
Abstract
Background:
Current consensus and position statements recommend that concussed patients be asymptomatic upon the initiation of the graduated return to activity (RTA) protocol. However, a significant number of concussed patients are beginning their RTA protocols while endorsing symptoms.
Purpose:
To characterize symptom endorsement at the beginning of the RTA protocol and examine the association between symptom endorsement and RTA protocol duration in service academy cadets.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
A prospective cohort study was conducted with cadets at 3 US service academies. Postconcussion symptom inventories were recorded upon the initiation of an RTA protocol. The Sport Concussion Assessment Tool Symptom Inventory was used to classify participants into 3 groups (0 symptoms, 1 symptom, and ≥2 symptoms) upon the initiation of the RTA protocol. The primary outcome of interest was RTA protocol duration. Kaplan-Meier survival estimates were calculated to estimate RTA protocol duration by symptom endorsement, sex, varsity status, academic break, and time to graduated RTA initiation. Univariate and multivariable Cox proportional hazards models were used to estimate the association between symptom endorsement at the initiation of the RTA protocol and RTA protocol duration (α < .05).
Results:
Data were analyzed from 966 concussed cadets (36% women). Headache (42%) and faintness/dizziness (44%) were the most commonly endorsed symptoms on the Sport Concussion Assessment Tool-Third Edition and the Brief Symptom Inventory-18, respectively. Univariate results revealed a significant association between endorsing ≥2 symptoms and RTA protocol duration. In the multivariable model, endorsing ≥2 symptoms maintained a statistically significant association with RTA protocol duration. Significant associations were observed between RTA protocol duration and nonvarsity status (27% longer), women (15% longer), academic breaks (70% longer), and time to the initiation of the RTA protocol (1.1% longer daily incremental increase) after controlling for covariates.
Conclusion:
Symptom endorsement at the initiation of an RTA protocol was associated with RTA protocol duration. Cadets who had returned to preinjury baseline symptom burden or improved from baseline symptom burden and endorsed ≥2 symptoms at the initiation of the RTA protocol took longer to RTA.
Recovery from a concussion is frequently marked by the resolution of symptoms and return to normal activities, including school, work, and sports. 43 Current consensus guidelines and position statements recommend that an individual completes a graduated return to activity (RTA) protocol before being cleared for unrestricted RTA.8,19,22,43 Determining the point at which a concussed patient is ready to begin a graduated exercise protocol can be challenging. Statements presented by a variety of organizations agree that graduated exercise is an important component of the RTA protocol and that the symptoms reported by the patient should be considered before initiating the vigorous exercise component of the protocol, although the specific recommendations vary across organizations.8,19,22,43 The National Athletic Trainers’ Association recommends that “A physical-exertion progression should begin only after the concussed athlete demonstrates a normal clinical examination, the resolution of concussion-related symptoms, and a return to preinjury scores on tests of motor control and neurocognitive function.” 8 Similarly, the Concussion in Sport Group recommends that a graduated RTA strategy be implemented after a period of initial rest (24-48 hours) and symptom-limited cognitive and physical exacerbation without a recurrence of concussion-related symptoms. 43 However, these recommendations are solely based on consensus, usual practice, or opinion rather than clinical evidence, and they offer varying guidance about beginning graduated RTA protocols.8,22
In 1986, the term “asymptomatic,” in regard to concussion, was broadly defined as having “no headache or dizziness or impaired orientation, concentration, or memory during rest or exertion.” 10 Since then, concussion management has continued to evolve, leading to a wider variety of approaches for identifying and managing the injury37,41 and a greater understanding of the negative sequelae that may ensue. 27 In an effort to recommend more comprehensive guidelines, the first International Conference on Concussion in Sport convened and recommended that athletes be “completely asymptomatic and have normal neurological and cognitive evaluations before the start of the rehabilitation program.” 6 Shortly thereafter, research emerged suggesting that light aerobic exercise should be initiated before symptom resolution, as prolonged periods of rest were detrimental to the healing process after a concussion.33,34,51,52 For the past 10 years, 36 initiating light aerobic exercise, below the symptom threshold, as soon as possible has been recommended after the acute stage of concussion to help promote recovery.33-35 Each day elapsed between sustaining a concussion and beginning light aerobic exercise has been correlated with longer concussion recovery times in athletes. 33 These findings led the Concussion in Sport Group to recommend subsymptom aerobic exercise after a brief rest period, followed by a more vigorous RTA protocol once asymptomatic as mentioned in the 2016 consensus statement. 43 Although the Concussion in Sport Group recommends that the rehabilitation protocol be initiated when individuals are “asymptomatic at rest,” the 2016 consensus statement 43 does not clearly define asymptomatic.
The lack of an operational definition for asymptomatic combined with the recommendation for subsymptom exercise, creates a degree of subjectivity when clinicians are trying to determine when an injured athlete is ready to begin an RTA protocol. 43 This also proves challenging for military medical professionals when making decisions about returning service members back to duty and service academy cadets back to athletics, physical education courses, and military training. With more than 342,000 concussions in US service members 17 since 2000, military medical practitioners have relied heavily on civilian sector guidelines for athletes 44 to inform clinical RTA or duty decisions. 45 However, recognizing that patients who are not concussed often report symptoms associated with concussion, the Progressive Return to Activity Following Mild Traumatic Brain Injury Working Group avoided the use of the term “asymptomatic” in their clinical recommendations to the Department of Defense and defined symptom resolution as a return to self-reported preconcussion symptom baseline. 45 Previous literature has suggested the use of symptom thresholds to aid decision making surrounding the initiation of an RTA protocol. Common examples include the return of all symptoms to zero and the return of acute postconcussion symptoms to zero. 1 Another approach is that patients under a specific total symptom score threshold, such as 7 symptoms, can begin an RTA protocol. 32 Given symptom differences by sex, the total symptom score threshold adjustments of 5 for men and 6 for women have also been suggested based on symptoms reported at rest and after exercise in a nonconcussed population. 1 In addition to sex differences in symptom endorsement, factors such as varsity sport status, psychological status, and concussion history have influenced symptom endorsement.21,26,53-55 Furthermore, up to 25% of uninjured athletes and cadets reported baseline symptoms consistent with the International Statistical Classification of Diseases and Related Health Problems, 10th Revision, criteria for the postconcussion syndrome.5,11 Nonconcussed cadets have also reported neurological symptoms after intense bouts of exercise. 2 Thus, relying on symptom scores that may be unrelated to the concussion could delay the RTA progression and necessitates a need for further understanding of these symptom thresholds.
A range of approaches4,15,32 have been implemented by clinicians in athletic and military settings to determine when a concussed patient is ready to begin an RTA protocol. However, to date, there is a lack of literature describing the symptom endorsement of concussed patients beginning the RTA protocol and how the symptom endorsement at the beginning of the protocol influences recovery.1,7 Previous research has shown that endorsing symptoms at the initiation of RTA protocols is associated with prolonged RTA protocol durations in an athletic population. 7 More specifically, athletes endorsing symptom severity scores >10 on the Sport Concussion Assessment Tool-Third Edition (SCAT-3) experienced longer RTA protocol durations. 7 The US military service academies offer a unique population to examine symptom endorsement of concussed patients upon the initiation of an RTA protocol and to monitor recovery. Cadets attending the service academies participate in athletics, making them similar to patients included in previous studies in this area. 7 However, guidance for concussions sustained in athletics are not always relevant to a military context, as they do not incorporate all of the facets associated with military training. 45 The purpose of this study was to describe the SCAT-3 and the Brief Symptom Inventory–18 (BSI-18) symptom endorsement at the beginning of an RTA protocol in military cadets and examine the association between the SCAT-3 symptom endorsement at the beginning of the RTA protocol and recovery time. We hypothesized that cadets endorsing symptoms upon the initiation of an RTA protocol would exhibit longer RTA protocol durations than cadets endorsing zero symptoms.
Methods
Design and Setting
A prospective cohort study was conducted with military cadets enrolled in the Concussion Assessment, Research and Education (CARE) Consortium to describe symptom endorsement at the beginning of the RTA protocol and determine the relationship between symptom endorsement at the initiation of an RTA protocol and recovery time. For this study, data were obtained from concussions that occurred at 3 US service academy sites participating in CARE from November 2014 to May 2018. The service academies represent a unique population in that every cadet must participate in an intramural, club, or varsity (ie, National Collegiate Athletic Association [NCAA]) sport in conjunction with their military training and academic requirements. The data set included male and female cadets competing at all levels of athletic competition who sustained a concussion during the study period. All procedures for this study were reviewed and approved by the institutional review board at each site and the US Army Human Research Protection Office. Informed consent was provided by all participants before data collection.
Procedures
The structure and procedures of the CARE Consortium have been described previously.9,23 The following is a summary of the procedures as they pertain to the current analysis. At the baseline assessment, all CARE participants provided basic demographic and medical history information, including sex, varsity sport status (ie, varsity or nonvarsity), and site. Baseline testing was conducted preinjury at the beginning of the academic year. Participants who sustained a concussion underwent symptom, balance, and cognitive assessments at standardized clinical time points (ie, postinjury [<24-48 hours], upon the initiation of a graduated RTA protocol [asymptomatic], when cleared for unrestricted activity). During the evaluations, symptoms were recorded via the SCAT-3 and the BSI-18. For this study, we specifically focused on the SCAT-3 and BSI-18 scores reported during the asymptomatic visit. The asymptomatic visit should occur in unison with the beginning of a graduated RTA protocol. The asymptomatic time point was a nonfixed (ie, “floating”) data collection time point that required the clinician to define “asymptomatic” and readiness to initiate the RTA protocol based on the unique needs of the individual athlete. 7 After the asymptomatic visit, all cadets, regardless of sport level, completed a graduated RTA protocol per institutional policies. Because of the floating nature of this time point, athletes may begin graduated RTA protocols when endorsing symptom scores >0, which would allow cadets to begin the protocol without necessarily being symptom-free. 7 Pertinent recovery information for the current study included time to graduated RTA protocol initiation and RTA protocol duration. Time to RTA protocol initiation was defined as time elapsed, in days, between the initial injury and the initiation of the RTA protocol. RTA protocol duration was defined as time elapsed, in days, between the asymptomatic time point and final clearance for unrestricted activity. 53 Thus, the asymptomatic time point and final clearance time point dates were used to calculate the RTA protocol duration. A physician at each service academy provided the final clearance; the decision to allow the cadet to RTA was based on multiple factors, including symptom endorsement and the cadet’s progression through his or her graduated RTA protocol.
Injury Surveillance
Concussion was defined as ‘‘a change in brain function following a force to the head, which may be accompanied by temporary loss of consciousness, but is identified in awake patients with measures of neurologic and cognitive dysfunction.” 12 All concussions sustained by service academy participants enrolled in CARE were documented by the site and entered into a computerized database (QuesGen Systems Inc). The current study analyzed all incident concussion cases, regardless of injury mechanism (ie, athletics, free time, physical education) documented between November 2014 and May 2018 at the United States Air Force, Coast Guard, and Military academies. Repeated cases were excluded. Participants were also excluded if no evaluation was performed at the asymptomatic time point, if they had multiple asymptomatic evaluations because of a complicated recovery (ie, had to restart the RTA progression), if they returned to activities without completing a graduated RTA protocol, if their case was designated as a complicated return (ie, participant regressed after unrestricted RTA), or if they took >90 days to start or finish the RTA protocol. 7 It was noted that winter and spring academic breaks occurred during some participants’ RTA protocols, potentially prolonging the protocol; thus, this was also taken into consideration. Academic calendars for all 3 service academies were acquired via Internet search to obtain winter and spring break dates from academic years 2014-2015 through 2017-2018. If an academic break occurred between the initiation of the RTA protocol (ie, asymptomatic visit date) and unrestricted RTA (ie, final clearance visit date), it was considered to have affected RTA protocol duration.
Instruments
Sport Concussion Assessment Tool-Third Edition. The SCAT-3 measures 22 concussion-related symptoms on a 0 to 6 Likert scale, with 0 indicating no symptoms and 6 indicating severe symptoms.24,42 The number of symptoms are tallied for a symptom total score, ranging from 0 to 22, with higher total symptom values indicating greater symptom burden. 24 The Likert responses are tallied to generate a symptom severity score 24 ranging from 0 to 132. The SCAT-3 symptom inventory has been validated in a concussed population and has demonstrated moderate (intraclass correlation coefficient [ICC], 0.62; 7 days after concussion) to poor (ICC, 0.43; 196 days after concussion) test-retest reliability among high school and collegiate athletes.14,29
Brief Symptom Inventory-18. The BSI-18 is a measure of psychological distress that offers a global severity index (GSI) score quantifying psychological distress; it is composed of 3 dimensions–somatization, anxiety, and depression.31,46 All 18 items are scored on a 0 to 4 Likert scale, with 0 indicating not at all and 4 indicating extremely often. 20 All 18 items are summed to provide a composite score ranging from 0 to 72, with higher scores indicating increased distress.31,46 The BSI-18 GSI has demonstrated good internal consistency (α = .83) and fair test-retest reliability (ICC, 0.69 [7 days after the initial evaluation] to 0.52 [165 days after the initial evaluation]) among high school and collegiate athletes. 31
Statistical Analysis
The mean, median, interquartile range (IQR), minimum, and maximum scores on the SCAT-3 and the BSI-18 were calculated to describe the symptom profiles at the asymptomatic time point. The absolute SCAT-3 symptom endorsement at the asymptomatic time point was used to classify participants into 3 groups: 0 symptoms, 1 symptom, and ≥2 symptoms. Wilcoxon signed-rank tests were used to examine within-participant differences in SCAT-3 total symptom scores between the baseline and asymptomatic time points among the 3 groups. Separate Kaplan-Meier survival estimates were used to examine the relationship between RTA protocol duration based on the SCAT-3 total symptom endorsement at the asymptomatic time point (0, 1, ≥2 symptoms) and sex (male, female), varsity status (varsity, nonvarsity), academic break (no break during RTA protocol, break occurred during RTA protocol), concussion history (no concussion history, history of concussion), and BSI-18 status (no symptoms endorsed, symptoms endorsed). Because most treatment decisions are based on SCAT-3 symptoms, we did not use the BSI-18 to classify participants and estimate RTA protocol duration. Univariate and multivariable Cox proportional hazards regression models were used to estimate the association between symptom endorsement at the asymptomatic time point and RTA protocol duration (α < .05). Only cases with a final clearance date for which RTA protocol duration could be calculated were analyzed in these models. Based on previous research,21,26,53,54 the association between RTA protocol duration and sex, varsity sport status, time to RTA protocol initiation, and BSI-18 scores at the asymptomatic time point were also examined. Because of the potential effect on the recovery timeline, academic breaks were also examined as a dichotomous variable. Academic breaks were defined as winter or spring leave from the respective academy for at least 1 week. Spring break at all 3 military service academies lasted 1 week and winter break lasted approximately 2 to 3 weeks. Predictor variables with significant univariate models (p < .100) were included in the multivariable model. The history of concussion was maintained in the multivariable model because of the current literature highlighting the relationship between these variables and prolonged recovery.3,4,53 Site was controlled for because of the potential RTA protocol differences at each institution. Hazard ratios and 95% confidence intervals were calculated for all regression models. Post hoc analyses were conducted to ensure that the assumptions for Cox proportional hazards regression models were met. All statistical analyses were completed using StataSE software Version 14.2 (StataCorp).
Results
During the study period, 1156 concussions were recorded and documented at 3 service academies participating in the CARE Consortium. Figure 1 outlines study enrollment and excluded cases. A total of 966 cases (36% women, 37% varsity athletes; 19.1 ± 1.4 years old, 175.4 ± 10.2 cm, 74.1 ± 14.2 kg) were retained for the analysis after applying the exclusion criteria. An additional 53 cases were excluded from the regression analyses for not having a final clearance date documented.
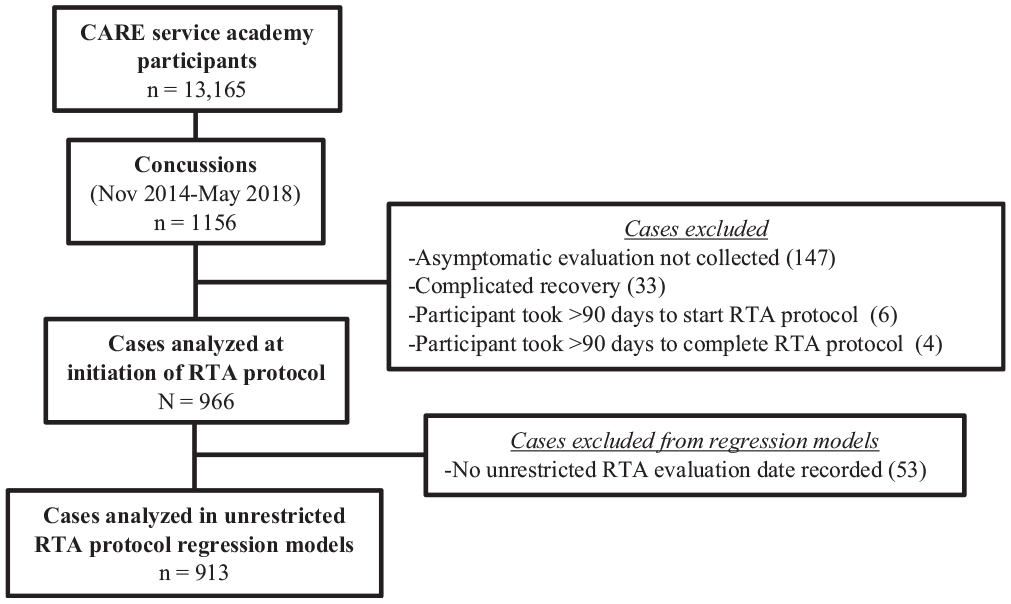
Study enrollment diagram. CARE, the Concussion Assessment, Research and Education; RTA, return to activity.
Symptom Endorsement
At the asymptomatic time point, 34% (326/966; 118 women; 122 varsity athletes) of the cohort endorsed symptoms on the SCAT-3 and 34% (326/966; 129 women; 111 varsity athletes) endorsed symptoms on the BSI-18. Descriptive statistics for the SCAT-3 and the BSI-18 are reported in Table 1 for those who endorsed 0 symptoms, 1 symptom, or ≥2 symptoms at the baseline, post-injury, asymptomatic, and unrestricted RTA time points.
Descriptive Statistics for SCAT-3 and BSI-18 Scores Among Asymptomatic and Symptomatic Cases at Baseline, After Injury, Asymptomatic, and Unrestricted RTA a
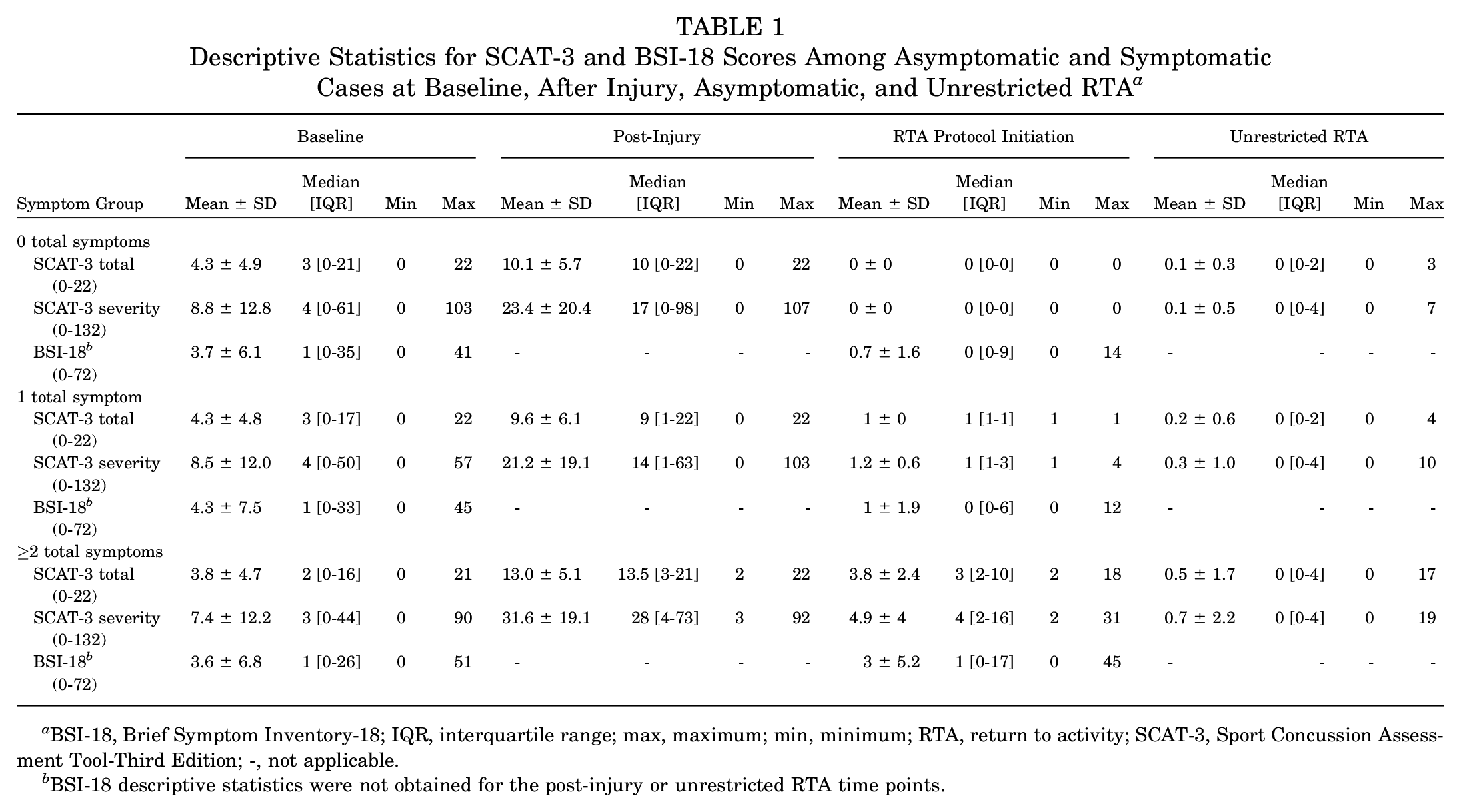
BSI-18, Brief Symptom Inventory-18; IQR, interquartile range; max, maximum; min, minimum; RTA, return to activity; SCAT-3, Sport Concussion Assessment Tool-Third Edition; -, not applicable.
BSI-18 descriptive statistics were not obtained for the post-injury or unrestricted RTA time points.
Table 2 reports the frequency of the SCAT-3 and BSI-18 symptoms endorsed among the symptomatic cohort at the asymptomatic timepoint. The Wilcoxon signed-rank test showed that the median SCAT-3 total symptom scores at the baseline time point were significantly higher than the median SCAT-3 total scores at the asymptomatic time point within the 0 symptoms (Z = -20.218; p≤ .001) and 1 symptom (Z = -7.758; p≤ .001) groups. No significant difference was observed between SCAT-3 total symptom scores at the baseline and asymptomatic time points within the ≥2 symptoms group (Z = 1.490; p = .136). Table 2 displays the proportion of participants who endorsed each symptom on the SCAT-3 and the BSI-18 at the asymptomatic time point. Headache (42%) and faintness/dizziness (44%) were the most commonly endorsed symptoms on the SCAT-3 and the BSI-18, respectively.
Frequency of Physical and Psychological Symptoms Endorsed at Initiation of the RTA Protocol a
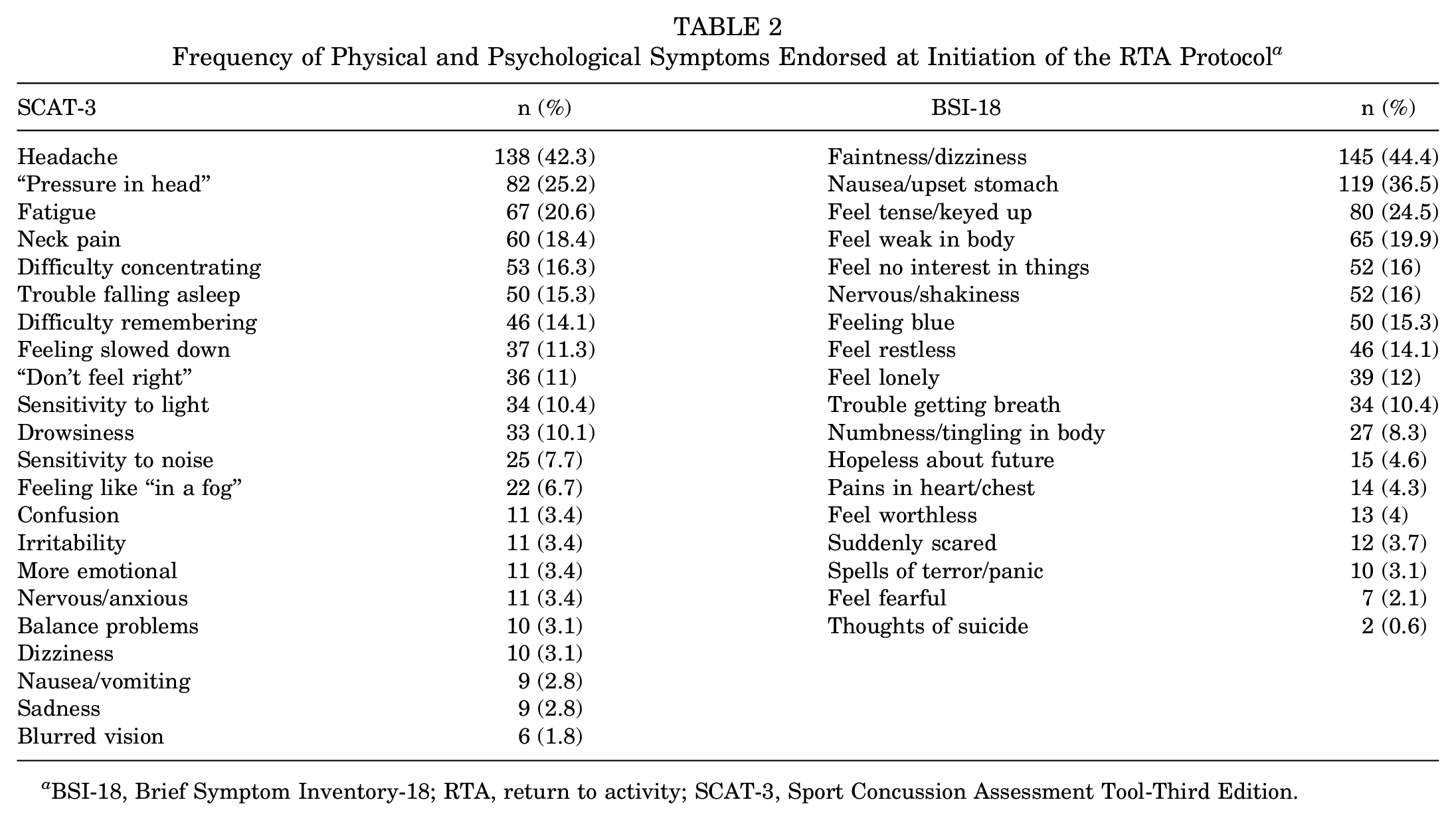
BSI-18, Brief Symptom Inventory-18; RTA, return to activity; SCAT-3, Sport Concussion Assessment Tool-Third Edition.
Symptom Endorsement and Recovery
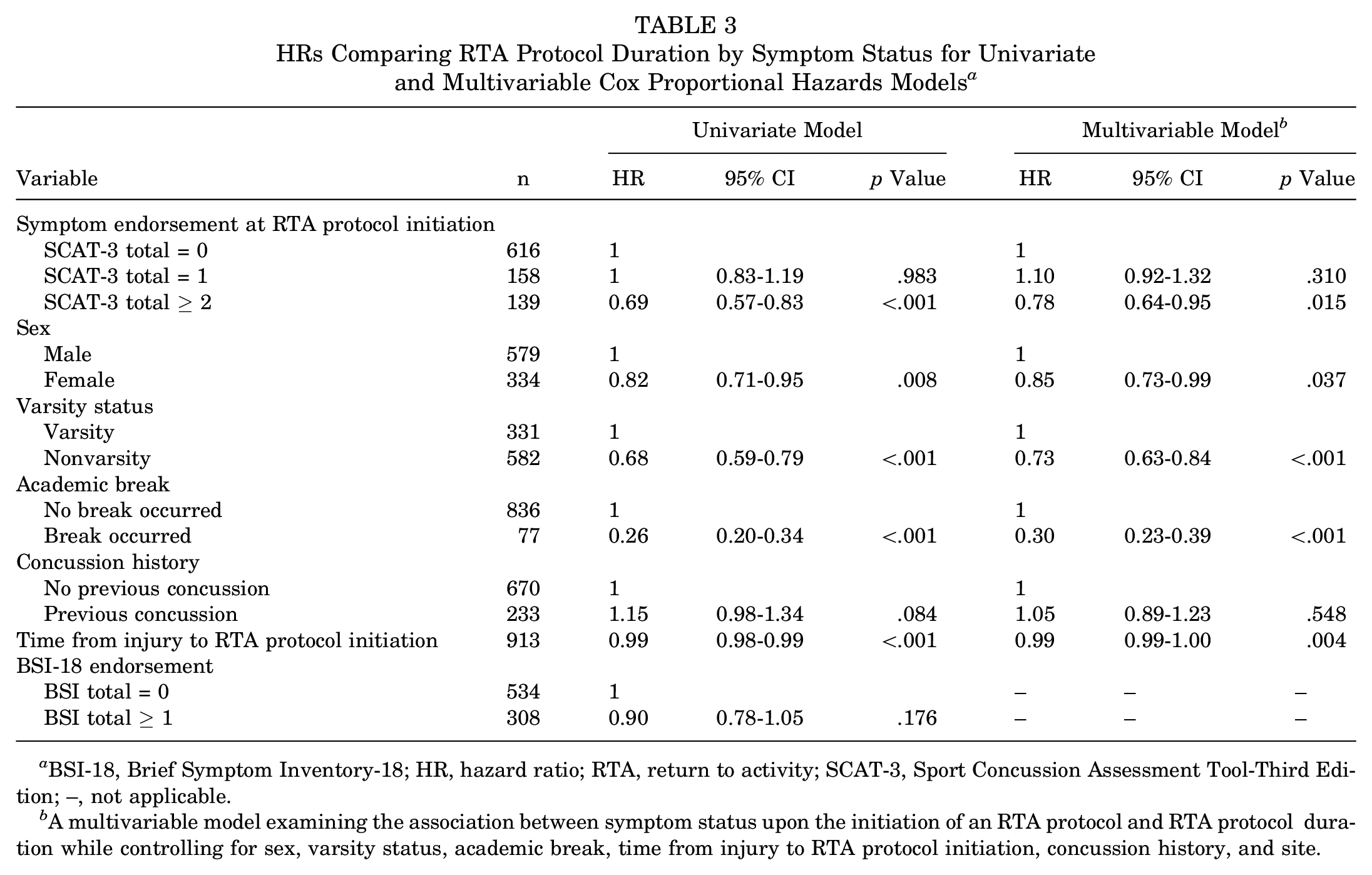
Figure 2 displays the Kaplan-Meier survival estimates for RTA protocol duration by the SCAT-3 symptom endorsement at the asymptomatic time point, sex, varsity status, academic break, concussion history, and BSI-18 endorsement. The median RTA protocol duration for the SCAT-3 asymptomatic group was 7 days (IQR, 1-50 days). For the SCAT-3 symptomatic groups, the median RTA protocol duration was 7 (IQR, 3-47) and 12 (IQR, 3-55) days, for 1 symptom and ≥2 symptoms, respectively. The univariate and multivariable regression models are summarized in Table 3. Results revealed a significant association between the SCAT-3 total symptom endorsement at the asymptomatic time point and RTA protocol duration. Cadets who endorsed
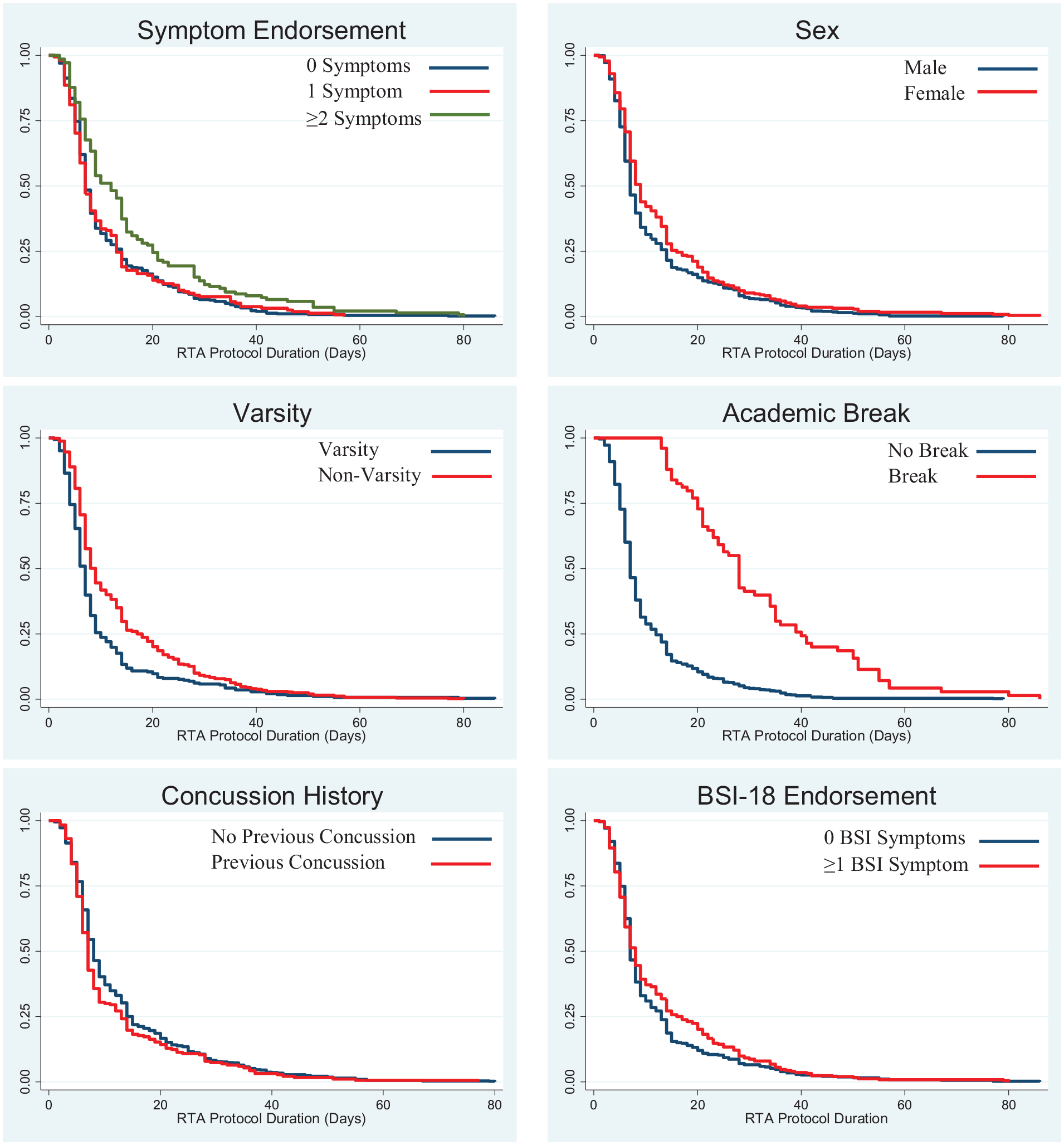
Kaplan-Meier survival estimates for RTA protocol duration by different covariates at the initiation of the RTA protocol. BSI-18, Brief Symptom Inventory-18; RTA, return to activity.
HRs Comparing RTA Protocol Duration by Symptom Status for Univariate and Multivariable Cox Proportional Hazards Models a
BSI-18, Brief Symptom Inventory-18; HR, hazard ratio; RTA, return to activity; SCAT-3, Sport Concussion Assessment Tool-Third Edition; –, not applicable.
A multivariable model examining the association between symptom status upon the initiation of an RTA protocol and RTA protocol duration while controlling for sex, varsity status, academic break, time from injury to RTA protocol initiation, concussion history, and site.
In the multivariable model, controlling for sex, varsity status, academic breaks, time to initiation of the RTA protocol, concussion history, and site symptom endorsement maintained a statistically significant association with RTA protocol duration. Participants who endorsed ≥2 symptoms took 22% longer to RTA when compared with those with no symptoms at the time of initiating the RTA protocol, and there were no differences in RTA protocol duration between those with 0 symptoms and those with 1 symptom. Significant associations were also observed between RTA protocol duration and women (15% longer), nonvarsity cadets (27% longer), academic breaks (70% longer for protocols with an academic break), and time to the initiation of the RTA protocol (1.1% longer daily incremental increase) after controlling for all other variables in the multivariable model. Concussion history was not significantly associated with RTA protocol duration in the multivariable model.
Discussion
The current study utilized the CARE Consortium service academy cohort to describe the symptom profiles of concussed military cadets at the beginning of the RTA protocol. Overall, we observed a range in the SCAT-3 (total: 0-18; symptom severity: 0-31) and BSI-18 (total: 0-45) symptom scores in cadets deemed ready to initiate an RTA protocol (ie, asymptomatic). Roughly one-third of cadets endorsed symptoms on the SCAT-3 upon the initiation of the RTA protocol. As hypothesized, greater SCAT-3 symptom endorsement was associated with a longer RTA protocol duration. Participants who endorsed ≥2 SCAT-3 symptoms took approximately 22% longer to RTA after accounting for sex, varsity status, academic breaks, time to RTA protocol initiation, concussion history, and site.
Symptom Endorsement and Reporting
The most commonly observed symptom at the initiation of RTA protocols among the active population in the current study was headache, which has been found previously in NCAA athletes. 7 This is unsurprising, as headache has also been found to be the most commonly reported symptom after concussion.38,48 The most commonly endorsed psychological symptom in the current study was somatic (faintness/dizziness). Somatic symptoms have previously been found to be the most commonly endorsed symptom after sustaining a mild to severe traumatic brain injury on the BSI-18. 46 Although faintness/dizziness was endorsed by 44% of participants on the BSI-18, dizziness was only endorsed by 3% of participants on the SCAT-3. These trends were also noted between nausea/upset stomach (37%) on the BSI-18 and nausea/vomiting (3%) on the SCAT-3, as well as nervous/shakiness (16%) and nervous/anxious (3%). It is possible that participants were endorsing the other symptoms listed (ie, faintness and not dizziness, upset stomach and not vomiting), but this observation suggests that wording and method of administration (ie, self-report vs clinician interview) may be important when querying patient symptoms. Patients are typically more honest when self-reporting.25,30 However, a clinician interview offers the opportunity for questions and discussions that may lead to further insight into the patient’s symptomology. 49
Although this is the first investigation to explore symptom endorsement at this recovery milestone and to report on symptoms in the service academy cohort, previous literature from the CARE Consortium reported comparable SCAT-3 symptom scores in NCAA athletes.
7
In an NCAA cohort, roughly 40% of athletes endorsed SCAT-3 symptoms, a figure similar to the 34% of cadets who endorsed SCAT-3 symptoms upon the initiation of the RTA protocol.
7
Thus, despite consensus statements using the term “asymptomatic,”
43
roughly a third of patients are not symptom free when the RTA protocol is initiated. Although not symptom free, the patients in the current study reporting symptoms at the asymptomatic time point had returned to baseline symptom values or reported fewer symptoms than at the baseline time point. Even though a graduated RTA protocol can be initiated before all symptoms have resolved or upon the individual returning to baseline symptom values, symptom severity scores >10 in NCAA athletes
7
and endorsement of
Covariates and RTA Protocol Duration
Sex, varsity status, and academic breaks also played a significant role, with women, nonvarsity athletes, and those who incurred an academic break during the RTA protocol taking more time to RTA. Women and nonvarsity athletes took roughly 15% and 27% longer to RTA, respectively, and participants who experienced an academic break during the RTA protocol took roughly 70% longer to RTA. This is consistent with most of the current literature, as women have previously displayed longer RTA timelines than men in both service academy and athletic settings.18,54 However, a more recent study found that women displayed no difference in recovery time compared with men playing comparable collegiate sports. 39 Nonvarsity cadets have also displayed longer RTA timelines when compared with varsity athletes. 18 These findings are not surprising because women have been more likely to report concussion symptoms,16,28,47 and health care for nonvarsity athletes may not always be readily accessible. 50 The differences observed in RTA protocol duration between varsity and nonvarsity athletes may also be attributed to the social and psychological aspects associated with varsity athletics, where there may be increased internal or external pressure placed on athletes to return to sports. 13 The longer RTA protocol duration among individuals who had an academic break during the RTA protocol is most likely because of a lack of access to care.50,54 Athletes and cadets generally do not have access to their primary health care provider if they are away for a week during winter or spring break. It is important to recognize the factors that may contribute to prolonged RTA protocol durations and work to account for those factors in estimating RTA duration after injury.
Time to graduated RTA protocol initiation was examined to gain a better understanding of how the total recovery process might influence RTA protocol duration. Not surprisingly, cadets who took longer to reach the beginning of the RTA protocol also took longer to complete the RTA protocol. A 1-day increase in the time it took to reach RTA protocol initiation resulted in a 1.1% longer RTA protocol duration. This finding has been supported by previous research, where a time to graduated RTA initiation period lasting >11 days resulted in an increased RTA protocol duration. 53 Although a longer symptom-free waiting period before beginning any exercise has been shown to reduce the chances of sustaining a subsequent concussion, 40 delaying light aerobic exercise for >3 days after sustaining a concussion has been associated with prolonged recovery trajectories. 33 With the benefits of light aerobic exercise during concussion recovery being well documented,33,35 it should be considered as part of the management plan.
Implications and Current Guidelines
Current position and consensus statements1,8,43 offer a generally subjective definition regarding when to initiate an RTA protocol after concussion. Most suggest that patients should be asymptomatic at this time; however, operational definitions for asymptomatic have varied or are simply nonexistent.8,19,22,43 Thus, clinicians have employed a range of approaches to determine when a patient is ready to begin the RTA exercise protocol. The results from our study found that individuals endorsing ≥2 symptoms on the SCAT-3 at the initiation of an RTA protocol took longer to recover. This would suggest that endorsing ≥2 total concussion-like symptoms when initiating an RTA protocol may affect the duration of the protocol. It should also be noted that an individual endorsing at least 2 symptoms at the baseline time point may never endorse <2 symptoms after concussion. Access to care should also be given further consideration to ensure all individuals have adequate access to health care regardless of competition level and while on an academic break.
Limitations and Future Research
The current study was not without limitations. We only assessed a young, physically active service academy cohort; although this cohort is reflective of a collegiate athletic cohort, it may not be reflective of the general population or enlisted military personnel. Our data set did not identify specific physical examination abnormalities (eg, cervicogenic headache, oculomotor problem) that may have affected the endorsement of concussion symptoms upon the RTA protocol initiation. Our data set also could not account for any specific issues that may have caused a delay in the RTA protocol duration. Additionally, the method of administration (self-report vs clinician interview) was not recorded for the SCAT-3, and the baseline SCAT-3 was administered during or after basic training at the academies, which may have influenced the scores. Last, these findings are only applicable to those who experienced a relatively normal recovery (ie, RTA protocol duration was <90 days or the RTA protocol did not need to be restarted because of recovery complications), as those who experienced a complicated recovery were excluded. Future research should assess the association between RTA protocol duration and psychological distress, balance, and cognitive function.
Conclusion
Symptom endorsement at the initiation of an RTA protocol was associated with prolonged RTA protocol duration in the current study. After controlling for potentially confounding variables, it was found that participants who endorsed ≥2 symptoms at the initiation of their RTA protocol, had returned to their baseline symptom burden, or reported fewer symptoms than at the baseline time point took 22% longer to RTA. Furthermore, women, nonvarsity athletes, cadets who experienced an academic break in the middle of the RTA protocol, and cadets who took longer to reach the RTA protocol initiation took longer to RTA. As a result, clinicians should be cautious when initiating an RTA protocol in patients endorsing ≥2 concussion-like symptoms. Even if the patients have returned to their baseline symptom burden or improved from the baseline time point, they may take longer to recover.
Footnotes
Acknowledgements
This study was conducted at 3 US service academies: the United States Military Academy, the United States Air Force Academy, and the United States Coast Guard Academy. The authors thank Bonnie Campbell, Lisa Campbell, Megan Jackson, Jennifer Miley, Joel Robb, and Kim Robb (United States Air Force Academy); Robin Miller and Jarrett Headley (United States Coast Guard Academy); Stephanie Carminati, Story Miraldi, Karen Peck, Jamie Reilly, Sean Roach, Jeremy Ross, and Jesse Trump (Unites States Military Academy) for data acquisition. Also, the authors thank the research and medical staff who assisted with baseline data collection at each of the 3 service academies. The authors also express their thanks to Jaroslaw Harezlak, Jody Harland, Janetta Matesan, Larry Riggen (Indiana University); Ashley Rettmann (University of Michigan); Melissa Koschnitzke (Medical College of Wisconsin); Michael Jarrett, Vibeke Brinck, and Bianca Byrne (QuesGen); and Thomas Dompier, Erin B. Wasserman, Milessa Niceley Baker, and Sara Quetant (Datalys Center for Sports Injury Research and Prevention).
Submitted April 30, 2021; accepted October 14, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: This publication was made possible in part with support from the Grand Alliance Concussion Assessment, Research, and Education Consortium, funded in part by the National Collegiate Athletic Association and the Department of Defense. The U.S. Army Medical Research Acquisition Activity (820 Chandler Street, Fort Detrick, MD 21702-5014) is the awarding and administering acquisition office. This work was supported by the Office of the Assistant Secretary of Defense for Health Affairs, through the Combat Casualty Care Research Program, endorsed by the Department of Defense, through the Joint Program Committee 6/Combat Casualty Care Research Program–Psychological Health and Traumatic Brain Injury Program under Award No. W81XWH1420151. S.J.S. has received support for education from Supreme Orthopedic Systems and Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.