
Abstract
Background:
No study has specifically evaluated how ulnar neuritis and ulnar nerve transposition affect outcomes in baseball players undergoing ulnar collateral ligament (UCL) reconstruction (UCLR).
Purpose:
To evaluate the effects of ulnar neuritis and ulnar nerve transposition in baseball pitchers undergoing UCLR in regard to return to sport, time to return to sport, and need for revision or additional surgery.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
At a single institution, all consecutive baseball pitchers undergoing UCLR between 2002 and 2015 were identified. Ulnar neuritis was diagnosed preoperatively by the following criteria: ulnar nerve symptoms, Tinel sign at the elbow, symptomatic subluxation, and numbness/paresthesia in an ulnar nerve distribution of the hand. The primary outcome of the study was return to sport. The secondary outcomes of the study were time to return to sport, length of playing career, and revision or additional surgery.
Results:
A total of 578 UCLRs were performed in baseball players; of these, 500 UCLRs were performed in pitchers. Ulnar neuritis was diagnosed in 97 (19.4%) baseball pitchers presenting with UCL injury. There were no significant differences in patient characteristics or surgical techniques performed for reconstruction between baseball pitchers with and without ulnar neuritis. In review of injury characteristics, ulnar neuritis was significantly more likely to be diagnosed in pitchers with an acute onset of UCL injury (P = .03). Transposition of the ulnar nerve was more commonly performed in players with ulnar neuritis (47%) versus those without ulnar neuritis (10%; P = .0001). The players who had ulnar neuritis and underwent UCLR had a significantly lower odds of returning to sport (odds ratio, 0.45; P = .04); however, no significant difference was found for time to return to sport and length of playing career for those with and without ulnar neuritis (P = .38 and .51, respectively).
Conclusion:
The study suggests that ulnar neuritis, when present preoperatively in baseball pitchers undergoing UCLR, may adversely affect their ability to return to sport, whereas ulnar nerve transposition at the time of UCLR does not alter the ability to return to sport.
Keywords
The medial side of the elbow can experience up to 64 N·m of varus torque during the act of throwing a baseball.4,7 During this motion, the ulnar collateral ligament (UCL), as well as other medial-sided structures such as the ulnar nerve, can experience heightened tensile stresses.6,11 For this reason, ulnar neuritis is a common pathology in the elbow of overhead throwing athletes.1,8 As an illustration, a previous report suggested that 24% of throwing athletes undergoing UCL reconstruction (UCLR) were noted to have had preoperative ulnar nerve symptoms. 13 Under these circumstances, an overhead throwing athlete who is evaluated for medial-sided elbow pain requires careful scrutiny of symptoms stemming from both UCL insufficiency and ulnar neuritis.
In 1974, Dr Frank Jobe initiated UCLR in throwing athletes. 9 The original description of the UCLR technique detailed anterior transposition of the ulnar nerve; however, a high rate (20%) of ulnar nerve symptoms was noted after reconstruction.9,13 Given this development, variations of the technique have progressed to limited decompression and transposition of the ulnar nerve during UCLR.4,13 In a systematic review, Vitale and Ahmad 14 noted that discontinuing the obligatory ulnar nerve transposition during UCLR was associated with better outcomes and a lower rate of postoperative ulnar neuropathy. Although various derivations have developed from the original description of the technique, the most common complication encountered after UCLR is postoperative ulnar neuropathy.4,14
The baseball pitcher appears to be at high risk for UCL injury. 5 In an epidemiological study, Conte et al 5 found that the prevalence of UCLR in Major League Baseball pitchers was 25% and the prevalence in Minor League Baseball pitchers was 15%. 5 Despite the commonality of surgery among pitchers, studies have shown a high rate of return to sport after UCLR. 10 At the same time, limited studies are available regarding risk factors for return to sport in baseball pitchers undergoing UCLR.3,6 To our knowledge, no study has evaluated how a concurrent presentation of ulnar neuritis at the time of UCL injury in baseball pitchers affects outcomes of surgery for UCLR. The purpose of this study was to evaluate the effects of ulnar neuritis and ulnar nerve transposition in baseball pitchers undergoing UCLR with regard to return to sport, time to return to sport, and need for revision or additional surgery.
Methods
Design
Institutional review board approval was obtained before initiation of the study.
At a single institution, all consecutive baseball pitchers undergoing UCLR between 2002 and 2015 were identified by diagnostic and procedural codes. All clinical notes, diagnostic imaging, and player statistics were manually reviewed in detail. From these sources, player characteristics, injury characteristics, surgical techniques, and outcome measures were collected for further analysis. The data, after manual review, were collected by 2 independent reviewers (A.F.D., R.A.K.).
Patient Selection
All baseball pitchers were diagnosed with UCL injury by means of physical examination and imaging verification by magnetic resonance arthrogram of the elbow interpreted by a musculoskeletal radiologist. Ulnar neuritis was diagnosed preoperatively by the following criteria: ulnar nerve symptoms, Tinel sign at the elbow, symptomatic subluxation, and numbness/paresthesia in an ulnar nerve distribution of the hand. Transposition of the ulnar nerve was not routinely performed for ulnar neuritis. Rather, at the discretion of the treating surgeon, the ulnar nerve was transposed for the following reasons: (1) symptomatic subluxation during a primary surgery or (2) exposure and/or protection during revision surgery. Based on the diagnosis of UCL injury, the following inclusion and exclusion criteria were established. All of the following inclusion criteria had to be met for participation in the study: (1) UCL injury requiring reconstruction surgery, (2) primary baseball position of pitcher, and (3) minimum follow-up of 16 months. Exclusion criteria were (1) incomplete assessment or documentation of ulnar nerve symptoms at the time of presentation, (2) inadequate description of ulnar nerve handling at the time of surgery, or (3) concurrent injury, other than elbow injury, requiring treatment or intervention.
Outcome Measures
The primary outcome of the study was return to sport. The criterion for return to sport was the ability of the baseball pitcher to return to perform, at the same level of previous play, in at least a single regular season game or playoff season game during competition. The secondary outcome measures were (1) time to return to sport, (2) length of playing career, (3) need for revision surgery, and (4) need for additional surgery other than UCLR. Time to return to sport was referenced from the date of surgery and not the date of injury. Length of playing career refers to the amount of time that the baseball pitcher was able to play after returning from UCLR. Need for additional surgery takes into account whether a decompression or transposition of the ulnar nerve was conducted after the initial UCLR.
Statistical Analysis
Statistical analysis included comparisons of baseball pitchers without ulnar neuritis versus baseball pitchers with ulnar neuritis, all of whom underwent UCLR, with regard to the primary outcome of return to sport. In the same fashion, comparisons were conducted between baseball pitchers with and without ulnar neuritis for the secondary outcomes of time to return to sport, length of playing career, and need for additional or revision surgery. Equally important, associations were assessed between baseball pitchers with and without ulnar neuritis with regard to player characteristics, injury characteristics, and surgical technique. Descriptive analysis of data was performed with means and standard deviations for continuous variables and percentages for dichotomous variables. Normality of data was assessed with the Shapiro-Wilk test. Normally distributed continuous variables were analyzed with a Student t test or analysis of variance for 3 or more comparisons; nonnormally distributed data were analyzed with the Mann-Whitney test. Categorical variables were analyzed with a chi-square test. Player, injury, and treatment characteristics were taken into consideration as potential confounding associations; for this reason, a multivariate regression analysis was performed for any factor that had a P value of <.1. A P value of .05 was used to define significance.
Results
Between 2002 and 2015, a total of 616 patients underwent UCLR. Of these patients, 578 were baseball players, of whom 500 pitchers had complete and adequate follow-up for inclusion in the study. Excluded from the study were 65 baseball pitchers with incomplete data. Among the study cohort, the average age of players undergoing UCLR was 21.3 years, and 392 (78.4%) players were right-handed pitchers. The level of competition at the time of UCL injury requiring reconstruction was 96 (19%) high school players, 224 (45%) college players, and 180 (36%) professional players. A primary injury to the UCL was present in 469 (93.8%) players with a complete tear of the ligament, and was present in 163 (32.6%) pitchers at the time of presentation. Previous nonoperative treatment, including activity modification, physical therapy, and medication, had been attempted in 188 (37.6%) players. Previous UCLR surgery of the throwing elbow had taken place in 65 (13%) pitchers.
Of the 500 baseball pitchers reviewed, 403 (80.6%) had no symptoms or signs of ulnar neuritis (no UN group), and 97 (19.4%) baseball pitchers did have symptoms and signs of ulnar neuritis (UN group). In comparison between the groups, no significant differences were seen in age (UN, 21.8 years; no UN, 21.3 years; P = .40), height (UN, 186.3 cm; no UN, 186.8 cm; P = .44), weight (UN, 88.3 kg; no UN, 90.6 kg; P = .17), or hand dominance (UN, 74% right-handed; no UN, 79% right-handed; P = .27). The level of competition was similar between both groups (UN, 20% high school, 42% college, 36% professional; no UN, 19% high school, 45% college, 33% professional; P = .87) (Table 1).
Characteristics of Baseball Pitchers With and Without Ulnar Neuritis a
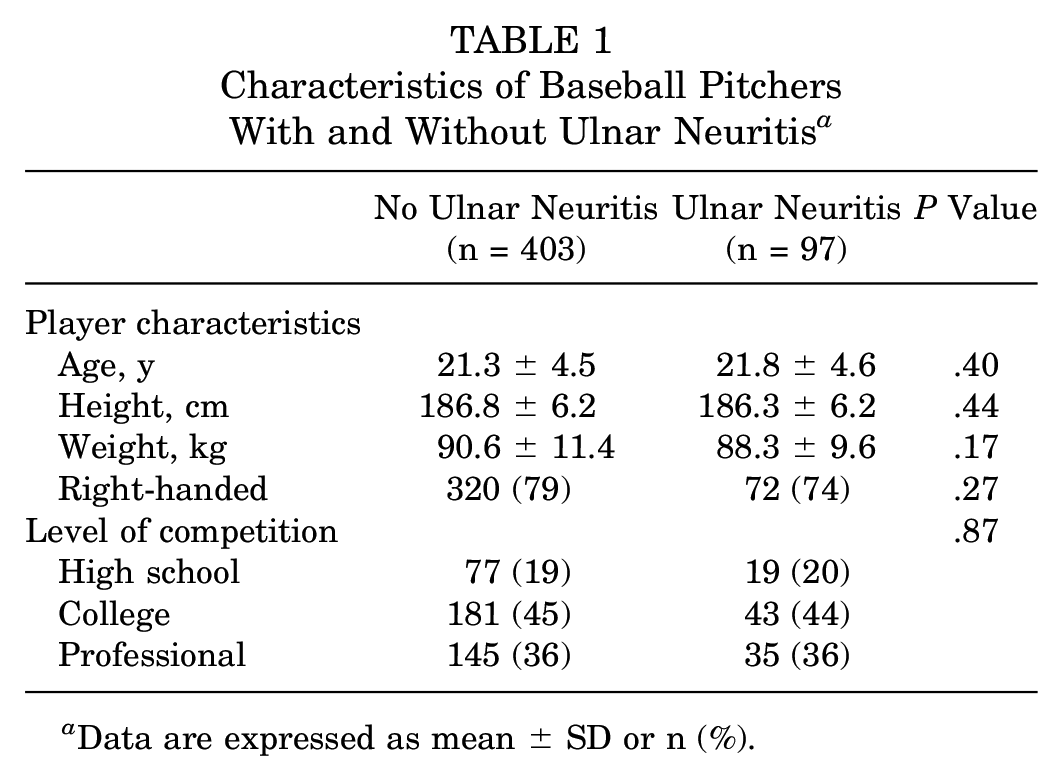
Data are expressed as mean ± SD or n (%).
With regard to injury characteristics in baseball pitchers with and without ulnar neuritis, no significant differences were noted in ligament calcification (UN, 31%; no UN, 24%; P = .16) or partial versus complete tear of the UCL (UN, 33% complete tear; no UN, 33% complete tear; P = .87). Likewise, location of the tear was not significantly different between those with and those without ulnar neuritis (UN, 52% proximal, 11% midbody, 37% distal; no UN, 53% proximal, 9% midbody, 38% distal; P = .70). Previous treatment and previous UCLR surgery were not significantly different between baseball pitchers with or without ulnar neuritis on presentation (previous treatment, P = .62; previous surgery, P = .14). Baseball pitchers who had signs and symptoms of ulnar neuritis on presentation were more likely to have sustained an acute injury with an acute onset (UN, 55% acute; no UN, 42% acute; P = .03) (Table 2). Acute injury and onset of symptoms were significantly associated with transposition of the ulnar nerve at the time of surgery (P = .01).
Injury Characteristics of Baseball Pitchers With and Without Ulnar Neuritis a
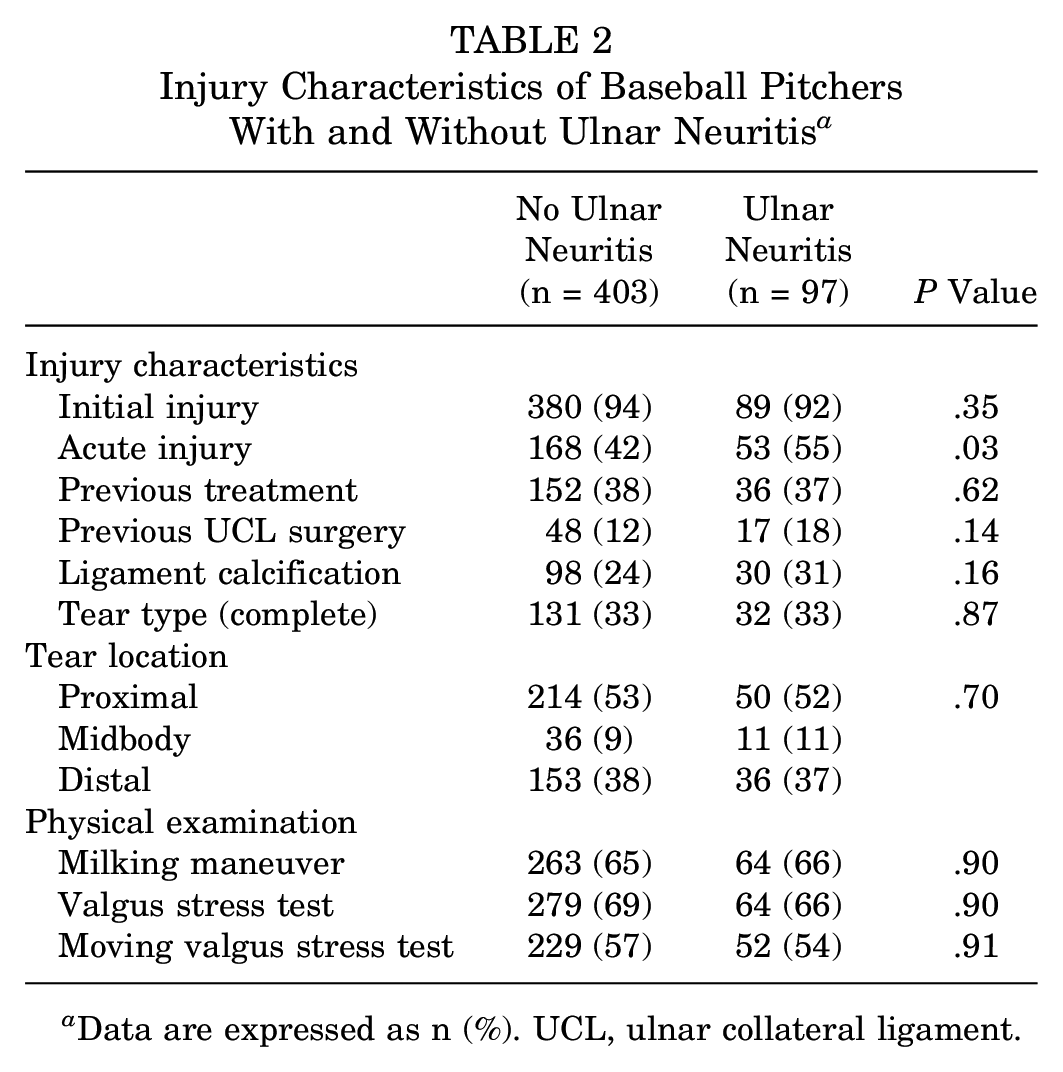
Data are expressed as n (%). UCL, ulnar collateral ligament.
At the time of UCLR, the most commonly performed surgical technique, by surgeon preference, was the modified Jobe UCLR (66.4%). Transposition of the ulnar nerve was not routinely performed for ulnar neuritis but rather was performed at the discretion of the surgeon. The ulnar nerve was transposed primarily for subluxation or secondarily for exposure and access, such as in the case of revision surgery. Nonetheless, transposition of the ulnar nerve was more commonly performed in those with ulnar neuritis (47%) than in those without ulnar neuritis (10%; P = .0001). No significant differences in surgical technique were noted between those with and those without ulnar neuritis undergoing UCLR (UN, 71% modified Jobe, 23% docking, 4% David Altcheck, Neal ElAttrache-Tommy John Technique (DANE-TJ), 2% primary repair; no UN, 65% modified Jobe, 29% docking, 4% DANE-TJ, 2% primary repair; P = .79) (Table 3).
Surgical Techniques for Ulnar Collateral Ligament Reconstruction in Baseball Pitchers With and Without Ulnar Neuritis a
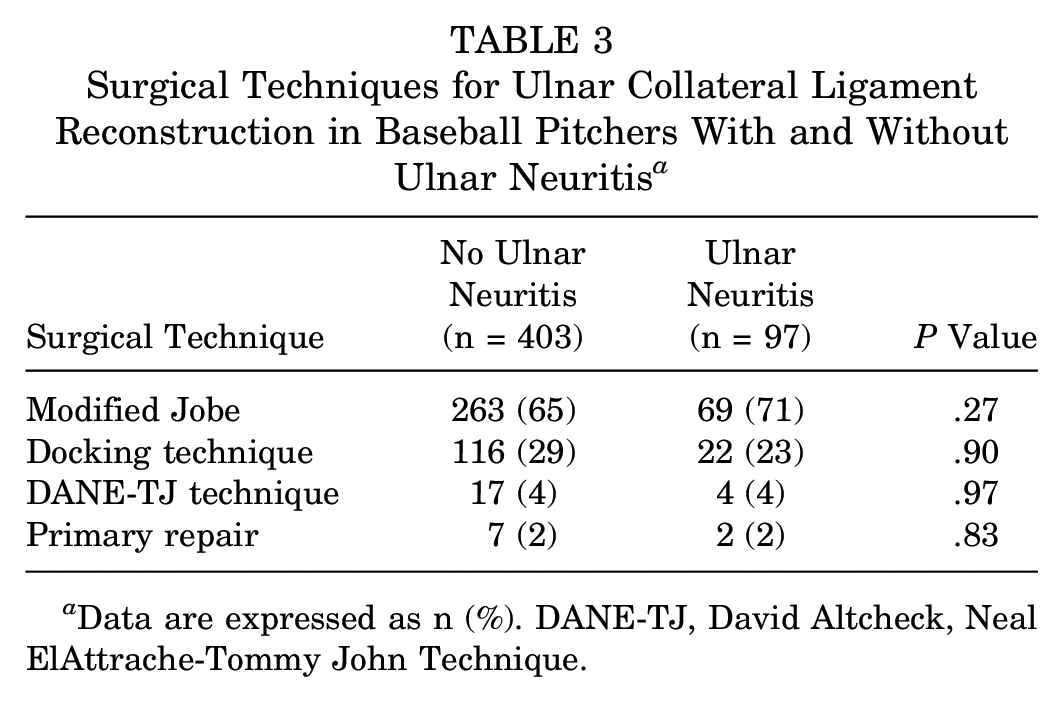
Data are expressed as n (%). DANE-TJ, David Altcheck, Neal ElAttrache-Tommy John Technique.
Baseball pitchers who had ulnar neuritis and underwent UCLR had a significantly lower odds of returning to pitch at the same level of play (odds ratio [OR], 0.45; 95% CI, 0.21-0.97; P = .04). Ulnar nerve transposition was not found to be significantly associated with return to sport (OR, 0.72; P = .46). After we controlled for ulnar nerve transposition, baseball pitchers with ulnar neuritis still had a significantly lower odds of returning to play. After UCLR, baseball pitchers who were able to return to sport in competition demonstrated no significant difference in time to return to sport or length of playing career between those with and those without ulnar neuritis on presentation (UN, return to sport 13.1 months, career length 3.2 years; no UN, return to sport 13.5 months, career length 4.1 years; P = .38 and P = .51, respectively). Additional surgery other than UCLR was required in 13% of players without ulnar neuritis and 10% of players with ulnar neuritis (P = .05), and revision UCLR was required in 4% of pitchers without ulnar neuritis and 1% of pitchers with ulnar neuritis (P = .08). Transposition of the ulnar nerve after the index UCLR procedure was not significantly different between pitchers with and without ulnar neuritis on presentation (UN, 3%; no UN, 3%; P = .85) (Table 4).
Outcomes of Ulnar Collateral Ligament Reconstruction in Baseball Pitchers With and Without Ulnar Neuritis a
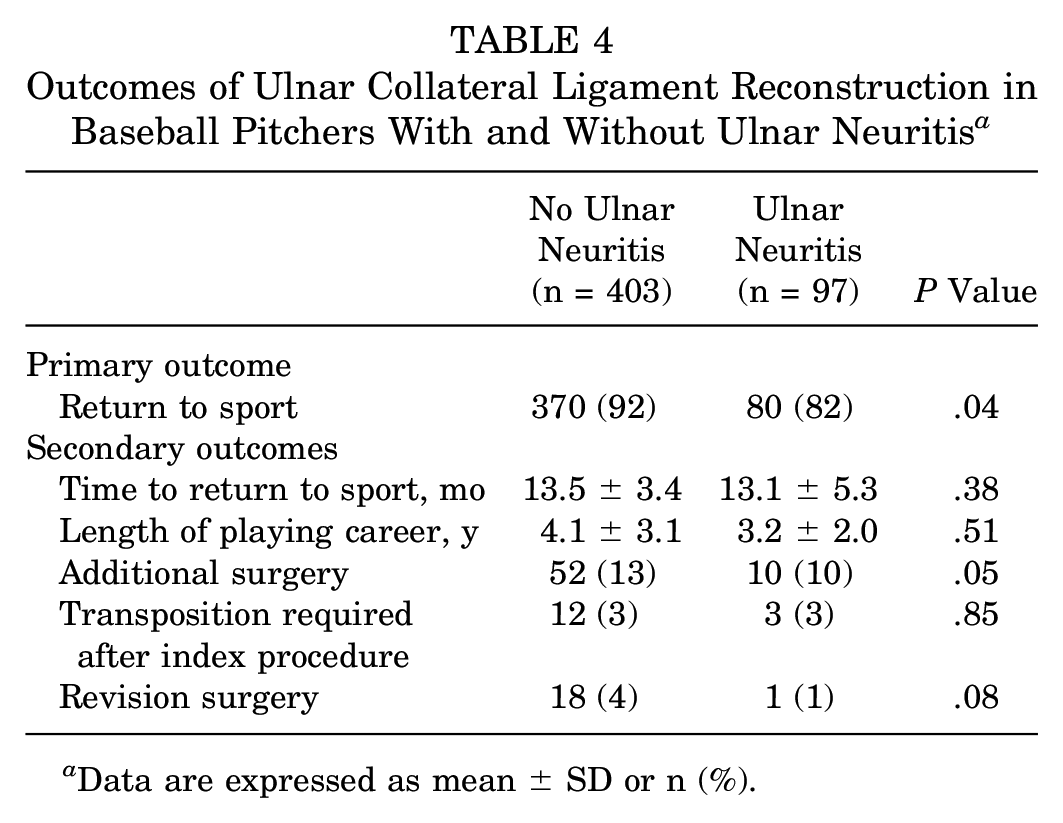
Data are expressed as mean ± SD or n (%).
Discussion
Several studies have demonstrated a high rate of return to sport after UCLR in baseball pitchers.5,9,10,13,14 Despite the encouraging outcomes of these studies, none of them emphasized risk factors identified at the time of presentation that alter the ability to return to sport after UCLR. The purpose of this study was to evaluate whether a common pathology occurring on the medial side of the elbow—ulnar neuritis—has ramifications after UCLR. In our study, baseball pitchers with ulnar neuritis on presentation had a lower rate of return to sport after UCLR. Under these circumstances, handling of the ulnar nerve during the primary surgical reconstruction was not found to be associated with return to sport. After the index UCLR, there was no difference in need for subsequent transposition of the ulnar nerve between baseball pitchers with and without ulnar neuritis.
At the elbow, the ulnar nerve lies posterior to the medial epicondyle in the cubital tunnel and then traverses through the flexor carpi ulnaris muscle before entering the anterior compartment of the forearm. Around the elbow, there are several sites where compression of the nerve can occur. In addition to the multiple potential sites of nerve entrapment, added insult to the ulnar nerve is experienced during the late-cocking and early-acceleration phases of throwing, when tensile stress strikes across structures of the medial elbow. In a biomechanical study, Aoki et al 2 measured the movement of and strain on the ulnar nerve during the throwing motion. In that study, movement of the ulnar nerve at the cubital tunnel was significantly increased during all throwing phases with increased elbow flexion; correspondingly, maximum movement of the ulnar nerve occurred during the wind-up phase of throwing. By the same token, an average maximum strain of 13.1% was recorded at the ulnar nerve during the early-acceleration phase of throwing, which approaches the known elastic limit of the ulnar nerve at 15%. 2 Equally important, the repetitive motion of throwing, near the elastic limit of the ulnar nerve, can lead to disruption of the collagen and circulation. Tai et al 12 used ultrasonography to visualize the ulnar nerve during different phases of throwing in baseball pitchers and nonpitchers to demonstrate greater anterior translation and greater flattening of the ulnar nerve in comparison with controls. In that study, symptoms of ulnar neuritis at the time of presentation were significantly associated with an acute onset and injury of the UCL in baseball pitchers. Taken together, the increased stress and movement experienced by the ulnar nerve during repetitive throwing can contribute to concomitant pathology seen in baseball pitchers evaluated for UCL injury.
Several studies have reported on the commonality of cubital tunnel syndrome in baseball players.1,6,8,11 In these overhead throwing athletes, insult to the ulnar nerve can originate from various elements such as osteophytes, Osborne ligament, anconeus epitrochlearis, arcade of Struthers, compression from adhesions, deep flexor pronator aponeurosis, hypertrophy of the medial head of the triceps, nerve subluxation friction, and traction from valgus stress during the throwing motion.3,4,11 Wei et al 15 compared the nerve conduction velocity of the ulnar nerve in baseball pitchers with an elbow injury versus those without an elbow injury to find a suboptimal, slowed conduction of the nerve in baseball pitchers with a history of injury. Del Pizzo et al 6 described treatment of ulnar neuritis in baseball players with submuscular transposition of the nerve, resulting in a 60% return to sport. Aoki et al 1 reported on the treatment of ulnar neuritis in adolescent baseball players with anterior subcutaneous transposition of the ulnar nerve, resulting in a 83% return to sport. Maruyama et al 11 identified the following risk factors associated with a poor outcome for ulnar neuritis in baseball players: hand numbness, ulnar nerve subluxation, and UCL injury. In that study, concurrent injury of the UCL in the presence of ulnar neuritis was found to contribute to a worse outcome for the pathology of the ulnar nerve. In a similar fashion, our study found that a concurrent injury of the ulnar nerve in the presence of UCL injury was associated with a lower rate of return to sport for baseball pitchers undergoing UCLR surgery.
The results of this study should be interpreted with the following limitations. The overall design of the study was retrospective in nature. Because this was a retrospective study, we can show an association but cannot show causation between ulnar neuritis and return to sport after UCLR. Ulnar neuritis is probably only a portion of a larger picture contributing to return to sport after UCLR. Despite the study design, this study provides the largest cohort of baseball pitchers undergoing UCLR to be evaluated for ulnar neuritis on presentation. The symptoms of ulnar neuritis were accounted for at the time of presentation; however, the chronicity of these ulnar nerve symptoms was not taken into account and may be another prognostic factor in determining return to sport. During chart review, the indication for transposition of the ulnar nerve at the time of index UCLR was not always available. Nevertheless, all UCLR procedures were performed at a single institution where a standard protocol has been developed whereby surgeons do not routinely transpose the ulnar nerve but rather tailor transposition of the ulnar nerve according to individual circumstances for exposure, symptomatic subluxation, chronic symptoms, or revision surgery. The exact indication for each transposition of the ulnar nerve was not clearly described on all operative reports and remains a limitation to the study.
In conclusion, ulnar neuritis at the time of presentation of UCL injury in baseball pitchers is common and, if diagnosed concurrently with UCL injury, may result in a lower rate of return to sport after UCLR surgery. In pitchers who are able to return to sport after UCLR surgery, career longevity does not seem to be affected by the presence or absence of ulnar neuritis at the time of UCL injury. Equally important, transposition of the ulnar nerve during UCLR does not seem to limit the ability to return to throwing a baseball. Future studies are warranted to further examine how ulnar neuritis affects baseball pitchers who undergo UCLR.
Footnotes
Submitted November 19, 2020; accepted July 13, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.F.D. has received research support from DJO; education support from Arthrex, Micromed, and Smith & Nephew; and hospitality payments from Stryker Corp. R.A.K. has received research support from DJO; education support from Arthrex, Pinacle, and Smith & Nephew; and hospitality payments from Stryker Corp. M.B. has received consulting fees from Stryker Corp and Vericel; education support from Arthrex; and hospitality payments from MAKO Surgical and Smith & Nephew. N.S.E. has received royalties and speaking fees from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.