
Abstract
Background:
Tendinopathy is a pervasive clinical problem that afflicts both athletes and the general public. Although the inflammatory changes in tendinopathy are well characterized, how the therapeutic effects of platelet-rich plasma (PRP) on tendinopathy are being modulated by the inflammatory environment is not well defined.
Purpose/Hypothesis:
In this study, we aimed to compare the therapeutic effects of PRP alone versus a combination of PRP with a primary glucocorticoid (GC) injection at the early stage of tendinopathy. We hypothesized that PRP treatment could promote better tendon regeneration through the suppression of inflammation with GC.
Study Design:
Controlled laboratory study.
Methods:
The gene expression profile of tendon stem/progenitor cells (TSPCs) cultured with PRP was analyzed with RNA sequencing. To evaluate the cell viability, senescence, and apoptosis of TSPCs under different conditions, TSPCs were treated with 0.1 mg/mL triamcinolone acetonide (TA) and/or 10% PRP in an IL1B–induced inflammatory environment. To further verify the effects of the sequential therapy of GCs and PRP, an early tendinopathy animal model was established through a local injection of collagenase in the rabbit Achilles tendon. The tendinopathy model was then treated with isopycnic normal saline (NS group), TA (TA group), PRP (PRP group), or TA and PRP successively (TA+PRP group). At 8 weeks after treatment, the tendons were assessed with magnetic resonance imaging (MRI), histological examination, transmission electron microscopy (TEM), and mechanical testing.
Results:
Gene Ontology enrichment analysis indicated that PRP treatment of TPSCs induced an inflammatory response, regulated cell migration, and remodeled the extracellular matrix. Compared with the sole use of PRP, successive treatment with TA followed by PRP yielded similar results in cell viability and senescence but less cell apoptosis in vitro. In vivo experiments demonstrated that the TA+PRP group achieved significantly better tendon regeneration, as confirmed by MRI, histological examination, TEM, and mechanical testing.
Conclusion:
This study showed that the primary use of GCs did not exert any obvious deleterious side effects on the treated tendon but instead enhanced the regenerative effects of PRP in early inflammatory tendinopathy.
Clinical Relevance:
The sequential therapy of GCs followed by PRP provides a promising treatment strategy for tendinopathy in clinical practice. PRP combined with the primary use of GCs appears to promote tendon regeneration in early inflammatory tendinopathy.
Tendinopathy is used to describe all forms of chronic tendon abnormalities, characterized by pain, decline in biomechanical function, and reduced exercise tolerance. 42 A tendon disorder is a pervasive and intractable clinical problem in musculoskeletal and sports-related medicine, afflicting both athletes and the general public. The American Academy of Orthopaedic Surgeons reported that approximately 2 million people underwent the clinical treatment of rotator cuff tendon injuries in 2008. 44 Based on the recent medical literature, this number has been increasing substantially in recent decades 29 and accounted for up to 30% to 50% of general practice musculoskeletal clinical cases. 42 According to previous reports, this constitutes an enormous cost in health care expenditure and lost productivity from illnesses annually in the United States.42,44 The Achilles, patellar, and supraspinatus tendons are particularly vulnerable to injuries among various tendon tissues, with a poor prognosis and currently without any ideal treatment regimen. 48 The mainstream clinical management of tendinopathy is based on nonoperative treatment modalities including cryotherapy, rest, immobilization, pharmaceutical formulations such as nonsteroidal anti-inflammatory drugs, and peritendinous injections. 3 Traditional nonoperative treatment methods of tendinopathy have focused mainly on relieving pain, which is the main complaint from most patients with symptomatic tendinopathy. With this treatment, the progression of this disease is mitigated, and 24% to 45.5% of patients ultimately require a surgical intervention.40,51 The poor regenerative capacity of the tendon and unclear mechanisms of this disease prevent the successful treatment of tendinopathy.
The pathological process of tendon disorders is currently controversial. The theory of degeneration became the mainstream concept of tendinopathy at the beginning of the 21st century. 49 Platelet-rich plasma (PRP) is an autologous blood product and consists of a minimum platelet concentration of more than 1 × 106/µL or an approximately 5-fold increase in platelets from baseline. 19 PRP contains abundant growth factors and cytokines, including platelet-derived growth factor, transforming growth factor–β (TGF-β), and insulin-like growth factor. 42 It has recently shown much promise in clinical applications of tendon repair and regeneration.21,31,61,63 The mechanism of PRP treatment has not been elucidated. It is now believed that PRP may regulate collagen turnover and activate tendon stem/progenitor cells (TSPCs) in tendinous tissue.1,5 However, the clinical efficacy of PRP treatment has not always been satisfactory, and some clinical research and meta-analyses have shown that, in some instances, PRP treatment may not improve the prognosis of tendon disorders.7,20,52 The presence of inflammation in certain types of tendinopathy may interfere with the therapeutic effects of PRP. 49 With the advancement of modern molecular techniques, key inflammatory interactions with both inflammatory cells and mediators can be observed during the earlier (acute and subacute) stages of tendinopathy because of repetitive tendon microtrauma.41,42,49 It has been demonstrated before that tissue more often heals by fibrovascular “scarring” instead of regeneration with inflammatory cell infiltration.25,58 Blocking of excessive inflammatory responses allows the activation of “innate” healing mechanisms and the regeneration of a more normal insertion site rather than reactive scar formation. 25 The different preparation methods of PRP have a different effect on tissue healing. Leukocyte-poor PRP was previously reported to cause a less acute inflammatory response than leukocyte-rich PRP after an injection in tendons 18 because leukocytes released inflammatory cytokines and metalloproteinases (MMPs) that could exacerbate the early inflammatory response to tissue injuries.
A local glucocorticoid (GC) injection is considered to be one of the most commonly performed clinical treatment options to relieve pain and/or inflammation in various types of musculoskeletal disorders, including tendinopathy. 23 Within the primary care setting of the United Kingdom alone, more than 500,000 intra-articular GC injections are performed per year for a wide variety of musculoskeletal disorders. 14 Also, for tendinopathy, GC injections are frequently applied in close proximity to tendons, with common examples including the rotator cuff, the flexor and extensor tendon origins around the elbow, the gluteus medius tendons, the Achilles and patellar tendons, the flexor tendons in the hand (ie, trigger finger), and the extensor tendons around the wrist (ie, de Quervain tenosynovitis).1,15 However, the clinical efficacy of GC injections is still ambiguous and controversial according to previous studies.10,11,24,53 Although some short-term benefits including pain reduction and functional improvements are observed after a GC injection, the long-term effects in tendon disorders are unsatisfactory. 11
In this study, we propose the hypothesis that both inflammation and degenerative changes play key roles in the pathogenesis progression of tendinopathy. Anti-inflammatory treatment methods such as GC injections alone are not enough to promote the regeneration of tendons but might provide a more conducive environment for PRP to exert its beneficial therapeutic effects. The combination of primary anti-inflammatory treatment and regenerative therapy may bring new hope for the management of tendinopathy. In this study, we aimed to compare the therapeutic effects of PRP on tendinopathy with or without primary GC treatment at early stages. For this purpose, we chose to use an intratendinous injection of collagenase to mimic early-stage tendinopathy. This tendinopathy model has been widely used to produce tendon lesions with the advantages of a small cost and consistent tendon damage. 39 We hypothesized that PRP would counteract the side effects of the GC and that the combination treatment may better promote tendon regeneration via suppression of the inflammatory environment. RNA sequencing (RNA-seq) data of TSPCs treated with PRP or not were used to show the effect of PRP on TSPCs. The purpose of the in vitro experiments was to evaluate the feasibility of “sequential therapy” by the results of cell viability, senescence, and apoptosis. Also, we compared the effects of different treatment options in a rabbit Achilles tendinopathy model.
Methods
PRP Preparation
On the basis of our previous study, 61 we chose leukocyte-poor PRP instead of leukocyte-rich PRP to avoid extra-inflammatory reactions caused by leukocytes. PRP was prepared by using density gradient centrifugation from rabbits as described previously. 61 Briefly, 5.4 mL of whole blood collected from the rabbit ear arteries with indwelling needles was mixed with 0.6 mL of acid-citrate-dextrose anticoagulant to prevent blood coagulation. Then, 1 mL of the mixed blood was used to perform blood tests, and the remaining volume was used for the PRP preparation. Whole blood was first centrifuged at a low speed of 200g for 10 minutes to sediment red blood cells, and the supernatant was collected and subjected to a second centrifugation at 180g for 10 minutes to discard the residual red blood cells and white blood cells. The supernatant was then subjected to a third centrifugation at 600g for 8 minutes. The sediments were resuspended with 0.3 mL of the supernatant to obtain PRP. Finally, 0.1 mL of PRP was used for routine blood analysis on an automatic hematology analyzer system (ADUIA2120; Siemens) to compare with whole blood. The remaining 0.2 mL was used for experiments. For in vitro experiments, PRP was further activated with 22 μM CaCl2, and the supernatant was collected after high-speed centrifugation of 2000g at 4°C for 10 minutes before use.
Isolation and Culture of TSPCs
We isolated and cultured TSPCs from the rabbit Achilles tendon using our previously reported protocols. 55 Rabbits were sacrificed, and tendon tissues were harvested and then chopped into 1- to 2-mm3 pieces in aseptic conditions. After digestion with collagenase type I (Thermo Fisher Scientific), the primary cells were resuspended and cultured in Dulbecco’s modified Eagle’s medium (low glucose; Thermo Fisher Scientific) containing 10% (vol/vol) fetal bovine serum (Thermo Fisher Scientific) and 1% (vol/vol) penicillin-streptomycin (Thermo Fisher Scientific). Bona fide TSPCs were acquired by selecting formative colonies that had a diameter larger than 2 mm when plated at a density of 2 cells/cm2. Multiclonal TSPCs between passages 4 and 6 were used in our experiments.
RNA-seq Experiments and Data Analysis
We assigned the TSPCs into 2 experimental groups: TSPCs cultured in medium with or without 10% (vol/vol) PRP. After the isolation of total RNA by TRIzol Reagent (Thermo Fisher Scientific), mRNA was purified by magnetic beads, digested into short fragments, and then reverse-transcribed into double-stranded cDNA. A sequencing library was constructed with the TruSeq RNA Sample Prep Kit (Illumina) and sequenced on a HiSeq platform (Illumina). The RNA-seq readings were aligned to the reference genome Oryctolagus_cuniculus.OryCun2.0.98 using STAR 16 (2.7.2a), and per gene counts were calculated using featureCounts 36 (v1.6.5) in the SourceForge Subread package. The R statistical programming language was used for all further statistical analyses of sequencing data. Differentially expressed genes (DEGs) were determined using DESeq2. 38 Gene Ontology (GO) and Kyoto Encyclopedia of Genes and Genomes (KEGG) analyses were performed using clusterProfiler. 62 The RNA-seq data are available through GEO accession number GSE159292.
Treatment of TSPCs and Evaluation of Cell Viability, Senescence, and Apoptosis
As shown in the in vitro experimental flow chart (see Appendix Figure A1, available in the online version of this article), the TSPCs were divided into 5 groups: normal (NOR) control group, normal saline (NS) treatment group, triamcinolone acetonide (TA) treatment group, PRP treatment group, and TA+PRP treatment group (Appendix Figure A1). In the TA+PRP group, cells were first allowed to attach to a culture plate for 24 hours without any treatment. Then, cells were successively treated with 1 ng/mL IL1B (recombinant human IL1B, 200-01B; PeproTech) for 24 hours, 0.1 mg/mL TA for 3 hours, and PRP (10% vol/vol) for 3 days. In the other treatment groups, the equivalent volume of NS was used to replace TA or PRP in the corresponding protocols. Nontreated cells were used as the control. Cell viability, senescence, and apoptosis were determined with the Cell Counting Kit-8 (Dojindo), Senescence β-Galactosidase Staining Kit (Beyotime Biotechnology), and Annexin V-FITC Apoptosis Detection Kit (Jiangsu KeyGen Biotech), respectively, according to the manufacturers’ protocols. Detailed procedures are described in Appendix Figure A1.
Animal Model
As described previously, 61 we used 33 New Zealand White rabbits with a body weight ranging from 2.0 to 2.5 kg to create the Achilles tendinopathy model in this study, with the approval of the Animal Ethical and Welfare Committee of Zhejiang Chinese Medical University (201903-0101). A total of 7 rabbits were included as the normal control.
Briefly, under general anesthesia using pentobarbital sodium, a 29-gauge needle was inserted into the Achilles tendon through the skin at 5 mm above the calcaneus and pushed forward along the axis of the tendon for approximately 10 mm. Subsequently, an intratendinous injection of collagenase type I (300 UI/rabbit, 260 U/mg; Worthington Biochemical) was carried out with gradual withdrawal of the needle. Then, 28 rabbits (56 Achilles tendon samples) were assigned to the 4 treatment groups (NS, TA, PRP, TA+PRP) of the in vitro experiments. At 1 week after collagenase induction, 10 rabbits were allocated to the NS and PRP groups for a peritendinous injection of 200 μL NS, while another 10 rabbits were allocated to the TA and TA+PRP groups for an injection of 200 μL/2 mg TA. The dosage consideration of TA was based on previous studies and recommended dose in human patients in clinical practice for both effectiveness and safety. At 2 and 3 weeks after collagenase induction, rabbits in the NS and TA groups received a peritendinous injection of 200 μL NS, while those in the PRP and TA+PRP groups received an injection of 200 μL PRP. At 8 weeks after collagenase induction, the Achilles tendons of the animals were scanned with magnetic resonance imaging (MRI) to assess their healing status. Upon animal death with excess pentobarbital sodium, the tendon samples were subjected to a histological assessment, immunohistochemical and specific staining, transmission electron microscopy (TEM), and biomechanical testing.
MRI Assessment
MRI was able to display the scope and extent of the injured areas. Before euthanasia, the treated tendons were scanned on a 3-T scanner (Siemens) after anesthesia with preset parameters (echo time, 90 milliseconds; repetition time, 4050 milliseconds). 22 A voxel size of 0.2 × 0.2 × 1.5 mm plus a 0.3-mm slice gap (matrix = 256 × 256) were used to prevent partial volume effects. The imaging sequence included T2-weighted proton density sagittal and coronal images, which were used for subsequent image processing. Then, the anterior-posterior tendon thickness, mean signal intensity, and lesion percentage of the tendon with a high T2 signal intensity (>150 in our study) were measured on the sagittal image of the tendon, 10 mm above the calcaneal attachment site, in triplicate.
Morphological and Histological Evaluation
Upon animal death via the administration of excess pentobarbital sodium, the Achilles tendon was exposed and photographed to obtain a gross morphological image. Then, 5 tendon samples in each group were harvested for a histological examination after fixation, dehydration, and embedment within paraffin blocks as described previously. 56 Histological sections stained by hematoxylin and eosin and Masson trichrome were obtained to observe cell morphological changes and collagen deposition. Overall, 3 sections randomly selected from each sample were single-blindly evaluated by 2 experienced observers independently, and the average scores among groups were compared. Histological scores of tendon samples were evaluated according to a modification of the Movin grading system 8 (Appendix Table 1). A 0-to-3 scale was used to quantify each of the 6 parameters in the scoring system, with 0 being normal and 3 being maximally abnormal. Sections stained with sirius red were observed on polarized light microscopy to further evaluate the alignment and maturation of collagen fibrils. Type I collagen (Col 1) and type III collagen (Col 3) could be distinguished by different birefringence, as Col 1 appeared either red or yellow, and Col 3 appeared green.
Immunohistochemistry and Special Staining
Paraffin sections (4 um) of samples (n = 3) were utilized for immunohistochemistry and special staining. Mouse monoclonal antibody against Col 1 and CD68 (1:200 dilution; Abcam) as well as mouse monoclonal antibody against Col 3 (1:200 dilution; Santa Cruz Biotechnology) were applied to visualize the expression levels of Col 1, CD68, and Col 3 in the repaired tendon according to the treatment group. The primary antibody in negative reagent controls of immunohistochemical assay was replaced by phosphate-buffered saline (PBS) to eliminate false-positive findings. The level of apoptosis in the different groups was determined by the In Situ Cell Death Detection Kit (Roche). Mast cells were detected using toluidine blue staining (Solarbio).
Analysis of Microscopic Structure by TEM
Tissue samples (n = 3) were prepared using standard procedures for TEM as described previously. 61 At least 1500 collagen fibrils were measured to accurately represent the diameter distribution. We sampled the same viewing area (at least 1500 collagen fibrils) in each group to measure the average value and distribution of collagen fibril diameters. The fibril diameter was calculated as the largest diameter from the longest axis of each fibril.
Mechanical Testing
Specimens (n = 8) for biomechanical testing were frozen in PBS at −80°C immediately after harvesting while avoiding repeated freeze-thaw cycles. The tendon samples were thawed at 37°C in PBS just before biomechanical testing. The tendon was fixed in a material testing system (5944; Instron). A small (5 N) preload was applied 5 times to remove specimen laxity. We then increased the axial tensile load continuously at a speed of 10 mm/min during the test until the tendon broke. The real-time load (N) and deformation (mm) were recorded to measure mechanical properties. The failure load (N) was the maximum load during the test process. Failure stress (MPa) was the failure load per unit area. Stiffness (N/mm) was calculated by dividing the deformation at the time of the maximum load by failure stress. The Young modulus (MPa) was calculated from the slope of the linear part of the stress-strain curve.
Statistical Analysis
In our experiments, SPSS software (version 22.0; IBM) and R software (version 3.6.1) were utilized for all quantitative data analyses. A P value <.05 was set as the threshold of statistical significance. All the data from cell assays, MRI, histological examination, TEM, and biomechanical testing were expressed as mean ± SD. The statistical significance of differences was determined using 1-way analysis of variance with post hoc analysis of the Tukey multiple comparison test. The R package “ggplot2” 59 was used for plotting statistical graphs.
Results
PRP Analysis
The quality of prepared leukocyte-poor PRP was controlled by analyzing the concentrations of platelets, leukocytes, and erythrocytes (Appendix Figure A2). Compared with the whole blood samples, our PRP showed an approximate 6.6-fold higher concentration of platelets. On the other hand, the concentrations of leukocytes and erythrocytes were less than 0.1 × 103/μL in our PRP. These results thus confirmed the reliability of our preparation method for leukocyte-poor PRP.
RNA-seq Analysis of TSPCs Cultured in Medium With or Without 10% PRP
The effects of PRP treatment on global gene expression profiles in TSPCs were analyzed with RNA-seq. The whole transcriptome RNA-seq data of TSPCs cultured with or without PRP were normalized, and DEGs were identified using DESeq2. 38 In total, we identified 701 DEGs including 409 downregulated genes and 292 upregulated genes (with a >1.5 log2 fold change and false discovery rate <0.05). TSPCs from the PRP-treated group displayed a broad range of changes in gene expression compared with the control nontreated TSPCs (Figure 1A). A detailed view of some specific DEGs associated with inflammation and tendon biology is presented in a heatmap (Figure 1B). Genes related to tissue remodeling such as CHI3L1, MMP1, and MMP12 were observed to be upregulated in the PRP group. Additionally, antiapoptotic genes such as TNFRSF1B and HMOX1 were also found to be upregulated in the PRP group. Moreover, proinflammatory cytokines such as S100A12 and the interleukin family members IL1A, IL1B, and IL7 made up the majority of all these upregulated genes in TSPCs treated with PRP.
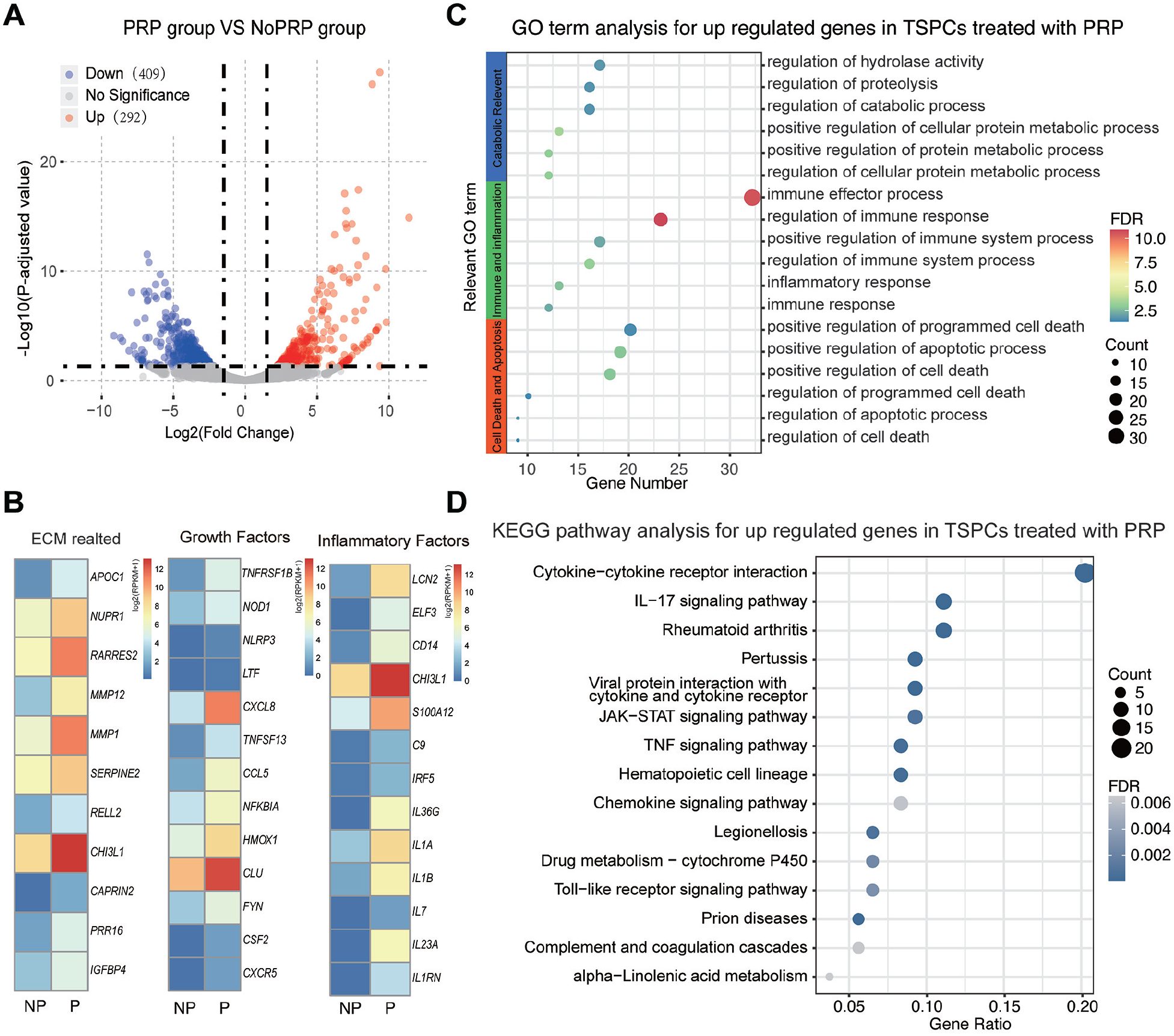
RNA sequencing analysis of tendon stem/progenitor cells (TSPCs) cultured in medium with and without 10% (vol/vol) leukocyte-poor platelet-rich plasma (PRP). (A) A volcano plot showing the upregulated and downregulated differentially expressed genes (DEGs). Log2 fold change >1.5 (adjusted P < .05). (B) A heatmap showing a detailed view of some specific DEGs associated with inflammation and tendon biology. (C) Some relevant representative Gene Ontology (GO) terms of significantly upregulated genes in PRP-treated TSPCs. (D) The top Kyoto Encyclopedia of Genes and Genomes (KEGG) pathways of significantly upregulated genes in the PRP-treated group. ECM, extracellular matrix; P, PRP group; NP, No PRP group.
We then performed GO enrichment analysis for DEGs. Significantly upregulated genes in PRP-treated TSPCs were characterized by GO analysis, and the relevant representative GO terms were selected and reassigned to 3 groups: cell death and apoptosis group, immune and inflammation group, and catabolic group (Figure 1C). The immune and inflammatory GO terms showed the influence of increased inflammation on the regenerative effects of PRP. These changes also shared a certain degree of similarity with previous microarray comparisons of gene expression in PRP-treated and nontreated tendon fibroblasts. 27 KEGG pathway analysis of the upregulated genes in the PRP-treated group is shown in Figure 1D. The “cytokine–cytokine receptor interaction” KEGG pathway was induced the most, which is different from the previous microarray data that only identified the tumor necrosis factor–alpha (TNF-α) and NF-κB pathways. 27 Additionally, more chemotactic and proinflammatory KEGG pathways such as the IL17 signaling pathway were found in our study than the previous microarray data.
Evaluation of Cell Viability, Senescence, and Apoptosis Within In Vitro Experiments
The PRP and TA+PRP groups displayed better stem cell–like characteristics such as the elongated spindle-shaped morphology of TSPCs (Figure 2A) than the other groups. The proliferation rates of TSPCs in the NOR, NS, TA, PRP, and TA+PRP groups were determined using the Cell Counting Kit-8 to confirm these observations (Figure 2D). The NS group showed that the inflammatory microenvironment exerted a negative effect on cell proliferation on both days 5 and 8 compared with the NOR group. The TA group showed not better but instead a little lower cell viability on both days 5 and 8 compared with the NS group. On day 8, the PRP and TA+PRP groups displayed significantly higher cell activity than the other groups. Although the TA+PRP group displayed higher cell activity than the PRP group, this was not statistically significant. According to the results of β-galactosidase staining (Figure 2B and 2E), more senescent cells were observed in the NS group versus the NOR group. The PRP and TA+PRP groups had significantly fewer senescent cells than the NS group and achieved an even better result than normal TSPCs. TA+PRP treatment resulted in the least senescent cells. With regard to cell apoptosis (Figure 2C and 2F), treatment with IL1B significantly increased cell apoptosis, which is consistent with previous observations. 32 Treatment with PRP or TA+PRP both significantly reduced cell apoptosis, while TA-only treatment did not work.
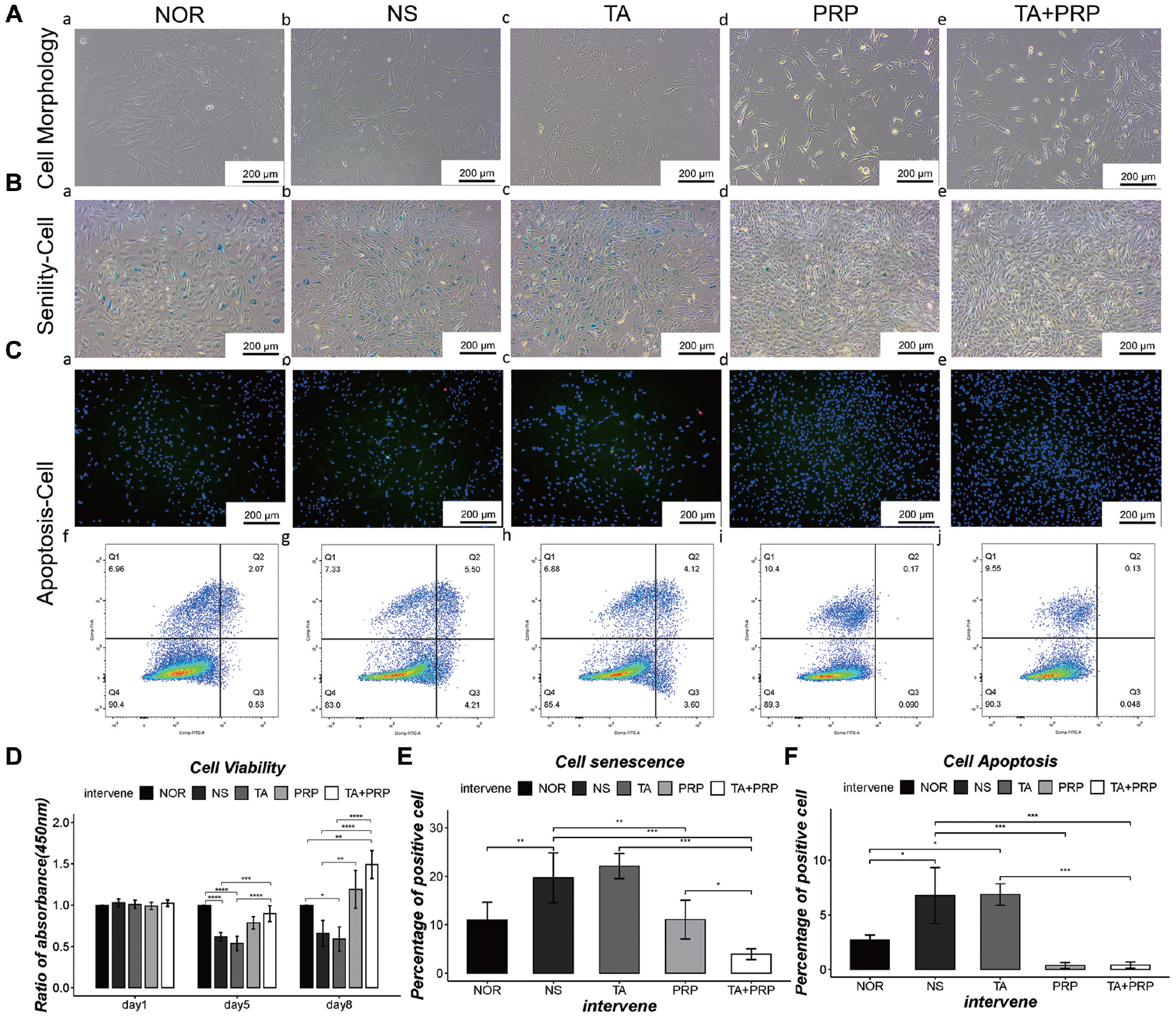
The evaluation of cell viability, senescence, and apoptosis of tendon stem/progenitor cells (TSPCs) in vitro. (A) Cell morphology of TSPCs in each group on day 5. (B) β-galactosidase staining assessed the senescence of TSPCs in each group. (C). The apoptosis state of TSPCs in each group was verified by (a-e) annexin V–FITC/propidium iodide fluorescence microscopy and (f-j) flow cytometry. Blue: DAPI; green: annexin V–FITC; red: propidium iodide. (D-F) Statistical data of cell viability (using the Cell Counting Kit-8), senescence, and apoptosis. (A-C) Scale bar: 200 μm. Data are presented as the mean ± SD. *P < .05. NOR, normal control; NS, normal saline; PRP, platelet-rich plasma; TA, triamcinolone acetonide.
Macroscopy and MRI Observations
After verifying the tendinopathy model in this study (Appendix Figure A3), the Achilles tendons in all treatment groups were harvested at 8 weeks after the collagenase injection. The overall morphology of the treated tendon of the TA+PRP group appeared shiny white, with less swelling and a smoother surface compared with the PRP group (Figure 3B). MRI was the most common way to assess a tendon injury in clinical practice, and the high T2 signal indicated the existence of a tissue injury. 22 According to MRI, the anterior-posterior tendon thickness (Figure 3D) also proved that TA but not PRP affected reduced swelling in tendinopathy. On the other hand, the T2 signal in the TA group was still high, and this indicated that TA-only treatment was not enough to promote tendon regeneration. Compared with the NS, TA, and PRP groups, a less abnormal T2 signal area and intensity (Figure 3E and 3F) in the TA+PRP group were observed, suggesting less edema and more ordered collagen fibers at the lesion site. Although PRP also showed a positive result in reducing the T2 signal, TA+PRP treatment appeared to be more effective.
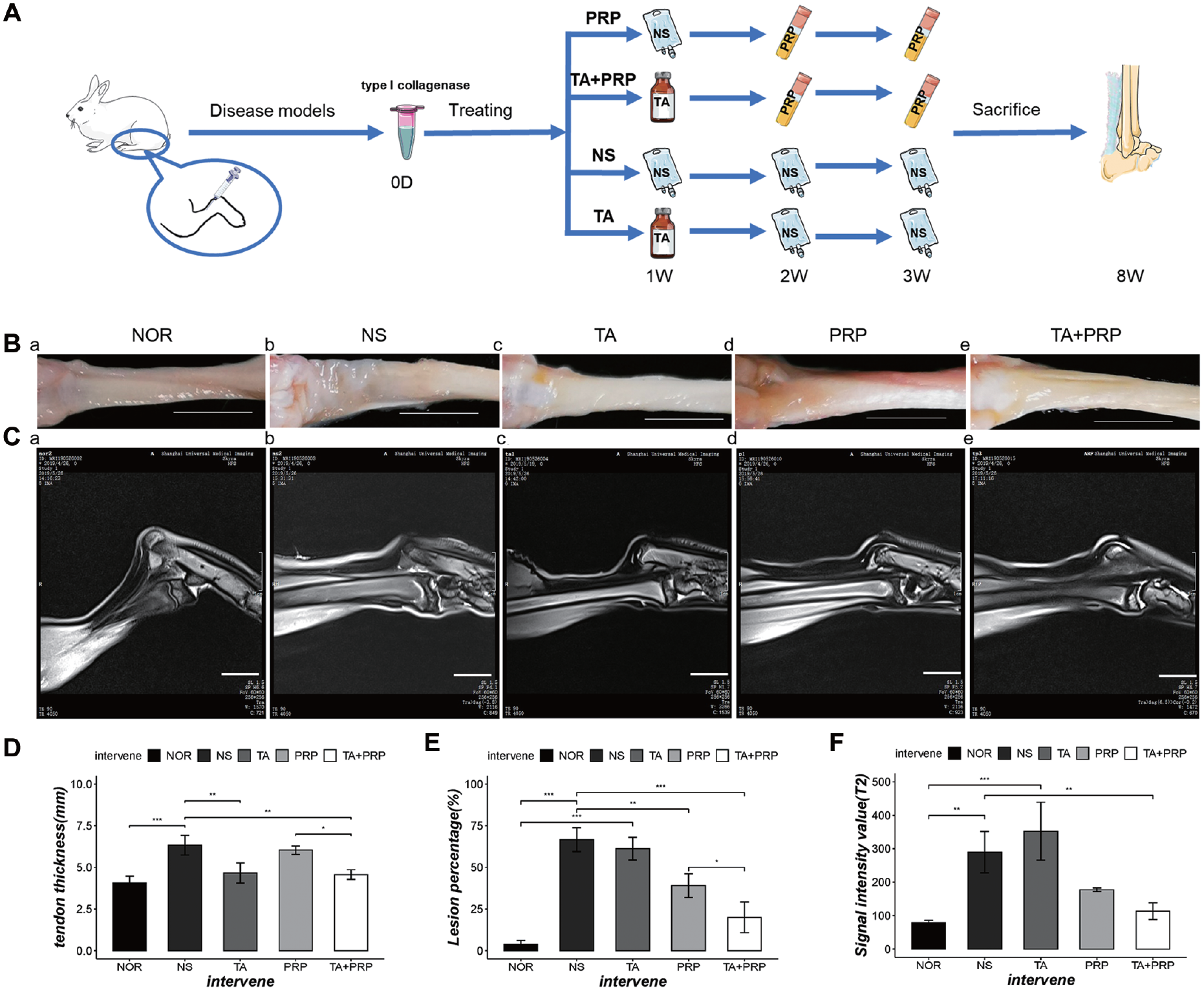
Macroscopy and magnetic resonance imaging (MRI) of T2-weighted images at 8 weeks after the tendinopathy model was induced by collagenase. (A) A schematic representation of treatment groups of the in vivo experiments. (B) A gross view of tendons in the normal control (NOR) and treatment groups. (C) Sagittal MRI of the Achilles tendon in the NOR and treatment groups. (D-F) Statistical data of (D) tendon thickness, (E) percentage of the lesion area, and (F) average T2 signal intensity values of the lesion areas. (B, C) Scale bar: 10 mm. Data are presented as the mean ± SD. *P < .05. NS, normal saline; PRP, platelet-rich plasma; TA, triamcinolone acetonide.
Evaluation of Tendon Regeneration by Histological Examination
From histological staining, the tendon samples in the NS group showed an increase in cellularity, vascularity, matrix disturbance with extracellular matrix degradation, rounding of cell nuclei, and acquisition of adipose tissue. We observed better tendon morphology in the TA+PRP group with a well-organized regenerated tendon tissue structure (Figure 4A and 4B). Only sparse collagen fibers were detected in the NS and TA groups, with the TA group displaying less blood vessel and cell density than the NS group (Figure 4A [b and c] and 4B [b and c]). For the PRP group, more vascular infiltration, a higher cell density, and more small disordered collagen fibers were observed compared with the TA+PRP group (Figure 4A [d and e] and 4B [d and e]). Histological scoring was utilized to evaluate fiber structure, fiber arrangement, rounding of nuclei, inflammation, increased vascularity, and cell density. The TA+PRP group had a lower score compared with the NS, TA, and PRP groups but a similar score compared with the NOR group both in terms of the total score and each item’s score (Figure 4D and 4E). Polarized light microscopy indicated the presence of more small Col 3 fibers (green color) and immature Col 1 fibers (red color) instead of mature Col 1 fibers (golden color) in the PRP group compared with the TA+PRP group (Figure 4C). The high level of Col 1 and the low level of Col 3 in the TA+PRP group represented mature fibrosis (Figure 4F). We further validated these observations with immunohistochemical staining of Col 1 and Col 3 (Figure 5A and 5B).
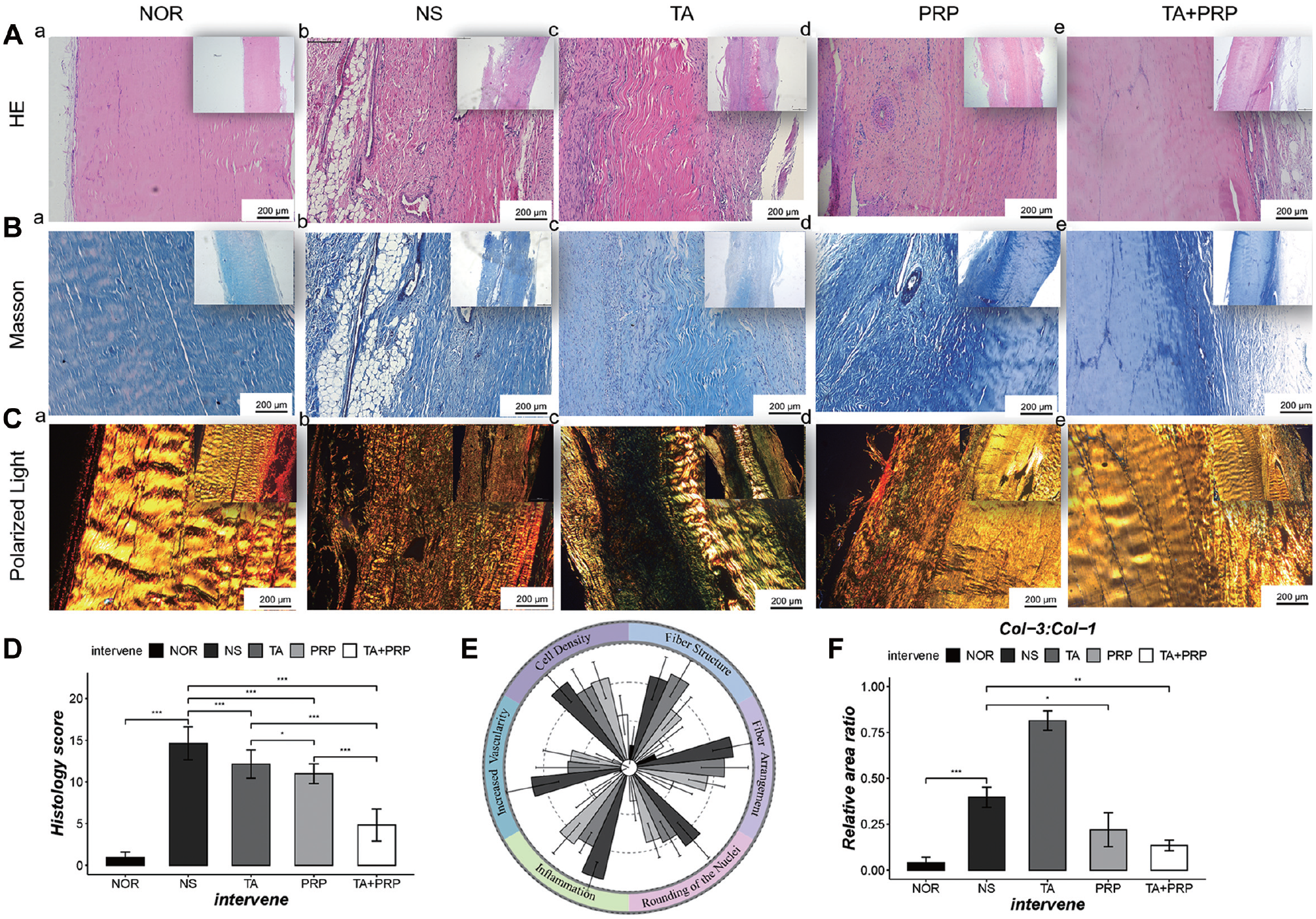
Histological evaluation of tendon samples at 8 weeks after the tendinopathy model was induced by collagenase. Representative (A) hematoxylin and eosin staining, (B) Masson trichrome staining, and (C) sirius red staining observed on polarized light microscopy of the tendons in all groups. (D) The total histology score indicated the best treatment effect in the TA+PRP group. (E) Histology score of 6 parameters. (F) The ratio of type III collagen (Col-3) to type I collagen (Col-1) evaluated by sirius red staining observed on polarized light microscopy. (A-C) Scale bar: 200 μm. Data are presented as the mean ± SD. *P < .05. NOR, normal control; NS, normal saline; PRP, platelet-rich plasma; TA, triamcinolone acetonide.
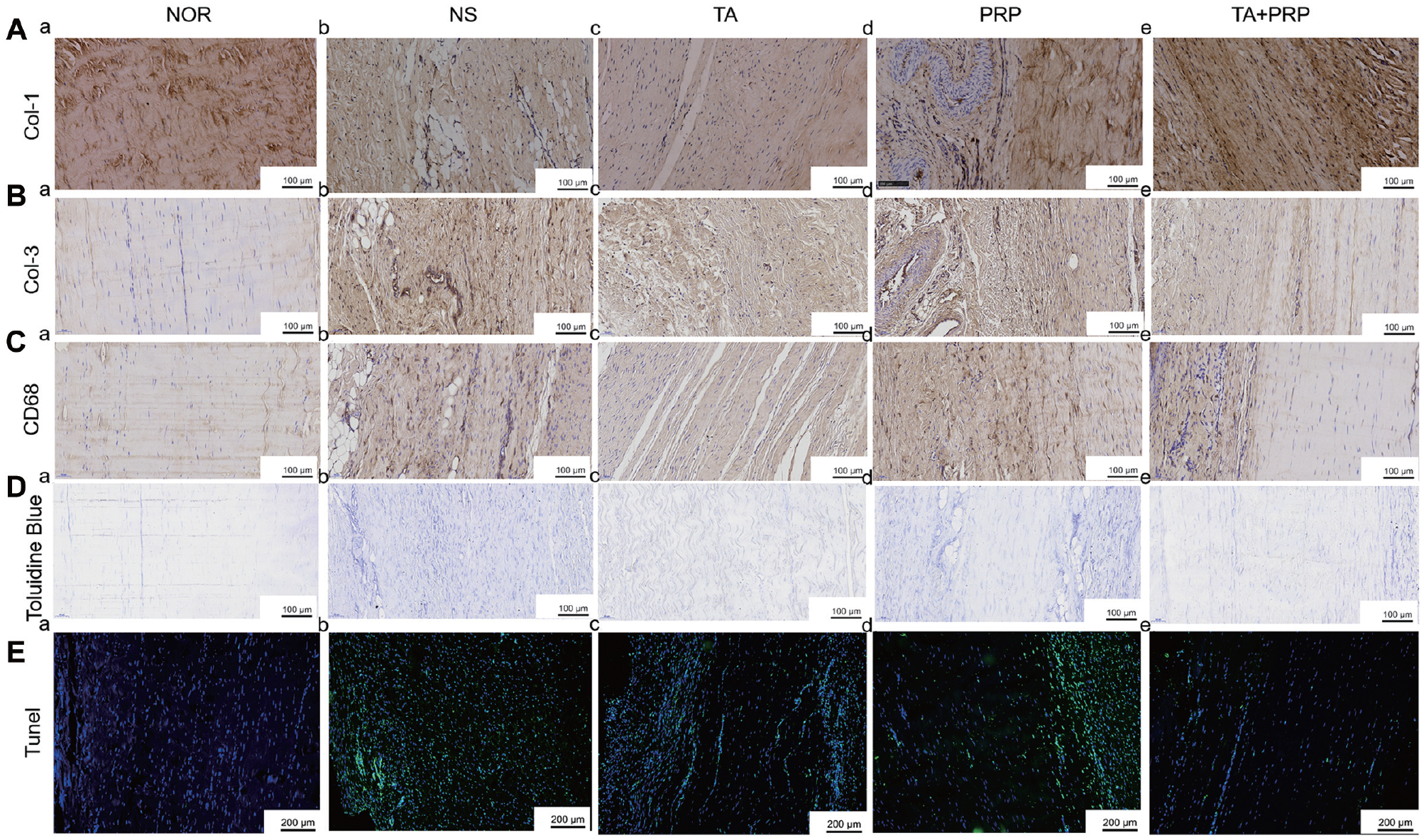
Immunohistochemical and specific staining at 8 weeks after the tendinopathy model was induced by collagenase. (A-C) Immunohistochemical staining of type I collagen (Col-1), type III collagen (Col-3), and CD68. (D) Mast cells were detected with toluidine blue staining. (E) Apoptosis in tendinopathy was detected by the TUNEL assay. Scale bars: (A-D) 100 μm and (E) 200 μm. NOR, normal control; NS, normal saline; PRP, platelet-rich plasma; TA, triamcinolone acetonide.
Evaluation of Inflammation and Cell Apoptosis
In addition to collagen fiber arrangement, the observed histology of tendon tissue also revealed the extent of inflammatory cell infiltration. In the TA+PRP group, less infiltration of inflammatory cells was detected compared with the PRP group on hematoxylin and eosin staining (Figure 4A). To evaluate inflammation, we further examined macrophages and mastocytes in these repaired tendons with macrophage marker CD68 immunohistochemical staining and mastocyte-specific toluidine blue staining (Figure 5C and 5D). In contrast to the PRP group, few macrophages and mastocytes could be observed in the TA+PRP group at 8 weeks after the collagenase injection. These results indicated that the remaining inflammatory response was significantly different between the PRP and TA+PRP groups. These observations were further corroborated by quantifying cell apoptosis via the TUNEL assay, with the TA+PRP group displaying few positive cells, whereas a great number of positive cells could be detected within the damaged area in the PRP group (Figure 5E).
Evaluation of Collagen Fibril Formation
The diameter of collagen fibrils was previously demonstrated to exert a profound influence on the mechanical characteristics of ligaments and tendons. 9 We thus further evaluated the ultrastructure of collagen fibrils by TEM (Figure 6A). More large collagen fibrils were observed in TEM transverse sections of the TA+PRP and PRP groups compared with the NS or TA group (Figure 6A). Although the PRP group exhibited slightly fewer large collagen fibrils than the TA+PRP group (Figure 6B [c and e]), more importantly, there was still the presence of extremely thin small fibers existing in the PRP group (Figure 6A and 6B). The quantification of collagen fibril diameters also revealed a different size distribution of collagen fibrils (Figure 6B). In summary, the TA+PRP group achieved the best result in terms of the collagen fibril diameter compared with the other treatment groups.
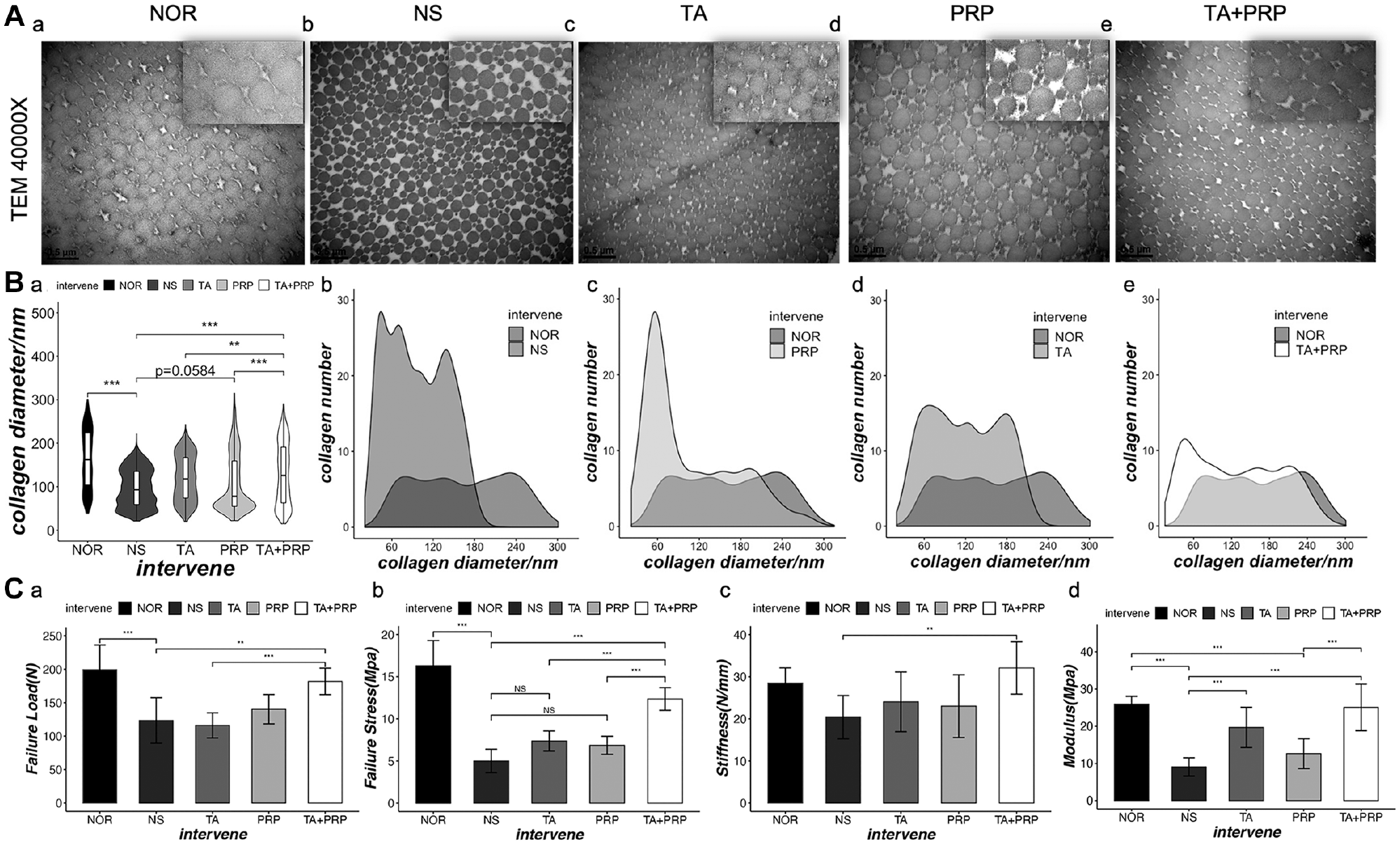
Transmission electron microscopy (TEM) and mechanical properties of tendons at 8 weeks after the tendinopathy model was induced by collagenase. (A) Representative TEM images of healed tendons in all groups. (B) Quantitative (a) mean diameters and (b-e) distribution of the collagen fibrils. (C) Mechanical properties of the healed tendons. Scale bars: (A) 0.5 μm and (A: picture-in-picture) 0.2 μm. Data are presented as the mean ± SD. *P < .05. NOR, normal control; NS, normal saline; PRP, platelet-rich plasma; TA, triamcinolone acetonide.
Evaluation of Biomechanical Properties
Mechanical performance is one of the key parameters for evaluating repaired tendons. During mechanical testing, the tendon samples were removed from the testing machine after reaching the maximum tension load. The failure load was significantly greater in the TA+PRP group than in the NS group (181.9 ± 19.82 vs 123.4 ± 34.00, respectively). Although the difference between the PRP and TA+PRP groups was not statistically significant (140.3 ± 21.96 vs 181.9 ± 19.82, respectively), the TA+PRP group was the only treatment group that showed significant improvement over the NS group (Figure 6C [a]). The TA+PRP group also exhibited improved scores in most of the other parameters being assessed including failure stress, stiffness, and the Young modulus (Figure 6C [b-d]). The TA+PRP group had significantly better results than the PRP group in failure stress (12.35 ± 1.346 vs 6.86 ± 1.073, respectively) and the Young modulus (25.05 ± 6.261 vs 12.62 ± 3.992, respectively). There were, however, no significant differences in the failure load and stiffness between the PRP and TA+PRP groups, which may likely be because of the relatively small sample size (n = 8).
Discussion
Because of limitations in the intrinsic healing capacity of the tendon and unclear pathological mechanisms of tendinopathy, the clinical treatment of tendinopathy remains an intractable challenge. PRP is a popular regenerative treatment modality with several advantages such as its low cost, abundant source, convenient preparation, and negligible immunogenicity. The strategy of enhancing the efficacy of PRP application in tendinopathy has always been a spotlight in the sports medicine field.4,61 To make the therapy more targeted, not only should the components of PRP be adjusted, but the usage mode should also be modified to suit the different periods and stages of tendinopathy in clinical practice to attain the best results. Our study suggests that the primary use of GCs could improve the regenerative effects of PRP in an early inflammatory rabbit Achilles tendinopathy model. The results (Table 1) demonstrated the following: (1) TSPCs treated with PRP showed the upregulation of proinflammatory and extracellular matrix remodeling–related genes but not anti-inflammatory genes. (2) The successive use of TA and PRP in vitro resulted in a conducive state of cell proliferation, senescence, and apoptosis. (3) The sequential therapy of GCs followed by PRP could promote enhanced tendon regeneration with a less inflammatory response, improved collagen remodeling, and better mechanical properties than the sole use of either one in an early inflammatory tendinopathy model.
Key Findings in Our Study a

MRI, magnetic resonance imaging; PRP, platelet-rich plasma; TA, triamcinolone acetonide; TSPC, tendon stem/progenitor cell.
Mechanisms of PRP in Tissue Regeneration
Despite numerous clinical and basic research studies that have been performed to explore the therapeutic effects of PRP in musculoskeletal system disorders, its underlying mechanisms remain unclear. To the best of our knowledge, we evaluated the entire transcriptome gene expression changes in TSPCs treated with PRP using RNA-seq. GO term analysis of upregulated genes in TSPCs treated with PRP suggested that the effects of PRP on TSPCs included the modulation of inflammation and immunity, cell migration, and matrix remodeling (Figure 1). Platelet granules were previously considered as crucial modulators of immune responses and important sources of chemokines, endothelial cell modulators, proinflammatory and anti-inflammatory mediators, and growth factors. 43 A multitude of inflammatory effects can be exerted by platelets both in the local environment and systemically. PRP was also previously considered to function in tissue repair and remodeling by promoting progenitor cell recruitment; releasing chemokines, proangiogenic factors, cytokines, and growth factors; and modulating the recruitment and activation of leukocytes and stromal cells through the secretion of MMPs. 47 Dragoo et al 18 demonstrated that even leukocyte-poor PRP caused greater inflammation than did an injection of saline. In an in vitro cartilage-related study, Pereira et al 45 demonstrated that platelet products (PRP and platelet lysate) triggered regeneration by enhancing the inflammatory response and promoting transient inflammation. Various inflammatory mediators such as TNF-α, IL15, and IL18 had been demonstrated before to play a positive role in wound healing after an injury. 42 Previous microarray and protein array data of tendon fibroblasts cultured in PRP-containing media also showed similar results, suggesting that PRP activated the proinflammatory TNF-α and NF-κB pathways. 27 PRP was reported to activate fibroblast activity and collagen remodeling but not collagen synthesis. 27 Our RNA-seq results provided even more data that are helpful for further exploring the mechanism of PRP treatment. Although a transient increase of proinflammatory cytokines could mediate repair and regeneration after a skeletal muscle injury, several research studies have demonstrated that the regenerative capacity will be diminished if inflammatory signaling is exceedingly high or persists chronically.26,30,34,50 Therefore, we hold the opinion that failure to resolve persistent proinflammatory signaling in inflammatory tendinopathy results in dysregulated regeneration and repair effects upon PRP treatment.
PRP Failed to Mitigate Inflammation in Tendinopathy
Previous studies had established the animal tendinopathy model by a local collagenase injection, which exhibits similar histological changes to the clinical human model.54,61 The PRP treatment in our study failed to alleviate the high inflammatory environment during early inflammatory tendinopathy, as PRP was observed to exert a proinflammatory but not anti-inflammatory effect. 27 In our study, there was still an obvious inflammatory response in the treated tendon at 8 weeks after the collagenase injection (Figure 4A [d]). Notably, a great number of mast cells still resided in the PRP group, in addition to macrophages (Figure 5C and 5D). Mast cells were reported to play a crucial role in the inflammatory process, neoangiogenesis, and cell activity by rapidly releasing various mediators and characteristic granules that mediate the recruitment and activation of B cells, T cells, neutrophils, monocytes, and dendritic cells. 41 Previous scientific evidence has demonstrated that neural “sprouting” or neoinnervation accompanied neovascularization and is responsible for the pain encountered in chronic tendinopathy. 2 Thus, the neoangiogenesis observed within tendon tissue of the PRP group might explain the residual pain observed in some patients with poorer efficacy. Furthermore, mast cells could cause pain by stimulating the synthesis of leukotrienes and prostaglandins. 57 All these results proved the persistence of chronic inflammatory tendinopathy after treatment with PRP alone.
The Inflammatory Environment Might Dysregulate the Tissue Remodeling Effects of PRP
Although M2 macrophages also showed an anti-inflammatory effect and promoted extracellular matrix deposition and tissue repair, 13 it was considered to be linked to scar formation rather than tissue regeneration. 25 The resulting newly formed tissue still does not regenerate the structure, composition, and material properties of a normal tendon. Growth factors in PRP including TGF-β were thought to play a critical role during the remodeling phase of tendon healing. 58 TGF-β isoforms are believed to play a key regulatory role in the healing of fetal tendon wounds, resulting in the regeneration of original tissue. 6 Yet, the treated area in the PRP group with macrophage infiltration in our study appeared similar to immature scar tissue with random and small collagen fibers and vascular infiltration (Figure 4A [d] and 4B [d]). Therefore, we speculated that the inflammatory environment mostly interfered with the tissue remodeling process of PRP treatment.
Col 3 often plays the role of a rapid “patch” to the area of damage/injury and is then gradually replaced by Col 1, with an eventual restoration of the normal tendon ultrastructure during the remodeling process. 42 In our study, widespread Col 3 fibers were still observed via sirius red staining (Figure 4C) and immunohistochemistry (Figure 5B) in the area of intense inflammation in the PRP group at 8 weeks after treatment. The incorporation of Col 3 into the main fiber bundles has been reported to reduce the average collagen fiber diameter. 33 Recent studies have indicated that the diameter of collagen fibrils significantly affects biomechanical properties in tendons and ligaments.35,37 In our study, the TEM results showing the tiny collagen fiber as being between near-normal and undesired biomechanics (Figure 6C) also support the association indirectly. Based on previous experience, the healing process of tendinopathy could be subdivided into 3 distinct phases: inflammation, proliferation, and remodeling. 17 The natural expression pattern of cytokines regulating the biological process varies dramatically during the different phases of healing. 58 Under normal conditions, the cytokines associated with tissue remodeling would be upregulated during the remodeling phase after inflammation has subsided. Thus, manipulation of the inflammatory environment is equally important by supplementing cytokines via the administration of PRP. This may explain the inflammatory environment as the prime cause of the contradictory results of PRP therapeutic effects on tendinopathy.
The Sequential Therapy of GCs and PRP Provides a New Strategy for the Clinical Management of Inflammatory Tendinopathy
Anti-inflammatory drugs are often used to decrease the level of proinflammatory mediators and suppress the recruitment and activation of leukocytes in affected areas. GCs are the most common and useful medications for the treatment of autoimmune and inflammatory diseases. 28 The transactivation and transrepression mechanisms through the binding of GCs to the GC receptor are known to be responsible for their anti-inflammatory effects. As a widely used GC in clinical practice, TA is recognized as exerting a strong and persistent anti-inflammatory effect and is readily available at a low price. 23 Also, although leukocyte-rich PRP is now widely used in tendinopathy treatment, previous studies12,46 showed that leukocytes were the main source of proinflammatory cytokines and catabolic enzymes such as IL1B, TNF-α, and MMPs. Yan et al 61 also demonstrated that leukocyte-rich PRP would impair the repair process because of incitation of the local inflammatory condition compared with leukocyte-poor PRP in tendinopathy. In this study, we believed that the inflammatory environment in early-stage tendinopathy would impair the treatment effect of PRP. On the basis of this, we chose leukocyte-poor PRP for our sequential therapy.
An acute classic inflammatory reaction was observed around the first 3 to 7 days with irregularly arranged collagen fibers, obvious edema, inflammatory cell infiltration, and vascular proliferation (Appendix Figure A3). Thus, TA treatment was carried out before PRP administration at 1 week after the collagenase injection to dissipate the strong inflammatory response during the early stages of tendinopathy. A significant decrease in the inflammatory response was detected at 8 weeks in the TA+PRP group compared with the PRP group (Figures 4 and 5). A previous concern about GC injections was that GCs could reduce collagen synthesis and cell proliferation and may affect the differentiation of tendon-derived cells as demonstrated by both in vitro and in vivo data. 14 There were also reports of poor long-term outcomes such as worsening of symptoms and tendon ruptures after multiple GC injections were performed for the treatment of tendinopathy. But, some researchers reported that PRP exerts a protective effect against the negative effects of corticosteroids on both normal and inflammatory tenocytes. 32 Wong et al 60 demonstrated that platelet-derived growth factor, which is one of the major components of PRP, could be used to mitigate the cytotoxicity of corticosteroids. The results of the in vitro experiments in our study also indicated that PRP could alleviate the detrimental effects of TA on cell viability, senescence, and apoptosis as well as enhance its efficacy. After the inflammatory environment was controlled by a TA injection, PRP was used at 2 weeks after the collagenase injection to start the tissue regenerative process. The different MRI results in the TA, PRP, and TA+PRP groups also suggested that TA and PRP worked on different parts in the repair process of tendinopathy and that TA could even play a critical role in assisting the regenerative effects of PRP. The improved regeneration, as evidenced by better organized collagen fibers, larger fiber diameters, and better mechanical properties in the in vivo experiments, further supported the effectiveness of sequential therapy.
Limitations and Future Studies
The complex pathological process of tendinopathy in humans could not be perfectly recapitulated with the collagenase-induced tendinopathy model. Further clinical testing is needed to verify the superiority of sequential therapy. Also, as leukocyte-rich PRP is now wildly used in musculoskeletal disorders, we should test whether sequential therapy is suitable for leukocyte-rich PRP in the future. An appropriate concentration of leukocyte-rich PRP may be helpful in the treatment of acute tendon disorders. Additionally, as it is for choosing GCs for sequential therapy, other popular GCs in clinical practice such as betamethasone and methylprednisolone need to be verified in the future. Furthermore, the core mechanisms of sequential therapy are not completely understood. We will further explore the key inflammatory cytokines and signaling pathways modulating the regenerative effects of PRP in inflammatory tendinopathy with varied sequencing at different time points, which could provide cues for developing a more targeted anti-inflammatory therapy with specific anti-inflammatory drugs in the future. Although macrophage polarization might also play an important role in this process, we lack knowledge about macrophage polarization. Further studies will verify the shift in macrophage polarization during the process of sequential therapy with the mouse/rat model and more time points.
Conclusion
This study demonstrated that the sequential therapy of GCs and PRP achieved a better therapeutic effect on tendinopathy than the sole use of PRP alone at an early stage in a rabbit model. The primary use of GCs dissipated the strong inflammatory response during the early stage of tendinopathy, which in turn provided a more conducive working environment for PRP.
Authors
Dengfeng Ruan, MD (Department of Orthopedic Surgery, Second Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, China; Orthopedics Research Institute, Zhejiang University, Hangzhou, China; Key Laboratory of Motor System Disease Research and Precision Therapy of Zhejiang Province, Zhejiang University School of Medicine, Hangzhou, China; Institute of Sports Medicine, Zhejiang University, Hangzhou, China; China Orthopedic Regenerative Medicine Group, Hangzhou, China); Chenqi Tang, MD (Department of Orthopedic Surgery, Second Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, China; Orthopedics Research Institute, Zhejiang University, Hangzhou, China; Key Laboratory of Motor System Disease Research and Precision Therapy of Zhejiang Province, Zhejiang University School of Medicine, Hangzhou, China; Institute of Sports Medicine, Zhejiang University, Hangzhou, China; Dr Li Dak Sum & Yip Yio Chin Center for Stem Cells and Regenerative Medicine, Zhejiang University School of Medicine, Hangzhou, China; Key Laboratory of Tissue Engineering and Regenerative Medicine of Zhejiang Province, Zhejiang University School of Medicine, Hangzhou, China); Yang Fei, MD, Shengjun Qian, MD (Department of Orthopedic Surgery, Second Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, China; Orthopedics Research Institute, Zhejiang University, Hangzhou, China; Key Laboratory of Motor System Disease Research and Precision Therapy of Zhejiang Province, Zhejiang University School of Medicine, Hangzhou, China; Institute of Sports Medicine, Zhejiang University, Hangzhou, China); Xinyu Xiang, BS (Zhejiang University -University of Edinburgh Institute, Zhejiang University School of Medicine, Haining, China); Jialu Xu (Department of Infectious Diseases, First Affiliated Hospital, Wenzhou Medical University, Wenzhou, China; Hepatology Institute, Wenzhou Medical University, Wenzhou, China; Key Laboratory of Hepatology, Wenzhou Medical University, Wenzhou, China); Zizhan Huang, MD (Department of Orthopedic Surgery, Second Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, China; Orthopedics Research Institute, Zhejiang University, Hangzhou, China; Key Laboratory of Motor System Disease Research and Precision Therapy of Zhejiang Province, Zhejiang University School of Medicine, Hangzhou, China; Institute of Sports Medicine, Zhejiang University, Hangzhou, China); Xiao Chen, PhD (Dr Li Dak Sum & Yip Yio Chin Center for Stem Cells and Regenerative Medicine, Zhejiang University School of Medicine, Hangzhou, China; Department of Orthopedic Surgery, Second Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, China; Key Laboratory of Tissue Engineering and Regenerative Medicine of Zhejiang Province, Zhejiang University School of Medicine, Hangzhou, China; China Orthopedic Regenerative Medicine Group, Hangzhou, China); Boon Chin Heng (Peking University School of Stomatology, Beijing, China); Zi Yin, PhD (Dr Li Dak Sum & Yip Yio Chin Center for Stem Cells and Regenerative Medicine, Zhejiang University School of Medicine, Hangzhou, China; Department of Orthopedic Surgery, Sir Run Run Shaw Hospital, Zhejiang University School of Medicine, Hangzhou, China; Key Laboratory of Tissue Engineering and Regenerative Medicine of Zhejiang Province, Zhejiang University School of Medicine, Hangzhou, China; China Orthopedic Regenerative Medicine Group, Hangzhou, China); Weishan Chen, MD (Department of Orthopedic Surgery, Second Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, China; Orthopedics Research Institute, Zhejiang University, Hangzhou, China; Key Laboratory of Motor System Disease Research and Precision Therapy of Zhejiang Province, Zhejiang University School of Medicine, Hangzhou, China; Institute of Sports Medicine, Zhejiang University, Hangzhou, China); Wanlu Liu, PhD (Department of Orthopedic Surgery, Second Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, China; Zhejiang University -University of Edinburgh Institute, Zhejiang University School of Medicine, Haining, China; Dr Li Dak Sum & Yip Yio Chin Center for Stem Cells and Regenerative Medicine, Zhejiang University School of Medicine, Hangzhou, China); Weiliang Shen, MD (Department of Orthopedic Surgery, Second Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, China; Orthopedics Research Institute, Zhejiang University, Hangzhou, China; Key Laboratory of Motor System Disease Research and Precision Therapy of Zhejiang Province, Zhejiang University School of Medicine, Hangzhou, China; Institute of Sports Medicine, Zhejiang University, Hangzhou, China; Dr Li Dak Sum & Yip Yio Chin Center for Stem Cells and Regenerative Medicine, Zhejiang University School of Medicine, Hangzhou, China; Key Laboratory of Tissue Engineering and Regenerative Medicine of Zhejiang Province, Zhejiang University School of Medicine, Hangzhou, China; China Orthopedic Regenerative Medicine Group, Hangzhou, China; Department of Sports Medicine, Zhejiang University School of Medicine, Hangzhou, China); and Hongwei Ouyang, MD, PhD (Dr Li Dak Sum & Yip Yio Chin Center for Stem Cells and Regenerative Medicine, Zhejiang University School of Medicine, Hangzhou, China; Department of Orthopedic Surgery, Second Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, China; Zhejiang University -University of Edinburgh Institute, Zhejiang University School of Medicine, Haining, China; Key Laboratory of Tissue Engineering and Regenerative Medicine of Zhejiang Province, Zhejiang University School of Medicine, Hangzhou, China; Department of Sports Medicine, Zhejiang University School of Medicine, Hangzhou, China; China Orthopedic Regenerative Medicine Group, Hangzhou, China).
Supplemental Material
sj-pdf-1-ajs-10.1177_03635465211037354 – Supplemental material for Early-Stage Primary Anti-inflammatory Therapy Enhances the Regenerative Efficacy of Platelet-Rich Plasma in a Rabbit Achilles Tendinopathy Model
Supplemental material, sj-pdf-1-ajs-10.1177_03635465211037354 for Early-Stage Primary Anti-inflammatory Therapy Enhances the Regenerative Efficacy of Platelet-Rich Plasma in a Rabbit Achilles Tendinopathy Model by Dengfeng Ruan, Chenqi Tang, Yang Fei, Shengjun Qian, Xinyu Xiang, Jialu Xu, Zizhan Huang, Xiao Chen, Boon Chin Heng, Zi Yin, Weishan Chen, Wanlu Liu, Weiliang Shen and Hongwei Ouyang in The American Journal of Sports Medicine
Footnotes
Acknowledgements
The authors acknowledge the staff at the Universal Medical Imaging Diagnostic Center for their assistance with MRI. The authors also thank the assistance of the Animal Research Center, Zhejiang University, and the Bioultrastructure Analysis Laboratory of the Analysis Center of Agrobiology and Environment Sciences, Zhejiang University, for the success of TEM in this research.
Submitted October 29, 2020; accepted May 4, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported by the National Natural Science Foundation of China (NSFC; 2017YFA0104900), NSFC grants (81874019, 81972099, 81772418, 81871764), the Zhejiang Provincial Natural Science Foundation (LR20H060001), the Program for the Top Young Clinical Talents of the Zhejiang University School of Medicine (A class), and Fundamental Research Funds for the Central Universities. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.