
Abstract
Background:
Current reconstruction techniques do not re-create the distal ulnar collateral ligament (UCL) insertion. Reconstructing the distal extension of the anterior band ulnar footprint may increase elbow stability and resistance against valgus stress after UCL reconstruction (UCLR).
Purpose/Hypothesis:
The purpose was to test a new technique for UCLR, a modification of the docking technique, aimed at re-creating the distal ulnar footprint anatomy of the anterior band. We hypothesize that this novel “anatomic” technique will provide greater resistance to valgus stress after UCLR when compared with the docking technique.
Study Design:
Descriptive laboratory study.
Methods:
Eighteen unpaired cadaveric arms were dissected to capsuloligamentous elbow structures and potted. With use of a servohydraulic load frame, 5 Nċm of valgus stress was placed on the UCL-intact elbows at 30°, 60°, 90°, and 120° of flexion. UCLR was performed on each elbow, randomized to either the docking technique or the anatomic technique. After UCLR, the elbow was again tested at 30°, 60°, 90°, and 120° of flexion. Ulnohumeral joint gapping was calculated using a 3-dimensional motion capture system applied to markers attached to the ulna and humerus. Differences in gapping among the intact state and docking and anatomic techniques were compared using a 2-way analysis of variance with significance set to P < .05.
Results:
There was no significant difference in gapping between the anatomic and docking technique groups regardless of elbow flexion angle. All reconstructed groups showed increased gapping relative to intact, but all increases were below the clinically relevant level of 1 mm.
Conclusion:
Ulnohumeral joint gapping and resistance to valgus stress were similar between the anatomic technique and the docking technique for UCLR.
Clinical Relevance:
This study provides evidence that the anatomic technique is a viable alternative UCLR method as compared with the docking technique in a cadaveric model.
Elbow ulnar collateral ligament (UCL) injury is a debilitating and potentially career-ending condition among adolescent and elite throwing athletes. 16 The UCL complex—the anterior bundle of the UCL in particular—is the major ligamentous restraint to valgus stress of the elbow through a large portion of the elbow arc of motion. It is subject to significant loads, especially during the late cocking and early acceleration phases of the throwing motion.10,17 During the past 2 decades, there has been a significant increase in the number of UCL reconstructions (UCLRs) performed in Major League Baseball pitchers, from 1 in 1986 to 32 in 2012 and 105 in 2018.7,13,15 There are also rising rates of UCL injuries in youth and adolescent sport participants. In a study examining surgical trends in New York State, the number of UCLRs increased by 343% from 2003 to 2014, with a disproportionately higher trend observed in those patients between 15 and 19 years old. 14 This age group is predicted to have an increase in average annual incidence of UCLR from 6.8 per 100,000 in 2014 to 14.6 per 100,000 in 2025. 14
In a large systematic review of UCLR cohorts from 1986 to 2012 using various reconstruction techniques, the overall return-to-play rate was 78.9%. 20 Additionally, the rate of UCLR revision has been reported as 13.2% to 15%,13,21 suggesting potential for improvement in reconstruction techniques. 20 One area of potential improvement is the ulnar attachment during reconstruction. Rather than a simple attachment on the sublime tubercle, the ligament insertion tapers as it extends distally along a consistent osseous ridge, with a mean length of 27.4 to 29.2 mm,9,19 a mean width of 4.0 to 7.6 mm,1,17 and an average insertional area of 187.6 mm.3,4,9 As a result, surgeons have considered moving their reconstruction position more distally. Although the distal UCL fibers do not significantly contribute to gap resistance, 6 Camp et al 3 showed that a reconstruction with a larger distal ulnar attachment fails at higher loads than a reconstruction with the more traditional proximal ulnar attachment. Load to failure is one metric to compare reconstructions; however, it is not something that can be clinically assessed, nor does it give insight into dynamic constraint. Gap measurement under valgus stress can be evaluated radiographically and at multiple elbow flexion angles within the same specimen.
The purpose of this study was to compare the gap size under valgus stress of the “anatomic” UCLR technique 3 versus the standard docking technique. We hypothesized that the anatomic technique, which restores the native UCL insertion using more distal fixation, would provide greater resistance to valgus stress (smaller increase in ulnohumeral gap) as compared with the standard docking technique. A clinically relevant increase in gap was set as 1 mm based on the Eygendaal et al 8 definition of partial instability.
Methods
Eighteen unpaired fresh-frozen cadaveric full arms (11 right; all male; 27-68 years old) were obtained from a national tissue bank after institutional review board approval and thawed overnight at room temperature. Because not all cadavers had palmaris longus tendons, flexor carpi radialis tendons were harvested from each cadaveric specimen to be used as a graft. Each specimen was then stripped of all soft tissue except for the capsuloligamentous structures of the elbow. Saline-soaked gauze was wrapped around the capsuloligamentous structures to preserve the integrity of the soft tissue until testing was performed. The ulna, radius, and humerus were all cut 20 cm from the ulnohumeral articulation and potted in epoxy (Bondo; 3M) with the forearm rotation set at neutral. The flexor carpi radialis graft was prepared to a size 3 mm in diameter.
Docking Technique
The docking technique was performed as described by Camp et al. 3 At the humeral insertion, a 4.0-mm socket was drilled to a depth of 15 mm. Two smaller tunnels were drilled connecting to the 15-mm socket using a 2.0-mm drill bit. Passing looped sutures were passed through the smaller tunnels out through the 4.0-mm tunnel in preparation for graft passage.
Attention was then turned to the sublime tubercle, where the UCL inserts on the ulna approximately 7 to 10 mm distal to the ulnohumeral joint line. Tunnels were prepared 5 mm anterior and 5 mm posterior to the apex of the sublime tubercle. Two 3.5-mm converging tunnels were drilled on the anterior and posterior sides of the sublime tubercle. Care was taken to maintain a distance of 15 mm between tunnels. A curved curette was used to confirm convergence. A looped No. 0 absorbable suture (Vicryl; Ethicon) was passed in preparation of graft passage.
Anatomic UCLR Technique
The humeral side was prepared using the same docking technique. Two all-suture anchors (FiberTak Soft Anchor; Arthrex) were placed approximately 5 mm distal to the joint line at the anterior and posterior aspects of the sublime tubercle. These anchors were separated by approximately 10 mm, which was the same distance as the 2 drill holes for the transosseous tunnel in the docking technique.
Next, the 2 distal limbs of the graft exiting the humeral socket were sutured in a whipstitch fashion using a No. 0 nonabsorbable suture (FiberLoop; Arthrex). The necessary graft length was approximated by referencing off the distal aspect of the native UCL distal insertion, and excess graft was removed. Suture ends were then loaded into a cortical suspensory button (Tenodesis Button; Arthrex). The graft was tensioned and cycled, after which the specimen was placed in 30° of flexion with a varus load applied. In this position, sutures from the anterior and posterior all-suture anchors were used to secure the anterior and posterior limbs of the graft to the bone at the sublime tubercle.
A 3.2-mm drill bit was used to drill a bicortical hole through the ulna at the distal-most aspect of the native UCL. The button that was previously loaded onto the graft was inserted through the ulna and deployed. Sutures were tensioned to reduce the graft to the ulna and secured with surgeon knots. This created fixation at the proximal and distal aspects of the distal extent of the UCL with graft-cortical contact between the points.
With the arm again reduced in 30° of flexion and varus, the suspensory loop on the humeral side was retensioned and tied over the humeral bone bridge, ensuring that all slack was removed from the system (Figure 1).
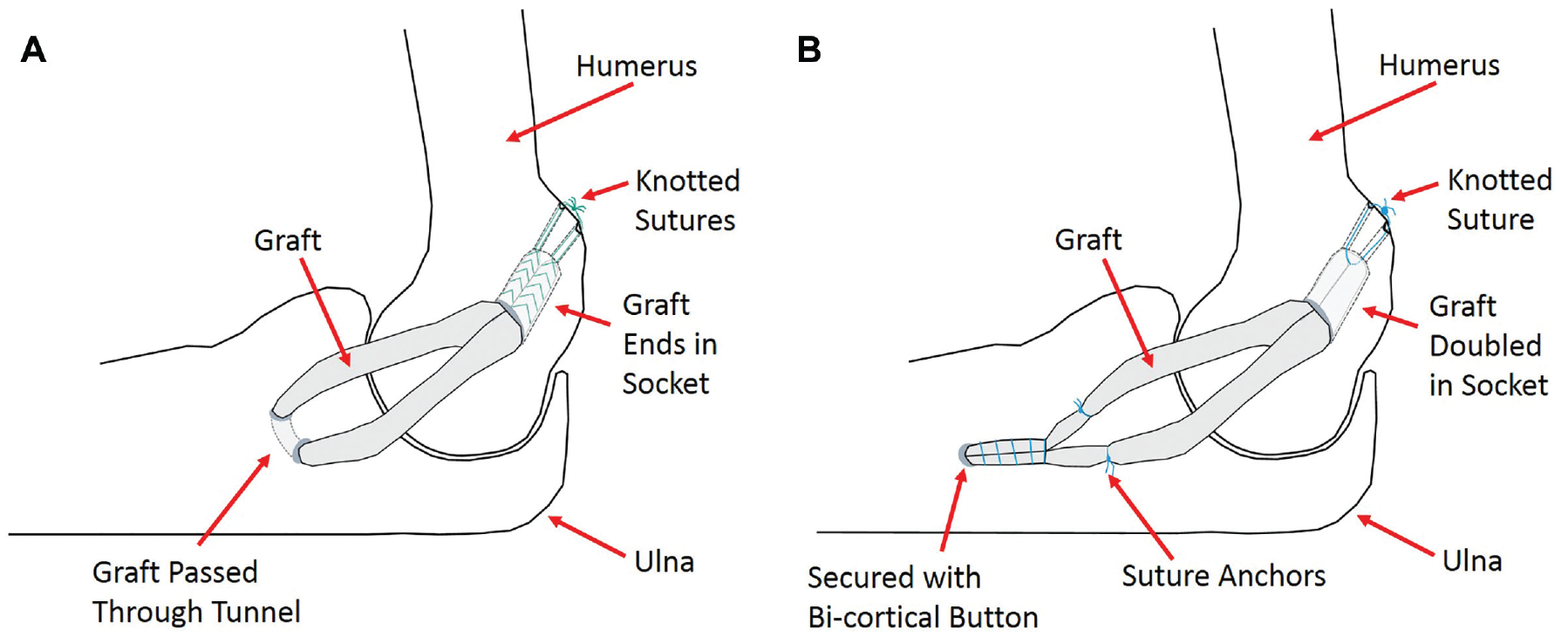
Examples of the reconstruction techniques. (A) Docking technique with proximal attachment of graft to the ulna. (B) Anatomic technique with ulnar attachment of graft extending distally.
Biomechanical Testing
Each specimen was mounted in custom fixtures on a servohydraulic load frame as previously described (Figure 2). 6 Retroreflective markers affixed to the humerus and ulna coupled with a motion capture camera system (Motion Analysis Corp) were used to track the motion of the bones throughout testing. Virtual markers were created on either side of the joint line at each flexion angle to facilitate measurement of gap change under valgus stress. A valgus load was applied to each specimen with an intact UCL at 30°, 60°, 90°, and 120° of flexion at 2 mm/s until a 5-Nċm moment was achieved. Load and piston displacement were recorded throughout the test along with the 3-dimensional coordinates of all physical and virtual markers. The resolution of the motion capture system was 0.1 mm. Specimens then underwent UCLR, as randomized to the docking or anatomic technique, and were retested. The primary outcome metric was the magnitude of the gap at the peak moment of 5 Nċm. A sample size analysis was performed comparing the gap in the intact versus reconstructed state for the first 4 specimens tested, to arrive at a sample size of 9. This analysis was set to detect a difference in gap of 1 mm with a 0.75-mm SD. Gap size was compared using a 2-way analysis of variance with the Holm-Sidak method for pairwise comparisons. The same method was used to compare gap change from the intact state for both UCLR techniques at each flexion angle. Significance was set at P < .05 for all comparisons.
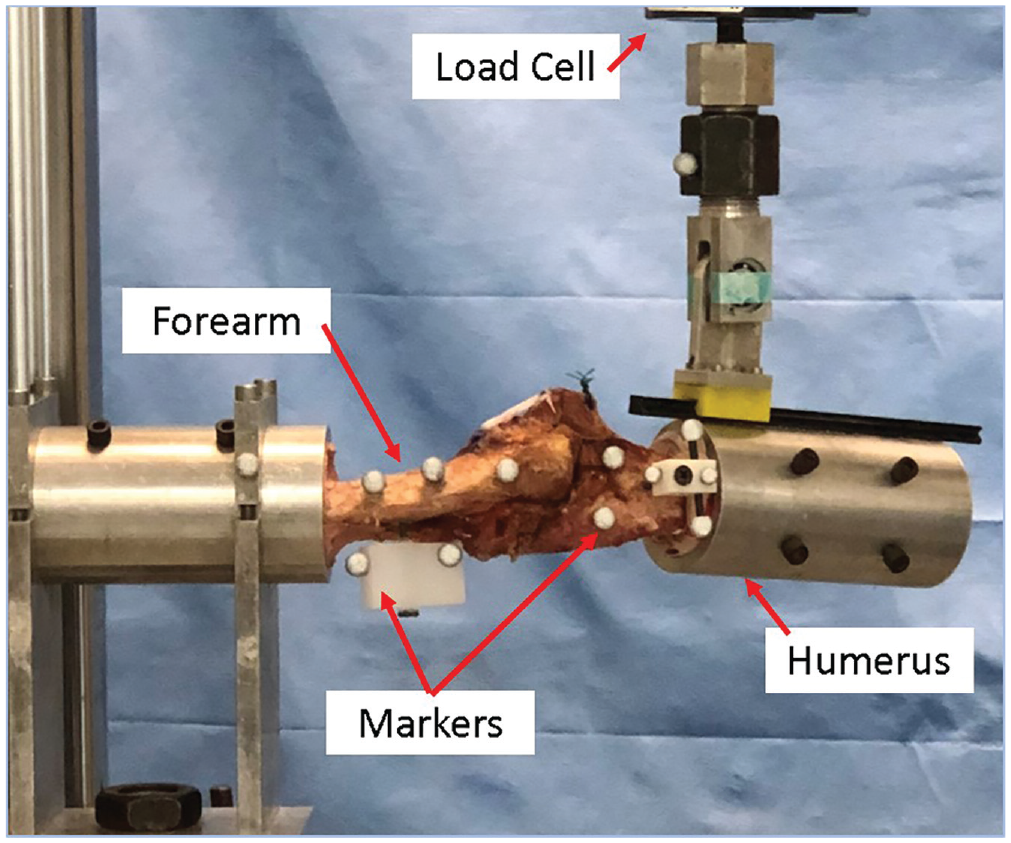
Test setup showing the specimen with motion-tracking markers. The hinge and slider on the humeral fixture allowed for valgus loading of the joint when the piston, connected to the forearm, moved.
Results
There were no significant differences in patient characteristics for the 2 reconstruction groups (Table 1). There was also no significant difference in the amount of gap created under 5-Nċm valgus versus the intact state in specimens used for either the docking technique or the anatomic technique. Finally, there was no difference in the amount of gap or the change in gap from the intact state between the reconstruction groups at any level of flexion (Figures 3 and 4).
Donor Characteristics a
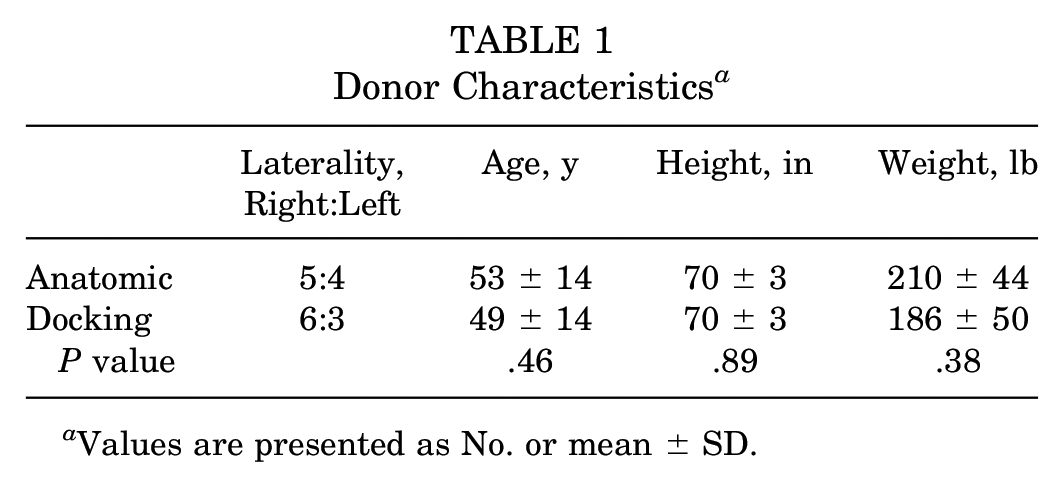
Values are presented as No. or mean ± SD.
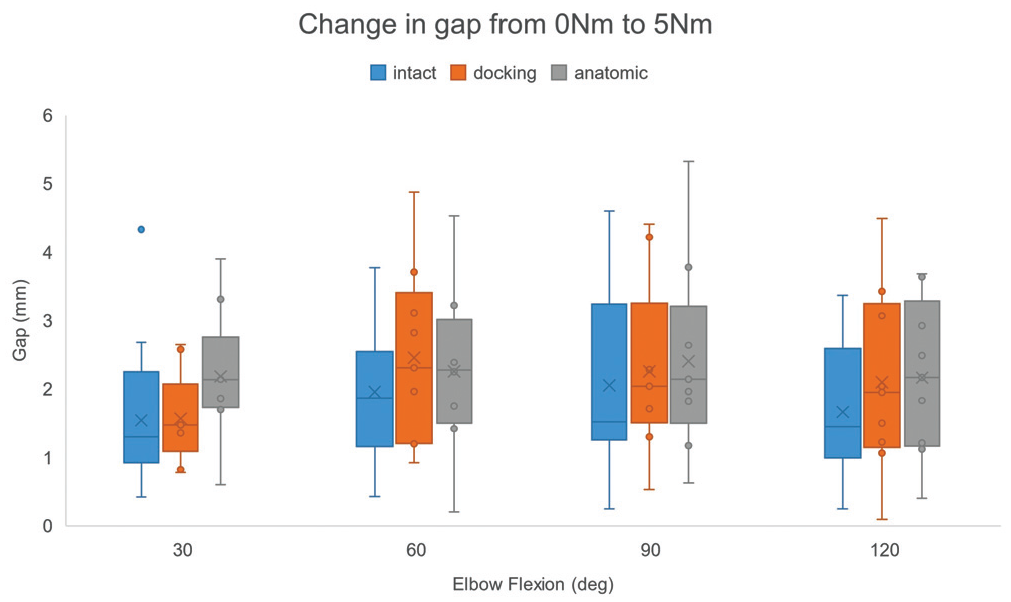
Gap change for intact and reconstructed ulnar collateral ligament. There were no significant differences at any flexion angle. ×, mean; line, median; box, interquartile range; error bars, local minimum and maximum. For example, at 90°, the mean gap was 2.3 mm and 2.4 mm for the docking and anatomic reconstructions respectively.
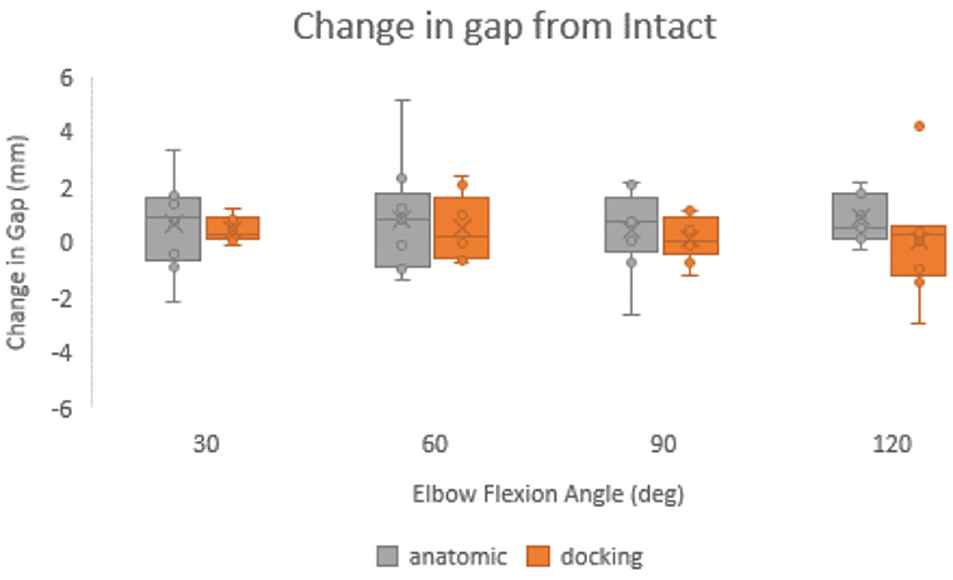
The change in gap from intact to reconstruction was not significantly different for either reconstruction type at any flexion angle. ×, mean; line, median; box, interquartile range; error bars, local minimum and maximum.
Discussion
The principal finding of this study was that a novel anatomic UCLR technique designed to reproduce the native UCL insertion distal to the sublime tubercle demonstrated similar gap resistance to valgus stress as compared with the docking technique in a cadaveric model. Although the gapping after reconstruction was within a clinically accepted range, both techniques had statistically larger gapping than their intact states.
Many UCLR techniques have been described and biomechanically investigated. The main mechanical outcomes when considering which technique to use are gap resistance and load to failure. Camp et al 3 showed that the anatomic UCLR technique had higher failure load and stiffness as compared with the docking technique. In this context, the results of the current study add to growing evidence in favor of the anatomic UCLR technique as a biomechanically sound construct and a viable alternative to the docking technique.
Bodendorfer et al, 2 Dugas et al, 5 and Leasure et al 12 have all investigated gapping after UCLR with the elbow at 90° flexion. Gapping at 90° in our study was 2.3 ± 1.3 mm (mean ± SD) for the docking technique and 2.4 ± 1.4 mm for the anatomic technique (as seen in Figure 3). Bodendorfer et al saw similar results with the docking reconstruction, with gapping of 2.3 ± 0.48 mm at 90° of elbow flexion. Dugas et al compared a modified Jobe reconstruction with a UCL repair with internal bracing. They reported gapping of 2.86 ± 2.14 mm and 2.02 ± 1.16 mm for their reconstruction and repair groups, respectively, at 90° elbow flexion. These values were similar to our findings, although they tested at a higher torque. Similarly, Leasure et al measured gapping at 90° of flexion, recording 2.78 ± 0.84 mm and 1.82 ± 1.22 mm with 10 Nċm of torque for each reconstruction technique. We removed all soft tissue with the exception of the capsular ligaments, as Bodendorfer et al did, while Dugas et al and Leasure et al left the soft tissues in place. This may be why they found similar gapping at larger torques. In our study as well as these, there was no difference in gapping between the reconstruction and repair groups.2,5,12 These studies also tested load to failure with similar results and no significant differences between the reconstruction and repair groups, while Camp et al 3 noted a higher load to failure for the novel anatomic reconstruction.
One potential long-term advantage of the anatomic technique is the onlay of the graft on the bone. Tan et al 18 evaluated graft tendon healing within a bone tunnel as compared with tendon healing on the cortical surface in a rabbit model of biceps tenodesis. They indicated that there was minimal interdigitation in the bone tunnels as compared with the healing of the graft on the surface of the cortical bone. Unfortunately, no study has yet to compare differences between standard UCLR techniques and this novel anatomic technique in the long term. Griffith et al 11 found no differences in return to play when comparing surgical outcomes among UCLR techniques or the graft type used in 566 Major League Baseball professional pitchers. The reconstruction techniques employed were predominantly the modified Jobe technique (51%) and the standard docking technique (30%). Return to play for all pitchers regardless of technique was approximately 80%. Return to play has not been investigated at this time for the novel anatomic technique.
Limitations of this study include the use of cadaveric specimens and that only the capsuloligamentous structures were left intact. This means that there were no active muscles to contribute to elbow stability. As our goal was to investigate the gapping of these 2 reconstructions, the removal of all other structures gave us a clean view of the contribution of each reconstruction. Furthermore, we compared the intact state with the reconstructed state. It should be noted that the UCL transected state was not tested. Although this may have shown clear valgus instability, our focus was on the comparison of reconstruction techniques. The other limitation to our cadaveric study is that stability and resistance to valgus load were tested at time zero and did not consider the effects of healing. Future in situ studies may demonstrate differences in bone-tendon healing and, perhaps, gap resistance after the final maturation phase of healing.
Conclusion
Ulnohumeral joint gapping and resistance to valgus stress were similar between the anatomic technique and the docking technique for UCLR in a cadaveric model. We thus provide evidence that the anatomic technique is a viable alternative to the standard docking technique for UCLR in a cadaveric model.
Footnotes
Submitted February 12, 2021; accepted November 22, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: K.K.M. has received support for education from United Orthopedics, Arthrex, and Smith & Nephew, and her sibling works for Smith & Nephew. M.C.F. has received honoraria from DJO; support for education from Medwest Associates and Smith & Nephew; consulting fees from Encore Medical; and grants from Arthrex and Acumed. J.S.D. has received research support, consulting fees, and royalties from Arthrex; royalties from Conmed Linvatec; and consulting fees from Merck Sharp & Dohme, Trice Medical, and Wright Medical. J.S.D is also part owner of ViewFi. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.