
Abstract
Background:
Different techniques to restore knee stability after posterolateral corner (PLC) injury have been described. The original anatomic PLC reconstruction uses 2 separate allografts to reconstruct the PLC. Access to allograft tissue continues to be a significant limitation of this technique, which led to the development of a modified anatomic approach utilizing a single autologous semitendinosus graft fixed on the tibia with an adjustable suspensory loop to enable differential tensioning of the PLC components.
Purpose/Hypothesis:
The purpose of this study was to compare the modified anatomic technique with the original anatomic reconstruction in terms of varus and external rotatory laxity in a cadaveric biomechanical model. The hypothesis was that both techniques would restore varus and external rotatory laxity after a simulated complete PLC injury.
Study Design:
Controlled laboratory study.
Methods:
Eight pairs of fresh-frozen cadaveric knee specimens were tested to compare the 2 techniques. Varus and external tibial rotation laxity of the knee were measured while applying 10-N·m varus and 5-N·m external rotatory torques at 0°, 30°, 60°, and 90° of flexion. These measurements were tested under 3 conditions: (1) intact fibular collateral ligament, popliteal tendon, and popliteofibular ligament; (2) complete transection of the fibular collateral ligament, popliteal tendon, and popliteofibular ligament; (3) after PLC reconstruction with either the modified (n = 8) or the original (n = 8) technique.
Results:
After PLC reconstruction, varus laxity was restored with no statistically significant differences from the intact condition after both reconstruction techniques. Similar outcomes were observed for external rotation in extension; however, in terms of the external rotation limit with respect to the intact joint, significant reductions of mean ± SD 4.1°± 6.3° (P = .036) and 5.1°± 6.6° (P = .016) were recorded with the modified technique at 60° and 90° of flexion, respectively. No significant effect was observed on the neutral flexion kinematics from 0° to 90° of flexion, and no significant differences were observed between reconstructions (P = .222).
Conclusion:
Both PLC reconstruction techniques restored the normal native varus as compared with the intact knee. Although the modified technique constrained end-range external rotation at 60° and 90° of flexion, no differences were noted with neutral flexion kinematics. Care should be taken when tensioning in the modified technique so that the tibia is in a neutral position to avoid overconstraining the knee.
Clinical Relevance:
The modified technique may prove useful in situations where there are limited graft options, particularly where allografts are not available or are restricted.
Once thought of as the “dark side” of the knee, owing to the relatively poor understanding of the anatomy and associated biomechanics, the posterolateral corner (PLC) is now much better understood. 12 The primary stabilizers of the PLC are composed of the fibular collateral ligament (FCL), the popliteal tendon (PT), and the popliteofibular ligament (PFL). Functionally, the FCL is a primary stabilizer of varus rotation with a secondary role in controlling hyperextension and external tibial rotation. The PT and the PFL are primary stabilizers of external tibial rotation with a secondary role in controlling varus rotation.
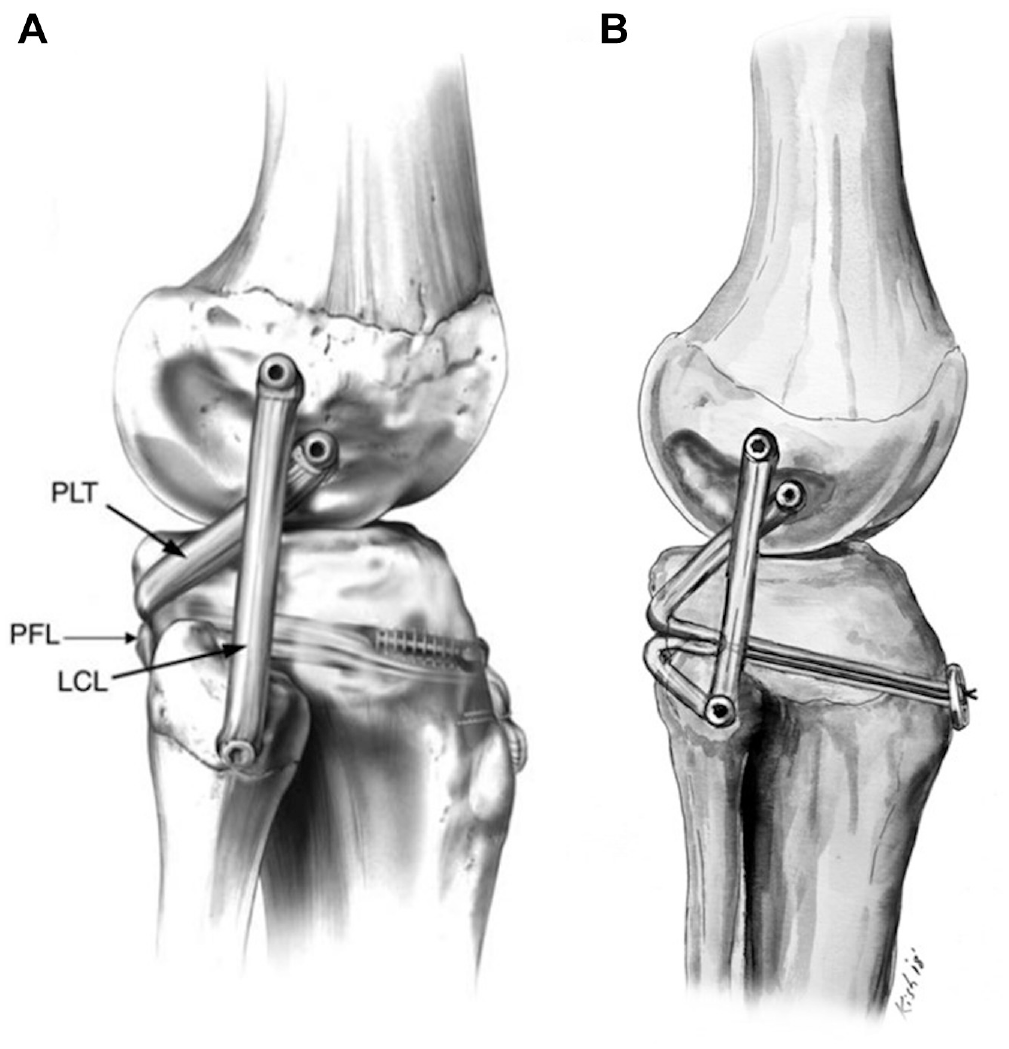
With this improved knowledge of the kinematics of the PLC, LaPrade et al 15 developed an anatomic PLC reconstruction, which has subsequently been validated in cadaveric biomechanical and clinical studies. 13 The original reconstruction utilized a split Achilles tendon allograft, providing 2 separate grafts to reconstruct the different components of the PLC (Figure 1A). 14 The 2-graft construct with fixation in the fibular head and tibia allows for the differential tensioning of the FCL at 30° of flexion and the PFL/PT complex at 70° of flexion.
Unfortunately, not all centers around the world have access to allograft tissue because of regulatory, ethical, or cost issues. Two semitendinosus, semitendinosus plus gracilis, or even peroneus longus autografts may be used instead; yet, in knee dislocation cases where multiple grafts are required for multiple-ligament reconstructions, this is not the most efficient use of autologous tissue. In these cases, some surgeons may prefer to utilize a nonanatomic fibular-based technique, such as that described by Larsen et al 16 or Arciero. 3 However, in cases where proximal tibiofibular joint laxity exists, these reconstructions may not provide the opportunity to stabilize the joint through the use of the PFL component of the reconstruction.
Given the aforementioned issues, we developed a modification of the anatomic LaPrade technique utilizing a single semitendinosus autograft fixed within the tibia by means of an adjustable-loop suspensory device (Figure 1B). 24 This allows for reconstruction of the FCL and PFL/PT components of the anatomic PLC reconstruction with a single graft while, importantly, permitting differential tensioning of the 2 components.
The purpose of this study was to compare the modified anatomic technique with the original anatomic reconstruction in terms of varus and external rotatory laxity in a cadaveric biomechanical model. The hypothesis was that the techniques would restore the stability of the PLC-injured knee in a manner similar to that of the intact knee.
Methods
Eight pairs of fresh-frozen cadaveric specimens (n = 16) without history of injury, surgery, osteoarthritis, or meniscal pathology were used for this study. The average specimen age was 55 years (range, 45-66 years; 5 male, 3 female). The use of deidentified specimens does not require research ethics board review at our institution; however, all research, tissue storage, and tissue disposal protocols were reviewed and approved by United Tissue Network, which is accredited by the American Association of Tissue Banks (9256).
Apparatus and Specimen Preparation
Biomechanical testing was performed with a servo-controlled 6 degrees of freedom joint motion simulator (VIVO; Advanced Mechanical Technology, Inc) (Figure 2). Specimens were stored at −20°C and then thawed at room temperature over a 20-hour period. The femur, tibia, and fibula were transected 20 cm from the transepicondylar axis of the knee. The femur was potted in PVC pipe (12-cm length; 2-in diameter) using dental stone (Golden Denstone Labstone; Modern Materials, Kulzer GmbH) and then mounted to the upper actuator of the VIVO via a custom-made adjustable aluminum fixture. Fixture adjustments were used to align the flexion axis of the knee to the mechanical flexion axis of the joint motion simulator. Our alignment technique, which has been previously described, determines an alignment for the femur that minimizes tibial secondary motions as the joint is passively flexed or extended during testing. 18 Reconstructed 3-dimensional geometries of the femur and tibia were segmented from computed tomography scans with 3-dimensional Slicer software (http://www.slicer.org/) with minimum threshold segmentation at +250 Hounsfield units and coregistered to the bones via attached optical motion tracker arrays (Optotrak Certus; Northern Digital Inc), providing visual guidance on femoral positioning with respect to the origin and motion axes of the joint motion simulator. The tibia and fibula were secured to each other distally using a wood screw and potted into the tibial pot with a styrene pipe adapter (10 cm long; rectangular [3 × 4 in] to circular [4-in diameter]), which was mounted onto the lower actuator of the joint motion simulator with an adjustable aluminum fixture.
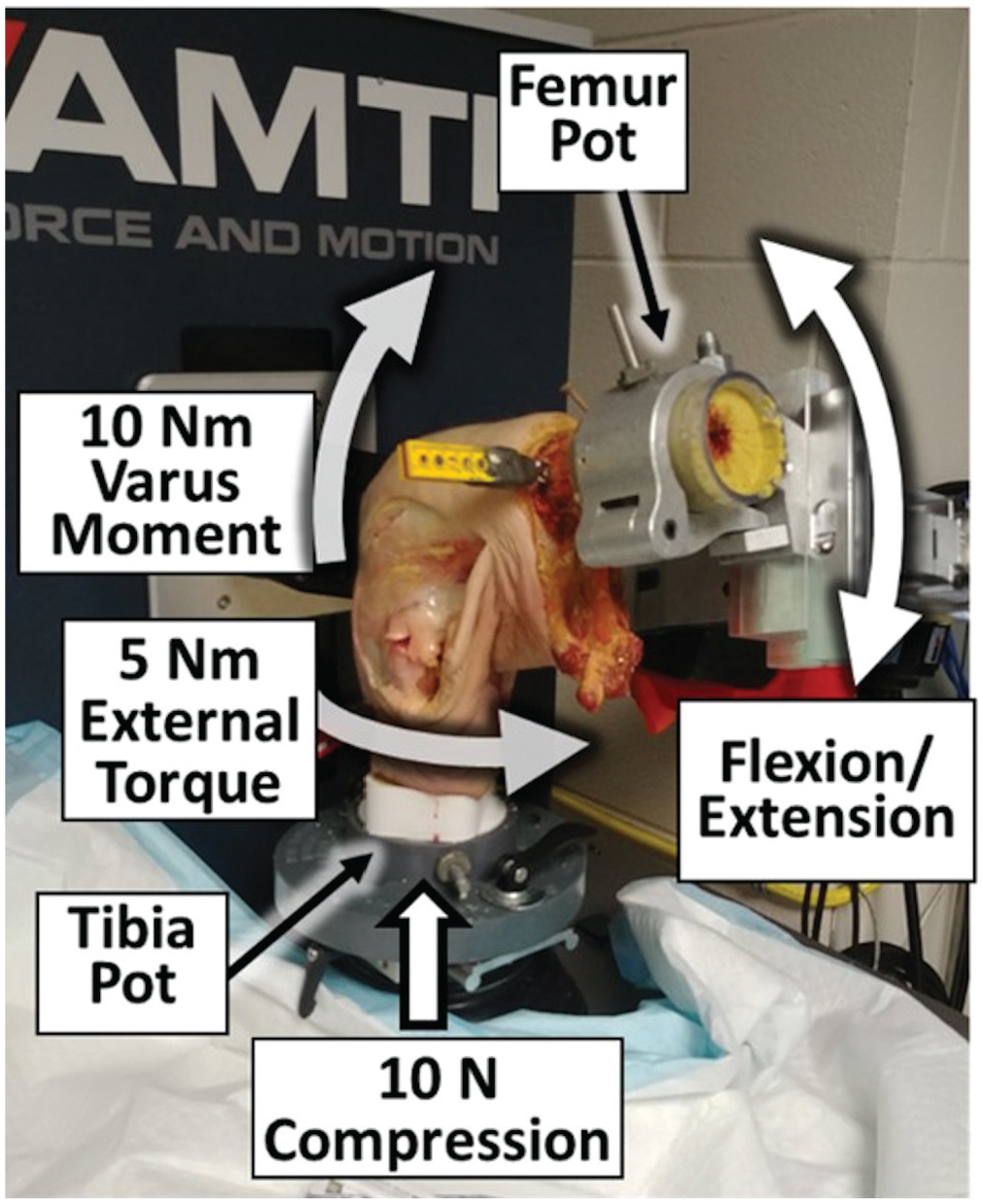
Cadaveric knee specimen shown mounted onto the joint motion simulator. Custom tibial and femoral pots secure the specimen and are adjustable to align (1) the long axis of the tibia with the vertical axis of the tibial pot and (2) the flexion axis of the knee with the flexion axis of the femoral pot. Specimen alignment is modified from the original joint motion simulator convention: the anterior tibia faces toward the back of the machine, and flexion of the femur is controlled using a supplementary high-torque stepper gearmotor.
Each knee was subjected to force-controlled loading scenarios designed to assess varus and external rotatory laxities. In a previous study with similar loading rates, the largest dynamic force- and torque-control errors of the joint motion simulator were 4.6 N (inferior/superior force) and 0.2 N·m (internal/external torque). 18 Resulting kinematics were measured (accurate to 0.1 mm and 0.1°) through sensors embedded in the actuators of the joint motion simulator. Forces and kinematics were described by the coordinate conventions of Grood and Suntay. 7
Testing Protocol
The varus/valgus and internal/external rotation during neutral flexion with a 10-N compressive load was measured at 0°, 30°, 60°, and 90° of flexion. The maximum achievable varus and external tibial rotation angles of the knee were then measured while separately applying 10-N·m varus moments and 5-N·m external rotatory torques at 0°, 30°, 60°, and 90° of flexion. These measurements were tested under 3 conditions: (1) intact FCL, PT, and PFL; (2) complete transection of the FCL, PT, and PFL; and (3) PLC reconstruction. The loads applied in this biomechanical analysis were based on previous studies of knee laxity.8,20,23
Sectioning Protocol, Graft Preparation, and Reconstruction Procedures
Pairs of knees were randomly assigned to the original or modified technique (n = 8). Under guidance from the senior author (A.M.G.), an orthopaedic fellow (T.V.) performed all the surgical procedures. After the intact testing, the primary stabilizers of the PLC were sectioned while mounted on the joint motion simulator. The posterior proximal tibiofibular joint capsule was also incised to create a “worst-case scenario” of external rotatory laxity.
After testing of the PLC-injured state, the knee was removed from the joint motion simulator and placed in a cadaveric leg holder (Sawbones Inc). The original PLC technique was performed per the original technique description, 15 using a split Achilles tendon allograft prepared with bone blocks (diameter, 8 mm). Both tendons were tensioned with a 20-N static load for 10 minutes before the reconstruction. PEEK interference screws (polyether ether ketone; Smith & Nephew Ltd) were used for graft fixation at the femoral, tibial, and fibular head attachments.
The modified anatomic reconstruction was performed as previously described with the autologous semitendinosus tendon 24 and harvested from the same cadaveric model. In the event where the semitendinosus tendon was <25 cm, a peroneus longus autograft from the same cadaver was used instead. This occurred in 1 of the 16 specimens.
PEEK interference screws were used at the femoral and fibular head attachments, and a cortical adjustable-loop suspension fixation, applied over a metal washer (Ultrabutton; Smith & Nephew Ltd), was used at the tibial attachment of the PT and PFL. For either technique, both tendons were tensioned with a 20-N static load for 10 minutes before the reconstruction.
The protocol for graft tension was similar in both surgical techniques. Reconstructions of the FCL were tensioned at 30° of flexion and neutral rotation. Valgus force was applied while the FCL reconstruction graft was tensioned and fixed in the fibular head. The PT and PFL were tensioned at 70° of flexion and neutral rotation. For the modified technique, the PT and PFL limbs of the graft are gradually retensioned by using the Ultrabutton.
After reconstruction, the knee was remounted on the joint motion simulator. The position and orientation with respect to the joint motion simulator remained consistent with earlier testing stages owing to the design of the fixtures, which uniquely and unambiguously reassemble, and proper reassembly was verified through the optical motion capture system.
Statistical Analysis
Repeated measures analysis of variance with a Greenhouse-Geisser correction was performed to determine the effects of joint condition (intact, PLC cut, and PLC reconstructed) and flexion angle when interacting with surgical reconstruction technique (original anatomic vs modified anatomic) on joint kinematics and laxity. Post hoc comparisons of means with a Bonferroni correction were used to compare the effects of the surgical reconstruction techniques on the change in the maximum varus and external tibial angulations (with respect to intact) at flexion angles of 0°, 30°, 60°, and 90°. All comparisons were performed with a threshold of α = .05 for statistically significant differences. Based on a total sample size of 16 (8 in either surgical reconstruction group), this study was adequately powered (80%) to find effect sizes >1.45 (very large).
Results
One specimen (modified anatomic group) exceeded the test apparatus varus range of limit at 90° of flexion after the PLC injury, but this was no longer an issue after the reconstruction. Therefore, any statistical comparisons with the varus laxity at the PLC injury stage have excluded that specimen.
Neutral Flexion Kinematics
There were no significant differences in the internal/external rotational kinematics by using the original (P = .509) or modified (P = .152) anatomic technique with respect to the intact joint behavior. There was also no difference in the internal/external kinematics of the 2 reconstructions (P = .222). In terms of varus/valgus kinematics, there were no significant differences with respect to intact joint behavior with either reconstruction technique (P = .554, original anatomic; P = .862, modified anatomic). Furthermore, the varus/valgus behaviors of the reconstructed joints were not different (P = .698).
External Rotation Laxity
The mean external rotation limits of the knees in the 2 reconstruction groups did not differ from each other when in the intact (P = .737) or PLC-injured (P = .986) state (Figure 3). When both groups were considered together, the simulated PLC injury had a significant effect (P < .001), increasing the external rotatory laxity by 5.7°± 3.4° (mean ± SD). When the external rotation limits of the reconstructed versus intact states were compared, there were no significant differences for knees reconstructed with the original anatomic technique (P = .403). Knees reconstructed using the modified anatomic technique, however, had a statistically significant reduction in the external rotation limit (with respect to intact joint) of 4.1°± 6.3° (P = .036) and 5.1°± 6.6° (P = .016) at 60° and 90° of flexion, respectively. Statistically, there was no difference between the outcomes of the 2 procedures (P = .112).
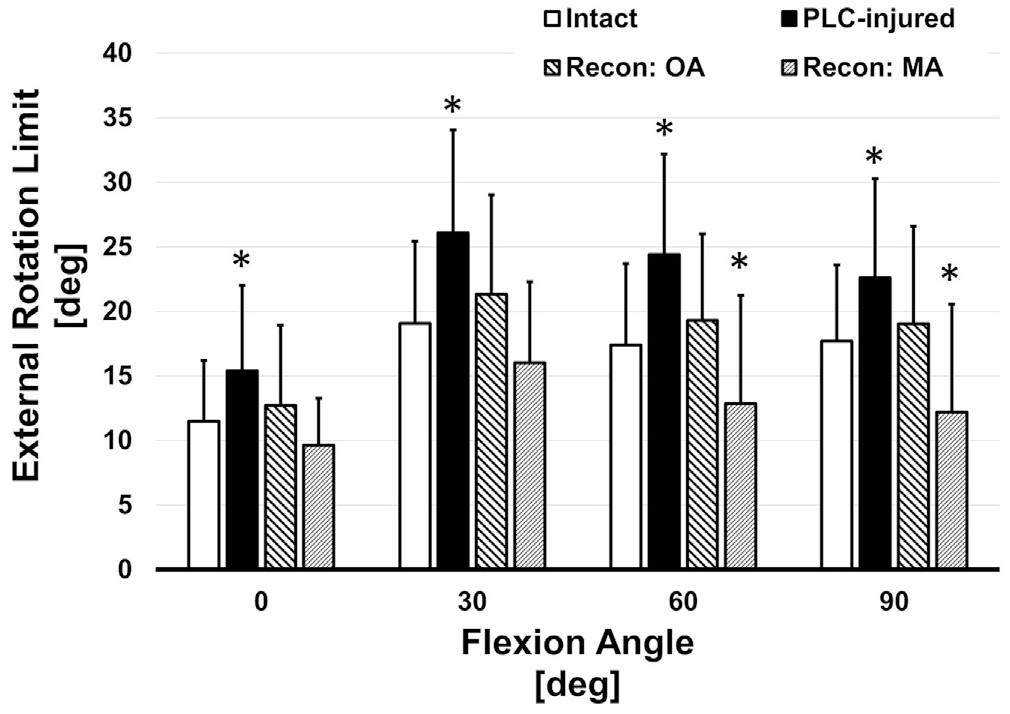
External rotation limits of intact, PLC-injured, and reconstructed knees (original anatomic [OA] and modified anatomic [MA]) measured while applying a 5-N·m external rotation moment. *Statistically significant differences (P < .05) from intact knee external rotation limits. Values are presented as mean ± SD. PLC, posterolateral corner.
Varus Laxity
The mean varus limits of the knees in the 2 reconstruction groups did not differ from each other when in the intact (P = .671) or PLC-injured (P = .957) state (Figure 4). With both groups together, the simulated PLC injury increased the varus laxity by 3.5°± 2.2° (P < .001). After PLC reconstruction, both techniques yielded outcomes that were not significantly different from the intact state (OA P≥ .999 and MA P = .117, respectively), and there was not a significant difference between the outcomes of the 2 procedures (P = .074).
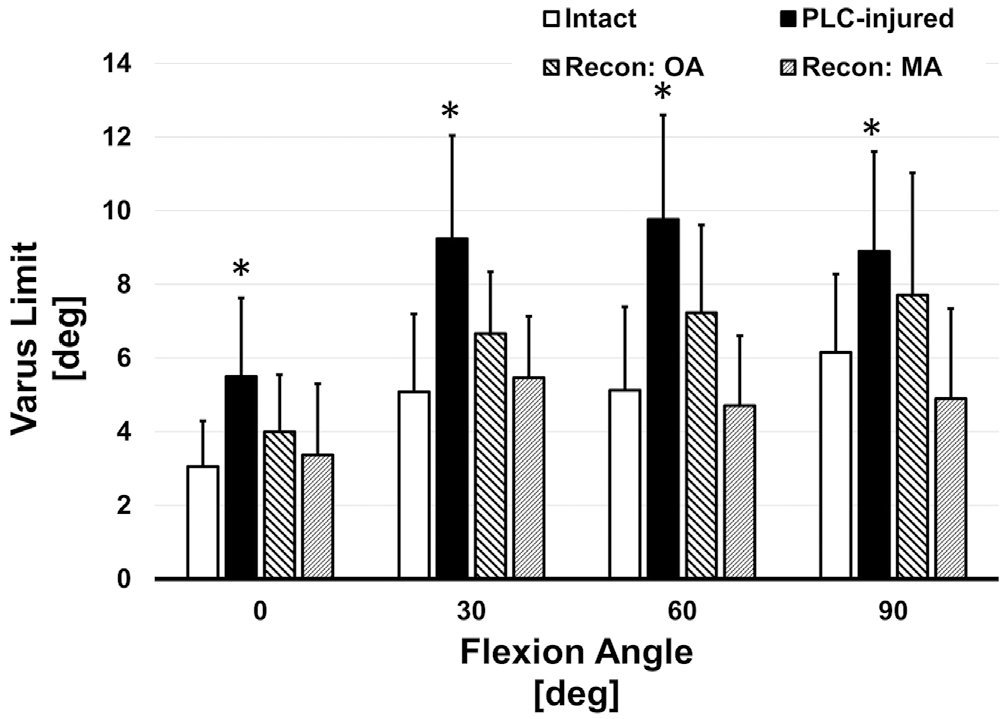
Varus limits of intact, PLC-injured, and reconstructed knees (original anatomic [OA] and modified anatomic [MA]) measured while applying a 10-N·m varus moment. *Statistically significant difference (P < .05) from intact knee varus limits. Values are presented as mean ± SD. PLC, posterolateral corner.
Discussion
The most important finding from this study was that the modified anatomic PLC reconstruction, using a single autograft fixated with an adjustable-loop suspensory device on the tibia, restored stability to a simulated PLC-injured cadaveric knee to a similar degree when compared with the original anatomic technique. Furthermore, both reconstruction techniques restored knee kinematics in PLC-injured knees close to the intact state.
The complete transection of the FCL, PFL, and PT significantly increased the maximum varus and external tibial rotatory laxity across all flexion angles as compared with the intact knee. These findings confirmed that even in knees with an intact anterior cruciate ligament and posterior cruciate ligament, these 3 structures are critical to controlling external rotation and varus knee laxity. After reconstruction, both anatomic surgical techniques tested were able to restore (or increase) the varus and external rotatory stability as compared with the intact state. Furthermore, no differences were seen in these parameters when comparing the 2 reconstruction techniques.
A significant increased constraint of external rotation with the modified anatomic technique was observed at 60° and 90° of flexion. Importantly, however, this was not observed in the neutral flexion kinematics, where no statistically significant differences in the internal/external rotation kinematics through the flexion path were observed, indicating no internal rotation contracture in flexion. The loss of end-range external rotation in flexion may be partly due to the difficulty of controlling tibial rotation in a cadaveric model, where the tibia was hanging freely in the leg holder during tensioning. In the clinical setting, this would be easier to control by foot position. Furthermore, the use of the adjustable loop has the potential of being “overtightened,” owing to the difficulty of measuring tension with this device. As such, it is recommended that the adjustable-loop suspensory button be gradually tensioned with the tibia held in a neutral position to avoid overconstraining rotation.
Multiple biomechanical studies have been performed investigating the variety of PLC reconstruction procedures that have been developed over the past 2 decades.1-5,9-11,15,17,19,23 LaPrade et al 12 extensively investigated the anatomic and biomechanical properties of the PLC, developing the concept of an anatomic reconstruction based on re-creating the kinematic properties of 3 key ligaments: the FCL, PFL, and PT. The original technique required the use of an Achilles tendon allograft, as 2 grafts are required to enable differential tensioning of the 2 main components of the reconstruction: the FCL and the PT/PFL complex. 15 Proponents of this technique state that the addition of the PFL and PT element to the reconstruction helps improve external rotation laxity control by stabilizing the proximal tibiofibular joint, while detractors articulate the addition of a PT component creates a falsely constrained tibiofemoral articulation on the lateral side. This issue was highlighted by Nau et al, 19 who studied a complex anatomic PLC reconstruction, albeit different from the LaPrade technique, that included a static femorotibial PT graft, as compared with the modified Larson fibular-based technique using 2 femoral tunnels. Both techniques restored external rotation and varus laxity levels as compared with the intact knee, although the anatomic reconstruction increased the internal rotation torque, indicating constraint of external rotation in flexion with resultant internal rotation. Importantly, this effect was not observed in the current study, indicating that the end-range external rotation was affected only by the modified anatomic procedure, and no internal rotation contracture occurred.
The complexity of the 2 grafts and the 3 tunnels has led many surgeons to prefer the easier nonanatomic fibular-based reconstructions. In combination with the rigorous preclinical and clinical validation of the anatomic LaPrade technique, one of the indications for the use of an anatomic reconstruction in the senior author’s practice is the control of the proximal tibiofibular joint, which can often be unstable in the multiple ligament–injured knee. 21 Interestingly, in a cadaveric study by Treme et al 23 comparing the LaPrade anatomic reconstruction with the fibular-based Arciero technique, no significant differences were observed in terms of controlling external rotation or varus laxity. However, when further sectioning of the proximal tibiofibular joint was performed (no clear description of how extensive this was), neither reconstruction was able to control rotation. In comparison with the current study, where a more complex sectioning of the PFL and posterior tibiofibular joint capsule was made to ensure a worst-case scenario for PLC injury, the original and modified techniques were able to return the sectioned knees back to the intact state, indicating satisfactory efficacy of both reconstruction procedures.
One of the significant barriers to uptake of the anatomic LaPrade technique has been the availability or cost of allograft tissue in some countries. Franciozi et al 6 published the clinical results of a technique using semitendinosus and gracilis autografts in a similar manner to the modified LaPrade technique as described in this study. However, they used a fixed-loop suspensory device on the tibial side, which may not provide the same degree of opportunity for differential tensioning as the adjustable loop. The use of a gracilis tendon also may influence the ability to perform the reconstruction, given the length of the graft. We have found that a semitendinosus tendon of at least 25 cm is required to perform this reconstruction, accounting for 2 cm of graft in each femoral tunnel, 3 cm in the fibula, 3 cm in the tibia (1.5-cm loop), 7 cm for the FCL, 2 cm for the PFL, and 6 cm for the PT. The use of the adjustable-loop device enables the minimum amount of tissue to be pulled into the tibial tunnel to preserve graft length. In cases where a semitendinosus graft is not long enough or the procedure is being performed in larger patients, a peroneus longus autograft may be utilized. 22 Alternatively, a contralateral semitendinosus graft may be harvested, and a traditional 2-graft anatomic LaPrade PLC reconstruction may be performed.
As with most cadaveric studies, there are some limitations to the clinical application of this study. The cadaveric specimens used were older than the average patient presenting with this type of injury pattern. This results in reduced bone quality and inferior soft tissue viscoelastic proprieties as compared with the young population that is more commonly involved in PLC injuries. Additionally, the kinematic analysis presented in this study does not include graft healing and the postoperative graft stretching frequently seen after PLC reconstruction. Last, it is possible that the study is underpowered to determine noninferiority between reconstructions.
Conclusion
In this cadaveric laboratory study, the modified anatomic single-graft PLC reconstruction utilizing an adjustable-loop suspensory fixation device on the tibia restored varus and external rotatory laxity of a PLC-injured knee back to the intact state. No statistically significant differences were observed between it and the original anatomic LaPrade technique. The use of a single autologous graft to perform a full anatomic PLC reconstruction is advantageous in countries where allograft is unavailable or cost-prohibitive, in cases where the use of autograft is limited because of multiple-ligament reconstruction, and in patients who decline the use of allograft tissue.
Footnotes
Submitted June 2, 2021; accepted November 15, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was sponsored through a research grant by Smith & Nephew. A.M.G. is a consultant for Smith & Nephew, Xiros, Olympus, and Precision OS, and receives research support from Smith & Nephew and Ossur. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.