
Abstract
We read with great enthusiasm the article entitled “Ultrasonic Percutaneous Tenotomy for Recalcitrant Lateral Elbow Tendinopathy: Clinical and Sonographic Results at 90 Months” by Ang et al 1 in the May 2021 issue of your journal. The authors have succinctly reported long-term clinical and sonographic results after ultrasonic percutaneous tenotomy (PT) of the brevis and the common extensor tendon in patients with recalcitrant lateral elbow tendinopathy. A total of 19 patients were assessed by authors at 90-month follow-up; no disease recurrence and adverse outcomes were reported. The visual analog scale and Disabilities of the Arm, Shoulder and Hand (DASH)–Compulsory scores reported significant improvement compared with preprocedure scores at 3-month follow-up. The scores at 90 months were compared with scores at 6 and 36 months. The ultrasound assessment at the final follow-up showed the resolution of hypervascularity in 79% of patients, reduced tendon swelling in all patients, and sustained resolution of the hypoechoic lesion. 1
Extensor tenotomy with variations as a treatment for tennis elbow has been reported in the literature with good to excellent outcomes. However, all these studies, including the present one, lack a comparison group. Thus, it is difficult to authenticate the advantage of PT over other available treatment modalities in patients with recalcitrant lateral epicondylitis elbow.2,3
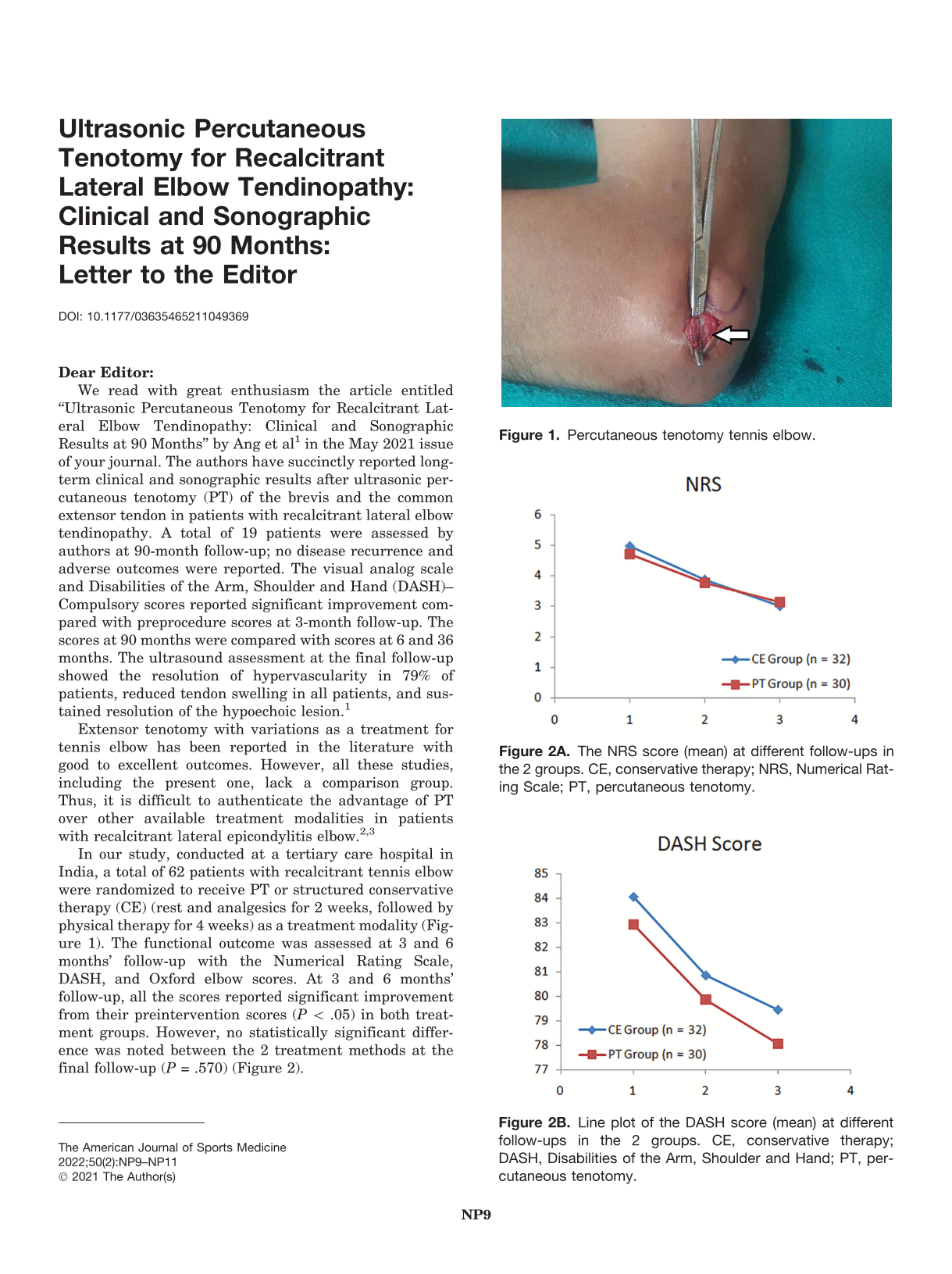
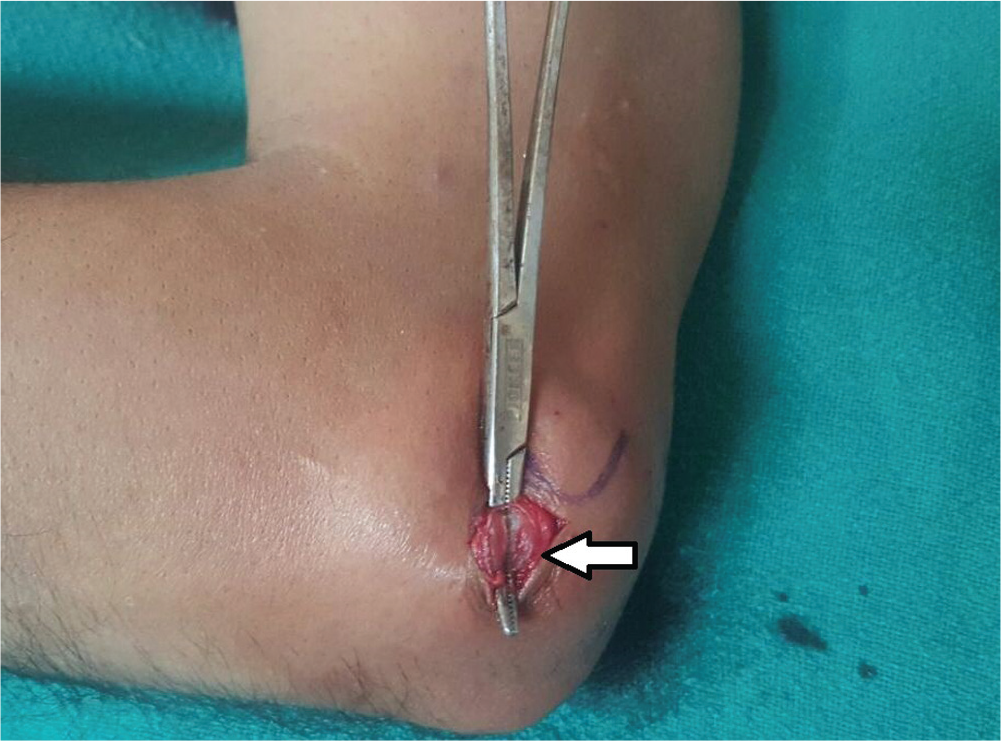
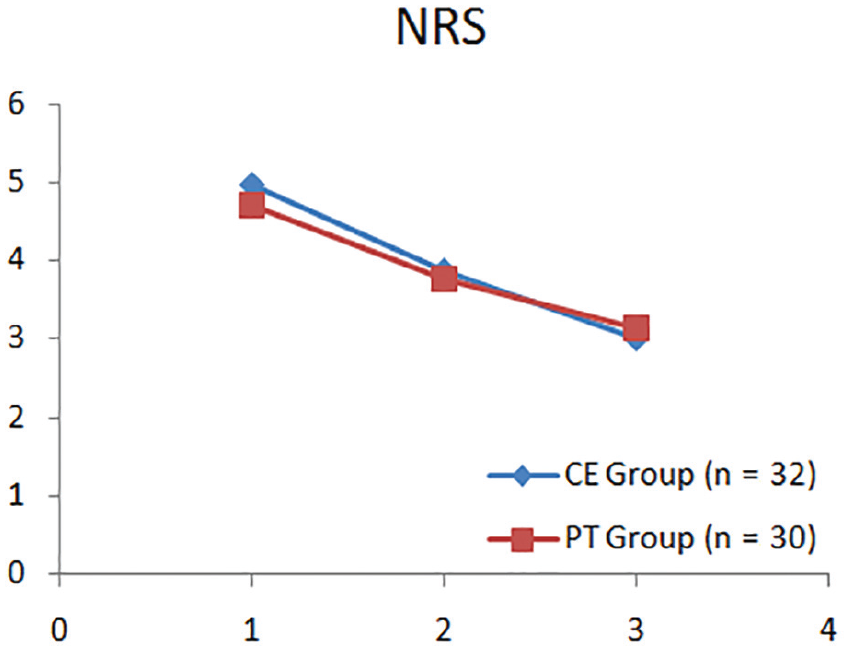
In our study, conducted at a tertiary care hospital in India, a total of 62 patients with recalcitrant tennis elbow were randomized to receive PT or structured conservative therapy (CE) (rest and analgesics for 2 weeks, followed by physical therapy for 4 weeks) as a treatment modality (Figure 1). The functional outcome was assessed at 3 and 6 months’ follow-up with the Numerical Rating Scale, DASH, and Oxford elbow scores. At 3 and 6 months’ follow-up, all the scores reported significant improvement from their preintervention scores (P < .05) in both treatment groups. However, no statistically significant difference was noted between the 2 treatment methods at the final follow-up (P = .570) (Figure 2).
Percutaneous tenotomy tennis elbow.
The NRS score (mean) at different follow-ups in the 2 groups. CE, conservative therapy; NRS, Numerical Rating Scale; PT, percutaneous tenotomy.
Line plot of the DASH score (mean) at different follow-ups in the 2 groups. CE, conservative therapy; DASH, Disabilities of the Arm, Shoulder and Hand; PT, percutaneous tenotomy.
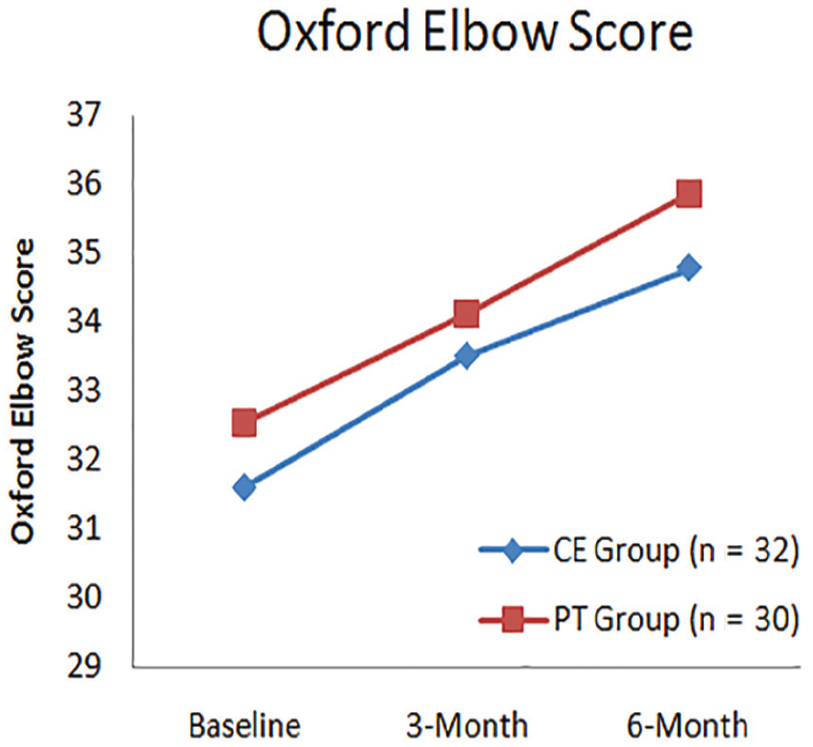
Line diagram of the Oxford score (mean) at different follow-ups in the 2 groups. CE, conservative therapy; PT, percutaneous tenotomy.
Hence, we believe that structured CE is an equally effective treatment modality in the treatment of patients with recalcitrant lateral epicondylitis elbow. This observation could be highly important in treating patients with this disease subgroup in areas where advanced diagnostic and operative facilities are not available.
Footnotes
Submitted June 12, 2021; accepted June 29, 2021.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.