
Abstract
Background:
Ulnar collateral ligament (UCL) reconstruction (UCLR) is a viable treatment option for patients with UCL insufficiency, especially in the overhead throwing athlete. Within the clinical literature, there is still no universally agreed upon optimal rehabilitation protocol and timing for return to sport (RTS) after UCLR.
Hypothesis:
There will be significant heterogeneity with respect to RTS criteria after UCLR. Most surgeons will utilize time-based criteria rather than functional or performance-based criteria for RTS after UCLR.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
All level 1 to 4 studies that evaluated UCLR with a minimum 1-year follow-up were eligible for inclusion. Studies lacking explicit RTS criteria, studies that treated UCL injury nonoperatively or by UCL repair, or studies reporting revision UCLR were excluded. Each study was analyzed for methodologic quality, RTS, timeline of RTS, and RTS rate.
Results:
Overall, 1346 studies were identified, 33 of which met the inclusion criteria. These included 3480 athletes across 21 different sports. All studies reported RTS rates either as overall rates or via the Conway-Jobe scale. Timelines for RTS ranged from 6.5 to 16 months. Early bracing with progressive range of motion (ROM) (93.9%), strengthening (84.8%), and participation in an interval throwing program (81.8%) were the most common parameters emphasized in these rehabilitation protocols. While all studies included at least 1 of 3 metrics for the RTS value assessment, most commonly postoperative rehabilitation (96.97%) and set timing after surgery (96.97%), no article completely defined RTS criteria after UCLR.
Conclusion:
Overall, 93.9% of studies report utilizing bracing with progressive ROM, 84.8% reported strengthening, and 81.8% reported participation in an interval throwing program as rehabilitation parameters after UCLR. In addition, 96.97% reported timing after surgery as a criterion for RTS; however, there is a wide variability within the literature on the recommended time from surgery to return to activity. Future research should focus on developing a comprehensive checklist of functional and performance-based criteria for safe RTS after UCLR.
Keywords
The first ulnar collateral ligament (UCL) reconstruction (UCLR) was performed by Dr. Frank Jobe on Major League Baseball (MLB) pitcher Tommy John in 1974. 8 Since then, the number of UCLR procedures performed on recreational as well as competitive athletes has risen dramatically. 12 Various iterations of UCLR have been described and several studies exist that demonstrate the biomechanical efficacy of the procedure.7,39,41,43 The return to sport (RTS) rate after UCLR is generally reported as >84% throughout all levels ranging from high school to the professional level.23,25,31 Performance of baseball players after UCLR appears to be similar to preinjury level regardless of technique or graft utilized.9,11,23,28,31 However, preprofessional players who undergo surgery may have an increased risk of injured list assignment at the major league level. 63
Baseball players represent the majority of athletes undergoing UCLR, yet there is no universally accepted rehabilitation program for their RTS. 23 Most surgeons employ a progressive overhead throwing program postoperatively for their patients. However, these throwing programs are highly variable. For athletes in other sports such as gymnastics, javelin, tennis, or volleyball, the RTS criteria and rehabilitation protocols after UCLR are even less clear. A primary expectation of any athlete undergoing surgery, regardless of age, sex, sport, or level of competition, is return to his or her preinjury performance level— something that requires meticulous rehabilitation and attention to detail. While various rehabilitation methods after UCLR have been proposed, an established protocol does not exist for RTS after UCLR, even at the professional level. There is also no consensus on functional measures including elbow or shoulder range of motion (ROM) or strength testing to determine if a player is ready to RTS.
Therefore, the purpose of this study was to perform a systematic review of the current literature and assess postoperative rehabilitation parameters as well as RTS criteria reported within UCLR scientific literature. It was hypothesized that the majority of surgeons utilize solely time-based criteria rather than functional or performance-based criteria when determining when to allow players to RTS after UCLR.
Methods
Search Strategy
We performed a systematic review of level 1 to 4 studies of patients undergoing UCLR. The literature search was conducted using PubMed, Embase, and Cochrane databases from inception to February 2020. The search criteria used were the following: (((((((UCL) OR “ulnar collateral ligament reconstruction”) OR “medial ulnar collateral ligament”) OR “medial collateral ligament”) OR “tommy john”)) AND ((((((“elbow”[Medical Subject Headings (MeSH) Terms]) OR elbow*) OR “elbow joint”[MeSH Terms]) OR “elbow joint*”) OR “upper extremity”[MeSH Terms]) OR “upper extremity*”)) AND ((((((((((reconstruction[MeSH Terms]) OR reconstruction) OR surgery[MeSH Terms]) OR surgery) OR surgical) OR rehabilitation[MeSH Terms]) OR rehabilitation*) OR “return to”) OR outcome*) OR “objective protocol”). An additional search of all references of the selected articles was performed to find potential articles that were missed.
Inclusion/Exclusion Criteria
Studies that were included were required to be (1) written in English and (2) conducted on patients who underwent UCLR with (3) a minimum of 1-year follow-up. Studies lacking explicit RTS criteria, review articles, biomechanical studies, technical notes, letters to the editor, studies with <1 year of follow-up, studies that treated UCL injury either nonoperatively or by repair or studies assessing revision procedures were excluded. The exact number of excluded articles with reasoning is detailed in the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart (Figure 1). If an article detailed follow-up data from a previously published patient group, the more recent and/or relevant article was included in this study.
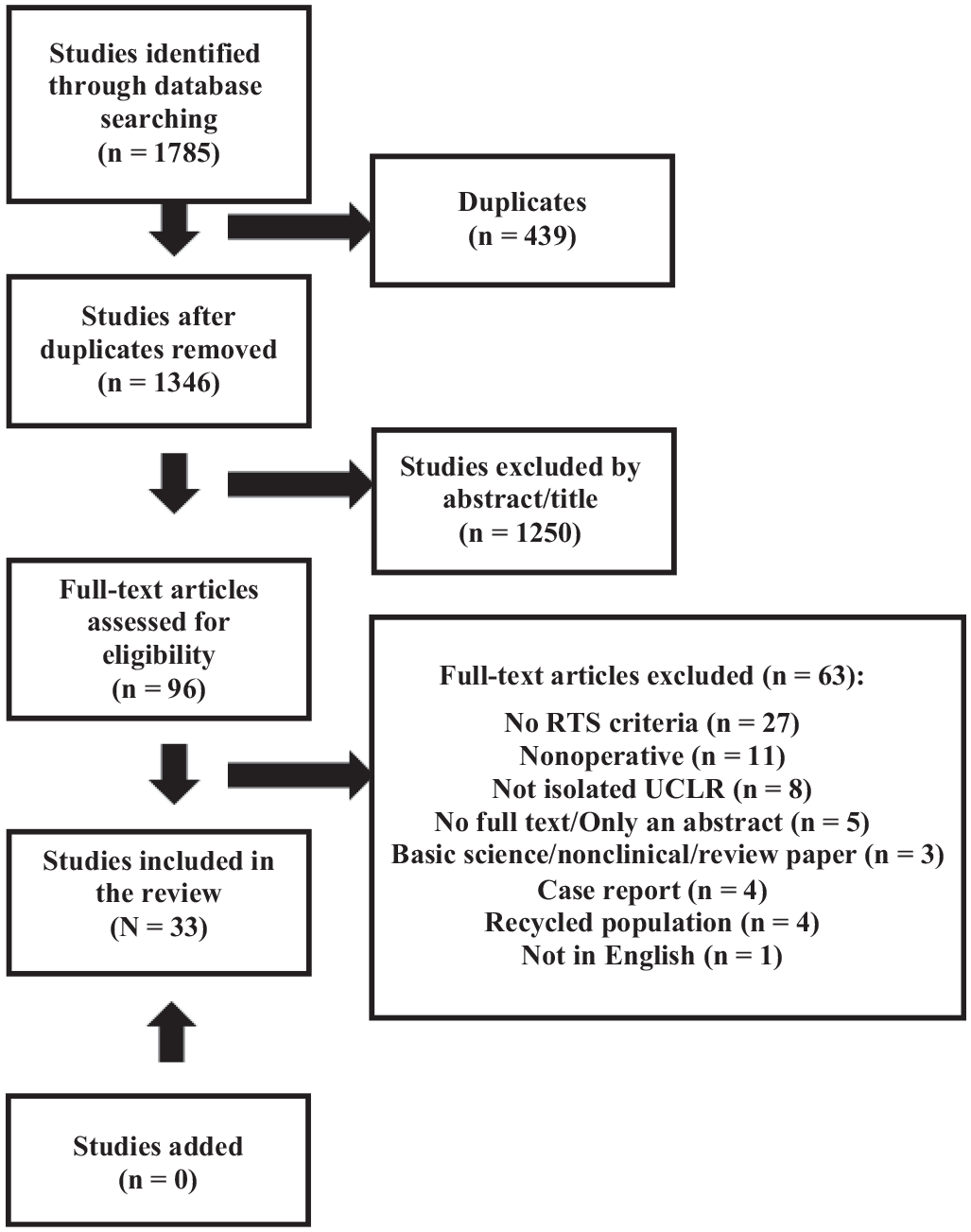
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram illustrating the assessment strategy for including studies in this systematic review. RTS, return to sport; UCLR, ulnar collateral ligament reconstruction.
The initial search and review was completed by 3 reviewers under the direct supervision of a sports-medicine trained clinical fellow (R.A.J.) and the senior author (M.G.C.). The methods section of each article meeting the inclusion criteria was thoroughly analyzed by the clinical fellow and senior author. The studies that met these inclusion criteria were compiled and extracted for data.
Patient Demographics and Outcomes
The number of patients, number of elbows operated on, mean age of the patient cohort, sex distribution, hand dominance, level of competition, and sport played were all noted. The decision was made not to report patient-reported outcomes (PROs) due to the wide variety of surveys used, but mean follow-up time and general success in RTS/full activity outcomes were collected. Each study was carefully analyzed for explicit criteria used to decide when patients would RTS or to full unrestricted activity.
Quality of Literature Methodology
The methodological quality of the included studies was independently assessed by 2 reviewers (S.R., D.P.W.) using the Coleman Methodology Score (CMS). The CMS contains 10 different criteria divided into 2 sections giving a final score ranging from 0 to 100. Scores from 85 to 100 are excellent, 70 to 84 are good, 55 to 69 are fair, and <55 are considered poor. The scores of each study are found in Table 1.
Coleman Methodology Scores Along With the Means and SDs for Each Scoring Category With a Maximum Score of 100 a
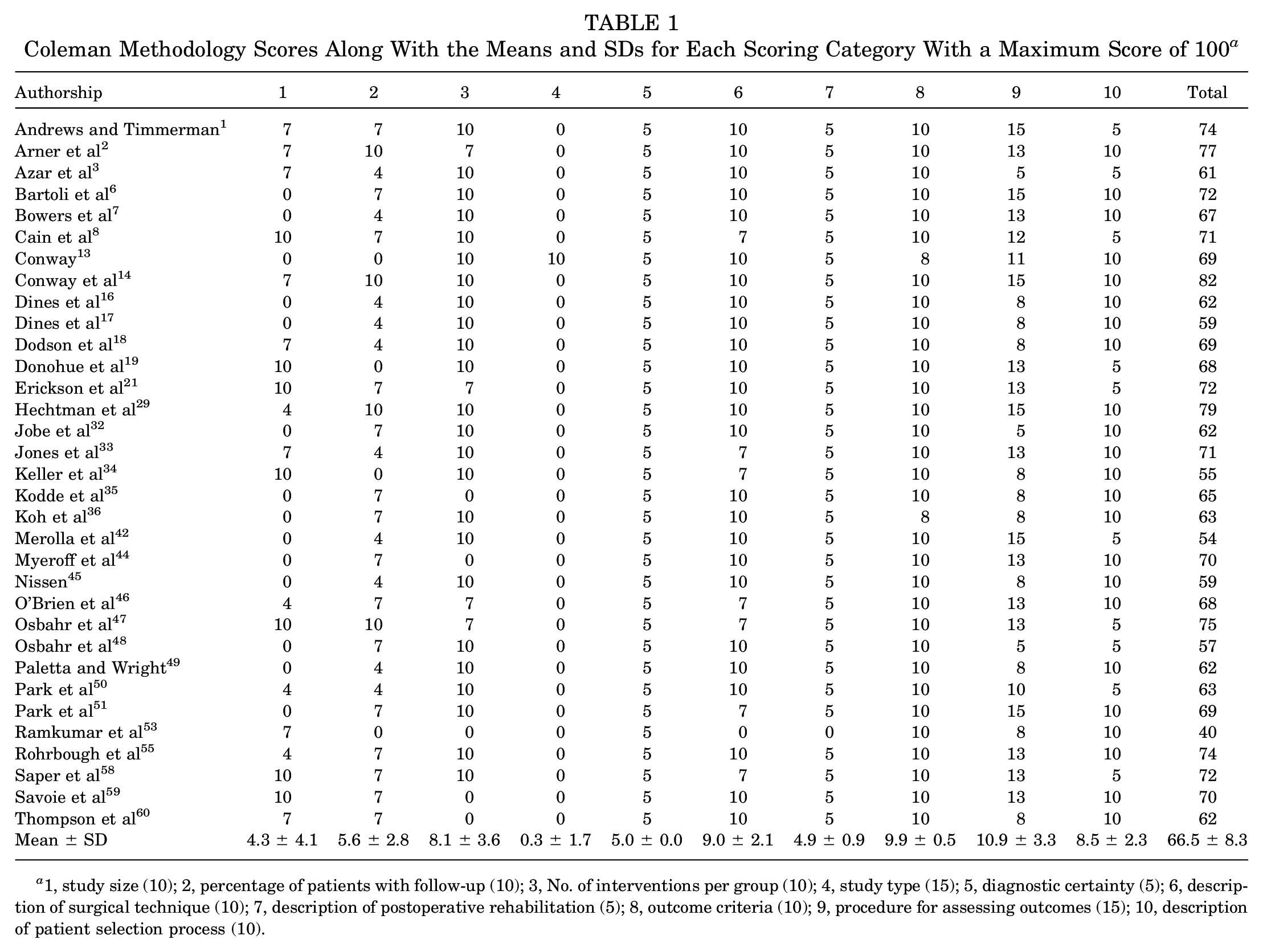
1, study size (10); 2, percentage of patients with follow-up (10); 3, No. of interventions per group (10); 4, study type (15); 5, diagnostic certainty (5); 6, description of surgical technique (10); 7, description of postoperative rehabilitation (5); 8, outcome criteria (10); 9, procedure for assessing outcomes (15); 10, description of patient selection process (10).
RTS Value Assessment
Each article was scored from 0 to 4 on its RTS criteria according to the methodology presented by Zaman et al. 64 One point was awarded when an article reported the use of a rehabilitation protocol, a desired timeline for RTS, the use of specific conditional criteria for RTS, or the use of specific measurements when returning an athlete to sport (Table 2).
Scoring Report for the RTS Value Assessment a
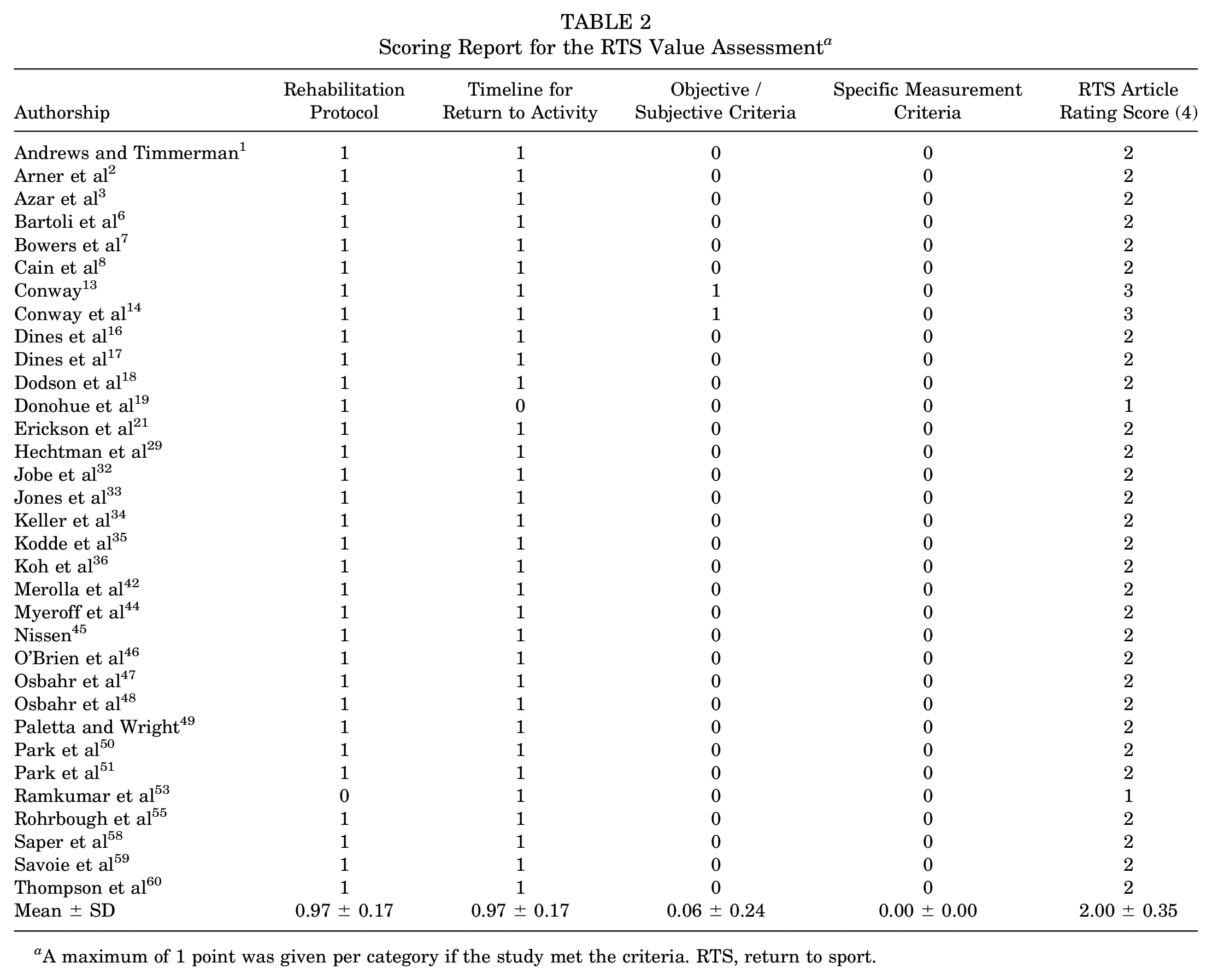
A maximum of 1 point was given per category if the study met the criteria. RTS, return to sport.
Study Design and Statistical Analysis
All data were collected and analyzed using Microsoft Excel. PRISMA criteria were followed throughout the systematic review (Figure 1).
Results
General Cohort Characteristics and Demographics
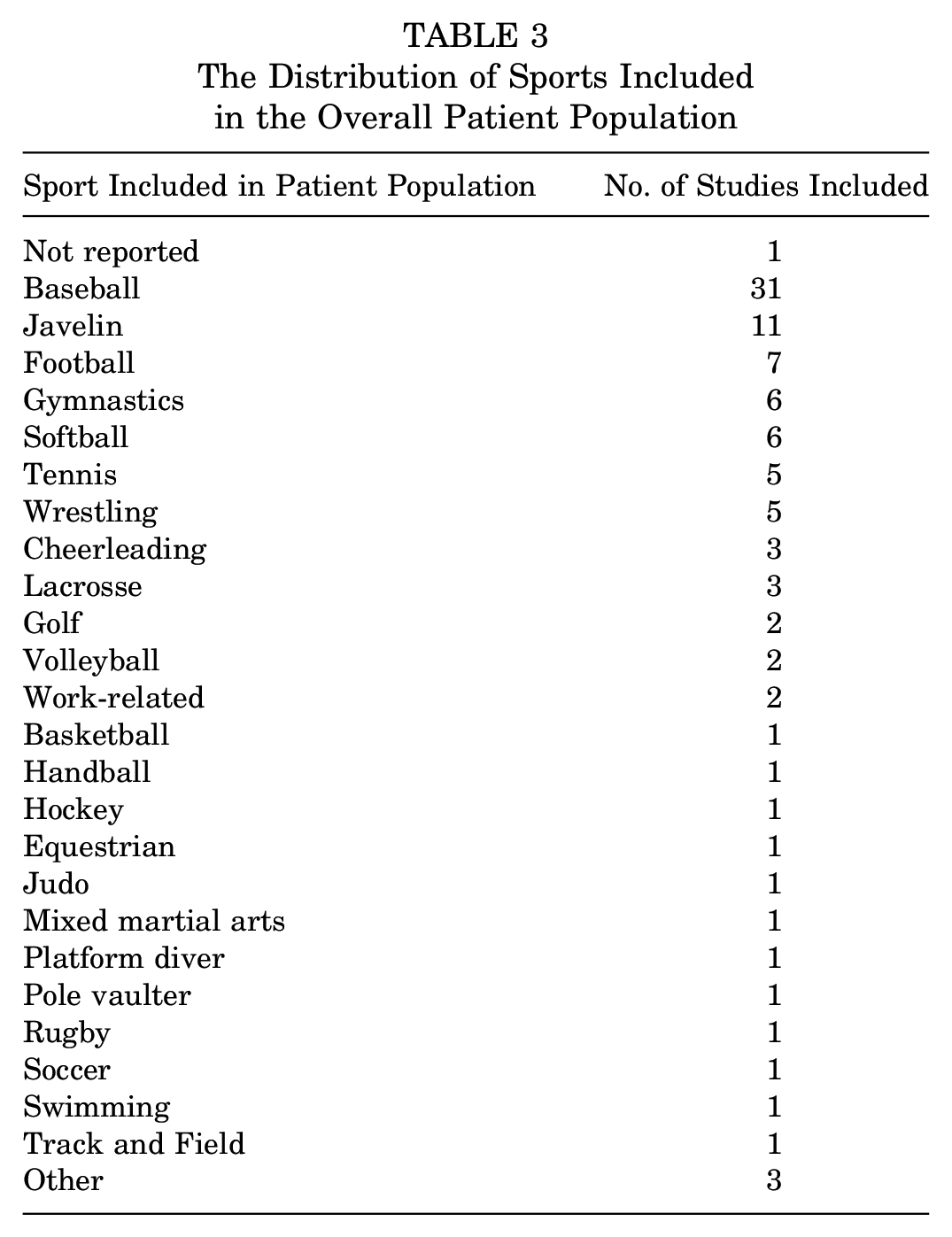
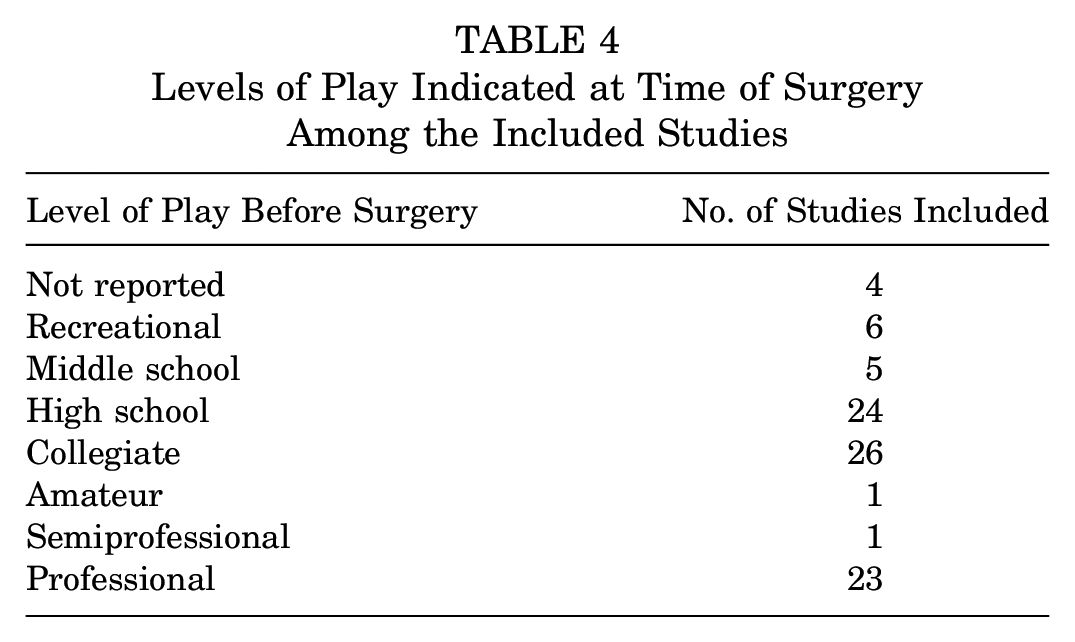
A total of 1346 unique published articles were eligible for inclusion. After implementation of inclusion and exclusion criteria, 33 studies were included in the analysis. The final 33 studies comprised 3480 patients (1519 male patients, 95 female patients, sex data unavailable for 11 studies [1866 patients]) and 3480 elbows who underwent UCLR. While UCLR was most commonly performed in baseball players, the studies in this review comprised athletes from 21 different sports across various levels of play (Tables 3 and 4). 23 In addition to athletes, there were 2 studies that included patients with work-related injuries in their analysis. Regarding the levels of evidence, 29 studies were level 4 studies and 4 studies were level 3.
The Distribution of Sports Included in the Overall Patient Population
Levels of Play Indicated at Time of Surgery Among the Included Studies
The surgical techniques varied widely across the 33 papers with Docking, Modified Jobe, Jobe, and modified Tommy John comprising the 4 most common techniques. Among grafts used in the studies, the use of autograft was far more common than allograft and a total of 9 different graft sources were utilized (Table 5).
UCLR Graft Sources Utilized Across the Included Study Patient Population a
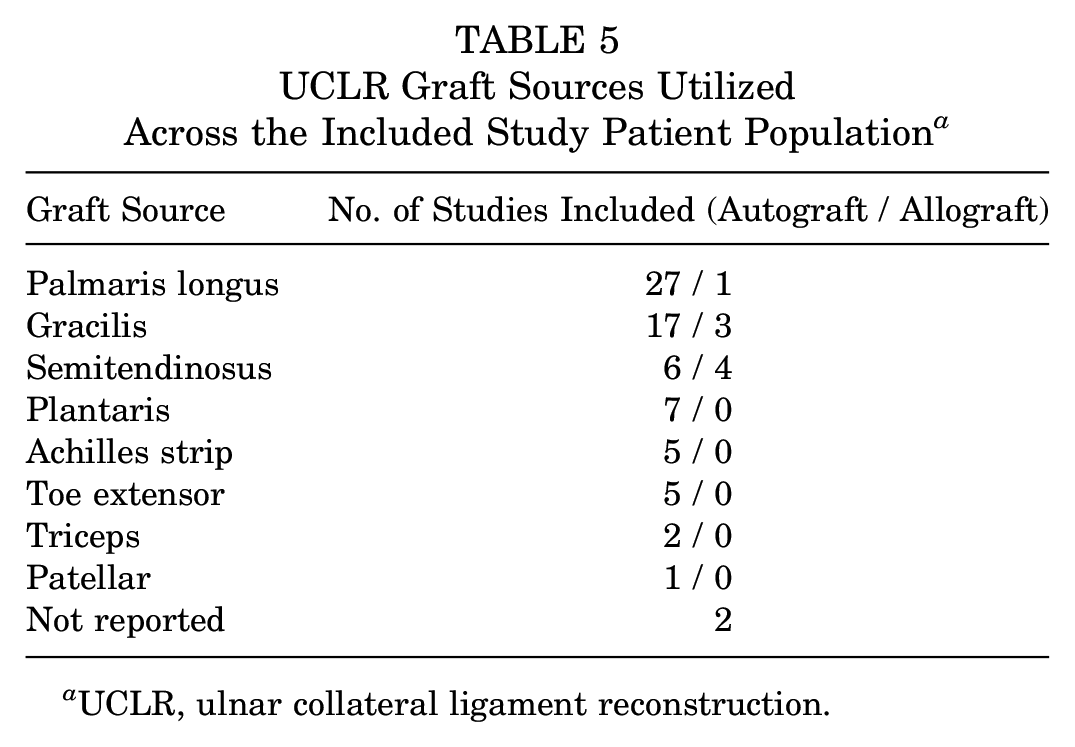
UCLR, ulnar collateral ligament reconstruction.
Quality of Literature
The quality of literature as determined by the CMS was fair (66.5 ± 8.3) with the majority of articles reporting good diagnostic certainty of the pathology, as well as adequate follow-up and compliance rates of the included patients (Table 1).
Postoperative Rehabilitation Parameters
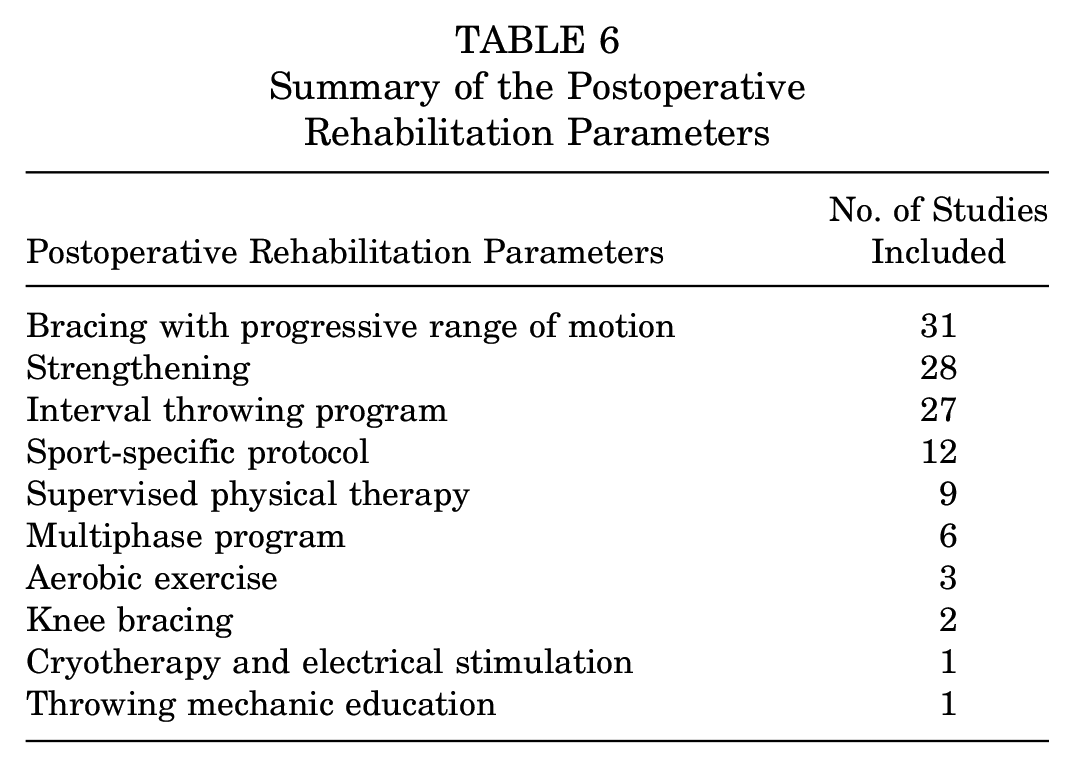
Postoperative rehabilitation parameters were detailed in 32 of the 33 studies. Information regarding the rehabilitation protocols was extracted and recurring themes are noted and summarized in Table 6. Twelve specific components of each protocol were extracted. Notably, early bracing with progressive ROM (93.9%), strengthening (84.8%), and participation in an interval throwing program (81.8%) were the most common parameters emphasized in these rehabilitation protocols. Twelve studies did indicate utilization of sport-specific protocols; however, only Dines et al 17 (javelin) and Jones et al 33 (javelin and gymnasts) detailed protocols that included sport-specific changes. Nine studies included use of formal supervised physical therapy. Six studies utilized a multiphasic approach, which varied between 4 and 5 phases. Other lesser utilized parameters (range, 1-6 studies) were as follows: aerobic exercise; knee bracing (to protect pes anserinus donor site after semitendinosus and/or gracilis autograft harvest); cryotherapy and electrical stimulation; and throwing mechanics education.
Summary of the Postoperative Rehabilitation Parameters
RTS Criteria
Time From Surgery
The timeline variations for RTS are fully listed in Table 7. Timing for return to play was detailed in 22 studies (66.67%). The earliest time to RTS was 6.5 months, while the longest time reported was 12 to 16 months. A total of 29 studies (87.88%) detailed timing for return to throwing, with the majority using 4 months (18 studies; 62.07%). Arner et al 2 was the only study to mention timing for return to hitting, which was described as 8 months.
Return to Competitive Sport Timelines a
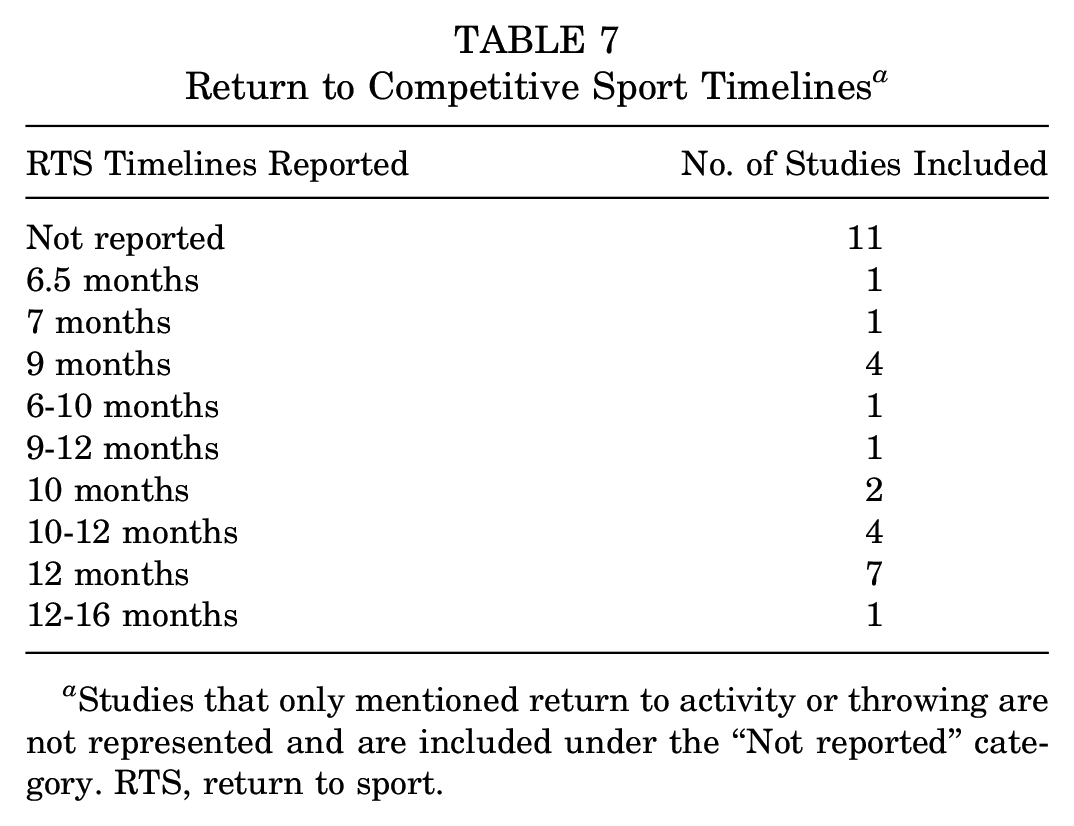
Studies that only mentioned return to activity or throwing are not represented and are included under the “Not reported” category. RTS, return to sport.
Conditional RTS Criteria
Other RTS criteria that were analyzed from the collected articles included any conditional criteria, whether objective or subjective, that the authors employed as a threshold for returning to sport activity. Only 2 articles used language that suggested that they used any sort of conditional criteria for RTS.13,14 In both cases, the authors described that for athletes to RTS they must report having no pain, normal upper extremity strength, and re-establishment of balance, coordination, and rhythm while throwing.13,14
Specific Measurements for RTS
No study reported the use of specific measurements with respect to ROM or imaging modalities such as ultrasound or magnetic resonance imaging assessment as a criterion for RTS.
RTS Value Assessment
All 33 studies included in this review reported at least 1 of the following 3 metrics of RTS criteria: rehabilitation protocol, return to activity timeline, and objective/subjective criteria. Overall, 32 of 33 studies (96.97%) detailed their postoperative rehabilitation protocol and 32 of 33 studies (96.97%) reported some type of expected timeline to return to throwing, sport, or full activity. Only 3 studies (9.09%) included conditional RTS criteria.3,13,14 No articles reported specific measurements (eg, ROM, strength) required for RTS. Overall, each article was rated on a scale from 0 to 4 in order to judge its value in reviewing RTS criteria as presented by Zaman et al. 64 Similar to their review, none of the included studies reached a 4/4 on this scale, meaning no article was able to effectively define RTS criteria after UCLR. Notably, only 2 articles received a rating of 3 and the other 31 articles received either a 2 or a 1 on this scale. The precise scoring of each article is listed in Table 2.
RTS Rates
RTS rates were reported in all 33 included studies. A total of 20 studies reported RTS rates utilizing the Conway-Jobe scale, 19 reported overall RTS percentages, and 6 reported RTS using both methods. Of the 20 studies, 13 (65%) achieved ≥80% with excellent outcomes according to the Conway-Jobe scale, with 4 achieving ≥90%. The range for excellent outcomes was 62.5 to 94.1. Only 4 studies reported good outcomes (range, 6.25-24), 3 reported fair outcomes (range, 1-14), and 2 reported poor outcomes (range, 2-5). One study reported the excellent and good outcomes combined as 88%. For overall RTS percentages, 17 of 19 studies (89.5%) achieved ≥80% RTS success as defined by the authors. The majority of overall RTS success was ≥90% (12 of 19 studies; 63.2%), with an overall range of 78% to 100%.
Discussion
Despite the increased frequency with which UCLR procedures are being performed, validated rehabilitation protocols as well as objective postoperative measurement data, including imaging and objective physical examination, are glaringly lacking in the literature. The authors’ hypothesis was correct, as 96.97% of studies utilized some sort of time-based criteria before athletes returned to activity.
Early bracing with progressive ROM was the most clearly indicated postoperative rehabilitation metric, which has been a mainstay of orthopaedic surgery for decades in order to protect the articular cartilage; assist in the synthesis, alignment, and organization of collagen tissue; and prevent scar formation.37,56,57,61 The implementation of this in conjunction with strengthening, neuromuscular control, and plyometric exercises for the duration of physical therapy has largely been the standard of care for elbow surgery in the overhead athlete since Wilk et al 61 published guidelines for rehabilitation of the thrower’s elbow in 1993. This article was revised in 2004 to include the interval throwing program originally defined by Reinold and colleagues.54,62 This throwing program formed the basis for those described in the majority of the articles reviewed; however, subsequent variations and modifications have not been well-documented, and despite evidence that pitch velocity may increase after UCLR, there is a paucity of defined objective criteria that may dictate progression through rehabilitation. 40
While postoperative time to return to activity was widely reported across the studies included in the review, disparity among surgeons still exists concerning the appropriate postoperative recovery timeline. In his initial study, Dr. Jobe 32 suggested >1 year for the graft to incorporate fully and therefore recommended a recovery timeline of 12 to 18 months before returning to pitching. The shortest timeline for RTS documented among the 33 studies was 6.5 months, while the longest was 16 months.3,34 A recent systematic review of 14 studies found that the mean time to RTS for baseball pitchers was 19.8 ± 13.5 months, and the mean time to return to competition for MLB pitchers was 17.3 ± 2.4 months. 16 Similar to the current study, Coughlin et al 15 found a large variation in the mean time to return to pitching (range, 11.5-20.5 months). This is likely due to differences in reporting RTS versus RTS at prior competitive level; however, several studies do not overtly outline this. A more accurate timeline would include time to initiating and completing an interval throwing program, time to return to competition, and time to return to prior level of sport. Timing of RTS is an important variable for professional development and reacclimatization to competition, but more study may be needed to determine risk of failure and/or subsequent revision as it pertains to timing. In a 2017 study by Erickson et al, 22 the authors found that pitchers who underwent UCLR and went on to require revision UCLR returned to their prior level of play on average >2 months earlier than those who did not require revision surgery. With quite a large range, however, this finding was not statistically significant.
Utilization of a published rating scale for identifying well-defined rehabilitation protocols is an advantage of the current review and validates the principal finding that the current literature inadequately defines the functional and objective guidelines for RTS after UCLR. 64 A recent systematic review analyzed UCLR rehabilitation protocols published online and found notable variability in both the composition and the timing of rehabilitation components. 38 Only 2 of the 33 studies analyzed in our study included defined subjective and/or objective criteria for rehabilitation, and none included specific radiographic or biomechanical measurements. While analysis suggests that early bracing and progressive ROM followed by strengthening and interval throwing likely form the foundation of a rehabilitation protocol, the conspicuous absence of any defined checklist in these studies highlights an area in need of improvement. RTS criteria are seemingly better defined in the anterior cruciate ligament reconstruction literature, with the incorporation of functional and dynamic testing becoming popularized and more frequently utilized.5,30 There appears to be a shift from chronologically based RTS toward a checklist of functionally based criteria.4,5,20 Pitchers who underwent UCLR and successfully returned to sport have been compared with uninjured pitchers and shown to have nearly identical biomechanics; however, these studies failed to include the functional and dynamic exercises and/or their measurements during postoperative rehabilitation.26,27
Most surgeons and team medical and training personnel approach RTS with a more nuanced protocol than those published. However, it remains a significant limitation that postoperative rehabilitation protocols and monitoring are not routinely published or discussed. Despite high return-to-play rates, reinjury remains a significant concern for these athletes. A retrospective multi-institutional study found that while graft type and reconstruction method used do not significantly influence postoperative performance in MLB players, subsequent throwing elbow injury in this cohort is as high as 46.3%. 28 A 2018 meta-analysis 52 found that 90% of athletes who underwent UCLR were able to RTS; however, the authors also determined that only 79% returned to their prior level of play.24,52 The current review included studies of gymnasts, javelin throwers, volleyball players, and football players, among others. RTS rates were not significantly different in these patient populations; however, descriptions of functional rehabilitation including specialized training are lacking and may help explain the discrepancy between those athletes who return to prior competition levels and those who do not. Studies on RTS after UCLR are much more numerous in the baseball literature than other sports; one of the goals of this study was to therefore analyze rehabilitation parameters for athletes competing in different sports in an attempt to identify universal protocols. It should be recognized, however, that sport-specific protocols certainly vary among athletes returning to different sports, and future studies should investigate these individual nuances.
Limitations
It is possible that several physicians or groups who regularly perform UCLR have published rehabilitation protocols and RTS criteria either on personalized web pages or as physical documents for patients, therapists, and team personnel. In an effort to remain standardized, this review followed a methodology used previously in studies of RTS criteria and would have therefore excluded any such published protocols.10,64 Second, there was a wide variability in the competitive level of athletes, with levels of play ranging from amateur to professional. It is likely that higher level athletes have a more personalized and sport-specific rehabilitation protocol. Additionally, there was inconsistency and/or absence of PRO scoring systems or metrics utilized in the included studies. The decision was therefore made to not include PROs despite their typical utility in surgical outcomes literature. Finally, this systematic review included 12 different surgical reconstructive techniques and variability in postoperative milestone timing and ultimate RTS may be partially due to differences among these techniques.
Conclusion
Overall, 93.9% of studies report utilizing bracing with progressive ROM, 84.8% reported strengthening, and 81.8% reported participation in an interval throwing program as rehabilitation parameters after UCLR. In addition, 96.97% reported timing after surgery as a criterion for RTS; however, there is a wide variability within the literature on the recommended time from surgery to return to activity. Future research should focus on developing a comprehensive checklist of functional and performance-based criteria for safe RTS after UCLR.
Supplemental Material
sj-pdf-1-ajs-10.1177_03635465211033994 – Supplemental material for Rehabilitation and Return to Sport Criteria Following Ulnar Collateral Ligament Reconstruction: A Systematic Review
Supplemental material, sj-pdf-1-ajs-10.1177_03635465211033994 for Rehabilitation and Return to Sport Criteria Following Ulnar Collateral Ligament Reconstruction: A Systematic Review by Bryson R. Kemler, Somnath Rao, Donald P. Willier, Robert A. Jack, Brandon J. Erickson, Steven B. Cohen and Michael G. Ciccotti in The American Journal of Sports Medicine
Footnotes
Submitted December 1, 2020; accepted March 30, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: R.A.J. has received educational support from Liberty Surgical and hospitality payments from Pacira Pharmaceuticals. B.J.E. has received consulting fees from Arthrex and research support from Arthrex, DePuy, Linvatec, Smith & Nephew, and Stryker. S.B.C. has received consulting fees from CONMED Linvatec, Zimmer, and Zimmer Biomet Holdings; and publishing royalties from Slack Inc. M.G.C. has received a grant from DJO and educational support from Liberty Surgical Inc. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.