
Abstract
Background:
Commercially available products used in knee cartilage reconstructive and restorative surgical practices fall under unique US Food and Drug Administration (FDA) regulatory pathways that determine the level of evidence required to market each product.
Purpose:
To evaluate the levels of evidence in the literature supporting commercially available cartilage repair procedures stratified by FDA regulatory pathway (section 351 vs section 361 of “Human Cells, Tissues, and Cellular and Tissue-Based Products” [HCT/P] in the Code of Federal Regulation) with the hypothesis that products requiring approval under a stringent regulatory pathway (351 HCT/P) have higher levels of evidence in the literature supporting use and that products with a less stringent regulatory pathway (361 HCT/P) have a higher number of products available for use in the United States.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A search of the PubMed database was performed to identify all peer-reviewed articles pertaining to either allograft or autologous cartilage repair technologies. Predefined inclusion and exclusion criteria were used to find clinical, preclinical, and laboratory studies while excluding duplicates, systematic reviews, and products not available in the United States. Articles were categorized by regulatory pathway (351 and 361 HCT/P), and variables including publication year, type of publication, level of evidence, and number of publications were analyzed.
Results:
After application of predefined criteria, 470 of 1924 articles were included in this study. The 351 HCT/P group was composed entirely of autologous chondrocyte implantation (ACI) technology; 94% of the 361 HCT/P group was composed of osteochondral allografts (OCA). The articles regarding 351 HCT/P were more likely to be clinical in nature than the articles on 361 HCT/P (80% vs 48%, respectively; P = .0001) and entailed significantly more level 1 studies (25 vs 0, respectively; P < .0001). Twice as many articles in the 351 HCT/P group were published in the American Journal of Sports Medicine compared with the 361 HCT/P group (71 vs 38, respectively; P = .18).
Conclusion:
Both ACI and OCA have robust evidence supporting their use, whereas the remaining regulated products have little or no supporting evidence. Technologies regulated by 351 HCT/P were more likely to be level 1 clinical studies and published in the highest impact journal. The 361 HCT/P pathway regulated many more products, with fewer articles supporting their use.
Cartilage restorative technologies fall under US Food and Drug Administration (FDA) approval to ensure their safety. The Code of Federal Regulation is the document that outlines the classification of therapies; specifically, cartilage therapies fall under the section titled “Human Cells, Tissues, and Cellular and Tissue-Based Products” (HCT/P). The HCT/P pathways are regulated through the Center for Biologics Evaluation and Research (CBER). The Public Health Service Act describes 2 pathways for HCT/P products, sections 351 and 361. The 351 HTC/P pathway requires the submission of a Biologics License Application that provides rigorous evidence of preclinical and clinical efficacy and safety. The 361 HCT/P pathway requires donor screening and certain infectious disease testing of the product but does not require the demonstration of safety and/or efficacy for clinical use. Several criteria are used to determine which of the 2 pathways under which a product falls; however, in general, autologous or allograft products that are deemed to be “minimally manipulated” qualify for the 361 HCT/P pathway, and the rest fall under the 351 HCT/P pathway. 1 Commonly used technologies such as microfracture10,13 and osteochondral autograft transfer2,9 fall outside of this domain because they are not regulated products. However, autologous chondrocyte implantation (ACI), 3 osteochondral allografts (OCA),5,8,11,12 and several newer technologies fall under these FDA regulatory pathways.
It is important for surgeons to understand the clinical evidence behind the products they use to treat their patients, as they strive to provide the best evidence-based care. Surgeons may assume that because a product makes it to market, it has undergone stringent testing to prove its safety and efficacy. Knowing how the FDA regulates these products and how that affects the rigor of the premarket scientific investigations of these products is invaluable when evaluating new technologies, particularly as the rate of cartilage restoration procedures continues to increase. 7
The purpose of this study was to investigate the literature supporting clinical evidence for the use of commercially available cartilage repair procedures stratified by FDA regulatory pathway. We hypothesized that products requiring more stringent regulatory pathways (351 HCT/P) would have higher levels of evidence in the literature supporting their use, and products with a less stringent regulatory pathway (361 HCT/P) would have a higher number of products available for use in the United States.
Methods
This bibliometric analysis draws on publicly available data and does not directly involve human participants; therefore, ethical review or oversight was not required.
A broad search of the PubMed database was conducted in compliance with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines to identify and retrieve peer-reviewed research articles regarding potential HCT/P products. Articles were included if they were clinical, preclinical, or laboratory studies of either technology. The queries were completed in May 2018. Inclusion criteria for the literature search strategy were the following terms: “ACI,”“MACI,”“autologous chondrocyte implantation,”“autologous chondrocyte transplantation,”“matrix associated autologous chondrocyte implantation,”“matrix associated autologous chondrocyte transplantation,”“matrix based autologous chondrocyte implantation,”“matrix induced autologous chondrocyte transplantation,”“biocartilage,”“extracellular matrix,”“DeNovo NT,”“particulated juvenile allograft cartilage,”“cartiform,”“viable osteochondral allograft,”“osteochondral allograft,”“prochondrix,”“fresh cryopreserved osteochondral allograft,”“chondrofix,” and “sterile decellularized osteochondral allograft.” Exclusion criteria were as follows: reviews, studies on joints other than the knee (hip, elbow, shoulder, foot, and ankle), and products not commercially available in the United States.
The search yielded 1924 citations (Figure 1). Duplicate citations were removed, and 2 independent reviewers (L.O., S.L.S.) performed a review of the abstracts from all identified articles. Full-text articles were obtained for review if necessary to allow for further assessment of inclusion and exclusion criteria, which resulted in a total of 470 articles for the analysis.
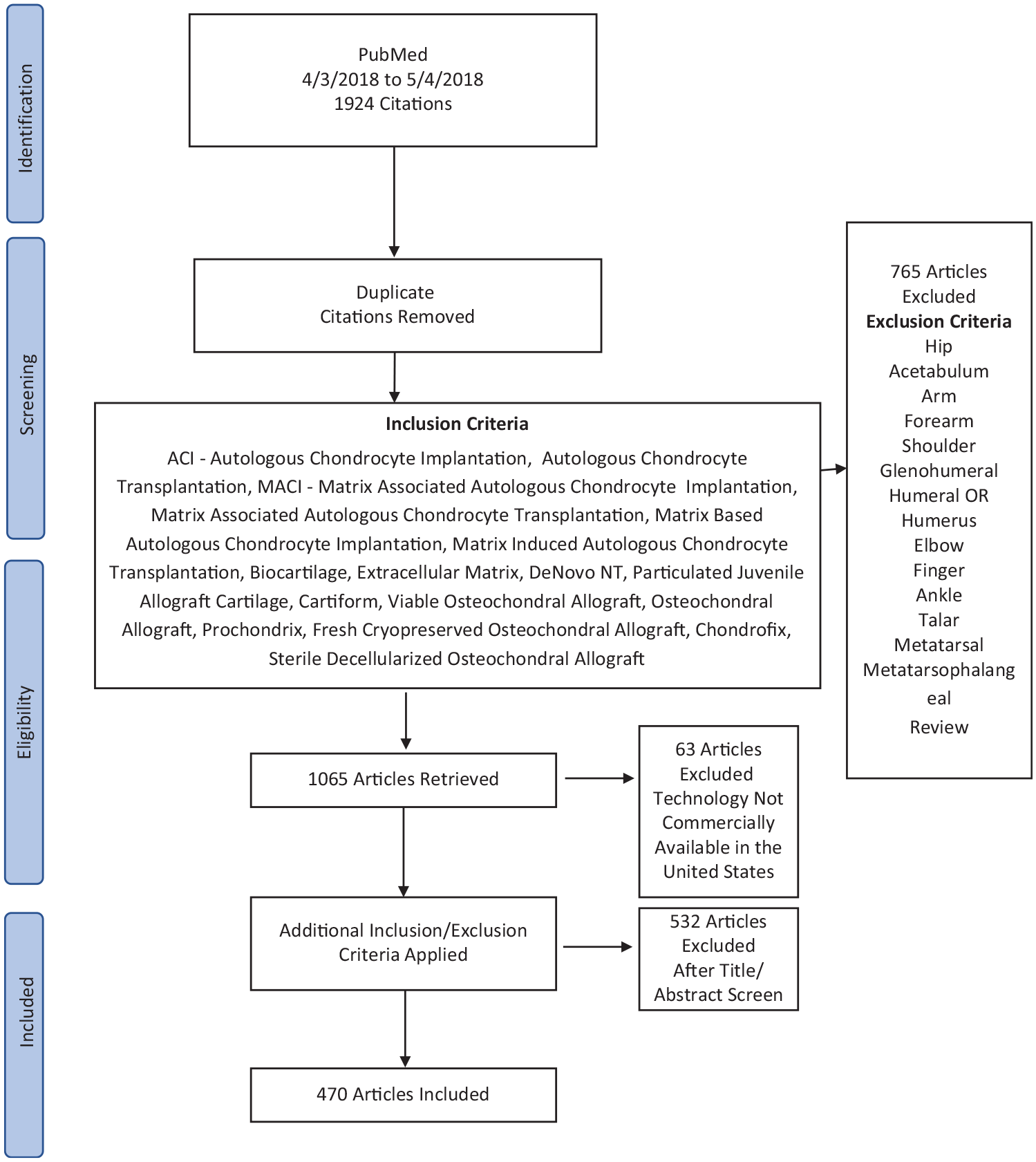
Flow diagram detailing the literature search and selection process.
The articles were independently reviewed and classified by an off-site team and 2 of the authors (L.O., S.L.S.). Studies reported in the literature were categorized according to FDA regulatory pathway (351 HCT/P or 361 HCT/P). FDA approval pathways were obtained from the FDA CBER approval website (https://www.fda.gov/vaccines-blood-biologics/development-approval-process-cber/biological-approvals-year) and individual product websites. Table 1 provides a list of reconstructive and restorative knee cartilage repair products found in the literature that are commercially available in the United States.
Reconstructive and Restorative Knee Cartilage Repair Products Commercially Available in the United States a
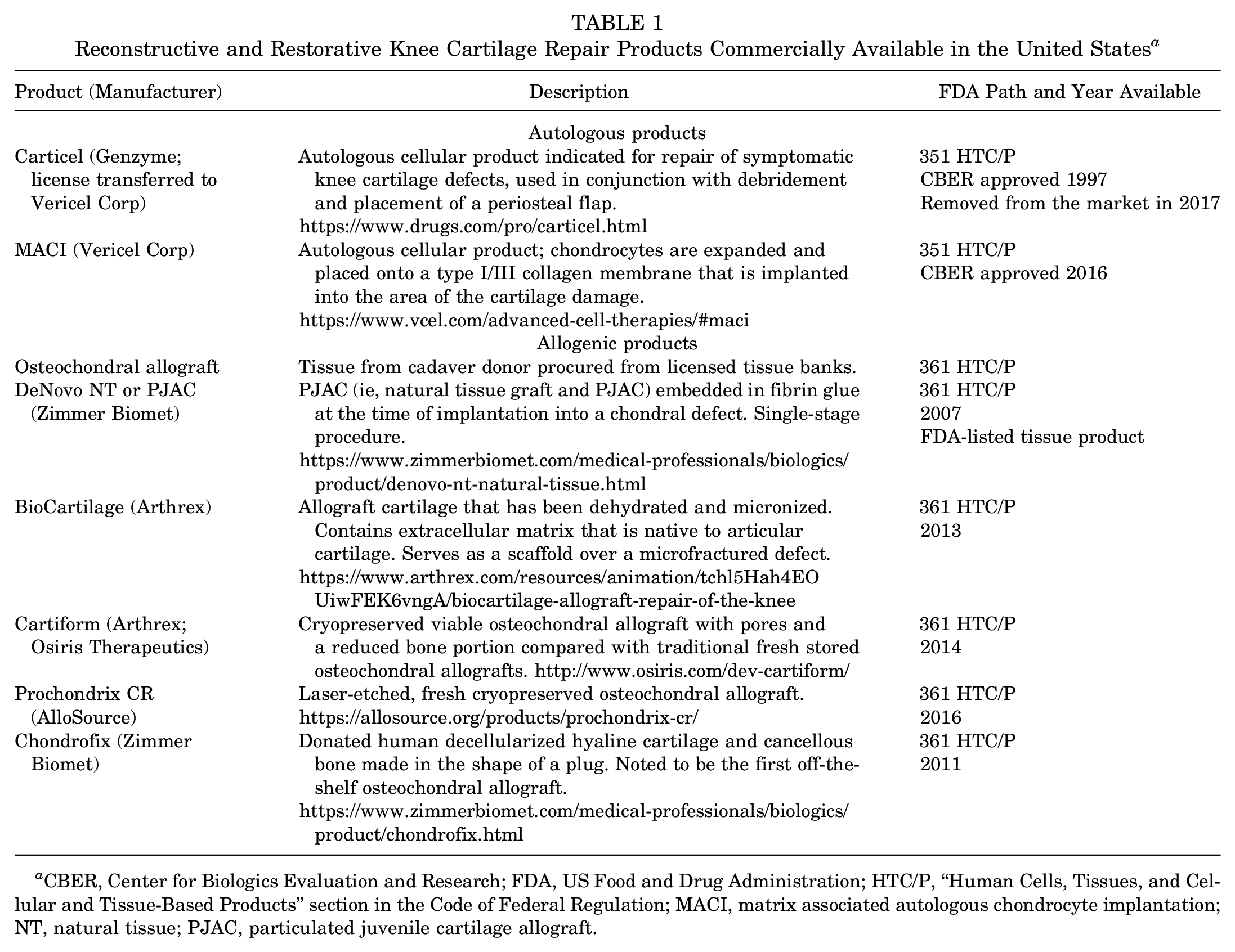
CBER, Center for Biologics Evaluation and Research; FDA, US Food and Drug Administration; HTC/P, “Human Cells, Tissues, and Cellular and Tissue-Based Products” section in the Code of Federal Regulation; MACI, matrix associated autologous chondrocyte implantation; NT, natural tissue; PJAC, particulated juvenile cartilage allograft.
Data collected within the FDA regulatory pathway (361 HCT/P or 351 HCT/P) included publication year, type of publication (clinical, preclinical, and laboratory), level of evidence, and number of publications broken down by the specific technology (matrix associated autologous chondrocyte implantation [MACI], osteochondral allograft, particulated juvenile cartilage allograft [PJAC], etc). Level of evidence (1-5) was determined as reported by the journal for each article. The number of publications per peer-reviewed journal and the weighted impact factor were determined.
Statistical Analysis
Statistical analyses of the data were performed using Microsoft Excel (Microsoft Corporation). Descriptive statistics were based on percentages for categorical variables. A 2-tailed Fisher exact test was used to test article type and level of evidence, with an alpha level of .05. Weighted impact factor was determined by the following formula:

Results
Regulatory Pathway
There were 279 publications in the 351 HCT/P ACI group (59%) and 191 publications in the 361 HCT/P allograft group (41%). Most of the publications in the 361 HCT/P group (94%; 180/191) were specific to osteochondral allografts. The other 5 techniques included in Figure 2 had few supporting publications. All of the publications in the 351 HCT/P group were specific to ACI/MACI, the only autologous products approved through FDA CBER (Figure 2).
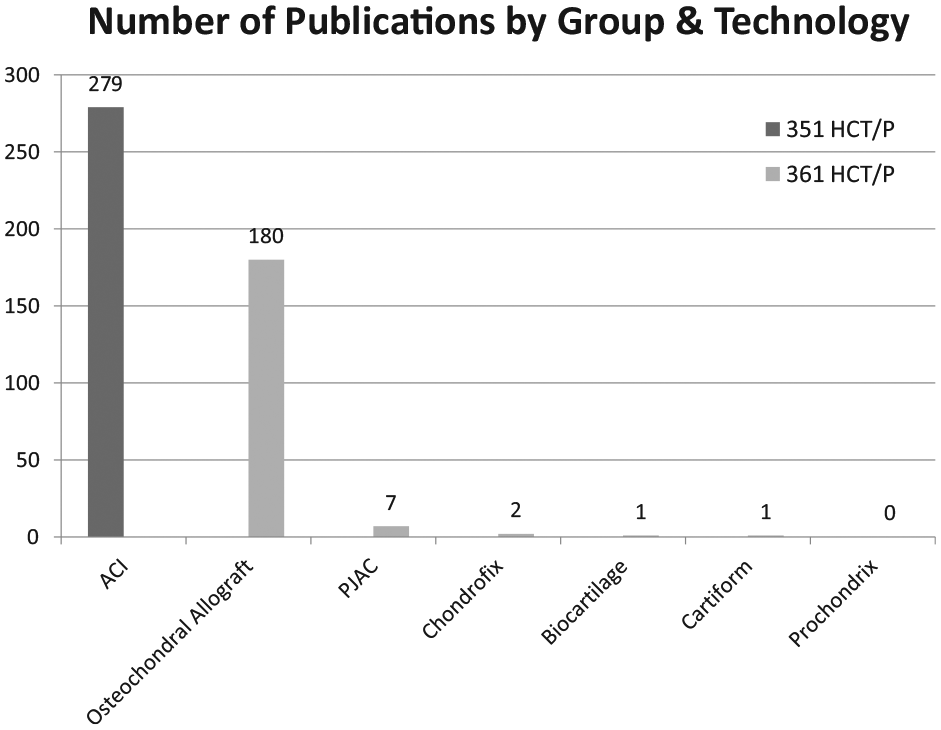
Publications by FDA regulation pathway and technology. ACI, autologous chondrocyte implantation; HTC/P, “Human Cells, Tissues, and Cellular and Tissue-Based Products” section in the Code of Federal Regulation; PJAC, particulated juvenile cartilage allograft.
By article type (clinical, preclinical, or laboratory), the greatest number of articles in either treatment category were clinical (361 HCT/P, 91/191 [48%]; 351 HCT/P, 224/279 [80%]) (Figure 3). Among all publication types, the 351 HCT/P publications were significantly more likely to be categorized as clinical relative to the 361 HCT/P publications (80% vs 48%, respectively; P = .0001).
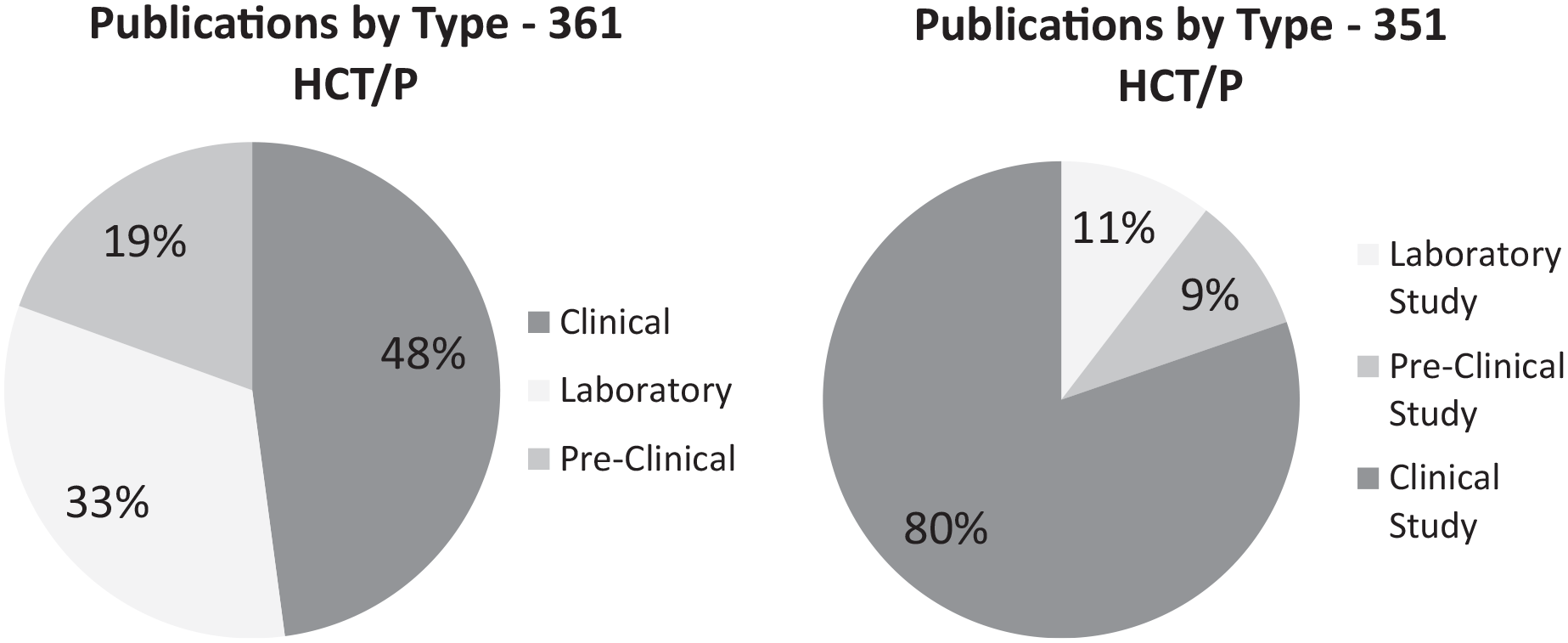
Pie charts showing the breakdown of publication type (laboratory, preclinical, and clinical). HTC/P, “Human Cells, Tissues, and Cellular and Tissue-Based Products” section in the Code of Federal Regulation.
Level of Evidence
Of the clinical articles for each treatment technology, 25 publications regarding 351 HCT/P and 0 publications regarding 361 HCT/P were classified as level 1 evidence. As shown in Table 2, subgroup analysis of clinical publications revealed a significantly greater proportion of level 1 publications describing 351 HCT/P therapies compared with 361 HCT/P therapies (25 vs 0; P = .0003).
Number of Publications by Level of Evidence a
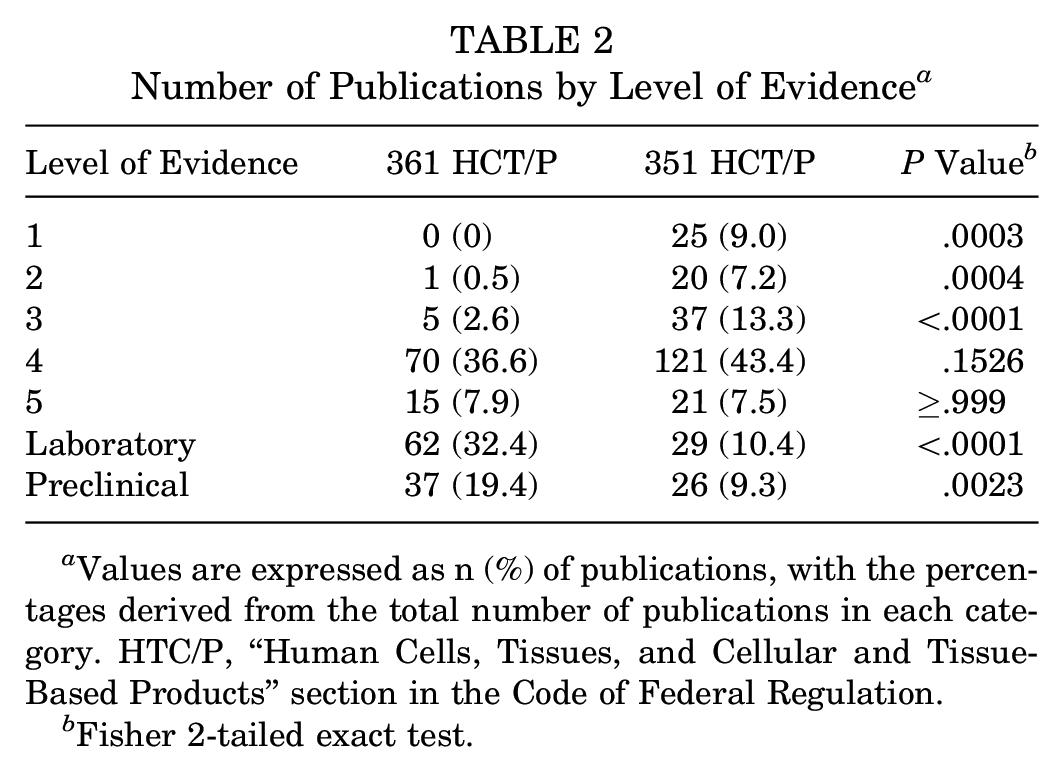
Values are expressed as n (%) of publications, with the percentages derived from the total number of publications in each category. HTC/P, “Human Cells, Tissues, and Cellular and Tissue-Based Products” section in the Code of Federal Regulation.
Fisher 2-tailed exact test.
Publications per Peer-Reviewed Journal and Weighted Impact Factor
The top 10 source journals containing publications for 351 HCT/P or 361 HCT/P technologies, with weighted impact values, are shown in Table 3. 4 The American Journal of Sports Medicine (AJSM) was the most popular journal for both cohorts; however, there were nearly twice as many articles in AJSM describing 351 HCT/P relative to 361 HCT/P technologies (71 vs 38; P = .18) (Figure 4).
Top 10 Journals by Weighted Impact Factor a
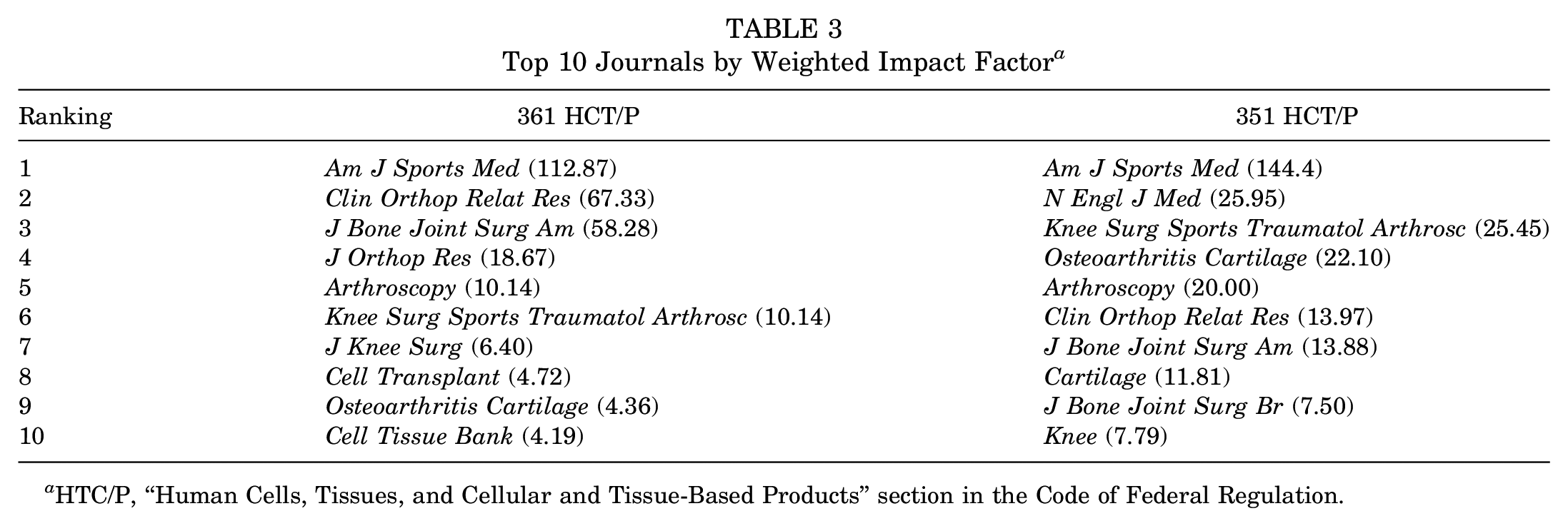
HTC/P, “Human Cells, Tissues, and Cellular and Tissue-Based Products” section in the Code of Federal Regulation.
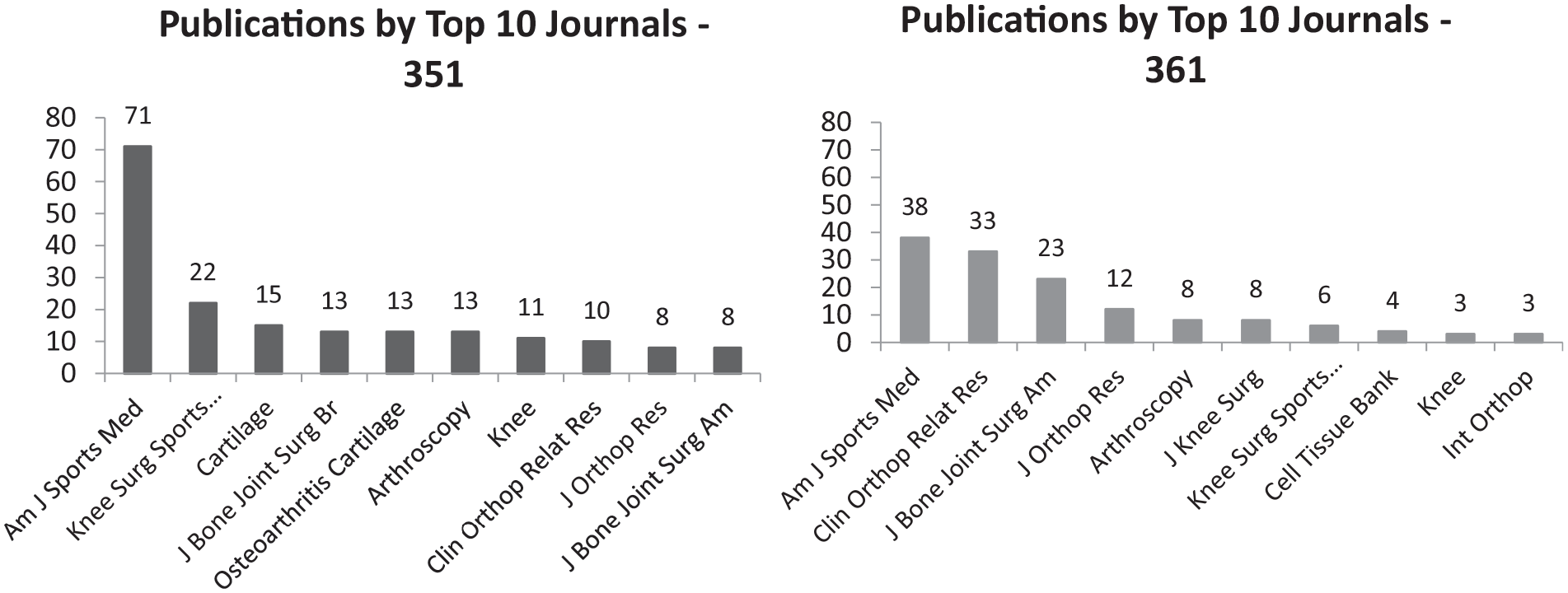
Number of publications in the autologous and allograft groups in high-impact journals.
Number of Publications by Year
The number of publications by year increased fairly steadily beginning in 2005 for both 351 HCT/P and 361 HCT/P technologies. The number of publications was greatest in the allograft group in 2016 with 16 publications and in the ACI group in 2014 with 34 publications (Figure 5).
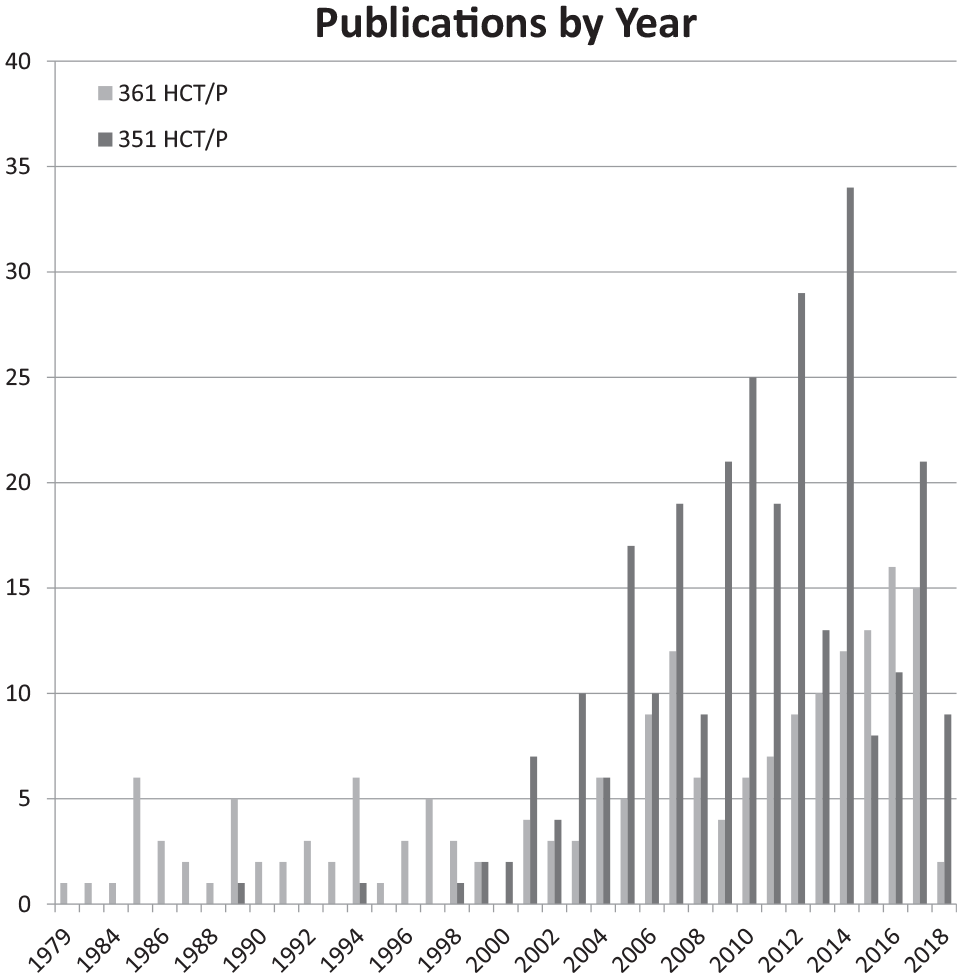
Number of publications per year. For 2018, only articles published before May 9, 2018, were included. HTC/P, “Human Cells, Tissues, and Cellular and Tissue-Based Products” section in the Code of Federal Regulation.
Discussion
To our knowledge, our study is the first to stratify cartilage restoration products by FDA approval pathway. Our most important finding is that ACI and OCA have robust bodies of evidence to support their use, whereas remaining FDA-approved products have little or no evidence. Commercially available products that require more stringent regulatory pathways (351 HCT/P [ACI/MACI]) have higher levels of scientific evidence as measured by the quality of publications (number of level 1 studies) compared with products that require a less stringent regulatory pathway (361 HCT/P). However, OCA was well-studied despite being regulated by the 361 HCT/P pathway, whereas the remainder of the products regulated by this pathway had few, low-quality studies.
ACI (Carticel) and MACI (Vericel) are the only cartilage products to date that have gained approval through the 351 HCT/P pathway; thus, they constitute 100% of articles approved in this regulatory pathway. The 361 HCT/P pathway is more lenient in its regulation, and therefore significantly more products fall under its jurisdiction. Although we found no statistical difference in the number of published manuscripts between the 2 cohorts, the 351 HCT/P products had significantly more level 1 studies compared with the 361 HCT/P group (25 vs 0, respectively; P < .0001). This suggests that the FDA requirements for approval through the 351 HCT/P pathway most likely affect the quality of the studies reported in the literature.
Additionally, both 351 and 361 HCT/P studies were primarily categorized as clinical investigations in their respective categories. However, the 351 HCT/P studies were more likely to be clinical than the 361 HCT/P group. This could be due to the nature of autologous tissue, the difficulty in effectively investigating these modalities in the laboratory, and the lack of appropriate animal models for autologous tissue compared with allograft tissue. In addition, allograft products that are not required to show efficacy in controlled clinical trials may use laboratory and shorter preclinical studies to establish proof of effectiveness and safety, along with smaller clinical case series, given the high cost of clinical trials. Even a small, randomized controlled, phase 3 study can cost $10 million or more and take 2 to 3 years to complete. These limitations have been proposed to be the reasons for a relative plateau in cartilage technologies over the past 10 to 20 years. 6
AJSM was the most popular journal for publication in both 351 and 361 HCT/P groups, but there were twice as many articles for 351 HCT/P technologies than for 361 HCT/P. According to the 2017 Journal Citations Report, AJSM was the highest-rated orthopaedics journal. 2 The higher number of 351 HCT/P product publications is likely a reflection of the higher level of evidence of these articles, which would increase the chances of acceptance in a peer-reviewed journal.
Both the 351 and the 361 HCT/P groups saw a surge in publications around the year 2005. The 351 HCT/P group peaked in 2014, whereas the 361 HCT/P group peaked in 2016. Cartilage restoration surgery has been used for decades but became more widespread during this time period. The recent downtick in publications could be related to the difficulty of performing these studies and the expense associated with them.
ACI/MACI and OCA are regulated by the FDA, as are several newly developed and poorly studied 361 HCT/P regulated technologies (prochondrix, cartiform, chondrofix, PJAC, and biocartilage)14 (Figure 1). Although many of these products have clinical scenarios in which they may be more favorable than the other products, ACI and OCA are the only ones well-supported in the literature. “Off the shelf” cartilage restoration options have increased in popularity due to their availability and ease of use. The purpose of this article is not to dismiss new cartilage technologies but rather serve as a reminder that ACI and OCA have a long-proven track record, whereas the newer 361 HCT/P products need further investigation to best determine their long-term outcomes and the ideal clinical scenarios for their use.
Because the 351 HCT/P pathway requires robust evidence to prove safety and efficacy, our results suggest that more rigorous regulations promote better science to support the products and less rigorous regulations promote increased number of licensed products. However, products on the 361 HCT/P pathway can also report good evidence, as seen with OCA.
As with all systematic reviews, it is possible that relevant articles or patient populations were not identified with our search criteria; however, we followed the PRISMA guidelines to decrease those chances. In addition, the quality of the findings is directly proportional to the quality of the studies. We found that only a small proportion of the studies had a high level of evidence (ie, levels 1 and 2), especially regarding the 361 HCT/P pathway.
Conclusion
ACI/MACI and OCA have a large body of evidence supporting their use, whereas the remainder of FDA-approved products have little evidence. The autologous cellular products regulated via 351 HCT/P had more level 1 studies and greater representation in the highest impact journals than those regulated by 361 HCT/P.
Footnotes
Acknowledgements
The authors acknowledge Andrew Kocher, MPT, CMPT, for assistance with data collection and analysis for this article.
Submitted December 20, 2020; accepted April 9, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.B.H. has received education support from Kairos Surgical, Pinnacle Inc, and Arthrex Inc. W.G. has received consulting fees from Active Implants, Bacterin International, RTI, Stryker, and Vericel. J.F. has received consulting fees from Aastrom Bioscience Inc, Aesculap/B.Braun, Arthrex Inc, Cartiheal, Ceterix Orthopaedics Inc, Collagen Matrix, Cook Biotech Inc, DePuy Synthes, Exactech Inc, ISTO Technologies Inc, Medshape Inc, Moximed Inc, Organogenesis Inc, Osiris Therapeutics Inc, Regentis, RTI Surgical Inc, Samumed Inc, Vericel, Zimmer Biomet Inc, and ZKR Orthopaedics Inc; research support from Active Implants, Arthrex Inc, Episurf, Fidia Pharma, JRF Ortho, Moximed Inc, Novartis, Organogenesis Inc, Samumed Inc, Vericel, and Zimmer Biomet Inc; and IP royalties from Arthrex Inc, Biopoly LLC, DePuy Synthes, and Organogenesis Inc; he holds stock or stock options in MedShape Inc and Ortho Regenerative Tech Inc. S.L.S. has received consulting fees from Arthrex, Bioventus, ConMed, Joint Restoration Foundation, Smith & Nephew, Vericel, Zimmer Biomet, and Olympus; speaking fees from Flexion Therapeutics; and royalties from ConMed; holds board membership with Epic Bio, Joint Restoration Foundation, and Vericel; has stock/stock options with Epic Bio and Vivorte; and has performed product evaluation for ConMed and Olympus. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.