
Abstract
Background:
Labral reconstruction has been described as a treatment option for irreparable labral tear. Labral graft size ranges from 5 to 7 mm2 for reconstruction. A thicker labral graft could support mechanical stability and protect cartilage better. No study has compared the effect of graft thickness on clinical outcomes.
Purpose/Hypothesis:
The purpose of this study was to compare patient-reported outcomes between hips reconstructed with an autologous iliotibial band (AUITB; 5 mm2) graft and with an allogenic tibialis anterior (ALTA; 7 mm2) tendon graft. Our hypothesis was that hips reconstructed with a thicker allograft (7 mm2) would have better clinical outcomes than those with a smaller autograft (5 mm2).
Study Design:
Cohort study; Level of evidence, 2.
Methods:
A total of 42 patients (aged 21 to 54 years) underwent arthroscopic hip segmental labral reconstruction during the study period of January 2016 to November 2018. Twenty patients had reconstruction with AUITB grafts (5 mm2) and 22 with ALTA grafts (7 mm2). Both groups had minimum 2 year follow-up. Patients were evaluated with patient-related outcome scores: modified Harris Hip Score, Nonarthritic Hip Score, and Hip Outcome Score–Sports Specific. Pain evaluation was performed using a visual analog scale.
Results:
There were significant differences in all studied variables when comparing pre- and postoperative scores. Yet, there were no differences in terms of patient-related outcome scores between the groups postoperatively. Postoperative visual analog scale scores averaged 2.1 for the AUITB group vs 1.9 for the ALTA group (P = .89); modified Harris Hip Score, 82.7 vs 83.3 (P = .77); Nonarthritic Hip Score, 81.1 vs 82.2 (P = .81); and Hip Outcome Score–Sports Specific, 81.6 vs 82.5 (P = .67).
Conclusion:
No differences were found in terms of clinical outcomes between the 7-mm2 ALTA graft and the 5-mm2 AUITB graft. Both graft types and thicknesses might be considered comparable choices for primary reconstruction. Although a thicker-graft labral reconstruction seemed to have more ability to cover joint surface, clinical results did not show any superiority of a thicker graft whether it is autologous or allogenic.
The primary function of a hip labrum is to augment joint stability.10,20,23 This is accomplished by increasing articular surface area and acetabular volume, as well as by creating a suction seal effect that maintains relative negative pressure within the joint.20,23 A torn labrum can result in increased anterior translation and external rotation, as well as higher contact stresses between femoral cartilage and acetabular cartilage. Therefore, the treatment of labral tears is focused on restoring the native hip joint anatomy.2,9,16
Labral reconstruction is performed to restore the natural biomechanics of the labral suction seal while decreasing pain attributed to resection of the damaged and irreparable labral tissue or native tiny labrum, which are known pain generators.3,6,16,20 In cadaveric studies, Nepple et al 16 and Philippon et al 20 found that labral reconstruction improved the strength of the labral suction seal, restored stability against distraction to levels similar to those of a native labrum, and restored peak fluid pressurization levels similar to the intact labrum. In a retrospective analysis of 82 patients who underwent labral reconstruction using autologous iliotibial band (AUITB) grafts with a mean follow-up of 10 years, Philippon et al 18 reported a survival rate of 61%, which improved to 90% in patients with >2 mm of remaining joint space. Trivedi et al 23 presented a systematic review of 11 studies reporting clinically significant functional improvements after arthroscopic labral reconstruction and low rates of complications, revision surgery, and progression of arthritis. However, these studies did not provide reliable information about the graft size.
Multiple graft options exist for labral reconstruction, such as autografts of the iliotibial band, gracilis, and semitendinosus tendons as well as allografts (tibialis anterior tendon and semitendinosus).1,7,11,12,14,19,22 In the cited studies, the labral graft size differed from 5 to 7 mm2. However, there is limited evidence about the effect of graft size on outcomes of labral reconstruction. Zhang 27 recommended that the diameter of the labrum should be >4 mm2 to restore the natural biomechanics of the labral suction seal. He also recommended use of a thicker graft for labral reconstruction or augmentation. As the natural labral diameter is between 5 and 7 mm2, there is no consensus on an optimal labral graft size for reconstruction.
The purpose of this study was to compare patient-reported outcomes (PROs) between hips reconstructed with AUITB (5 mm2) grafts and allogenic tibialis anterior (ALTA; 7 mm2) tendon grafts. The hypothesis was that hips reconstructed with bigger allografts (7 mm2) would have better clinical outcomes than those with smaller autografts (5 mm2) in terms of clinical and functional findings.
Methods
After the institutional ethical board authorization was obtained, a prospective analysis was performed of patients at one institution who underwent arthroscopic hip labral reconstruction between January 2016 and November 2018. The grafts were either iliotibial band autografts (AUITBs) with a diameter of 5 mm2 or tibialis anterior allografts (ALTAs) with a diameter of 7 mm2. The patients were aged 21 to 54 years at the time of surgery. Hips were excluded if they underwent previous ipsilateral hip surgery; if they had a concomitant Ganz osteotomy; or if they had a preoperative lateral center-edge angle <25°, overcoverage, or Outerbridge grade 3 or 4 cartilage lesions on either the femoral head or the acetabulum at the time of surgery. The patients were informed and signed the consent about the study protocol and graft type that might be used.
Labral pathology was diagnosed by clinical examination, including a diagnostic local anesthetic injection, anterior impingement maneuver, and magnetic resonance imaging. Patients were offered hip arthroscopy if they had recalcitrant hip pain with a preserved joint space (Tönnis 0 and 1) and had failed nonoperative treatment including physical therapy and corticosteroid injection.
The indications for labral reconstruction were any labrum thicker than 8 mm2 or thinner than 4 mm2 and irreparable labral tear between 5 and 7 mm2. Among the 50 patients who had arthroscopic hip labral reconstruction within the study period, 48 met the inclusion criteria for labral reconstruction: 6 patients were lost at follow-up and 42 were evaluated (Figure 1). AUITB grafts were used in 20 patients (20 hips; AUITB group) and ALTA grafts in 22 patients (22 hips; ALTA group). Randomization of the patients was made by a random number generator, and patients were informed about the type of the procedure.
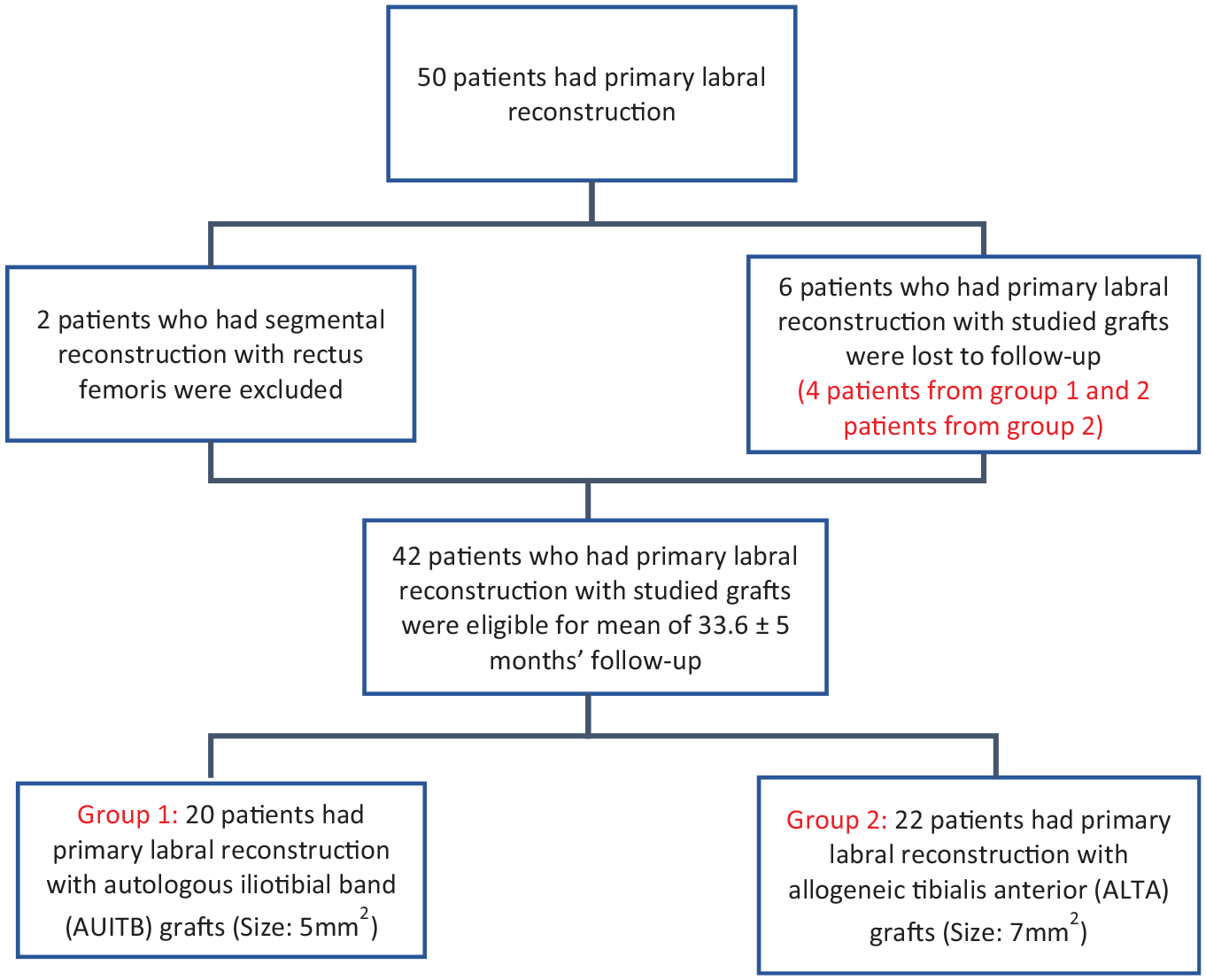
Flowchart of patient selection.
Surgical Technique
All patients underwent an arthroscopic labral reconstruction. The possibility of performing a reconstruction was typically considered after reviewing the relevant imaging and previous procedures, including hip corticosteroid injection and physical therapy, but the final decision was made intraoperatively if the labrum was tiny and irreparable. Patients were informed about reconstruction options.
Arthroscopic hip labral reconstruction surgery was performed via a 3-portal approach with the patient in the supine position on a traction table. Diagnostic arthroscopic surgery confirmed the extent of damage to native labral tissue. If necessary, osteoplasty at the femoral head-neck junction and/or an acetabular rim trim were performed to decompress the cam and pincer components. Irreparable labral tissue was removed, and the remaining labrum was debrided to a stable base of healthy tissue on either side of the defect, while the acetabular rim was prepared.
For the AUITB group, a longitudinal incision was made over the greater trochanter, and a rectangular graft was harvested from the iliotibial band. Ideally, the tissue removed was 15 to 20 mm in width and 30% greater than the measured size of the defect in length. The graft was tubularized with absorbable sutures; the size was set at 5 mm2; and the length was 34 ± 4.7 mm (mean ± SD; Figure 2). The graft was inserted through the midanterior portal. A side-to-side anastomosis with the native labral stump was created. Three or four 2.9-mm PushLock anchors (Arthrex) were placed according to acetabular length at 1-cm intervals until the graft was secured to the acetabular rim.17,24 In the ALTA group, fresh-frozen ALTA grafts were used with a size of 7 mm2 and a length of 32.5 ± 4.3 mm. Fixation was identical to the AUITB group (Figure 3). Traction was released and the hip taken through a dynamic range of motion examination to confirm that the labral seal had been successfully reestablished.
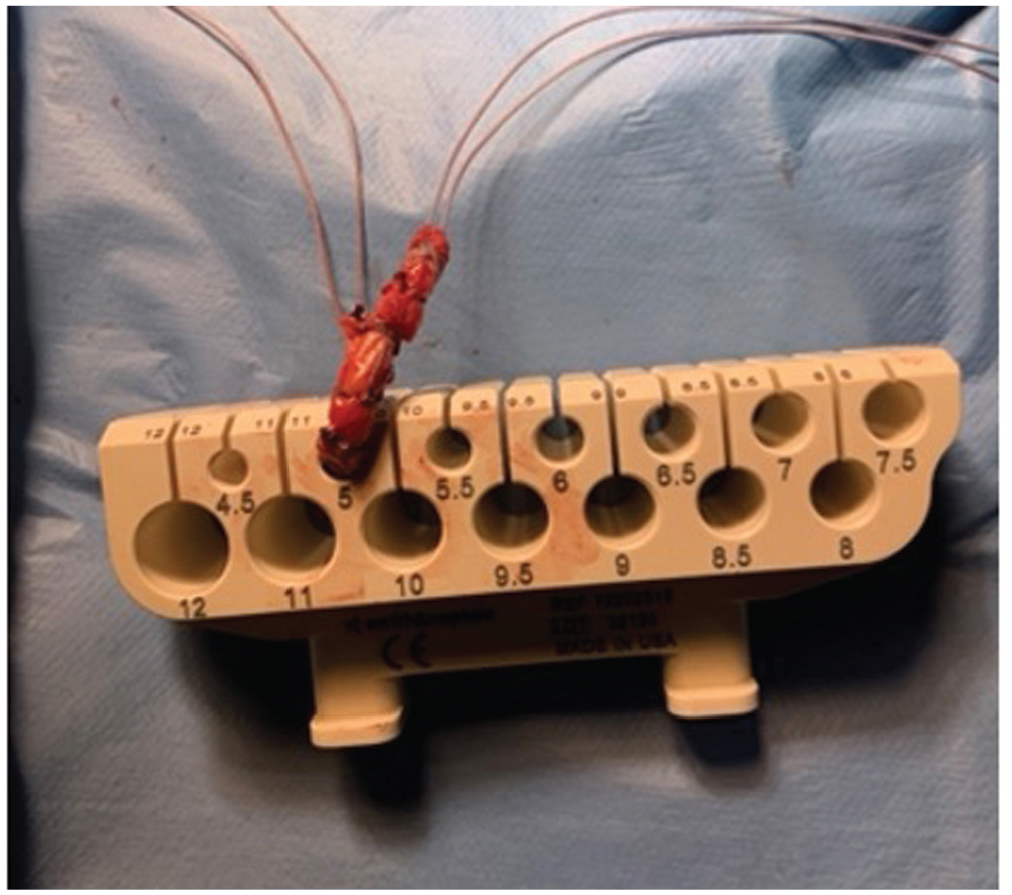
Iliotibial band was tubularized with absorbable sutures, and size was set at 5 mm2.
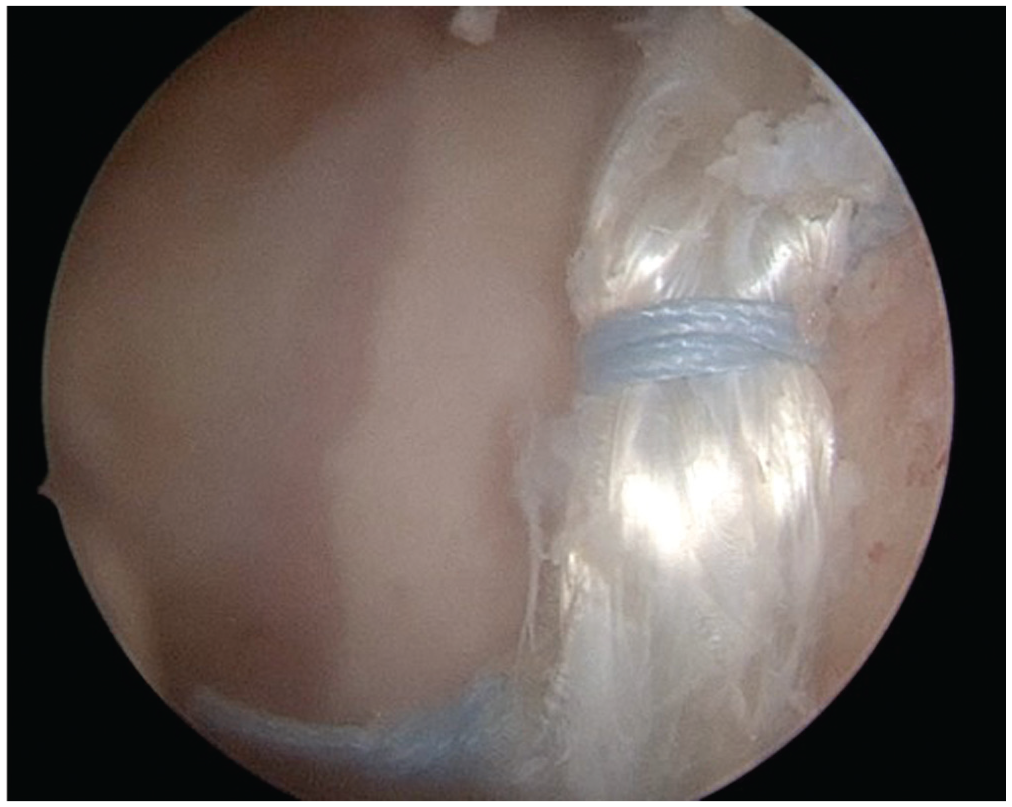
Hip labral reconstruction with fresh-frozen tibialis anterior tendon allograft.
Follow-up Protocol
Postoperative management has been described and was the same for all hips regardless of the graft type used.25,26 Patients were allowed partial weightbearing for 2 weeks and progressed to weightbearing as tolerated over the fourth week. Physical therapy was initiated during the second postoperative week and continued for 4 to 6 weeks.
Postoperative Outcome Measures
Preoperative clinical examination, imaging, and surgical data were recorded prospectively by the lead author, who was the lead surgeon in all cases (B.K.). The following PROs were included: modified Harris Hip Score (mHHS), Nonarthritic Hip Score (NAHS), and Hip Outcome Score–Sports Specific (HOS-SS). Pain evaluation was done by visual analog scale (VAS).21,25,26
To establish baseline PROs, all patients completed preoperative questionnaires within the month before surgery. After surgery, these same outcome scores were also collected. PROs were collected postoperatively at the 3-, 6-, 9-, and 12-month follow-up visits, as well as annually afterward. Clinical failure was defined as the need for revision ipsilateral hip surgery.
Statistical Analysis
Statistical power analysis was performed to calculate the sample size. A mean difference of 5 points in mHHS, NAHS, and HOS-SS was defined as the minimal clinically relevant difference. With a power of 80%, a 95% confidence level, and an alpha value of .05, the results of the power analysis determined a sample size of 20 in each group. The data were analyzed using SPSS Version 25.0 (IBM). The results were presented as frequency, percentage, mean, and standard deviation. The Kolmogorov-Smirnov test was performed to test if the numerical variables were normally distributed. The independent samples t test, paired-samples t test, and chi-square (or Fisher exact) test were used to compare statistical significance between groups. P < .05 was considered statistically significant.
Results
A total of 42 patients were included in the study: 20 in the AUITB group (47.6%) and 22 in the ALTA group (52.4%). There were 28 female and 14 male patients. The average age was 32.6 ± 7 years. There were no significant differences between the groups concerning demographic and baseline data. Mean follow-up times were 32.7 ± 5.5 months for the AUITB group and 34.6 ± 5.7 months for the ALTA group, which proved to be a nonsignificant difference (P = .29). The average follow-up time was 33.6 ± 5 months. Patient demographics and findings are summarized in Table 1.
Comparison of Variables Between the Groups a
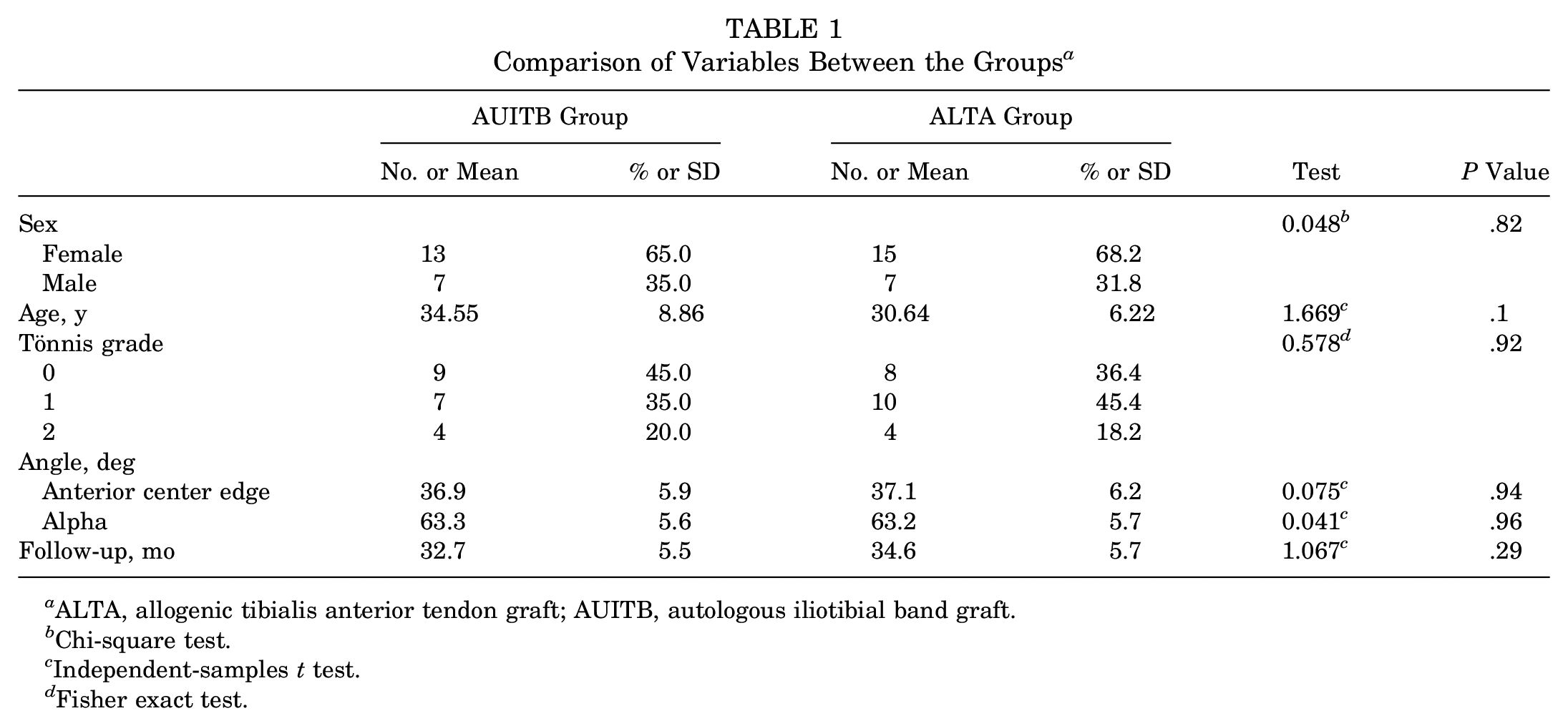
ALTA, allogenic tibialis anterior tendon graft; AUITB, autologous iliotibial band graft.
Chi-square test.
Independent-samples t test.
Fisher exact test.
In terms of preoperative radiographic measurements, the mean alpha angle for the AUITB group was 63.3°± 5.6° and for the ALTA group, 63.2°± 5.7° (P = .96). In terms of hip dysplasia, the anterior center-edge angle was calculated as 36.9°± 5.9° and 37.1°± 6.2° in the AUITB and ALTA groups, respectively (P = .94). Additionally, 80% of the patients had Tönnis grade 0 or 1 hips in the AUITB group and 81.8% in the ALTA group. The length of the graft was 34 ± 4.7 mm and 32.5 ± 4.3 mm in the AUITB and ALTA groups, respectively (P = .67), which also showed the defect of the labrum which was reconstructed.
Table 2 illustrates the intraoperative findings documented during diagnostic arthroscopic surgery. No differences were noted between groups in terms of acetabular labrum articular disruption (ALAD) grade,19-21 acetabular Outerbridge grade, Seldes-defined labral tears, or femoral head Outerbridge grade. Table 3 shows the intraoperative procedures that were performed. There were no differences between groups in terms of intraoperative procedures. No patients underwent an isolated femoroplasty or a pincer excision procedure. All patients in both groups underwent combined acetabuloplasty and femoroplasty.
Comparison of the Intraoperative Findings Between the Groups a
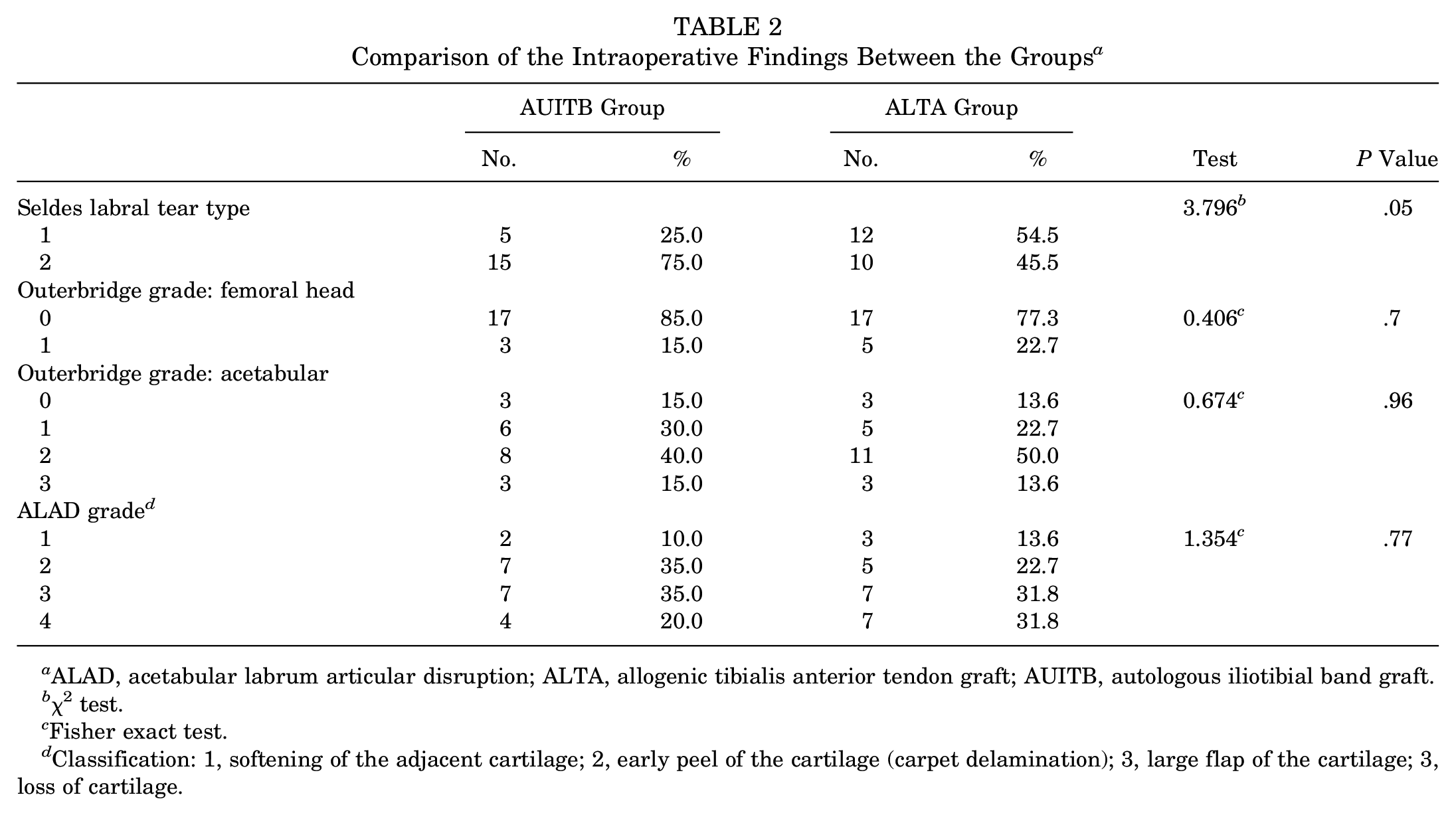
ALAD, acetabular labrum articular disruption; ALTA, allogenic tibialis anterior tendon graft; AUITB, autologous iliotibial band graft.
χ2 test.
Fisher exact test.
Classification: 1, softening of the adjacent cartilage; 2, early peel of the cartilage (carpet delamination); 3, large flap of the cartilage; 3, loss of cartilage.
Intraoperative Procedures Performed During Arthroscopic Hip Labral Reconstruction Surgery
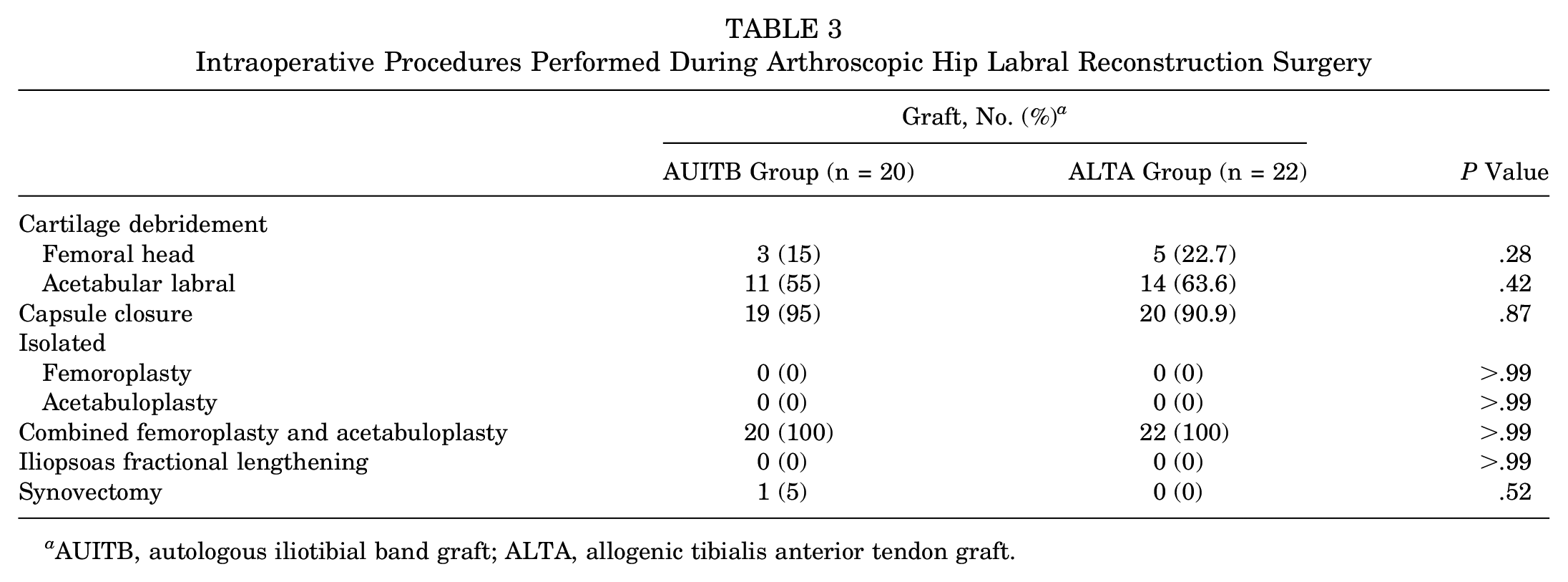
AUITB, autologous iliotibial band graft; ALTA, allogenic tibialis anterior tendon graft.
There were significant differences in all studied variables when pre- and postoperative data were compared. Postoperatively, there were no differences in terms of PROs between groups (Table 4). Average postoperative VAS scores were 2.1 in the AUITB group and 1.9 in the ALTA group (P = .89); mHHS, 82.7 and 83.3 (P = .77); NAHS, 81.1 and 82.2 (P = .81); and HOS-SS, 81.6 and 82.5 (P = .67).
Comparison of the Outcome Variables Before and After the Operation a
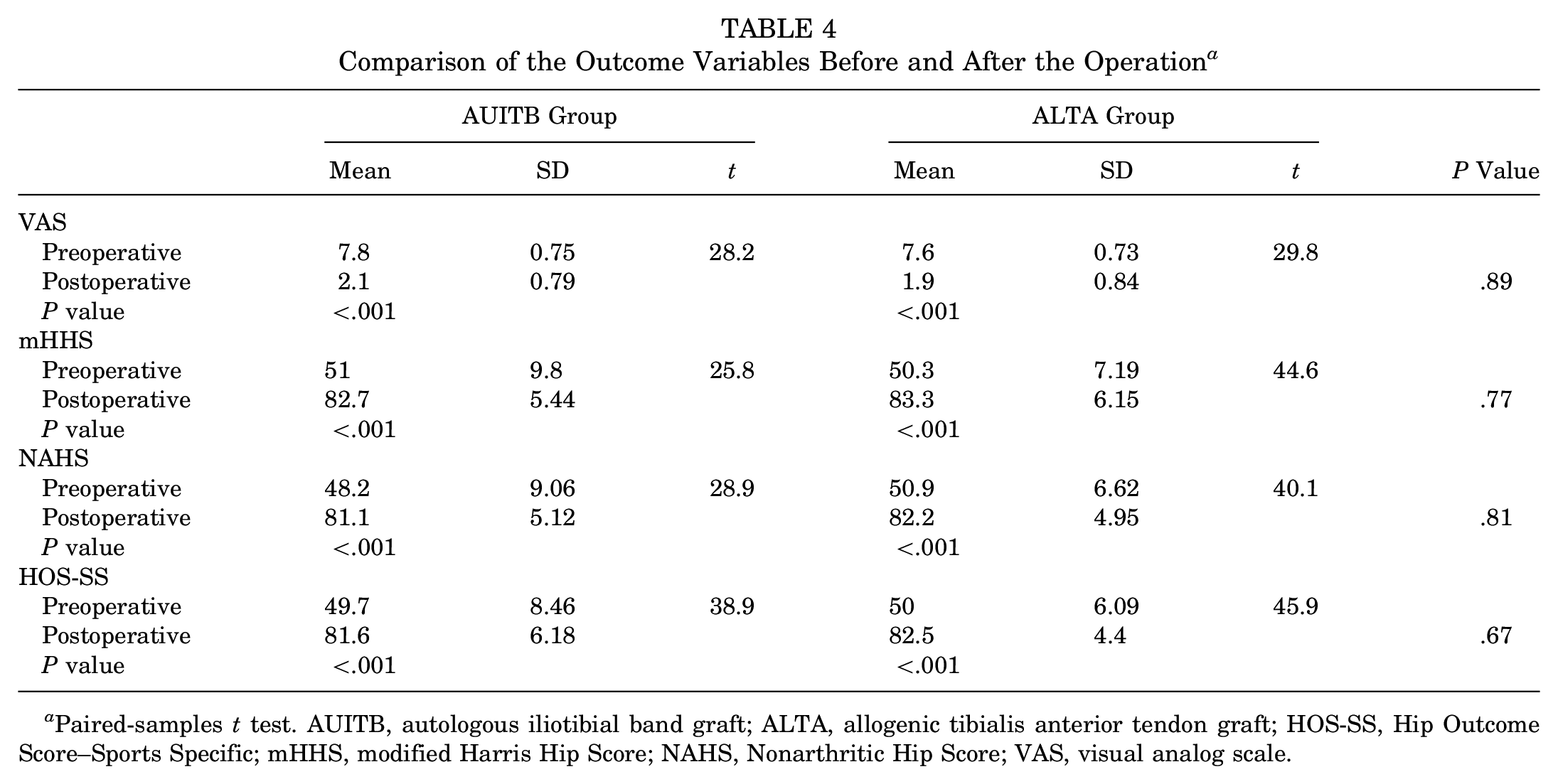
Paired-samples t test. AUITB, autologous iliotibial band graft; ALTA, allogenic tibialis anterior tendon graft; HOS-SS, Hip Outcome Score–Sports Specific; mHHS, modified Harris Hip Score; NAHS, Nonarthritic Hip Score; VAS, visual analog scale.
There were no major postoperative complications, such as femoral neck fractures, osteonecrosis, deep infections, pulmonary embolism, and abdominal compartment syndrome. Five patients had transient neurapraxias of the pudendal nerve that resolved completely by 3 months. There were no sciatic, femoral, or lateral femoral cutaneous neurapraxias. Patients reported an average 2 weeks of incisional hip pain (range, 1-3 weeks) at the iliotibial band graft area without residual complaints of pain, weakness, or knee functional deficit. There were no revision procedures or conversions (or scheduled conversions) to resurfacing hip arthroplasty or total hip arthroplasty.
Discussion
Primary arthroscopic hip total labral reconstruction yielded significant improvements in PROs and high patient satisfaction. The current study found no significant differences in PRO scores between patients who underwent labral reconstruction using 5-mm2 AUITB grafts or 7-mm2 ALTA grafts at a minimum 2-year follow-up. Previous studies recommended a labrum >4 mm2 to restore the natural biomechanics of the labral suction,13,21,27 assuming that bigger augmentations or reconstructions would provide better clinical results. 27 The study hypothesis that a thicker labrum would have a better clinical outcome was rejected.
The main function of the labral tissue is to keep the joint fluid inside the joint, like a water-tight seal.4,5,8,15 Joint liquid balances the amount of pressure on the cartilage. Seldes et al 22 reported that mean labral thickness was 5.5 ± 1.5 mm at the anterosuperior quadrant. The purpose of reconstruction is to make a labrum-like tissue that mimics the seal function. For that reason, the thickness and nature of the graft tissue have importance. 13 Labral tissue decreases contact stress via increasing the contact area on the cartilage.16,20 When compared with a thinner graft, a thicker graft increases the contact area; therefore, positive results can be expected. However, there are some issues caused by using thicker grafts, such as decreasing vascularity of reconstruction. At the same time, a thicker graft means a greater area to feed by the vascular system.
A number of factors may determine graft choice, such as patient preference, surgeon experience, operative time, morbidity, and cost. Autografts and allografts are both options for hip labral reconstruction.3,13 Autologous and allogenic semitendinosus, tibialis anterior tendon, and AUITB grafts and indirect head of the rectus femoris are commonly used.1,7,11,12,14,19,22 Lee et al 12 showed in a biomechanical study that there was no statistical diversity between iliotibial band and semitendinosus grafts by their cross-checking the contact area, contact pressure, and peak forces. Thus, advantages of allogenic and autogenic grafts over each other could not be shown, and previous research does not recommend an ideal graft.13,22,23
In previous studies,12-14,19 labral autograft and allograft size has differed from 5 to 7 mm2. However, there is limited literature about the effect of graft size on clinical outcomes of labral reconstruction. In an editorial, Zhang 27 recommended a labral size >4 mm2 to restore the natural biomechanics of the labral suction seal. As the natural labral size is between 4 and 8 mm2, there is no consensus on an optimal labral graft size for reconstruction.
Another question might be the effect of the graft type used rather than the graft size. According to recent studies and review articles, no difference was found between allogenic and autogenic grafts on clinical outcomes of labral reconstruction.13,23,24 Maldonado et al 13 presented a cohort of 29 patients who had undergone labral reconstruction with hamstring allograft (17 hips) or autograft (12 hips). The authors concluded that there were no differences in clinical outcomes between the graft types. In the present study, graft size and type were compared. As clinical outcomes and comparison of allografts and autografts were well studied previously, we focused on the clinical effect of the graft size.
In the current study, there were significant differences in all studied variables when comparing pre- and postoperative function, which showed that all patients from both groups were satisfied from labral reconstruction surgery. Yet, there were no differences in PROs between groups postoperatively. Postoperative VAS scores averaged 2.1 for the AUITB group and 1.9 for the ALTA group; mHHS, 82.7 and 83.3; NAHS, 81.1 and 82.2; and HOS-SS, 81.6 and 82.5. This showed no difference between groups in terms of clinical outcomes.
According to the hypothesis, a thicker-graft labral reconstruction might have more ability to cover cartilage surfaces, which increases the volume of the acetabulum and supports mechanic stability, as compared with a thinner graft. Clinical outcome results showed that the hypothesis was rejected. The 7-mm2 ALTA graft was not superior to the 5-mm2 AUITB graft in terms of clinical and functional results. However, more research is needed before drawing conclusions. Another important point was the condition of the cartilage at the acetabulum and femoral head. No differences were noted between groups in terms of ALAD, acetabular Outerbridge, and femoral head Outerbridge grades. These data might show that superior clinical results could be due to cartilage defects at the acetabulum and femoral head rather than labral reconstruction choices. Furthermore, this study is one of the first to compare the effect of thickness of grafts on clinical outcomes for patients undergoing primary labral reconstruction.
Limitations
There are some limitations of the study. Although we met the sample size calculation, more patients in the groups would be better to make stronger scientific outcomes. Second, a longer follow-up is still needed to determine the durability of our findings. Third, subjective or objective measurements of iliotibial band site morbidity were not taken into account. Fourth, other tendon diameters in terms of thickness were not compared. For example, we do not know the clinical results of 4 vs 8 mm2, but it can be assumed that labral grafts thinner than 4 mm2 can not make a good seal and that labral grafts thicker than 8 mm2 could form impingement. This might also be investigated. Fifth, the same graft type was not used for comparison, but our aim was to compare the clinical outcomes of the 2 most popular graft types and thicknesses. Finally, the groups were not matched per the other procedures performed; thus, these associated procedures may influence the results.
Conclusion
Primary arthroscopic hip labral reconstruction yielded improvements in PROs and high patient satisfaction. No differences were found in clinical outcomes between 7-mm2 ALTA grafts and 5-mm2 AUITB grafts. Both graft types and thicknesses might be considered comparable choices for primary reconstruction. Although thicker allografts might have better ability to cover the cartilage surface and improve mechanical stability, clinical results did not demonstrate any superiority. These data might show that superior clinical results could be due to cartilage defects at the acetabulum and the femoral head rather than labral reconstruction choices.
Footnotes
Submitted July 8, 2021; accepted December 15, 2021.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.