
Abstract
Background:
Short- and midterm follow-up studies suggest that arthroscopic labral refixation/preservation leads to superior outcomes compared with labral excision/debridement.
Purpose:
To update the previous early (16 months) and midterm (mean, 42 months) follow-up of this cohort, which reported better patient-reported outcome measures and lower failure rates in the repair/refixation group.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
The authors identified patients who underwent labral debridement/focal labral excision during a period before the development of labral repair techniques. A consecutive group of patients within the labral debridement group thought to be repairable with the authors’ current arthroscopic techniques were compared with a group of consecutive patients who underwent labral repair/refixation. In 46 hips, the labrum was focally excised/debrided consistent with pincer- or combined pincer- and cam-type impingement; in 54 hips, the labrum was repaired/refixed. Subjective outcomes were measured with the modified Harris Hip Score (mHHS), 12-Item Short Form Health Survey (SF-12), and visual analog scale (VAS) for pain preoperatively and postoperatively.
Results:
The mean age was 34.0 years in the debridement group and 28.3 years in the repair/refixation group, with a mean follow-up of 7.3 years (range, 2-13.6 years). At the mean follow-up of 7.3 years, subjective outcomes were significantly improved (P < .01) for both groups compared with preoperative scores. The mHHS (P = .008), SF-12 score (P = .012), and VAS pain score (P = .002) were all significantly better for the repair/refixation group compared with the debridement group. Although most recent outcomes for both groups fell slightly at the mean follow-up of 7.3 years in comparison with the 16-month and 3.5-year follow-ups, these differences were not significant. However, the failure rate in the debridement group did get significantly worse (P = .014). Good to excellent results were 47.7% in the debridement group and 86.3% in the refixation group (P < .001), and failure rates were 30.4% (debridement) and 13% (refixation) (P = .033). There were 4 revisions in the debridement group and 3 revisions in the refixation group.
Conclusion:
Longer term, >7-year follow-up comparing focal labral excision/debridement with repair/refixation revealed better patient-reported outcomes and lower failure rates in the labral repair/refixation cohort. Additionally, despite an absolute decrease in patient-related outcome scoring and number of good/excellent results in both groups compared with the 3.5-year report, there was a significantly greater increase in failure rates over time for the excision/debridement group with better maintenance of good to excellent results in the repair/refixation group.
Keywords
The acetabular labrum is a fibrocartilaginous ring surrounding the acetabulum of the hip and is primarily composed of circumferential type 1 collagen fibers. 14 It was previously believed that the labrum had little functional value, and as such, excision/debridement was considered the primary surgical option for symptomatic labral tearing.11,13,26 However, subsequent literature suggests that the acetabular labrum serves an important role with respect to hip joint preservation and maintenance of hip joint integrity.2,5,8,9,15,18-20,29-32 The prevalence of labral tears among patients with hip or groin pain has been reported to be 22% to 55%.13,23,25
Previous studies by the current authors have examined outcomes after arthroscopic excision/debridement of labral lesions versus labral refixation in the setting of pincer-type femoroacetabular impingement (FAI).18,20 These studies determined that the refixation group demonstrated superior clinical outcomes at a minimum of 1 year and 2 years of follow-up and means of 16.4 months and 42 months, respectively.18,20 Five other studies looking at labral excision/debridement versus labral preservation have also reported better outcomes with labral repair/refixation as part of an open or arthroscopic FAI corrective procedure.1,8,30,32,33
The purpose of the current study was to report an update of arthroscopic labral repair/refixation versus focal excision/debridement at long-term follow-up. Given the success of our previous short- to midterm investigations, we hypothesized that the repair/refixation cohort would maintain superior subjective patient-reported outcome scores compared with the focal excision/debridement group in the setting of pincer-type FAI. 3
Methods
This study was conducted under institutional review board approval (No. 1006M83832). Arthroscopic management of pincer-type FAI has been performed by the senior author (C.M.L.) since November 2004. Initially, this consisted of focal labral excision/debridement, followed by resection of the acetabular rim. Beginning in June 2006, we performed labral takedowns to resect acetabular rim overcoverage, followed by labral refixation when appropriate. The indications for acetabular rim resection included a combination of imaging and intraoperative findings consistent with pincer-type FAI. Radiographic and intraoperative findings consistent with pincer-type FAI in this cohort have been previously described. 18 Pincer-type findings were defined on a well-centered anteroposterior plain radiograph. Acetabular retroversion was present when there was a crossover sign, a positive posterior wall sign, and a lateral center-edge (LCE) angle >25° to 30°.17,18 Focal anterior overcoverage was present when there was a crossover sign, a negative posterior wall sign, and an LCE angle >25° to 30°.17,18 Coxa profunda was present when the teardrop was medial to the ilioischial line with an LCE angle >35° to 40°.17,18 Protrusio acetabuli was present when the medial aspect of the femoral head was medial to the ilioischial line.17,18 Cam-type FAI was present when the alpha angle was >55° on plain radiographs.18,35,36
Our indications for labral refixation included a hip with pincer- or combined pincer-type and cam-type FAI, labral injury, and an adequate amount of healthy labral tissue available for refixation. An ideal labrum for refixation lacked significant intrasubstance degeneration, calcification, ossification, or complex degenerative tearing and was typically located anterosuperiorly. To compare the results of this method, we retrospectively reviewed the operative reports, intraoperative images, and preoperative imaging studies of those patients treated with focal labral excision/debridement before the implementation of labral repair/refixation techniques that would have fulfilled the current criteria for labral repair/refixation. Labral lesions associated with isolated cam-type impingement did not necessarily require formal takedown, which was the primary technique at the time of this study. To better standardize the treatment of the labrum, we chose to include pincer and mixed pincer- and cam-type FAI. Therefore, only labral lesions due to pincer-type or combined pincer- and cam-type FAI were included to provide more appropriately matched groups with respect to labral management techniques.
The inclusion criteria for both groups were the same, and the only differences were in the treatment for each group based on the senior author’s change in labral management from debridement to repair/refixation. The debridement group included radiographic and intraoperative findings consistent with pincer- or combined pincer- and cam-type impingement and subsequent arthroscopic labral debridement and management of FAI before the senior author’s use of labral repair/refixation techniques. All patients included in the study had magnetic resonance imaging (MRI), plain radiographs, detailed operative notes, and intraoperative images revealing a relatively healthy portion of the labrum available for repair/refixation without complex tearing, intralabral ossification, or calcification. Additional inclusion criteria included minimal to no radiographic degenerative changes and a minimum 2-year follow-up.
The standard imaging evaluation and technique for arthroscopic management of FAI in the current cohort have been described in previous reports.17,18,20,21 In summary, rim resections were performed over the area of acetabular overcoverage, and femoral resections were performed for cam-type FAI when present (Figure 1). Appropriate bony resections for FAI were evaluated with intraoperative fluoroscopy and confirmed with arthroscopic dynamic assessment.17,18,20,21 The senior author performed all surgical procedures with the patient in a supine position. In the debridement group, a focal excision of the labrum was performed along the area of acetabular overcoverage, leaving the remainder of the healthy portion of the labrum intact. This provided exposure of the acetabular overcoverage and allowed for appropriate rim resection (Figure 2). In the refixation group, the labrum was taken down over the area of acetabular overcoverage, the prominent rim was resected, and labral repair/refixation was performed (Figure 2).
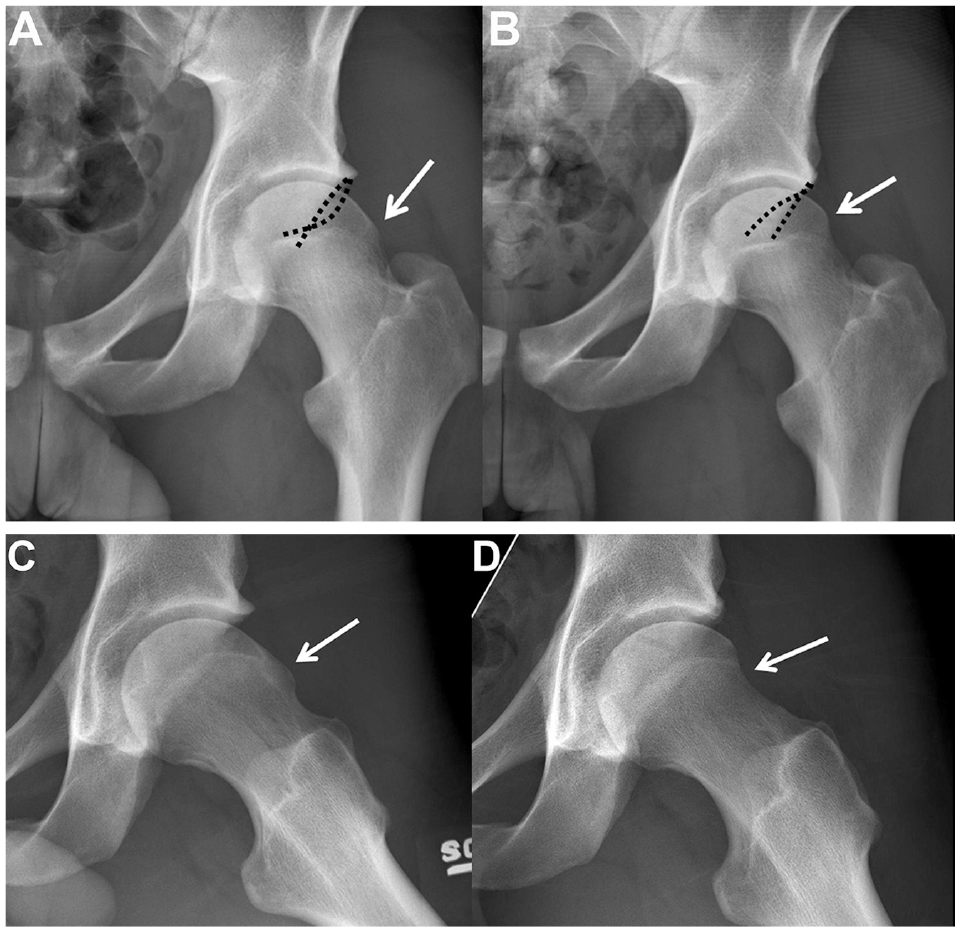
Anteroposterior (AP) pelvis of the left hip in a 21-year-old collegiate hockey player with mixed pincer- and cam-type morphological characteristics. (A) Preoperative AP radiograph reveals acetabular retroversion (dashed curved line) and cam-type femoroacetabular impingement (FAI) (white arrow). (B) Postoperative AP radiograph reveals appropriate arthroscopic rim resection with an anteverted acetabulum (dashed curved line) and improved head-neck offset (white arrow). (C) Preoperative lateral radiograph reveals cam-type FAI (white arrow), and postoperative lateral radiograph (D) reveals improved head-neck offset after arthroscopic femoral resection osteoplasty.
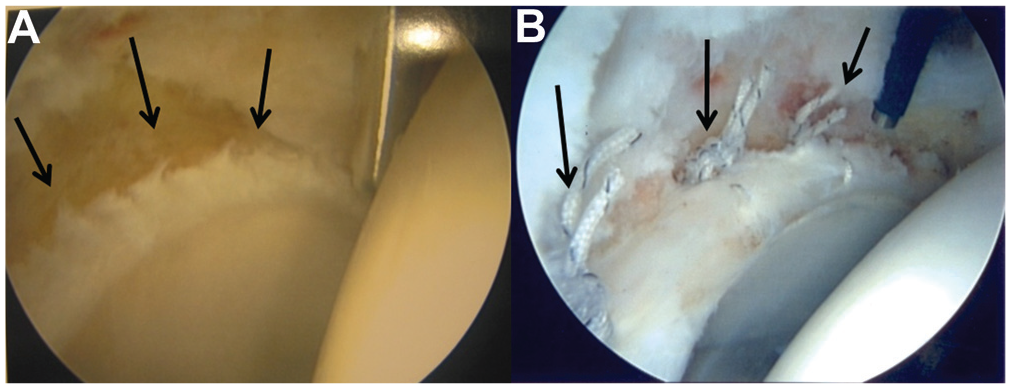
(A) Intraoperative image of the right hip after focal labral excision and arthroscopic rim resection (arrows) for pincer-type femoroacetabular impingement (FAI). (B) Intraoperative image of the right hip after labral takedown, rim resection, and labral refixation (arrows) for pincer-type FAI.
Rehabilitation
Postoperative rehabilitation was guided according to the specific parameters of the procedure. Patients in debridement group were allowed to bear weight as tolerated with crutches until they were able to ambulate with a nonantalgic gait. In general, these patients typically required 2 to 3 weeks of crutch assistance. Patients in the repair/refixation group were kept toe-touch/foot-flat weightbearing for 2 weeks, with range of motion encouraged, but instructed to avoid the extremes of external rotation. Patients who underwent microfracture for full-thickness acetabular defects in either group were kept toe-touch/foot-flat weightbearing for 6 to 8 weeks.
Outcome Scores
Outcomes for both groups were prospectively measured with the modified Harris Hip Score (mHHS), 12-Item Short Form Health Survey (SF-12), and visual analog scale (VAS) for pain preoperatively and at 6 weeks, 3 months, 6 months, and yearly thereafter. Patient-reported outcome scores were collected during clinic visits or by mail. Patients were either seen in the clinic annually or followed yearly by mail. All alpha angles6,7 for patients with cam-type FAI were measured on preoperative and 2-week postoperative anteroposterior pelvis and cross-table lateral radiographs by the senior author. The Tönnis classification was used to grade radiographic degenerative changes preoperatively, and the degree of chondromalacia was graded according to the Outerbridge classification system.28,35,36 Failure was defined as an mHHS score <70 or ipsilateral total hip arthroplasty (THA) or surgical hip dislocation. Good to excellent results were defined as mHHS ≥80.18,20
Statistical Analysis
The differences between preoperative and mean latest follow-up outcome measures were analyzed using paired-sample t tests, with a P value <.05 used to determine significance. Differences between groups were analyzed using independent-sample t tests as well as analyses of variance where appropriate. For analyzing Tönnis grade, Mann-Whitney U tests were utilized. Fisher exact tests were used to determine significant differences between failure rates and percentage of good/excellent results.
Finally, an a priori power analysis was performed. From our preliminary data, we estimated that a clinically significant between-group difference in mHHS would be 6.0 with an SD in each group of 8.0. Using these numbers, a large effect size of 0.75 would be yielded, and thus to obtain a power of 0.80 or higher, each group would need to include at least 29 hips.
Results
Over the study period (November 2004 to September 2007), 172 hips (168 patients) with minimal to no radiographic degenerative changes underwent arthroscopic management of FAI. All patients who fulfilled the inclusion criteria with a minimum 2-year follow-up were included in the final analysis. The patient characteristics are presented in Table 1. This represents the same population as the senior author’s most recent study on outcomes with a mean 3.5-year follow-up 20 and represents a similar length of time since surgery between groups.
Characteristics of Patients a
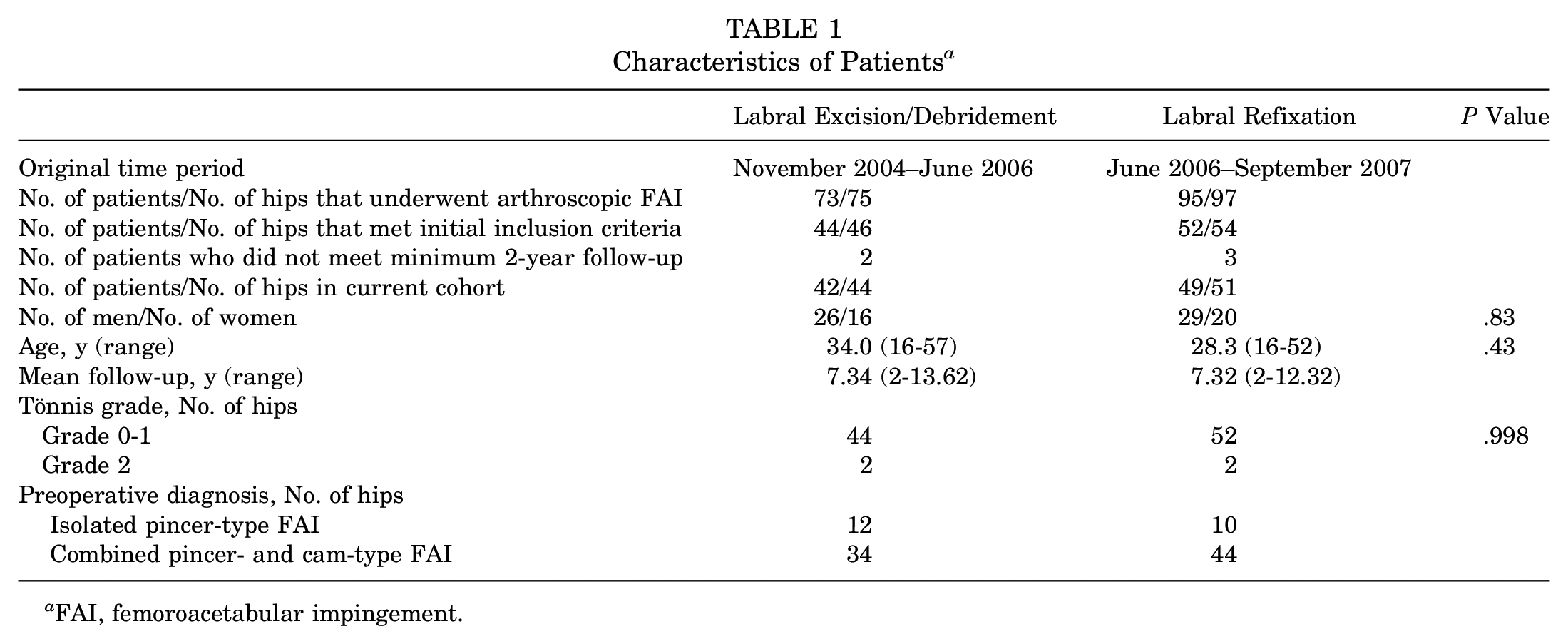
FAI, femoroacetabular impingement.
The mean decreases in alpha angle after femoral resection osteoplasty on anteroposterior and lateral radiographs were 18.4° and 28.2°, respectively, in the debridement group compared with 15.4° and 25.2°, respectively, in the repair/refixation group. There were no statistically significant differences for femoral bone resection on anteroposterior or lateral radiographs between groups based on the reduction in alpha angle (P > .05). There were no statistically significant differences between groups for the degree of chondromalacia found intraoperatively on the acetabulum (P = .34) or femoral head (P = .998) (Table 2). Overall, 77% of hips in the debridement group and 82% of hips in the refixation group were found to have focal areas of Outerbridge grade 3 or 4 chondromalacia, primarily involving the anterosuperior acetabular rim at the time of surgery. There were no statistically significant differences for microfracture or other additional procedures performed at the time of arthroscopy between groups (Table 3).
Degree (Outerbridge Grade) of Chondromalacia Found Intraoperatively a
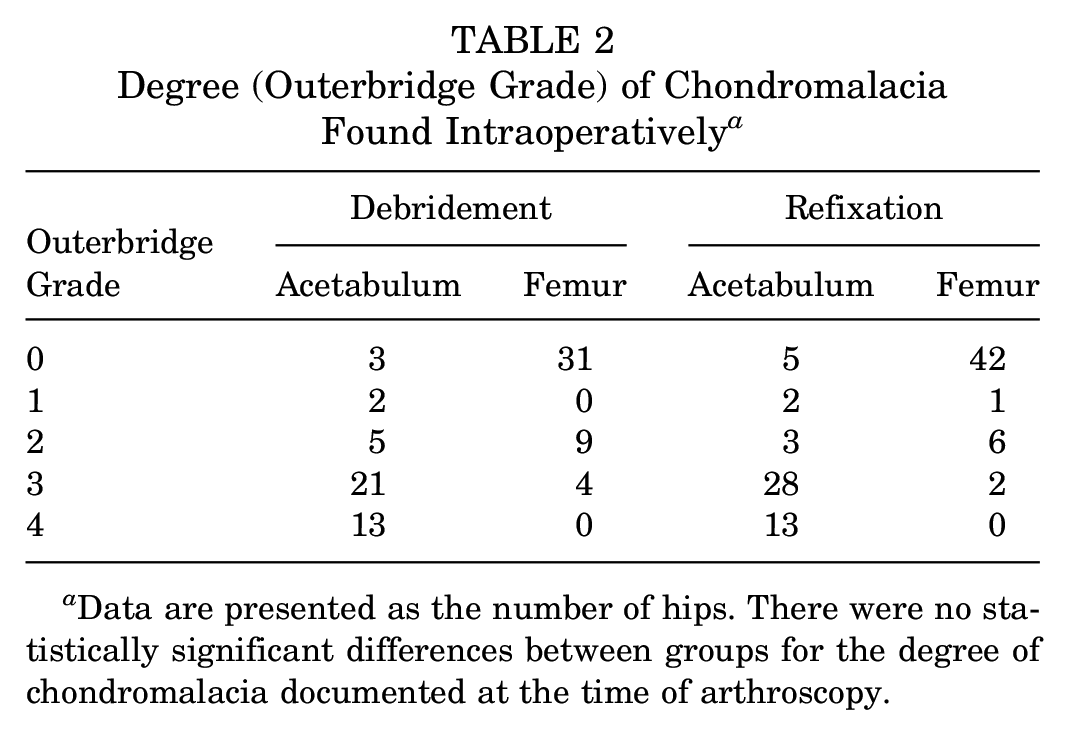
Data are presented as the number of hips. There were no statistically significant differences between groups for the degree of chondromalacia documented at the time of arthroscopy.
Concomitant Procedures Performed at the Time of Arthroscopic Femoroacetabular Impingement Correction (Hips)

The most recent postoperative outcome measures were significantly improved compared with preoperative measures for both groups (P < .01). The mHHS was significantly better in the repair/refixation group (89.9) compared with the debridement group (81.4) at the latest follow-up of 7.3 years (range, 2-13.6 years) (P = .008) (Figure 3 and Table 3). In addition, SF-12 scores were significantly better in the repair/refixation group (88.4) compared with the debridement group (82.0) (P = .012), and VAS scores were significantly lower in the repair/refixation group (1.33 cm) compared with the debridement group (2.70 cm) at the mean latest follow-up (P = .002) (Figures 4 and 5). In addition, there was a greater mean improvement in outcome scores postoperatively for the repair/refixation group compared with the focal labral excision/debridement group for mHHS and SF-12 scoring (Tables 4 and 5).
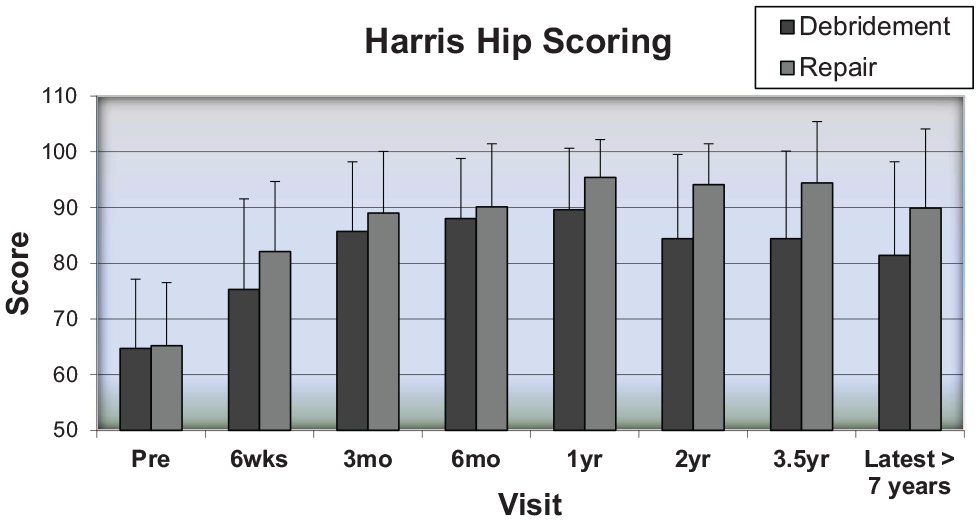
Harris Hip Scores were not significantly different preoperatively between groups. Scores were significantly better for the repair/refixation group at 1 year postoperatively and were maintained throughout the remainder of the study at a mean follow-up of 7.3 years (P < .01).
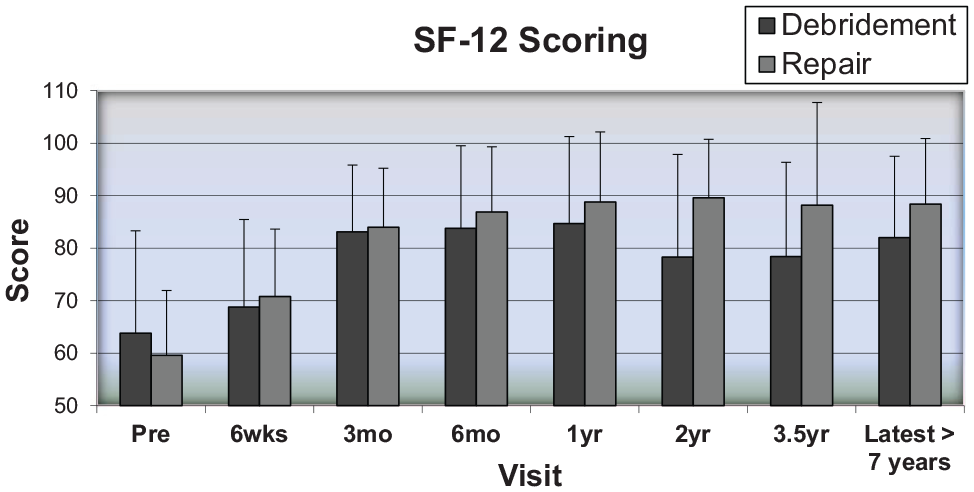
The 12-Item Short Form Health Survey (SF-12) scores were not significantly different preoperatively between groups. The SF-12 scores were significantly better for the repair/refixation group at the most recent follow-up of 7.3 years postoperatively (P = .012).
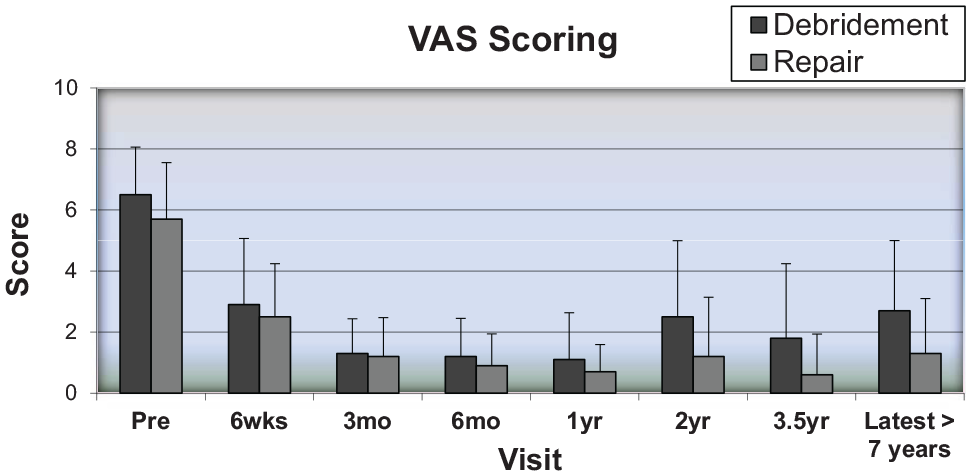
Visual analog scale (VAS) scoring was not significantly different between groups preoperatively. The VAS scores were significantly better for the repair/refixation group at the mean latest follow-up of 7.3 years postoperatively (P = .002).
Preoperative and Postoperative Outcome Scores for the Refixation Group Compared With the Focal Labral Excision/Debridement Group a
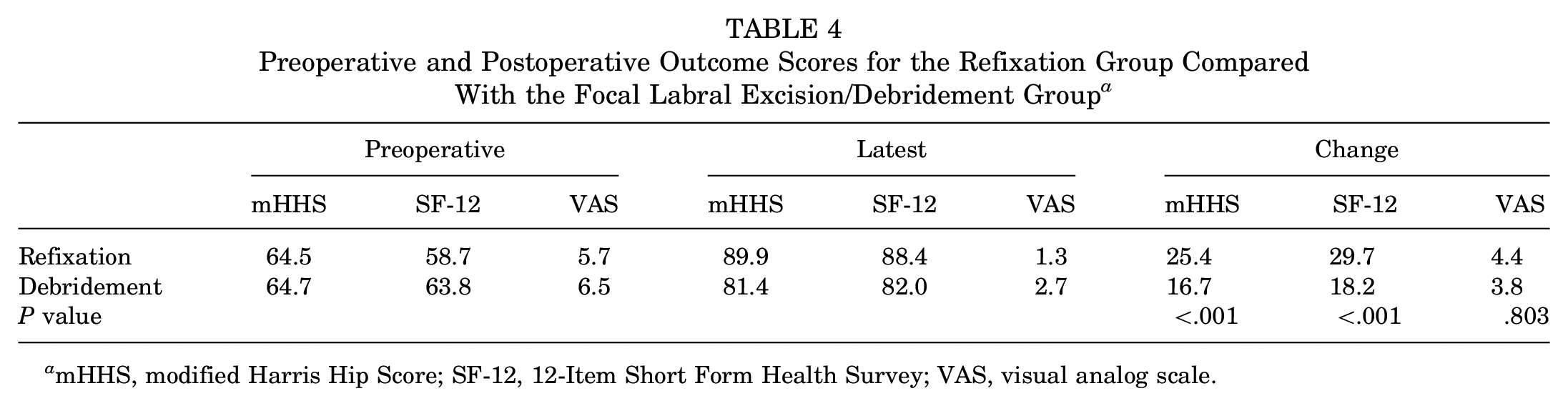
mHHS, modified Harris Hip Score; SF-12, 12-Item Short Form Health Survey; VAS, visual analog scale.
Mean Outcome Scores and Failure Rates for the Repair/Refixation Group Compared With the Labral Excision/Debridement Group Across All 3 Time Points

HHS, Harris Hip Score; SF-12, 12-Item Short Form Health Survey; VAS, visual analog scale.
At the most recent follow-up, good to excellent results (mHHS ≥80) were noted for 47.7% of hips in the debridement group compared with 86.3% of hips in the repair/refixation group (P < .001). Failure was defined as an mHHS <70 (n = 14) or conversion to an open surgical approach, such as open surgical dislocation (n = 1) or THA (n = 6). The failure rate was 30.4% (14 hips: mHHS <70 [n = 10] or THA [n = 4]) in the debridement group compared with 13% (7 hips: mHHS <70 [n = 4] or open surgical dislocation [n = 1] or THA [n = 2]) in the refixation group (P = .033).
Although the most recent mHHS and VAS score for both groups fell slightly at the mean 7.3-year follow-up in comparison with the 16-month and 3.5-year follow-ups, these differences were not significant (P > .05). However, the failure rate in the debridement group did get significantly worse (P = .014) (Table 5).
Complications included 3 patients in the focal excision/debridement group who developed heterotopic bone postoperatively. Two of these patients subsequently had revision hip arthroscopy and postoperative irradiation to remove and prevent recurrent symptomatic heterotopic bone. After we recognized this complication, subsequent patients were treated with naproxen (500 mg twice a day) for 3 weeks postoperatively. No patients in the repair/refixation group developed heterotopic bone postoperatively. Two other patients in the debridement group underwent revision femoral osteochondroplasty for inadequate initial decompression. In the repair group, 1 patient with a 2.5-cm full-thickness acetabular chondral defect at the time of arthroscopy underwent THA at 1-year follow-up. Another patient in the repair group subsequently underwent revision hip surgery with an open surgical dislocation for a symptomatic posterior cam-type lesion at the 2.5-year follow-up. Both of these patients in the repair/refixation group were considered to have experienced failure. No patients sustained femoral neck stress fractures or iatrogenic hip instability or developed avascular necrosis postoperatively.
Discussion
The principal findings of the current study were that labral repair/refixation resulted in a better mHHS, SF-12 score, and VAS score and a greater percentage of good to excellent results and lower failure rates compared with labral excision/debridement in the setting of arthroscopic management of pincer- and combined-type FAI at a mean 7.3-year follow-up. This study represents an update of 2 previous studies performed by the senior author and includes patient-reported outcomes for the same cohort of 100 hips at a longer term, mean 7.3-year follow-up.18,20 The current study also demonstrated that patient-reported outcome measures declined for both groups in comparison with the 3.5-year follow-up study. Failure rates, however, increased significantly in the debridement group, while there was no significant increase in the repair/refixation cohort failure rates over this further follow-up time.
Biomechanical and finite element models have shown that the acetabular labrum contributes to hip joint stability and hip joint congruity and may function to distribute synovial fluid through a sealing function.5,9 Furthermore, biomechanical studies have shown that in the absence of the labrum there is up to a 92% increase in the axial load across the joint9,22 and a 40% increase in cartilage consolidation. 10 In a sheep model, surgically induced labral tears were repaired with a single-suture anchor, and all specimens were later found to heal via fibrovascular scar tissue to the capsule and/or underlying acetabular bone. 29 A human biomechanical study of 6 specimens found that labral repair demonstrated a significant decrease in both mean and maximal cartilage strain compared with labral debridement. 12 Finally, a more recent biomechanical study by Suppauksorn et al 34 demonstrated that suture repair was able to successfully restore the suction seal that is disturbed in labral tears and not restored after labral debridement procedures. 27 These biomechanical studies are the justification for the systemic shift from labral excision/debridement to emphasizing repair or refixation of the labrum whenever possible, despite the previous lack of clinical data to support this transition. These results have also increased the interest in labral reconstruction techniques for the irreparable labrum. The current analysis adds clinical support for the superiority of labrum preservation.
In addition to demonstrating that the labral repair/refixation cohort had a significantly larger portion of good or excellent subjective clinical outcomes and lower failure rates at longer term follow-up compared with the labral debridement group, the average mHHS of the labral repair/refixation cohort was 8.5 points higher than that of the labral excision/debridement group. This difference is more than the minimal clinically important difference of 8 points as defined by Kemp et al. 16 These findings are in line with previous studies that looked at labral refixation versus excision performed with an open surgical dislocation technique for FAI,1,8 which found significantly better subjective clinical outcomes and radiographic results in the refixation group at early, 1- and 2-year, 8 as well as a mean 10-year follow-up. 1 Three previous studies evaluated arthroscopic labral repair versus labral debridement with a minimum 2-year follow-up.24,30,32 Each of the studies found that labral repair resulted in higher mHHS with lower failure rates or rates of subsequent THA.24,30,32 These studies considered repairs and debridements that were performed during the same time period. Therefore, in these previous studies, hips that underwent repairs may have had less labral damage, degenerative changes, or different patterns of impingement when compared with those undergoing debridement, making it difficult to determine how well the 2 groups were matched. Moreover, a recent meta-analysis of labral repair versus debridement that included 5 studies concluded that repair was favored with respect to mHHS, VAS, and patient satisfaction. 37 The results of the current arthroscopic study, previous arthroscopic and surgical dislocation studies, and recent meta-analysis1,8,18,20,24,30,32 support labral preservation/refixation over labral excision/debridement. Despite the conclusions by the aforementioned case series and systematic reviews, a recent study by Chen et al 4 reported no significant difference in subjective clinical outcomes at a 5-year follow-up between patients with labral repair and those who underwent selective debridement with labral preservation, despite 13.9% of patients in the selective debridement group requiring THA. A possible reason for the difference in conclusions could be secondary to previous authors utilizing focal excision of the labrum versus more conservative selective strategies focused on conservation of the labrum.
The current study represents further follow-up on a cohort that was the first to compare the results of arthroscopic labral excision/debridement with labral repair/refixation.18,20 The better patient-reported outcome scores noted at longer term follow-up in the repair/refixation group are in line with the results previously published by the current authors at a mean of 16.4 and 42 months of follow-up.18,20 In addition, the current study reports that the failure rate had increased to a statistically greater degree in the excision/debridement group than in the repair/refixation group in comparison with the 3.5-year follow-up study. 20 This conclusion suggests that there is a significant deterioration of the debridement surgery outcomes observed between the 3.5- and 7-year postoperative time points and relative maintenance of results with labral preservation. This is further supported by a recent study that reported that conversion of selective labral debridement to THA occurred at an average of 47 months after arthroscopic surgery. 4 Moreover, Dwyer et al 7 published on long-term outcomes after arthroscopic debridement of labral tears and determined that the 10-year survival was 70% and the 20-year survival, with THA as an endpoint, was 59%. Domb et al 6 reported that survivorship rates were 96.9% after 2 years and 90.6% after 5 years. These previous reports support the conclusions derived in the current analysis, which suggest that arthroscopic labral debridement demonstrates less favorable outcomes at longer term follow-up.
This study does have significant recognized shortcomings that were previously mentioned in our initial reports and remain consistent in the current analysis.18,20 Most evident are the limitations imposed by the use of a historical control. Every effort was made to properly match patients in the historical debridement group with those selected for labral refixation, but the potential bias cannot be eliminated. It is possible that improvements seen in the later refixation group could be affected by improved techniques for management of FAI and a better understanding of this disorder over time. In addition, improved management of pincer-type impingement with greater experience and newer surgical breakthroughs may have also influenced the results of the current study. In recent years, labral debridement techniques in the setting of pincer-type impingement have evolved to allow rim resection behind the labrum with less aggressive articular-sided labral debridements in some cases. Moreover, although radiographic improvements in the alpha angle were not significantly different between the 2 groups, cam-type impingement is a 3-dimensional entity, and significant improvements for the management of cam-type impingement with greater experience may not be reflected by plain radiographs alone. Differences between groups with respect to the amount of rim resection and correction of pincer-type impingement, however, would also be difficult to evaluate without postoperative 3-dimensional imaging. These variables could only be eliminated by a modern prospective randomized study. However, with the growing awareness of the importance of the acetabular labrum and its potential for healing, the current authors would not be comfortable randomly assigning patients to have the labrum debrided. Thus, this historical control group is likely the most practical method for continued evaluation of this important topic. Finally, the consecutive group nature of this study might allow for greater follow-up in the initial cohort and therefore represent a different time frame after surgery. However, the follow-up range was similar between groups, and therefore the consecutive nature of this study affected the final results to a lesser degree.
Conclusion
Longer term, >7-year follow-up comparing focal labral excision/debridement with repair/refixation revealed better patient-reported outcomes and lower failure rates in the labral repair/refixation cohort. Additionally, despite an absolute decrease in patient-related outcome scoring and number of good/excellent results in both groups compared with the 3.5-year report, there was a significantly greater increase in failure rates over time for the debridement group, with better maintenance of good to excellent results for the labral repair/refixation group.
Footnotes
Submitted March 29, 2021; accepted October 23, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: C.M.L. has received consulting fees from Smith & Nephew and Responsive Arthroscopy; speaking fees from Synthes GmbH; and support for education from Elite Orthopedics; he holds stock options in Responsive Arthroscopy. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.