
Abstract
Background:
Arthroscopic-assisted meniscal allograft transplantation (MAT) has become a viable and effective treatment option for young active patients with postmeniscectomy pain. The minimal clinically important difference (MCID) of patient-reported outcome measures (PROMs) is imperative to evaluate the clinical significance of surgical interventions and inform clinical practice guidelines in orthopaedic surgery.
Purpose:
To perform a systematic review of clinical outcome studies of patients undergoing MAT and compare postoperative improvement with established MCID thresholds.
Study Design:
Systematic review and meta-analysis; Level of evidence, 4.
Methods:
A systematic review was performed using the PubMed, Web of Science, and Cochrane Library databases. A meta-analysis was performed using data obtained from studies reporting patient-reported outcomes. Subgroup analysis was performed on patients undergoing isolated lateral MAT using fresh-frozen grafts. Weighted mean postoperative improvements in the International Knee Documentation Committee (IKDC), Lysholm, and visual analog scale for pain (VAS pain) were calculated and compared with MCID values to determine if they met the MCID threshold.
Results:
A total of 35 studies were identified, including 1658 unique patients. Weighted mean postoperative score improvements exceeded MCID thresholds for the VAS pain, IKDC, and Lysholm. Subgroup analysis of patients undergoing isolated lateral fresh-frozen MAT demonstrated postoperative improvements exceeding the MCID for the Lysholm and VAS pain.
Conclusion:
Evaluating postoperative PROMs with respect to the MCID is crucial to evaluate the effect of MAT on functional improvement. The results of the present meta-analysis suggest that postoperative improvements after MAT are clinically meaningful as reflected by PROMs exceeding the MCID threshold for the IKDC, Lysholm, and VAS pain.
Keywords
The meniscus is an important structure for biomechanical joint stability, load mechanics, proprioception, and lubrication. The multifaceted importance of the meniscus is highlighted in patients after meniscectomy, who often experience pain, loss of function, and early degenerative osteoarthritis in the knee.25,28 For select patients with meniscal deficiency, meniscal allograft transplantation (MAT) is a viable treatment option to delay degenerative changes. 45
MAT is generally considered safe and reliable for treatment of refractory postmeniscectomy symptoms. Recent retrospective cohort and systematic review studies have demonstrated improvements in clinical and radiographic outcomes for up to 10 years after MAT.29,39,40 However, no systematic review or meta-analysis has evaluated whether postoperative improvements after MAT are clinically relevant, as reflected by the minimal clinically important difference (MCID) threshold.
The MCID is a value defined as the minimum difference in a given patient-reported outcome measure (PROM) that is reflective of a patient’s detectable improvement. MCID thresholds have been established for individual surgical interventions and PROMs. 12 It is well-established in the orthopaedic literature that improvements in PROMs must be compared with MCID thresholds to determine not just statistical but also clinical significance.5,10,26 The purpose of this study was to perform a systematic review of clinical outcome studies of patients undergoing MAT and to compare postoperative improvements with MCID thresholds.
Methods
A systematic review of the PubMed, Web of Science, and Cochrane Library databases was performed on November 15, 2019. The search query performed was “(meniscal allograft) OR (meniscus allograft) OR (meniscal graft) OR (meniscus graft).” All Medical Subject Headings terms were included. Duplicate studies and published abstracts without an associated full-text article were excluded.
After the primary search, a manual review of titles and abstracts of the remaining papers was performed in accordance with the standard PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) checklist. 23 If relevant information was identified, articles were systematically assessed to determine compliance with the following inclusion criteria: (1) a minimum of 5 patients (eg, no case reports or small case series), (2) surgical intervention consisting of arthroscopic-assisted MAT, (3) minimum 1-year clinical follow-up, and (4) study published in the English language. Articles were excluded if they were systematic reviews, meta-analyses, review articles, or technique guides. Cadaveric, animal, and in vitro studies were also excluded. Studies describing revision and MAT with an open technique were excluded, as the arthroscopic-assisted technique is the current standard of care. Remaining articles then underwent full-text review for further application of the inclusion and exclusion criteria.
Studies meeting criteria were used to extract a cohort of patients who had undergone MAT. For each study, the following cohort information was collected: number of patients, age, sex, length of follow-up, location of transplant (medial/lateral), fixation technique (bone plugs, keyhole technique, soft tissue), method of allograft preservation (cryopreserved, fresh-frozen), and concomitant surgery. All reported clinical baseline and follow-up outcome scores were collected and reviewed. Visual analog scale for pain (VAS pain), International Knee Documentation Committee (IKDC), and Lysholm were selected for the analysis, as they were the most commonly utilized PROMs among studies. In addition, IKDC and Lysholm scores have established MCID values for MAT specifically.
In studies not reporting necessary descriptive data for the clinical outcome scores (mean and standard deviation at baseline and follow-up), the study’s primary author was contacted to request this information. Studies with incomplete data and authors who did not respond were excluded from the meta-analysis. Studies with patient populations from the same institution that took place in the same time frame were deemed to cover duplicate patient populations, and the more recent study was included and the less recent excluded.
Cohorts were combined from included studies by performing a meta-analysis utilizing inverse variance weighting in a DerSimonian-Laird random-effects model. Weighted mean preoperative to most recent postoperative improvements in IKDC, Lysholm, and VAS pain scores were calculated. For each outcome score, postoperative improvement was calculated as the weighted mean difference between baseline preoperative and follow-up postoperative scores and compared with MCID values for outcomes after knee injuries (IKDC = 16.7, Lysholm = 10.1, and VAS pain = 2.7), as reported by the AOSSM Outcomes Task Force. 9 MAT-specific MCID values 24 were also used (IKDC = 9.9, Lysholm = 12.3); no such value was found for VAS pain score. MAT-specific MCID values were determined with preoperative and 1-month postoperative PROMs and based on a distribution method, which halves the standard deviation of the difference between pre- and postoperative scores.
Mean values were compared with previously established and MAT-specific 24 MCID values to determine if they significantly exceeded the MCID using 2-tailed 1-sample Student t tests. A random-effects model was chosen because it is the most appropriate and conservative method for assessment in the setting of possible study heterogeneity and it accounts for within- and between-study variance. Furthermore, random-effects modeling is considered to be appropriate in medical decision-making contexts. A subgroup analysis of patients undergoing isolated lateral MAT using fresh-frozen grafts was performed in the same fashion for Lysholm and VAS pain scores.
Results
The PRISMA flowchart (Figure 1) outlines the inclusion and exclusion criteria applied to the 2197 unique published articles identified in the initial search. In total, 35 studies met the study inclusion criteria, with 1658 unique patients.
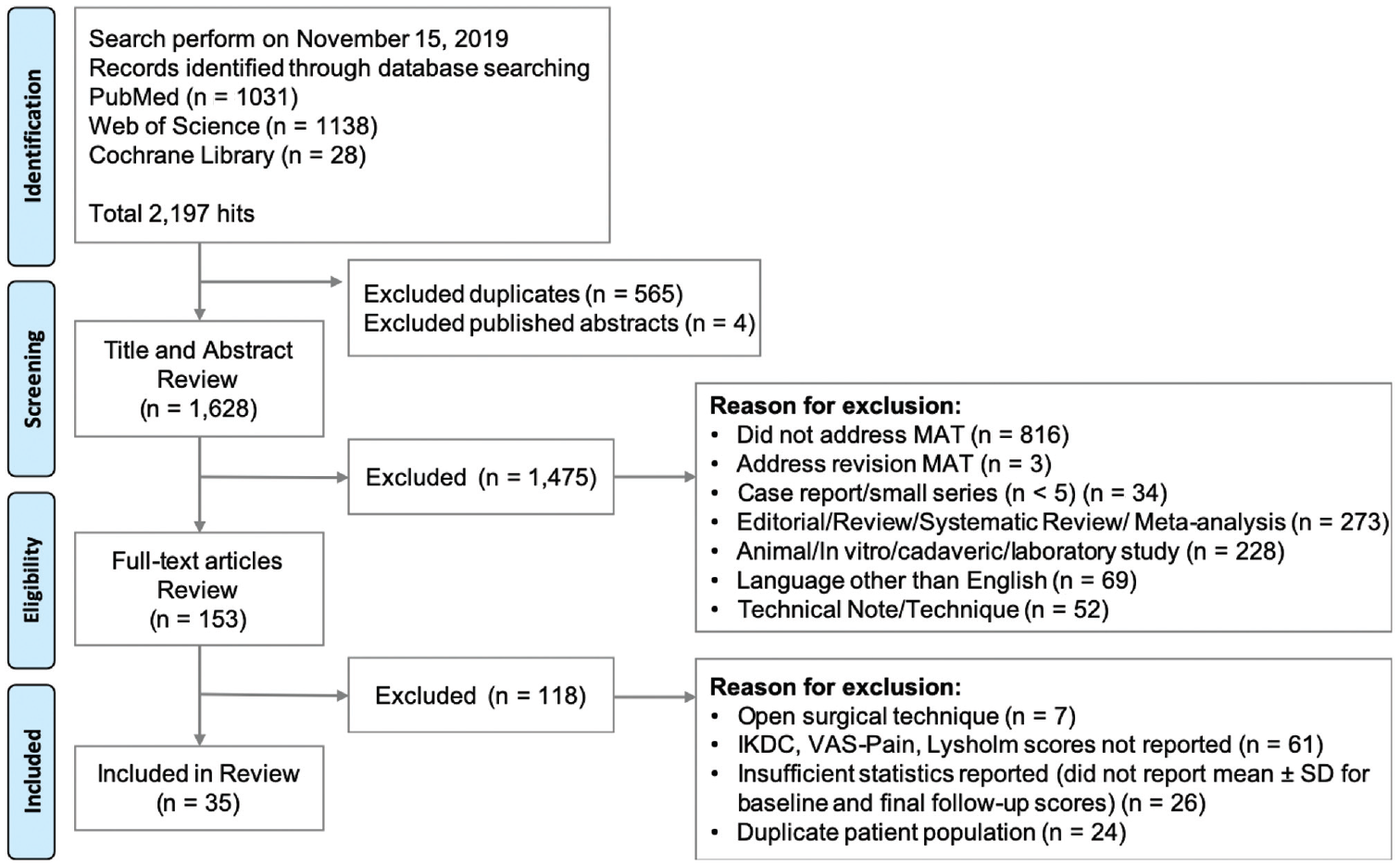
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart outlining application of inclusion and exclusion criteria. IKDC, International Knee Documentation Committee; MAT, meniscal allograft transplantation; VAS, visual analog scale.
Of the 35 studies meeting inclusion criteria, 14 reported on VAS pain scores (Table 1), ** 16 on IKDC scores (Table 2), †† and 30 on Lysholm scores (Table 3). ‡‡
Articles Identified in Systematic Review Reporting VAS Pain Score a
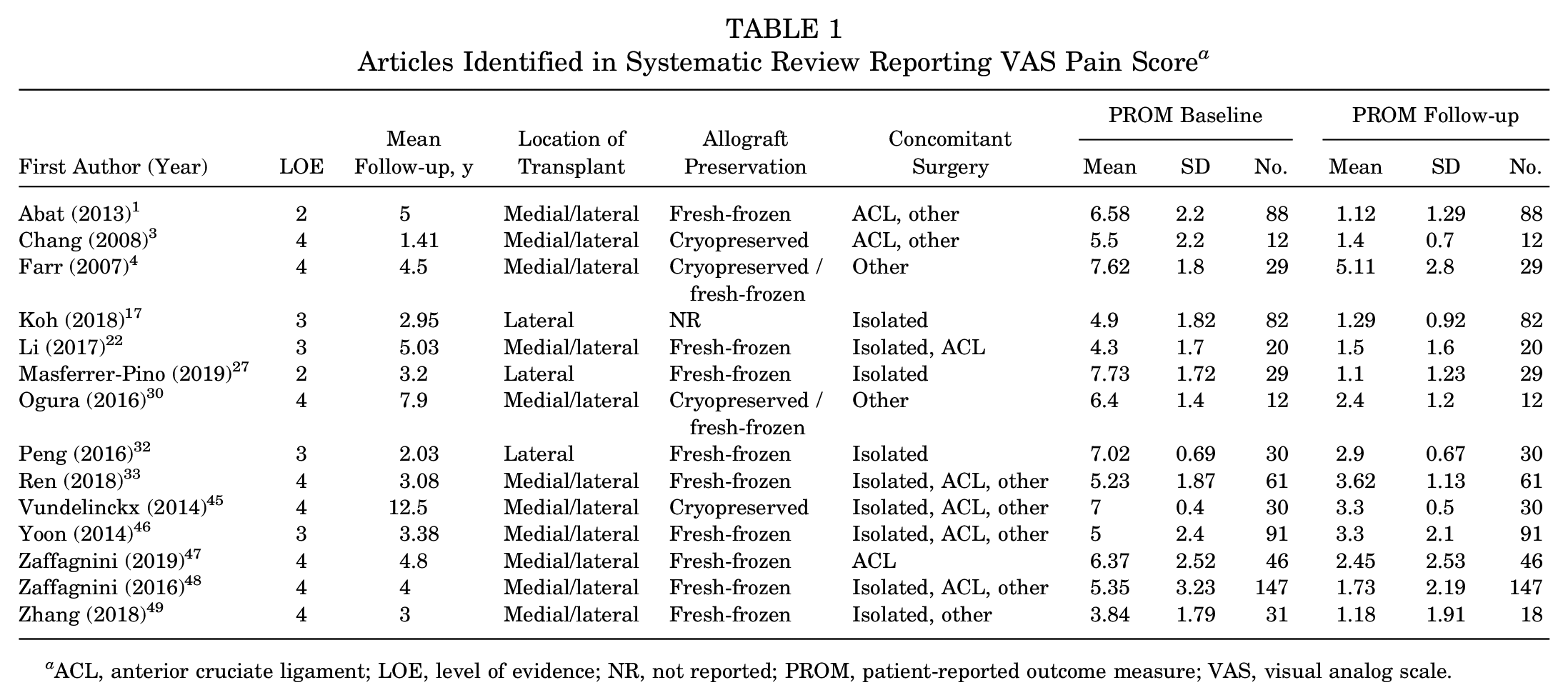
ACL, anterior cruciate ligament; LOE, level of evidence; NR, not reported; PROM, patient-reported outcome measure; VAS, visual analog scale.
Articles Identified in Systematic Review Reporting IKDC Score a
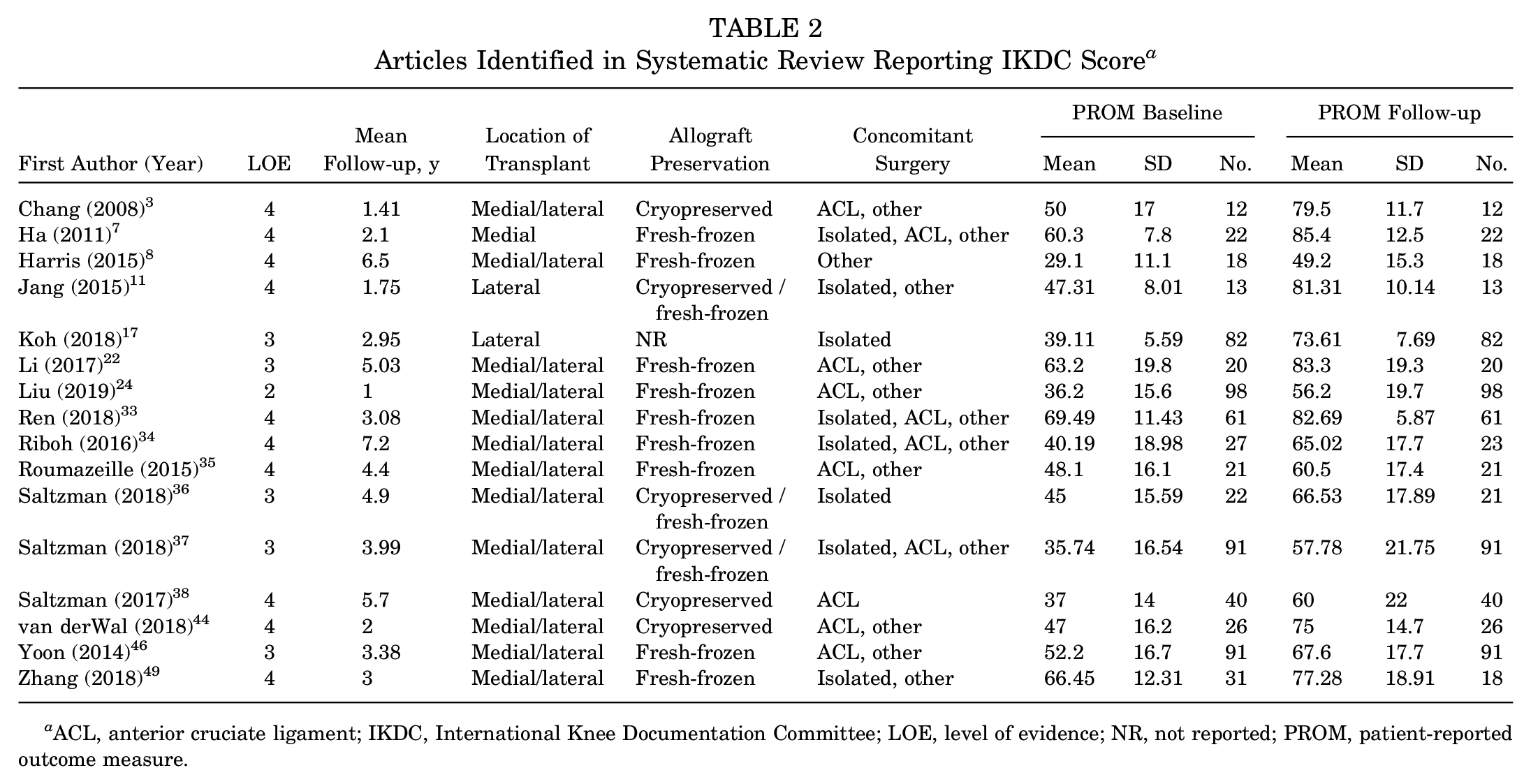
ACL, anterior cruciate ligament; IKDC, International Knee Documentation Committee; LOE, level of evidence; NR, not reported; PROM, patient-reported outcome measure.
Articles Identified in Systematic Review Reporting Lysholm Score a
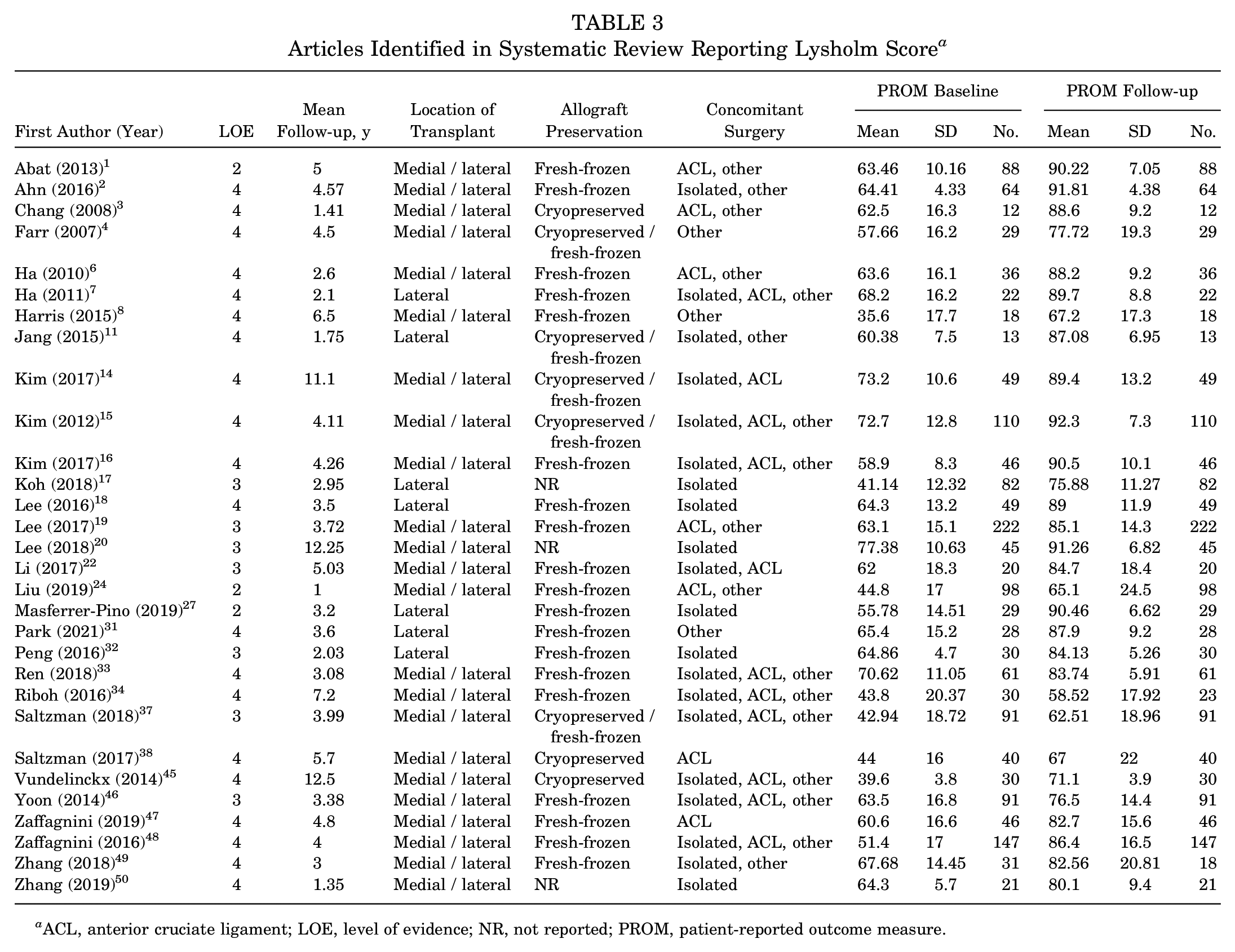
ACL, anterior cruciate ligament; LOE, level of evidence; NR, not reported; PROM, patient-reported outcome measure.
Mean published improvements in outcome scores exceeded the MCID in all categories for the IKDC, Lysholm, and VAS pain scores for all studies during the meta-analysis. Individually, the MCID was exceeded in 12 of 14 studies for the VAS pain, 12 of 16 for the IKDC, and 30 of 30 for the Lysholm. Regarding MAT-specific MCID values, improvements in outcomes were also found for the IKDC and Lysholm scores (Table 4). Subgroup analysis of patients undergoing isolated lateral MAT using fresh-frozen grafts demonstrated that postoperative improvements exceeded MCID thresholds for Lysholm and VAS pain scores (Table 5). None of the included studies reported the IKDC score in this subgroup of patients.
Mean Improvement in PROMs for All Patients vs Previously Published MCID a
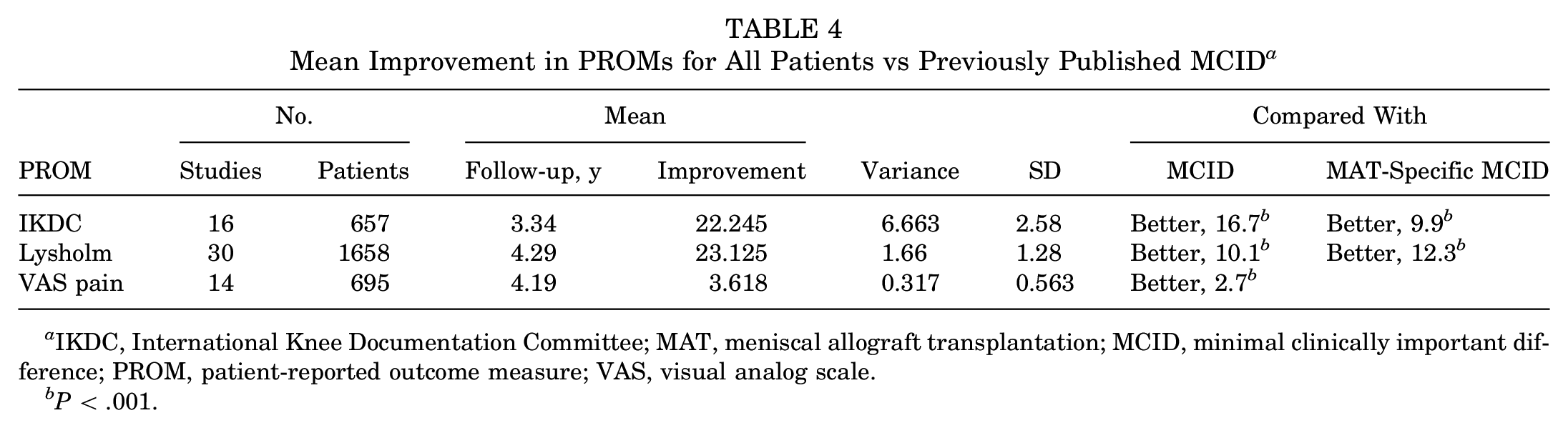
IKDC, International Knee Documentation Committee; MAT, meniscal allograft transplantation; MCID, minimal clinically important difference; PROM, patient-reported outcome measure; VAS, visual analog scale.
P < .001.
Mean Improvement in PROMs for Patients Who Received Isolated Lateral MAT Using Fresh-Frozen Grafts vs Previously Published MCID a
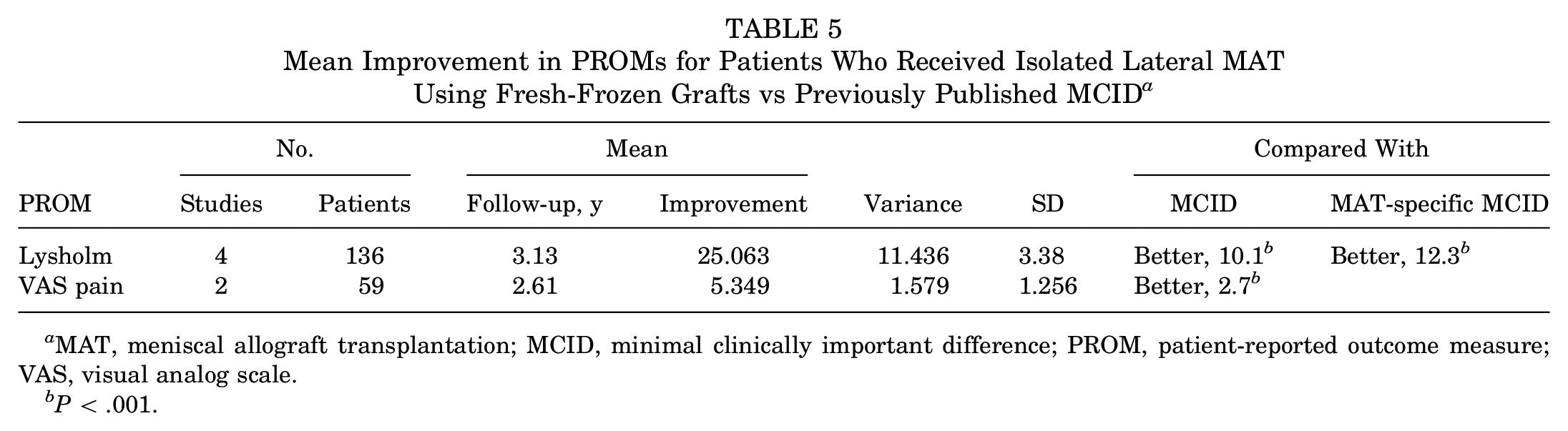
MAT, meniscal allograft transplantation; MCID, minimal clinically important difference; PROM, patient-reported outcome measure; VAS, visual analog scale.
P < .001.
Discussion
Arthroscopic-assisted MAT is a viable and effective treatment option for young active patients with postmeniscectomy pain25,40 and a useful tool in the armamentarium utilizing the concept of “biological knee reconstruction.”13,30 While many studies have demonstrated improvements in clinical and radiographic outcomes for up to 10 years after MAT, there has been no systematic evaluation of these outcomes relative to MCID thresholds. The MCID threshold reflects not just statistical but also clinical significance and is imperative to include when assessing the effect of an intervention. To address this knowledge gap, the present systematic review and meta-analysis is the first study to assess PROMs with respect to the MCID after MAT. The results of the meta-analysis show that postoperative improvements in PROMs after MAT exceeded the MCID threshold for the IKDC, Lysholm, and VAS pain. In addition, subgroup analysis indicated that lateral fresh-frozen MAT met the MCID for the Lysholm and VAS pain.
Defining outcomes is challenging in the field of MAT and postmeniscectomy pain. 42 Historically, the primary outcome of interest has been survivorship as continued improvement without need for reoperation or radiographic evidence of extrusion or retear, which is reported to be between 10 and 16 years with an overall failure rate of 10% to 29% (need for revision, knee arthroplasty, pain on daily living).29,39 However, as MAT and the biological reconstruction treatment paradigm aim for postponement rather than prevention of arthroplasty, alternative outcome measures including PROMs become more important to consider.40,43 Several studies reporting clinical outcomes of MAT have demonstrated improved symptoms, function, and quality of life at 7 to 14 years of follow-up.39,41 Yet, PROMs represent only part of the picture regarding a patient’s return to function and activity. Other nonpatient measures, such as reoperation rates and range of motion testing, were seen and should continue to be recorded as measures of success.
While the present study is the only systematic review and meta-analysis to evaluate PROMs with respect to the MCID after MAT, 2 retrospective cohort studies did utilize MCID thresholds. Saltzman et al 37 reported on 91 patients treated with MAT, 22 of them without chondral defects and 69 with full-thickness chondral defects treated with cartilage restoration procedures at the time of MAT, with a mean follow-up of 4.48 and 3.84 years, respectively. Improvements in the Lysholm, IKDC, Knee injury and Osteoarthritis Outcome Score (KOOS), and 12-Item Short Form Health Survey exceeded the MCID at 2 years and final follow-up, irrespective of the presence or absence of full-thickness chondral defects treated at the time of MAT. However, Zhang et al 49 evaluated 31 patients who had undergone lateral MAT with intra-articular platelet-rich plasma injection with a mean follow-up of 37 months. That study demonstrated that PROM improvements exceeded the MCID for the Lysholm, IKDC, and Tegner but not the Western Ontario and McMaster Universities Osteoarthritis Index or VAS pain. According to the authors, 1 possible reason for the smaller improvements was the higher preoperative score levels, as surgery was performed early after the initial evaluation.
Both studies utilized non–MAT specific values in their analyses. As MCIDs are diagnosis and intervention specific, these values can have a large amount of variation, leading to a number of problems with interpretation. Establishing these threshold scores specific to a procedure of interest allows physicians to reliably measure clinical improvements after surgery. Liu et al 24 established values for the MCID and Patient Acceptable Symptom State for patients undergoing MAT with respect to the Lysholm (12.3 and 66.5), IKDC (9.9 and 36), and KOOS. They also found that lower preoperative PROM scores were associated with achieving the MCID. In our study, MAT met these MAT-specific MCID values.
This study has several limitations. The most important limitation lies in the heterogeneity found across included studies. The wide range of concomitant procedures, surgical techniques, length of follow-up, and preservation methods may have influenced results. While we did attempt to track these variables, we had only enough information to do meaningful statistical analysis of graft preservation on isolated lateral MAT using fresh-frozen grafts. Data were heavily skewed toward early and midterm follow-up with very few studies having follow-up past 10 years. Additionally, each study reported the follow-up data as a cohort-level statistic rather than an individual-level statistic. Therefore, given the wide variability of follow-up length, even within each study, there is too much crossover per study/cohort between time points such that doing a subgroup analysis would be impossible. However, Lee et al 20 found no difference in postoperative PROMs between isolated MAT and MAT combined with other procedures. Second, a variety of PROMs were used among the study populations. We used only the IKDC, Lysholm, and VAS pain scores, as they were the most commonly observed among studies and these validated outcome tools have established MCID values. Finally, there was variable follow-up, and unfortunately, just 3 studies with long-term follow-up (>10 years) were included.
Conclusion
Evaluating clinical improvement with respect to the MCID is essential to assess the meaningful, not just statistical, effect of MAT on patient outcomes. The results of this study demonstrate that the majority of patients undergoing MAT reached or exceeded PROM MCID thresholds, indicating the procedure’s positive effect on patient outcomes.
Footnotes
Submitted August 12, 2020; accepted March 26, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: K.J.J. has received research support from Aesculap/B. Braun and Musculoskeletal Transplant Foundation and consulting fees from Arthrex Inc, CONMED Linvatec, JRF Ortho, and Vericel Corporation. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.