
Abstract
Background:
The relationship between posterior capsule adaptations and soft tissue glenohumeral internal rotation deficit (GIRD) in healthy pitchers remains unclear.
Purpose/Hypothesis:
This study aimed to identify if posterior capsule thickness (PCT) was associated with soft tissue GIRD in healthy pitchers. We hypothesized that there would be a positive relationship between soft tissue GIRD and PCT in the dominant arm, no relationship between soft tissue GIRD and PCT in the nondominant arm, and a strong positive relationship between soft tissue GIRD and the bilateral difference in PCT (posterior capsule hypertrophy [PCH]).
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A total of 45 healthy collegiate and professional pitchers were included. Glenohumeral internal rotation and external rotation range of motion, humeral retroversion, and PCT were measured bilaterally. PCT was determined for unilateral posterior capsule measurements, and PCH of the throwing shoulder was calculated as the bilateral difference in PCT. Soft tissue GIRD was calculated as the sum of clinical GIRD and the bilateral difference in humeral retroversion. Pearson correlation coefficients were determined to evaluate the relationships between dominant arm PCT, nondominant arm PCT, and PCH and soft tissue GIRD.
Results:
Pearson correlations showed that both dominant arm PCT (R = −0.13; P = .378) and nondominant arm PCT (R = 0.21; P = .165) were not related to soft tissue GIRD. However, Pearson correlations did show that the amount of PCH was moderately related to soft tissue GIRD (R = 0.40; P = .007). Therefore, as the posterior capsule hypertrophied, soft tissue GIRD moderately increased.
Conclusion:
Increased PCH was associated with an increase in soft tissue GIRD in healthy pitchers. If PCT measurements are feasible, clinicians should consider performing bilateral ultrasound assessments to isolate posterior capsule adaptations (ie, PCH). This will allow clinicians to identify pitchers with potentially maladaptive structural adaptations and optimize management strategies throughout the season to counteract them.
Baseball pitchers generate tremendous forces and torques at the glenohumeral joint throughout the acceleration and deceleration phases of pitching. 12 For example, internal rotation (IR) velocity of the shoulder joint has been shown to reach 7000 deg/s and is the fastest recorded motion of the human body. 9 Distraction forces have been reported to reach 1090 N and, combined with the large repetition involved with pitching, can lead to clinical shoulder adaptations. 12 The most commonly observed clinical adaptation at the glenohumeral joint in pitchers is rotational range of motion (ROM). Overhead throwing often causes a decrease in glenohumeral IR and an increase in glenohumeral external rotation (ER) in the dominant arm compared with the nondominant arm.4,15,25,31,33 The difference in ROM between the pitching and nonpitching arms, or the bilateral difference, has been defined as glenohumeral internal rotation deficit (GIRD) and ER gain. 2 GIRD has been associated with overuse injuries in overhead athletes,36,37 possibly caused by tightening of the posterior rotator cuff and/or thickening of the posterior capsule.
One clinical challenge when measuring GIRD is that it can be misinterpreted because of the combined effects of 3 potential tissue adaptations: humeral retroversion (HR), posterior capsule thickness (PCT), and/or posterior rotator cuff tightness.5,16,18,20,29,33 HR describes the bony torsion (increased ER ROM) that occurs in the humeri of baseball players in the dominant arm. At birth, the humeri are in large amounts of retroversion and, throughout normal development, slowly become more anteverted (increased IR and decreased ER ROM). 10 However, it is possible that throwing halts this normal progression, leaving the dominant humeri in a more retroverted position compared with the nondominant arm. 26 This bony adaptation can cause a shift in the arc of motion into more net ER and less IR in the dominant arm.22,35 However, it is still unclear what portion of clinical GIRD is caused by HR and/or soft tissue restrictions. To accurately isolate soft tissue adaptations at the glenohumeral joint, a previous study suggested measuring and subtracting the bony contribution (ie, HR) from clinical GIRD. 23 This value is then reported as soft tissue GIRD, which isolates the contribution of posterior shoulder tightness. 23
Posterior shoulder tightness can represent tightness of the posterior rotator cuff and/or thickness/tightness of the posterior capsule.13,14,16-18,22,28,30 Unfortunately, no methodology exists to isolate and accurately measure posterior rotator cuff tightness; therefore, an assessment of this specific tissue adaptation is currently not available. Fortunately, PCT has been previously assessed with the use of diagnostic ultrasound and elastography, demonstrating validity and reliability.23,27 PCT is thought to develop after posterior rotator cuff fatigue when the majority of the deceleration force is no longer absorbed by the posterior rotator cuff but instead placed on the capsule at the end of ROM. 3 The external rotators of the rotator cuff, along with the scapular stabilizing muscles, operate as dynamic stabilizers; however, if the dynamic stabilizers cannot efficiently dissipate these eccentric forces, the surrounding posterior capsule, serving as a static stabilizer, may be responsible for absorbing the residual force. 3 According to Davis’s law, the capsule may begin to adapt and hypertrophy because of repetitive loading. 8 In fact, it has been demonstrated that the dominant arm of baseball players has a thicker and stiffer posterior capsule compared with the non-dominant arm.27,29
In addition, players with increased HR were found to have a thicker posterior capsule likely because of having less IR ROM to decelerate the shoulder. 30 As the capsule hypertrophies, it will likely increase its ability to absorb energy and resist distraction, but kinematics of the glenohumeral joint and scapulothoracic articulation has been shown to be negatively affected.6,17 For example, posterior capsule tightness has been shown to force the humeral head posteriorly and superiorly during the late cocking phase. 6 Also, a tight posterior capsule may cause excessive scapular IR and protraction. 17 Previous research on collegiate baseball players has found that an increase in PCT is related to increased clinical GIRD27,29; however, no study has evaluated the relationship between PCT and soft tissue GIRD. Therefore, this study aimed to identify the degree to which PCT contributes to soft tissue GIRD in healthy pitchers. We hypothesized that there would be a direct correlation between PCT and soft tissue GIRD in the dominant arm, no relationship between PCT and soft tissue GIRD in the nondominant arm, and a strong positive relationship between soft tissue GIRD and the bilateral difference in PCT (posterior capsule hypertrophy [PCH]).
Methods
Participants and Study Design
This single-group posttest-only study was conducted with institutional review board approval and participants provided informed consent. A total of 45 collegiate and professional Minor League Baseball pitchers were evaluated. To minimize the acute effects of throwing, data were collected before the start of the competitive season: collegiate pitchers were assessed before the National Collegiate Athletic Association Division I season, while Minor League Baseball players were assessed at the beginning of spring training. Participants were only included if (1) their primary position was pitcher, (2) they had no current injury, and (3) they had not undergone surgery in the past 6 months. Glenohumeral IR and ER, HR, and PCT were measured bilaterally for each participant by a single investigator (S.J.T.) with over a decade of musculoskeletal ultrasound imaging experience. The investigator was blinded to the arm dominance of players.
Glenohumeral IR and ER
Glenohumeral IR and ER were determined utilizing a previously validated and reliable method.1,32 Glenohumeral IR and ER were measured using a digital inclinometer (Saunders Group), with the participant lying supine and the arm at 90° of shoulder abduction in the frontal plane. Glenohumeral motion was isolated by stabilizing the scapula manually and rotating the arm to maximum IR and ER. IR and ER were recorded by placing the digital inclinometer on the ulnar side of the forearm. Each variable was measured 3 times and averaged. Clinical GIRD and soft tissue GIRD were then calculated using the equations in Table 1.
Equations for Calculating Clinical GIRD, Bilateral Difference in HR, Soft Tissue GIRD, and Bilateral Difference in PCT a
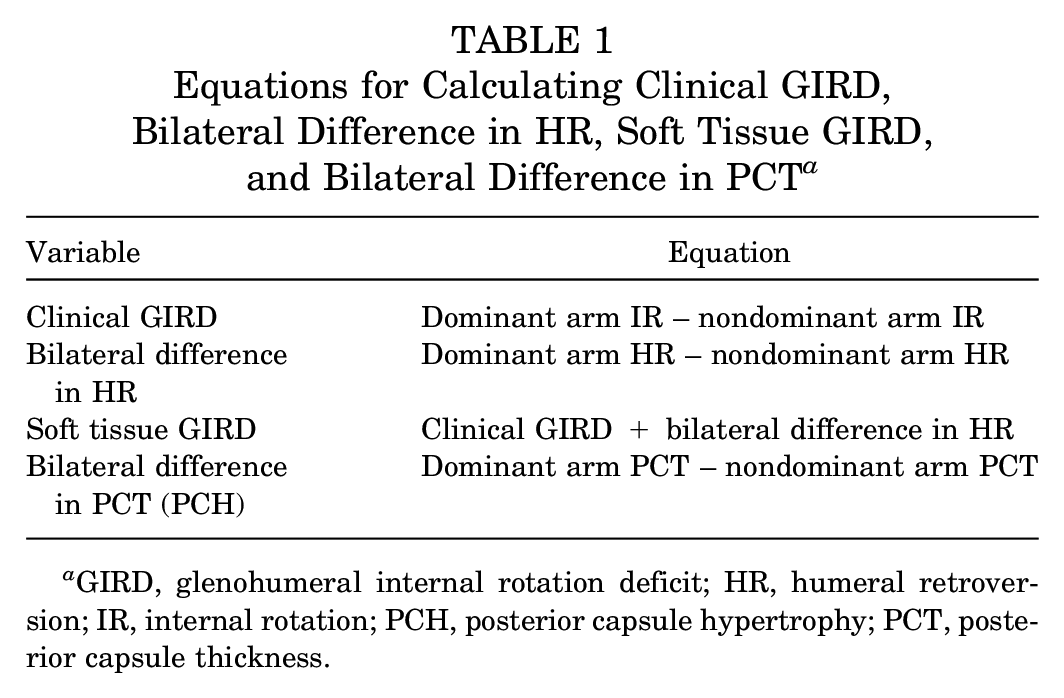
GIRD, glenohumeral internal rotation deficit; HR, humeral retroversion; IR, internal rotation; PCH, posterior capsule hypertrophy; PCT, posterior capsule thickness.
Humeral Retroversion
HR was measured using a previously described and validated ultrasound technique.19,30 Participants lay supine with the arm at 90° of shoulder abduction and elbow flexion. A 15-MHz linear transducer (SonoSite Titan diagnostic ultrasound scanner; Fujifilm SonoSite) was positioned in the frontal plane, perpendicular to the participant’s long axis of the humerus on the anterior shoulder. The humerus was then rotated so that the bicipital groove was centered on the ultrasound image. The ultrasound probe was then slightly moved until a line connecting the lesser and greater tubercles of the humerus lined up with the horizontal grid on the ultrasound screen. When the ultrasound probe was in place, the assisting researcher measured the forearm inclination angle, representing HR, by placing the digital inclinometer on the ulnar side of the forearm. HR was measured 3 times and averaged. The bilateral difference in HR was then calculated using the equation in Table 1. A positive bilateral difference in HR indicates that the humerus of the throwing arm is in a more retroverted (ER) position compared to the nonthrowing arm.
Posterior Capsule Thickness
PCT was measured using a previously described and validated ultrasound technique of the posterior shoulder.29,30 Construct validity and criterion-related validity of PCT measurements on ultrasound have previously been established using a 10-MHz transducer. 29 Intratester reliability of ultrasound has also been previously established using a 10-MHz transducer with an SEM of 0.02 cm. 29
To enable visualization of the posterior capsule, participants sat upright in a chair and rested their forearm on their thigh. A 15-MHz linear transducer (SonoSite Titan diagnostic ultrasound scanner) was positioned to visualize the humeral head, glenoid labrum, and rotator cuff. The posterior capsule was identified as the tissue immediately lateral to the tip of the labrum that was between the humeral head and rotator cuff (Figure 1). A standard B-mode image was used to measure PCT on ImageJ software (National Institutes of Health). PCT was measured 3 times and averaged. PCH was then calculated using the equation in Table 1.
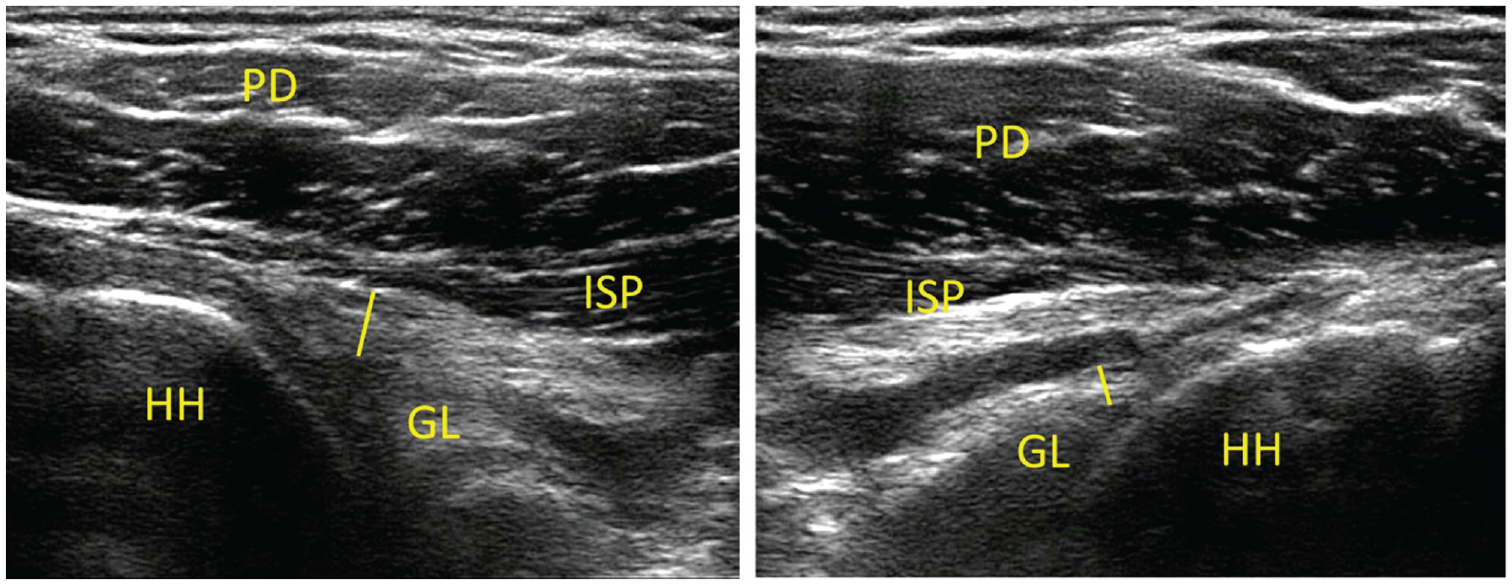
Ultrasound images of dominant arm (left image) and nondominant arm (right image) posterior capsule thickness (line), showing noticeable posterior capsule hypertrophy in the dominant arm. GL, glenoid labrum; HH, humeral head; ISP, infraspinatus; PD, posterior deltoid.
Statistical Analysis
Variables were calculated using the equations presented in Table 1. Pearson correlation coefficients were determined to evaluate the relationship between PCT (dominant, nondominant, and bilateral difference) and soft tissue GIRD. Statistical significance was set at .05. All statistical analyses were conducted using SPSS Version 25 (IBM Corp).
Results
The 45 included pitchers had a mean age of 21.6 ± 3.2 years, with a mean height of 189.0 ± 5.2 cm and a mean weight of 93.8 ± 8.5 kg. Of these pitchers, 14 (31%) had a previous upper extremity injury, with the only shoulder injuries in 2 pitchers with biceps tendinitis and 1 pitcher with shoulder soreness. Also, 8 (18%) had undergone previous upper extremity surgery, with no pitchers having undergone previous surgery of the shoulder. Both pitchers who had experienced biceps tendinitis were treated nonoperatively. Dominant and nondominant arm HR, IR and ER ROM, and PCT are shown in Table 2.
Humeral Retroversion, Internal Rotation and External Rotation ROM, and Posterior Capsule Thickness a
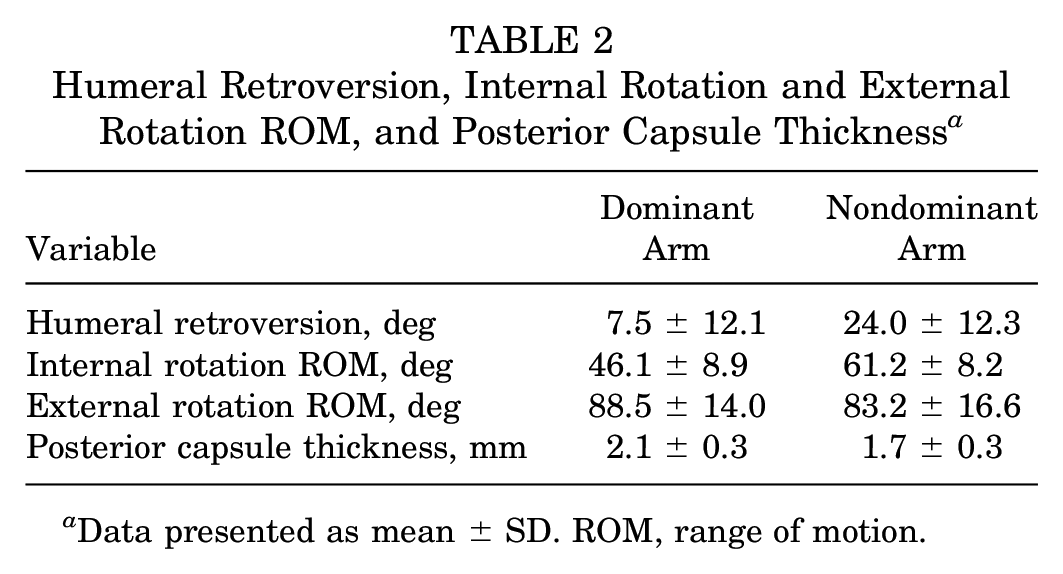
Data presented as mean ± SD. ROM, range of motion.
Pearson correlations showed that both dominant arm PCT (R = −0.13; P = .378) and nondominant arm PCT (R = 0.21; P = .165) were not related to soft tissue GIRD (Figures 2 and 3). However, Pearson correlations did show that the amount of PCH was moderately related to soft tissue GIRD (R = 0.40; P = .007) (Figure 4). Therefore, as the posterior capsule hypertrophied, soft tissue GIRD moderately increased.
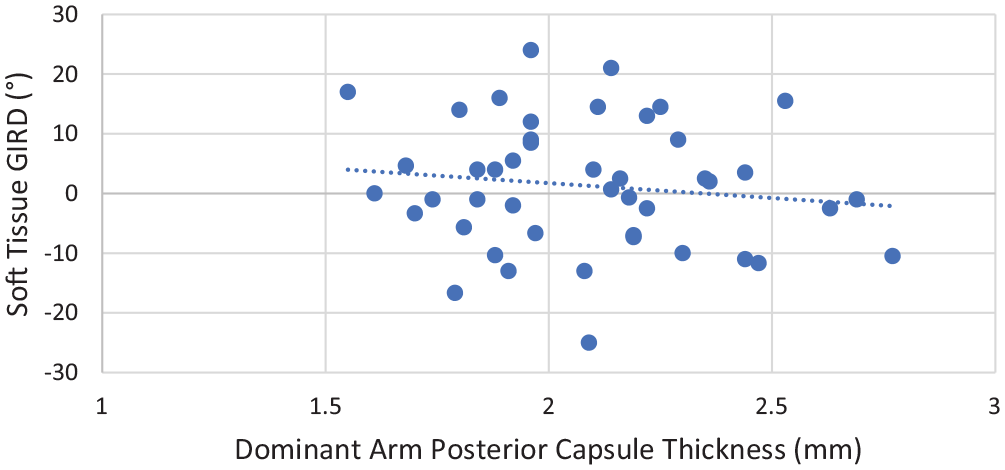
Relationship between dominant arm posterior capsule thickness and soft tissue glenohumeral internal rotation deficit (GIRD) (R = −0.13; P = .378).
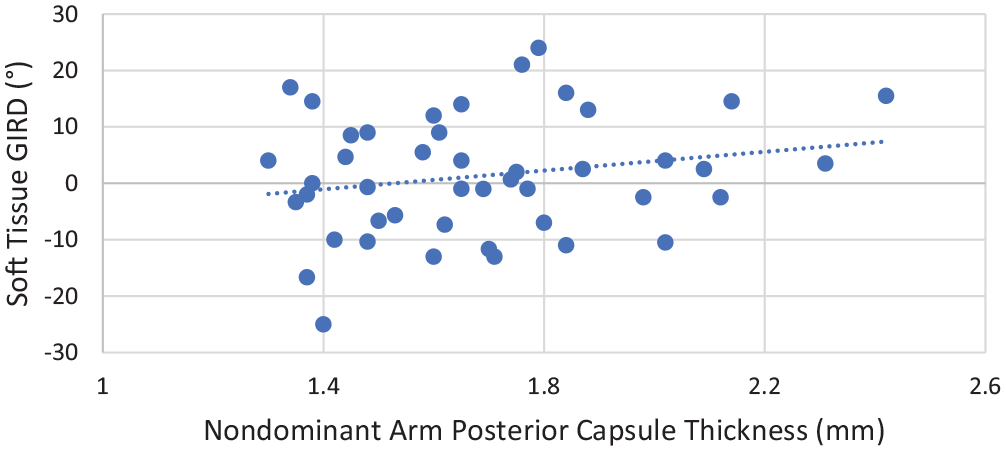
Relationship between nondominant arm posterior capsule thickness and soft tissue glenohumeral internal rotation deficit (GIRD) (R = 0.21; P = .165).
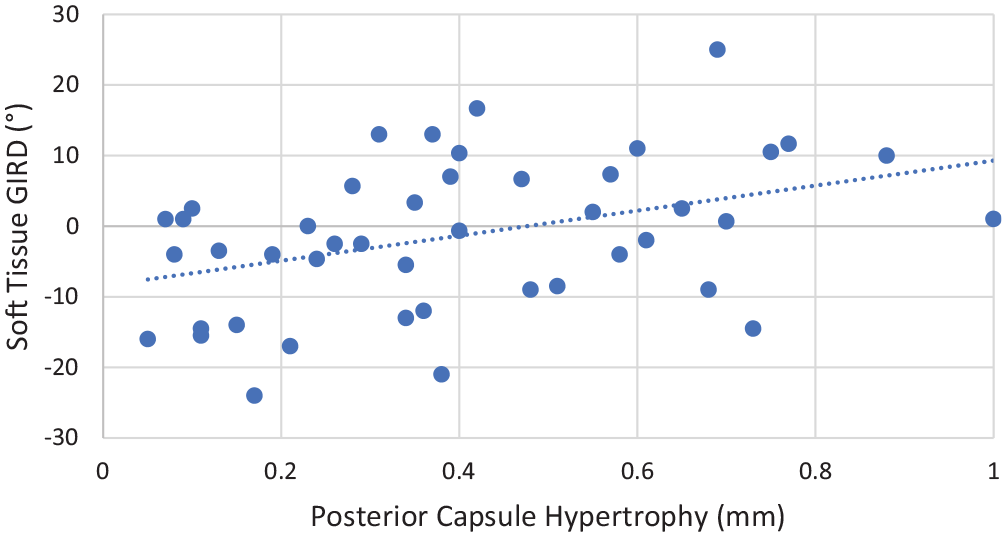
Relationship between posterior capsule hypertrophy (bilateral difference in posterior capsule thickness) and soft tissue glenohumeral internal rotation deficit (GIRD) (R = 0.40; P = .007).
Discussion
This study aimed to identify the relationship between PCT and soft tissue GIRD in healthy pitchers. Soft tissue GIRD accounts for the effects of bone (HR), thereby isolating the contribution that the surrounding soft tissue has on glenohumeral ROM. We found that both dominant and nondominant arm PCT were not related to soft tissue GIRD. However, the amount of PCH (bilateral difference in PCT), which controls for potential confounders and isolates an important structural adaptation caused by the stress of pitching, was positively correlated with soft tissue GIRD. This demonstrates that an increase in PCH is in fact associated with an increase in soft tissue GIRD. These findings together may showcase the importance of using the pitcher’s nonthrowing arm as an internal control to evaluate the chronic adaptations of the throwing shoulder.
Our hypothesis that PCT in the nondominant arm would not be related to soft tissue GIRD was confirmed. Unlike the dominant arm, the nondominant arm does not experience large torques at the glenohumeral joint during the throwing motion. Without these rotational forces to cause a hypertrophic response in the nonthrowing arm, the posterior capsule is not expected to adapt.
Our hypothesis that dominant arm PCT would be related to soft tissue GIRD was not supported. While cadaveric studies have found a negative correlation between posterior capsule contracture and IR,7,11 these studies were comparing outcomes before and after posterior capsule plication. Posterior capsule plication does not accurately reflect adaptations in the pitching shoulder because only tissue length is adjusted while tissue mechanical properties are not changed. 7 In vivo studies have also found a negative correlation between PCT and IR ROM in collegiate baseball players27,29; however, as stated previously, IR ROM may likely be composed of 3 possible tissue adaptations: HR, PCT, and/or posterior rotator cuff tightness. By measuring and subtracting HR from clinical GIRD to obtain soft tissue GIRD, the ROM contribution of posterior shoulder tightness (PCT and/or posterior rotator cuff tightness) is isolated. Although we were unable to isolate the ROM contribution of the posterior capsule, we did isolate PCT and determine the relative contribution to soft tissue GIRD. The lack of significance when examining the relationship between dominant arm PCT and soft tissue GIRD may have been caused by soft tissue GIRD representing a bilateral comparison while dominant arm PCT represents a unilateral isolated measure. Therefore, our results suggest that a bilateral ultrasound assessment may be more appropriate clinically to identify pitchers with posterior capsule adaptations.
Finally, we hypothesized that the amount of PCH would be positively related to soft tissue GIRD. Our hypothesis was supported, as a positive, moderate relationship (R = 0.40) was observed between PCH and soft tissue GIRD. As previously stated, if PCT is only evaluated in the dominant arm, many confounding variables are present that limit the clinical applicability of this measure. However, by using the nondominant arm as each pitcher’s internal control, we eliminated the confounding factors and isolated PCT adaptations related to the stress of throwing.
Other researcher and clinicians have suggested that PCH is initiated after repetitive fatigue and overuse.2,3 Interestingly, fatigue has previously been demonstrated to increase the risk of injuries. A previous study utilized a survey of 140 adolescent (aged 14-20 years) baseball players and found that pitching while fatigued leads to an astonishing 36 times increase in the injury risk. 21 When the posterior rotator cuff is fatigued during pitching, the posterior capsule will assume an increased responsibility for dissipating the deceleration forces at the end of IR ROM. 3 As this occurs chronically throughout the season and/or multiple seasons, the posterior capsule will undergo hypertrophy due to increased and repetitive tissue stress. 2 In fact, several studies have found a thicker 29 and stiffer 27 posterior capsule in the dominant arm of collegiate baseball players. These previous studies ultimately demonstrated that there was a significant bilateral difference in PCT, while the current study went further, examining how the amount of PCH relates to soft tissue GIRD. This study showed that focusing on ROM alone is suboptimal and that bilateral HR and PCT should be evaluated as well. If significant PCH is identified, clinicians can implement protocols to increase tissue extensibility such as low-load long-duration stretching or joint mobilization that targets the posterior capsule.24,34 This will also allow clinicians to optimize management strategies throughout the season to prevent injuries or track the effectiveness of a treatment strategy.
Limitations
This study is not without limitations. Only collegiate and professional pitchers were included in this study; therefore, our conclusions may not apply to youth pitchers or position players. Also, this study examined healthy asymptomatic pitchers, with only 3 players having a history of shoulder injuries (treated nonoperatively); thus, the relationship between PCT and shoulder injuries could not be determined. In addition, we did not isolate the effects of posterior rotator cuff tightness, which can also affect IR. Finally, this study was performed during spring training, so adaptations that occur throughout the season could not be evaluated. A longitudinal study should be performed to determine if these adaptations develop throughout a competitive season.
Conclusion
Increased PCH was associated with an increase in soft tissue GIRD in healthy pitchers. If PCT measurements are feasible, clinicians should consider performing bilateral ultrasound assessments to isolate posterior capsule adaptations (ie, PCH). This will allow clinicians to identify pitchers with potentially maladaptive structural adaptations and optimize management strategies throughout the season to counteract them.
Footnotes
Submitted May 20, 2021; accepted September 14, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.D.K. has received consulting fees from Flexion Therapeutics and publishing royalties from SLACK and Springer. S.J.T. has received publishing royalties from Human Kinetics. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.