
Abstract
Background:
The choice of surgical option for unstable large capitellar osteochondritis dissecans (OCD) lesions in skeletally immature athletes remains controversial.
Purpose/Hypothesis:
The purpose was to investigate functional and radiographic outcomes after arthroscopic fragment resection and osteochondral autograft transplantation (OAT) for unstable large capitellar OCD lesions in skeletally immature athletes with a minimum 5 years’ follow-up. We hypothesized that the outcomes after OAT for large capitellar OCD lesions would be superior to those after arthroscopic fragment resection.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A total of 19 elbows in 19 patients (17 male and 2 females) who underwent arthroscopic resection were assigned to group 1 (mean age, 14 years [range, 13-15 years]), whereas 29 elbows in 29 patients (29 male) who underwent OAT were assigned to group 2 (mean age, 14 years [range, 13-15 years]), with the mean follow-up of 8 (range, 5-11 years) and 7 (range, 5-13 years) years, respectively. All OCD lesions were larger than one-half of the radial head diameter. Functional scores, patient satisfaction, and range of motion were compared between the groups. Radiographic changes, including superior migration, radial head enlargement, and osteoarthritis (OA) grade, were examined.
Results:
All patients returned to sports activity. Functional scores, patient satisfaction, and flexion at the final follow-up were significantly improved in both groups compared with preoperative values, and differences were not significant between groups at the final follow-up. Extension showed a significant improvement in both groups (group 1: –17° to 0°; group 2: –18° to −6°; P < .001). Extension in group 1 was significantly better than that in group 2 at the final follow-up (P = .045). No elbows developed postoperative severe OA in group 1, whereas 3 elbows in group 2 had grade 3 OA; these 3 elbows had preoperative superior migration and radial head enlargement.
Conclusion:
No differences were observed in clinical and radiographic outcomes between patients undergoing arthroscopic fragment resection and OAT, except for elbow extension, at a minimum 5 years’ follow-up. We believe that for adolescents with large capitellar OCD lesion, OAT is a good option for skeletally immature elbows and that arthroscopic fragment resection is a reliable and less invasive surgical option for relatively mature elbows.
Keywords
Capitellar osteochondritis dissecans (OCD) frequently occurs in adolescent throwing athletes and gymnasts, 25 and surgical treatment is frequently indicated for unstable lesions. 26 Several studies have reported excellent functional and radiographic outcomes after arthroscopic fragment resection for unstable small capitellar OCD lesions.1,20,21,28 However, the choice of surgical options for unstable large capitellar OCD in skeletally immature athletes remains controversial: open or arthroscopic fragment resection,18-20,28 osteochondral autograft transplantation (OAT),4,10,16,22,23,31 fragment fixation,8,14 or closing-wedge osteotomy of the lateral condyle.12,29
OAT was developed for osteochondral lesions of the knee in the early 2000s,6,7 and several authors have reported good functional and radiographic outcomes after an OAT for large capitellar OCD lesions with good restoration of the joint congruity.4,10,16,22,23,31 We had been performing arthroscopic debridement and fragment excision exclusively for unstable OCD lesions since 2000. However, after we performed our first OAT procedure with cylindrical osteochondral autografts in 2007, OAT was randomly indicated for patients with large OCD lesions until 2011 to evaluate its efficacy. After 2011, we performed the OAT procedure exclusively for unstable large capitellar OCD lesions in patients with open contralateral radial physis. Therefore, we performed arthroscopic fragment resection for large lesions until 2011, but OAT is currently indicated for all large capitellar OCD lesions in skeletally immature athletes and arthroscopic fragment resection for unstable small lesions. 28
Only Matsuura et al 17 have reported long-term clinical outcomes after an arthroscopic fragment resection in adolescent athletes, with good outcomes at a mean 11.5 years. Other studies have reported that clinical outcomes after arthroscopic fragment resection for large OCD lesions in adolescent athletes were acceptable, but most studies were short-term case reports.1-3,13,21,26 Similarly, only Sato et al 22 have only reported mid-term outcomes after OAT in adolescent athletes, with good outcomes at a mean 4.8 years, but others have reported shorter-term follow-up studies.4,10,16,23,31 Osteoarthritic (OA) changes may occur at long-term follow-up after OAT, and high-level athletics and lateral capitellar lesions have been reported as factors for high risk of OA changes after OAT.3,22 The previous reports with a short-term follow-up may be insufficient to evaluate the OA changes after surgery.4,10,16,22,23,31 Thus, clinical outcomes of fragment resection and OAT for large OCD lesions in adolescent athletes with a long-term follow-up are still limited,17,22 and no reports have compared outcomes of fragment resection and OAT for large capitellar OCD lesions.
We aimed to investigate functional and radiographic outcomes after osteochondral grafting and fragment resection for unstable large capitellar OCD lesions in skeletally immature athletes with a minimum 5 years’ follow-up. We hypothesized that the outcomes after OAT for large capitellar OCD lesions would be superior to those after arthroscopic fragment resection.
Methods
Study Population
An institutional review board approval for this retrospective study was obtained at Funabashi Orthopaedic Hospital. We reviewed patients who underwent arthroscopic fragment resection or OAT for large, unstable capitellar OCD lesions in our institute between May 2003 and October 2013. Large and unstable capitellar OCD lesions were defined using Takahara criteria: lesions with a width exceeding one-half of the radial head diameter that are symptomatic and displaced or detached.25,26 The lesion width was determined with preoperative anteroposterior radiographs with 45° of elbow flexion (tangential view).
A total of 33 patients (n = 33 elbows) underwent arthroscopic fragment resection between May 2003 and December 2011. Among them, 19 elbows in 19 patients (group 1) were followed for a minimum of 5 years (Table 1). The patients consisted of 17 male and 2 female patient, with the mean age of 14 years (range, 13-15 years), including 9 central and 10 lateral lesions, and the mean follow-up was 8 years (range, 5-11 years). There were 16 baseball athletes, 2 gymnastics athletes, and 1 handball athlete.
Patient Data a
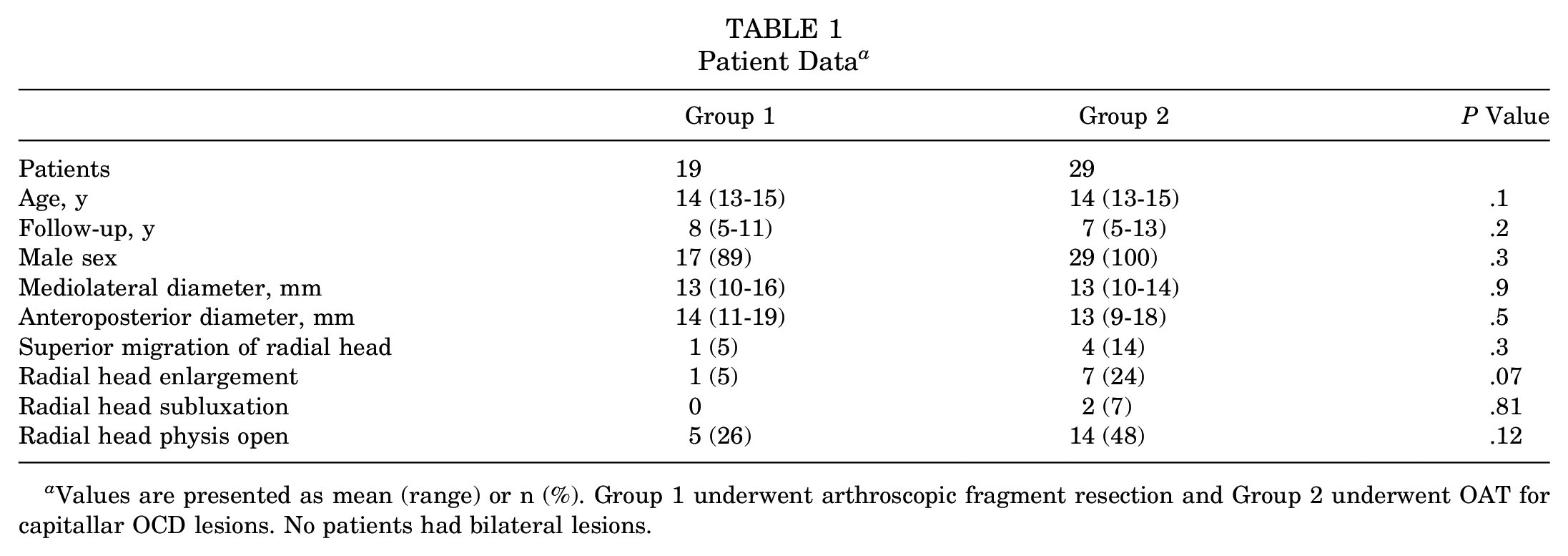
Values are presented as mean (range) or n (%). Group 1 underwent arthroscopic fragment resection and Group 2 underwent OAT for capitallar OCD lesions. No patients had bilateral lesions.
A total of 36 male patients athletes underwent OAT between May 2007 and October 2013. Among them, 29 patients (n = 29 elbows) (group 2) were followed for a minimum of 5 years (Table 1). They consisted of 29 male patients (mean age, 14 years [range, 13-15 years]), including 9 central and 20 lateral lesions, with a mean follow-up of 7 years (range, 5-13 years). There were 26 baseball athletes, 2 badminton athletes, and 1 gymnastics athlete.
Surgical Techniques and Postoperative Procedures
All arthroscopic surgeries were performed with the patient in the prone position under general anesthesia by 1 of the 2 senior surgeons (H.S., N.T.). First, a routine diagnostic arthroscopy was performed in the elbow joint, and then the osteochondral fragment was removed, and the capitellar OCD lesion was debrided in both groups as reported in a previous study. 28
After the arthroscopic surgery, patients in group 2 underwent OAT in the supine position. Two or 3 cylindrical osteochondral autografts were harvested from the lateral condyle of the ipsilateral knee and transplanted to the capitellum through a small skin incision at the posterior elbow using the osteochondral autograft transfer system (Arthrex) (Figure 1).
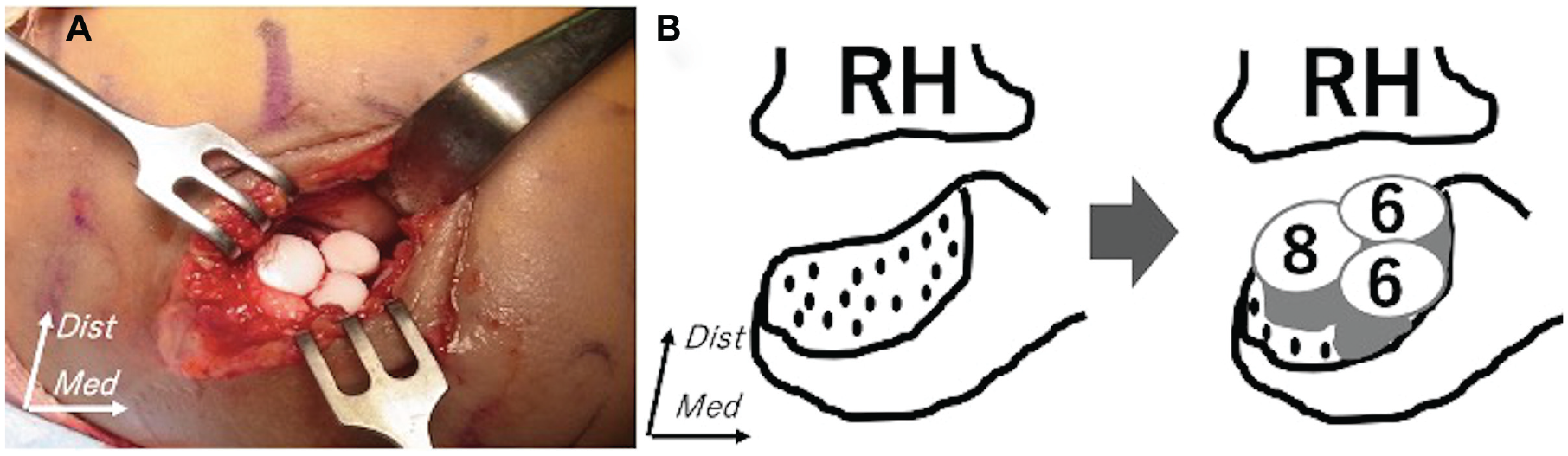
Osteochondral autograft transplantation. (A) After an arthroscopic debridement, osteochondral autografts were harvested from the knee and transplanted to the capitellum through a small skin incision. (B) The most frequent pattern was 3 grafts (one 8 mm–diameter and two 6 mm–diameter grafts). Two 6-mm grafts were transplanted in the medial aspect of the defect extending the normal capitellum, and one 8-mm graft was placed just lateral to the 6-mm grafts. Dist, distal; Med, medial; RH, radial head.
Postoperatively, an arm sling was used for 1 week, and then patients were allowed to use their arm for daily life activities, regardless of surgical procedures. Physical therapy was initiated immediately after the surgery to improve elbow range of motion (ROM) and scapular function. Based on their functional recovery, patients were allowed to return to their sports activity at 1 month postoperatively in group 1 and at 3 months postoperatively in group 2.
Clinical Evaluation
One of the senior surgeons evaluated all patients. Patients were assessed preoperatively and postoperatively using the Timmerman-Andrews score 27 ; the Disabilities of the Arm, Shoulder and Hand (DASH) score for daily activity evaluation 5 ; and ROM, including flexion and extension. Postoperative return to sports and patient satisfaction (0-100 scale) were also assessed.
Radiographic Evaluation
Patients underwent preoperative and postoperative radiographs of both elbows, including anteroposterior, lateral, and tangential views, and an anteroposterior view with 45° of elbow flexion. Preoperatively, 3-dimensional computed tomography (3D-CT) scans were performed using a 16-detector CT system (Alexion, Toshiba); image matrix, 512 × 512; pixel size, 0.468 × 0.468 mm; and slice pitch, 0.5 mm). Coronal and sagittal images were subsequently reconstructed from the axial data, and 3D-CT images of the distal humerus were also created, with the radius and ulna digitally subtracted.
The mediolateral and anteroposterior widths of OCD lesions were measured using 3D-CT images. The superior migration of the radial head was defined as a >2-mm side-to-side difference on tangential anteroposterior radiographs. 28 Radial head enlargement was defined as a >20% difference compared with the contralateral side, according to a study by Sato et al. 22 Radial head subluxation was defined on a lateral radiograph if the line drawn along the long axis of the radius intersected the upper third of the capitellum, according to a study by Matsuura et al. 16 The state of the radial head physis was assessed to determine whether it was open or closed. OA grades were evaluated with tangential and lateral views using the Kellgren-Lawrence grade. 11
Statistical Analysis
Statistical analysis was conducted with the use of Statcel software (Version 3; OMS Institute). The paired t test was used to compare preoperative and postoperative clinical scores and ROM. The Welch t test was used to compare time to return to sport, satisfaction, clinical scores, and ROM between the 2 groups. The chi-square test was used to compare preoperative and postoperative radial head enlargement and OA grades between the 2 groups. The level of significance was set at P < .05. The post hoc power analysis was performed based on Timmerman-Andrews and DASH scores.
Results
Clinical Evaluation
All patients returned to sports activity. However, 1 patient in group 1 (baseball to basketball) and 3 patients in group 2 (baseball to basketball, 2 patients; baseball to tennis, 1 patient) changed sports for reasons other than elbow problems. The time to full return to sport was significantly different between the 2 groups (group 1: 4 months [range, 2-9 months]; group 2: 6 months [range, 3-12 months]; P = .008). Preoperative and postoperative functional scores significantly improved postoperatively in both groups and were not different. The patient satisfaction score showed no significant difference between the 2 groups (Table 2). Flexion at the final follow-up did not show any significant improvement in the 2 groups as compared with preoperative values (group 1: 131° [range, 120°-140°] to 132° [range, 100°-150°]); group 2: 130° [range, 105°-155°] to 133° [range, 120°-145°]). The difference in flexion at the final follow-up was not significant between the 2 groups. Extension showed a significant improvement in both groups (group 1: –17° [range, –50° to 0°] to 0° [range, –10° to 20°]; group 2: –18° [range, –35° to 0°] to −6° [range, –30° to 10°]; P < .001 for both). Group 1 had a significantly better extension than group 2 at the final follow-up (P = .045).
Comparison of Clinical Scores and Satisfaction a
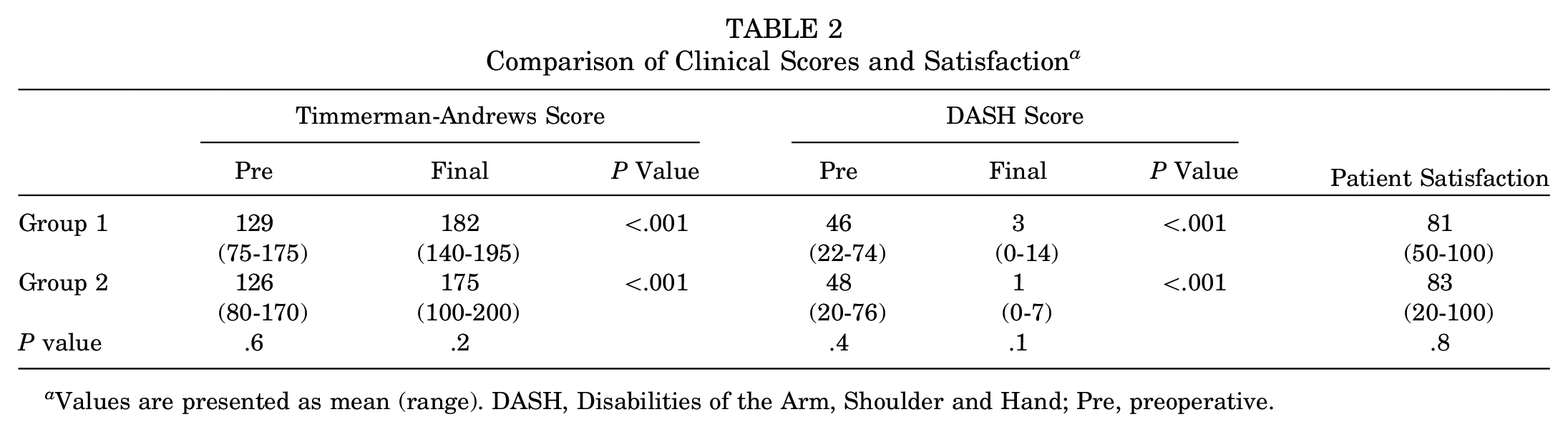
Values are presented as mean (range). DASH, Disabilities of the Arm, Shoulder and Hand; Pre, preoperative.
The results of the post hoc power analysis indicated that statistical powers for Timmerman-Andrews and DASH scores were 0.66 and 0.78, respectively.
Radiographic Evaluation
Preoperatively, the epiphyseal line of the capitellum in the affected side was closed and that in the contralateral side was open in all patients. The mean mediolateral and anteroposterior diameters of lesions were not different between the groups (Table 1). Superior migration of the radial head was observed in 1 elbow in group 1 and in 4 elbows in group 2, and radial head enlargement was observed in 1 elbow in group 1 and in 7 elbows in group 2. Radial head subluxation was only found in 2 elbows in group 2. The radial head physis was open in 5 elbows in group 1 and in 14 elbows in group 2 (Table 1). The incidence of radial head enlargement significantly increased postoperatively in group 1 (n = 6 elbows; P = .04). In group 2, radial head enlargement was observed in 10 elbows, and the difference between the preoperative and postoperative incidence was not significant.
Preoperatively, grade 1 OA was observed in 14 elbows and grade 2 OA in 5 elbows in group 1; in group 2 there were 3 grade 0, 22 grade 1, and 4 grade 2 OA cases. The difference in the preoperative OA grades was not significant between the 2 groups. OA progressed in 9 elbows (47%) in group 1 and in 14 elbows (48%) in group 2 (Figure 2). However, OA grades at the final follow-up did not show significant differences as compared with preoperative grades in either group. No elbows had severe OA, but 1 elbow in group 1 developed a 2.5-mm superior radial head migration with grade 2 OA changes at the final follow-up (10 years postoperatively); preoperatively this patient had superior migration and radial head enlargement (Figure 3). Most elbows did not show severe OA changes in group 2 (Figure 4). However, 3 elbows had grade 3 OA, all of which had lateral lesions and preoperative superior radial head migration and enlargement (Figure 5).
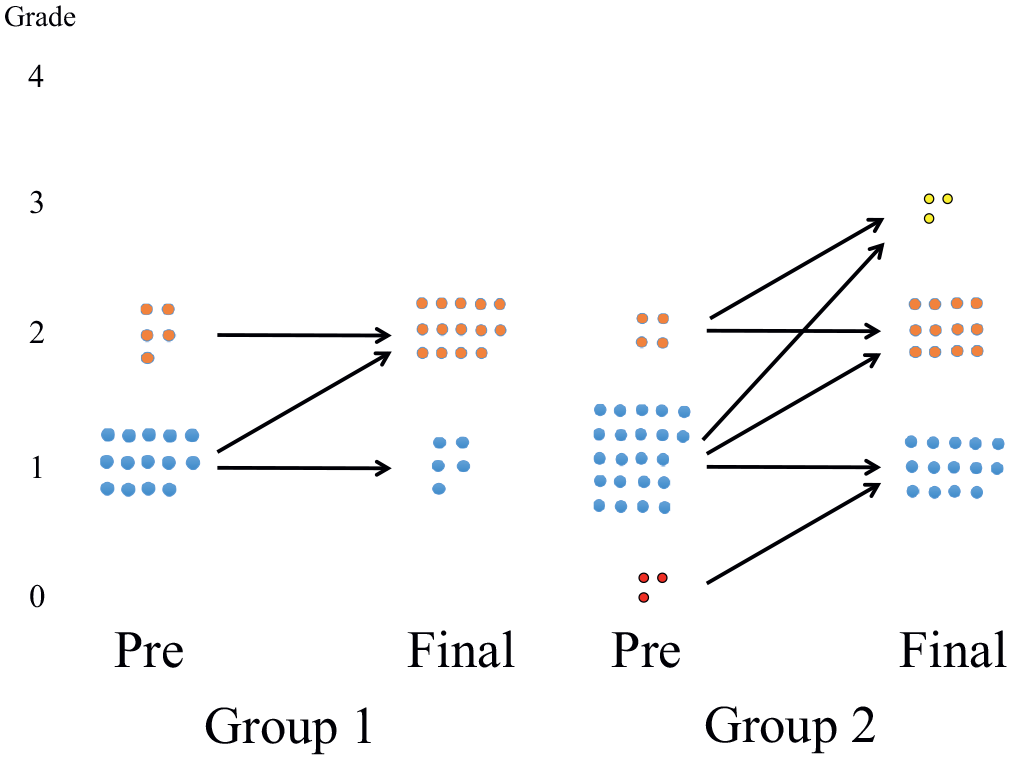
Diagram comparing preoperative (Pre) and final Kellgren-Lawrence osteoarthritis (OA) grades. OA progressed by 1 grade in 9 elbows in group 1. OA progressed by 1 grade in 15 elbows and by 2 grades in 1 elbow in group 2. Changes were not significant in either group.
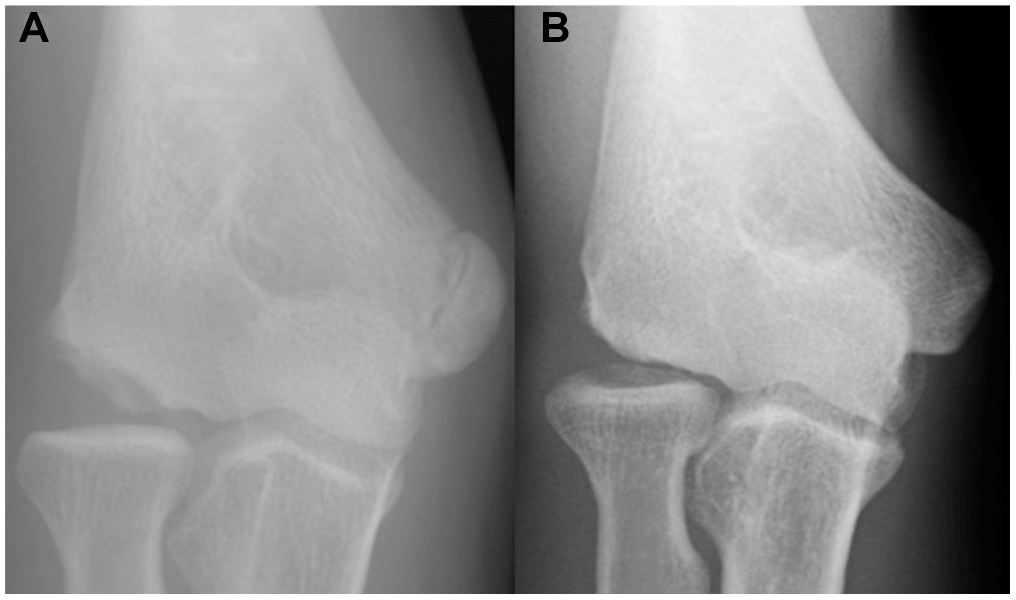
A right elbow of a 14-year-old male baseball player in group 1. (A) Preoperative tangential view shows superior radial head migration (flexion 130°; extension −10°). (B) Tangential view at 10 years after the arthroscopic fragment resection. Although the capitellum was remodeled, the radial head migration progressed (flexion 120°; extension 0°).
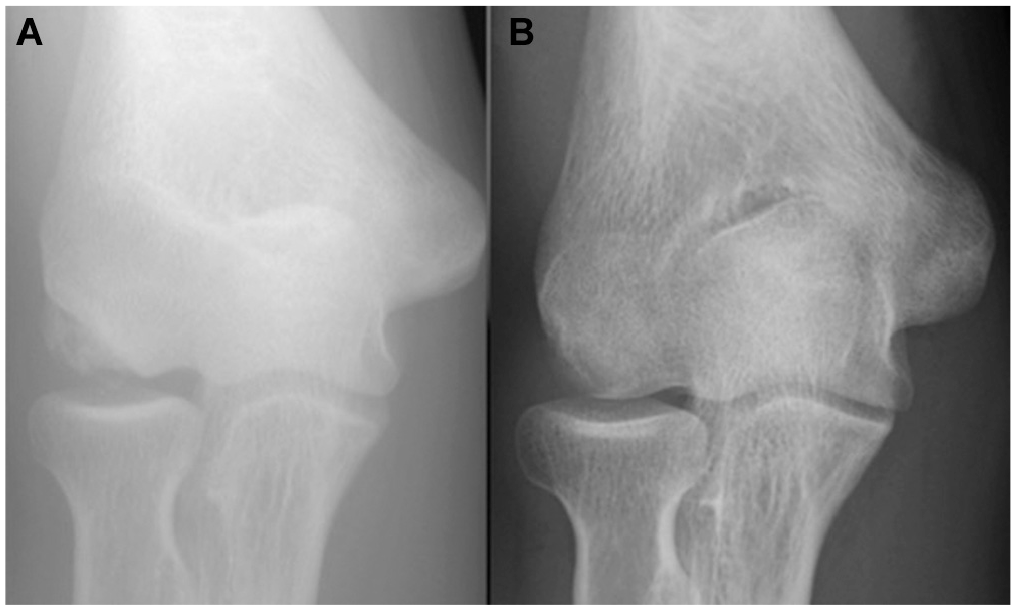
A right elbow of a 15-year-old male baseball player in group 2. (A) Preoperative tangential view (flexion 150°; extension 0°). (B) Tangential view at 11 years after an osteochondral autograft transplantation. The lesion was well-remodeled (flexion 150°; extension 5°).
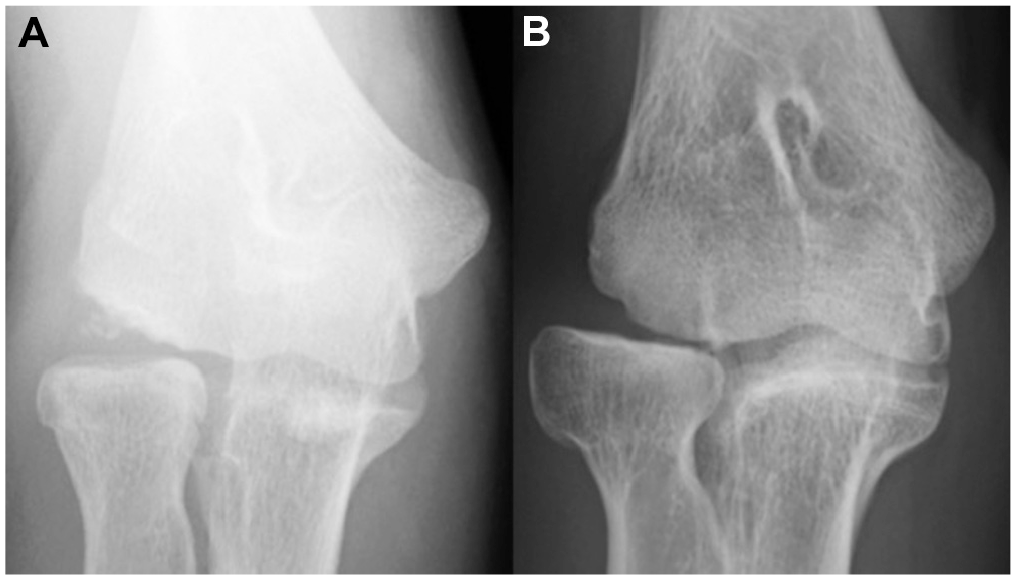
A right elbow of a 13-year-old male baseball player in group 2. (A) Preoperative tangential view shows superior radial head migration and enlargement (flexion 105°; extension −25°). (B) Tangential view at 8 years after an osteochondral autograft transplantation. Although grade 3 OA was observed with progressed superior radial head migration and enlargement, the range of motion improved at the final follow-up and the patient’s satisfaction was high (flexion 127°; extension −15°).
Discussion
In this study, all adolescent athletes with an unstable large capitellar OCD lesion returned to sports activity after either arthroscopic fragment resection or OAT. Functional scores, patient satisfaction, and extension were significantly improved postoperatively in both groups, and no significant differences were observed at the final follow-up between the groups except for extension, which was significantly better in elbows with fragment resection. No severe OA changes were observed after a fragment resection. However, 3 elbows had grade 3 Kellgren-Lawrence OA after OAT; these elbows already had superior radial head migration and enlargement preoperatively.
Several articles have reported outcomes after arthroscopic fragment resection for large OCD lesions.2,17,20,26,28 Regarding unstable small capitellar OCD lesions, several authors have reported excellent long-term outcomes after arthroscopic resection in terms of return to sports as well as clinical and functional outcomes.17,26,28 However, Matsuura et al 17 recently reported good long-term outcomes (mean 12 years’ follow-up) after an arthroscopic resection of unstable capitellar OCD lesions in 23 adolescent baseball players that include 6 cases of large lesions. Excellent outcomes have been reported with 5- to 12-year follow-up after an arthroscopic fragment resection for both small and large unstable capitellar OCD lesions, although patient satisfaction in elbows with large lesion was lower than in those with small lesions. 28 Conversely, Miyake and Masatomi 20 have reported that outcomes in small lesions with both open and closed radial physis were excellent, with a mean 13 months’ follow-up. However, in 13 patients with large lesions, 9 elbows with closed radial physis had excellent outcomes but the remaining 4 elbows with open radial physis demonstrated poor outcomes because of radial head hypertrophy progression and arthritic changes. Therefore, the authors reported that arthroscopic fragment resection for large OCD lesions was contraindicated if the radial physis remained open.
In the present study, 5 of 19 elbows (26%) had open radial physis; however, their physes were almost closing at the time of surgery. Therefore, the maturity of the skeletal age might have contributed to obtaining acceptable outcomes after an arthroscopic fragment resection in elbows in group 1. The elbows with fragment resection even showed better extension than those with OAT; however, the difference was only 6° and may not be clinically significant. The long-term outcomes of arthroscopic fragment resection for large capitellar OCD lesions remain controversial. The results of the present study suggest that the overall clinical and radiographic outcomes of arthroscopic fragment resection were acceptable, although surgical indication was a bit different than that of OAT. The lower incidence of preoperative changes in the radial head, such as superior migration, enlargement, and subluxation, as well as the lower incidence of open radial physis in the arthroscopic resection group might be a part of the reasons for favorable outcomes, although differences in the incidence were not statistically significant.
Takahara et al 25 advocated that the reconstruction of the articular surface should be performed for lesions >50% of the capitellar width because of better outcomes compared with simple excision. Other authors also reported good clinical outcomes after an OAT.4,10,16,22,23,30 Therefore, we initiated OAT for large unstable capitellar OCD lesions in 2007 and gradually increased the number of selected patients with large lesions. Then, in 2011, we performed the OAT procedure exclusively for unstable large capitellar OCD lesions in elbows with open contralateral radial physis. 24 Therefore, from 2007 to 2011, it was not clearly indicated which procedure, arthroscopic fragment resection or OAT, to perform for unstable large capitellar OCD lesions. Although no statistical difference was observed, more elbows in group 2 showed poor joint congruity preoperatively than in group 1 because of superior migration and enlargement of the radial head and skeletal immaturity (Table 1). According to our previous study 28 and a study by Miyake and Masatomi, 20 preoperative poor joint congruity and skeletal immaturity are risk factors for poor clinical and radiological outcomes after an arthroscopic fragment resection. Therefore, some selection bias existed in patients who underwent either arthroscopic resection or OAT between 2007 and 2011. This was one of the limitations in this study; however, it was very interesting to find that both groups demonstrated comparable long-term outcomes.
Treatments for skeletally immature elbows with large capitellar OCD lesions associated with arthritic change are challenging. In this study, we saw grade 3 OA changes after OAT in elbows with lateral type OCD lesions that had superior radial head migration and enlargement preoperatively. As the high joint pressure of the radiohumeral joint can be a risk for OA progression, 9 preventing OA progression in such cases seems difficult, even with OAT. In fact, some authors reported that lateral capitellar OCD lesions, especially in joints with poor congruity, were at risk of severe OA progression after OAT.4,16 Therefore, surgical timing is also a very important factor that affects postoperative outcomes after OAT. 24 We believe that reconstructive surgery for skeletally mature patients is unnecessary because it is too invasive and no excellent remodeling can be expected postoperatively. Indeed, determining the best time for a reconstructive surgery is difficult because nonoperative treatments work well for patients with large capitellar OCD lesions if they are skeletally immature. Therefore, we always examine the radial physis of both elbows, as the physis on the affected side normally closes earlier than that on the unaffected side. 24 We believe that the best time to perform OAT is when the radial physis on the affected side is almost closed or when it has just closed and the physis on the unaffected side remains open. 24
Regarding the grafting technique, some surgeons prefer to use multiple small cylindrical autografts 3 to 5 mm in diameter and 10 to 15 mm in length.4,10 This is suitable for relatively small lesions with the lateral wall mostly preserved. However, for large lesions with a lateral wall defect, graft stability remains a problem after multiple small graft transplantations before achieving the bone union. Therefore, although some surgeons prefer to use costal osteochondral autograft for large lesions with lateral wall defect,22,23 others utilize multiple larger grafts from 5 to 9 mm in diameter,15,16 which is similar to our technique. 24 We usually transplant one 8-mm and two 6-mm grafts right next to the remaining normal capitellum (Figure 1). 24 This technique may provide good graft stability that requires no postoperative immobilization and provides better support for the radial head by extending the articular surface. 24
This study had several limitations. First, this was a retrospective study. Second, patients who underwent surgery, either an arthroscopic fragment resection or an OAT, were compared in different periods. This might cause the lower incidence of radiographic changes in the elbows with arthroscopic fragment resection, although the differences in the incidence were not statistically significant. This might be associated with preferable outcomes after an arthroscopic fragment resection. Last, the study cohorts were relatively small. The statistical power seemed acceptable but was not sufficient, and the insignificant differences between the outcomes of the 2 groups might be due to this constraint.
Conclusion
No differences were observed between patiens undergoing arthroscopic fragment resection and OAT for capitellar OCD lesions in clinical and radiographic outcomes at a minimum 5 years’ follow-up, except for elbow extension. We believe that for adolescents with large capitellar OCD lesion, OAT is a good option for skeletally immature elbows and that arthroscopic fragment resection is a reliable and less invasive surgical option for relatively mature elbows. In addition, OAT is also a viable option for elbows in the advanced stage of large capitellar OCD associated with elbow joint incongruity due to radial head hypertrophy if the radial physis in the contralateral side remains open.
Footnotes
Submitted May 22, 2020; accepted November 19, 2020.
Presented as a poster at the AOSSM Annual Meeting, Boston, Massachusetts, July 2019.
One or more of the authors has declared the following potential conflict of interest or source of funding: H.S. is a paid speaker for DePuy Synthes, Smith & Nephew, Zimmer Biomet, and Wright Medical Technology Inc. K.M. has received research grants from Arthrex and Exactech Inc. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.