
Abstract
Background:
Changes in the intra-articular inflammatory state during the immediate period after an acute anterior cruciate ligament (ACL) rupture are not well defined.
Purpose:
To evaluate changes in the concentration of select proinflammatory and anti-inflammatory synovial fluid cytokines during the interval between an ACL injury and surgical reconstruction.
Study Design:
Descriptive laboratory study.
Methods:
In patients with an acute ACL injury, a synovial fluid sample was obtained from the injured knee during the initial office visit within 2 weeks of the inciting traumatic event. An additional synovial fluid sample was collected at the time of ACL reconstruction just before the surgical incision. Synovial fluid samples from both the acute injury and the surgery time points were processed with a protease inhibitor, and the concentrations of 10 cytokines of interest were measured using a multiplex magnetic bead immunoassay. The primary outcome was the change in cytokine concentrations between time points.
Results:
A total of 20 patients with a mean age of 30.2 ± 8.3 years were included. The acute injury synovial fluid samples were collected at 6.6 ± 3.8 days after the injury. The surgical synovial fluid samples were collected at 31.6 ± 15.6 days after the acute injury samples. Based on a series of linear mixed-effects models to control for the effect of concomitant meniscal injuries and by-patient variability, there was a statistically significant increase in the concentrations of RANTES and bFGF and a statistically significant decrease in the concentrations of IL-6, MCP-1, MIP-1β, TIMP-1, IL-1Ra, and VEGF between time points.
Conclusion:
This study demonstrates the ongoing alterations in the intra-articular microenvironment during the initial inflammatory response in the acute postinjury period. We identified 6 synovial fluid cytokines that significantly decreased and 2 that significantly increased between the first clinical presentation shortly after the injury and the time of surgery 1 month later.
Clinical Relevance:
This study describes the molecular profile of the inflammatory changes between the time of an acute ACL injury and the time of surgical reconstruction 1 month later. A greater understanding of the acute inflammatory response within the knee may be helpful in identifying the optimal timing for a surgical intervention that balances the risk of chondral damage with the likelihood of successful, well-healed reconstruction.
Anterior cruciate ligament (ACL) reconstruction is a commonly performed procedure, with success rates ranging from 82% to 95% with respect to the restoration of stability.25,41,46 However, postoperative recovery is variable and has not been shown to mitigate the development of posttraumatic osteoarthritis (PTOA). As many as 50% to 60% of reconstructed knees demonstrate evidence of arthritic changes at long-term follow-up.14,17
Despite the frequency of this athletic injury, there are inconsistent data on the optimal timing for a surgical intervention. While previous studies have suggested that early reconstruction is associated with a greater risk of arthrofibrosis and a delayed return of quadriceps strength,42,43,50 recent analyses suggest that outcomes are comparable for patients with early versus delayed reconstruction, and an early intervention may be associated with a reduced risk of developing PTOA.3,21,26,31 The relationship between inflammation, the timing of ACL reconstruction, and postoperative outcomes is poorly understood. Without a consensus on the optimal timing of ACL surgery, a better characterization of the inflammatory changes that occur between the injury and surgery is warranted.
Synovial fluid biomarkers show promise as indicators of inflammation and healing in the setting of orthopaedic injuries. There are measurable changes in the joint microenvironment after an injury, including an increased expression of proinflammatory cytokines, matrix metalloproteinases (MMPs), aggrecanases, growth factors, and apoptotic factors.4,35 Changes in the expression profile of these same proteins have been measured in the synovial fluid of patients with an ACL injury preoperatively and postoperatively as well as in controls with an intact ACL.2,12,27-29,36 These reports indicate the possible utility of synovial fluid biomarkers in predicting associated cartilage abnormalities, postoperative pain, and functional outcomes.13,29,38 However, changes in synovial fluid cytokine levels during the short-term postinjury period before surgery have yet to be characterized in patients with an acute ACL rupture. Changes in the intra-articular inflammatory profile may help identify an optimal time for a surgical intervention, with maximized anabolic cytokines and minimized catabolic cytokines.
The purpose of the current study was to evaluate the change in the concentration of select proinflammatory and anti-inflammatory synovial fluid cytokines during the interval between an ACL injury and surgery. We hypothesized that synovial fluid samples collected at a patient’s initial office visit would exhibit a higher expression of proinflammatory markers and a lower expression of anti-inflammatory markers than synovial fluid samples collected at the time of surgery. These findings would provide an initial step toward a more complete description of the intra-articular microenvironment after structural knee injuries and how the concentrations of several major players in the acute inflammatory response change over time. Ultimately, these data may be used in identifying targets for future therapy to not only improve postoperative outcomes and limit complications after ACL reconstruction but also potentially reduce the incidence of PTOA.
Methods
Study Design
This was an institutional review board–approved, prospectively designed study based on data collected for a database of synovial fluid cytokines in the context of a knee injury. This analysis consisted of patients presenting with an acute ACL injury between October 2016 and May 2019. The patients in this analysis were indicated for primary surgical reconstruction based on pain or functional impairment in addition to magnetic resonance imaging evidence of an ACL injury corresponding to a clinical presentation according to the standard of care. To evaluate the changes in the synovial fluid microenvironment in the short-term postinjury period, synovial fluid aspiration was performed at 2 time points: the first aspiration was performed at the time of the initial presentation after an acute ACL injury, and the second aspiration was performed on the day of surgical reconstruction. The primary outcome of this study was the difference in the concentration of 10 preselected synovial fluid cytokines between the acute injury time point and the surgery time point. The secondary outcomes were the difference in the MMP-3 to tissue inhibitor of metalloproteinase (TIMP)–1 ratio and the difference in the MMP-3 to TIMP-2 ratio between time points.
Inclusion criteria included a duration of no more than 2 weeks between the injury and initial presentation (and first synovial fluid sampling), 2 successful synovial fluid aspirations at the specified time points, and confirmation of a complete ACL tear intraoperatively. Exclusion criteria included a previous ipsilateral knee injury, previous ipsilateral knee surgery, an extensive ipsilateral cartilage injury with an International Cartilage Regeneration & Joint Preservation Society (ICRS) grade of greater than 1, systemic inflammatory disease, autoimmune disease, previous intra-articular corticosteroid injections, use of an immunomodulatory medication, chemotherapy within the previous year, and patients younger than 18 years. Overall, this study included patients with an acute ACL rupture with an initial synovial fluid sample drawn less than 2 weeks from the acute injury, with ICRS grade 1 cartilage based on an intraoperative assessment.
Funding was provided through a gift from the Bady Foundation. The funding source did not have any involvement in the study design, collection of data, analysis or interpretation of data, and generation or review of the manuscript.
Synovial Fluid Collection
For all included patients, synovial fluid sampling was first performed at the initial office consultation shortly after the acute knee injury. Synovial fluid sampling was performed again at the time of surgery, after standard sterile preparation and draping but immediately before the surgical incision was made. The methods used to collect, store, and analyze the synovial fluid samples were identical to those described previously by Clair et al. 11 An 18-gauge needle was inserted into the joint space via the superolateral knee portal site before the surgical incision for the operative samples. The maximal amount of synovial fluid was aspirated from the injured knee and transferred to a sterile tube. A protease inhibitor cocktail solution (EDTA-Free Halt Protease Inhibitor Cocktail; Thermo Fisher Scientific) was then added to the sample. The samples were immediately centrifuged at 3820 rpm (2288g) and 20°C for 10 minutes. Centrifuges were located in the immediate vicinity of both the clinic and the operating room, and there was no difference in the sample processing time between locations. After centrifugation, the supernatant was aliquoted into sterile cryotubes and stored at −80°C until the time of cytokine analysis.
Cytokine Analysis
The synovial fluid samples from both time points were analyzed to determine the concentrations of 10 cytokines that have previously been suggested to play a role in joint space inflammation and cartilage degradation (Table 1). 12 Custom and standard precoated multiplex V-PLEX Plus Human assay plates (Meso Scale Discovery) were used, including the Human MMP-3 Ultra-Sensitive Kit, Human RANTES (regulated on activation, normal T cell expressed and secreted) Ultra-Sensitive Kit, Human bFGF (basic fibroblast growth factor) Kit, Human TIMP-1 Kit, Human TIMP-2 Kit, Human IL-1Ra (interleukin-1 receptor antagonist) Kit, and MULTI-SPOT Human 4-Plex Assay: IL-6, vascular endothelial growth factor (VEGF), monocyte chemoattractant protein–1 (MCP-1), and macrophage inflammatory protein–1β (MIP-1β).
Basic Functions of Tested Cytokines a
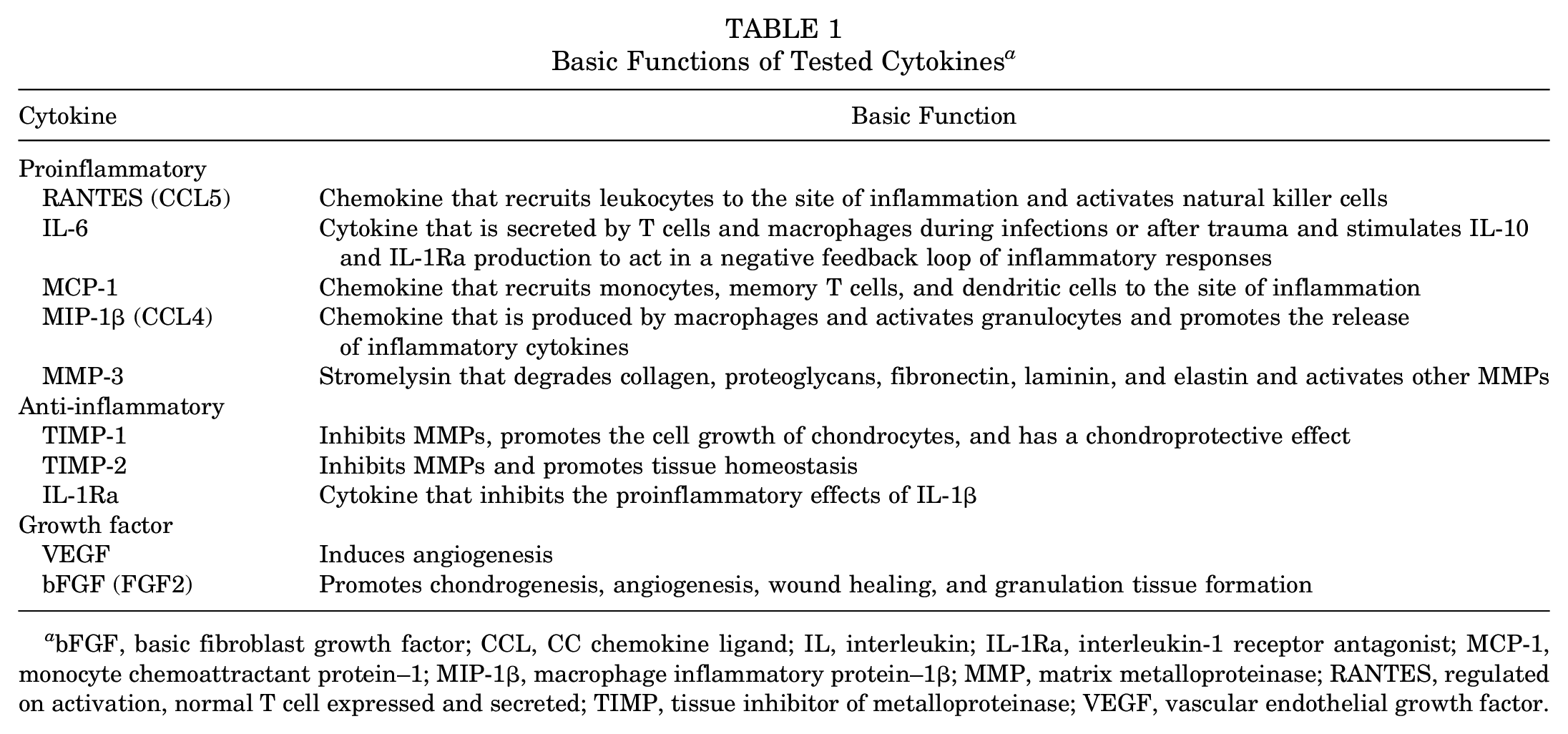
bFGF, basic fibroblast growth factor; CCL, CC chemokine ligand; IL, interleukin; IL-1Ra, interleukin-1 receptor antagonist; MCP-1, monocyte chemoattractant protein–1; MIP-1β, macrophage inflammatory protein–1β; MMP, matrix metalloproteinase; RANTES, regulated on activation, normal T cell expressed and secreted; TIMP, tissue inhibitor of metalloproteinase; VEGF, vascular endothelial growth factor.
The synovial fluid samples were thawed and then assayed in duplicate. The plates were read using the QuickPlex SQ 120 Plate Reader/Scanner (Meso Scale Discovery). Discovery Workbench software 4.0 (Meso Scale Discovery) was used to generate a standard curve that was compared with the standard curve provided with each kit. If the results fell within the range determined by the standard curve, they were accepted.
Statistical Analysis
Statistical analysis was performed using R (R Foundation for Statistical Computing) and the lme4 package in R. 5 Sample size calculation for a comparison of correlated samples based on dz = 0.8 (effect size), α = .05, and 1–β = 0.80 revealed a necessary sample size of 15 patients. The differences in synovial fluid cytokine concentrations at the acute injury time point and the surgery time point were first compared using a series of Wilcoxon signed-rank tests. The differences in concentrations between time points were further evaluated using a series of linear mixed-effects models to control for the potentially confounding effect of a concomitant meniscal injury. Because of the nonparametric nature of the data, the cytokine concentrations were log-transformed. The fixed effects for each model included the time point of the synovial fluid sample (acute injury vs surgery) and the presence or absence of concomitant meniscal injuries. Each model included by-patient random effects to account for individual variability in synovial fluid cytokine concentrations. The MMP to TIMP ratios were log-transformed and compared using paired t tests.
Results
Patient Demographics and Surgical Characteristics
A total of 345 patients underwent ACL reconstruction within the 2.5-year study period; of these, 180 patients agreed to participate in the general synovial fluid sampling study. Of these patients, 40 agreed to synovial fluid sampling in the office at the acute injury time point. However, 19 of these patients presented more than 2 weeks after their injury, and 1 patient had an ICRS grade of greater than 1. This led to a total of 20 patients (12 female [60%]) with a mean age of 30.2 ± 8.3 years who were included in the study (Figure 1). All 20 patients completed follow-up, and there were no missing data. The mean body mass index was 24.3 ± 3.4. The preoperative Tegner score was 7 (interquartile range, 6-7). All patients had preoperative Lachman grade 2B, and 18 patients (90%) had a preoperative range of motion deficit compared with the uninjured, contralateral side. Surgery occurred at a mean of 39 ± 7 days after the initial injury. The acute injury synovial fluid samples were obtained at a mean of 6.6 ± 3.8 days after the inciting traumatic event. The acute injury and surgery samples were collected at a mean of 31.6 ± 15.6 days apart. On the basis of arthroscopic findings, all patients had complete ACL tears, and 12 patients (60%) had a concomitant meniscal injury. All patients had an ICRS grade of 1. A summary of the clinical characteristics for the study population is shown in Table 2.
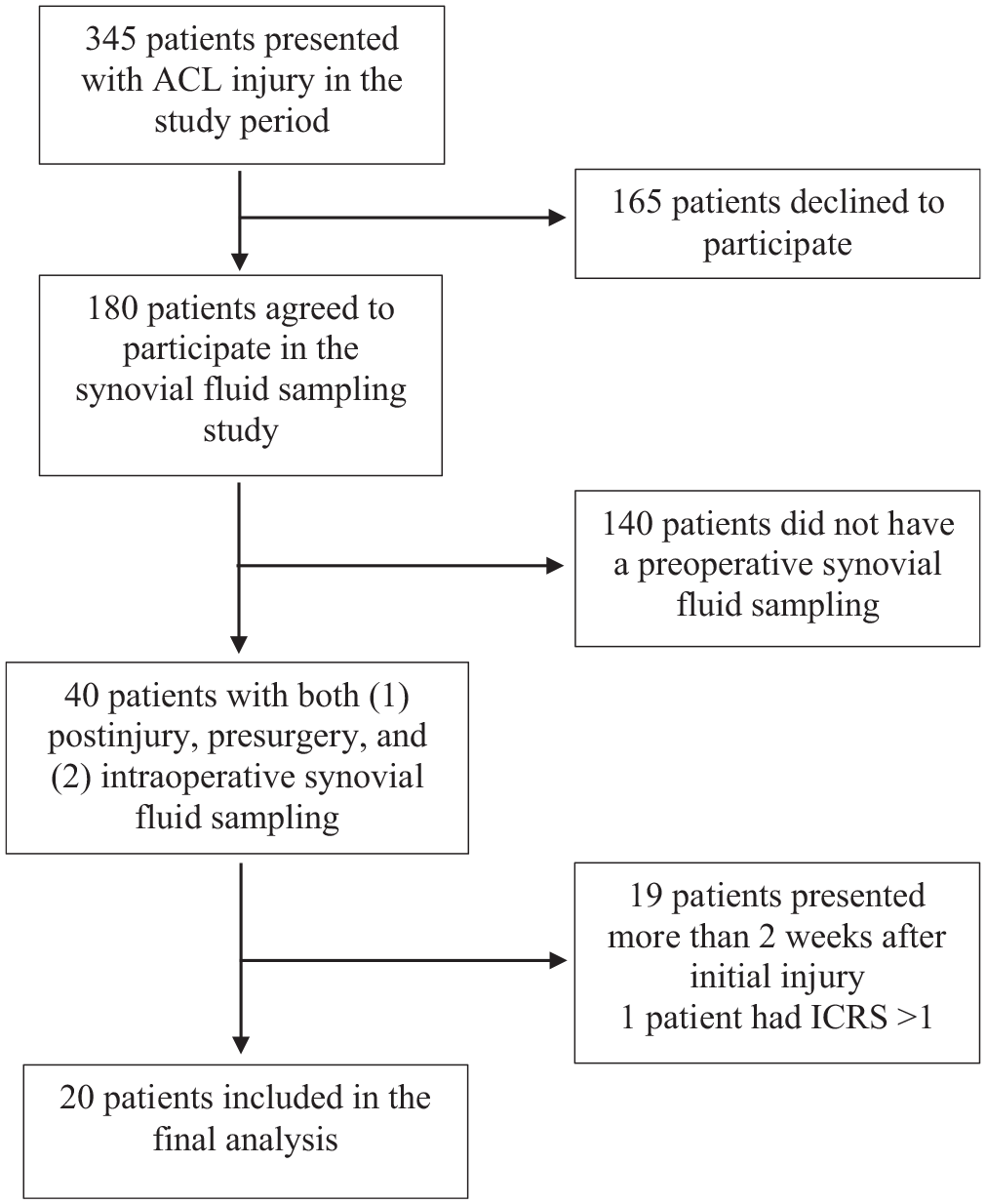
Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) diagram of included patients. ACL, anterior cruciate ligament; ICRS, International Cartilage Regeneration & Joint Preservation Society.
Preoperative Clinical Characteristics of Study Population a
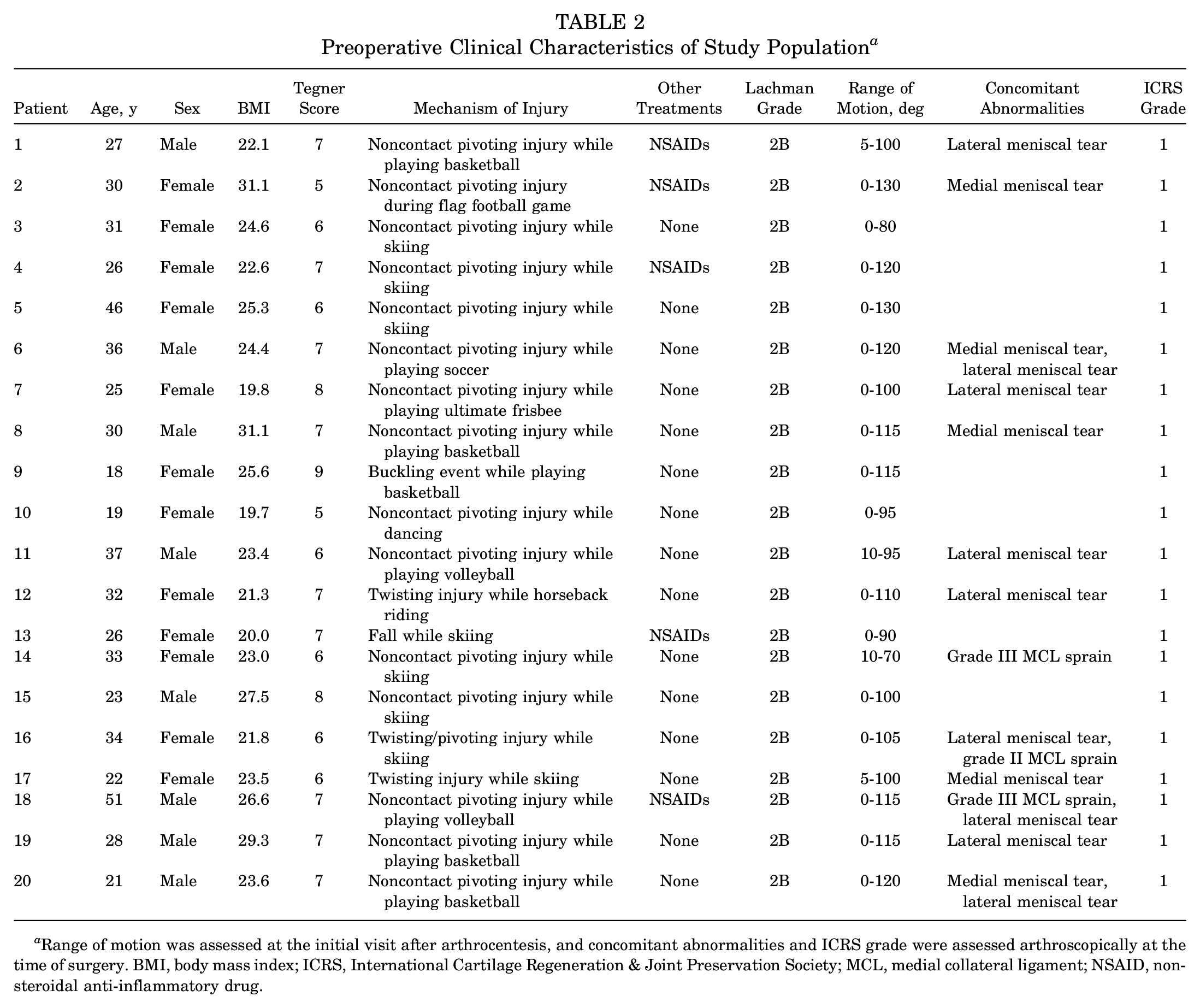
Range of motion was assessed at the initial visit after arthrocentesis, and concomitant abnormalities and ICRS grade were assessed arthroscopically at the time of surgery. BMI, body mass index; ICRS, International Cartilage Regeneration & Joint Preservation Society; MCL, medial collateral ligament; NSAID, nonsteroidal anti-inflammatory drug.
Changes in Synovial Fluid Cytokine Concentrations Between the Acute Injury and Surgery
Based on the Wilcoxon signed-rank test, from the time of the initial presentation after the acute injury to the time of surgery roughly 1 month later, there was a statistically significant increase in the concentrations of RANTES, bFGF, and MMP-3 and a statistically significant decrease in the concentrations of IL-6, MCP-1, MIP-1β, TIMP-1, IL-1Ra, and VEGF. There was no significant change in the concentration of TIMP-2 (Table 3). Individual changes in cytokine concentrations between time points are visualized in Figure 2.
Concentrations of Synovial Fluid Cytokines a
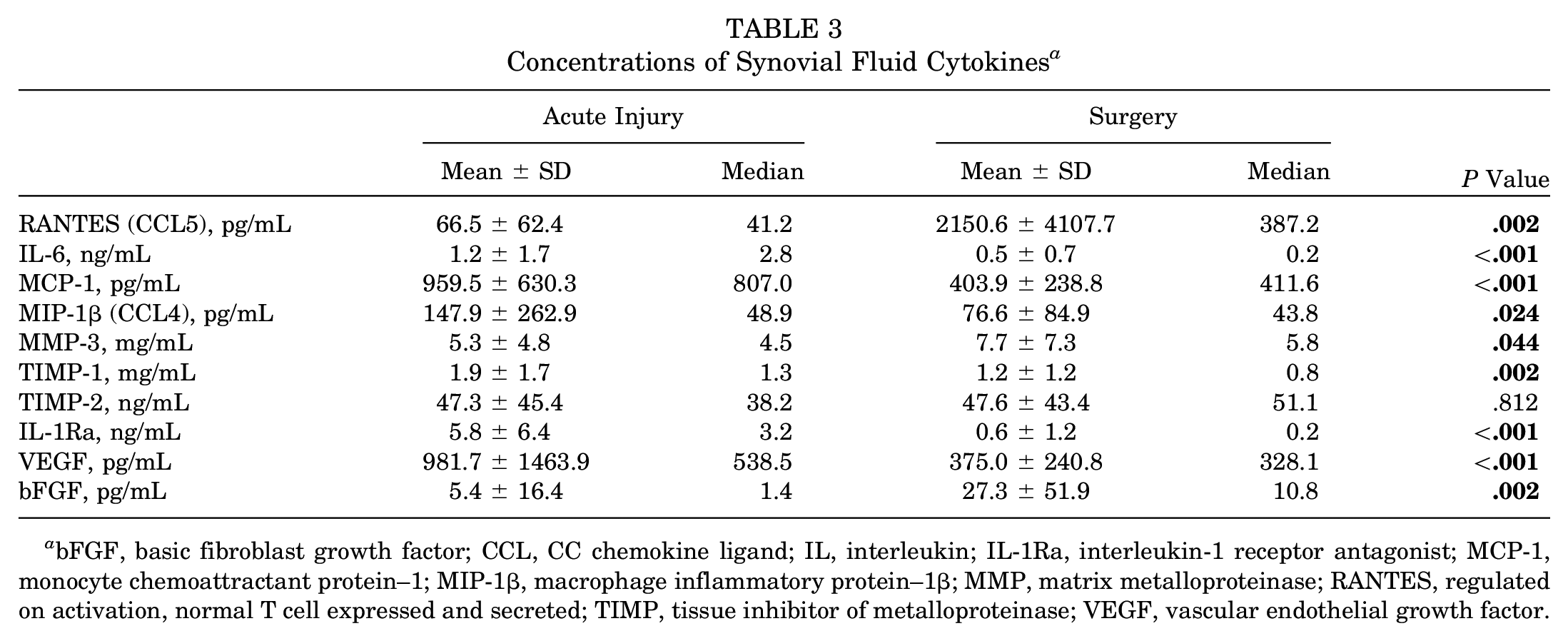
bFGF, basic fibroblast growth factor; CCL, CC chemokine ligand; IL, interleukin; IL-1Ra, interleukin-1 receptor antagonist; MCP-1, monocyte chemoattractant protein–1; MIP-1β, macrophage inflammatory protein–1β; MMP, matrix metalloproteinase; RANTES, regulated on activation, normal T cell expressed and secreted; TIMP, tissue inhibitor of metalloproteinase; VEGF, vascular endothelial growth factor.
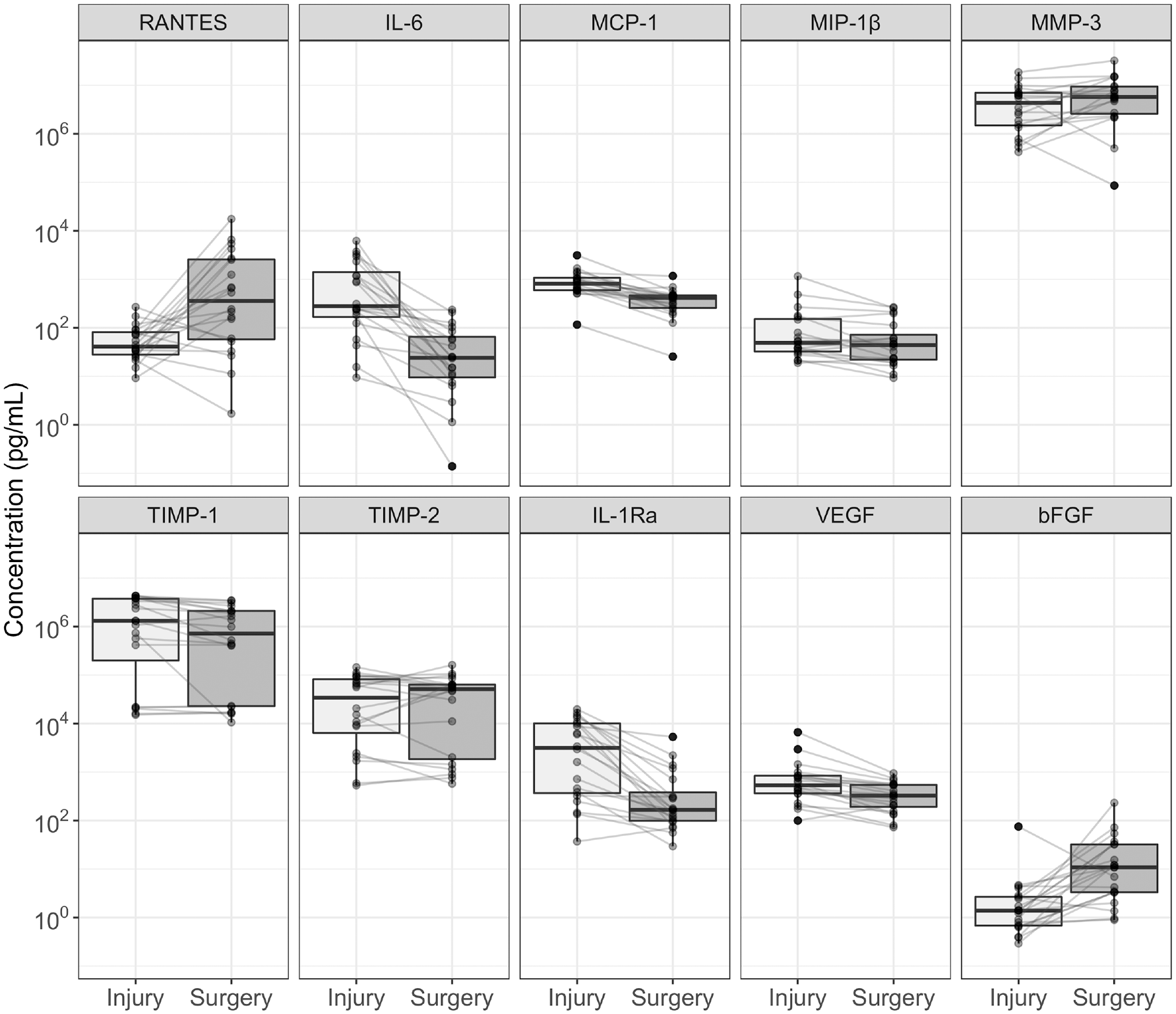
Boxplots demonstrating concentrations of synovial fluid cytokines at the time of the acute injury and the time of surgery. Lines represent changes among individual patients. bFGF, basic fibroblast growth factor; IL, interleukin; IL-1Ra, interleukin-1 receptor antagonist; MCP-1, monocyte chemoattractant protein–1; MIP-1β, macrophage inflammatory protein–1β; MMP, matrix metalloproteinase; RANTES, regulated on activation, normal T cell expressed and secreted; TIMP, tissue inhibitor of metalloproteinase; VEGF, vascular endothelial growth factor.
The same changes in concentrations were observed using a series of linear mixed-effects models to control for the effect of concomitant meniscal injuries and by-patient variability (Table 4). Between the acute injury and surgery time points, there was a 608% increase in the RANTES concentration (t = 3.63; P < .001) and a 500% increase in the bFGF concentration (t = 4.34; P < .001) when holding the other variables constant. Likewise, there was a 95% decrease in IL-6 (t = −6.53; P < .001), a 59% decrease in MCP-1 (t = −6.92; P < .001), a 34% decrease in MIP-1β (t = −3.02; P = .007), a 41% decrease in TIMP-1 (t = −2.42; P = .025), an 87% decrease in IL-1Ra (t = −6.37; P < .001), and a 48% decrease in VEGF (t = −5.19; P < .001). The increase in the MMP-3 concentration observed in the previous analysis was not significant in the mixed-effects analysis (t = 1.32; P = .202).
Exponentiated Beta Coefficients a
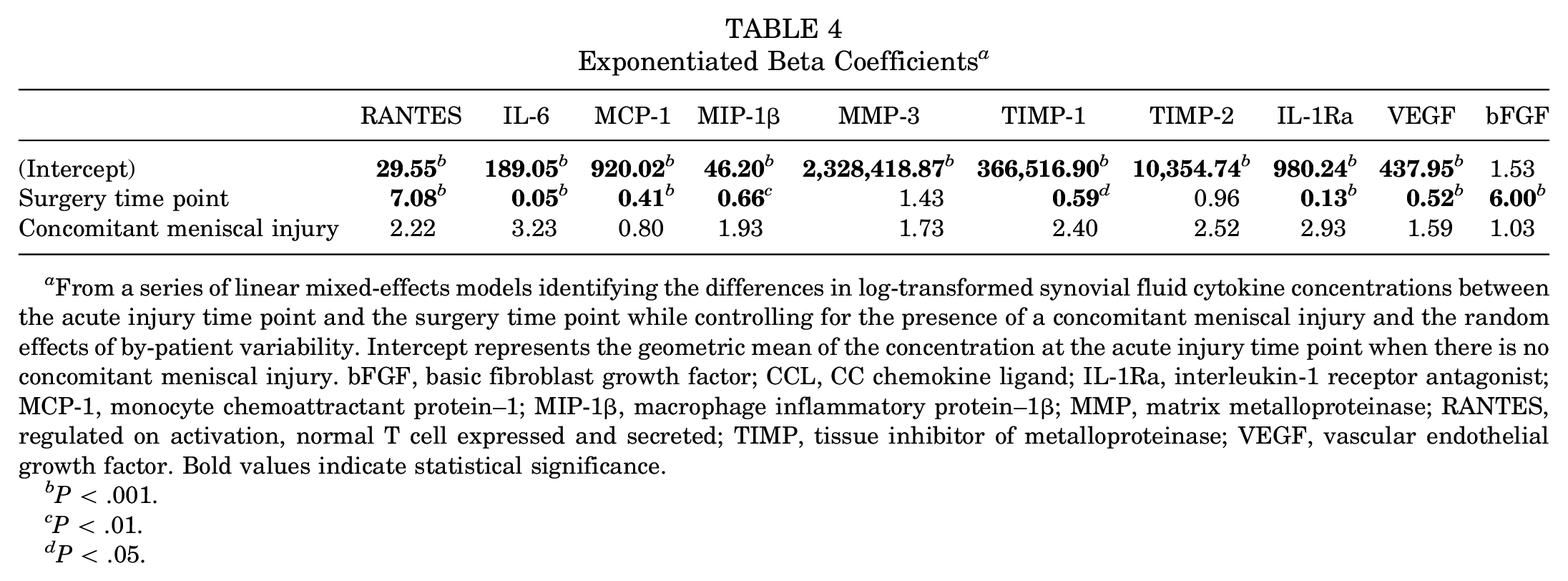
From a series of linear mixed-effects models identifying the differences in log-transformed synovial fluid cytokine concentrations between the acute injury time point and the surgery time point while controlling for the presence of a concomitant meniscal injury and the random effects of by-patient variability. Intercept represents the geometric mean of the concentration at the acute injury time point when there is no concomitant meniscal injury. bFGF, basic fibroblast growth factor; CCL, CC chemokine ligand; IL-1Ra, interleukin-1 receptor antagonist; MCP-1, monocyte chemoattractant protein–1; MIP-1β, macrophage inflammatory protein–1β; MMP, matrix metalloproteinase; RANTES, regulated on activation, normal T cell expressed and secreted; TIMP, tissue inhibitor of metalloproteinase; VEGF, vascular endothelial growth factor. Bold values indicate statistical significance.
P < .001.
P < .01.
P < .05.
MMP to TIMP Ratios
There was a statistically significant increase in the log-transformed MMP-3 to TIMP-1 ratio from the acute injury time point to the surgery time point (from 1.65 ± 2.12 to 2.54 ± 1.95 [95% CI, 0.42-1.35]; P < .001) (Figure 3). There was no statistically significant difference in the log-transformed MMP-3 to TIMP-2 ratio between time points (from 5.19 ± 1.66 to 5.58 ± 2.04 [95% CI, –0.20 to 0.99]; P = .182).
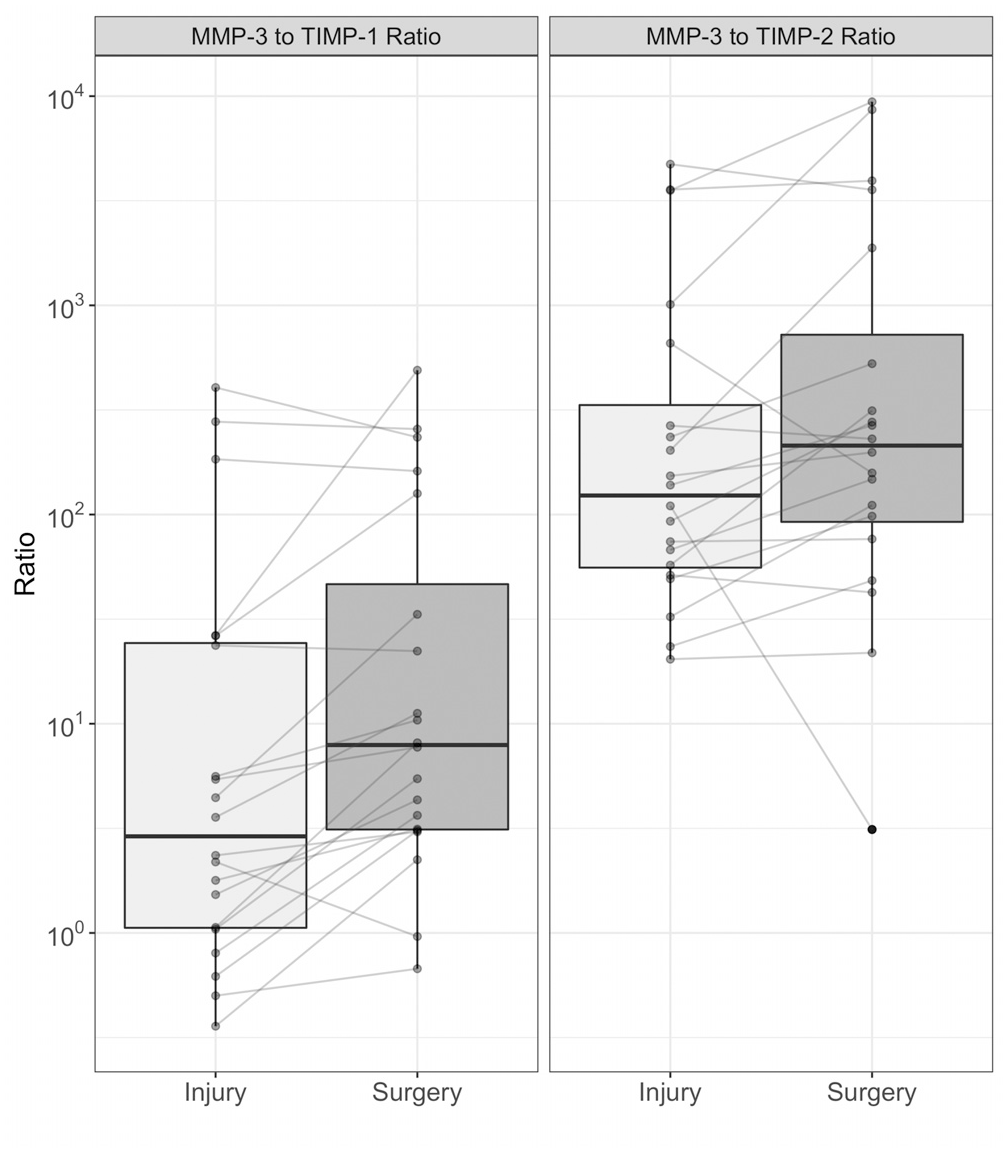
Boxplots demonstrating changes in the MMP-3 to TIMP-1 ratio and the MMP-3 to TIMP-2 ratio between the acute injury and surgery. MMP, matrix metalloproteinase; TIMP, tissue inhibitor of metalloproteinase.
Discussion
In the current study, we longitudinally evaluated the intra-articular microenvironment of 20 knees with acutely ruptured ACLs over the short-term postinjury period. Our analysis identified 2 synovial fluid cytokines whose concentrations increased and 6 cytokines whose concentrations decreased in the time between the initial office visit and surgery for the ACL rupture roughly 1 month later. The concentration of bFGF significantly increased between the 2 time points, while the concentration of VEGF significantly decreased. Of the proinflammatory cytokines measured, 1 significantly increased (RANTES), 3 significantly decreased over time (IL-6, MIP-1β, MCP-1), and 1 exhibited no significant change (MMP-3). Also, 2 of the anti-inflammatory cytokines significantly decreased over time (IL-1Ra, TIMP-1), and 1 had no significant change (TIMP-2).
A better understanding of the underlying pathophysiological process of acute inflammation and the eventual development of PTOA will require not only a description of which molecular players are involved in the onset and perpetuation of the degradative process but also a deeper knowledge of how the level of each cytokine changes over time. The results of this study demonstrate that in the month after an acute ACL injury, the concentrations of intra-articular inflammatory cytokines changed significantly. This has important implications for studies attempting to describe the molecular process of acute knee injuries and early PTOA. When building models for the purpose of using intra-articular inflammatory patterns to predict the risk of PTOA, the timing of synovial fluid sampling will need to be incorporated. Furthermore, a better understanding of the intra-articular milieu over time has an important clinical correlate of identifying the most appropriate interval between the injury and surgery for optimized clinical outcomes.
Many molecular markers demonstrated fluctuations in their concentrations over time, with the levels of bFGF and RANTES showing the strongest and most dramatic changes in the synovial fluid of patients with an ACL injury between preoperative and intraoperative measurements. There was a significant increase in the level of bFGF between the injury and surgery, which is consistent with previous studies demonstrating the role that bFGF plays in chondrogenesis, angiogenesis, wound healing, and granulation tissue formation.32,48 A study by Cameron et al 8 showed that bFGF increases in the setting of ACL injuries and remains elevated for as long as ≥4 weeks. The physiological process initiated by bFGF likely begins shortly after the acute injury and may be upregulated to a certain point over time, which is reflected in the increased level of the growth factor in this cohort. bFGF has shown promise as a positive biomarker of tendon-to-bone healing after ACL reconstruction in animal models, and elevated bFGF has been implicated as a marker of osteoarthritis and cartilage injuries.10,23,27,49 Future studies are warranted to evaluate if bFGF levels are predictive of postoperative outcomes and developing PTOA in the setting of an ACL rupture and subsequent repair.
Conversely, VEGF was found to decrease in the short-term period after the injury. VEGF is an angiogenic factor secreted by endothelial cells, synoviocytes, and chondrocytes. 16 While VEGF has been shown to increase in the setting of articular cartilage injuries and osteoarthritis, VEGF concentrations are similar in synovial biopsy specimens from ACL-deficient knees and healthy controls.13,27,34 This may indicate that VEGF plays a more dominant role in the initial chondral injury and bony edema caused by a traumatic ACL rupture, and VEGF concentrations may decrease as acute inflammation after the injury subsides.
Many of the cytokines that are known to be active during the acute phase were also observed to decrease in concentration between time periods. This process may be activated and reach its peak early in the postinjury period before decreasing by the time of surgery, which was a mean of roughly 32 days after the injury in this cohort. Of note, IL-6 was shown to be elevated by over 20-fold at the time of the injury compared with the time of surgery, which is consistent with the increase in expression reported by Kaplan et al, 27 Struglics et al, 47 Higuchi et al, 22 Papathanasiou et al, 38 and Cuellar et al 12 in ACL injuries. IL-6 is a cytokine secreted by T cells and macrophages in the setting of infections or trauma that can stimulate the release of anti-inflammatory cytokines, which serves as a negative feedback loop in regulating the inflammatory response. Consistent with this model, anti-inflammatory IL-1Ra levels also decreased over time in this study, perhaps as a result of reduced IL 6–signaled release. IL-6 elevation has been implicated in cartilage destruction and osteoarthritis, and patients who underwent early as opposed to delayed ACL reconstruction were shown to have a sustained elevation of IL-6 up to 8 months after surgery.12,27,28 IL-6 levels may prove to be a key indicator in identifying an optimal time for a surgical intervention as well as serve as a biomarker for an increased risk of developing PTOA.
MIP-1β, MCP-1, and RANTES are all chemokines involved in the recruitment of inflammatory cells. MIP-1β is released by macrophages in response to lipopolysaccharides to recruit neutrophils, eosinophils, and basophils. 44 MCP-1 is a chemokine that recruits monocytes, memory T cells, and dendritic cells to the site of inflammation by tissue injuries or infections. 15 Both of these proinflammatory chemokines have been consistently reported as elevated in knees with ACL ruptures12,27 and were found in this study to significantly decrease in the time between the ACL injury and surgery. This is consistent with the idea that acute inflammation may be activated and then subside during this period.
RANTES, which recruits natural killer T cells and leukocytes to the site of injury, was increased over the injury-to-surgery interval. Previous studies of ACL biomarkers have not exhibited a significant difference in RANTES in ACL-deficient knees compared with contralateral controls and may actually exhibit decreased RANTES expression.13,27 While a mechanism for this opposite pattern has yet to be proposed, there are limited data suggesting that monocyte recruitment in knee osteoarthritis is mediated by MCP-1 but not RANTES. 40 This may explain why RANTES and MCP-1 do not exhibit similar changes in expression over the study duration, but it does not explain why this proinflammatory marker would increase between the injury and surgery.
Finally, our study measured the expression of MMP-3 and its regulators: TIMP-1 and TIMP-2. MMP-3 is a key enzyme in cartilage destruction that is regulated by the TIMP family of protease inhibitors, which limits articular damage secondary to MMP-3 activity.19,22,39 The balance of MMPs and TIMPs in a joint is typically within a careful homeostasis that appears to become disrupted by an injury, causing the upregulation of catabolic metalloproteases to remodel the damaged tissues. 18 However, this catabolic state may be detrimental to the reconstructed ligament as it heals. While the expression of TIMP-1 significantly decreased in this study, the changes in MMP-3 and TIMP-2 failed to meet statistical significance. This differs from the findings of Lattermann et al, 30 who reported a statistically significant increase in MMP-3 levels over time after an ACL injury. Previous studies have suggested that the expression of MMPs and TIMPs tend to concurrently increase in the setting of an injury. 24 Notably, while recent meta-analyses demonstrated that elevated MMP-3 is a consistent diagnostic marker for osteoarthritis, these have cast doubt on whether MMP-3 levels alone reliably correlate with osteoarthritis severity. 7 Subsequently, some studies report the ratio of MMP-3 to TIMP-1 expression to evaluate changes in metalloproteinase-mediated cartilage damage.11,33,51 Our analysis demonstrated a significant increase in the MMP-3 to TIMP-1 ratio during the acute postinjury period. This suggests an increase in metalloproteinase-mediated joint destruction in the time between the injury and surgery, perhaps contributing to concerns that delaying surgery can result in a greater risk of cartilage damage, given this evidence of unopposed catabolic enzymatic activity within the joint space. The importance of this increased ratio is highlighted by the findings of Cuellar et al 13 in which an increased MMP-3 to TIMP-1 ratio at a single time point is correlated with worse preoperative pain and poorer functional outcomes. We posit that an increased MMP-3 to TIMP-1 ratio likely represents a molecular environment primed for cellular degeneration rather than remodeling, which may compromise the likelihood of postoperative healing, tendon autograft or allograft ligamentization, and chondrocyte remodeling. 24 Therefore, this study would suggest that an earlier intervention is associated with an intra-articular molecular environment more conducive to improved outcomes, but future studies expanding on the data reported here with consistent results are warranted to strengthen this hypothesis.
Taken altogether, synovial fluid analysis suggests that the concentrations of growth factors associated with healing increase in the weeks after an ACL injury, while the concentrations of inflammatory cytokines and chemokines decrease. This finding contributes to the ongoing debate about the optimal timing for ACL reconstruction by indicating that a 1-month delay in surgery is associated with a molecular environment that is potentially more conductive to postoperative healing.
Limitations
This study provides insight into changes in the intra-articular environment during the short-term period after an injury, but this is only a small piece of the inflammatory process after an acute ACL rupture. Given that many cross-sectional studies have evaluated these cytokines at different postoperative time points, there are few studies that have prospectively followed a cohort from an injury to long-term outcomes, and further longitudinal evaluations of synovial fluid biomarkers are warranted.1,20,27 Furthermore, this study followed patients with an acute ACL rupture but did not compare changes in the biomarker profile over time to a control group. It is possible that there are natural fluctuations in intra-articular proinflammatory and anti-inflammatory molecules without the presence of joint injury. In addition, patients may have taken nonsteroidal anti-inflammatory drugs or other anti-inflammatory medication before their initial presentation that may have affected knee inflammation. This may theoretically alter the synovial fluid cytokine profile between the time points assessed.
Our study also was limited to an analysis of biomarkers at 2 time points: preoperatively and intraoperatively. While it is possible that some biomarkers may rapidly fluctuate and their changes may have been missed based on when our samples were collected, this is unlikely from the findings of the (albeit limited) literature published on temporal trends in synovial fluid markers of an ACL injury. In a subanalysis of Multicenter Orthopaedic Outcome Network Early-Anti-inflammatory Treatment in Patients with Acute ACL Tear and Painful Effusions trial data that assessed synovial fluid biomarkers at 4 days, 11 days, and 5 weeks after an ACL injury, there were no markers that peaked and decreased or hit a nadir and increased; all markers either consistently increased or decreased over time. 30 Notably, this trial randomized patients to receive an intra-articular corticosteroid injection, which likely affected synovial fluid cytokine levels in their experimental group.
Several other factors may affect a patient’s inflammatory cytokine profile, including but not limited to alcohol, smoking, obesity, illicit drug use, diet, stress and sleep cycles, and recent illnesses. These factors have a demonstrated effect on serum cytokines, but there are limited data demonstrating their effect on synovial fluid cytokines. In terms of potential confounders affecting the intra-articular inflammatory state, we chose to evaluate only the effect of concomitant meniscal injuries, a known contributor to synovial fluid cytokine concentrations. 11
This study was also limited to a predetermined list of biomarkers chosen based on previous studies with similar methodologies.11,12,27 Other synovial fluid biomarkers have been implicated in intra-articular inflammation and healing, including aggrecan (a proteoglycan that allows cartilage to withstand compressive forces), 45 cartilage oligomeric matrix protein (a known biomarker of cartilage breakdown), 37 ghrelin (a known chondrocyte growth factor), 52 IL-8 and IL-10 (other cytokines known to vary after ACL reconstruction), 6 and fibronectin (an extracellular matrix protein associated with cartilage degradation). 9 Last, this study may only comment on the change in the concentration of these synovial fluid biomarkers. To date, no study has assessed any minimal clinically important difference in intra-articular biomarker levels. Future studies should identify the degree of change in cytokine expression that correlates with a meaningful difference in patient outcomes.
Conclusion
This study demonstrates the ongoing alterations in the intra-articular microenvironment during the initial inflammatory response in the acute postinjury period. We identified 6 synovial fluid cytokines that significantly decreased (IL-6, MIP-1β, MCP-1, IL-1Ra, TIMP-1, VEGF) and 2 that significantly increased (bFGF, RANTES) between the first clinical presentation shortly after the injury and the time of surgery 1 month later. These findings could help identify the optimal molecular environment for the timing of ACL reconstruction, which may mitigate negative surgical outcomes and PTOA.
Footnotes
Submitted November 15, 2020; accepted August 30, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported through a gift from the Bady Foundation. E.J.S. has received consulting fees from Smith & Nephew, Arthrex, Vericel, the Joint Restoration Foundation, Fidia Pharma, Gotham Surgical Solutions, Horizon Therapeutics, Flexion Therapeutics, and Organogenesis and hospitality payments from Liberty Surgical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.