
Abstract
Background:
Outcomes of revision hip arthroscopy in the athletic population have not been well established.
Purpose:
(1) To report clinical outcomes for high-level athletes undergoing revision hip arthroscopy in the setting of femoroacetabular impingement syndrome (FAIS) or labral tears and (2) to compare these outcomes against a propensity-matched group of high-level athletes undergoing primary hip arthroscopy.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Data for professional, college, and high school athletes were prospectively collected and retrospectively reviewed between January 2012 and October 2018. Patients were included if they underwent revision or primary hip arthroscopy and had preoperative and minimum 2-year patient-reported outcome (PRO) scores for modified Harris Hip Score (mHHS), Non-Arthritic Hip Score (NAHS), Hip Outcome Score Sports-Specific Subscale (HOS-SSS), and visual analog scale (VAS) for pain. The findings and outcomes of revision athletes were compared with a propensity-matched control group of high-level athletes undergoing primary hip arthroscopy.
Results:
A total of 32 hips (29 patients) undergoing revision hip arthroscopy and 92 hips (88 patients) undergoing primary hip arthroscopy were included in our final analysis with a median follow-up time of 29.5 months (95% CI, 27.2-32.1 months) and 36.5 months (95% CI, 33.5-37.7 months), respectively. Athletes undergoing revision surgery showed significant improvement in all recorded PRO measurements and achieved patient acceptable symptomatic state (PASS) and minimal clinically important difference (MCID) for mHHS at high rates (80.6% and 83.9%, respectively). When compared with a propensity-matched primary control group, patients undergoing revision surgery demonstrated lower preoperative and postoperative scores for mHHS, NAHS, and HOS-SSS, but the magnitude of improvement in functional scores was similar between groups. Athletes undergoing revision surgery achieved PASS for HOS-SSS at lower rates than the control group (P = .005), and they were less likely to attempt to return to sport compared with the control group (62.5% vs 87.0%; P < .01).
Conclusion:
Revision hip arthroscopy is a viable treatment option to improve PROs in high-level athletes at minimum 2-year follow-up. The study group showed significant improvement in functional scores and a high rate of successful outcomes. They experienced similar magnitude of improvement as that of a propensity-matched control group; however, they achieved lower postoperative PRO scores and attempted to return to sport at lower rates.
Successful outcomes and high rates of return to sport (RTS) after primary hip arthroscopic surgery in athletes have been well established in the literature.11,28,36,52 Several factors, including younger age, shorter duration of symptoms, and the absence of high-grade cartilage damage, have been associated with higher rates of RTS and outcomes in high-level athletes undergoing primary hip arthroscopy; however, there is limited information on the rate of revision hip arthroscopic surgery in these patients.6,8,46,51 Further, few studies report the outcomes and clinical course of athletes undergoing revision arthroscopic surgery.35,61
Revision rates of hip arthroscopy in the general population have been reported between 1.8% and 10.3%, with age >60 years, male sex, and preoperative opioid use being risk factors for undergoing revision arthroscopic surgery.21,31-33,45,59,60 A recent systematic review on revision hip arthroscopic procedures found that the most frequent cause of revision hip arthroscopy was inadequate cam and/or pincer resection. 53 Although outcomes of revision hip arthroscopy have been well studied in the general population, there is a lack of literature on revision surgery in the athletic population.10,39,48
The purpose of this study was (1) to report clinical outcomes for high-level athletes undergoing revision hip arthroscopy in the setting of femoroacetabular impingement syndrome (FAIS) or labral tears and (2) to compare these outcomes against a propensity-matched group of high-level athletes undergoing primary hip arthroscopy. It was hypothesized that (1) high-level athletes undergoing revision hip arthroscopy would demonstrate significant improvement in patient-reported outcome (PRO) scores at minimum 2-year follow-up, and (2) high-level athletes undergoing revision hip arthroscopy would show lesser improvement in PRO scores compared with high-level athletes undergoing primary surgery.
Methods
Data Collection
All patients consented to participate in the American Hip Institute hip preservation registry. Patients who received revision or primary hip arthroscopy treatment between January 2012 and October 2018 were eligible if they reported participating in high-level competition (ie, professional, collegiate, or high school sports) within 1 year before surgery. All procedures were performed by the senior author (B.G.D.). Patients were included in the analysis if they had preoperative and minimum 2-year scores for the modified Harris Hip Score (mHHS), 1 Non-Arthritic Hip Score (NAHS), 15 Hip Outcome Score Sports-Specific Subscale (HOS-SSS), 43 and visual analog scale for pain (VAS). Patients were excluded from our analysis if they had a diagnosed ipsilateral hip condition (eg, avascular necrosis, slipped capital femoral epiphysis, or Legg-Calvé-Perthes disease), had osteoarthritis (Tönnis grade ≥2), did not have preoperative or minimum 2-year PRO measurements available, or had not undergone intra-articular procedures.
Propensity matching was performed between revision and primary hip arthroscopy cases to reduce treatment assignment bias and to make the groups comparable based on matching criteria. Patients were assessed preoperatively, 3 months postoperatively, and then at annual intervals. Patients completed an outcomes questionnaire via encrypted email, during a telephone interview, or in clinic. Preoperatively, this questionnaire included sport information and the mHHS, NAHS, HOS-SSS, and VAS scores. Postoperatively, the same outcome scores were measured in addition to the International Hip Outcome Tool 12 (iHOT-12) 30 and a questionnaire regarding RTS. Patients reported whether they had attempted to RTS within 2 years postoperatively and were considered successful if they could participate without hip pain.
Clinical outcomes were measured using the patient acceptable symptomatic state (PASS) and minimal clinically important difference (MCID). For mHHS, a value of at least 74 and >8 was used as a threshold for PASS and MCID, respectively.19,22 For HOS-SSS, a value of at least 75 and >6 was used as a threshold for PASS and MCID, respectively.19,22
Participation in the American Hip Institute Registry
Although the present study describes a unique analysis, some patient data may have been reported in other studies. All data collection received institutional review board approval (ID No. 5276).
Physical Examination
Preoperative evaluation was performed by the senior surgeon (B.G.D.) on all patients. This includes an assessment of the patient’s gait and hip range of motion (internal rotation, external rotation, flexion, abduction, and adduction) measured with the patient in the supine position. Hips were also evaluated using impingement tests and for the presence of painful internal snapping.7,18,42
Radiography
As part of the standard of care at this institution, preoperative radiographic imaging was performed with standing and supine anteroposterior pelvic, modified 45° Dunn, and false-profile views.17,26,47,65 These images were evaluated and reviewed by a clinical team of hip arthroscopy fellows and attending orthopaedic surgeons using the General Electric Healthcare Picture Archiving and Communication System. The anteroposterior supine view was used to assess the level of osteoarthritis as graded with the Tönnis system 19 and the lateral center-edge angle.17,69 Alpha angle was measured using the 45° Dunn lateral view with a cam deformity defined as an angle >55°. 50 Anterior center-edge angle of Lequense and de Seze 34 was measured using the false-profile view. The institution’s radiographic measurements have demonstrated good interobserver reliability in previously published studies.24,57,58 Magnetic resonance arthrography or magnetic resonance imaging was used to determine the presence of labral tears and other extra- and intra-articular defects.
Surgical Indication
Surgical intervention for patients undergoing both revision hip arthroscopy and primary hip arthroscopy was recommended if the combination of a patient’s medical history, physical examination, and radiographic findings indicated evidence of FAIS or labral tears in the primary setting or residual FAIS or labral retear in the revision setting. Patients experiencing moderate-to-severe pain that interfered with daily activities and their sport-specific activities were required to undergo at least 3 months of nonsurgical treatment including physical therapy, activity modification, intra-articular injections, and nonsteroidal anti-inflammatory medications.12,29
Surgical Procedure
Patients underwent revision or primary hip arthroscopy under general anesthesia on a traction table in the modified supine position. The anterolateral, midanterior, and distal lateral accessory portals were used to access the hip joint. After an interportal capsulotomy but before any intra-articular procedures were performed, a diagnostic arthroscopic examination was completed to identify and assess labral tears, articular cartilage lesions, and ligamentum teres tears. 37 Labral tears were graded using the Seldes classification system. 62 Acetabular and femoral head articular cartilage lesions were graded using the Outerbridge classification system, and chondrolabral junction damage was graded using acetabular labrum articular disruption (ALAD).44,54,64 Ligamentum teres tears were graded using the Domb and Villar classification systems.5,27 Labral tear treatment was determined intraoperatively by the senior surgeon according to the quality of the labrum and the extent of the tear.22,40 Patients were considered for labral reconstruction if nonviable labral tissues were found during diagnostic arthroscopy.23,68 Labral reconstruction was performed according to a previously published technique.13,20,55 Acetabuloplasty and femoroplasty were performed under fluoroscopic guidance to correct pincer- and cam-type morphologies, respectively.41,56 The capsule was plicated with the hip flexed to 45° and using absorbable sutures (No. 2.0 coated Vicryl polyglactin 910; Ethicon) in patients who presented without excessive stiffness, adhesive capsulitis, or insufficient capsular tissue14,25 and the 70° SlingShot Suture Manager (Pivot Medical, Inc).
Rehabilitation Protocol
All patients were instructed to use crutches to limit weightbearing (20 pounds of foot-flat weightbearing) and a brace for stability (DJO Global) to limit flexion to 90° and extension to 0°. Depending on the specific intraoperative procedures performed, a patient’s protocol was tailored ranging from 2 to 8 weeks of recovery. Patients were prescribed physical therapy for 3 months, starting as early as 1 day after surgery. In some cases, patients were advised to avoid sport-related activities based on the nature of their condition.
Statistical Analysis
An a priori power analysis was used to determine that in a 1:3 matching ratio, 20 revision cases and 60 primary cases were necessary to achieve at least 80% power based on the assumption that a mean difference of 8 points in mHHS between groups was clinically significant. Patients who underwent revision hip arthroscopy were matched to a cohort who received primary hip arthroscopy using a nearest-neighbor (Euclidean distance) propensity score matching algorithm. Matching was performed without replacement in a 1:3 ratio, and a caliper of 0.25 times the standard deviation of the logit propensity scores was used. Patients who were outside the caliper (“propensity range”) were excluded from analysis.2,3 Patients were controlled for body mass index (BMI), age at time of surgery, sex, and sports competition level. Descriptive statistics were reported for patient characteristics, intraoperative findings, surgical procedures, and PRO measurements. Statistically significant differences were noted if P < .05.
Because of the small sample size, medians accompanied by 95% confidence intervals (CIs) were reported for continuous variables. The Shapiro-Wilk test was performed to evaluate parametricity, followed by an F test to assess the variance of data. Normally distributed data with equal variances were analyzed using a 2-tailed t test, and nonparametric data were compared using a nonparametric equivalent test. Chi-square or Fisher exact test was performed to analyze categorical variables. Statistical analysis was performed using RStudio Desktop (Version 1.2.1093; RStudio) and the Real-Statistics Add-In using Microsoft Excel.
Results
Patient Characteristics
A total of 376 cases were eligible for the study. Of these, 336 (89.4%) had adequate follow-up data and met the inclusion criteria, which were (1) revision hip arthroscopy (39 cases) or primary hip arthroscopy (297 cases) performed by the senior author (B.G.D.); (2) participation in high-level sports competition within 1 year before surgery; and (3) preoperative and minimum 2-year follow-up PRO data. Ultimately, 32 of the 39 revision cases (29 patients) were successfully matched and compared with 92 cases (88 patients) from the primary hip arthroscopy control group with a median follow-up time of 29.5 months (95% CI, 27.2-32.1 months) and 36.5 months (95% CI, 33.5-37.7 months), respectively. The patient selection process is depicted in Figure 1. Patient characteristics are presented in Table 1. Most of the patients were female in both the revision and primary groups (71.9% and 67.4%, respectively) and played collegiate athletics (56.3% and 54.3%, respectively). Similarly, the median age and BMI of the patient athletes were similar between groups (Table 1).
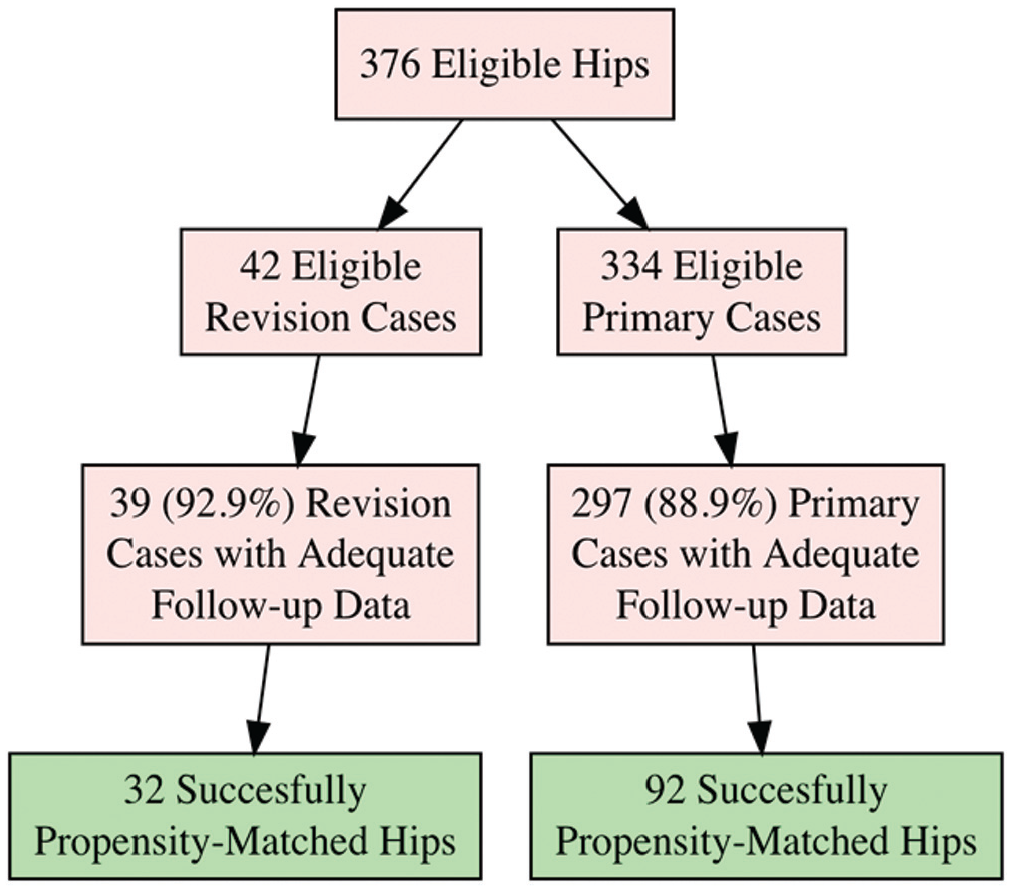
Patient selection flowchart.
Characteristics of Cohorts After Propensity Score Matching a
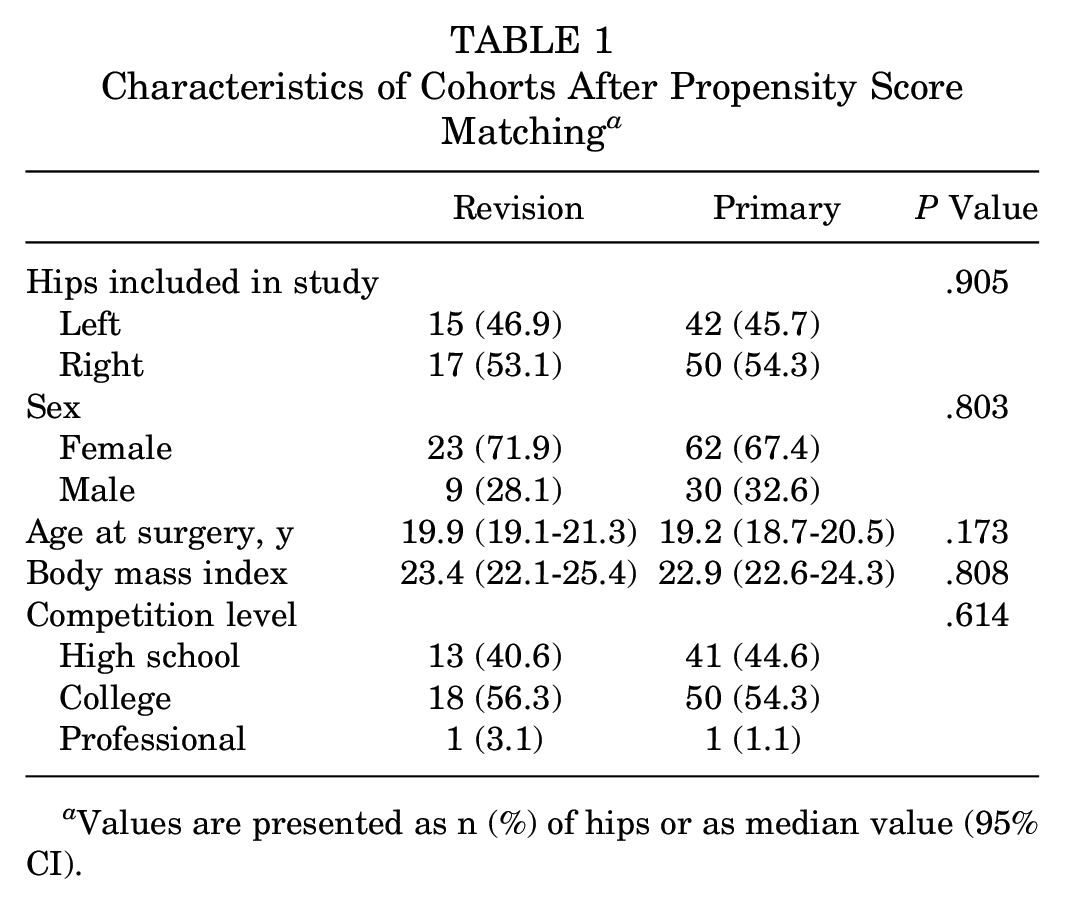
Values are presented as n (%) of hips or as median value (95% CI).
Radiographic Findings
Patients treated with revision hip arthroscopy had comparable radiographic finding to those of patients who underwent primary procedures. The majority of patients in both groups had Tönnis grade 0 (75.0% vs 69.6%; P =.616). Median preoperative alpha angle for the revision group was 50.0° (95% CI, 46.9°-55.4°). This significantly differed from the primary group, who had a median preoperative alpha angle of 60.0° (95% CI, 56.9°-62.5°). Radiographic findings are summarized in Table 2.
Radiographic Findings a
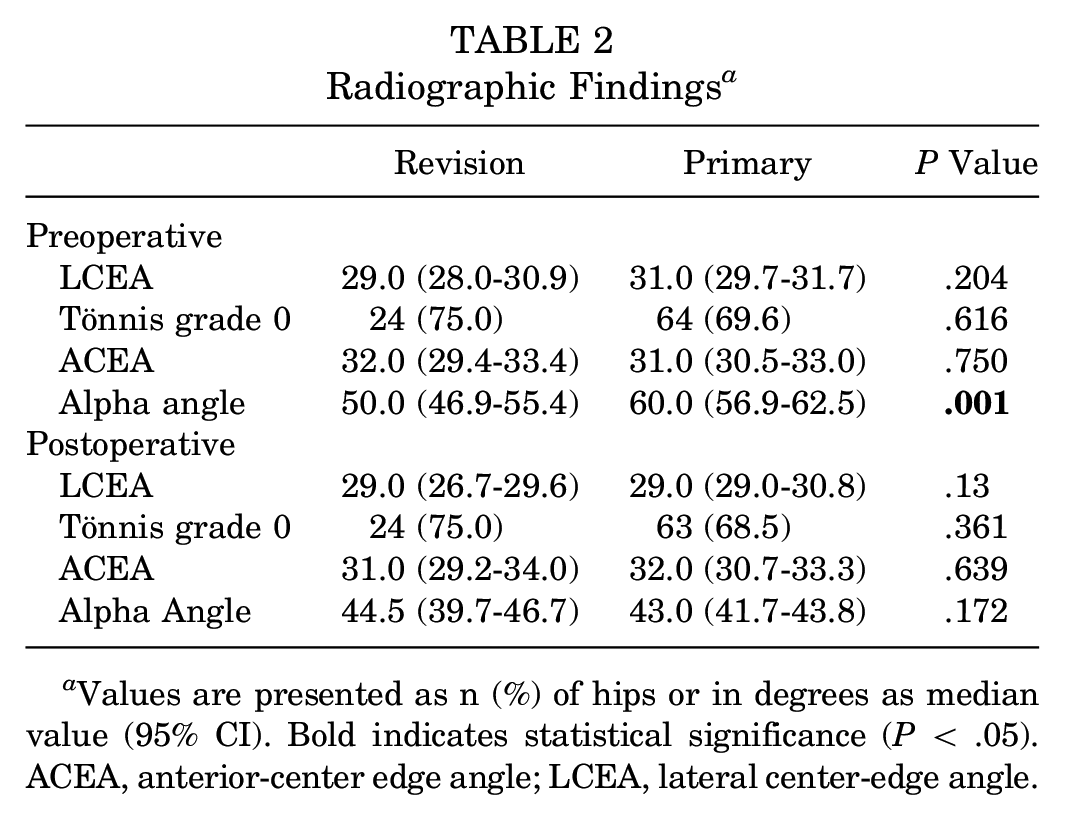
Values are presented as n (%) of hips or in degrees as median value (95% CI). Bold indicates statistical significance (P < .05). ACEA, anterior-center edge angle; LCEA, lateral center-edge angle.
Intraoperative Findings
Intraoperative findings are presented in Table 3. Type II Seldes labral tears were present in 62.5% of revision cases compared with 31.5% of primary cases. ALAD and acetabular Outerbridge grades were similar between groups. The majority of patients in both groups had no ligamentum teres damage based on the Domb classification (87.5% and 74.7% for revision and primary cases, respectively) and the Villar classification (87.5% and 74.4%, respectively).
Intraoperative Findings of the Hip Arthroscopy Groups After Propensity Score Matching a
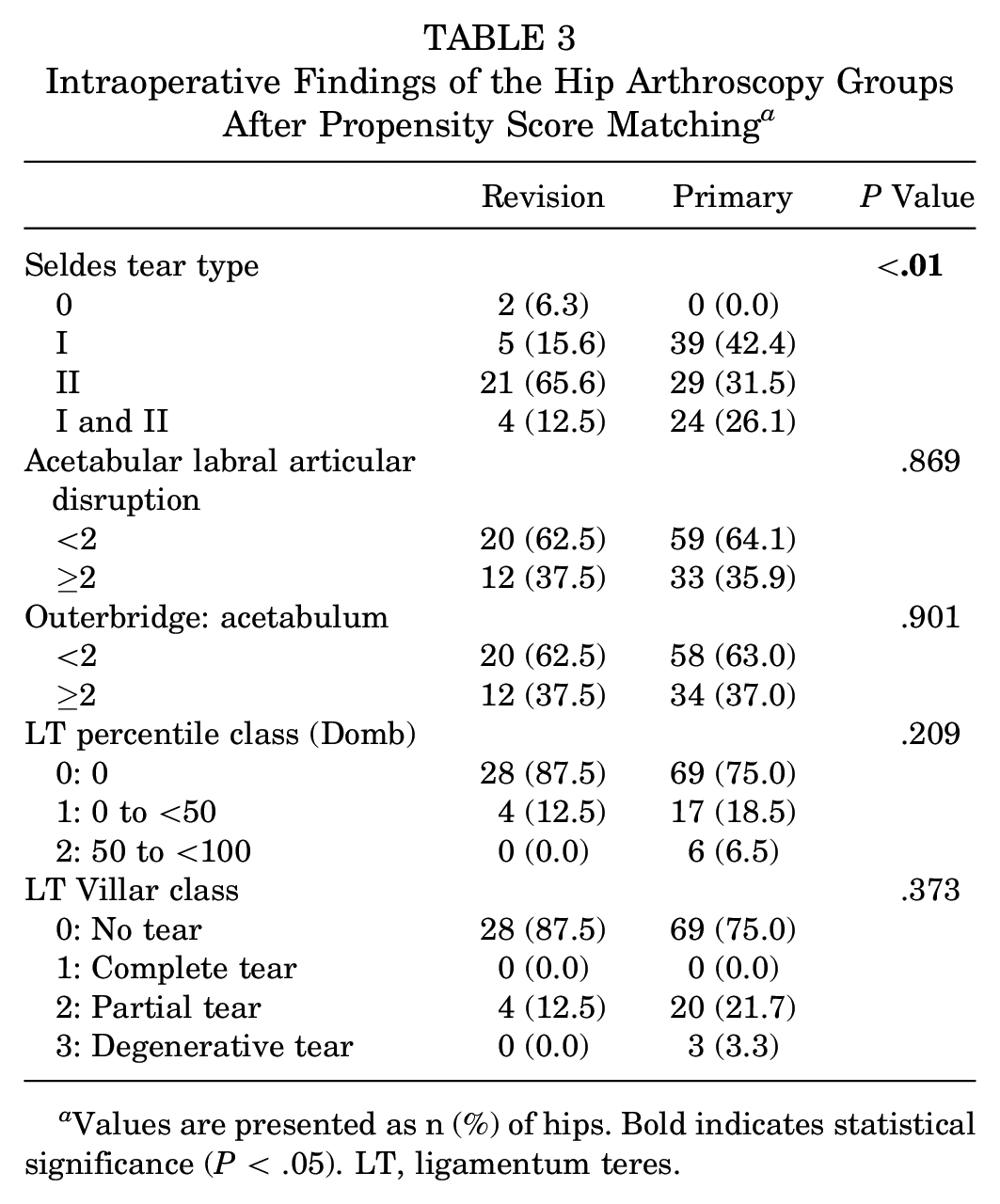
Values are presented as n (%) of hips. Bold indicates statistical significance (P < .05). LT, ligamentum teres.
Intraoperative Procedures
Surgical procedures varied between the revision and primary cohorts. Most notably, labral reconstruction was performed more commonly in the revision surgery group compared with the primary surgery group (28.1% vs 2.2%, respectively) (Figure 2). Additionally, femoroplasty was performed at lower rates in the revision surgery group than the primary surgery group (75% and 98.9%, respectively; P = .001). Acetabuloplasty was also performed at lower rates in the revision group compared with the primary group (46.9% and 82.6%, respectively; P = .002). The capsule was plicated in 68.8% of revision cases and 90.2% of primary cases. Surgical procedures are summarized in Table 4.
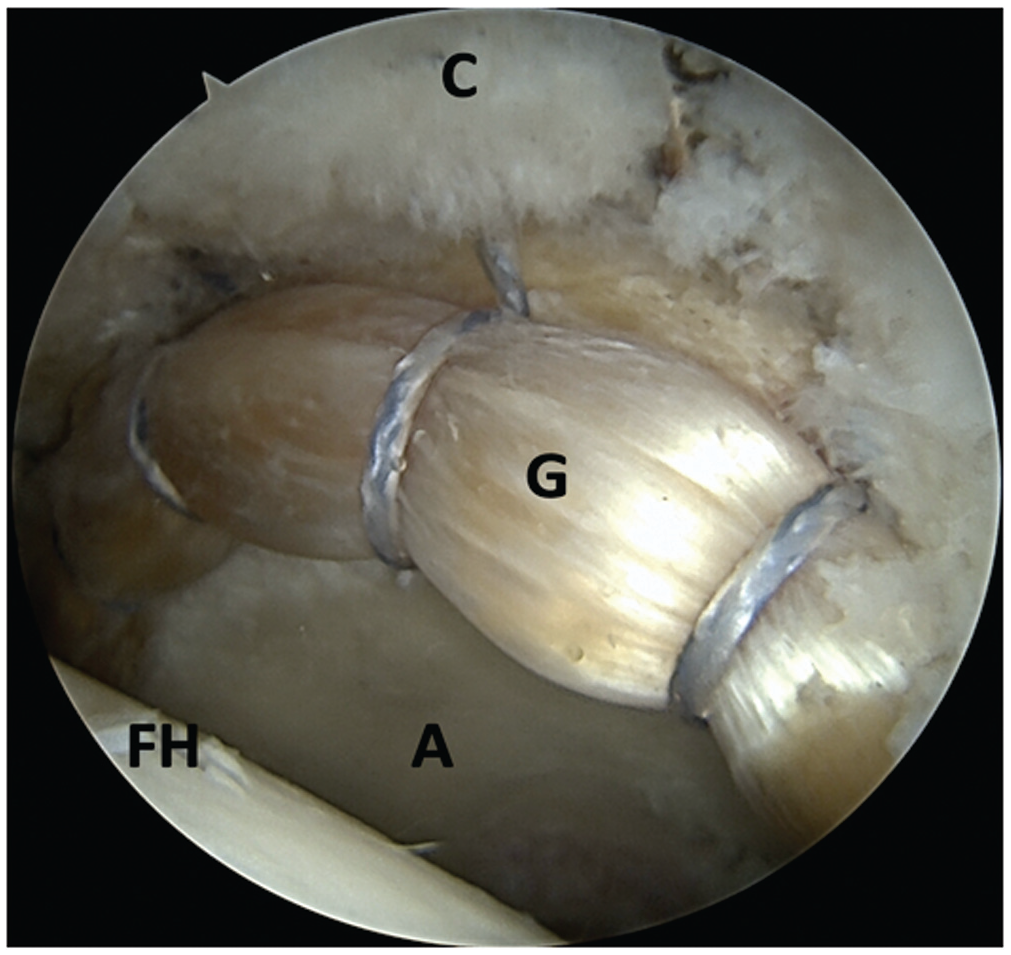
Completed labral reconstruction with allograft as viewed from the anterolateral portal in a left hip. A, acetabulum; C, capsule; FH, femoral head; G, allograft.
Surgical Procedures for Patients a
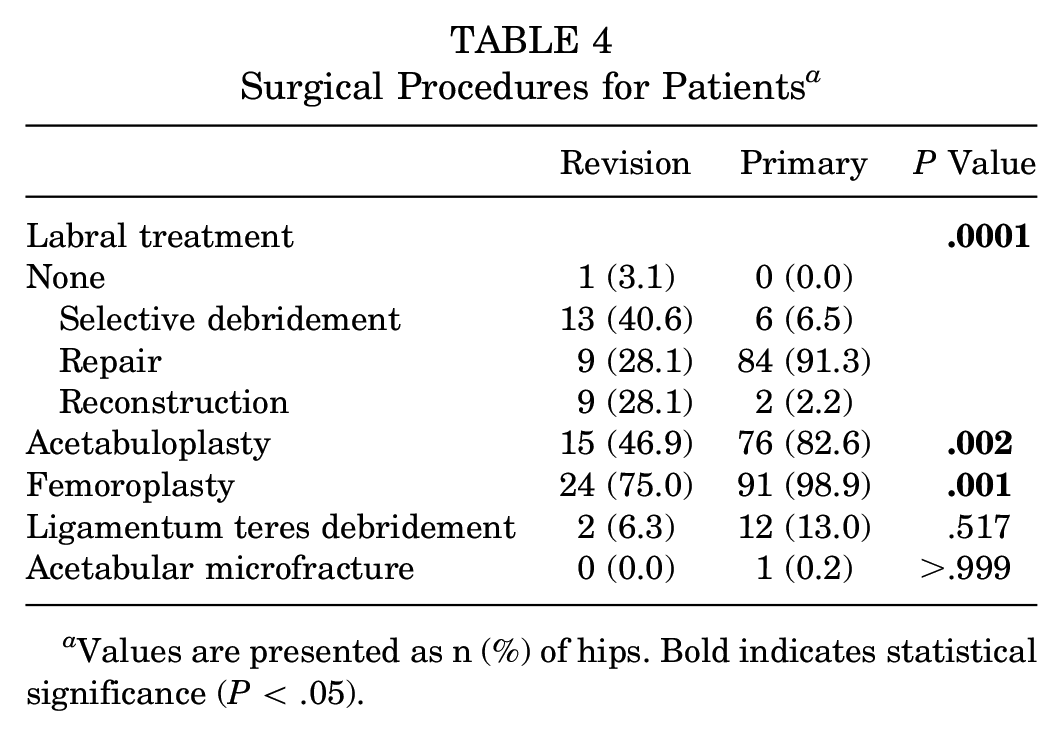
Values are presented as n (%) of hips. Bold indicates statistical significance (P < .05).
Surgical Outcomes
PRO measurements are presented in Table 5 and Figure 3. Patients undergoing revision hip arthroscopy reported significant improvements in mHHS, NAHS, HOS-SSS, and VAS for pain from preoperative to minimum 2-year follow-up (P < .001). Median mHHS improved by 22.0 points (P < .001), NAHS by 20.0 points (P < .001), HOS-SSS by 25.1 points (P < .001), and VAS by 1.9 points (P < .001).
Preoperative and Minimum 2-Year Patient-Reported Outcome Scores for Revision and Primary Hip Arthroscopy Groups After Propensity Score Matching a
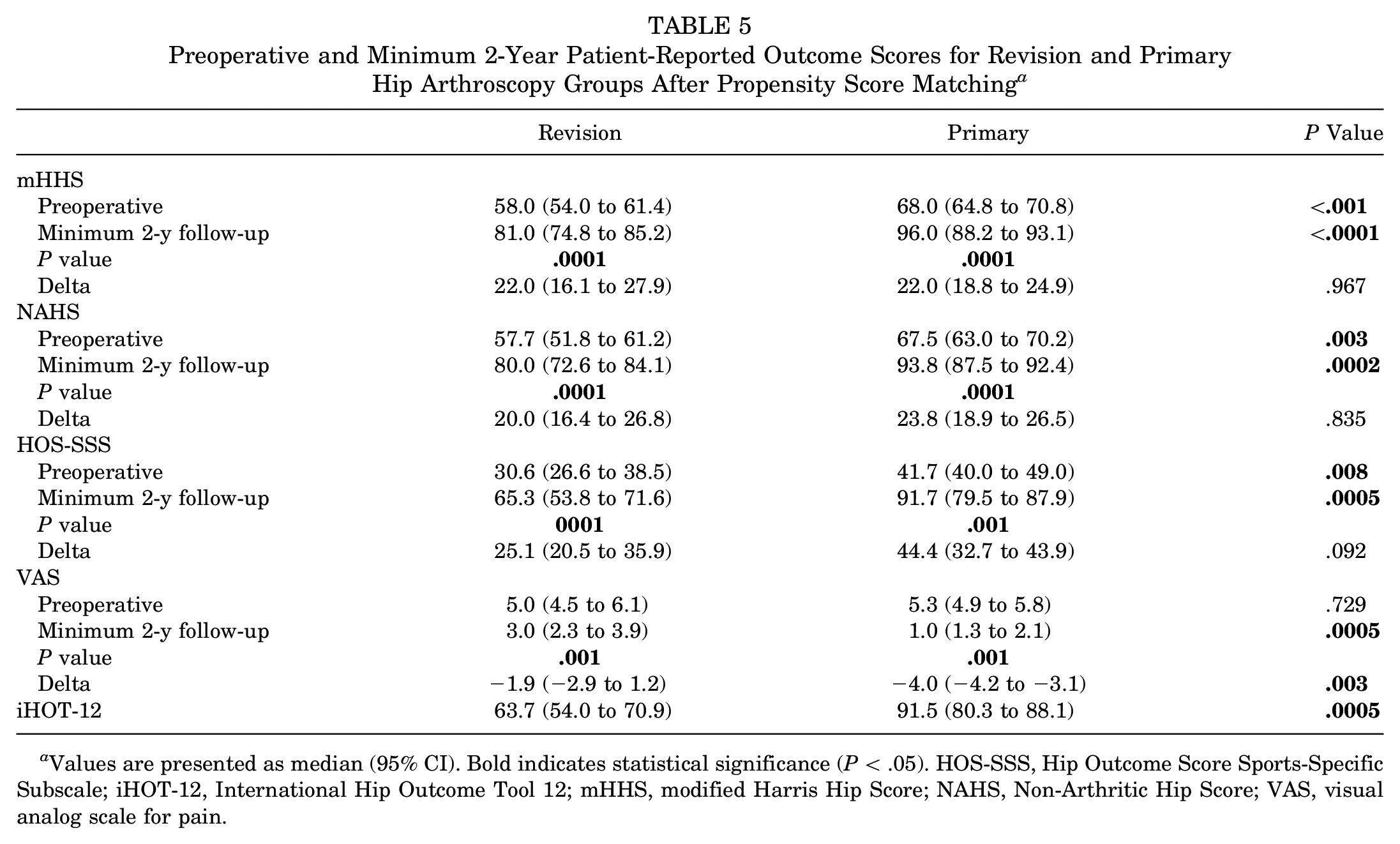
Values are presented as median (95% CI). Bold indicates statistical significance (P < .05). HOS-SSS, Hip Outcome Score Sports-Specific Subscale; iHOT-12, International Hip Outcome Tool 12; mHHS, modified Harris Hip Score; NAHS, Non-Arthritic Hip Score; VAS, visual analog scale for pain.
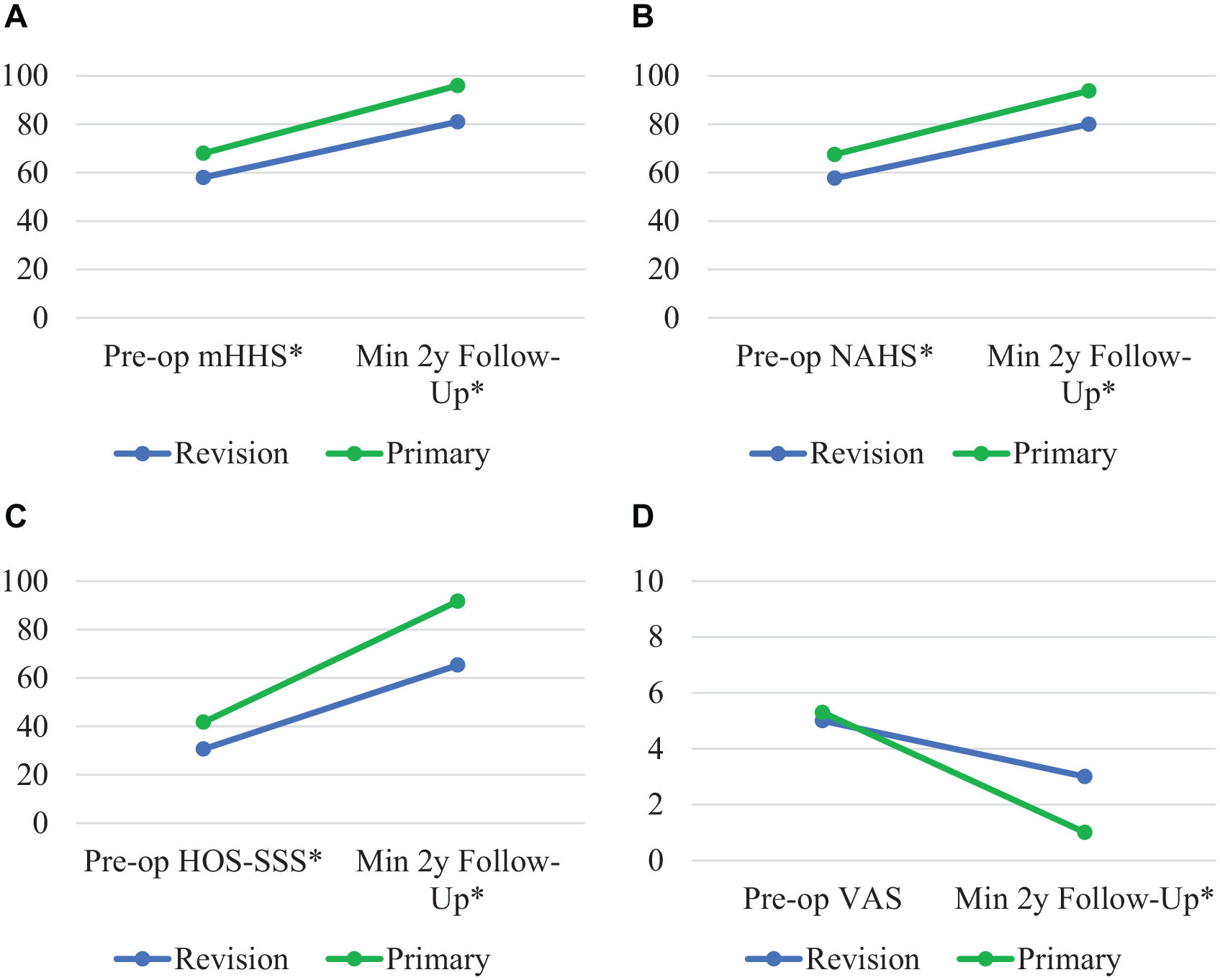
Outcome scores for the preoperative and minimum 2-year follow-up time intervals in the revision status group (blue) and primary status group (green) for (A) mHHS, (B) NAHS, (C) HOS-SSS, and (D) VAS. *Significant differences between groups (P < .05). HOS-SSS, Hip Outcome Score Sports-Specific Subscale; mHHS, modified Harris Hip Score; NAHS, Non-Arthritic Hip Score; VAS, visual analog scale.
In terms of clinical outcomes, revision patients experienced improvement that met or exceeded PASS and MCID for the mHHS at high rates (80.6% and 83.9%, respectively). For the HOS-SSS outcome measure, 24 (92.3%) met or exceeded the MCID and 11 (39.3%) achieved the PASS threshold. MCID and PASS outcomes are summarized in Figure 4.
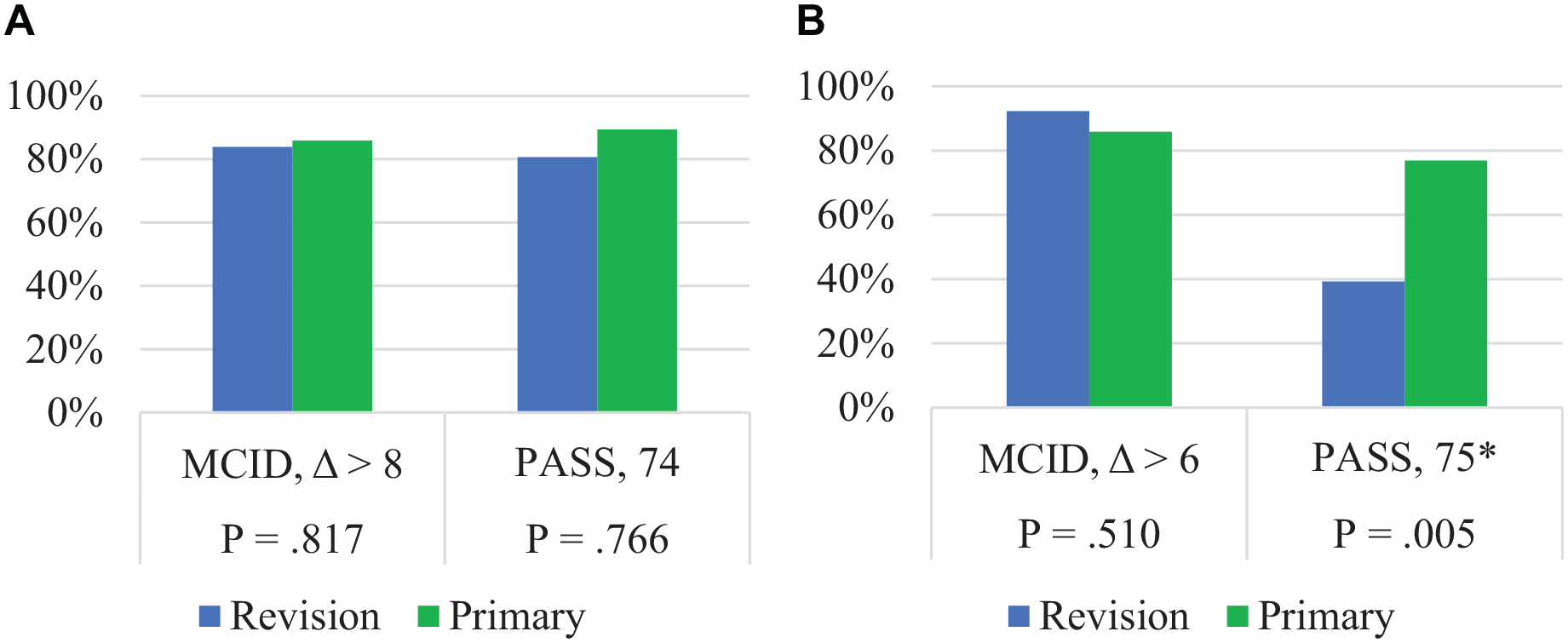
Minimal clinically important difference (MCID) and patient acceptable symptomatic state (PASS) based on revision status for (A) modified Harris Hip Score and (B) Hip Outcome Score Sports-Specific Subscale. *Statistical significance (P < .05).
RTS Outcomes
A comparison of RTS outcomes is presented in Table 6. A statistically significant difference was seen in the number of patients who attempted to RTS in the revision and primary hip arthroscopy groups (62.5% vs 87.0%; P < .01). A total of 9 patients in the revision hip arthroscopy group successfully returned to their sport, whereas 11 were unable to return because of hip pain. Patients who accounted for the remaining 12 (37.5%) cases did not attempt to return to their sport for reasons unrelated to hip pain (ie, loss of interest, lifestyle transition, aging, graduation).
Comparison of Athletes Who Attempted to Return to Sport After Revision and Primary Hip Arthroscopy a
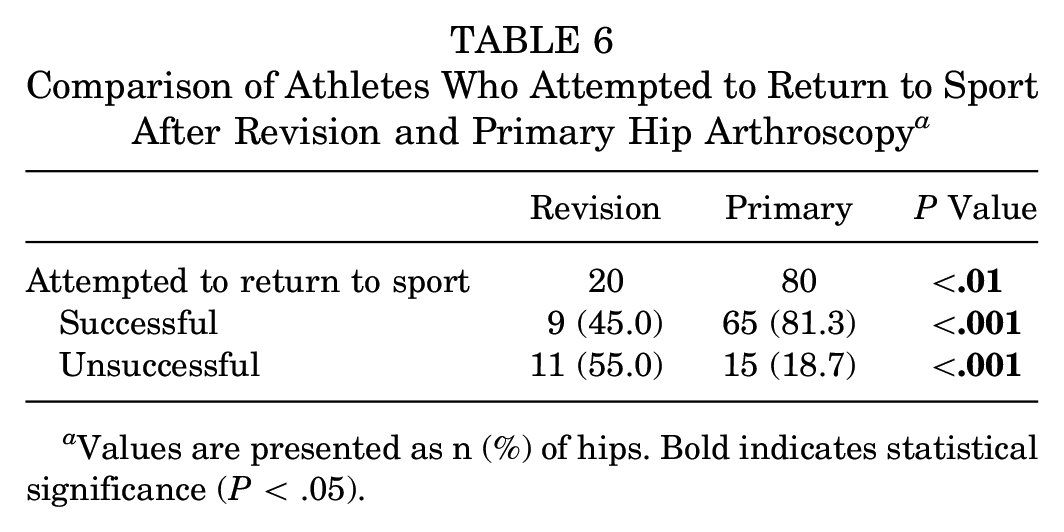
Values are presented as n (%) of hips. Bold indicates statistical significance (P < .05).
Propensity-Matched Outcomes Comparison
Like the revision group, the primary group also demonstrated significant improvement from preoperative to latest follow-up PRO measurements (P < .001) and did so at similar rates as the revision group. The pre- and postoperative scores showed significant differences in favor of the primary group (P < .001) except for the preoperative VAS. The delta value was similar for the groups except for HOS-SSS. Patients in both groups achieved PASS and MCID at similar rates for the mHHS. Patients also achieved MCID for HOS-SSS at similar rates but showed significant differences in their ability to achieve PASS for this PRO (P < .001). A statistically significant difference was seen in the number of patients who attempted to RTS in the revision group (62.5%) compared with the primary group (87.0%) (P < .01). The reasons for not returning to sport (hip pain vs unrelated to hip pain) were similar between groups (P = .586).
Discussion
The primary finding in this study was that high-level athletes undergoing revision hip arthroscopy experienced significant improvement in all PRO measures. Although the postoperative outcome scores in revision patients were lower than those in a control cohort of athletes undergoing primary hip arthroscopy, the magnitude of improvement in outcome scores was similar between groups. The study group achieved MCID/PASS for mHHS and MCID for HOS-SSS at high rates. Conversely, athletes undergoing revision surgery achieved PASS for HOS-SSS and attempted to RTS at significantly lower rates compared with primary hip arthroscopy high-level athletes.
Results of revision hip arthroscopic surgery have mainly been limited to nonathletic populations thus far in the literature. Mygind-Klavsen et al 48 reported on 331 patients undergoing revision hip arthroscopic surgery from the Danish Hip Arthroscopy Registry and compared them with data from 4154 primary hip arthroscopy patients. At 1-year follow-up the investigators found significant improvements in all PROs measured in the revision surgery group, but the primary arthroscopy cohort demonstrated significantly higher postoperative outcomes. Main reasons for revision arthroscopy were scar tissue, residual femoroacetabular impingement, and insufficient healing of labral repair, which were similar to the current study in which labral retear and residual cam impingement were the most common indications for revision surgery. Similarly, Newman et al 49 evaluated 42 adolescent patients undergoing revision surgery compared with a matched cohort of 84 patients undergoing primary arthroscopy and found that revision patients showed significant improvement in all recorded outcome scores. Magnitude of improvement in the study group was similar to that in the control group for HOS-ADL (activities of daily living) and HOS-SSS, but less improvement was observed for the mHHS (27 vs 19). Additionally, postoperative outcome scores were lower in the revision group for mHHS (79.5 vs 72), HOS-SSS (91.2 vs 73.4), and HOS-ADL (91.2 vs 73.4). This trend was echoed in the current study, which demonstrated significant improvements in all outcome scores by the athletes undergoing revision surgery even though preoperative and postoperative scores were lower overall when compared with the control group.
Further, the present study found that athletes undergoing revision surgery achieved PASS for HOS-SSS at significantly lower rates than the control group (P = .005). Although magnitudes of improvement for HOS-SSS were similar between the 2 groups, preoperative scores were significantly lower in the revision hip arthroscopy group compared with the control group, making it more difficult to reach the PASS threshold. Further, athletes undergoing revision hip arthroscopy were more likely to undergo labral reconstruction compared with the control group. Primary labral reconstruction has shown favorable outcomes in athletes, but outcomes of labral reconstruction in the revision setting have not been well established and warrant further study.6,38,61
Outcomes after primary hip arthroscopic surgery in athletes have generally shown excellent results with high RTS rates.4,9,16,63 The present study noted a novel finding that a plurality of high-level athletes undergoing revision surgery (12/32; 37.5%) elected not to attempt to RTS for reasons other than hip pain (eg, loss of interest, desire to prevent further injury to hip, graduation, aging). Although outcomes of athletes who RTS are heavily studied, much less is known about athletes who fail to RTS or choose to retire from competitive sports. 67 Weber et al, 67 in a systematic review and meta-analysis, sought to determine the rate of nonreturning athletes who undergo hip arthroscopy and to explore the reasons for their inability to RTS. The investigators found that in the primary setting, the proportion of athletes who did not RTS because of hip-related issues was significantly greater than the percentage of athletes who did not return for reasons unrelated to their hip (74.3% vs 22.3%; P < .0001). Those investigators also noted that only 4 of their 20 included studies commented on rates of revision surgery in nonreturning athletes, and they highlighted the need for further study on patients who do not RTS or who have revision surgery. Important differences outlined in the current study were that labral reconstruction was performed more commonly in the revision hip arthroscopy cohort compared with the control group (28.1% vs 2.2%, respectively) and that acetabuloplasty (46.9% vs 82.6%) and femoroplasty (75.0% vs 98.9%) were performed significantly less commonly in the revision group. These findings suggest that residual cam impingement and labral retear were common indications for revision surgery and that revision hip arthroscopy often presents higher levels of complexity compared with the primary setting as evidenced by the significantly higher rates of labral reconstruction. As a result, surgeons should be prepared for the unique challenges presented by the high-level athlete undergoing revision surgery, and these patients should be appropriately counseled preoperatively.
The current study presents findings consistent with those in the established literature but in an understudied population of athletes undergoing revision hip arthroscopy. This study has several noteworthy strengths. This is one of the few studies to report PRO scores for high-level athletes undergoing hip arthroscopy with minimum 2-year follow-up. Further, a propensity-matched method was selected to isolate potential confounding effects of sex, age, BMI, and sport competition level. The use of several PRO measurements designed for active patients with nonarthritic hips limits a potential ceiling effect. 66 The current study evaluated a narrow patient population in the hip preservation field, but an adequate sample size based on a priori power analysis was achieved for the study and control groups. Additionally, to assess clinical significance, the fraction of patients who achieved the MCID for the mHHS and HOS-SSS was calculated.
Limitations
The present study had several limitations that must be discussed. This study was nonrandomized. Despite data collection occurring prospectively, this study was also retrospective, which introduces bias. The analysis was based on a single high-volume surgeon who specializes in hip preservation surgery, which may limit the generalizability of the results. The current investigation included a minimum 2-year follow-up, but longer follow-up is needed to determine the durability of the results. Although an a priori power analysis was performed to ensure adequate power, the current study’s sample size may have limited power to detect further differences between the revision and primary hip arthroscopy groups. Hip arthroscopic surgery is becoming more prevalent, but the number of high-level athletes undergoing revision surgery remains relatively limited compared with other patient groups. Last, all athletes were treated as equal in this analysis even though significant heterogeneity exists in the cohort in regard to level (high school vs professional) and sport type (flexibility vs contact).
Conclusion
Revision hip arthroscopy is a viable treatment option to improve PROs in high-level athletes at minimum 2-year follow-up. The study group showed significant improvement in functional scores and a high rate of successful outcomes. Patients in the study group experienced similar magnitude of improvement as that of a propensity-matched control group; however, they achieved lower postoperative PROs and attempted to return to sport at lower rates.
Footnotes
Submitted February 22, 2021; accepted June 1, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.G.D. has had ownership interests in Hinsdale Orthopaedics, the American Hip Institute, SCD#3, North Shore Surgical Suites, and Munster Specialty Surgery Center; has received research support from Arthrex, ATI, the Kauffman Foundation, Stryker, and Pacira Pharmaceuticals; consulting fees from Adventist Hinsdale Hospital, Arthrex, MAKO Surgical, Medacta, Pacira Pharmaceuticals, and Stryker; education support from Arthrex, Breg, and Medwest; speaking fees from Arthrex and Pacira Pharmaceuticals; hospitality payments from Arthrex, Medacta, and Stryker; honoraria from Medacta; and royalties from Amplitude, Arthrex, DJO Global, MAKO Surgical, Medacta, Stryker, and Orthomerica. B.G.D. is the medical director of hip preservation at St Alexius Medical Center and a board member for the American Hip Institute Research Foundation, AANA Learning Center Committee, the Journal of Hip Preservation Surgery, and the Journal of Arthroscopy. The American Hip Institute Research Foundation funded the research and is where our study was performed. A.C.L. has received education support from Arthrex, Medwest, and Smith & Nephew; research support from Arthrex, Stryker, and Medacta; hospitality payments from Smith & Nephew, Stryker, Zimmer Biomet, and Arthrex; and consulting fees from Arthrex and Graymont Medical. B.R.S. has received grants from Arthrex and speaker fees from DJO Global. D.R.M. has received hospitality payments from Arthrex, Stryker, and Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.