
Abstract
Background:
Elbow flexion at late portions of the pitch has been associated with increased elbow varus torque, a kinetic surrogate associated with injury risk. Direct examinations of injury incidence with elbow flexion angles have not been conducted in professional pitchers.
Purpose:
To compare elbow and shoulder injury incidence among professional baseball players stratified by degree of elbow flexion at ball release (BR).
Study Design:
Descriptive laboratory study.
Methods:
Professional pitchers (N = 314) were instructed to pitch between 8 and 12 fastballs while being evaluated using motion capture technology. Upper extremity injury incidence was recorded upon interview. Pitchers were subsequently subdivided into 3 groups based on increasing elbow flexion at BR. Analysis of variance was used to compare participant characteristics and kinematic and peak kinetic variables. An odds ratio (OR) was calculated to determine the risk of having a previous upper extremity injury based on the degree of elbow flexion at BR.
Results:
A total of 116 pitchers (132 documented injuries) had a previous upper extremity injury, with elbow injury (76 injuries; 57.6%) being the most common. Evaluation of kinetic values showed that pitchers with the smallest elbow flexion at BR had significantly less peak elbow flexion torque than did those with greatest elbow flexion at BR (3.8 ± 0.5 vs 4.1 ± 0.6 %weight × height; P = .003). Pitchers who demonstrated a greater than average degree of elbow flexion at BR when pitching were more likely to have a history of elbow injury (OR, 1.97; 95% CI, 1.14-3.40; P = .015) and olecranon spur formation or stress fracture (OR, 5.79; 95% CI, 1.25-26.85; P = .025).
Conclusion:
Pitchers with greater elbow flexion at BR had significantly higher odds of previous injury of the elbow and olecranon. Increasing elbow flexion has been shown to place the medial elbow in a position to carry a greater amount of load, which may be exacerbated during the final moments of the pitching motion. Professional pitchers can consider decreasing elbow flexion at BR as a potential, modifiable risk factor for elbow injury, in particular for olecranon spur formation and fracture.
Clinical Relevance:
This study attempts to associate injury incidence with a modifiable, kinematic variable for an at-risk population.
Professional baseball, with >1000 players in Major League Baseball (MLB) and >5000 players in Minor League Baseball, is plagued by injuries. These injuries can cost teams victories and millions of dollars of revenue each year but, most importantly, can forever alter an individual pitcher’s career. 14 Injury rates have increased steadily for the past 20 years, with pitchers disproportionately affected.14,16,37 Pitchers make up 48% of injury list reports and account for >56% of days spent on the injury list. 15 The majority of injuries to pitchers affect the throwing elbow (26.3%) and shoulder (30.7%). 37 Upper extremity pitching injuries are predominantly noncontact injuries and include ligament and tendon tears, osteophyte formation, and stress fractures.5,6 These injuries can be problematic setbacks for pitchers; in extreme cases, these injuries can jeopardize a ballplayer’s career. These noncontact injuries highlight the importance of proper pitching mechanics at all levels of play.1,13,17,24,27,29
Motion analysis technology allows researchers to identify favorable and unfavorable aspects of pitching mechanics. These aspects, or kinematics, are quantifiable variables that describe the positions of the body at various points throughout the pitching motion. Kinematic parameters can correlate with favorable attributes like increased ball velocity and accuracy and negative attributes like injury rates. Although static factors such as elbow range of motion have shown no correlation with injury rates in pitchers, 11 dynamic factors such as elbow varus torque (EVT) have been linked to both performance and rates of injury.2,7,39 EVT, as defined by Aguinaldo and Chambers, 2 is the bending moment about the elbow joint that causes increased compressive force on the lateral structures and tensile force on medial side structures.
The biomechanical basis of upper extremity injury in pitchers has been thoroughly investigated, with increased EVT associated with injury risk.7,12 The elbow is the weakest link of the kinetic chain of the pitching motion and can experience a valgus load of >115 N·m during maximum external rotation.13,22,44 Increased EVT places strain on the ulnar collateral ligament (UCL), which is the primary structure that resists valgus loading. Overexertion of the UCL can lead to tears that often require surgery.14,40 Increased EVT directly increases stress on the elbow joint, which Bennett and Brand 9 associated with formation of osteophytes at the olecranon process and medial epicondyle of the humerus. These osteophytes are a major source of pain and disability and may require operative excision in pitchers.
One kinematic variable that has been directly linked to EVT, used as a surrogate for elbow joint loading in motion capture studies, is elbow flexion at ball release (BR)2,12,44 and after BR. 41 Several theories about the role of elbow flexion in the pathomechanics of shoulder and elbow injury have been postulated. Elbow flexion increases the length of the lever arm as well as the inertial moment of humeral rotation. Sabick et al 38 found that humeral fractures in pitchers were generally spiral in nature, suggesting that such fractures are caused by this increased humeral torsion. Elbow flexors and extensors serve a protective role against humeral torsion by generating compressive axial loads,10,28 but this protection may diminish as a pitcher fatigues. Although elbow flexion has been theorized to be a risk factor for upper extremity injury, no study has demonstrated a direct link between elbow flexion and increased injury. Therefore, the purpose of this study was to compare elbow and shoulder injury incidence among professional baseball players stratified by degree of elbow flexion at BR. We hypothesized that increased elbow flexion would be associated with higher EVT as well as an elevated incidence of previous elbow injury.
Methods
Player Enrollment
The data sets of the participants selected for this study were from baseball pitchers who had previously undergone a 3-dimensional biomechanical pitching assessment between 2013 and 2017, provided by Motus Global.33,34 Inclusion criteria were: (1) at the time of testing, pitchers were currently on the MLB or Minor League Baseball (Low A, High A, AA, and AAA) roster and (2) pitchers had no record of serious injury (requiring >2 weeks of rest or rehabilitation) in the past 6 months. All data were deidentified, and an exemption was granted by our institutional review board at the Hospital for Special Surgery (NY, NY).
Player Data Collection
Pitchers reported to the test site, provided their consent, and were administered privacy waivers. Pitchers provided data regarding age, sex, throwing arm, and experience level. Pitchers were also asked to report on any injury within the past 10 years including date of injury, time missed because of injury, and any surgical interventions. Pitchers reported these previous injuries using their own terms and vernacular, which were later clarified when communicating with supporting staff. Research staff then measured and recorded each pitcher’s height and weight.
Pitching Assessment
Pitchers were given unlimited time to warm up with their preferred routine (eg, arm bands, stretching, plyometric care, long-toss). When the pitcher was ready, he had 46 reflective markers placed on anatomic landmarks as previously described by Luera et al. 32 An 8-camera Raptor-E motion analysis system (Motion Analysis Corp) was used to record the marker data at 480 Hz.
At regulation distance (18.4 m), pitchers were instructed to pitch between 8 and 12 fastballs off a mound with gamelike effort to a catcher behind home plate. The pitchers were allowed to pitch from the wind-up or stretch, as previous research has shown no difference in mechanics between the 2 types. 19 Ball speed was collected using a radar gun located behind the pitcher (Stalker Sports Radar).
Data Processing
Kinematic and kinetic analysis was performed using custom scripts in MATLAB (MathWorks) as previously described by Luera et al. 32 Data from the markers were filtered using a low-pass filter (fourth-order, zero-lag Butterworth filter; 13.4-Hz cutoff frequency). 31 Pitch time began at foot contact and ended at BR. Foot contact was defined as the first frame when the lead toe or heel had reached the minimum in the z-axis. Maximum shoulder external rotation was established as the maximum angle formed between the forearm and an anterior-posterior line created in the z-axis of the elbow joint. BR was established at 0.01 seconds after the wrist passed the elbow in the forward direction.18,31 Shoulder rotation was the angle formed between the forearm and the anterior-posterior line created in the z-axis of the elbow joint. 43 The angle between the distal directions of the upper arm and forearm of the throwing arm was used to define elbow flexion. 21 Kinetic values collected included shoulder internal rotation torque, elbow varus torque, elbow medial force, elbow anterior force, elbow flexion torque, and elbow distractive force. All forces and torque values were normalized by player body weight (BW) and BW multiplied by player body height (BH), respectively.31,32
Statistical Analysis
Pitchers with no injury history were included for final analysis, and upper extremity injury incidence was identified and characterized for the remaining pitchers. Pitchers who fit the following 2 criteria for injury characterization were excluded from analysis in an attempt to most accurately characterize comparable injury types. (1) We excluded pitchers with any injury occurring <1 year from testing or >4 years from testing. This was done to reduce the effect of factors such as aging, minor injuries, reduced ball velocity, and changes in pitching approach that change over time as well as reduce the incidence of recall bias for injuries that had occurred in the more distant past. 25 (2) We excluded pitchers with previous injury who missed <1.0 months or >12.0 months of play in order to adequately characterize an injury of sufficient and similar severity.
Pitches were then averaged per pitcher for all calculations, with both strikes and balls included. Pitchers were subdivided into 3 groups based on increasing elbow flexion at BR to better characterize the kinetic and kinematic variables of pitchers that differ by elbow joint angle (ie, EF1 < EF2 < EF3). Analysis of variance was used to compare demographic, kinematic, and peak kinetic variables. For each elbow flexion group, a Fisher-Freeman-Halton exact test was conducted to assess for significant differences in the incidence of injury in any of the following categories: general shoulder, general elbow, elbow tendinitis, UCL sprain or tear, olecranon fracture, superior labrum anterior to posterior (SLAP) tear, and rotator cuff tendinitis or impingement.
As an additional means of analysis, average elbow flexion at BR was compared between pitchers in injury categories versus noninjured pitchers using Wilcoxon rank sum test to account for nonparametric distributions and varied number of pitchers in each subgroup of comparison. An a priori test for elbow flexion at BR was conducted. With an anticipated effect size (Cohen d) of 0.5, desired statistical power of 0.8, and α value of .05, it was determined that a minimum total sample size of 102 pitchers was required. Lastly, an odds ratio (OR) with 95% CI was calculated to determine the odds of having a history of a specific injury based on the degree of elbow flexion at BR. An “exposure” was defined as having elbow flexion at BR greater than the mean value for the entire population (N = 314). The OR was calculated by comparing the ratio of previous injury occurrence in the exposed group to no previous injury occurrence in the exposed group versus the ratio of previous injury occurrence in the control group to no previous injury occurrence in the control group. Statistical significance was set at an α value of .05. Statistical analyses were performed using MATLAB Version R2020a (MathWorks).
Results
A total of 314 professional pitchers were ultimately included in the final analysis. Of the 132 previous upper extremity injuries (n = 116 pitchers), elbow injury (n = 76; 57.6%) was the most common, followed by shoulder injury (n = 35; 26.5%). The most common previous injury was UCL tear or sprain (n = 46; 34.8%), followed by SLAP tear (n = 20; 15.2%) and olecranon spur formation or stress fracture (n = 12; 9.1%). In total, 29 (25%) pitchers with a history of upper extremity injury reported 1 additional previous injury. We noted that 49 (42.2%) pitchers with a previous upper extremity injury underwent surgical management of their injury. The mean ± SD time missed because of injury was 2.8 ± 3.4 months for pitchers who did not receive surgical intervention versus 11.1 ± 2.2 months for the surgical cohort. Upper extremity injury incidence for the entire cohort is reported in Table 1.
Upper Extremity Injury Incidence of Professional Cohort Evaluated a
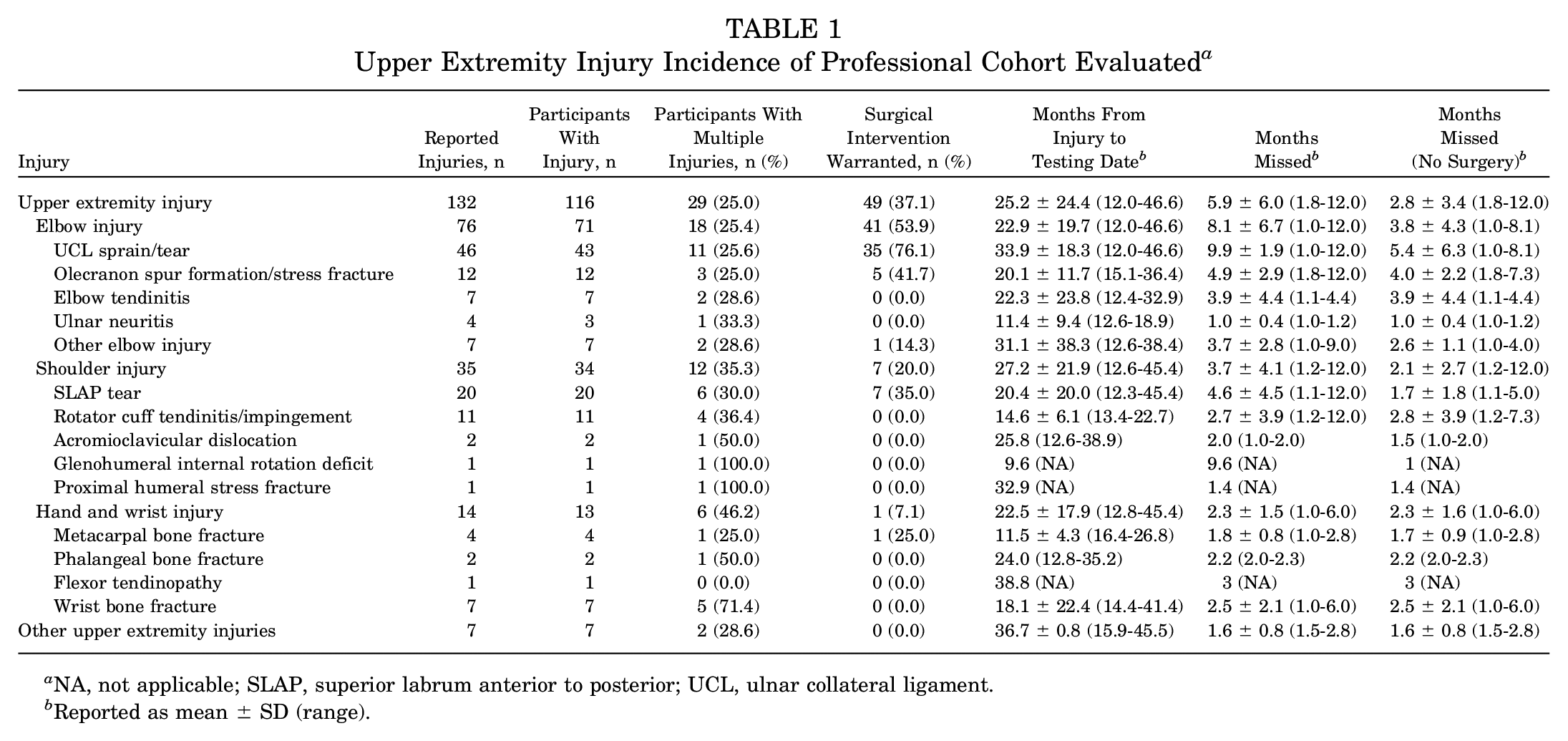
NA, not applicable; SLAP, superior labrum anterior to posterior; UCL, ulnar collateral ligament.
Reported as mean ± SD (range).
Table 2 provides demographic, kinematic, and kinetic values for pitchers subdivided into groups based on elbow flexion at BR (EF1 = 25.5°± 2.7°; EF2 = 31.8°± 1.7°; EF3 = 38.4°± 3.0°). Pitchers with the greatest degree of elbow flexion at BR, the EF3 cohort, had a significantly higher body mass index than all other cohorts, in addition to the study population as a whole (EF1 = 25.7 ± 2.2; EF2 = 26.2 ± 2.1; EF3 = 27.0 ± 2.6; Population = 26.3 ± 2.4 kg/m2; P = .001). The EF3 cohort had significantly greater forearm pronation at BR compared with the EF1 cohort (6.5°± 13.8° vs –0.4°± 13.5°, respectively; P < .001) and also had the longest pitch time (EF1 = 167.9 ± 19.3; EF2 = 171.3 ± 19.0; EF3 = 179.9 ± 25.1; Population = 173.0 ± 21.8 milliseconds; P < .001). In evaluation of kinetic values, pitchers with the smallest degree of elbow flexion at BR, the EF1 cohort, had significantly smaller peak elbow flexion torque compared with all other cohorts (EF1 = 3.8 ± 0.5; EF2 = 4.1 ± 0.7; EF3 = 4.1 ± 0.6; Population = 4.0 ± 0.6 %BW×BH; P = .003).
Characteristics of Professional Pitcher Cohorts by Degree of Elbow Flexion at Ball Release a
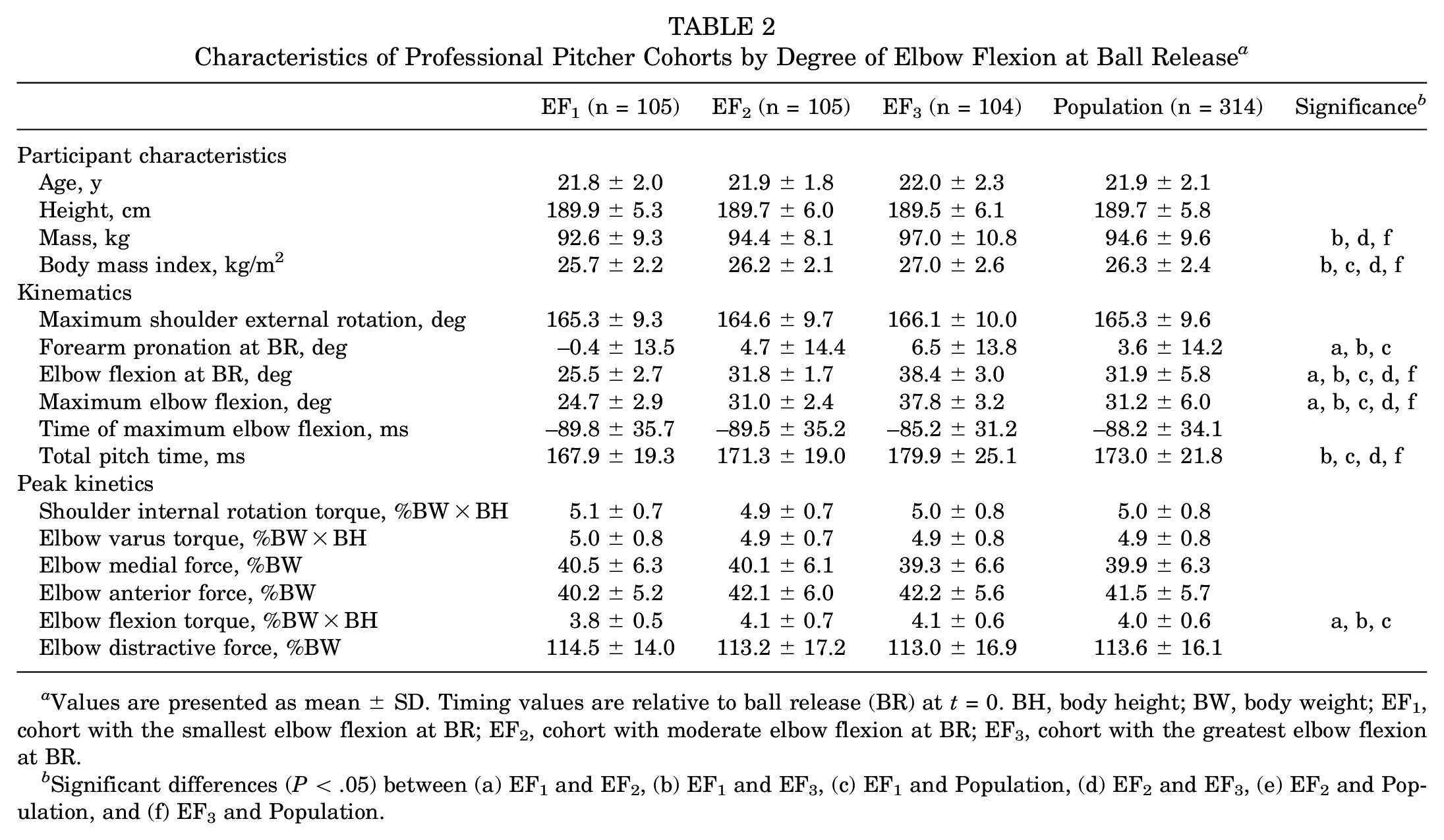
Values are presented as mean ± SD. Timing values are relative to ball release (BR) at t = 0. BH, body height; BW, body weight; EF1, cohort with the smallest elbow flexion at BR; EF2, cohort with moderate elbow flexion at BR; EF3, cohort with the greatest elbow flexion at BR.
Significant differences (P < .05) between (a) EF1 and EF2, (b) EF1 and EF3, (c) EF1 and Population, (d) EF2 and EF3, (e) EF2 and Population, and (f) EF3 and Population.
Comparison of upper extremity injury incidence and history in the elbow flexion groups is shown in Table 3. Pitchers with the most elbow flexion at BR, when compared with pitchers who had the smallest amount of elbow flexion at BR, had a significantly higher incidence of upper extremity injury (48, 46.2% vs 27, 25.7%, respectively; P = .003), elbow injury history (32, 30.8% vs 12, 11.4%, respectively; P < .001), and olecranon spur formation or stress fracture history (7, 6.7% vs 0, 0.0%, respectively; P = .003). No other injury categories showed significant differences between groups.
Fisher Exact Test for Injury Incidence by Elbow Flexion at Ball Release Percentiles a
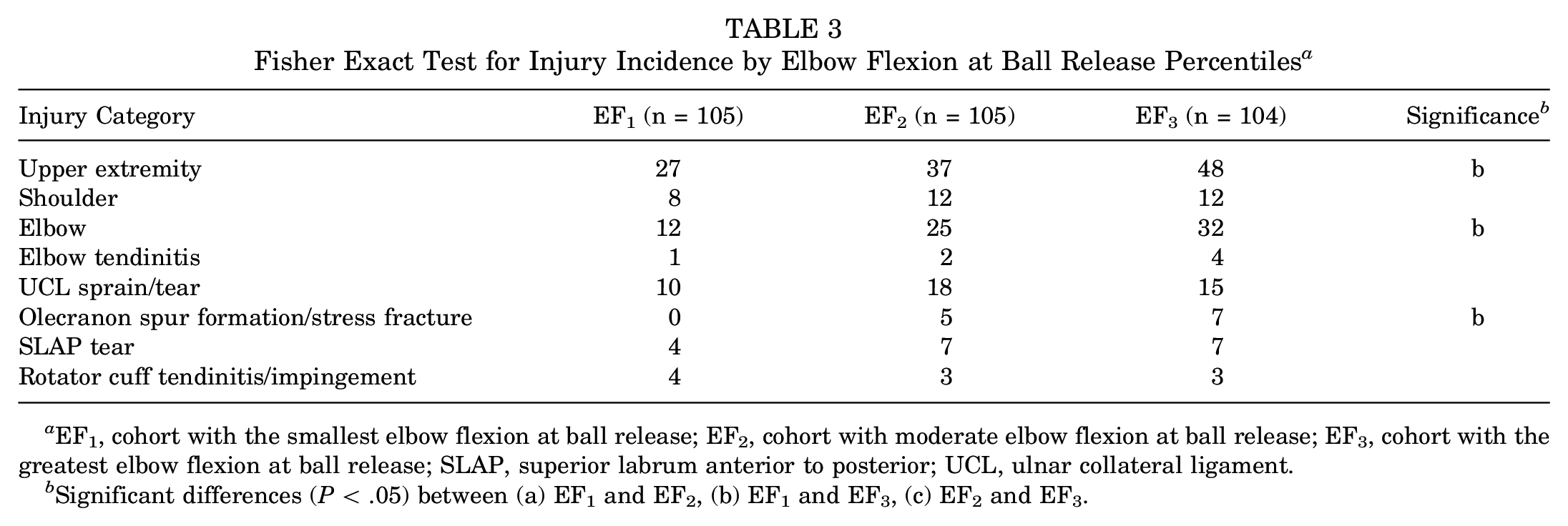
EF1, cohort with the smallest elbow flexion at ball release; EF2, cohort with moderate elbow flexion at ball release; EF3, cohort with the greatest elbow flexion at ball release; SLAP, superior labrum anterior to posterior; UCL, ulnar collateral ligament.
Significant differences (P < .05) between (a) EF1 and EF2, (b) EF1 and EF3, (c) EF2 and EF3.
Average elbow flexion at BR by previous injury type was compared with data for pitchers with no history of injury, and ORs were calculated (Table 4). Pitchers who demonstrated a greater than average degree of elbow flexion at BR when pitching were more likely to have a history of elbow injury (OR, 1.97; 95% CI, 1.14-3.40; P = .015) and history of olecranon spur formation or stress fracture (OR, 5.79; 95% CI, 1.25-26.85; P = .025). Although previous upper extremity injury and UCL sprain or tear did not derive significant OR calculations, pitchers with these previous injuries were noted to have a significantly greater degree of elbow flexion at BR compared with pitchers with no previous injury (P = .006 and P = .040, respectively).
Descriptive Measures and Odds Ratios for Risk of Previous Injury Determined by Degree of Elbow Flexion at Ball Release a
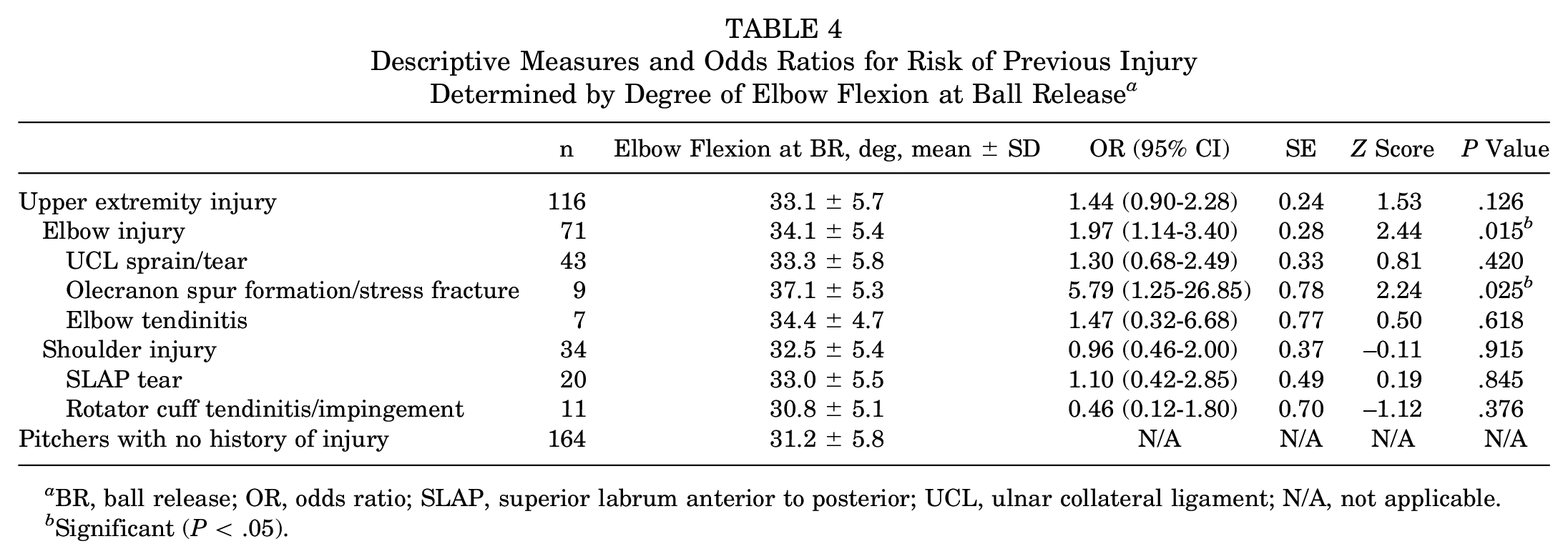
BR, ball release; OR, odds ratio; SLAP, superior labrum anterior to posterior; UCL, ulnar collateral ligament; N/A, not applicable.
Significant (P < .05).
Discussion
Previous studies have suggested that elbow flexion at BR may be a modifiable kinematic parameter that can reduce the incidence of elbow injury in baseball pitchers2,12,39,41; this study is the first to report a direct link between elbow flexion angle and a higher odds of previous elbow injury. The major findings of this study were as follows: (1) Pitchers with greater elbow flexion at BR had a significantly higher incidence of previous injury of the upper extremity, elbow, or olecranon, and (2) a significantly higher peak elbow flexion torque was noted in pitchers with greatest elbow flexion at BR. On the basis of our results, professional pitchers may consider decreasing elbow flexion angle at BR as a potential strategy for reducing the risk of elbow injury.
Previous motion capture studies have postulated that elbow flexion at BR leads to elevated risk of elbow injury in pitchers, yet this is the first series to our knowledge that has used injury incidence data in professional pitchers.2,39,41 As the elbow flexes, the osseous congruence of the elbow joint decreases, exposing the medial and posterior portions of the elbow to stress. The force distribution about the elbow joint becomes less widely distributed across soft tissue structures and articulating surfaces, localizing peak loads to smaller regions. Coupling this phenomenon with the acceleration phase of the pitch where the elbow moves to a position of extension at a rate of 2300 deg/s, even the slightest angle change in flexion can significantly redistribute the tensile force distribution about the elbow joint.
Cadaveric studies have substantiated elbow joint load redistribution when moving from positions of flexion to extension. 35 In full elbow extension, the UCL is subjected to 31% of the total joint torque, whereas the bony congruence and other soft tissue structures account for the remaining 69%.20,35 However, as the elbow is flexed to 90°, the contribution of the UCL to resist the moment increases to 54%. 35 When extrapolated to the pitching cycle, increased elbow flexion places the UCL in a position to carry a greater amount of the elbow torque. 41 Although our OR calculations did not directly support the correlation between this increased tensile load and the incidence of UCL injury, pitchers with previous UCL sprain or tear did demonstrate significantly greater elbow flexion at BR when a direct t test was used to compare these pitchers versus those with no previous injury (P = .040). Ultimately, more data are needed to elucidate the relationship between UCL injury risk and the degree of elbow flexion at BR.
Elbow flexion at BR also had a positive correlation with olecranon injury history, a diagnosis most common in children given the open physis. 30 A pathophysiological mechanism by which elbow flexion at BR can put pitchers at risk of olecranon fracture was not intuitive to us, given that the relative contribution of the joint articulation to valgus stability increases with extension rather than flexion.3,35 Alternatively, one can consider that pitchers increase elbow flexion at BR as a consequence of these previous olecranon fractures. Humeral hypertrophy, decreased volume of the olecranon fossa, and olecranon process hypertrophy have all been noted in professional pitchers evaluated using radiographic imaging. 30 As olecranon size increases, its abutment into the fossa can be thought to occur earlier and with less extension. If the fossa also decreases in size, decreased area is available for smooth engagement. In an effort to reduce the amount of contact of these surfaces, which may bring about posteromedial pain or discomfort, these pitchers release the ball before the elbow reaches full extension; interestingly, pitchers with the greatest elbow flexion at BR also notably had the highest degree of maximal elbow flexion.
One can also consider the modeling work conducted by An et al, 4 who evaluated pressure distribution on articular surfaces. With the force directed at the center of the olecranon fossa, pressures are evenly distributed; however, with force applied toward the periphery of the articular surface, closer to the edge of the notch, contact pressure increases and becomes asymmetrically distributed.35,42 An et al demonstrated that even when the magnitude of the overall resultant joint force was low, the magnitude of peak pressure was relatively high given the decreased amount of available contact area. In an effort to minimize these peak pressures, pitchers with previous olecranon injuries may release the ball at larger flexion angles to avoid achieving these elevated forces at maximal extension, where contact shifts toward the periphery of the fossa.26,36 This adjustment diminishes the magnitude of load about the olecranon. However, these pitchers may in turn increase the amount of force distribution on the UCL at BR as an unintended consequence.20,35 Previous studies have highlighted the intricate relationship between UCL sprain and olecranon fracture. King et al 30 stated that with excessive valgus force, UCL laxity exacerbates impingement of the posteromedial olecranon within the olecranon fossa, demonstrating their complex interplay in posteromedial elbow stability. Ultimately, evaluating pitchers using radiographic imaging for olecranon hypertrophy, interviewing pitchers regarding discomfort at specified points of the pitch cycle, and conducting motion capture kinematic evaluation may provide a comprehensive assessment of these pitchers’ adaptations and differences.
In this study we noted significantly greater peak elbow flexion torque in pitchers with increased elbow flexion (EF3). Increased elbow flexion torque as a byproduct of increasing elbow joint angle is supported by Bechtel and Caldwell, 8 who noted that the highest flexion torque occurred at 90° of elbow flexion. Increasing flexion torque has previously been postulated as a risk factor for SLAP tears of the glenoid fossa as well as biceps tendinopathy, given the role that the biceps brachii plays in generating this torque. 23 The muscular contraction required to generate elbow flexion torque can place strain on the biceps tendon labrum complex through the attachment of the long head of the biceps brachii to the anterosuperior glenoid labrum. Although our study was unable to support this theory with injury incidence, future work should be directed toward evaluation of elbow flexion at BR as a risk factor for biceps tendinopathy or SLAP tears in larger motion capture and injury incidence evaluations.
Limitations of this study were as follows: (1) A small sample size of players with olecranon fracture history was analyzed (n = 12). Future studies should evaluate elbow flexion at BR as a risk factor for elbow injury on a larger scale. (2) Recall bias affected pitchers’ descriptions of injuries. There was, for example, a lack of characterization of the exact severity, location, or type of injuries pitchers incurred. Although this was a limitation, it should be noted most MLB Health and Injury Tracking System (HITS) studies use pitcher injury data only during a players tenure as a professional. HITS does not account for youth, high school, or college years, where additional injuries may have occurred. This study provides data on the history of pitcher injury up to 10 years before the motion capture assessment. (3) Only fastballs were analyzed in the current study, and therefore we are unable to extrapolate these results to other pitching types, including offspeed pitches. (4) It was unclear whether the kinematic variations seen in pitchers who have been injured previously occurred before the injury or arose as an adaptation to the injury. A potential study design would involve a prospective, longitudinal study evaluating pitcher kinematics before and after injury.
Conclusion
Pitchers with greater elbow flexion at BR had a significantly higher incidence of previous injury of the elbow and olecranon. Increasing elbow flexion has been shown to place the medial elbow in a position to carry a greater amount of load, which may be exacerbated during the final moments of the pitching motion. Professional pitchers can consider decreasing elbow flexion at BR as a potential, modifiable risk factor for elbow injury, in particular for olecranon spur formation and fracture.
Footnotes
Submitted June 17, 2021; accepted November 22, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.S.D. has received consulting fees from Arthrex, Linvatec, Merck Sharp & Dohme, Trice Medical, and Wright Medical and royalties from Zimmer Biomet and Linvatec and is a previous unpaid consultant for Motus Global. M.C.C. has received support for education from Liberty Surgical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.