
Abstract
Background:
There are few reports on the return to sports after complex patellar-stabilizing surgery.
Purposes:
To evaluate patients’ ability to return to sports and to investigate the extent to which the preoperative level of sports participation influences sports activity after deepening trochleoplasty (TP) and concomitant patellar-stabilizing procedures.
Study Design:
Case series; Level of evidence, 4.
Methods:
Between April 2015 and April 2019, 144 patellar-stabilizing procedures, including deepening TP and medial patellofemoral ligament reconstruction or medial reefing with and without concomitant realignment procedures, were carried out in 142 patients. The Banff Patellofemoral Instability Instrument 2.0 (BPII 2.0) and the Tegner activity score were used to assess patients’ quality of life and sports activity level. In addition, a numerical analog scale was used to evaluate patellofemoral pain intensity during rest and activity and subjective knee joint function.
Results:
Outcomes were available for 111 patients (112 knees) (male/female, 77/34; mean age, 23.4 ± 7.8 years), yielding a 77.7% follow-up rate at a mean of 39.2 ± 9.9 months (range, 24-48 months). Two-thirds of the patients returned to their preoperative level of activity or higher, but their Tegner scores did not change significantly (4.5 ± 2.4 vs 4.7 ± 1.6; P = .365). Low-level athletes (preoperative Tegner score 0-4) participated at a higher level of sports activity (2.7 ± 1.4 to 4.1 ± 1.2; P < .0001), whereas higher-level athletes (preoperative Tegner score 5-10) participated at a lower level (6.8 ± 1.3 to 5.5 ± 1.7; P < .0001). The likelihood of returning to the preoperative activity level (Tegner score) was significantly higher in the low-level activity group than in the high-level activity group (P = .0001; 95% CI, 4.055-27.05; odds ratio, 10.47). All of the patient-reported outcome measures improved postoperatively, independent of the patients’ age, sex, and body mass index.
Conclusion:
Patients undergoing deepening TP and medial soft tissue stabilization with or without concomitant realignment surgery for complex patellar instability can expect good clinical results and a high rate of return to sports participation, with two-thirds of patients returning to their preoperative Tegner-level of activity or higher. However, higher-level athletes should be informed that their likelihood of returning to sports at the preoperative level or full participation at a competitive level is reduced.
The correction of the dysplastic trochlea with deepening trochleoplasty (TP) is an established operative procedure performed to treat lateral patellar dislocations in patients in whom severe trochlear dysplasia has been identified as the most relevant factor of patellar instability.5,22,24,38 TP has been demonstrated to yield good clinical outcomes, low redislocation rates, and significant improvements in clinical outcome scores, although the reoperation rate is significant, ranging between 14% and 27%.8,22,24 Based on the individual’s risk factor profile, TP is often performed concurrently with medial patellofemoral ligament reconstruction (MPFLR) and, if deemed necessary, with other bony realignment procedures to restore patellar stability and patellofemoral functionality. 38
Previous studies evaluating TP procedures have focused on patellar stability and improvement in patient-reported outcomes from pre- to postoperatively. However, there are few reports on the return to sports or activities. Although a systematic review concluded that patients’ activity levels improve after TP, 12 the results are inconsistent within the literature, as some studies report that the level of sports activity remained limited or even decreased after TP.25,34
Therefore, the primary purposes of this study were (1) to evaluate patients’ ability to return to sports after complex patellar-stabilizing procedures, including deepening TP and patellar soft tissue stabilizing with or without additional bony realignment procedures, and (2) to investigate whether the preoperative level of sports participation influences postoperative sports performance. The secondary purpose was to evaluate patient-reported outcome measures after complex patellar-stabilizing surgery. The hypotheses were that (1) most patients are able to return to at least their preoperative level of sports activity and (2) a higher preoperative level of physical activity has a positive effect on the return to sports after surgery.
Methods
This study is a retrospective analysis of a longitudinally maintained database that received approval from the ethics committee in Baden-Württemberg, Germany (F-2019-070). Between April 2015 and April 2019, 144 complex patellar-stabilizing procedures in 142 patients were carried out according to the “a la carte” treatment concept of lateral patellar instability. To be included, patients had to have undergone a deepening TP (inclusion criterion) with or without MPFLR or medial reefing, and with and without concomitant realignment procedures (tibial tuberosity osteotomy [TTO], varization/derotational osteotomy). Patients who underwent patellar-stabilizing or knee extensor apparatus realignment procedures that did not include a TP (ie, isolated MPFLR, isolated TTO, or combinations of MPFLR, TTO, and/or femoral osteotomy) were excluded. In addition, patients who underwent realignment surgery for patellofemoral pain without objective findings of lateral patellar instability and those with previous knee ligament surgery (eg, anterior cruciate ligament or posterior cruciate ligament reconstruction) were excluded.
Demographic factors (age, sex, body mass index [BMI]), clinical data, and pathoanatomic risk factors were assessed in all patients at the time of the initial outpatient consultation. The physical examination included an evaluation of the long axis of the leg in both the standing and the supine positions, measurement of knee joint range of motion (using a goniometer), the Reversed Dynamic Patellar Apprehension Test (ReDPAT), 39 and evaluation of the J-sign (graded I-III according to Zhang et al 37 ). In addition, the patients were screened for femoral and tibial torsional deformities according to the methods described by Staheli et al 31 and Stuberg et al. 32 Patients with signs of increased femoral and/or tibial torsion underwent additional torsional magnetic resonance imaging (MRI) investigations. 4
MRI data and routine radiographs (standing long-leg radiograph and true-lateral view radiograph) of the knee joint were obtained for all patients and were evaluated to determine the severity of trochlear dysplasia (absent, low grade [Dejour type A], or high grade [Dejour types B-D]), 10 patellar height (Caton-Deschamps index), tibial tuberosity–trochlear groove distance, tibial tuberosity–posterior cruciate ligament distance, and varus-valgus alignment. 13 A Caton-Deschamps index ≥1.2 was defined as elevated, 9 a tibial tuberosity–trochlear groove distance >16 mm was defined as elevated, 3 and a tibial tuberosity–posterior cruciate ligament distance >24 mm was defined as elevated. 29
Deepening TP was considered in patients with Dejour type B or D trochlear dysplasia combined with a positive J-sign (grades II-III) 37 and a ReDPAT result ≥50° 39 ; concomitant TTO was considered when the tibial tuberosity–trochlear groove distance exceeded 20 mm, when the tibial tuberosity–posterior cruciate ligament distance exceeded 24 mm, and/or when the Caton-Deschamps index was ≥1.3. Femoral derotational osteotomy or valgus correction osteotomy was considered when the degree of femoral antetorsion exceeded 25° and the degree of valgus deformity was ≥4°. 17 For varization/derotation osteotomy, the patients underwent a 2-stage procedure in which the osteotomy was performed first. TP and soft tissue procedures were performed 9 to 12 months later, in combination with the removal of the implant.
TP was carried out using the thin-flap technique described by von Knoch et al. 35 In brief, a lateral parapatellar arthrotomy was performed with the lateral retinaculum prepared in a Z-plasty fashion to enable its lengthening during wound closure as required. A thin flap of the cartilage-bone lamella was raised with chisels, starting superolaterally and extending distally to the notch. Then, the prominent trochlear bump was removed (asterisk in Figure 1A), and the trochlear groove was deepened, allowing the bottom of the newly created trochlear groove to become flush with the anterior cortex of the femur (asterisk in Figure 1, A and B).
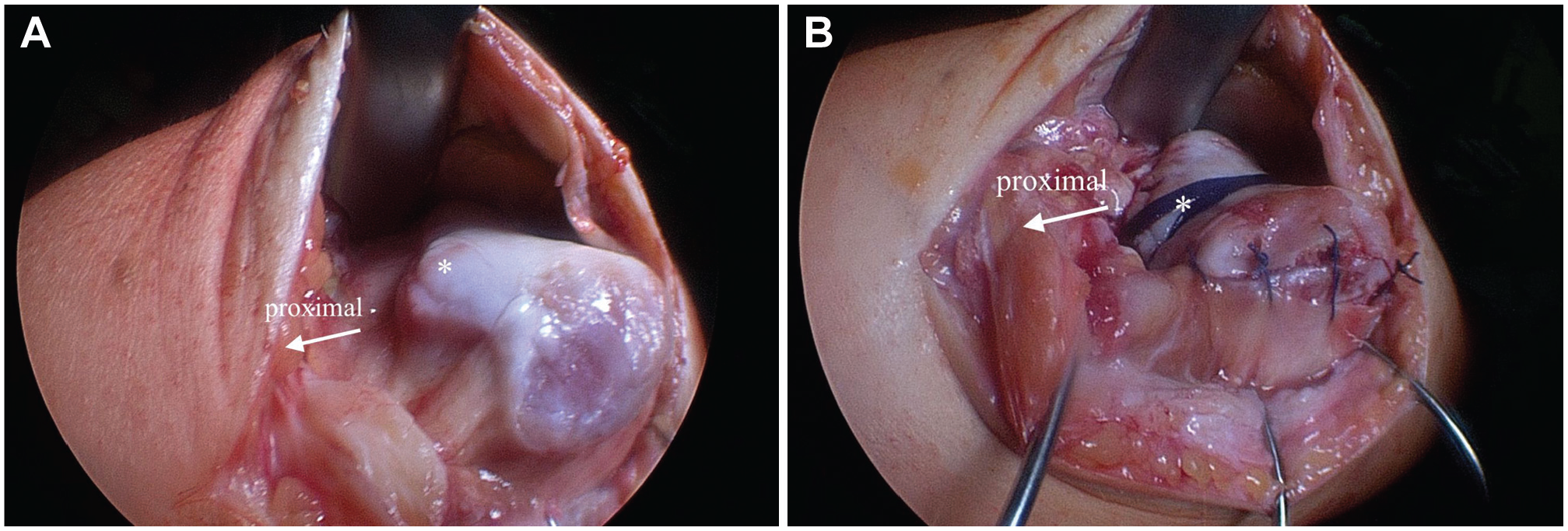
View of the trochlea after lateral parapatellar arthrotomy. The asterisk indicates the center of the trochlear groove (A) before and (B) after deepening trochleoplasty.
The flexible cartilage-bone flap was gently pressed into the new cavity and fixed centrally with a 3-mm strip of Vicryl tape (Ethicon) and 3.5-mm PushLock (Arthrex) anchors proximally and distally. If necessary, a second strip of Vicryl tape was used medially or laterally for additional fixation. The decision to perform additional MPFLR or medial reefing was made intraoperatively based on the patellar stability after the TP procedure and, if deemed necessary, after additional TTO.
After the TP procedure, all patients underwent the same postoperative rehabilitation protocol. Mobilization was initiated on the second day after the operation with active and passive exercises, including continuous passive motion as tolerated. Partial weightbearing was recommended for 3 to 4 weeks, and the transition to full weightbearing occurred afterward as tolerated. All patients were seen 6 and 12 weeks postoperatively, and every patient underwent physical therapy rehabilitation for a minimum of 3 months postoperatively. Patients with ongoing quadriceps atrophy, limited range of motion, effusion, or ongoing feelings of instability continued physical therapy for an additional 6 to 12 weeks. The patients were advised to return to activity approximately 4 to 6 months after the operation and to return to participation (Table 1) no earlier than 6 months postoperatively. In addition, the patients were instructed to perform the single-leg hop for distance test and the Star Excursion Balance Test as brief self-assessments of readiness to return to sports. However, these tests were not controlled, and the patients did not undergo functional testing before returning to sports. All operations were performed by the senior author (P.B.) of this study.
Criteria for Return to Sports a
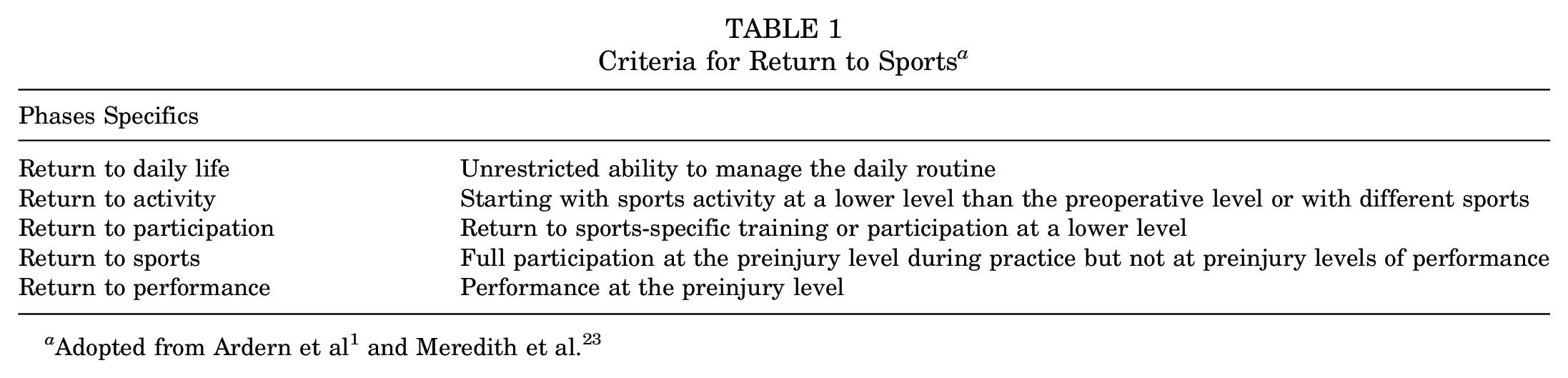
For the evaluations, the validated Banff Patellofemoral Instability Instrument 2.0 (BPII 2.0) 7 was used to assess patient-reported disease-specific quality of life, and the Tegner activity score 36 was used to assess the patients’ level of sports activity. In addition, a numerical analog scale (0-10 points) was used to evaluate the intensity of patellofemoral pain (0 = no pain; 10 = most severe pain) during rest and activity and to evaluate subjective knee joint function (0 = severely restricted; 10 = normal function). 38 All parameters were assessed preoperatively and at the final follow-up. The criteria for return to sports were adopted from Ardern et al 1 and Meredith et al 23 (Table 1). During the follow-up evaluation, the patients were asked to recall specific events during rehabilitation.
Statistical Analysis
Continuous data were assessed for normality and are presented as the mean ± SD (range). Categorical and dichotomous data are presented as frequencies. Contingency tables, the unpaired 2-tailed t test, the Mann-Whitney U test, and the Wilcoxon signed-rank test were used to assess the differences between the pre- and postoperative clinical data and between the low-level (preoperative Tegner score 0-4) and high-level (preoperative Tegner score 5-10) athlete subgroups. The effects of age and BMI on the BPII 2.0 score were assessed by linear regression. All analyses were performed using GraphPad Prism (Version 4; GraphPad Software). The level of significance was set at .05.
Results
Outcomes were available in 111 patients (112 knees), yielding a 77.7% follow-up rate at a mean of 39.2 ± 9.9 months (range, 24-48 months). There were 77 women and 34 men with a mean age of 23.4 ± 7.8 years (range, 11-52 years) and a mean BMI of 24.5 ± 4.6 (range, 17.8-43.0). Of the remaining 31 patients, 19 were lost to follow-up, and 12 refused to participate. The treatment procedures performed for the study group are listed in Table 2.
Distribution of Surgical Treatment Procedures Performed for the Study Group a
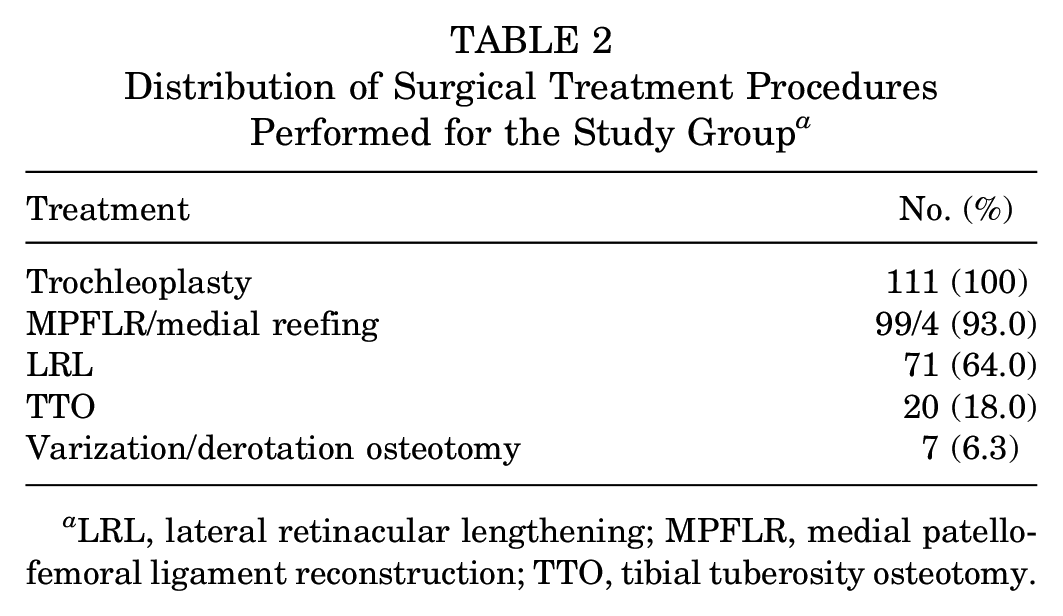
LRL, lateral retinacular lengthening; MPFLR, medial patellofemoral ligament reconstruction; TTO, tibial tuberosity osteotomy.
Overall, the BPII 2.0 score increased from 46.5 ± 21.3 (range, 3.0-96.1) points preoperatively to 80.4 ± 16.9 (range, 32-99.2) points postoperatively (P < .0001), and the subjective rating of knee joint function increased from 4.8 ± 1.9 (range, 0-9) preoperatively to 8.3 ± 1.5 (range, 3-10) postoperatively (P < .0001). The patellofemoral pain at rest and during activity improved from 3.5 ± 2.8 (range, 0-10) and 6.4 ± 2.2 (range, 0-10) to 1.1 ± 1.7 (range, 0-6) and to 2.4 ± 2.1 (range, 0-8), respectively (P < .0001; P < .0001).
Although nearly two-thirds of the patients returned to their preoperative Tegner level of activity or higher, the overall Tegner score did not change significantly (from 4.5 ± 2.4 [range, 0-9] preoperatively to 4.7 ± 1.6 [range, 1.5-9] postoperatively; P = .365). However, the low-level athletes (preoperative Tegner score 0-4) participated in a significantly higher level of sports activity after surgery (2.7 ± 1.4 to 4.1 ± 1.2; P < .0001), whereas the high-level athletes (preoperative Tegner score 5-10) participated in a significantly lower level of sports activity (the preoperative Tegner score was 6.8 ± 1.3, and the postoperative score was 5.5 ± 1.7; P < .0001). In addition, the likelihood of returning to the preoperative level of activity or a higher level was significantly greater in the low-level activity group than in the high-level activity group (P = .0001; 95% CI, 4.055-27.05; odds ratio, 10.47) (Table 3). The high-level athletes tended to experience greater fear of reinjury than the low-level athletes did (BPII 2.0 item No. 12: 67.9 ± 35.3 vs 77.2 ± 30.0; P = .064), but there were no differences in the postoperative BPII 2.0 scores or subjective rating of knee joint function between groups (Table 3).
Level of Sports Activity and Patient-Reported Outcome Measures Based on the Preoperative Tegner Score a
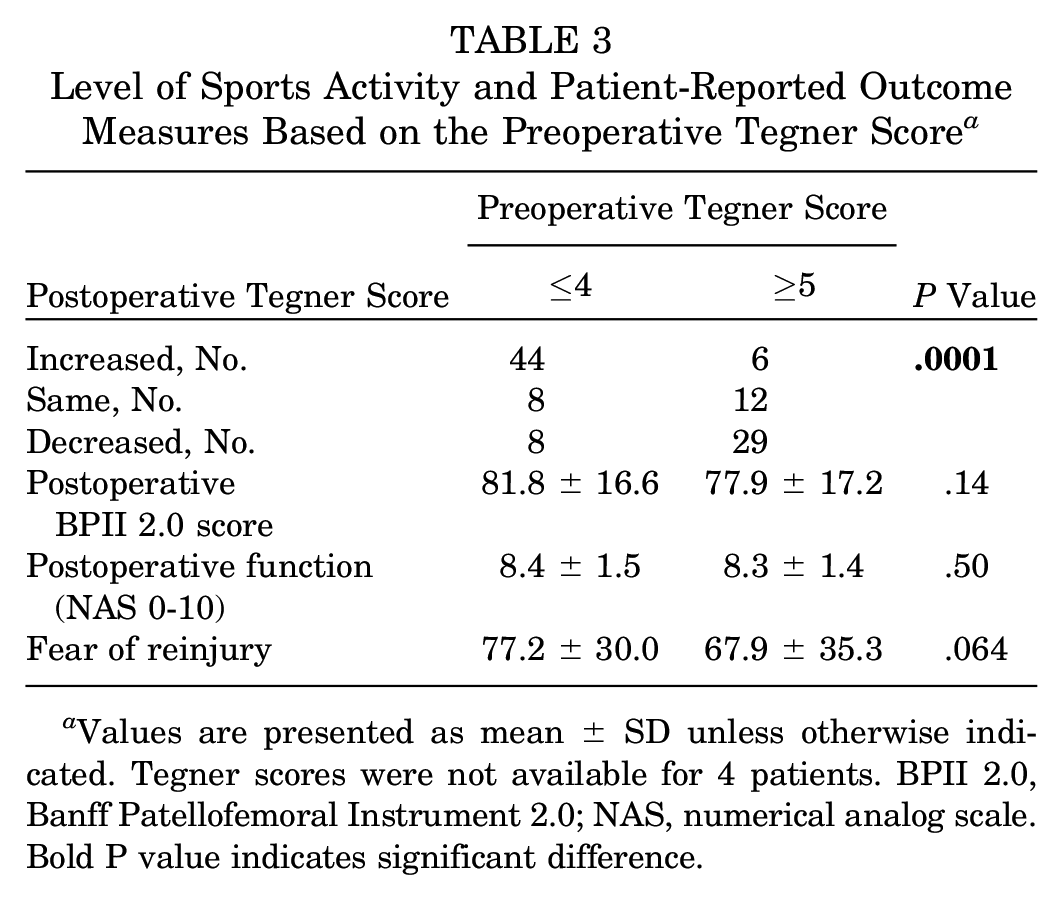
Values are presented as mean ± SD unless otherwise indicated. Tegner scores were not available for 4 patients. BPII 2.0, Banff Patellofemoral Instrument 2.0; NAS, numerical analog scale. Bold P value indicates significant difference.
Return to daily life was achieved by all patients after a mean of 4.5 ± 3.4 (range, 1-25) months. Return to activity and return to participation were achieved by 97% and 95% of patients after a mean of 7.7 ± 6.3 (range, 1-36) months and 12.6 ± 7.8 (range, 3-36) months, respectively. Return to sports and return to performance were achieved by 53% and 42% of patients after a mean of 10.8 ± 5.5 (range, 3-24) months and 13.8 ± 6.2 (range, 6-24) months, respectively (Figure 2).
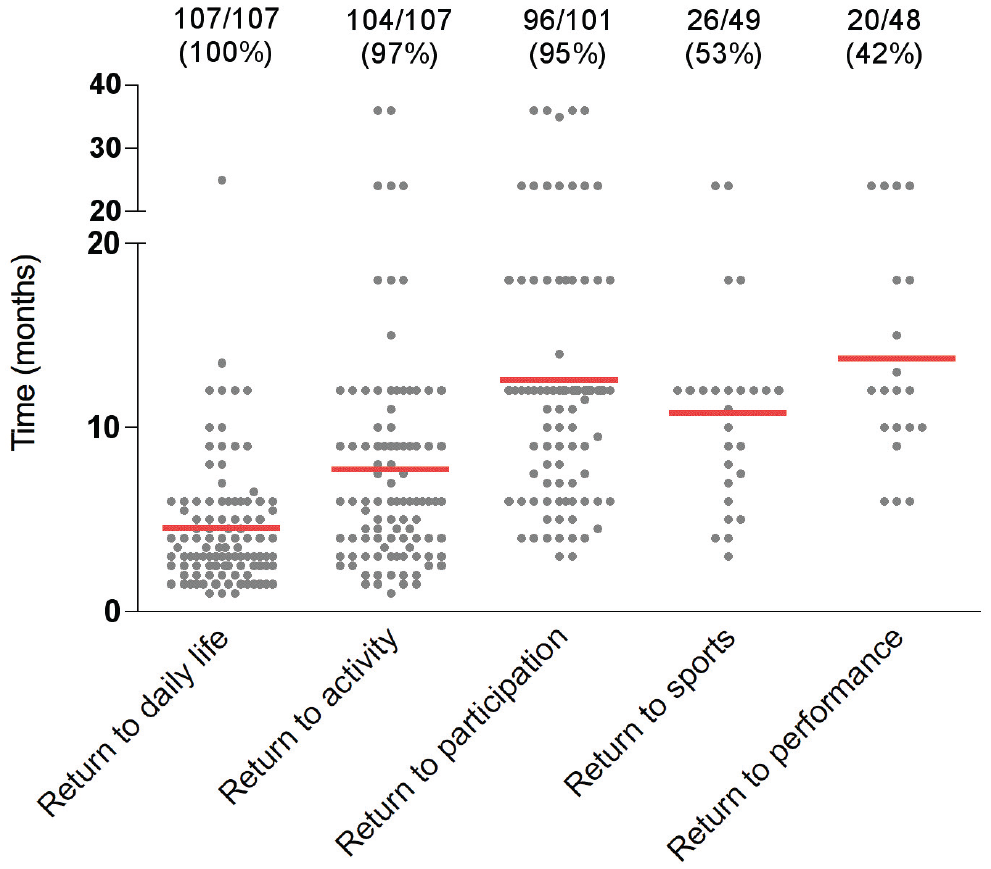
Patient rehabilitation continuum. Time course and number (%) of patients who regained different levels of sports activity during rehabilitation. The percentages were calculated with respect to the number of patients who participated at that level of activity before surgery.
Patellar redislocation/subluxation occurred in 3 (2.7%) patients. Of those, 2 patients required TTO distalization because of persistent patella alta, and 1 patient required additional MPFLR. The overall reoperation rate was 14.4% (16 patients). The major reasons for revision surgery were planned hardware removal in 6 (37.5%) and arthroscopic arthrolysis in 6 (37.5%) because of persistent knee joint flexion deficits (Table 4).
Type and Incidence of Revision Surgery a
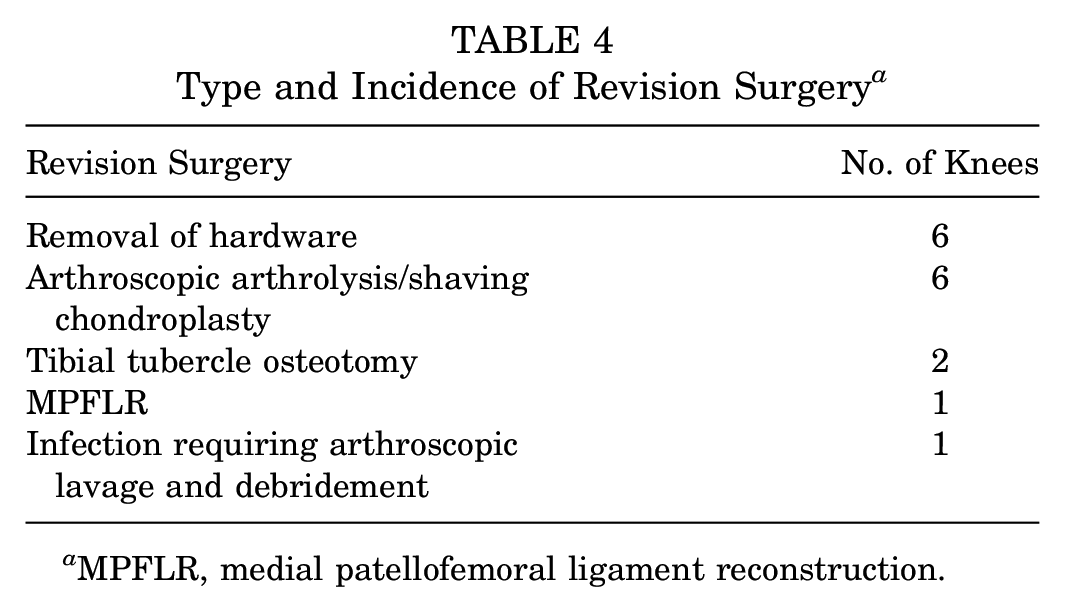
MPFLR, medial patellofemoral ligament reconstruction.
Age, sex, and BMI did not influence the postoperative BPII 2.0 score (age, r2 = 0.004, P = .48; sex, P = .86; BMI, r2 = 0.014, P = .21), although higher BMI values were significantly correlated with poorer BPII 2.0 scores before surgery (r2 = 0.04; P = .04).
Discussion
The primary purpose of this study was to assess patients’ ability to return to sports and to investigate the extent to which the preoperative level of sports participation influences patients’ postoperative return to activity. The results showed that approximately two-thirds of patients returned to their preoperative Tegner level of sports activity or higher. This finding, however, was most commonly observed in low-level athletes (preoperative Tegner score 0-4), as higher-level athletes (preoperative Tegner score 5-10) had a significantly lower level of sports activity postoperatively. However, the disease-specific patient-reported quality of life, subjective knee joint function, and patellofemoral pain improved significantly in both low- and high-level athletes, independent of whether they returned to sports activity at a lower level than preoperatively.
The biomechanical effect of trochlear dysplasia on patellofemoral instability has been confirmed by several studies, and the shape of the proximal trochlea has been identified to be the most important component of the total patellofemoral constraint11,33; moreover, numerous studies have shown that TP is clinically beneficial for recurrent patellar instability.5,6,12,22,24,38 The results are encouraging as TP is associated with a very low redislocation rate and complication rates that are comparable with those of other patellar-stabilizing procedures.12,19
Results regarding the return to sports after TP have been reported by several studies.8,22,25,26 This study provides additional information about the expected time course of rehabilitation and patients’ ability to return to sports considering their preoperative level of activity. Recently, Carstensen et al 8 reported that 85% of a group of 40 patients were able to participate in sports postoperatively. However, the patients were not stratified by their level of competition. In a large study of 90 patients (107 knees), McNamara et al 22 found that TP surgery improved patient participation in sports and exercise but did not lead to a significant improvement in sports activity at a competitive level. In their study, the Tegner score increased moderately, from 3.3 ± 2.7 preoperatively to 4.3 ± 2.1 postoperatively. Similarly, Nelitz et al 25 reported that 17 of 23 (74%) patients returned to sports at or above their preoperative level. However, their pre- to postoperative Tegner scores remained unchanged and even decreased nonsignificantly.
The results of this study indicate that the preoperative level of sports activity, evaluated with the Tegner score, has a relevant influence on patients’ postoperative performance. The likelihood of returning to the same or even a higher level of activity was significantly greater in the low-level activity group than in the high-level activity group. Thus, when evaluating sports activity, the ratio and distribution of the Tegner score values within a study group should be taken into account as an isolated interpretation of pre- to postoperative Tegner score changes appears to be too imprecise to draw meaningful conclusions regarding the successful return to sports. In addition, the results indicate that a (sub)group of patients with recurrent patellar instability associated with severe trochlear dysplasia is able to maintain a relatively high level of sports activity (copers). On the basis of the current data, we are increasingly aware of the critical need for a TP to be performed in these patients. In particular, the results of previous investigations achieved good clinical outcomes with isolated MPFLR among patients with trochlear dysplasia.16,18
Return to participation—defined as the return to sports-specific training or participation at a lower level—was achieved in 95% of the patients. However, only 53% of the patients returned to sports at their preinjury level, and only 42% returned to their preinjury levels of performance. Interestingly, returning to sports activity at a lower level than preoperatively did not negatively affect disease-specific quality of life (BPII 2.0) or influence subjective ratings of knee joint function in the subgroup of higher-level athletes. Accordingly, Matassi et al 21 recently reported that clinical scores provide little information about patients’ rate of (and readiness for) returning to sports after patellar-stabilizing surgery. Findings reveal parallels to rehabilitation after anterior cruciate ligament reconstruction, with marked differences between the reports of return-to-sports rates and patients’ subjective rating of knee joint function. A systematic review by Ardern et al 2 reported that although nearly 90% of patients reported normal or nearly normal knee joint function, only 59% to 72% of patients returned to their preinjury sport, and only 46% to 63% returned to competitive sports.
Hurley et al 14 reported that after MPFLR, patients who do not return to sports exhibit poor psychological readiness, and the most common reason is a fear of reinjury. The higher-level athlete group in our study also tended to exhibit more fear of reinjury than the low-level athlete group. In addition, during the follow-up examination, it became clear that other factors might have affected the level of postoperative sports participation. Although this was not investigated in detail, many patients reported a significant change in their daily lifestyle during the follow-up period. The changes in work and professional lifestyles, particularly in the young patients, were striking, as sports became less important to them.
Data on the return to sports after patellar-stabilizing surgery remain underreported in the literature, with most studies reporting data on MPFLR.15,27 Krych et al 15 studied 39 athletes who underwent MFPLR for recurrent lateral patellar instability. The authors found this procedure to be effective for returning athletes to competitive sports. However, strength deficits persisted at 6 months after surgery, especially in the patients who underwent concomitant TTO. In a recent systematic review of 23 articles (930 patients), the rate of return to sports after MPFLR was 92.8%. 27 A total of 71.3% of patients returned to or surpassed their preoperative level of activity, and the patients returned to sports at a mean of 6.7 months (range, 3.0-6.4 months) postoperatively. Another systematic review by Manjunath et al 20 reported that 68.3% of patients returned to the same level of play and that the average time to return to play was 7.0 months postoperatively. However, a prolonged rehabilitation program (longer than 8 months) has been recommended to allow the adequate recovery of muscle strength for a safe return to sports in adolescents after MPFLR. 28 Because the rehabilitation continuum after deepening TP has not been evaluated in detail in the literature, and a scarcity of evidence regarding guidelines for the return to sports is evident, 30 the current study might provide reference information for physicians who counsel patients and athletes undergoing complex patellar-stabilizing surgeries.
Limitations
Although a goal of this study was a minimum follow-up rate of 80%, and attempts were made to reach all patients with a minimum of 2 years postoperatively by phone or email, we noticed a 22.3% dropout rate. This rate was mainly due to the previously mentioned changes in work and professional lifestyles, including changes in contact details, that occurred in many of the young patients. Second, it is important to note that this study used patient-reported outcome measures only and that the results were not correlated with objective clinical findings, such as patellar apprehension test results, functional performance results, or imaging. Third, rehabilitation was only controlled within the first 3 (to 6) months after surgery. Afterward, the patients were not routinely screened for eligibility to return to sports, and the patients had to recount their sports recovery process during follow-up evaluations, which naturally led to the limitations and potential bias characteristic of retrospective studies. In addition, some patients had adjunctive procedures, which may confound interpretation of the results. Thus, this study reports only the natural time course of rehabilitation after TP and concomitant patellar-stabilizing surgery and does not provide recommendations regarding the return to sports activity.
Conclusion
Patients undergoing deepening TP and medial soft tissue stabilization with or without concomitant realignment surgery for complex patellar instability can expect good clinical results and a high rate of return to sports participation, with two-thirds of patients returning to their preoperative Tegner-level of activity or higher. However, higher-level athletes should be informed that their likelihood of returning to sports at the preoperative level or full participation at a competitive level is reduced.
Footnotes
Submitted April 18, 2021; accepted September 30, 2021.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.