the implementation of sports safety policies at the high school level, 23 the zero cost associated with heat acclimatization and emergency action plan policies may help explain the observed highest changes in scores in the related rubric.
In AY19/20, the rubric topic area that resulted in the highest mean (12.72) and median (14.00) scores was sudden cardiac arrest. This was closely followed by appropriate health care coverage (mean, 12.45; median, 10.00) and emergency preparedness (mean, 10.29; median, 10.00). Sudden cardiac arrest remains the leading cause of death in all sports and physical activity. Epidemiologic data over a 37-year period across all sports showed that sudden cardiac death accounted for 67.4% of all deaths and catastrophic injuries observed. 19 Given existing evidence supporting an approximately 90% sudden cardiac arrest survival rate when an AED is accessible and utilized, 16 policy makers may deem this topic a priority when addressing health and safety policies. Further, the higher scores in the appropriate health care coverage and emergency preparedness categories may be supported by the importance of (1) having a credentialed health care provider qualified and trained in managing the leading causes of sudden death and catastrophic injuries in sports and (2) having a structured and rehearsed plan of action in place to promptly triage patients with potential emergency considerations. Although the mean (8.89) and median (8.50) scores were lower for the exertional heatstroke area than the aforementioned topics, exertional heatstroke policies improved 11.40% in AY19/20 compared with AY16/17. Given the low implementation costs associated with heat acclimatization and environment-based activity modification policies, some states may have decided to focus on addressing these components compared with more costly policies (eg, requiring the employment of a trained and qualified health care provider, acquiring AEDs).
The large variability in health and safety policy implementation at the state level that was noted in AY16/17 was still evident in AY19/20, although the gap has grown slightly smaller. Because the final decision regarding the implementation of health and safety policies for high school sports is typically made by the SHSAA executive committee, it is important to continue providing education on the importance of these policies and maintain positive collaborative working relationships. 23 Encouraging states to make changes by highlighting changes in other states could help propel reform. Institutional theory explains that organizations will implement change to remain competitive with other organizations. 30 If a specific SHSAA sees changes made in a neighboring state, it may help encourage policy adoption in its own state.
Limitations and Future Research
The current study is not without limitations. The annual reviews of health and safety policies are conducted by experienced researchers, but they are not void of possible human errors. As evidenced in our reassessment of New York’s score, it is possible that errors in scoring can occur. To reduce the risk of human errors, the rubrics for all states are publicly accessible on websites, and conversations related to scoring are encouraged. If an error is found, the rubric will be updated after the verification of relevant policy materials. Additionally, the current study only credited policies that were effective as of AY19/20. Therefore, the current scores do not reflect policies that will go into effect at a later date. Because scores are updated biannually, the hope is that they are updated close to the implementation of new policies. As we mentioned, the categories of greatest improvement on the rubric were exertional heatstroke and emergency preparedness. It is important to note that both of these sections of the rubric have the greatest number of policies and stakeholders organizing the TUFSS meetings have expertise in these 2 areas. It is important to mention these factors, as they could have influenced the changing scores in some states. Future research should investigate any relationship between public health concussion policies and educational initiatives for the general public and the greater compliance with traumatic brain injury policies compared with other categories of the rubric, as this could assist in driving change of a greater magnitude within these other categories. This study only aimed to identify mandated policies but did not intend to measure policy implementation. Future studies should explore the implementation of these policies in high schools along with patient outcomes after implementation.
Conclusion
The notable progress made by many states since AY16/17 for the development and implementation of health and safety policies specific to preventing and managing the leading causes of sudden death and catastrophic injuries in high school athletics is encouraging. Further efforts, however, are needed to continue to progress policy implementation to ensure that all high school student-athletes participating in sanctioned sports are protected.
Supplemental Material
sj-pdf-1-ajs-10.1177_03635465211031849 – Supplemental material for State-Level Implementation of Health and Safety Policies to Prevent Sudden Death and Catastrophic Injuries Within High Schools: An Update
Supplemental material, sj-pdf-1-ajs-10.1177_03635465211031849 for State-Level Implementation of Health and Safety Policies to Prevent Sudden Death and Catastrophic Injuries Within High Schools: An Update by Samantha E. Scarneo-Miller, Christianne M. Eason, William M. Adams, Rebecca L. Stearns and Douglas J. Casa in The American Journal of Sports Medicine
Footnotes
Submitted December 10, 2020; accepted April 21, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: Funding for this project was provided by philanthropic donations made to the Korey Stringer Institute with partial support from the National Football League (NFL) Foundation. S.E.S.-M. has received funding from the Korey Stringer Institute as an employee and a consultant; while as an employee, she was funded by grants from the NFL Foundation. S.E.S.-M. also serves as an expert witness for legal cases related to catastrophic outcomes from sports-related participation. W.M.A. has received royalties from Springer Nature; has received consulting fees from the Korey Stringer Institute, Clif Bar & Company, Gatorade, BSX Athletics, and Samsung; has received honoraria from the North Carolina Athletic Trainers’ Association, Mid Atlantic Athletic Trainers’ Association, National Athletic Trainers’ Association (NATA), and Peach Belt Conference; has received grants from the NATA, Statim Technologies, QCK, and TechGuard Security; and has served as an expert witness on legal cases surrounding heat-related illnesses. R.L.S. has received fees for speaking at educational programs along with royalties from Jones & Bartlett Learning. D.J.C. has received research grants, clinical grants, corporate sponsorships, or foundation donations from Mission, General Electric, CamelBak, the NFL, Kestrel, Defibtech, Heartsmart, Eagle, BrainScope, WHOOP, the NATA, Polar, Gatorade, the National Center for Catastrophic Sport Injury Research at the University of North Carolina at Chapel Hill, the National Collegiate Athletic Association, the Biotechnology High Performance Computing Software Applications Institute, the United States Air Force, the United States Army, Kraft Heinz, First Line, the Falmouth Road Race, and AMP; serves as a consultant and on the advisory boards for Sports Innovation Lab, Clif Bar & Company (ended December 2018), and the NFL; receives royalties from Jones & Bartlett Learning, Springer, Lippincott Williams & Wilkins, Wolters Kluwer, UpToDate, and Routledge/Taylor & Francis Group; has received honoraria from Gatorade and educational institutions; and serves as an expert witness on legal cases regarding heatstroke, exertional sickening, and dehydration. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.