
Abstract
Background:
In shoulders with irreparable massive rotator cuff tears (RCTs) with high-grade fatty degeneration (Goutallier stage 3 or 4) of the supraspinatus tendon and low-grade fatty degeneration (Goutallier stage 1 or 2) of the infraspinatus tendon (ISP), arthroscopic patch grafting (PG) has been reported as superior to partial repair (PR) regarding the ISP retear rate at short-term to midterm follow-up. However, the longer term outcomes are unclear.
Purpose:
To compare clinical and structural outcomes in the PG and PR groups at a minimum of 7 years postoperatively.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
We evaluated 24 patients in the PG group and 24 patients in the PR group. We primarily used the Constant score for clinical outcomes and performed magnetic resonance imaging for structural outcomes in the PG and PR groups. The risk factors for a retear of the ISP were identified by univariate and multivariate (forward stepwise selection method) logistic regression analyses. We primarily compared values at midterm follow-up (<4 years) with values at the final follow-up (minimum 7 years) for each patient.
Results:
The mean midterm and final follow-up times for the PG group were 41.0 and 95.1 months, respectively, compared with 35.7 and 99.3 months, respectively, for the PR group. We found significant differences for the midterm and final follow-up Constant total scores in the PG and PR groups (midterm follow-up: 79.1 vs 69.9, respectively [P = .001]; final follow-up: 76.0 vs 65.3, respectively [P = .006]) and in the Constant strength scores (midterm follow-up: 14.6 vs 8.5, respectively [P < .001]; final follow-up: 13.1 vs 8.3, respectively [P = .001]). Treatment group (PR) was a significant predictor of an ISP retear in the logistic regression analysis (odds ratio, 3.545; P = .043).
Conclusion:
Patients with low-grade massive RCTs treated with PG or PR improved significantly in terms of clinical outcomes at the midterm and final follow-up time points. However, Constant scores were significantly better in the PG group at the final follow-up.
Keywords
Selecting the best operative option for massive irreparable rotator cuff tears (RCTs) from among multiple surgical options remains a difficult challenge for orthopaedic surgeons.3,5,17 Various factors, such as graft material and operative technique, differ in studies, resulting in diverse clinical and structural outcomes.20,31,40,42 Some studies have reported satisfactory or worsened clinical outcomes after conventional partial repair.4,6,8,10,13,16,44,46 Therefore, controversy remains regarding the operative indications for graft surgery and partial repair.
We previously compared an arthroscopic fascia lata autograft patch procedure with partial repair for the treatment of posterosuperior massive RCTs with Goutallier15,20,21 stage 3 or 4 fatty degeneration of the supraspinatus tendon (SSP) and with lower than stage 3 fatty degeneration of the infraspinatus tendon (ISP) (massive RCTs with low-grade fatty degeneration of the ISP, referred to here as “low-grade massive RCTs”) (Figure 1A), paying attention to the severity of fatty degeneration of the ISP. 37 Our previous study showed that the patch graft (PG) group was significantly superior to the partial repair (PR) group in terms of the retear rate of the repaired ISP during the short-term to midterm follow-up periods. However, it was unclear whether the patch was sufficient to maintain an intact repair site and achieve better clinical outcomes for a longer period for the treatment of patients with low-grade massive RCTs. Therefore, we continued to follow patients with low-grade massive RCTs who underwent the patch procedure or partial repair.
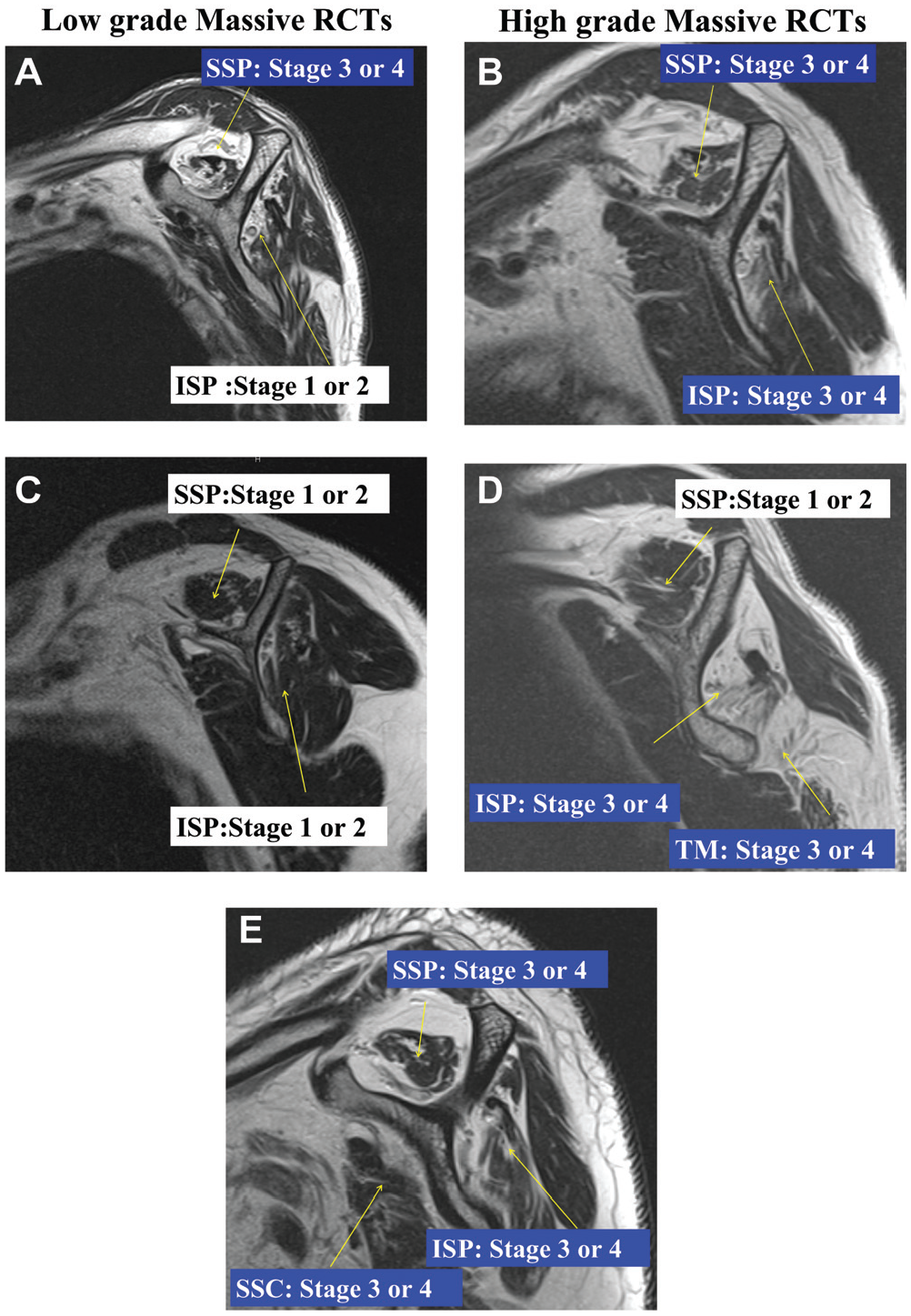
Study (A) inclusion and (B-E) exclusion criteria. Sagittal oblique T2-weighted magnetic resonance imaging. (A) Low-grade massive rotator cuff tears (RCTs): high-grade fatty degeneration (Goutallier stage 3 or 4) of the supraspinatus tendon (SSP) and low-grade fatty degeneration (Goutallier stage 1 or 2) of the infraspinatus tendon (ISP) without severe fatty degeneration of the subscapularis tendon (SSC) and teres minor (TM). (B) High-grade massive RCTs: high-grade fatty degeneration (Goutallier stage 3 or 4) of the SSP and ISP without severe fatty degeneration of the SSC and TM. (C) Goutallier stage 1 or 2 of the SSP and ISP. (D) Goutallier stage 1 or 2 of the SSP and stage 3 or 4 of the ISP with or without severe fatty degeneration of the TM. (E) Goutallier stage 3 or 4 of the SSP, ISP, and SSC.
The current study compared the results of the PG group and PR group for the treatment of low-grade massive RCTs with a minimum 7-year follow-up. In accordance with our previous study with short-term to midterm follow-up periods, we hypothesized that the PG group would be better than the PR group in terms of clinical and structural outcomes at the final follow-up.
Methods
Patient Selection
The study protocol was approved by our institutional review board, and informed consent was obtained from all patients. Data were prospectively collected from our database and retrospectively reviewed. Between June 2007 and March 2011, a total of 277 consecutive patients with RCTs, for which nonoperative treatment had failed, underwent arthroscopic surgery by a single surgeon. Overall, 75 consecutive patients with irreparable large or massive RCTs underwent a fascia lata autograft patch procedure or partial repair (Figure 2). The surgical procedure was chosen based on the preference of the patient after an informed discussion regarding the 2 techniques. 38 An RCT was defined as irreparable when the retracted tendon could not be advanced to cover the original footprint after tendon mobilization, such as with partial or complete capsulotomy and coracohumeral ligament release. Of the 75 patients, 48 patients with Goutallier stage 3 or 4 fatty degeneration of the SSP and stage 1 to 4 fatty degeneration of the ISP underwent the patch procedure. Of the 48 patients who underwent the patch procedure, 28 had Goutallier stage 1 or 2 fatty degeneration of the ISP (low-grade massive RCTs), and 20 had Goutallier stage 3 or 4 fatty degeneration of the SSP and ISP (referred to here as “high-grade massive RCTs”) (Figure 1B). Of the 28 patients with low-grade massive RCTs who underwent the patch procedure, 1 patient did not meet the minimum follow-up duration, and 1 refused postoperative magnetic resonance imaging (MRI). Consequently, we investigated 26 patients with low-grade massive RCTs who underwent the patch procedure, with a mean 41.0-month follow-up (midterm follow-up). 38 After midterm follow-up, we were unable to follow 2 patients because of their refusal to visit our office (see the Appendix A1, available in the online version of this article). In comparison, 26 patients with low-grade massive RCTs, as well as 1 patient with Goutallier stage 4 of the SSP and Goutallier stage 3 of the ISP, were treated with partial repair.
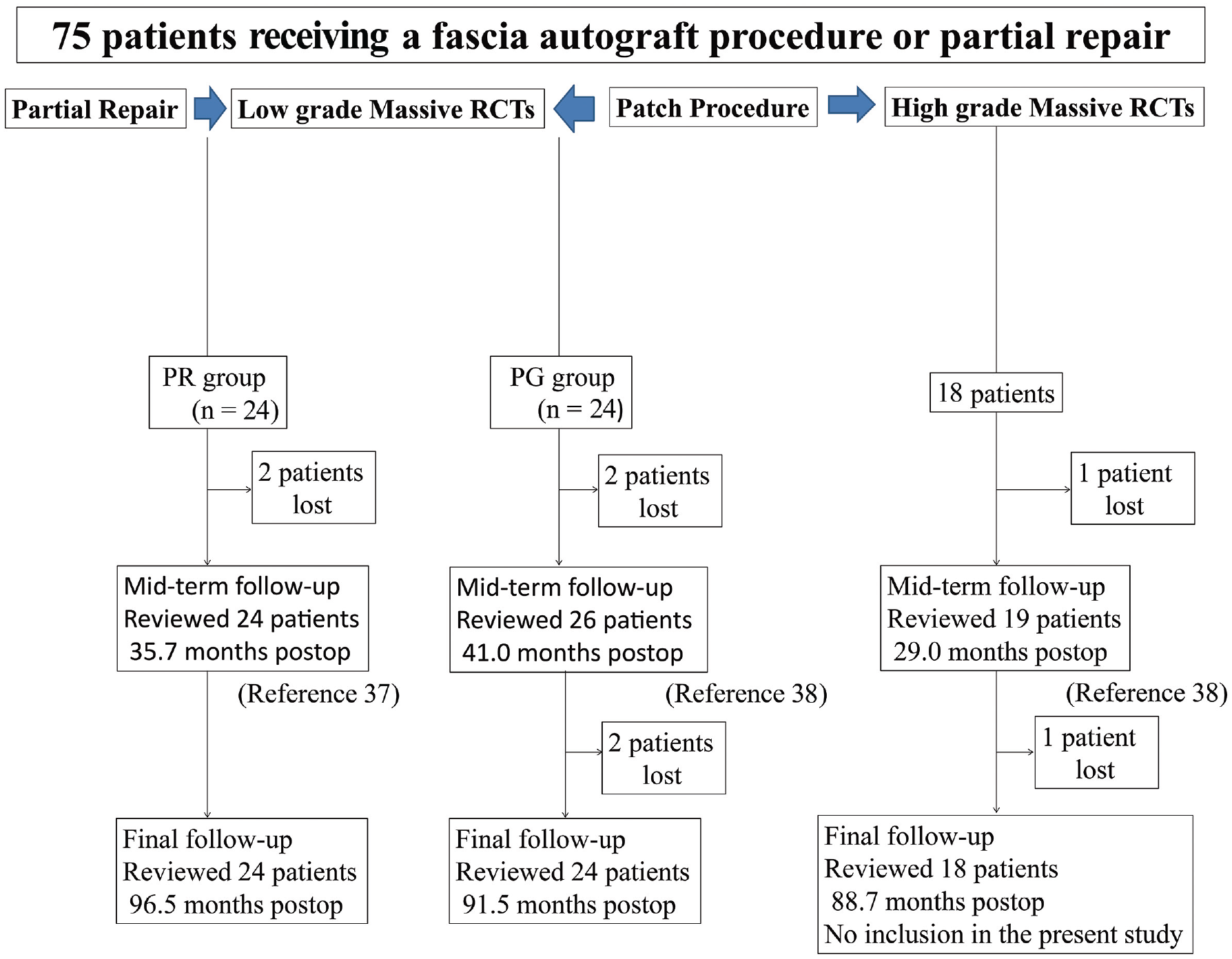
Flowchart demonstrating 75 patients with rotator cuff tears (RCTs) undergoing the patch graft procedure (PG group) and partial repair (PR group). Partial repair was performed in 1 patient with Goutallier stage 4 of the supraspinatus tendon and Goutallier stage 3 of the infraspinatus tendon; the patient was not included in the present study.
Of the 27 patients who underwent partial repair, 1 had preoperative Goutallier stage 3 fatty degeneration of the ISP, 1 who met the inclusion criteria (described below) was lost to follow-up, and 1 refused to undergo postoperative MRI. Consequently, we investigated 24 patients with low-grade massive RCTs who underwent partial repair, with a mean 35.7-month follow-up (midterm follow-up). 37 After midterm follow-up, we were able to follow the 24 patients who underwent partial repair up to the final visit, constituting the same cohort as in a previous study. 38 On the other hand, we investigated 19 patients with high-grade massive RCTs after the patch procedure at a mean 29.0-month follow-up. 38 We then continued to follow 18 of the 19 patients with a mean follow-up of 88.7 months because we lost 1 patient to follow-up. In the present study, however, we did not include patients with high-grade massive RCTs because of the purpose of the study (Appendix A2, available online). Consequently, the remaining 24 shoulders of 24 patients in the PG group and 24 shoulders of 24 patients in the PR group were included in the present study. The follow-up rate was 88.0% (66/75 patients) at a minimum 7-year follow-up.
A large or massive irreparable RCT, which makes complete anatomic repair impossible, was defined as a tear with an anterior-to-posterior or medial-to-lateral dimension of ≥3 cm and fatty degeneration in any rotator cuff muscle as seen on preoperative MRI. 4 We suspected preoperatively that large to massive RCTs in any rotator cuff muscle with high-grade fatty degeneration (Goutallier stage 3 or 4) would be difficult to completely and anatomically repair and considered these as irreparable RCTs. 37 The final evaluation was performed at the time of surgery, and the operative procedure was chosen after an informed discussion regarding the 2 techniques. 37
General inclusion and exclusion criteria have been previously described in detail. 37 Briefly, the inclusion criteria were as follows: (1) irreparable large or massive RCTs with pain and functional disability refractory to nonsurgical treatment, including anti-inflammatory medications, corticosteroid injections, and physical therapy; (2) stage 1 or 2 fatty degeneration of the ISP and stage 3 or 4 fatty degeneration of the SSP, including a positive tangent sign,45,53 according to the classification of Goutallier et al20,21 as assessed on preoperative MRI (Figure 1A); (3) postoperative MRI scans available at the final follow-up (minimum 7 years) to evaluate the integrity of the rotator cuff tendons and/or autografts (MRI scans before surgery and at 12 and 24 months after surgery were available in the previous study); (4) an intact teres minor tendon; and (5) absence of the drop-arm sign. The exclusion criteria were the following: (1) Goutallier stage 1 or 2 fatty degeneration of the SSP on preoperative MRI (Figure 1C); (2) Goutallier stage 3 or 4 fatty degeneration of the subscapularis tendon (SSC) and teres minor (Figure 1, D and E); (3) previous surgery; (4) a history of nerve palsy; (5) arthritic changes in the glenohumeral joint (grade III-V according to the classification of Hamada et al 24 ) and the presence of glenoid erosion (type IA-IIB according to the Seebauer classification 50 ); (6) symptom development after motor vehicle accidents because patients did not receive long-term follow-up (workers’ compensation cases were included in this study); (7) a history of diabetes; (8) rheumatoid arthritis; and (9) full-thickness SSC tears.
The sizes of all tears were assessed with a calibrated probe during surgery (as described later). RCTs were defined as massive if the tear was ≥5 cm in diameter 12 and as large if the tear was ≥3 cm but <5 cm in diameter. There were 8 large and 16 massive tears in the PG group and 4 large and 20 massive tears in the PR group.
Surgical Procedure and Rehabilitation
All surgical procedures (patch procedure or partial repair) were performed by the senior author (D.M.). The operative techniques and rehabilitation protocol have been described in detail.37,38 We performed all procedures using general anesthesia with the patient in the beach-chair position. A posterior portal was established for an initial assessment of the glenohumeral joint. An anterior portal through the rotator interval was established as the working portal for the treatment of intra-articular lesions, such as SSC tears, labral or biceps tears, or subluxation. If the SSC was torn, it was repaired with a suture anchor. No shoulder had full-thickness SSC tears in this study. If the long head of the biceps tendon was partially torn or severely degenerated, biceps tenotomy was performed in patients older than 70 years, and biceps tenodesis was performed in younger patients. If the biceps lesion involved less than one-fourth of the tendon, debridement was performed. The arthroscope was then removed from the glenohumeral joint and redirected into the subacromial space. A posterolateral portal was established as the viewing portal, and an anterolateral portal was established as the working portal for treatment in the subacromial space. The mobility of the residual rotator cuff and tear pattern were evaluated using a tendon grasper. The length (mediolateral dimension) and width (anteroposterior dimension) of the tear were measured with a calibrated probe. All the shoulders in this study had U-shaped tears; none had L-shaped or reverse L-shaped tears. Acromioplasty was only performed to remove spurs, and the coracoacromial ligament was preserved to prevent anterosuperior escape of the humeral head. Osteophytes in the inferior portion of the acromioclavicular joint were removed if necessary; however, we did not perform distal clavicle excision in this series. Subtotal removal of the subacromial bursa and debridement were performed, together with a tendon mobilization procedure, such as partial or complete capsulotomy in conjunction with coracohumeral ligament release. Then, we reassessed tendon mobility with the arm in 30° of abduction. If the SSP could not be advanced to the medial footprint of the greater tuberosity, we then diagnosed the tear as irreparable. The goal was to achieve balanced anatomic repair, including the insertion of the ISP into the middle facet and the posterolateral third of the superior facet of the greater tuberosity, as reported by Mochizuki et al. 36 Therefore, we did not perform margin convergence or posterior interval slide. All procedures were performed with double-loaded suture anchors and external rotation to avoid undue tension on the repaired tendon after surgery.
The rehabilitation protocol was started on the first postoperative day with relaxation of the shoulder girdle muscles. After 2 weeks, the patients were instructed to commence isometric exercises and active-assisted exercises. The shoulders in the PR group were immobilized postoperatively for 6 weeks using an abduction pillow. After 6 weeks, patients started strengthening exercises of the rotator cuff and the scapular stabilizers. The shoulders in the PG group were immobilized postoperatively for 8 weeks. This 2-week difference in the immobilization period was because of the necessity for a longer immobilization period after the more invasive patch procedure. Patients were allowed to return to sports and heavy lifting after 9 months, depending on each individual patient’s functional recovery.
Patch Procedure
After assessing the SSP with an irreparable tear, we utilized a graft as a bridging technique.5,41 After the defect size was measured, a fascia lata autograft was harvested at the site of the greater trochanter. The graft was cut to the shape of the defect but larger. No. 2 permanent anchor sutures were placed through the ISP, and the graft was introduced into the subacromial space through the anterior portal. The graft was attached to the native rotator cuff tendons (SSC, SSP, and ISP) in a mattress fashion. The graft and ISP were attached directly to the greater tuberosity using double-loaded suture anchors (TwinFix, 5.0 or 6.5 mm, with No. 2 UltraBraid [Smith & Nephew] and HEALIX ADVANCE BR Anchor, 4.5 or 5.5 mm, with ORTHOCORD [DePuy Mitek]) (Figure 3).
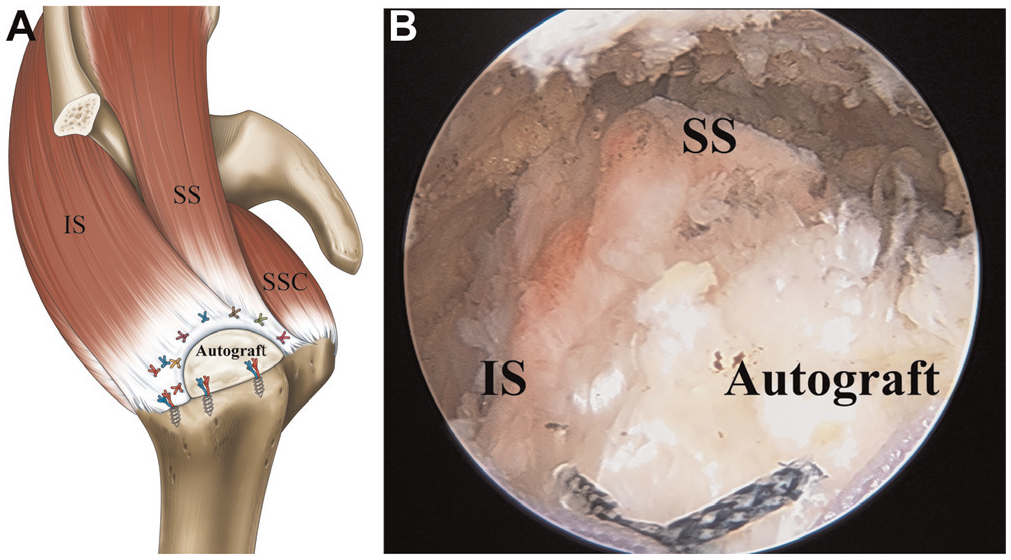
Fascia autograft patch procedure. (A) Illustration. (B) Arthroscopic image of a right shoulder viewed from the posterolateral portal: final view of the repaired rotator cuff tendon (IS) and autograft. There was no residual defect at the tendon insertion footprint. IS, infraspinatus tendon; SSC, subscapularis tendon; SS, supraspinatus tendon.
Partial Repair
After tendon mobilization, the ISP was generally repaired using the single- or double-row technique, depending on tissue quality and mobility, with the same concept of achieving anatomic repair. 37 All the ISP repair procedures were performed using the double-row technique. However, 1 patient with high-grade massive RCTs (exclusion in the present study) underwent single-row repair of the ISP. If anatomic reinsertion of the SSP to the medial footprint of the greater tuberosity was possible, the patients were excluded from the present study as having a repairable tear. In the present study, we had no shoulder with a repairable tear. We repaired the SSP after anterior interval slide and coracohumeral ligament release to minimize tension. After an evaluation of the repair configuration, repair of the SSP was performed by inserting a double-loaded suture anchor (TwinFix, 5.0 or 6.5 mm, with No. 2 UltraBraid) 1 to 1.5 cm medial to the junction between the articular cartilage and the greater tuberosity for all shoulders. Oizumi et al 39 reported satisfactory clinical outcomes for massive RCTs repaired on top of the humeral head by the McLaughlin procedure. Therefore, we performed relatively medialized SSP repair based on the abovementioned study to avoid undue tension on the repaired SSP, although we were aware that the moment arm may be reduced by medial shift of the SSP of ≥17 mm, as reported by Liu et al, 33 or ≥10 mm, as reported by Yamamoto et al. 54 Knot tying for the simple sutures attached to the ISP was performed first, followed by knot tying for the simple sutures attached to the SSP. Repair was completed with knot tying for the medial-row mattress sutures attached to the ISP (Figure 4).
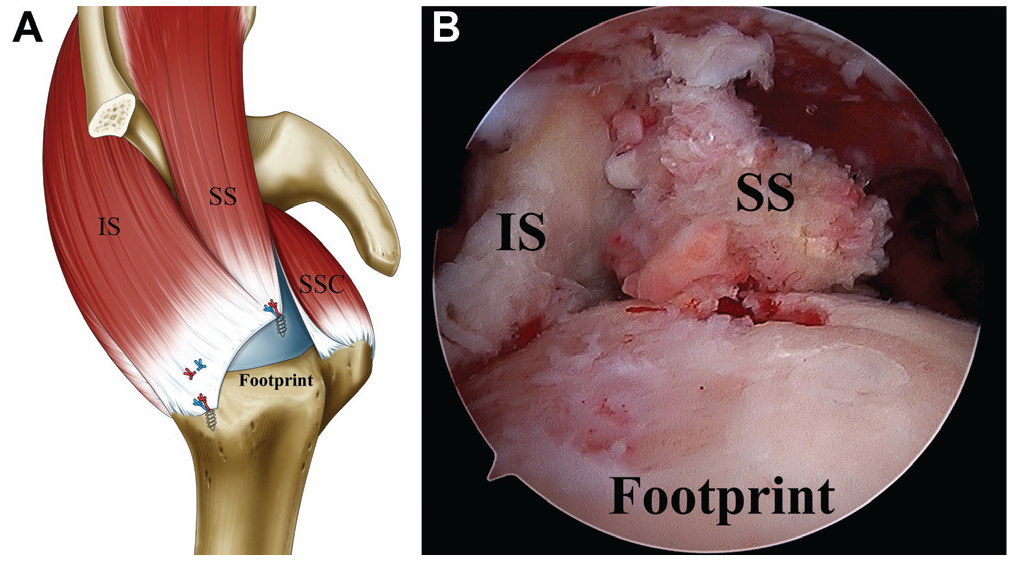
Partial repair. (A) Illustration. (B) Arthroscopic image of a right shoulder viewed from the posterolateral portal: final view of the repaired rotator cuff tendon (IS) and autograft. There was a residual defect at the footprint. IS, infraspinatus tendon; SSC, subscapularis tendon; SS, supraspinatus tendon.
Differences Between Procedures
In the PG and PR groups, we performed direct repair of the ISP without margin convergence or posterior interval slide.6,8 However, we performed medialized repair of the SSP in the PR group and did not reattach the SSP directly to the humeral bone in the PG group as a bridging technique. We investigated how these differences in the procedures affected healing of the repaired rotator cuff tendon (the ISP).
Patient Assessment
Patients were assessed using clinical scoring systems on the day before surgery, at 12 months postoperatively, at midterm follow-up (<4 years), and at the final follow-up (minimum 7 years): namely, the Constant score with a minimal clinically important difference (MCID) of 10.4 points, 29 the American Shoulder and Elbow Surgeons (ASES) shoulder score with an MCID of 11.1 points, 14 and a pain visual analog scale (PVAS) with an MCID of 2.4 points. 48 Range of motion (ROM), such as active forward flexion, external rotation with the arm at the side, and internal rotation at the back, was measured. For ease of statistical analysis of internal rotation, we converted the vertebral level reached to a number: T1-T12 was converted to 1-12, L1-L5 to 13-17, sacrum to 18, and buttock to 19. 27 An Isobex dynamometer (Cursor) was used to quantitatively assess isometric abduction muscle strength with the patient in the seated position. Abduction muscle strength was tested with the arm abducted to 90° in the scapular plane, the elbow extended, and the forearm pronated. The mean of 3 measurements was used for calculating the Constant score. ROM and muscle strength measurements were conducted by the treating surgeon and a clinical assistant (who was not involved in this study and who double-checked the measurements to avoid assessment errors).37,38 At the final follow-up, patient satisfaction with the operatively treated shoulder was assessed on a 10-point Likert scale. Satisfaction was scored from 1 to 10, with 1 indicating “not satisfied at all and very unhappy,” 3 indicating “a little better but not quite satisfied,” 5 indicating “somewhat satisfied,” 7 indicating “quite satisfied,” and 10 indicating “can’t be happier than this and best ever” according to a study by Kim et al. 26
Radiography was used to evaluate the acromiohumeral distance (AHD) and Hamada grade (stage of rotator cuff tear arthropathy). 25 The degree of rotator cuff muscle fatty degeneration was assessed according to the Goutallier stage using the global fatty degeneration index (GFDI).16,22 MRI scans were routinely available before surgery, at 12 and 24 months after surgery, at midterm follow-up, and at the final follow-up.37,38 Full-thickness rotator cuff tendon retears were diagnosed as the presence of a high signal intensity or when discontinuity of the graft, the SSP, the ISP, or the SSC was found on ≥1 of the T2-weighted images. These criteria were based on previous studies using MRI and ultrasonography (Figure 5).15,23,24,37,38,42,43 The diagnosis of a retear was made by 1 treating and 2 nontreating orthopaedic surgeons. In cases in which there was a discrepancy between the assessments, the poorer assessment was used.
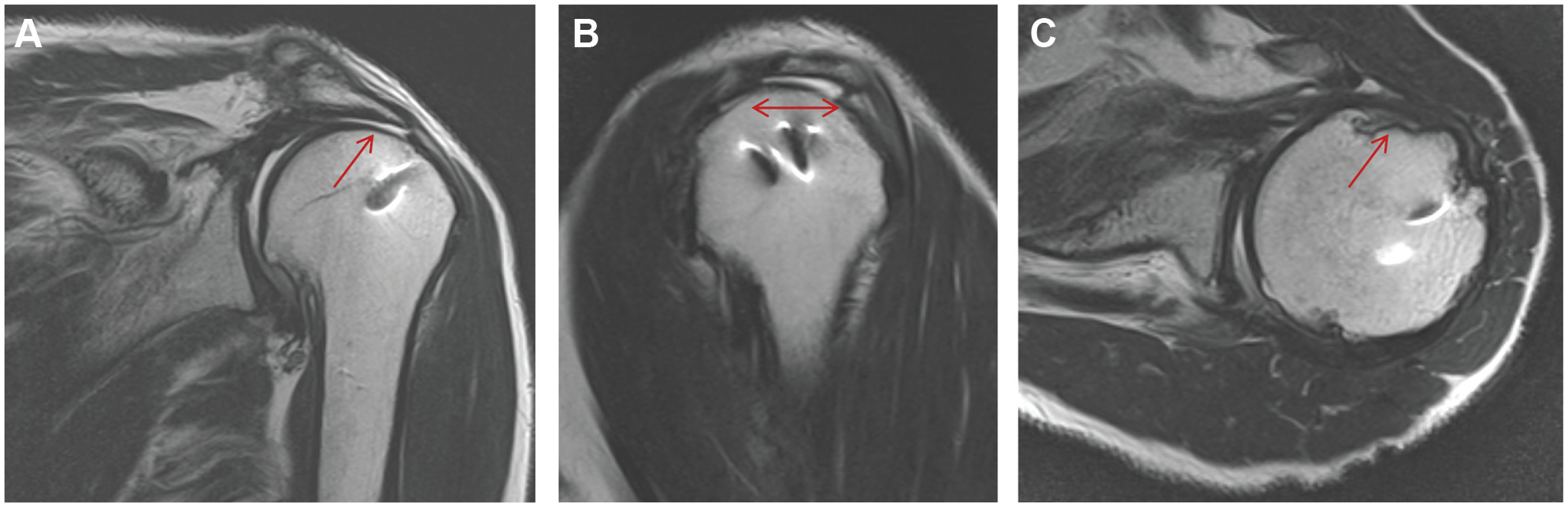
Evaluation of repair integrity for a left shoulder on magnetic resonance imaging after the patch procedure at the final follow-up. (A) Oblique coronal T2-weighted image. (B) Oblique sagittal T2-weighted image. (A, B) A high-signal intensity area, indicating a retear of the repaired infraspinatus tendon (arrow). (C) Axial T2-weighted image showing the presence of a high-signal intensity area, indicating a torn subscapularis tendon (arrow).
Complications Other Than Retears
We investigated intraoperative or perioperative complications, including neural injuries and wound infections, in the 2 groups. In addition, we evaluated residual thigh pain, thigh numbness, and claudication in the PG group.
Statistical Analysis
Baseline patient characteristics for the 2 groups were compared using several tests, namely, the Fisher exact test, Welch t test, and Mann-Whitney U test, with the Bonferroni correction. Changes over time were compared between the 2 groups, between shoulders with and without retears of the ISP, and between shoulders with large tears and those with massive tears in the PG and PR groups using a mixed model. The risk factors for a retear of the ISP were identified by univariate and multivariate (forward stepwise selection method) logistic regression analyses using the generalized linear mixed model. The potential risk factors analyzed were treatment group, sex, age, follow-up time, dominant arm, workers’ compensation status, smoking status, number of large tears, partial SSC tear, mediolateral tear size, anteroposterior tear size, biceps tenotomy, biceps tenodesis, stage 3 versus 4 fatty degeneration of the SSP, and GFDI. Additionally, we used a 2-way random-effects model to calculate the intraobserver reliability of the Goutallier stage and retear diagnosis. P values <.05 were considered significant, and 95% confidence intervals were calculated. All statistical analyses were performed using SAS version 9.2 (SAS Institute).
Results
Preoperative Patient Demographics
Preoperative patient characteristics of the PG and PR groups are shown in Table 1. There were no significant differences between the groups in terms of sex, age, follow-up time, dominant hand, workers’ compensation status, smoking status, existence of a partial SSC tear, mediolateral tear size, anteroposterior tear size, performance of biceps tenotomy, performance of biceps tenodesis, or GFDI (P > .05).
Baseline Patient Characteristics a
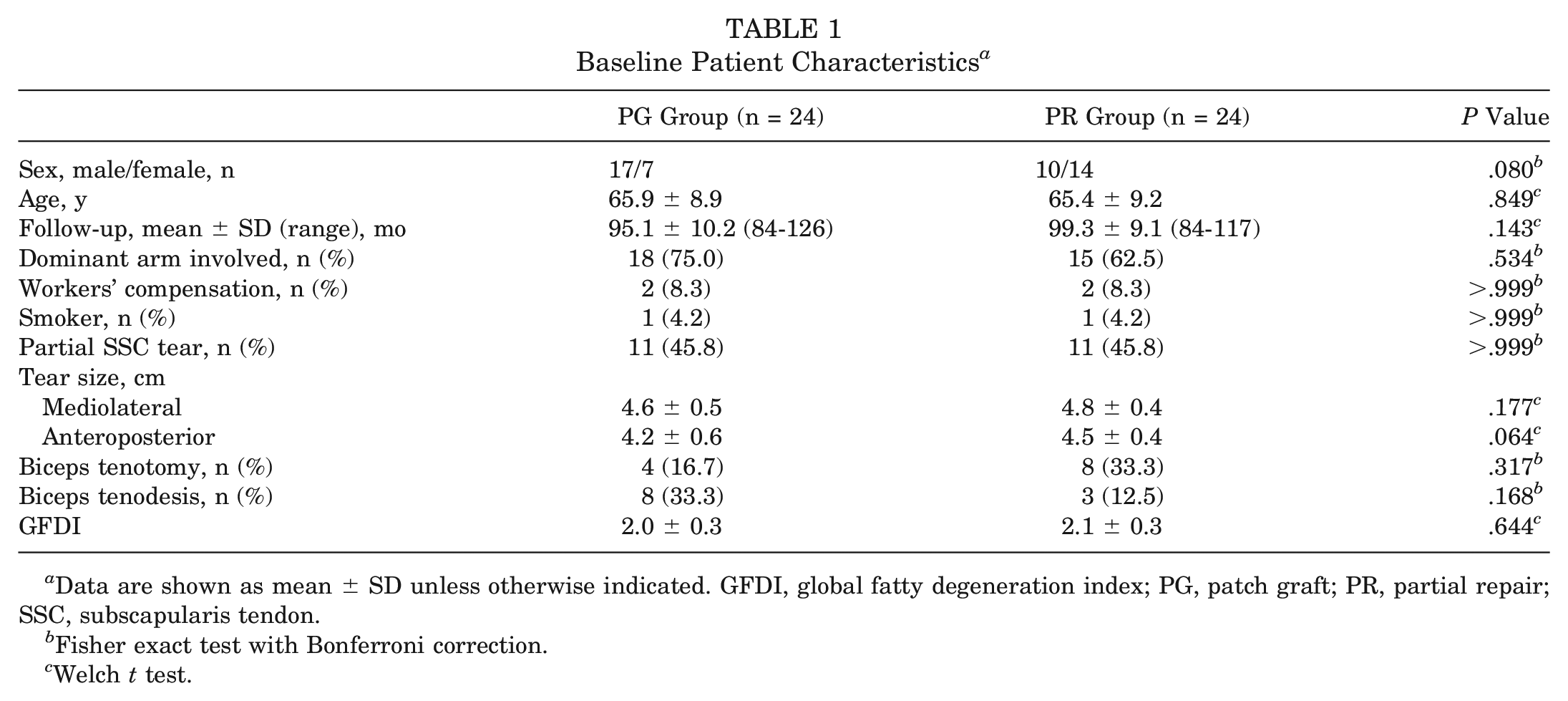
Data are shown as mean ± SD unless otherwise indicated. GFDI, global fatty degeneration index; PG, patch graft; PR, partial repair; SSC, subscapularis tendon.
Fisher exact test with Bonferroni correction.
Welch t test.
Structural Findings
The intraobserver reliability of multiple variables is shown in Appendix A3 (available online). Postoperative MRI at midterm follow-up showed that 5 of 24 (20.8%) shoulders had retears of the repaired ISP in the PG group and that 10 of 24 (41.7%) shoulders had retears of the repaired ISP in the PR group. Postoperative MRI at the final follow-up showed that 6 of 24 (25.0%) shoulders had retears of the repaired ISP in the PG group and that 13 of 24 (54.2%) shoulders had retears of the repaired ISP in the PR group. Of the repaired shoulders with a torn ISP, 3 shoulders (12.5%) in the PG group and 7 shoulders (29.2%) in the PR group had a torn SSC at the final follow-up, although no patients in either of the groups had a torn SSC at midterm follow-up. Only the treatment group variable emerged for inclusion in the final stepwise multivariable model. Therefore, treatment group (PR) was the only significant predictive factor for retears of the ISP (odds ratio, 3.545 [95% CI, 1.042-12.058]; P = .043) (Table 2).
Odds Ratios for Retears of the ISP a
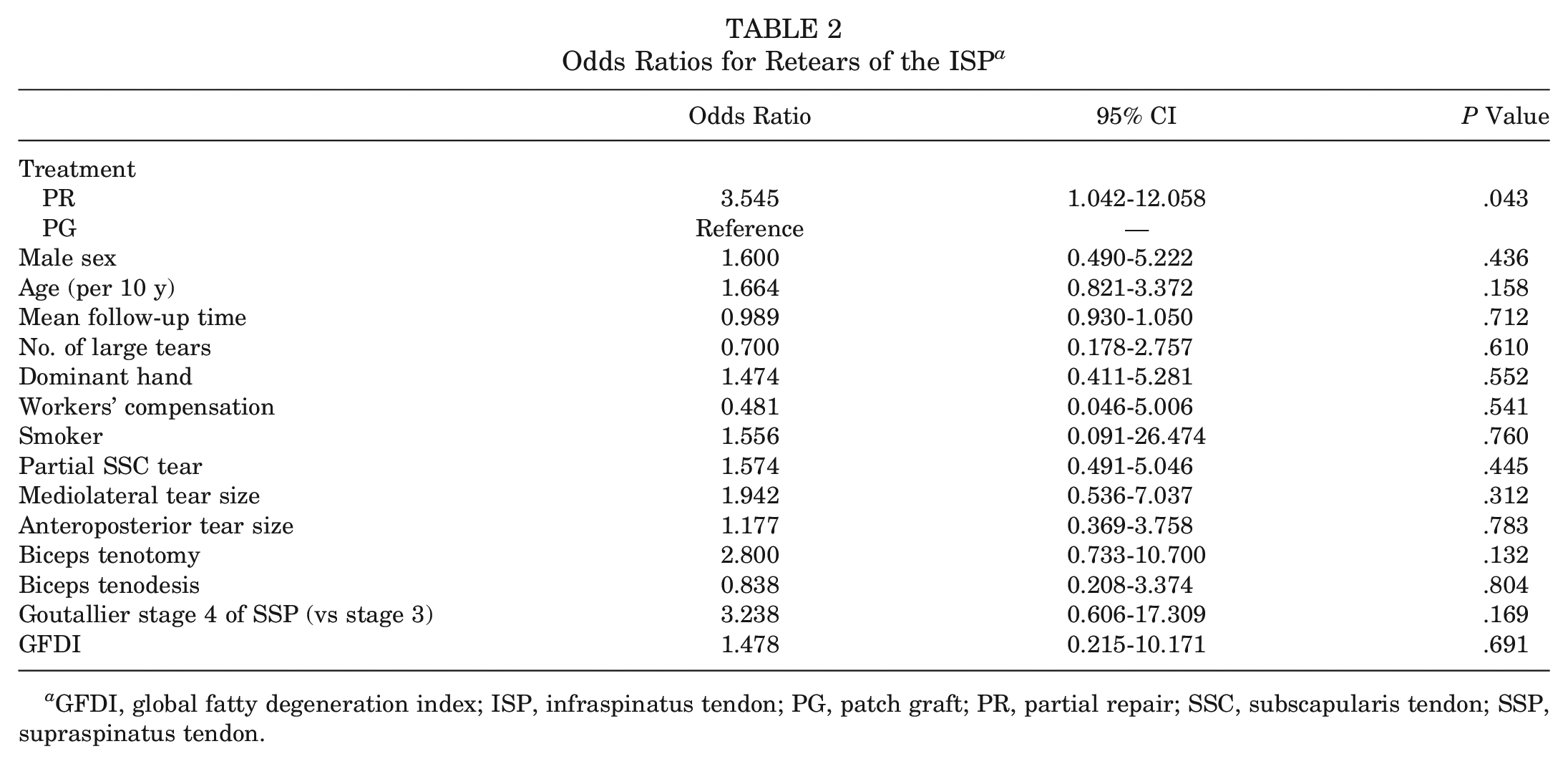
GFDI, global fatty degeneration index; ISP, infraspinatus tendon; PG, patch graft; PR, partial repair; SSC, subscapularis tendon; SSP, supraspinatus tendon.
Comparison of Multiple Outcomes Between the 2 Groups
Detailed multiple outcomes are shown in Table 3 and Figure 6. Compared with preoperatively, scores improved significantly at 12 months postoperatively and at the midterm and final follow-up time points in the 2 groups (P < .001). There were significant differences in the mean Constant total score (79.1 vs 69.9, respectively [P = .001], at midterm follow-up and 76.0 vs 65.3, respectively [P = .006], at the final follow-up) (Figure 5B) and Constant strength score (14.6 vs 8.5, respectively [P < .001], at midterm follow-up and 13.1 vs 8.3, respectively [P = .001], at the final follow-up) (Figure 5D) between the PG and PR groups at the midterm and final follow-up time points. There was a significant difference in mean satisfaction between the PG and PR groups (7.6 vs 6.2, respectively; P = .016).
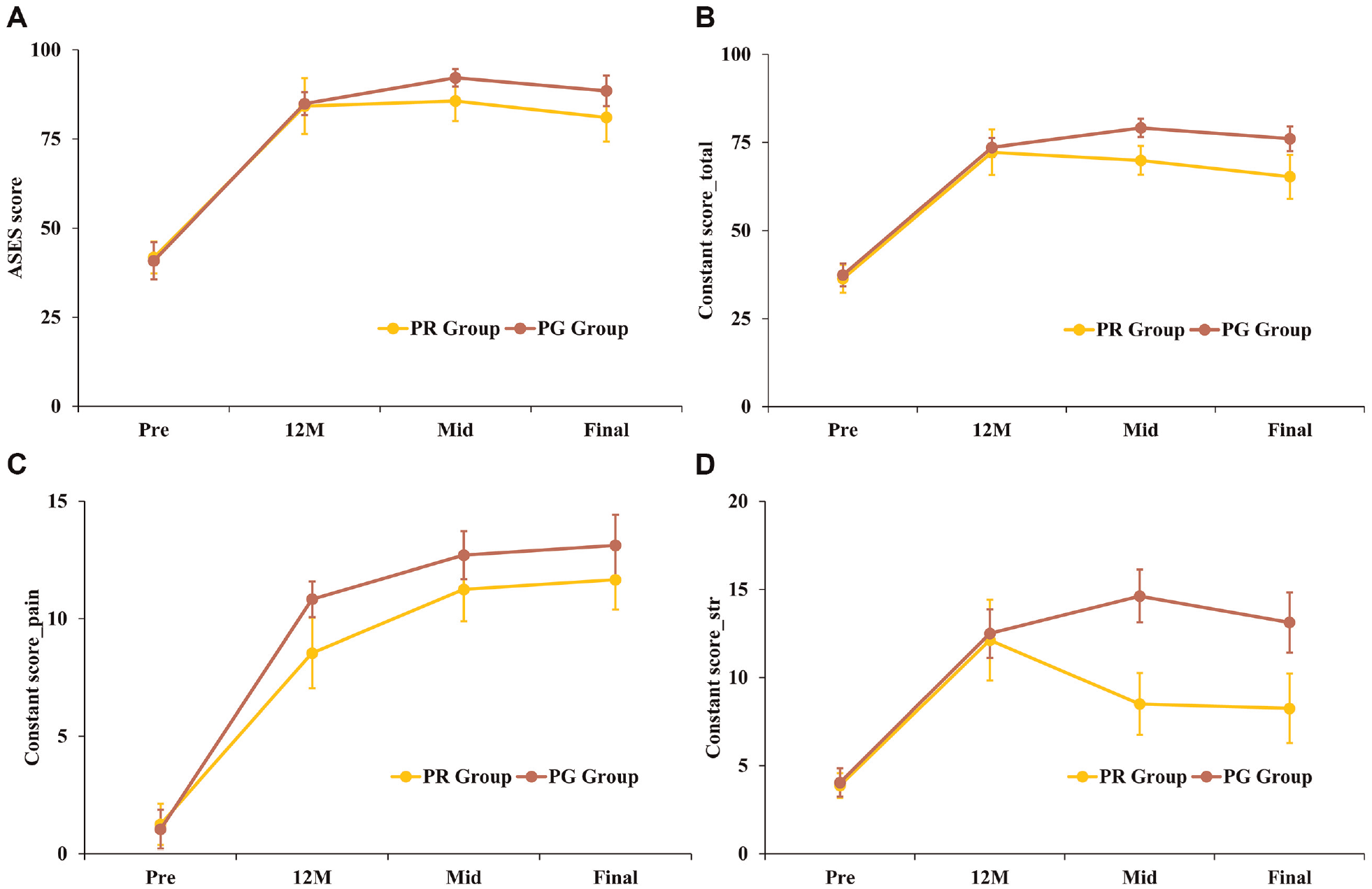
Plots showing multiple scores preoperatively (Pre), at 12 months postoperatively (12M), at midterm follow-up (Mid), and at the final follow-up (Final) for the patch graft (PG) and partial repair (PR) groups. The error bars indicate 95% CIs. (A) Mean American Shoulder and Elbow Surgeons (ASES) score. (B) Constant total score. (C) Constant pain score. (D) Constant strength score.
Pain
At the final follow-up, the mean PVAS score had improved significantly in both groups, and there was no significant difference in the mean PVAS score between the PG and PR groups (0.8 vs 1.4, respectively; P = .143) (Table 3).
Range of Motion
At the midterm and final follow-up time points, active forward flexion, external rotation, and internal rotation had improved significantly in both groups (P < .001). However, there was no significant difference in these parameters between the 2 groups (Table 3).
Comparison of Outcomes Between Groups PG and PR From Preoperative to the Final Follow-up and Between Shoulders With and Without Retears of the ISP at the Final Follow-up a
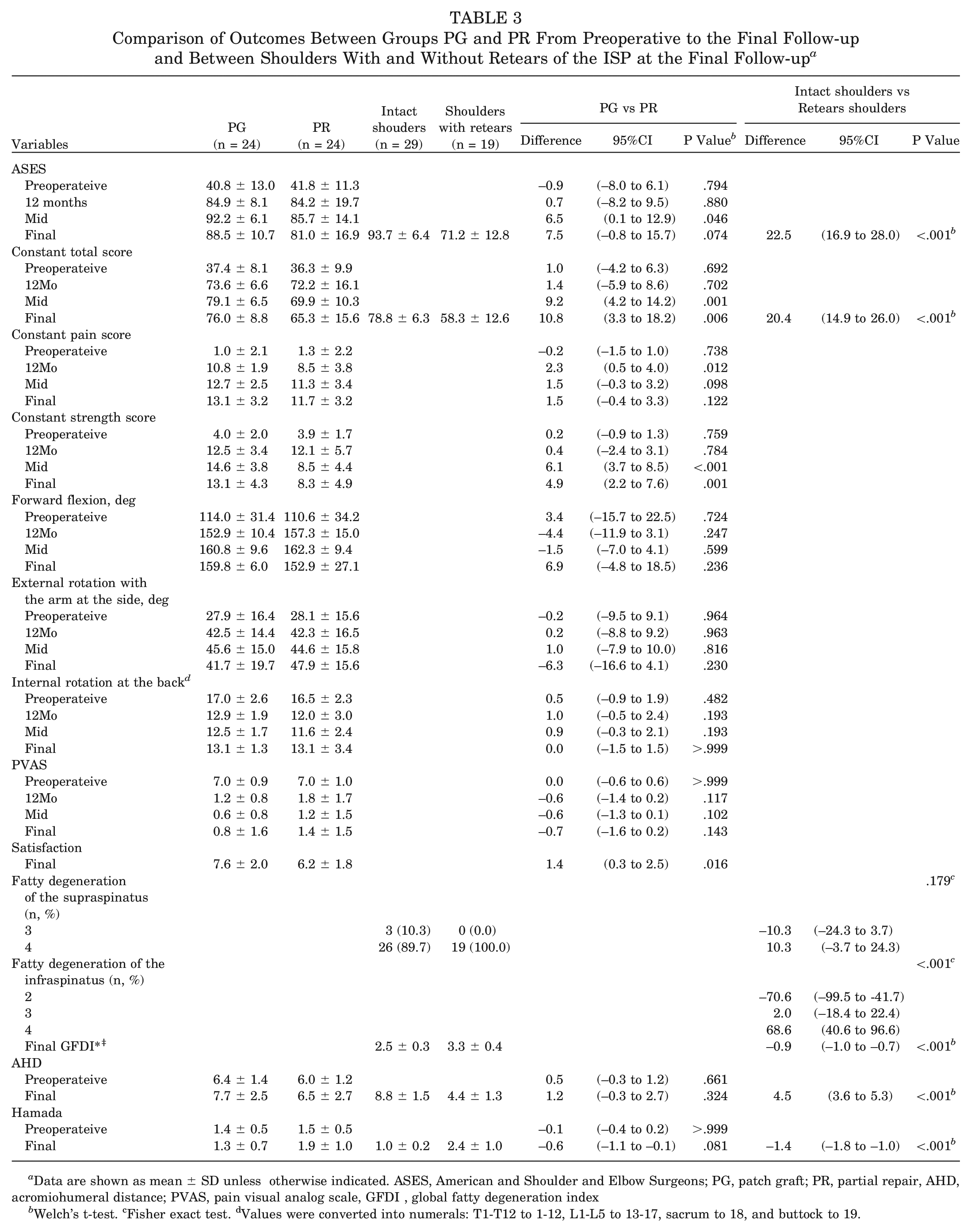
Data are shown as mean ± SD unless otherwise indicated. ASES, American and Shoulder and Elbow Surgeons; PG, patch graft; PR, partial repair, AHD, acromiohumeral distance; PVAS, pain visual analog scale, GFDI , global fatty degeneration index
Welch’s t-test. cFisher exact test. dValues were converted into numerals: T1-T12 to 1-12, L1-L5 to 13-17, sacrum to 18, and buttock to 19.
Comparison of Outcomes Between Shoulders With and Without Retears of the ISP
Multiple detailed outcomes are shown in Table 4 and Appendix A4 (available online). There were significant differences between patients with and without retears of the ISP in terms of the ASES score, Constant score, GFDI, AHD, and Hamada grade at the final follow-up in all shoulders (P < .001). Among the repaired shoulders with an ISP retear and torn SSC, there were no significant differences in the clinical scores or ROM between the 2 groups (Appendix A4).
Comparison of Outcomes Between Shoulders With and Without Retears of the ISP at the Final Follow-up a
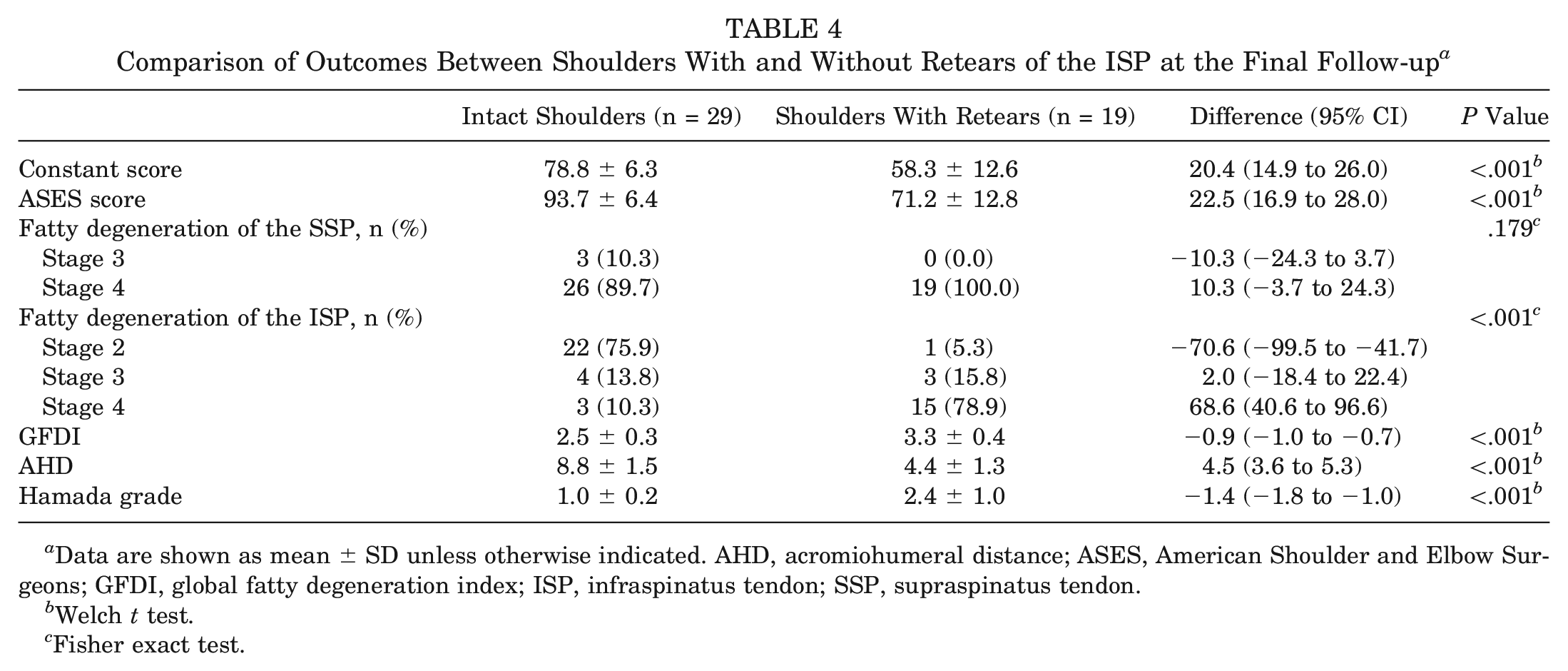
Data are shown as mean ± SD unless otherwise indicated. AHD, acromiohumeral distance; ASES, American Shoulder and Elbow Surgeons; GFDI, global fatty degeneration index; ISP, infraspinatus tendon; SSP, supraspinatus tendon.
Welch t test.
Fisher exact test.
Subgroup Analysis of Shoulders With Large Versus Massive Tears in the PG and PR Groups
We assessed the clinical scores and determined differences in the change from baseline to the final follow-up between shoulders with large versus massive tears in the PG and PR groups. The PG group included 8 shoulders with large tears (large tear subgroup) and 16 shoulders with massive tears (massive tear subgroup), and the PR group included 4 shoulders with large tears (large tear subgroup) and 20 shoulders with massive tears (massive tear subgroup). In the PR group, the large and massive tear subgroups had 2 (50.0%) and 11 (55.0%) shoulders with a retear of the ISP, respectively. In the PG group, the large and massive tear subgroups had 2 (25.0%) and 4 (25.0%) shoulders with a retear of the ISP, respectively. Compared with preoperatively, the mean Constant and ASES scores were significantly improved at the final follow-up in all subgroups. Moreover, there were no significant differences in the change from baseline to the final follow-up for either the large or massive tear subgroup of the PG and PR groups. However, there were significant differences in the massive tear subgroup of the PG and PR groups (P = .044 for ASES score and P = .004 for Constant score) (Table 4).
Complications Other Than Retears
There were no other postoperative complications, such as infections or suture anchor failure, in either group. Additionally, no thigh pain, numbness, or claudication had occurred at the final follow-up in the PG group.
Discussion
We compared outcomes between the PG and PR groups for treating low-grade massive RCTs according to rotator cuff muscle severity (degree of fatty degeneration, and muscle atrophy as a positive tangent sign) with a minimum 7-year follow-up. Although our findings showed significant clinical improvements in the PG and PR groups at the midterm and final follow-up time points for the treatment of low-grade massive RCTs the Constant total and Constant strength scores in the PG group were significantly better than those of the PR group at the midterm and final follow-up time points.
To our knowledge, the mean follow-up time in our study is the longest among comparative studies of the 2 procedures (patch grafting and partial repair) for the treatment of irreparable massive RCTs in a cohort of patients with similar tear severity.31,40 While some studies have compared the clinical and structural outcomes after rotator cuff repair with and without the use of grafts, outcomes differ.2,11,18,25,37,40,51 In a systematic meta-analysis of multiple studies2,11,18,25,37,51 by Ono et al, 40 the authors concluded that the use of grafts generally provides superior tendon healing and clinical outcomes compared with repair. However, inclusion and exclusion criteria in the individual studies differ.2,11,18,25,37,51 Barber et al 2 performed arthroscopic dermal matrix augmentation in patients with repairable large (3-5 cm) RCTs and found intact repair sites in 85% of these patients, as detected by MRI, compared with 40% in the control group at a mean 28-month follow-up. The mean follow-up time in other studies ranged from 14 to 36 months. In the present study, we evaluated whether a graft is useful to keep the repaired tendon intact for a longer period.
This study showed that the Constant total score and the Constant strength score in the PG group were significantly superior to those of the PR group at the final follow-up. In addition, this study showed that the postoperative clinical outcomes (clinical measures and PVAS) and AHD of shoulders with ISP retears were significantly inferior to those without retears. Some previous studies reported that the ISP is the main depressor of the humeral head, and fatty infiltration of the muscle can result in proximal migration of the humerus with subacromial impingement and loss of strength in external rotation and elevation.19,30,34,49,52 Indeed, the present results showed treatment group (PR) as the only significant predictive factor for retears of the ISP (odds ratio, 3.545 [95% CI, 1.042-12.058]; P = .043). In addition, the present study showed that there were significant differences between patients with and without retears of the ISP in terms of the Constant score at the final follow-up in all shoulders (P < .001) (Table 4). The Constant score is heavily influenced by muscle strength in conjunction with rotator cuff healing.2,19,30,37 Together with the findings of previous studies,2,20,31,38 the present study suggests that the fascia autograft patch procedure might prevent retearing of the repaired rotator cuff tendon (the ISP), resulting in the recovery of muscle strength and improved clinical outcomes for a longer time in shoulders with a healed ISP after the treatment of low-grade massive RCTs.
We graded massive RCTs according to the degree of fatty degeneration in the rotator cuff muscles, resulting in clinical and radiographic differences between the PG and PR groups. Theoretically, preoperative tear severity of the ISP and teres minor would affect the clinical outcome after any rotator cuff surgery.30,34,52 Some studies have shown that increased fatty degeneration and rotator cuff atrophy are associated with increased retear rates and poorer functional outcomes.19,34,49 Other studies have shown that tear size is a negative factor for structural outcomes after rotator cuff repair, with larger tears resulting in worse clinical outcomes.28,47 In the present study, there were no significant differences in the clinical outcomes of the large tear subgroup of the PG and PR groups (Table 5). Our stepwise multivariate logistic regression analysis showed that the presence of a large tear was not a significant risk factor for retears of the ISP; however, treatment group was a significant predictive factor for retears. Therefore, the difference in the number of large tears between the 2 groups would not affect the clinical and structural outcomes in either group, considering that there were no significant differences in the mediolateral or anteroposterior tear size (Table 1) in conjunction with the results of the regression analysis and the significant differences in clinical outcomes of shoulders with and without retears of the ISP (Table 4). We previously reported a 10.5% healing rate after performing the patch procedure for shoulders with high-grade massive RCTs (severe fatty degeneration of the SSP and ISP) as well as significantly inferior clinical outcomes compared with those of shoulders with low-grade massive RCTs after the patch procedure. 38 In the present study, we found clinical features (Tables 3 and 4, Appendix A2) in terms of clinical and structural outcomes in shoulders with low- and high-grade massive RCTs after the patch procedure. 38 Considering our results and the results of previous studies,18,32,38 we believe that grading of massive RCTs based on the degree of fatty degeneration of the ISP can be useful for determining the appropriate treatment strategy among multiple treatment options for irreparable massive RCTs. 9
Comparison of Outcomes Between Shoulders With Large Versus Massive Rotator Cuff Tears a
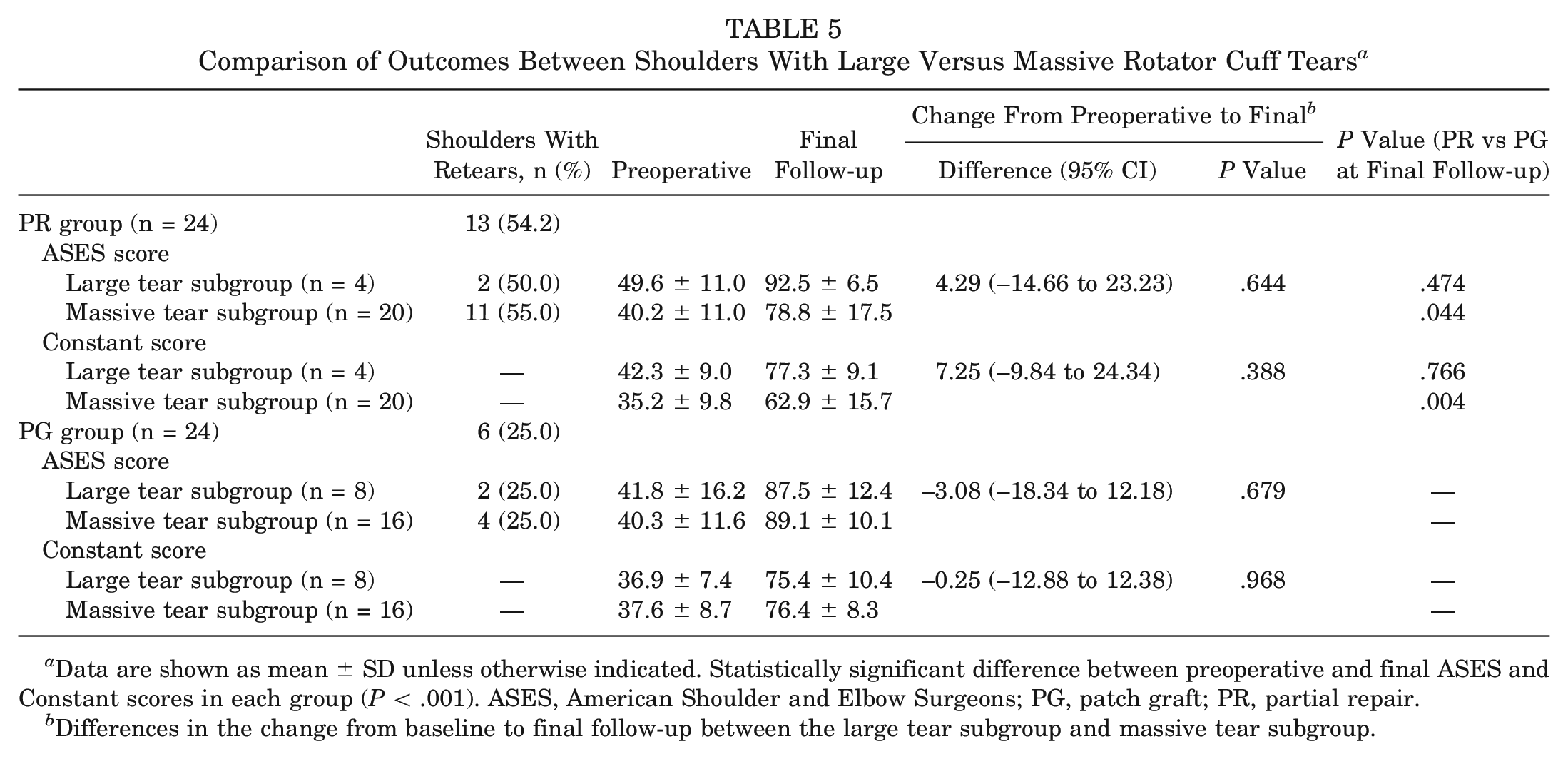
Data are shown as mean ± SD unless otherwise indicated. Statistically significant difference between preoperative and final ASES and Constant scores in each group (P < .001). ASES, American Shoulder and Elbow Surgeons; PG, patch graft; PR, partial repair.
Differences in the change from baseline to final follow-up between the large tear subgroup and massive tear subgroup.
This study has 2 major strengths. First, as previously mentioned, the mean follow-up time in the present study (95.1 months in PG group and 99.3 months in PR group) is the longest reported follow-up among comparative studies of the patch procedure and partial repair. Second, we performed the patch procedure or partial repair for shoulders with a similar level of fatty degeneration (severe fatty degeneration isolated to the supraspinatus) as well as other cuff severity (tear size, GFDI) in such homogeneous condition, resulting in clinical and structural differences between the two groups. Therefore, it is reasonable to consider that our comparisons were appropriate.
Noticeable limitations in the present study should be discussed, although we previously described several limitations in detail.37,38 First, there were inherent patient selection biases because the surgical procedure was chosen according to the patient’s preference after an informed discussion of the 2 techniques.37,38 Second, there were relatively low numbers of patients in the 2 groups. Third, although the postoperative rehabilitation protocol was identical in the PG and PR groups, the immobilization period differed by 2 weeks. This was because of the necessity for longer immobilization after the more invasive patch graft surgery. Fourth, the patch procedure was performed using a fascia autograft. Although several studies have shown the efficacy of fascia autografts, further studies should be performed to compare the procedure’s outcomes with those of other graft materials.31,32,35,40,42 Fifth, this was a retrospective study, not a prospectively randomized study. Sixth, we did not compare our patch procedure to other graft procedures, such as superior capsular reconstruction (SCR), for the treatment of irreparable RCTs. Mihata et al 35 and Burkhart and Hartzler 7 obtained better results for massive RCTs with severe fatty degeneration of the ISP after SCR. 32 On the other hand, Azevedo et al 1 reported that moderate to severe fatty degeneration of the ISP was correlated with the presence of a complete graft tear at 3 years after SCR. SCR might be a better option for shoulders with fatty degeneration of the ISP, but it was not investigated in this study so no statement can be made on this point.
Conclusion
Our findings showed significant clinical improvements in the PG and PR groups at the midterm and final follow-up time points for the treatment of low-grade massive RCTs. However, the Constant total and Constant strength scores in the PG group were significantly better than those of the PR group at the midterm and final follow-up time points.
Supplemental Material
sj-pdf-1-ajs-10.1177_03635465211043501 – Supplemental material for Irreparable Large to Massive Rotator Cuff Tears With Low-Grade Fatty Degeneration of the Infraspinatus Tendon: Minimum 7-Year Follow-up of Fascia Autograft Patch Procedure and Partial Repair
Supplemental material, sj-pdf-1-ajs-10.1177_03635465211043501 for Irreparable Large to Massive Rotator Cuff Tears With Low-Grade Fatty Degeneration of the Infraspinatus Tendon: Minimum 7-Year Follow-up of Fascia Autograft Patch Procedure and Partial Repair by Daisuke Mori, Kazuha Kizaki, Noboru Funakoshi, Fumiharu Yamashita, Yasuyuki Mizuno, Takaaki Shirai and Masahiko Kobayashi in The American Journal of Sports Medicine
Footnotes
Acknowledgements
The authors are grateful to Hajime Yamakage, MD, for statistical analyses; Mutsumi Nishida, PhD, for valuable discussions; and Yoshihiko Tsuda for medical illustrations (Davinci Medical Illustration Office).
Submitted December 18, 2020; accepted June 7, 2021.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.