
Abstract
Background:
Rotator cuff tears represent a significant cause of shoulder pain and dysfunction in the United States. The development of these injuries is associated with older patient age and higher levels of physical activity; however, data regarding the rate of return to work after arthroscopic rotator cuff repair in patients older than 50 years of age who have physically strenuous jobs is inconclusive.
Purpose/Hypothesis:
The purpose of this study was to report short term outcomes and return to work rates after arthroscopic rotator cuff repair in a cohort of patients aged 50 to 60 years working in manual labor jobs. It was hypothesized that arthroscopic rotator cuff repair would result in good functional outcomes for these patients and allow for return to work rates in excess of 80%.
Study Design:
Case series; Level of evidence, 4.
Methods:
Preoperative and final evaluations including the pain visual analog scale (VAS), the Single Assessment Numeric Evaluation (SANE), and the American Shoulder and Elbow Surgeons (ASES) Shoulder Score were collected. A total of 73 patients were screened for inclusion. Nineteen patients were outside of the inclusion age range, 2 underwent exclusionary concomitant procedures, and 4 patients were lost to follow up, leaving a total of 48 patients with a mean follow up of 34.02 months (range, 24-67 months) available for analysis. None of the patients were involved in a workers’ compensation claim. Subgroup analysis was performed to determine if arm dominance or tear size affected surgical outcomes or return to work rates.
Results:
After arthroscopic rotator cuff repair, 43 of 48 patients (89.6%) were able to return to manual labor positions. Tears were classified using the Southern California Orthopaedic Institute Classification at the time of repair as massive (C4) in 9 patients (18.75%), large (C3) in 13 patients (27.08%), medium (C2) in 21 patients (43.75%), and small (C1) in 5 patients (10.42%). At latest follow up, the mean VAS decreased from 8.0 ± 1.81 to 0.46 ± 1.20, the average SANE increased from 47.50 ± 18.59 to 91.88 ± 12.30, and the average ASES score improved from 39.58 ± 10.71 to 93.44 ± 11.97 (P < .0001). Outcomes did not differ between patients who underwent surgery on their dominant shoulder and those who underwent surgery on their nondominant shoulder. The overall postoperative complication rate was 8.33%.
Conclusion:
Arthroscopic rotator cuff repair portended favorable outcomes and high rates of return to work in this cohort of manual laborers, with 89.6% of patients able to return to work.
Rotator cuff tears represent a significant cause of shoulder pain and dysfunction, with >250,000 repairs performed annually in the United States.12,15,22 Patients with rotator cuff injuries are evaluated with symptoms ranging from mild discomfort to severe, disabling pain and weakness.11,12,37 Rotator cuff tears are associated with older age and higher levels of physical activity, and it is estimated that more than two thirds of rotator cuff repairs are performed on working age patients.15,22 As our workforce continues to age, it is expected that the incidence of rotator cuff pathology will rise.15,36
Arthroscopic rotator cuff repair (aRCR) is a well studied and reliable procedure that consistently produces excellent functional outcomes.1,2,10,13,24,26,38 Multiple studies have reported on return to work rates after aRCR.6,14,15,21 A recent systematic review by Haunschild et al 15 reported that 62.3% of patients returned to their previous level of work at an average of approximately 8 months after aRCR. There is less robust literature, however, regarding the rate of return to work among manual laborers older than 50 years of age after aRCR. Strenuous physical labor has been associated with lower postoperative functional outcomes and delayed return to work.6,12,25 Furthermore, age and workers’ compensation status are known risk factors for poor outcomes after aRCR. 31 It therefore follows that middle aged manual laborers with symptomatic rotator cuff tears may represent a challenging population to treat.
The purpose of this study was to report short term outcomes and return to work rates after aRCR in a cohort of patients aged 50 to 60 years working in manual labor jobs. The secondary purpose was to determine if arm dominance and/or tear size affected outcomes and/or return to work. We hypothesized that aRCR would result in good functional outcomes for these patients and allow for return to work rates in excess of 80%.
Methods
This study was a retrospective analysis of prospectively collected data of manual laborers 50 to 60 years of age who underwent aRCR between January 2015 and January 2019. Institutional review board approval was obtained before beginning the study and informed consent was obtained from all participants.
Patient Population
Included were patients working manual labor jobs who were aged 50 to 60 years and underwent aRCR for a full thickness rotator cuff tear with a minimum 2 years of follow up, which was defined as complete outcome scores both pre- and postoperatively at last follow up. As a single unifying definition for manual labor has not been established, manual labor was defined as any job that requires physical strength, such as heavy lifting or prolonged heavy use of the operative shoulder.6,14,23,28,30,32 All the professions included in this study, according to the Bureau of Labor Statistics, required heavy lifting and high levels of upper body strength. 28 Degree of shoulder use was further stratified according to the Canadian Classification and Dictionary of Occupations to fully capture patient specific shoulder use within his or her profession. 5 Furthermore, all patients reported marked on the job limitations preoperatively because of limitations of their affected shoulder. All surgical procedures were performed by the senior author (N.P.) who is a shoulder and elbow fellowship–trained orthopaedic surgeon.
Excluded from this study were patients with Goutallier stage 3 or greater fatty atrophy on preoperative magnetic resonance imaging (MRI) scans, patients who had previous shoulder surgery, patients with evidence of glenohumeral degenerative joint disease and/or rotator cuff arthropathy, patients who were younger than 50 years or older than 60 years, and patients who were covered under workers’ compensation. 33 Patients who underwent concomitant labral repair were excluded, as they would require a more restrictive rehabilitation protocol. Patients older than 60 years of age were excluded because of fear that patients in this age range may have less than full motivation to return to work and could possibly introduce bias into our results. Patients with workers’ compensation were excluded to eliminate possible secondary gain as a confounder. During this study period, the senior surgeon (N.P.) surgically managed 73 patients with rotator cuff tears who worked in jobs that required regular manual labor. Sixteen patients were older than 60 years, and 3 were younger than 50 years. Two of these patients underwent concomitant capsulolabral repair. As a result, 52 patients were eligible for inclusion in this study. Four patients were unable to be contacted for follow up, leaving 48 patients available for final analysis (Figure 1).
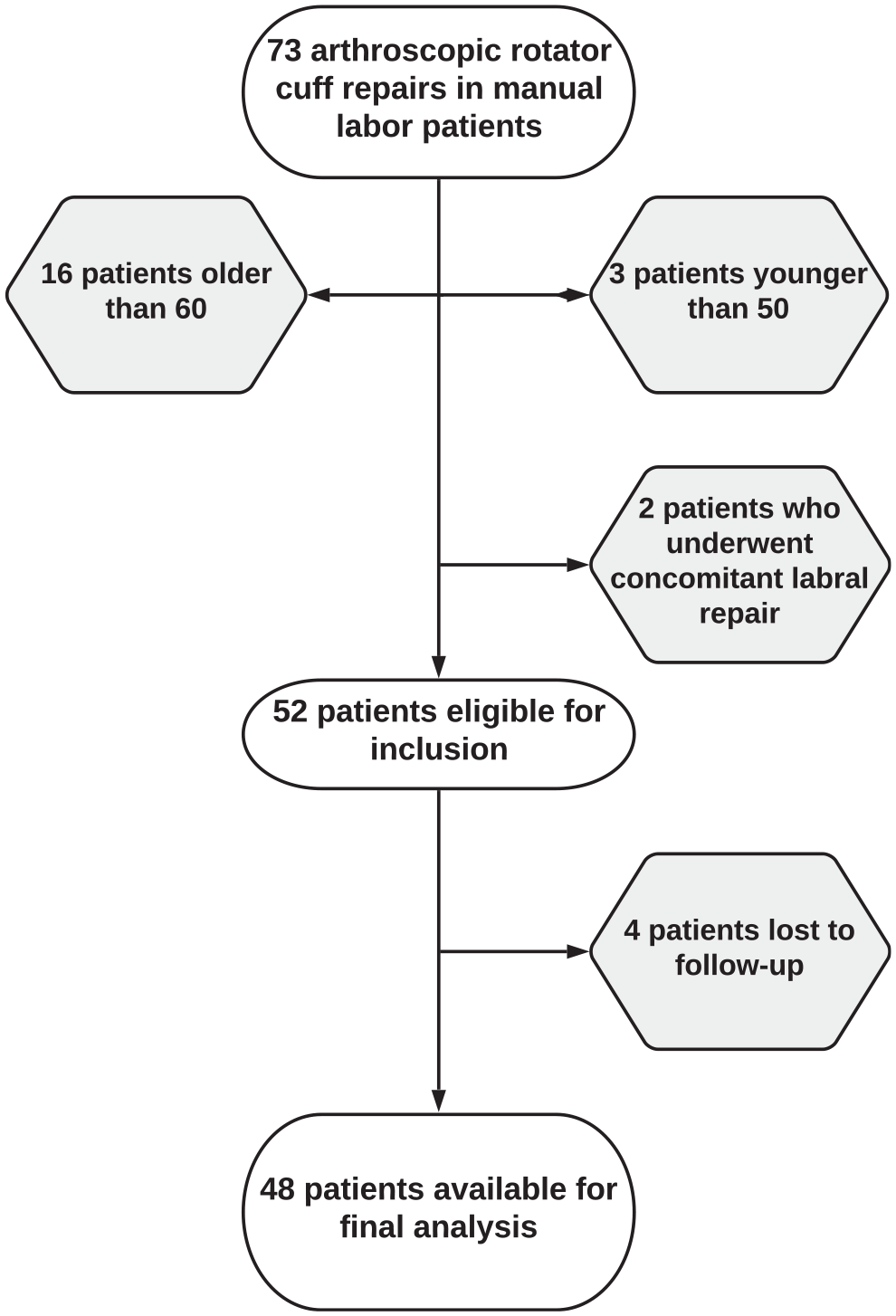
Flowchart for patient selection.
After evaluation in office, the decision was made to proceed with surgery by the senior surgeon. All patients had at least 3 months of unsuccessful nonoperative management, including nonsteroidal anti inflammatory drugs, home exercise programs, activity modification, and physical therapy. All patients had rotator cuff tears that were confirmed on preoperative MRI scans. On diagnostic arthroscopy, all patients were found to have a full thickness tear of at least 1 of the rotator cuff muscles.
Patient characteristics including age, sex, occupation, and laterality were collected. Level of manual labor was classified according to the Canadian Classification and Dictionary of Occupations guidelines. 5 Tear size was classified according to the Southern California Orthopaedic Institute Classification for full thickness tears as proposed by Snyder. 34 Pre- and postoperative evaluations with a minimum 24 months of follow up including the American Shoulder Elbow Surgeons (ASES) score; Single Assessment Numeric Evaluation (SANE); pain visual analog scale (VAS); and active range of motion in forward flexion, external rotation, and internal rotation were collected.18,20 Outcome measures are collected as part of standard of care at all patient visits. Range of motion in forward flexion and external rotation was measured using a goniometer, internal rotation was measured by determining the highest spinal level to which the patient could place the dorsum of the hand, and all measurements were provided by the treating surgeon. Complications and return to work were also recorded as part of routine postoperative follow up. Patients with profound weakness or continued pain at 4 to 6 months postoperatively underwent MRI to assess for adequacy of rotator cuff healing. Nonhealing tears were classified according to the classification system described by Sugaya et al. 35
Surgical Technique
Patients were positioned in a modified beach chair position after administration of general anesthesia and a preoperative interscalene block. A Spider hydraulic arm holder (Smith & Nephew) was then used to stabilize the operative shoulder, and the patient was draped. Examination under anesthesia was performed for all patients. Diagnostic arthroscopy was performed through a standard posterior portal. All patients underwent repair using suture anchors, with a mean of 3.5 anchors used per case. All massive (C4), large (C3), and medium (C2) tears were repaired using a double row anchor technique. Small tears (C1) were repaired via a single row anchor technique.
With regard to concomitant procedures, patients with preoperative tenderness with cross body adduction, point tenderness to the acromioclavicular (AC) joint, and radiographic and/or MRI findings consistent with AC joint pathology were treated with arthroscopic AC joint resection. Subacromial decompression was performed ubiquitously, as postoperative bursitis has been shown to have a potentially deleterious effect on patient reported outcomes. 6 Biceps tenotomy or tenodesis was performed for patients with physical examination findings consistent with biceps tendon pathology and diagnostic arthroscopic findings of biceps lesions. Patients received a description of the risks and benefits of tenodesis versus tenotomy and informed the treating surgeon of their preferred treatment modality.
Postoperative Rehabilitation
Patients were discharged home the same day of their procedure. The operative arm was immobilized in a neutral rotation position in a SmartSling (Ossur). Patients were instructed to wear the sling continuously for 6 weeks except during physical therapy. Active elbow flexion and extension were encouraged. In patients who underwent biceps tenodesis, active terminal extension was restricted for 6 weeks. Otherwise, all patients followed an identical postoperative rehabilitation protocol. At 6 weeks, the sling was discontinued, and active range of motion was permitted. Strengthening exercises were initiated 12 weeks postoperatively. Patients were allowed to return to work with restricted duty at a minimum of 2 months after surgery, with full duty allowed at a minimum of 4 months after surgery, at least 1 month after the initiation of strengthening exercises. Determination of readiness to return to work was based primarily on feedback from both the patient and his or her physical therapist. All patients attended physical therapy with the same physical therapy group.
Statistical Analysis
Statistical analysis was conducted using IBM SPSS Statistics Version 25.0 (IBM Corp). Subgroup analysis was performed to determine if differences in outcomes existed between patients who underwent surgery on their dominant shoulder and those who underwent surgery on their nondominant shoulder and to determine if patients with small/medium tears had different outcomes from those with large/massive tears. Previously published values for the Patient Acceptable Symptom State (PASS), substantial clinical benefit (SCB), and minimal clinically important difference (MCID) after aRCR were used.9,17 Continuous data were described using a combination of mean, standard deviation, range, and 95% CI. The chi square test was used to analyze categorical variables. Multiple 2 tailed Student t tests were used to compare continuous data. As multiple comparisons were made, the false discovery rate was controlled via the 2 stage step up method as described by Benjamini et al. 3 Statistical significance was set at P < .05 in all cases.
Results
A total of 48 manual laborers who underwent aRCR between January 2015 and January 2019 were included in this study (Table 1). A majority of the patients (n = 41; 85.42%) were male (Table 2). The average patient age was 55.31 ± 3.18 years. The average time to surgery from date of injury was 16.69 ± 28.30 months. The average follow up was 34.02 ± 15.02 months. There was a dominant arm predominance (56.25%), with the left and right shoulder involved equally. Tears were classified at the time of repair as massive (C4) in 9 patients (18.75%), large (C3) in 13 patients (27.08%), medium (C2) in 21 patients (43.75%), and small (C1) in 5 patients (10.42%). Forty-three patients underwent double row RCR, and 5 underwent a single row repair. The supraspinatus tendon was repaired in 44 patients (92%); the infraspinatus tendon, in 19 patients (40%); and the subscapularis, in 15 patients (31%). The concomitant procedures performed can be seen in Table 2.
Patient Labor Characteristics a
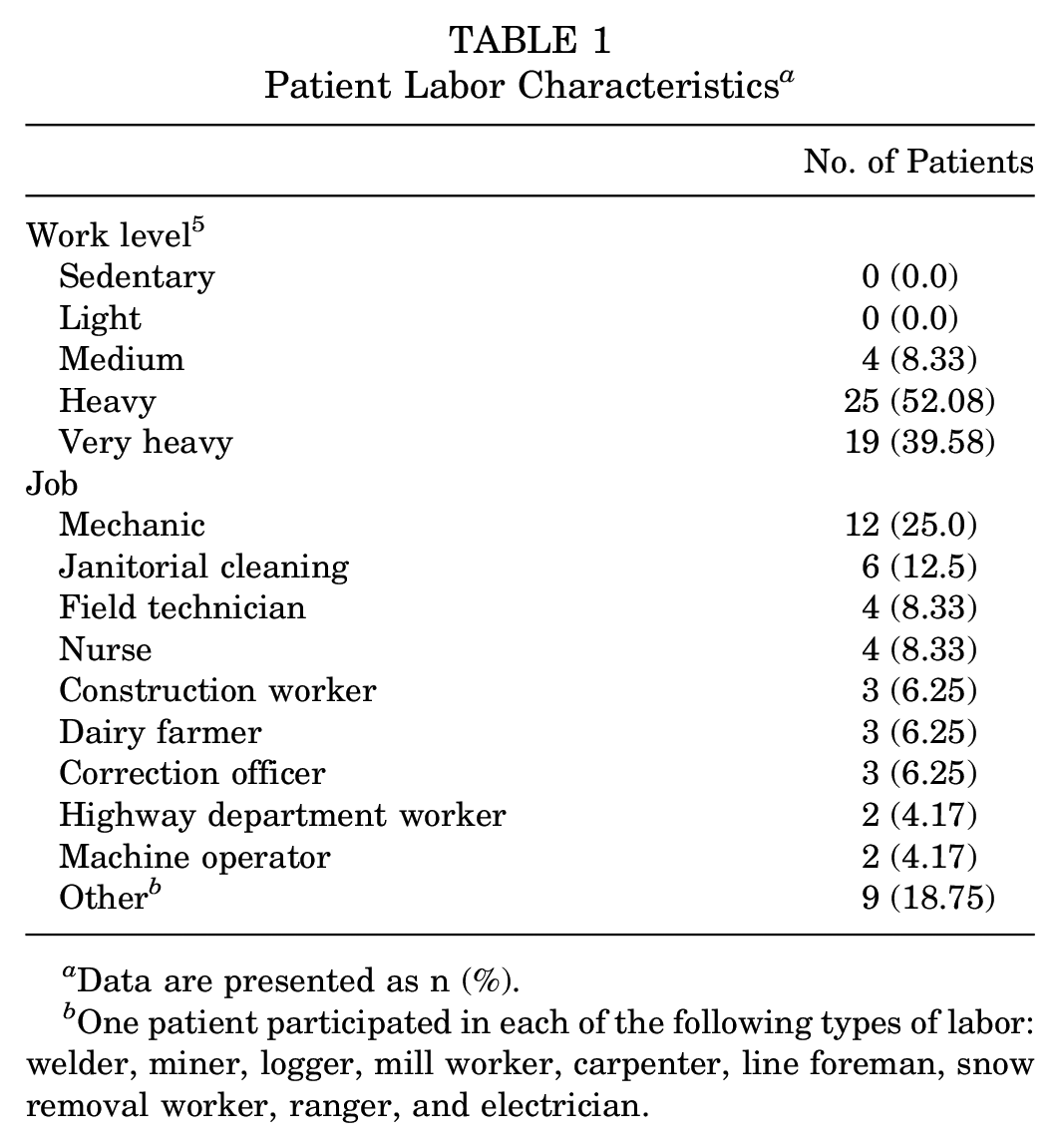
Data are presented as n (%).
One patient participated in each of the following types of labor: welder, miner, logger, mill worker, carpenter, line foreman, snow removal worker, ranger, and electrician.
Study Population Characteristics a
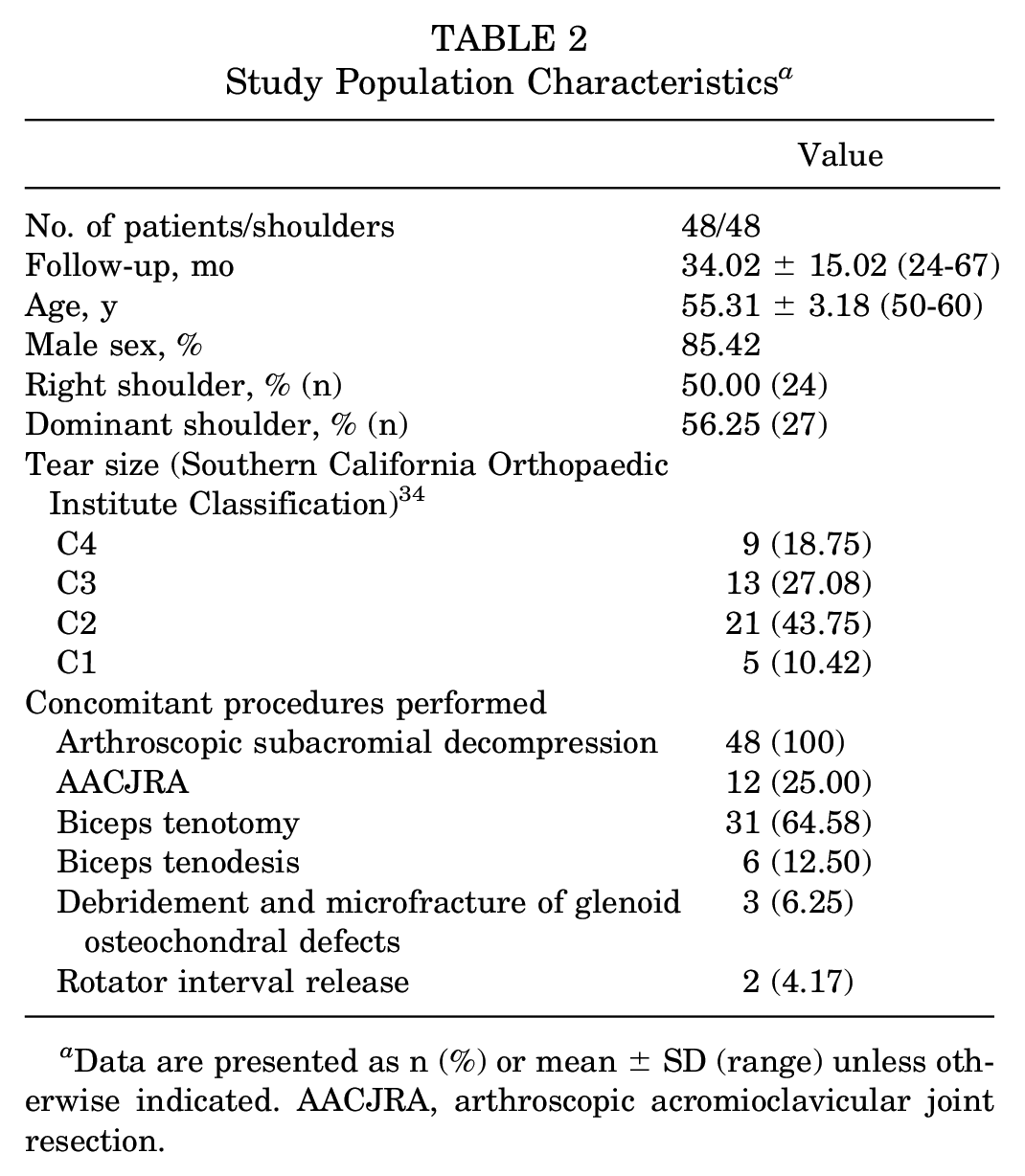
Data are presented as n (%) or mean ± SD (range) unless otherwise indicated. AACJRA, arthroscopic acromioclavicular joint resection.
Of the 48 patients, 43 (89.58%) in this study were able to return to manual labor work after aRCR. Significant improvements were noted in postoperative functional outcome scores (Table 3). After repair at the latest follow up, pain VAS improved from a mean of 8.0 ± 1.81 preoperatively to 0.46 ± 1.20 (P < .0001), SANE scores increased from 47.50 ± 18.59 to 91.88 ± 12.30 (P < .0001), and ASES scores improved from 39.58 ± 10.71 to 93.44 ± 11.97 (P < .0001). There was a statistically significant improvement in forward flexion from 154.38 ± 7.12 to 157.40 ± 4.25 (P = .0206). No statistically significant change was observed in internal or external rotation. Overall, 47 of 48 patients (97.92%) exceeded the MCID, 46 of 48 (95.83%) achieved the SCB, and 42 of 48 (87.50%) met the PASS as defined for the ASES score; 43 of 48 patients (89.58%) exceeded the MCID, 38 of 48 (79.17%) achieved the SCB, and 41 of 48 (85.42%) reached the PASS as defined for the SANE; and 47 of 48 (97.92%) reached both the MCID and the SCB for the VAS (Table 4). Arm dominance did not significantly affect functional outcome scores (VAS, ASES, or SANE) or range of motion (forward flexion, internal rotation, and external rotation). A majority of patients underwent aRCR on both their dominant arm (24/27; 88.89%) and nondominant arm (19/21; 90.48%), with no differences in return to work rates between the 2 groups (P = .8582).
Pre- and Postoperative Functional Outcome Scores a
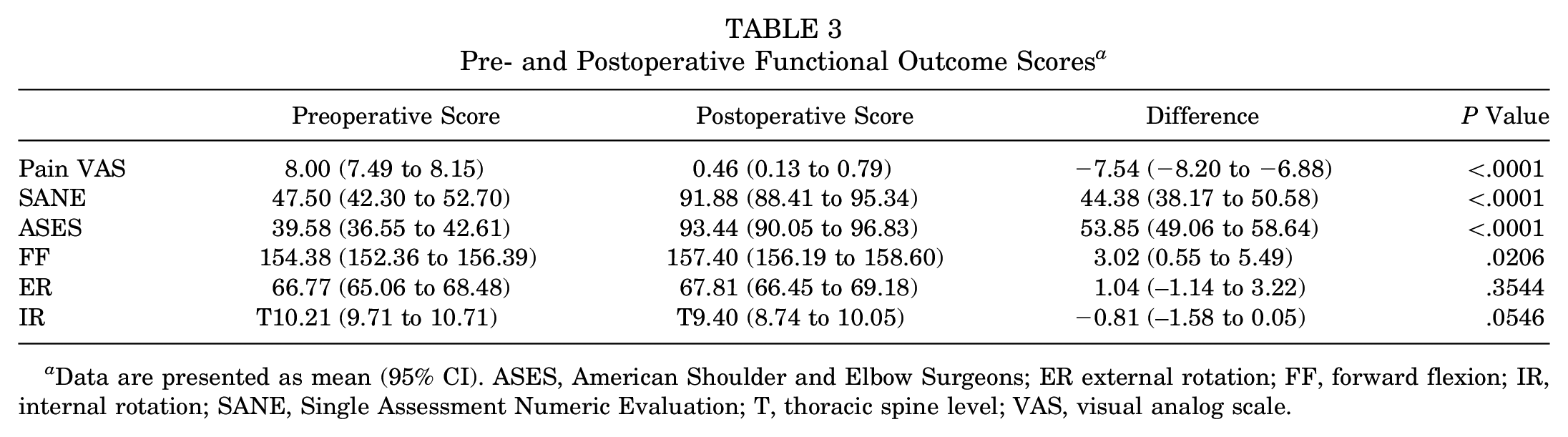
Data are presented as mean (95% CI). ASES, American Shoulder and Elbow Surgeons; ER external rotation; FF, forward flexion; IR, internal rotation; SANE, Single Assessment Numeric Evaluation; T, thoracic spine level; VAS, visual analog scale.
Percentage of Patients Meeting the MCID, SCB, and PASS a
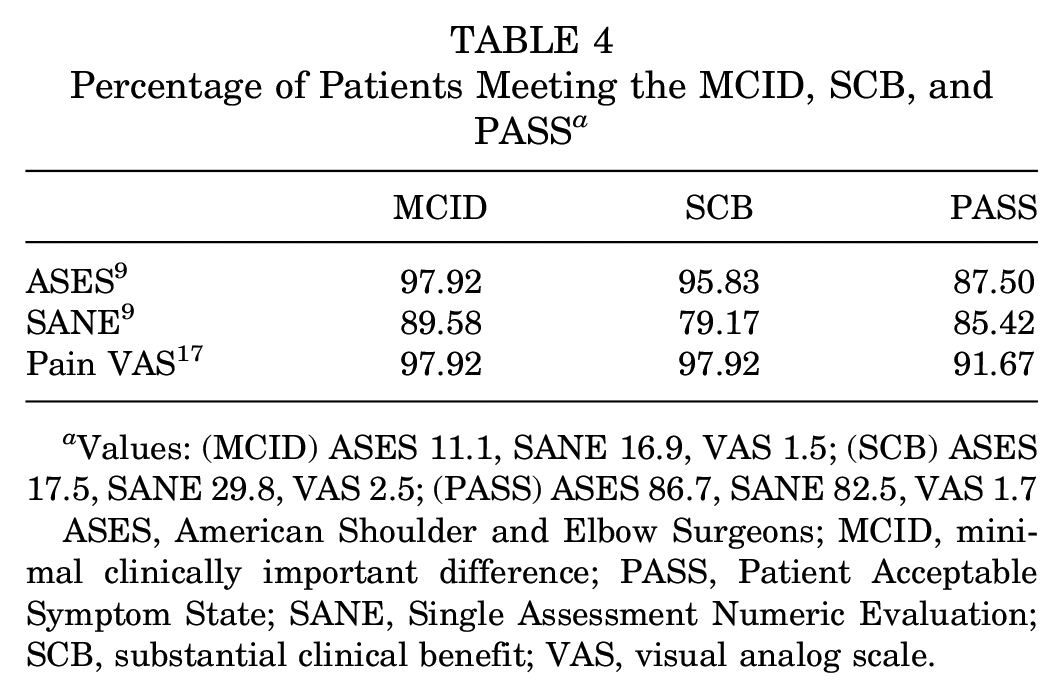
Values: (MCID) ASES 11.1, SANE 16.9, VAS 1.5; (SCB) ASES 17.5, SANE 29.8, VAS 2.5; (PASS) ASES 86.7, SANE 82.5, VAS 1.7
ASES, American Shoulder and Elbow Surgeons; MCID, minimal clinically important difference; PASS, Patient Acceptable Symptom State; SANE, Single Assessment Numeric Evaluation; SCB, substantial clinical benefit; VAS, visual analog scale.
With regard to tear size, 26 patients had Southern California Orthopaedic Institute C1 or C2 tears, and 22 had C3 or C4 tears (Table 5). Preoperative pain, ASES, and SANE scores and range of motion did not vary between patients with smaller tears and those with larger tears. At the final follow up, however, patients with smaller tears had statistically significantly lower pain VAS and higher ASES scores. These differences did not exceed the MCID for the pain VAS and ASES scores, respectively. Furthermore, time to return to both restricted and unrestricted work did not vary significantly between patients with smaller tears and those with larger tears (P = .4978 and .4689, respectively).
Comparison of Outcome Measures Between Tear Sizes a
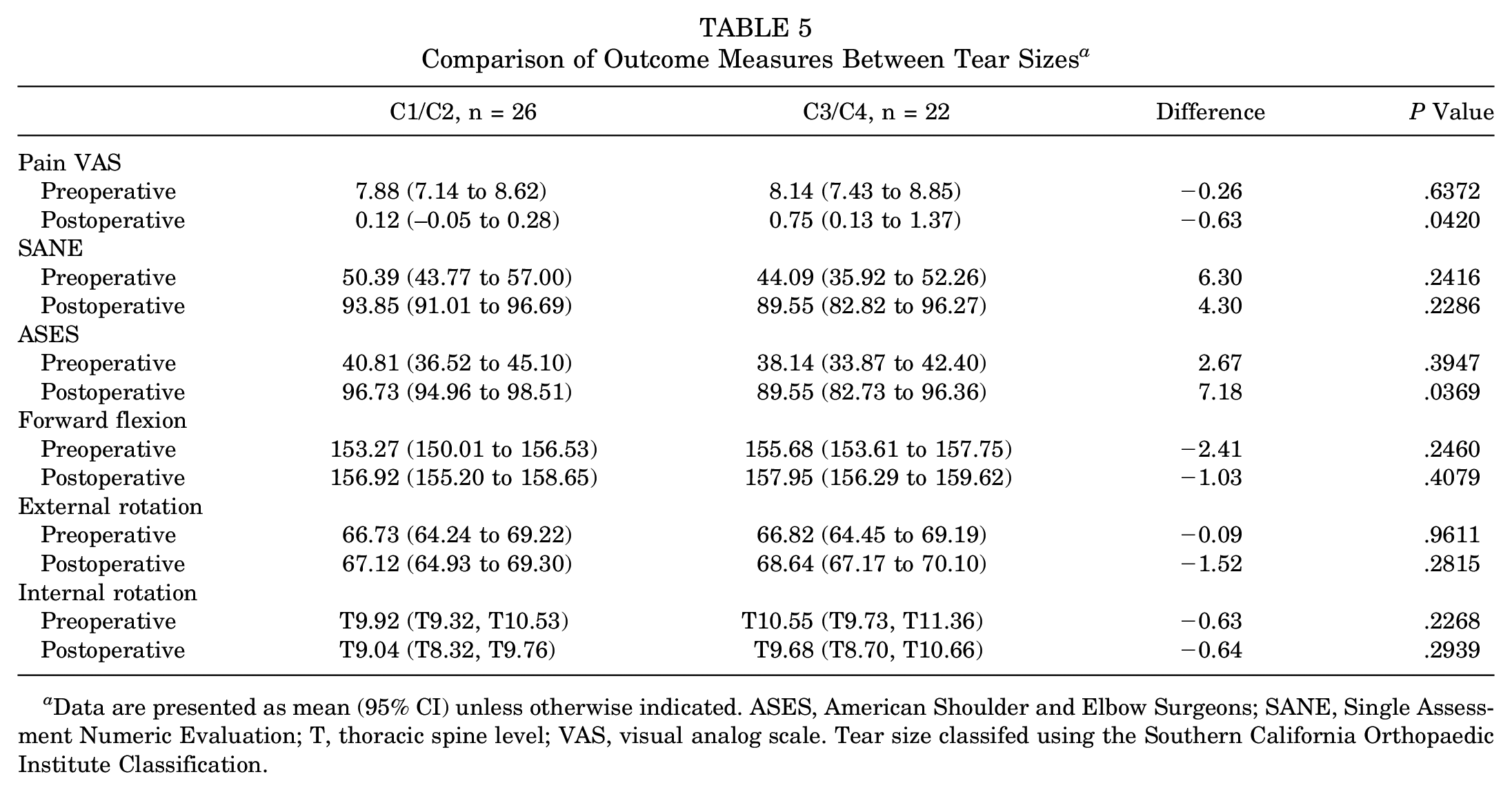
Data are presented as mean (95% CI) unless otherwise indicated. ASES, American Shoulder and Elbow Surgeons; SANE, Single Assessment Numeric Evaluation; T, thoracic spine level; VAS, visual analog scale. Tear size classifed using the Southern California Orthopaedic Institute Classification.
A majority (43/48; 89.58%) of patients were able to return to unrestricted work. Of the 5 patients who could not return to work, 4 (2 mechanics, 1 corrections officer, and 1 carpenter) had pain and weakness, and 1 patient (mechanic) had pain without weakness that required permanent job modifications. The average time to return to restricted duty was 3 ± 0.95 months (range, 2.0-6 months) after surgery. Return to full, unrestricted duty occurred at, on average, 5.05 ± 1.26 months (range, 4-10 months) after surgery (Table 6).
Time to Return to Work a
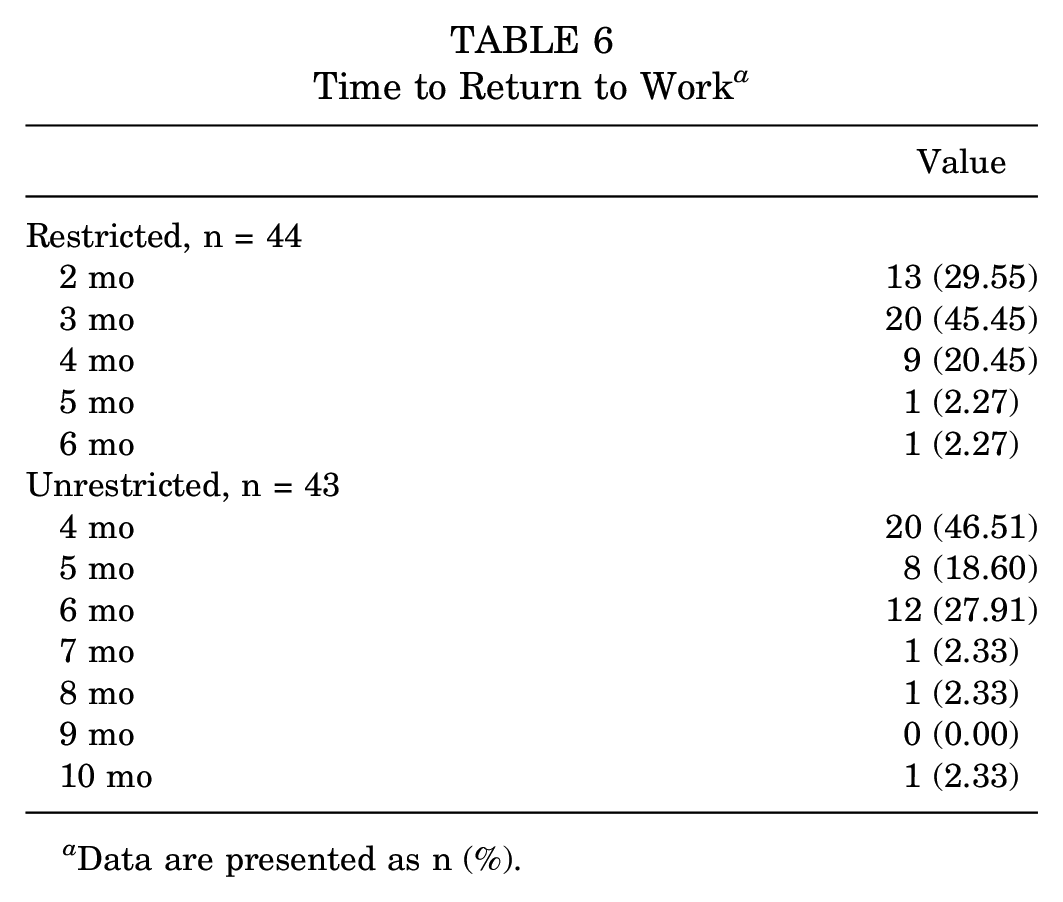
Data are presented as n (%).
Regarding complications, 3 patients (6.25%) had nonhealing repairs. Of these 3 patients, 1 patient had a deep postoperative infection, 1 patient sustained a trauma during the recovery period, and 1 patient had persistent pain and weakness. All 3 patients were unable to return to work (Table 7). One additional patient developed a lower extremity deep vein thrombosis in the acute postoperative period. Altogether, 4 patients (8.33%) reported postoperative complications.
Structural Integrity of Nonhealing Tears (n = 3) a
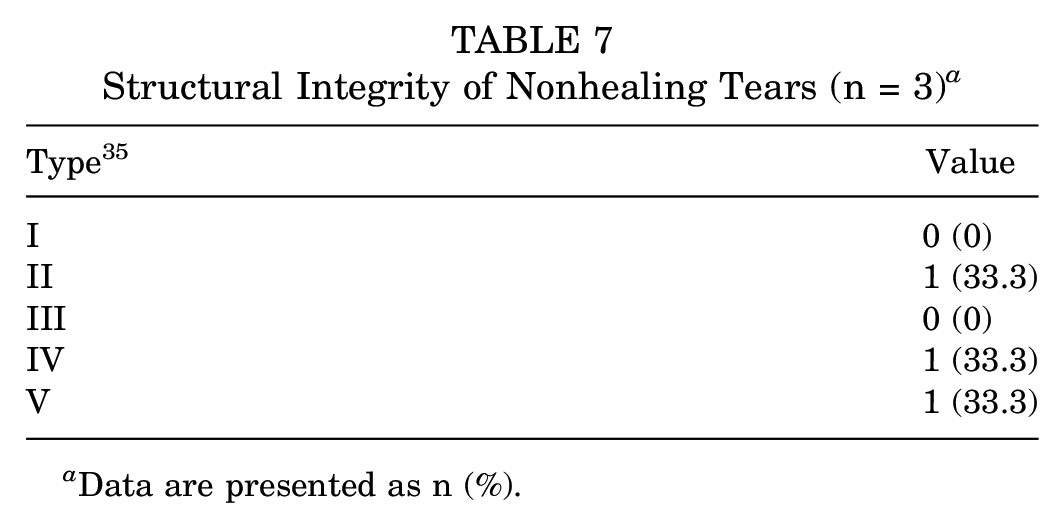
Data are presented as n (%).
Discussion
The results of this study support our hypothesis. aRCR was found to produce good functional outcomes and allowed for a high rate of return to work postoperatively. At the latest follow up, 89.58% of patients were able to maintain manual labor positions and had returned to preinjury levels of work. Only 8.33% of patients reported postoperative complications.
Manual laborers comprise a significant sector of the US workforce. According to a 2017 US Bureau of Labor Statistics report, nearly half of all jobs require medium physical strength, and 16.9% of jobs require heavy or very heavy strength. 29 Additionally, recent Current Population Survey results demonstrated that the average age of many manual labor industries is rising. In 2020, close to 25% of the construction workforce was over the age of 55 years. 19 Manual labor workers have been shown to be at increased risk for upper limb disorders, including rotator cuff pathology, which not only affects the individual patient but also places an enormous burden on society as a whole.12,23,32 An analysis by Mather et al 22 found that rotator cuff repair lessens this burden, with surgical interventions estimated to generate lifetime societal savings of $3.4 billion. Additionally, their findings suggest that while these procedures are cost effective and increase quality adjusted life-years for individuals of all age groups, patients younger than 60 years of age experience a net cost savings from surgical repair. Successful surgical repair of rotator cuff tears in this patient population enables an important sector of the workforce to remain economically productive, lightening individual financial burden associated with injury and providing societal economic benefit. In light of the aging workforce and increased risk of rotator cuff pathology in these workers, it is likely that the number of manual laborers undergoing aRCR will continue to grow. Despite this, the literature regarding outcomes and return to work in this important patient population remains wholly inconclusive.
Multiple studies have postulated that heavy physical labor is associated with lower rates of return to work after aRCR.6,12,25 On the other hand, Bhatia et al 4 found that 88.5% of manual laborers were able to return to work by 7.6 months postoperatively. This was echoed by Gowd et al, 14 who demonstrated that 63.3% of manual laborers were able to return to work after aRCR and that patients who achieved the PASS for patient reported outcomes demonstrated higher levels of return to work. The authors went on to highlight that patients with dominant arm involvement had lower levels of return to work. Haunschild et al 15 found that while a majority of the patients in their study were able to return to work by 8 months postoperatively, >35% were unable to return to their previous level of activity. These findings are consistent with the work of Aagaard et al, 1 who found that 1 in 5 patients require permanent job modifications upon return to work after aRCR. In addition to physically strenuous work, older age and workers’ compensation status increase the likelihood of unsatisfactory outcomes after aRCR.4,6,27,30 Attempts to summarize these findings prove difficult, as it is difficult to accurately capture what truly drives poor outcomes. Is it the poor tissue quality secondary to advanced patient age, high rotator cuff demand upon return to work, secondary gain because of a workers’ compensation claim, or some combination thereof?
In light of these findings, it would be reasonable to predict that our cohort of 50- to 60-year-old manual laborers may represent a challenging population to treat. However, our analysis yielded promising results, with nearly all patients returning to preinjury levels of work and an overwhelming majority of patients demonstrating statistically and clinically significant improvement in outcome scores. We believe that there are a few key characteristics of our cohort that drive these favorable outcomes. First, our cohort comprised entirely patients without workers’ compensation, which we believe lessens the potential for secondary gain to be the primary reason for nonreturn to work.7,16 Second, a majority of our patients met or exceeded the PASS for the ASES, SANE, and pain VAS scores. 14 Interestingly, of the 5 patients who did not return to work, 4 (80%) of them did not meet the PASS for at least 2 of 3 outcome scores. While we do not obtain routine postoperative MRI scans, only 3 patients had postoperative subjective shoulder symptoms severe enough to warrant advanced imaging. These findings suggest that aRCR is a viable treatment option for manual laborers desiring to return to physical strenuous activities and should be considered for the management of symptomatic rotator cuff injuries in this population.
Our study was not without its limitations. This study excluded patients with workers’ compensation, as including them in our analysis could potentially have introduced additional confounding variables.8,16 Additionally, this study was a case series and, therefore, included no control group to account for differences in type of manual labor performed by our patients. Furthermore, no consensus definition exists for what is considered manual labor. Last, our analysis included only individuals aged 50 to 60 years and was composed of a primarily male cohort (85.42%), potentially limiting the generalizability of these results to larger populations.
Conclusion
Rotator cuff tears represent a significant cause of shoulder pain and disability in the United States. Our results demonstrated favorable outcomes after arthroscopic repair of rotator cuff tears in a cohort of manual laborers 50 to 60 years of age at midterm follow up, with 89.58% of patients successfully returning to work postoperatively. These findings suggest that aRCR is an appropriate treatment option for the management of rotator cuff tears in patients who desire to return to physically strenuous jobs.
Footnotes
Submitted October 11, 2021; accepted February 24, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.C.D. has received hospitality payments from Styker. N.P. has received consulting payments from Mitek. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.