
Abstract
Background:
Sports-related concussions may have a neurobiological recovery period that exceeds the period of clinical recovery, and one consequence of an extended neurobiological recovery may be the risk of subsequent musculoskeletal injuries. Most literature citing an increased risk of musculoskeletal injury after a sports-related concussion has been reported in populations other than adolescent athletes.
Purpose/Hypothesis:
The purpose was to prospectively determine if incidence rates of musculoskeletal injury differ between adolescent athletes with and without a previous sports-related concussion, while controlling for sex, sport, and age. A secondary aim was to determine if this relationship differs between male and female athletes of the same sport. Our hypotheses were that acute-noncontact injury rates would be higher in athletes with a previous sports-related concussion when compared with athletes without a previous sports-related concussion, and that this relationship would exist only in female athletes and not male athletes.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
High school soccer and volleyball players were recruited in 2 prospective cohort studies that observed 4837 athletes during their sporting season (females, 80%; soccer, 57%; mean [SD] age, 15.6 [1.1] years). At preseason, all participants self-reported demographics and previous sports-related concussion within the past 12 months. During the sport season, team athletic trainers electronically recorded athlete exposures and injury data, including injury characteristics. Injury rates per 1000 athlete exposures and injury rate ratios (IRRs) with 95% confidence intervals were calculated. All injury rates and IRRs were adjusted for sex, age, and sport.
Results:
The rate of acute-noncontact lower extremity injury was 87% greater (IRR, 1.87; 95% CI, 1.29-2.74) in participants with a previous sports-related concussion versus those without one. The acute-noncontact lower extremity injury rates (IRRs) for females and males with a previous sports-related concussion were 1.76 (95% CI, 1.19-2.59) and 2.83 (95% CI, 0.85-9.50), respectively. No difference was detected in acute-contact (IRR, 0.98; 95% CI, 0.56-1.73) or overuse (IRR, 1.09; 95% CI, 0.51-2.37) lower extremity injury rates by previous sports-related concussion.
Conclusion:
Female adolescent athletes who reported a sports-related concussion within the past 12 months were more likely to sustain an acute-noncontact lower extremity injury during their high school sports season when compared with female athletes without a previous sport-related concussion.
Sports-related concussions (SRCs) have several short-term clinical symptoms and may include neurobiological recovery that exceeds the period of clinical recovery. 29 One consequence of an extended neurobiological recovery may be the risk of subsequent musculoskeletal injuries.32,38 An increased risk of musculoskeletal injury after a concussion incident has been observed in several studies on intercollegiate4,16,24 and professional8,26,34,35 athletes, but only 1 study has examined this risk in adolescent athletes. 25
In the United States, an estimated 1.1 to 1.9 million sports or recreational activity-related concussions occur annually in those <18 years of age. 5 Adolescent recovery from an SRC is prolonged as compared with their adult counterparts1,19,29 and may be due to changes in cerebellar development, brain processing speed, and bimanual coordination during rapid maturation.27,40,41 Additionally, SRC recovery trajectories and symptom profiles are known to differ between males and females.3,11,21 However, most studies of subsequent injury after an SRC have been in male cohorts exclusively.8,26,34,35 Few studies have utilized a large prospective cohort design to determine incidence rates of injuries after an SRC. 32 Therefore, the primary aim of this study was to prospectively determine if musculoskeletal injury incidence rates by injury mechanism differ between adolescent athletes with and without a previous SRC, while controlling for sex, sport, and age. A secondary aim was to determine if this relationship differs between male and female athletes of the same sport. Our hypotheses were that acute-noncontact injury rates would be higher in athletes with a previous SRC as compared with athletes without a previous SRC, and that this relationship would exist only in female athletes and not male athletes.
Methods
This study is a secondary analysis of 2 prospective cohort studies of high school athletes in the state of Wisconsin. The data from one study were collected in adolescent male and female soccer athletes, 31 and the other was from data of a study of adolescent female volleyball athletes. 30 Utilizing the Wisconsin Sports Injury Research Network, 123 high schools in Wisconsin were used as data collection sites across both studies. The soccer cohort data were collected in the 2016-2017 and/or 2017-2018 school year, and the volleyball cohort data were collected in the fall of 2018. The methodology used for data collection was consistent across both studies. The same preseason information was collected, and high school athletic trainers were utilized to record data during the soccer or volleyball interscholastic regular season and postseason. All students (and parents, if athletes were <18 years old) signed a consent/assent document to participate in the studies. No identifiable patient or personal medical history is included in this article. Both studies were approved by the Health Sciences Institutional Review Board at the University of Wisconsin–Madison.
Participants
Potential participants (14-18 years old, grades 9-12) were recruited before the start of the interscholastic soccer or volleyball sport season and had to be members of their interscholastic soccer or volleyball team. All were free of injuries that would prevent them from full participation in team activities on the first day of practice. A total of 255 enrolled athletes (n = 94 males, n = 161 females; n = 144 volleyball, n = 111 soccer) dropped out of the study before the start of the regular season and were not included in the analyses.
Data Collection
All participants completed a self-reported questionnaire capturing their sex, date of birth, grade in school, and SRC injury history. SRC injury history included month and year of the SRC, whether the individual saw a medical professional (athletic trainer or physician) for the SRC, and how many days he or she missed from their sporting activity because of the SRC. For this analysis, a previous SRC was defined as a reported SRC that occurred within the past 12 months of the questionnaire administration and was evaluated by a medical professional. Licensed athletic trainers at each school recorded all sports-related injuries and all athlete exposures (AEs). An AE was defined as an athlete’s participation in a coach-led practice, a conditioning session, or a competition event in the interscholastic sport of interest. Athletic trainers recorded injury characteristics of all sports-related injuries.
Musculoskeletal Injury Definition
To be considered for analysis, the injury (1) must have happened during participation in interscholastic conditioning, practice, or competition for the participant’s given sport (soccer or volleyball), (2) must have required medical attention by the athletic trainer or a physician, and (3) was determined to be an injury to the musculoskeletal system (excluding abrasions or bruises). Injury onset was defined as an acute injury (one that occurred from a specific incident at a specific time) or an overuse injury (one resulting from repetitive use and having an insidious occurrence). Each acute injury was further classified as contact (acute-contact) or noncontact (acute-noncontact) based on how it was sustained. If athletic trainers selected “unknown” or “general play” for mechanism of injury, not allowing for appropriate classification as a contact or noncontact injury, it was analyzed as a general acute injury, not acute-contact or acute-noncontact. All injury events and their characteristics were reported electronically by the athletic trainers via REDCap, a secure web-based software platform designed to support data capture for research studies. 15
Statistical Analysis
Standard descriptive statistics were used to describe all data: means (standard deviations) were used for continuous variables and frequencies (percentages) for categorical variables. Poisson regression with AE offset was used to estimate adjusted injury rates (per 1000 AEs) for different injury onsets (acute, acute-contact, acute-noncontact, or overuse) and injury locations (upper or lower extremity). Adjusted injury rate ratios (IRRs) with 95% confidence intervals were also calculated. All injury rates and IRRs were adjusted for sex, age, and sport. An interaction between sex and previous SRC was considered to evaluate whether the association between previous SRC and injury differed by sex. All 95% confidence intervals for IRRs that did not contain 1.0 were considered statistically significant. All data were analyzed using SPSS Version 26 (IBM Corp).
Results
Participant Demographics and Injury Counts by Sport
There were 4837 high school participants, with a higher percentage of female participants (80%) because the volleyball cohort consisted of only female athletes (Table 1). A small proportion (n = 354, 7%) reported an SRC in the past 12 months. A total of 254,646 AEs were recorded throughout the volleyball and soccer seasons for the 4837 participants.
Participant Demographics and Injury Onset and Mechanism by SRC in the Past 12 Months a
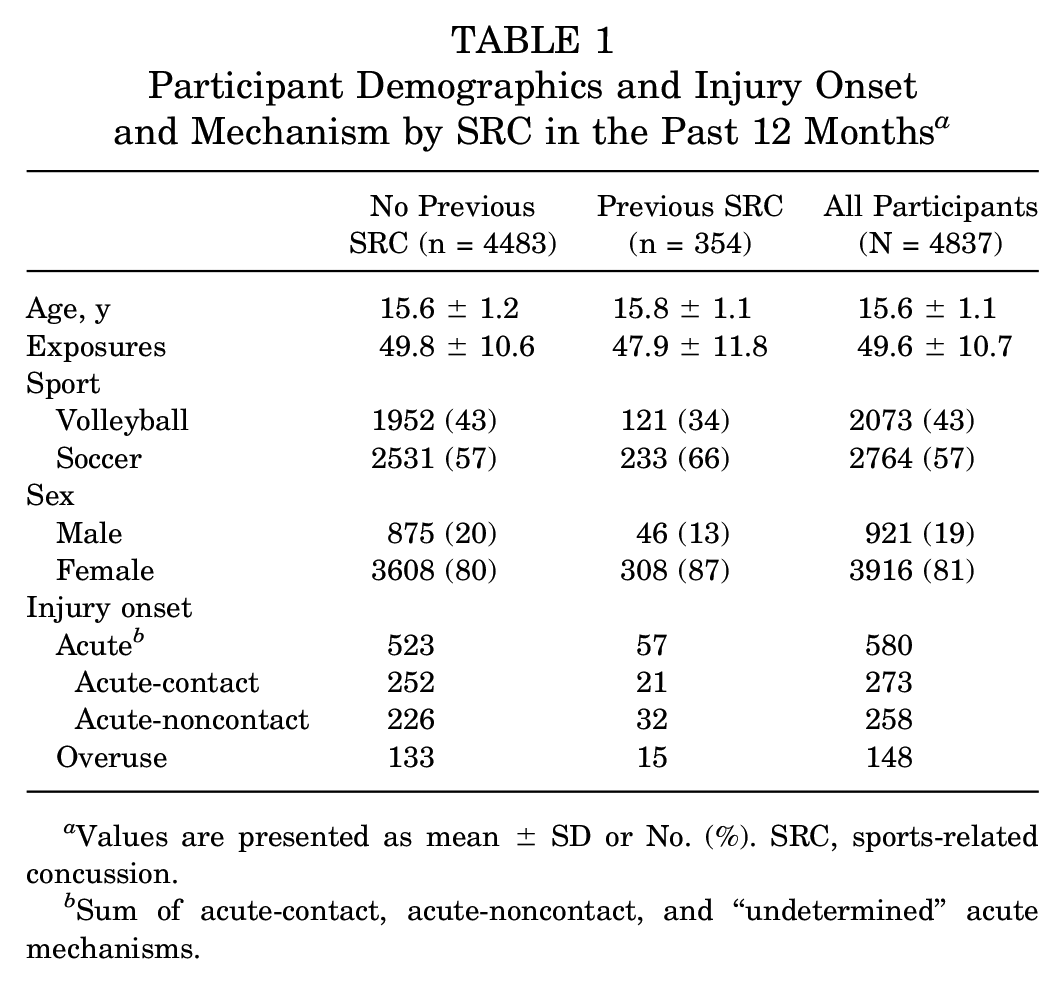
Values are presented as mean ± SD or No. (%). SRC, sports-related concussion.
Sum of acute-contact, acute-noncontact, and “undetermined” acute mechanisms.
An overall 728 injuries were recorded during the participants’ athletic seasons: 580 (80%) acute musculoskeletal injuries and 148 (20%) overuse musculoskeletal injuries. Forty-six athletes had multiple acute injuries occur in the same season, and 6 had multiple overuse injuries occur in the same season. Overall, there were more lower extremity injuries (n = 556) than upper extremity injuries (n = 178), and most lower extremity injuries were classified as noncontact-acute (43%) (Table 2). The ankle was the most injured lower extremity region for acute injuries, whereas the knee was the most common site for overuse lower extremity injuries.
Injury Counts for Injury Location, Onset, and Mechanism by Sport and SRC in the Past 12 Months a
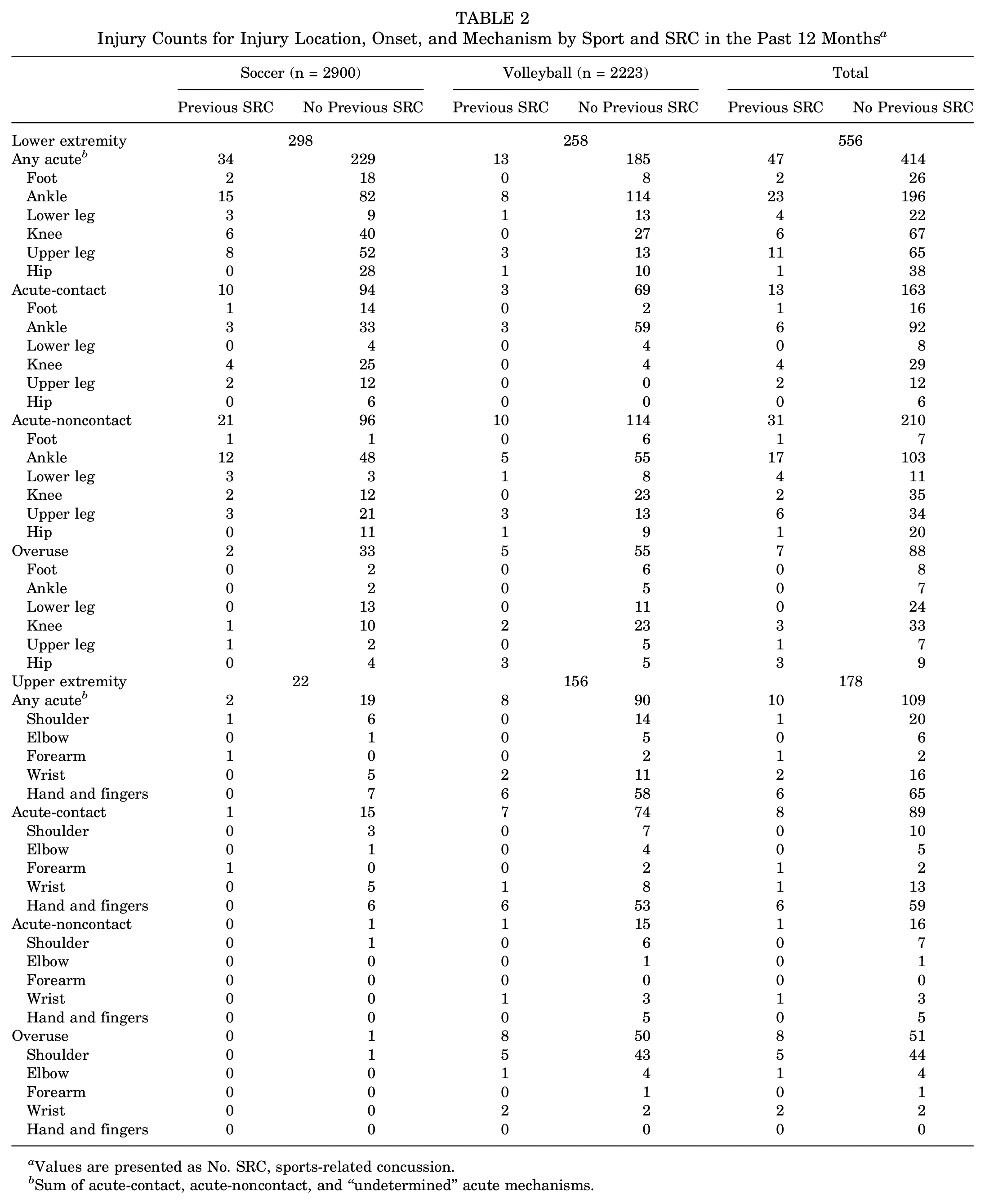
Values are presented as No. SRC, sports-related concussion.
Sum of acute-contact, acute-noncontact, and “undetermined” acute mechanisms.
Subsequent Musculoskeletal Injury by Onset and Extremity
The rate of acute injury was 41% (95% CI, 7%-85%) greater in participants with a previous SRC as compared with those without a previous SRC (Table 3). The rate of acute-noncontact injury in athletes with a previous SRC was 82% greater (95% CI, 26%-164%) than in those without a previous SRC. No significant difference was found in acute-contact and overuse injury rates between those with and without a previous SRC. The rate of acute lower extremity injuries for participants with a previous SRC was 40% greater (95% CI, 3%-90%) when compared with those without a previous SRC. The rate of acute noncontact lower extremity injury was 87% (95% CI, 29%-174%) greater in athletes with a previous SRC than those without a previous SRC. However, no significant difference was identified in acute-contact lower extremity rates between the groups. No significant difference was found in upper extremity acute injury rates (any, contact, or noncontact) between athletes with and without a previous SRC. A significant difference was found in overuse upper extremity injury rates between athletes with and without a previous SRC, but this difference did not exist for overuse lower extremity injury rates.
SRC in the Past 12 Months and Injury Rate, Injury Rate Ratio, and 95% CI by Injury Onset and Extremity, Adjusted for Sex, Sport, and Age a
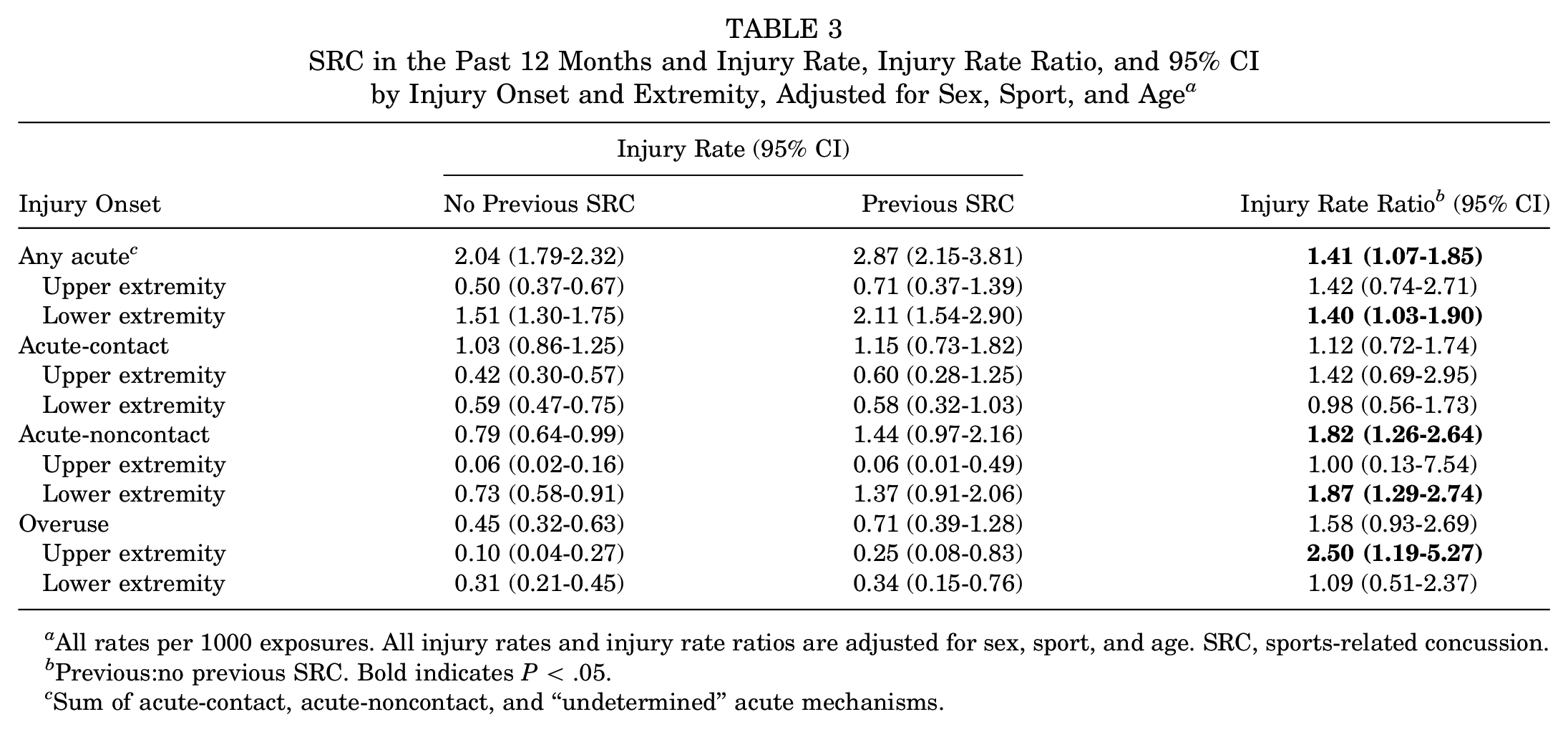
All rates per 1000 exposures. All injury rates and injury rate ratios are adjusted for sex, sport, and age. SRC, sports-related concussion.
Previous:no previous SRC. Bold indicates P < .05.
Sum of acute-contact, acute-noncontact, and “undetermined” acute mechanisms.
Subsequent Musculoskeletal Injury by Sex
Females had a higher proportion of overuse (4% vs 1%) and acute (12% vs 7%) injuries than males (Table 4). No overuse injuries were recorded for males with a previous SRC during their sport seasons.
Injury Counts for Injury Onset and Mechanism by Sex and Previous SRC in Past 12 Months a
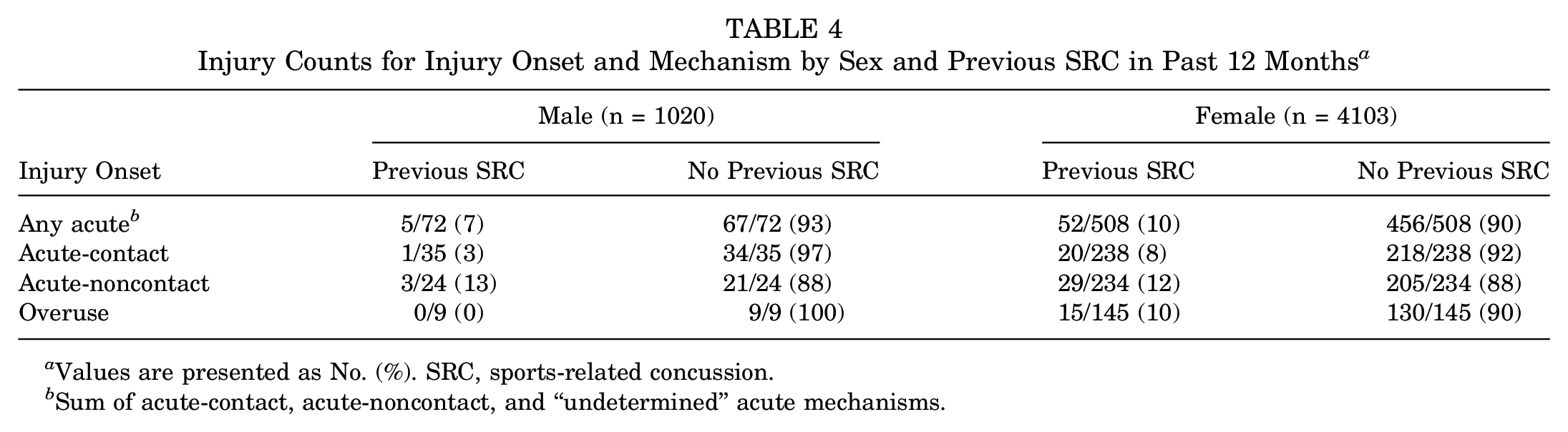
Values are presented as No. (%). SRC, sports-related concussion.
Sum of acute-contact, acute-noncontact, and “undetermined” acute mechanisms.
No injury rate (acute, acute-contact, acute-noncontact, or overuse) was significantly different between male participants with and without a previous SRC (Table 5). The rate of acute and noncontact-acute injury was 38% (95% CI, 4%-85%) and 76% (95% CI, 19%-159%) greater, respectively, in females with a previous SRC as compared with females without a previous SRC. No significant difference was found in acute-contact or overuse injury rates between females with and without a previous SRC.
SRC in the Past 12 Months and Injury Rate, IRR, and 95% CI by Injury Onset and Sex, Adjusted for Sex, Sport, Age, and Sex × Previous SRC a
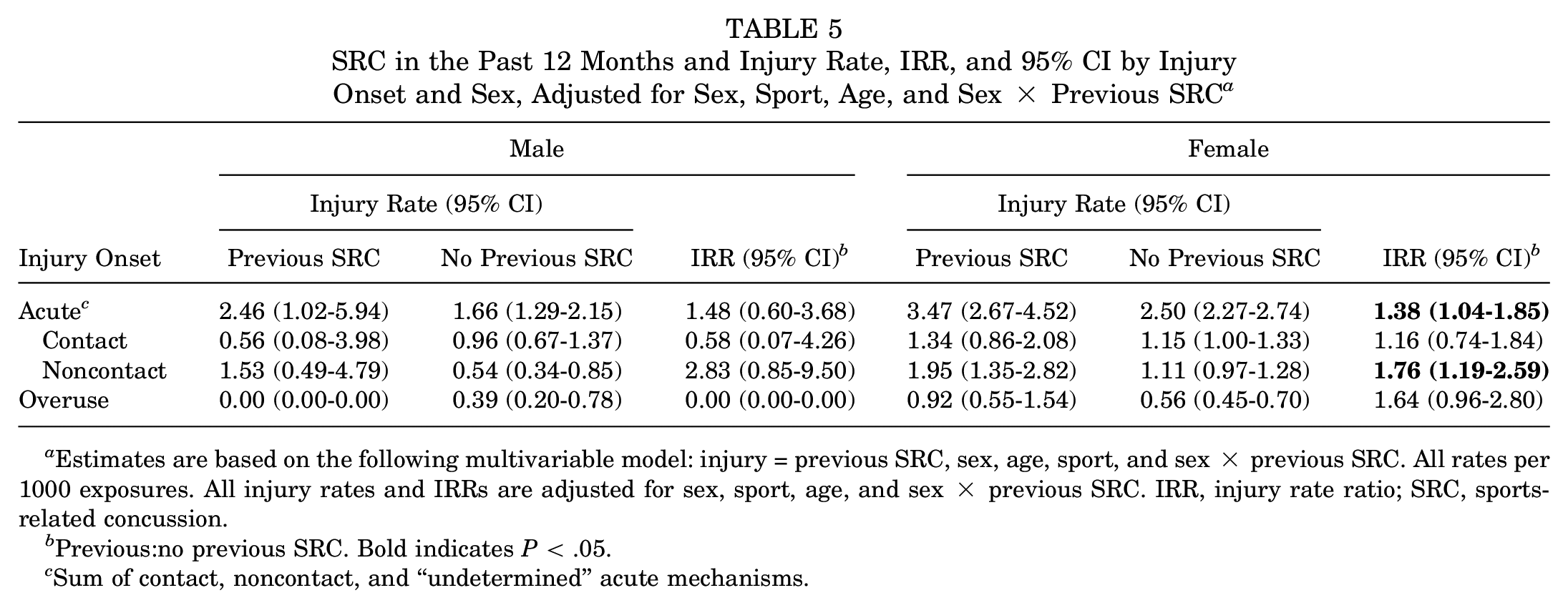
Estimates are based on the following multivariable model: injury = previous SRC, sex, age, sport, and sex × previous SRC. All rates per 1000 exposures. All injury rates and IRRs are adjusted for sex, sport, age, and sex × previous SRC. IRR, injury rate ratio; SRC, sports-related concussion.
Previous:no previous SRC. Bold indicates P < .05.
Sum of contact, noncontact, and “undetermined” acute mechanisms.
Discussion
Female adolescent athletes with a previous SRC were more likely to sustain an acute-noncontact lower extremity injury as compared with female athletes without a previous SRC. This relationship did not exist for acute-noncontact upper extremity injury rates; however, for the entire cohort, upper extremity overuse injury rates were higher for athletes with a previous SRC than athletes without one.
There is a lack of large prospective cohort studies in high school athletes to compare the incidence rates of musculoskeletal injuries between athletes with and without a previous SRC and to assess injury rates after an SRC by injury onset (eg, acute or overuse). Our results support previous medical history and retrospective studies that demonstrated an increased risk of acute musculoskeletal injury after a concussion incident.32,38 Particularly, our study is in agreement with Lynall et al, 25 who have the only other study to evaluate SRC and the association of subsequent musculoskeletal injury in high school athletes. Both studies used high school athletic trainers to collect data; however, Lynall et al were able to control for previous injury and number of SRCs before a subsequent lower extremity injury. Although our study considered just the occurrence of a previous SRC, we accounted for AEs to report an injury rate for this population and measured upper extremity injuries, unlike the previous study. 25 Despite the different strengths of Lynall et al 25 and our study, our incidence rates for any acute injury and for an acute-noncontact injury are similar to the odds ratios reported in Lynall and colleagues’ high school populations.
Injury Onset and Location
Rates for any acute injury were higher in the group with a previous SRC than in the group without a previous SRC. This relationship was because of the higher injury rate of acute-noncontact injuries between the groups. This relationship existed only for lower extremity acute-noncontact injuries. Our results are most in line with the findings of Brooks et al, 4 who used distinct injury outcome measures as compared with other studies in this area of research.8,16,24,25 The authors assessed the risk of sustaining an acute-noncontact lower extremity musculoskeletal injury between college athletes with and without a history of SRC and reported an increased risk of injury in athletes with a previous SRC versus athletes without one. 4 The reported odds ratio of Brooks et al (2.48; 95% CI, 1.04-5.91) is higher than that of many previous studies that used “any injury” as a primary outcome,8,24-26 with the exception of 1 study. 16 This may be attributed to the strict injury outcome used, and our results would support that claim, as acute-contact injury rates for either the upper or lower extremity were not significantly different between participants with and without a previous SRC. Previous studies have demonstrated that neuromuscular control deficits may increase the risk of noncontact injuries.12,13,23 Neuromuscular changes after a concussion have been observed to persist past clinical recovery and have been interestingly observed only in lower extremity biomechanics,19,20,28,36 leading to the hypothesis that subsequent musculoskeletal injury risk after a concussion may be linked with lower extremity neuromuscular impairments. 17
A surprising finding in our study was the increased rate of upper extremity overuse injury in the previous SRC group versus the group without a previous SRC. To our knowledge, Nordstrom et al 34 have the only study to report that SRC was not associated with subsequent overuse injuries; however, this analysis was not differentiated by extremities. 34 Several studies used any sports-related injury as an outcome measure and were done in contact or lower extremity–dominant sports.8,26,34 Unlike these previous studies, our study included a large number of volleyball players and observed upper extremity injury rates after SRC in upper and lower extremity–dominant sports. 32 Although it is limited, there is some evidence that neuromuscular control is related to overuse lower extremity injuries.2,9 To the best of our knowledge, no such report exists for overuse upper extremity injuries. Deficits in upper or lower extremity neuromuscular control could plausibly be associated with overuse upper extremity injuries, especially in upper extremity–dominant sports such as volleyball, which drove the overuse upper extremity injury rate in our cohort (Table 2). This is hypothetical, and future research is needed in sports that are upper extremity dominant.
Injury Risk Interpretation
A prominent theory for the increased risk of musculoskeletal injury after an SRC is the presence of neuromuscular deficits after an SRC that extends past clinical recovery.10,17 However, the exact neuromuscular mechanism is still unknown. 6 This is an area of conflicting evidence, as some have postulated that injury risk after an SRC is an artifact of an athlete having an overall increased risk of injury regardless of the concussion event.7,24,34 These authors hypothesized that the increased risk of injury before and after an SRC may be due to “risk-taking behavior” or play style.7,34 Our study was unable to control for musculoskeletal injury rates before reported previous SRCs; however, our findings may have implications for this theory as well. If musculoskeletal injury risk before and after an SRC event was due to risky behavior or play style, one could expect the rate of acute-contact injuries to differ between those with and without a previous SRC. Furthermore, one might expect injury rates for acute-contact and acute-noncontact upper extremity injuries to differ between the groups. That was not observed in our study. Therefore, it is plausible that participants with a previous SRC had lower extremity neuromuscular deficits before and after an SRC event that increase the risk for acute-noncontact lower extremity injuries, or that SRC injury rates themselves may be affected by lower extremity neuromuscular deficits. This would be a novel discovery, as SRC risk has mostly been assessed with neck and head biomechanics and not lower extremity biomechanics.22,39 Regardless of the hypothesis, future research is needed to understand the mechanisms behind the relationship between musculoskeletal injury risk and an SRC.
Subsequent Injury in Male and Female Athletes
For females, the rate of acute-noncontact injuries was significantly different for those with a previous SRC as compared with those without a previous SRC. These differences were not statistically significant in male athletes, but this was almost certainly because of the smaller number of males who reported a concussion (n = 46) (Table 1). When comparing the effect of sex on previous SRCS, we found no difference in acute injury rates or acute-noncontact injury rates between females and males with a previous SRC (acute IRR, 1.41 [95% CI, 0.56-3.53]; acute-noncontact IRR, 1.27 [95% CI, 0.39-4.18]). There is conflicting evidence on male-only populations and the association of previous concussion with subsequent injury.14,26,34,35 Current research has demonstrated a difference between males and females in symptoms and recovery rates after an SRC.3,11,21 However, this is not ubiquitous in the literature, as Howell et al 18 recently observed that females recover dual-task gait parameters more quickly than males. However, Howell et al used a collegiate athlete population rather than a pediatric population, and the authors acknowledged that the tasks performed may be easier for females in general. Although our results support the idea that subsequent injury risk after a concussion is increased in females, future research is needed to elucidate the differences in injury risk after an SRC for male and female adolescent athletes.
Limitations
This study has several limitations. The combination of 2 high school sport cohort studies over 2 different periods may introduce contextual error or bias. However, these potential sources of bias were minimized given the close time frame of data collection in both studies (<3 years) and the similar study design and methodology. Additionally, both studies were conducted in the same state and utilized many of the same athletic trainers who underwent similar training for the data collection process. Additionally, we lacked power to definitively assess the association between male concussions and subsequent risk of injury based on the small number of concussions among males in our data. The wide confidence interval associated with our estimated risk is indicative of the lack of confidence in our estimated IRR; thus, that estimate should be interpreted with caution. However, these data can be used to help power future prospective research on this topic. A second limitation is that our SRC definition could affect our results owing to recall bias. To mitigate this possibility, we restricted a reported SRC to the previous 12 months. Furthermore, we created a conservative operational definition of a previous SRC where participants had to (1) report the month and year of the SRC and (2) confirm that they saw a medical professional for the SRC. This conservative approach may have removed individuals who identified an SRC but did not seek medical treatment, as is common in adolescent athletics. 37 These results cannot be interpreted as causal, as we were unable to control for injury rates before a reported SRC. There may be other potential confounders. For instance, we did not know what position each athlete played throughout the season, and we do not have an accurate estimate of each athlete’s time on the field. In addition, concussion and noncontact lower extremity injuries may be seen more commonly in athletes of a certain body type (perhaps weaker neck and core muscles) or with a certain style of play. The current study design cannot determine whether the SRC might predispose to acute lower extremity injury or whether there might be a common causal factor that predisposes to both types of injury. Our results may not be generalizable to athletes who do not play soccer or volleyball. Additionally, these results are limited to the state of Wisconsin and may not be generalizable to other regions of the country.
Conclusion
Female adolescent athletes who reported an SRC within the past 12 months were more likely to sustain an acute-noncontact lower extremity injury during the high school sports season as compared with female athletes without a previous SRC. However, this relationship did not exist for any acute upper extremity injuries. Regardless of the theory linking musculoskeletal injuries with SRCs, our results imply that further investigation of lower extremity neuromuscular control and biomechanics is warranted before and after an SRC. There is emerging evidence to suggest that multiple SRCs may increase the risk of subsequent musculoskeletal injury 14 and are associated with greater neuromuscular control deficits. 33 Therefore, longer prospective studies may be needed to examine how multiple SRCs affect injury rates for different injury mechanisms and if this association differs by sex.
Footnotes
Acknowledgements
The authors thank Abbey DeBruin, Allison Weidman, and Allison Schwarz for their assistance and support through all aspects of this study. The authors also thank all participating high schools, athletic trainers, players, coaches, and parents for their willingness to take part in this study.
Submitted July 20, 2020; accepted November 19, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: P.J.L. has received education support from Smith & Nephew, Arthrex, and Kairos Surgical. M.A.B. has received research support from DJO. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.