
Abstract
Background:
Questions remain about whether circumferential labral reconstruction (CLR) using an iliotibial band (ITB) allograft can effectively restore the labral suction seal of the hip.
Hypotheses:
(1) CLR with an ITB allograft >6.5 mm would restore distractive stability force to that of the intact labrum. (2) CLR with an ITB allograft >6.5 mm would achieve significantly superior distractive stability force compared with CLR with an ITB allograft <6.5 mm.
Study Design:
Controlled laboratory study.
Methods:
A total of 6 fresh-frozen pelves with attached femurs (n = 12 matched hemipelves) from male donors were procured and dissected free of all soft tissue, including the hip capsule but preserving the native labrum, transverse acetabular ligament, and ligamentum teres. Potted hemipelves were placed in a saline bath and securely fixed to the frame of a hydraulic testing system. A 500-N compressive load was applied, followed by femoral distraction at a rate of 5.0 mm/s until the suction seal ruptured. Force and femoral displacement were continually recorded. Force versus displacement curves were plotted, the maximum force was recorded, and the amount of femoral distraction to rupture the suction seal was determined. After intact testing, the labrum was excised, and specimens were retested using the same protocol. CLR was subsequently performed twice in a randomized fashion using (1) an ITB allograft with a width >6.5 mm (7.5-9.0 mm) and (2) an ITB allograft with a width <6.5 mm (4.5-6.0 mm). Specimens were retested after each CLR procedure. Force (in Newtons) and femoral distraction (in millimeters) required to rupture the suction seal were measured and compared between the 4 testing states (intact, deficient, CLR <6.5 mm, and CLR >6.5 mm) using repeated-measures analysis of variance.
Results:
On average, intact specimens required 148.4 ± 33.1 N of force to rupture the hip suction seal, which significantly decreased to 44.3 N in the deficient state (P < .001). CLR with ITB allografts <6.5 mm did not improve the maximum force (63 ± 62 N) from the deficient state (P = .42) and remained significantly lower than the intact state (P < .01). CLR with ITB allografts >6.5 mm recorded significantly greater force to rupture the suction seal (135.8 ± 44.6 N) compared with both the deficient and CLR <6.5 mm states (P < .01), with a mean force comparable with the intact labrum (P = .59). The amount of femoral distraction to rupture the suction seal demonstrated similar findings.
Conclusion:
In a cadaveric model, CLR using ITB allografts >6.5 mm restored the distractive force and distance to the suction seal rupture to values comparable with hips with an intact labrum. CLR using ITB allografts >6.5 mm outperformed CLR with ITB allografts <6.5 mm, demonstrated by a significantly higher force to rupture the suction seal and increased distraction before the rupture.
Clinical Relevance:
The results of this cadaveric investigation suggest that using wider labral allografts during CLR will provide the distractive force required to rupture the suction seal and immediate postoperative stability of the hip, although further studies are required to determine if these results translate to improved clinical outcomes.
Keywords
The function and importance of the acetabular labrum as the sealing mechanism of the hip have previously been determined. 9 A labral tear is one of the most common findings in hip-preservation surgery 3 and is often associated with femoroacetabular impingement syndrome. Furthermore, the restoration of labral anatomy and function are key factors to improve patient-reported outcomes after hip arthroscopic surgery in the context of femoroacetabular impingement syndrome.14,22
Labral repair is the current standard when addressing labral tears, particularly in the primary setting.5,16,20 However, acetabular labral reconstruction has risen as an alternative to labral excision or resection when repair is not an option because of labral tissue deficiency.1,21,26,35 The ultimate goal of both, labral repair and reconstruction, is to restore the labral sealing mechanism of the hip. Labral reconstruction is a well-described procedure used to restore labral function when facing an irreparable labral tear. 18 Compared with labral debridement, superior patient-reported outcomes have been reported with labral reconstruction.6,14,19 Overall, 2 options for labral reconstruction have been described: segmental labral reconstruction (SLR) and circumferential labral reconstruction (CLR).1,21 Specifically for the CLR option, good results have been reported at short-term follow-up in the primary and revision settings.7,8,28,29,34
In a human cadaveric model, labral repair reportedly outperforms SLR in preserving the hip suction seal. 4 Nonetheless, SLR was able to partially restore time-zero acetabular contact areas and pressures compared with segmental labral resection.15,23 In a cadaveric study of CLR, Suppauksorn et al 31 reported loss of the suction seal when using an iliotibial band (ITB) allograft with an average width of 5 mm. However, Storaci et al 30 recently reported that native labra that were <6 mm in height had a significantly weaker suction seal compared with native labra that were >6 mm. These findings suggest that a reconstructed labrum may have better suction seal biomechanics if the graft width is >6 mm, although there are currently no specific guidelines on the optimal graft size when performing CLR.
The purposes of the present study were (1) to evaluate the role of CLR using an ITB allograft in restoring distractive force and distance to the suction seal rupture of the hip and (2) to evaluate whether graft width affects the ability to restore distractive stability of the hip after CLR. It was hypothesized that (1) CLR with an ITB allograft >6.5 mm would restore distractive stability force to that of the intact labrum and (2) CLR with an ITB allograft >6.5 mm would achieve significantly superior distractive stability force compared with CLR with an ITB allograft <6.5 mm.
Methods
Institutional review board approval was not required for this laboratory investigation utilizing de-identified cadaveric specimens. A total of 12 matched pairs of hemipelves (12 hips) with attached femurs from male donors were obtained from an institute-approved tissue bank with a mean age of 54.4 ± 15.5 years (range, 37-68 years) and a mean body mass index of 22.0 ± 5.0 (range, 14.4-28.2). All specimens were screened radiographically by 2 orthopaedic surgeons (D.R.M. and M.B.B.) before shipment to ensure that there was no evidence of previous surgery, injuries, advanced osteoarthritis (Tönnis grade >1), acetabular dysplasia (lateral center-edge angle <25°), or acetabular overcoverage (lateral center-edge angle >40°). Upon arrival, specimens were stored at −30°C and thawed at room temperature for 48 hours before testing.
Specimen Preparation
The surrounding soft tissue, including the hip capsule, was removed from each specimen, taking care to avoid damage to the native labrum, transverse acetabular ligament (TAL), and ligamentum teres. In an open fashion, the labrum and ligamentum teres were assessed, and any specimen with evidence of a calcified labrum, labral tear, or complete ligamentum teres tear was excluded from the study. Following these criteria, all specimens were included in the data analysis. The femur was cut 6 cm from the inferior aspect of the lesser trochanter, and the hip joint was oriented in a neutral position as defined by Fagotti et al. 10 Briefly, a neutral position was obtained by placing the pelvis on a table in the supine position with the tip of the sacrum and the pubic symphysis aligned in the sagittal plane. Next, pelvic tilt was established by alignment of the anterior superior iliac spine with the posterior superior iliac spine from a lateral standpoint. Neutral rotation of the femur was obtained by drilling a K-wire through the linea aspera at the midline of the femoral shaft to the lesser trochanter. 10
A quarter-inch by 4-inch lag screw was inserted into the femoral head in line with the femoral neck and was potted in a cylindrical aluminum pot with a 2-part epoxy resin (Smooth-Cast 300; Smooth-On). Excess bone was removed from the pelvis to allow potting of the acetabulum, which was further secured via carefully placed wood screws. The femur was held in 10° of abduction and 15° of flexion with a K-wire pin that passed through the femur and pelvis to ensure that the hip was properly positioned when placed onto the testing system. 30
Surgical Technique
ITB Allograft Preparation
There were 2 sizes of ITB allografts (AlloSource) that were created with a final width of either >6.5 mm or <6.5 mm. The use of a 6.5-mm cutoff was based on recent findings reported by Storaci et al. 30 Once thawed, the grafts were folded into thirds and tubularized using multiple No. 2-0 absorbable sutures (Vicryl; Ethicon). 28 To allow control of the allograft when reconstructing, 3 Krackow stitches were placed at both ends of the graft using No. 2-0 nonabsorbable sutures (FiberWire; Arthrex). 17 After the allografts were prepared, the final diameter was measured using a graft sizing block with 4.5- to 12-mm holes in 0.5-mm increments. Allograft preparation was performed by 1 orthopaedic surgeon (D.R.M), and each allograft size was verified by 2 orthopaedic surgeons (D.R.M. and S.K.).
Circumferential Labral Reconstruction
Before CLR, the most anterior and posterior points of the TAL were identified and marked using a surgical pen, and the native acetabular labral height was measured at the 9-o’clock position. 30 Afterward, the native labrum was entirely excised using the anterior and posterior marked references of the TAL. Before allograft fixation, drill holes were placed from the most anteromedial aspect to the most posterolateral aspect of the acetabular rim, approximately 7 to 10 mm apart (Figure 1A). Meticulous care was taken to place the most anterior and posterior anchors as close as possible to the anterior and posterior points of the TAL, respectively. Furthermore, all drill holes were placed as near as possible to the inferior border of the acetabular rim without violating the chondral surface. ITB allograft fixation was executed in the same order of drilling using a 2.4×12-mm knotless anchor with No. 1 ultra-high molecular weight polyethylene sutures (CinchLock SS; Stryker). Between 9 and 11 anchors were used per CLR procedure (Figure 1B). The drill bit used was 2.4×17 mm, and new drills were used for each CLR procedure.
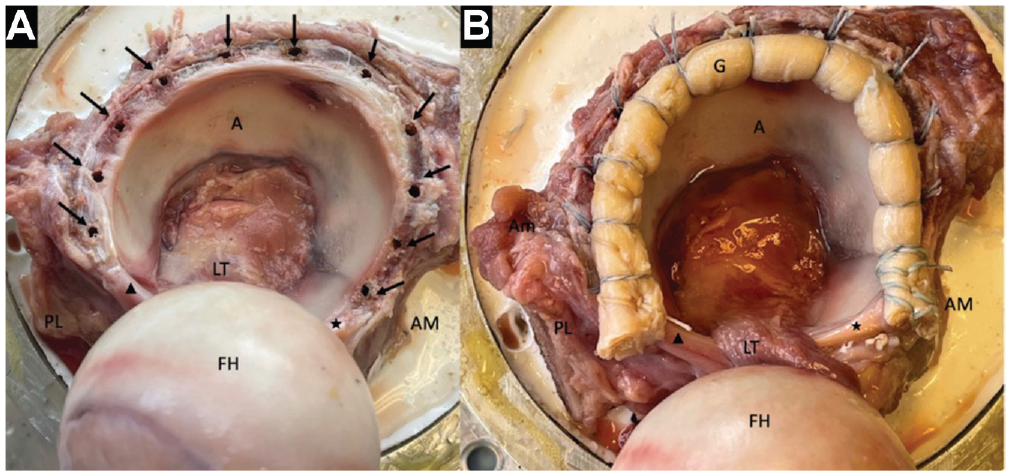
(A) A right hip. The most anteromedial (AM) and posterolateral (PL) aspects of the acetabulum (A) and the most AM (★) and PL (▲) points of the transverse acetabular ligament were marked. The native labrum was excised, and anchor drill holes (black arrows) were made. (B) The same right hip after performing circumferential labral reconstruction using an iliotibial band allograft (G). There were eleven 2.4-mm CinchLock SS PEEK knotless anchors with No. 1 ultra-high molecular weight polyethylene sutures used. FH, femoral head; LT, ligamentum teres.
All hips underwent 2 CLR procedures (>6.5 mm and <6.5 mm) in random order using the same pilot holes and the same number of anchors for both CLR procedures (Figure 2). Randomization was conducted with Excel (Microsoft) using the random number generator function. Anchors were not reused. All CLR procedures were performed by a single hip preservation fellowship–trained orthopaedic surgeon (D.R.M.).
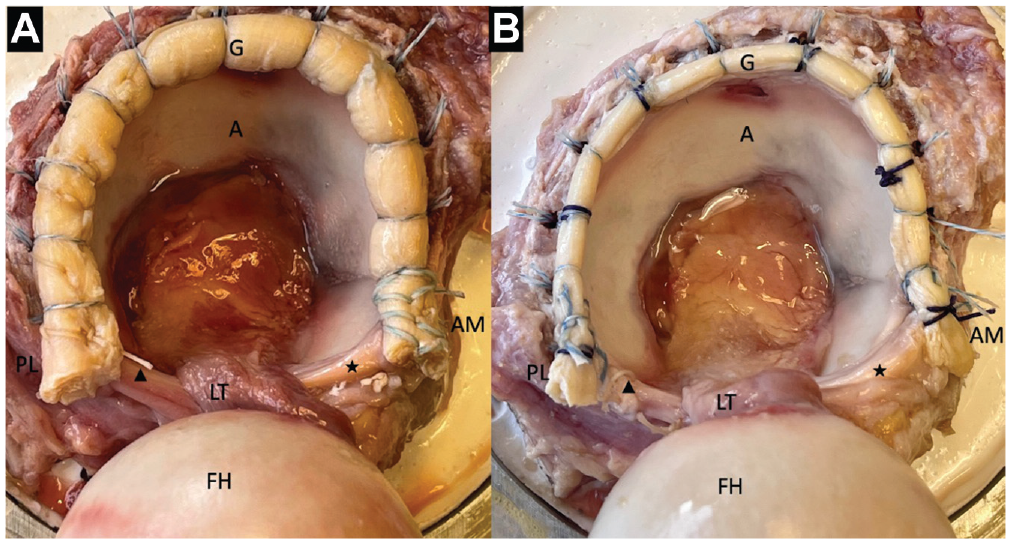
The same right hip. (A) Circumferential labral reconstruction (CLR) using an 8-mm iliotibial band (ITB) allograft (G). (B) CLR using a 5-mm ITB allograft (G). The most anteromedial (AM) and posterolateral (PL) aspects of the acetabulum (A), the most AM (★) and PL (▲) points of the transverse acetabular ligament, and the femoral head (FH) and ligamentum teres (LT) are marked.
Biomechanical Testing
Distractive force and distance to the suction seal rupture of the hip were repeatedly tested in 4 different states: (1) intact labrum, (2) deficient labrum, (3) CLR with 1 graft size (wide [>6.5 mm] or narrow [<6.5 mm]), and (4) CLR with the other graft size (narrow or wide). The order for the CLR was assigned randomly using the random number generator.
To prepare for testing, the acetabular pot was secured in an acrylic tank fixed to the frame of the hydraulic mechanical testing system (Bionix 370.02 actuator; MTS Systems). The femoral pot was fastened to the actuator, and the positional K-wire was removed (Figure 3A). Once secured, the tank was filled with phosphate-buffered saline solution heated to 37°C (Figure 3B).
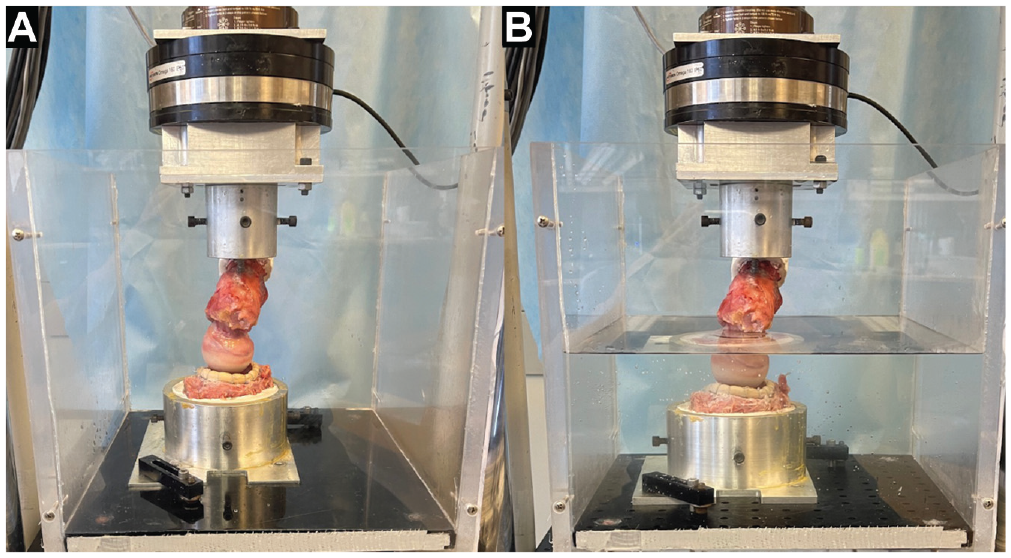
(A) A right hip was secured to the hydraulic mechanical testing system after circumferential labral reconstruction. (B) The tank was filled with phosphate-buffered saline solution heated to 37°C.
A 20-N compressive load was applied between the femoral head and the acetabulum, and the femoral position was recorded as neutral. 30 Once neutral was defined, the compressive load was increased to 500 N at a rate of 50 N/s and held for 15 seconds. The femoral head was then distracted via displacement control at a rate of 5.0 mm/s until the hip suction seal was ruptured, indicated by a significant (>20%) drop in loading, while force and femoral displacement were continually recorded. Force versus displacement curves were plotted, the maximum force was recorded, and the amount of femoral distraction to rupture the suction seal was determined using Python programming software, with a suction seal rupture defined as the inflection point in the graft at which force began to significantly decrease (Figure 4). The saline solution was replaced before each testing state. Each specimen was repeatedly tested 4 times for each state, and the values recorded during the final 3 tests were averaged and used for statistical analysis. The first test was used as preconditioning for the saline solution to fully enter the hip joint, ensuring consistent testing conditions for the 3 subsequent tests.
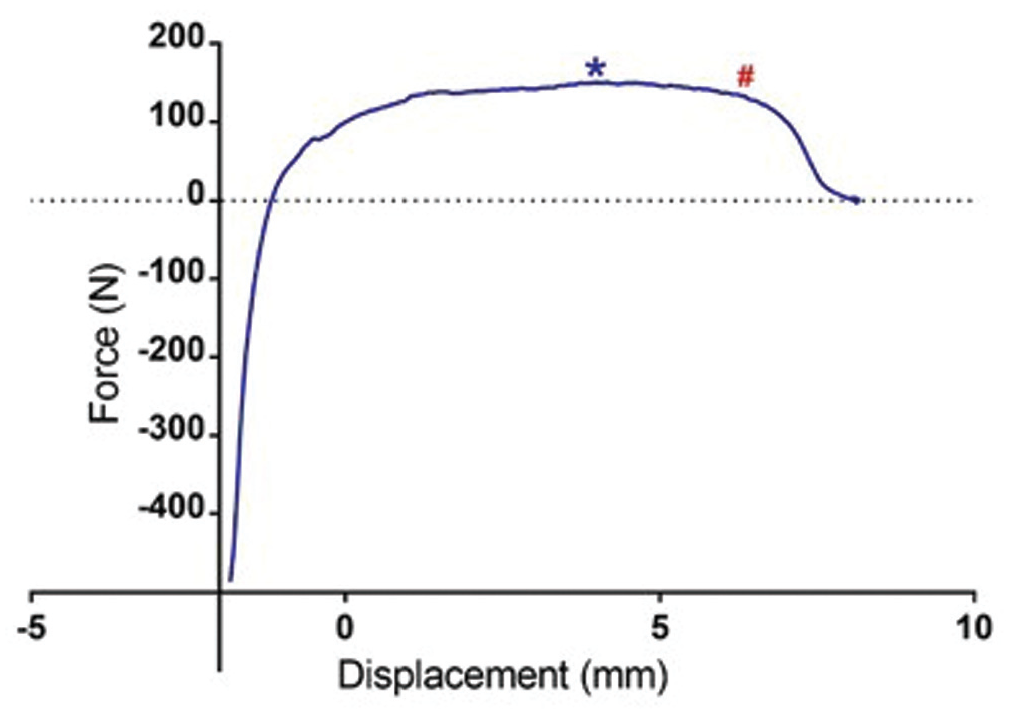
Force versus displacement curve for a hip specimen after circumferential labral reconstruction with an 8-mm allograft, with maximum force (*) and the inflection point where the suction seal ruptured (#).
Statistical Analysis
A total of 12 hips were chosen based on a power analysis using the mean and standard deviation of femoral distraction to achieve a suction seal rupture in large and small intact labra reported by Storaci et al, 30 which suggested that a minimum of 8 specimens would be required to achieve a power of 0.80 (α = .05). Statistical analysis was performed using Prism statistical software (Version 7.04; GraphPad Software). After the verification of normally distributed data, a repeated-measures model was used to compare the maximum distraction force and distance with the suction seal rupture for each hip condition (intact, deficient, CLR >6.5 mm, and CLR <6.5 mm). Pearson correlation coefficients were calculated to determine the relationship between labrum height (intact and graft size), donor demographics, distraction distance to the suction seal rupture, and maximum distraction force. The Tukey-Kramer test was used to adjust for multiple comparisons with P < .05 as the significance criterion. All data are presented as mean ± standard deviation.
Results
On average, the height of intact native labra measured 5.89 ± 1.53 mm (range, 3.40-8.50 mm) and was not significantly correlated with the donor’s weight, height, or age at the time of death. The mean maximum distraction force recorded when testing intact labra was 148.4 ± 33.1 N (Figure 5A). All 12 specimens displayed a measurable suction seal, which ruptured at a mean distance of 4.9 ± 1.6 mm (range, 2.6-6.8 mm) (Figure 5B). In the intact state, maximum force was not significantly correlated with distance to the suction seal rupture (R2 = 0.28; P = .07), and neither maximum force nor rupture distance was significantly correlated with the native labral height (R2 = 0.13 [P = .24] and R2 = 0.05 [P = .49], respectively).
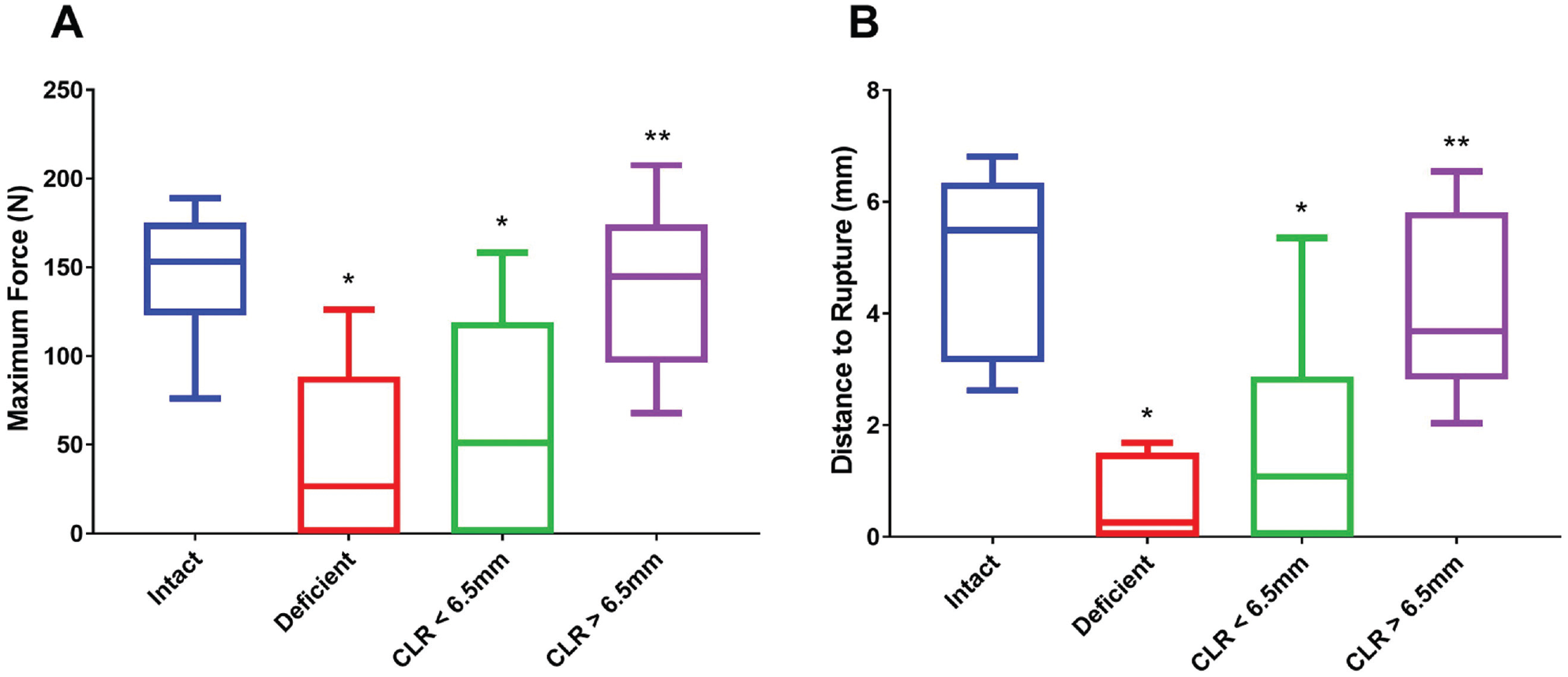
The (A) maximum force and (B) distance to the suction seal rupture of the hip were significantly lower in hips that were labrum deficient and underwent circumferential labral reconstruction (CLR) with a narrow allograft (<6.5 mm) compared with hips with an intact labrum (*P > .01). CLR with a wide allograft (>6.5 mm) significantly improved the maximum force and distance to the rupture from the deficient state (**P > .01).
Removal of the native labrum (deficient state) resulted in a significant decrease in maximum force and distance to the suction seal rupture of 44.3 ± 50.3 N (range, 0.0-126.0 N) and 0.6 ± 0.7 mm, respectively (Figure 5). Half of the specimens tested (n = 6) had no measurable suction seal once the labrum was removed. Overall, 5 of the 6 specimens with a measurable suction seal reached a maximum force that was ≥50% of the intact value.
CLR with ITB allografts with a width <6.5 mm (n = 9 were 4.5 mm, n = 2 were 5 mm, and n = 1 was 6 mm) did not significantly increase the mean maximum force (63 ± 62 N; P = .42) or distance to the suction seal rupture (1.7 ± 1.9 mm; P = .07) from that of the deficient state (Figure 5). Of the 6 specimens with no suction seal, 4 in the deficient state also had no measurable suction seal after CLR with narrow ITB allografts. In addition, the maximum force and distance to the rupture recorded for CLR with narrow grafts remained significantly lower than those recorded for the native intact labrum (P < .01) (Figure 5).
When CLR was performed using ITB allografts with a width >6.5 mm (n = 2 were 9 mm, n = 9 were 8 mm, and n = 1 was 7.5 mm), the mean maximum force was 135.8 ± 44.6 N, and the mean distance to the suction seal rupture was 4.1 ± 1.6 mm. Both measurements were significantly greater than those recorded in labrum-deficient hips (P < .01) and were not significantly different from the maximum force and rupture distance recorded in hips with an intact native labrum (P = .59). CLR with wide allografts also had a significantly greater maximum force and distance to the rupture compared with CLR with narrow allografts (P < .01) (Figure 5).
Discussion
Key findings of the present study were that CLR performed with a wider ITB allograft (>6.5 mm) restored distractive force and distance to the suction seal rupture from the deficient state to levels comparable with the native intact labrum. Further, wider allografts outperformed narrow (<6.5 mm) allografts, providing significantly superior distractive stability. Comparatively, CLR with narrow ITB allografts remained similar to the labrum-deficient state.
Under loading, the labrum provides a suction seal of the hip that effectively prevents the efflux of synovial fluid from the central compartment, protecting the articular cartilage by preserving chondrocyte nutrition via diffusion while decreasing contact stresses via hydrostatic fluid distribution.11,12 Biomechanical studies of labral reconstruction have primarily focused on SLR. Cadet et al 4 reported that SLR using ipsilateral ITB autografts did not effectively prevent fluid efflux compared with the intact labrum. Furthermore, they demonstrated that SLR had high fluid permeation, similar to the partially resected condition. However, these authors did not report graft width or specifics on the SLR technique used.
In a biomechanical study on native labral height, Storaci et al 30 reported that specimens with a labrum <6 mm in height had significantly reduced peak negative pressure and therefore a weaker suction seal compared with specimens with a native labrum >6 mm. The mean labral native height reported by these authors was 6.48 mm. Although the ideal width of labral reconstruction remains to be determined, Storaci et al proposed that a reconstructed labrum may have better suction seal biomechanics if its width is >6 mm.
The present study corroborates previous research that suggests that labral resection significantly alters the hip suction seal and can be effectively restored via reconstruction. 4 Philippon et al 25 reported that partial and complete labral resection resulted in a 47% and 76% decrease in fluid pressurization, respectively, compared with the intact labrum. Furthermore, SLR improved fluid pressurization by 56%, which was significantly higher than the partially resected labrum and similar to that of the intact labrum. The graft width selected for their SLR was between 6 and 7 mm. Nepple et al 23 concluded that the acetabular labrum is a primary hip stabilizer against distraction forces at small displacement values and that partially resecting the labrum decreases the distractive strength of the hip by 71%. After SLR, they found that resistance to distraction was improved to 66% of the intact state, with a significant increase of 36.8% compared with partial labral resection. These authors also used a graft width of 6 to 7 mm. Lee et al 15 also reported that SLR can restore some labral function. In their study, they performed SLR using ITB or semitendinosus grafts with a mean diameter of 6.6 mm and found that the contact area and pressure were restored to those of the intact state.
Suppauksorn et al, 31 on the other hand, reported that CLR with an ITB allograft resulted in loss of the suction seal in 7 of 8 specimens tested. This study was one of the first to biomechanically analyze CLR, but there are significant differences compared with the present investigation. First, they did not use a saline bath in their analysis. Immersion of the hip joint helps re-create synovial fluid, translating to more realistic data. In addition, the distraction force in the study of Suppauksorn et al was applied manually, which may introduce bias (observer-expectancy effect). To avoid this, we selected a standardized methodology using a hydraulic mechanical testing system. Further, Suppauksorn et al used ITB allografts with a mean width of 5 mm, which, according to our results, may explain why the suction seal was not restored after CLR in their study.
The native labrum is triangular shaped, and therefore its height is not necessarily the same as its width. 24 The contact area between the native labrum and the femoral head depends more on its height than its width. Notwithstanding, a cylindrical shape instead of a triangular one is obtained when performing CLR; hence, the increase in the graft width is a way to compensate the labral acetabular surface over the femoral head (height). In the clinical setting, improvements in patient-reported outcomes have been reported after CLR in primary and revision scenarios by using grafts between 6.5 and 7.5 mm1,7,8,21,28,29,36; however, further studies are necessary to demonstrate the importance of the allograft width in CLR.
As with all cadaveric studies, there are several limitations that should be noted. Labral reconstruction was performed open, which does not represent the current arthroscopic approach applied by the majority of hip surgeons.20,26,32 The cadaveric model used does not fully reproduce in vivo conditions; therefore, we cannot extrapolate the results obtained to the clinical scenario, which may limit clinical applicability. The hip suction seal was evaluated on a hydraulic mechanical testing system, which may not perfectly simulate normal physiological conditions. Even though distraction tests were performed in a saline solution at physiological temperatures, its composition is not identical to that of native synovial fluid. 13 In addition, only 1 position was evaluated for hip distraction, and the capsule and surrounding musculature were dissected completely, removing key anatomic stability structures of the hip. The labrum plays a major role in hip stability (resisting distractive forces) and in evenly distributed compressive loads. 2 The present study focused on distractive forces; hence, conclusions cannot be extrapolated for compression properties after CLR in a cadaveric model. Moreover, the distractive forces applied were supraphysiological. The decision to form 2 groups using 6.5 mm as a cutoff for the allograft width was based on a previous native labral biomechanical study 30 ; however, it remains somewhat arbitrary. The CLR >6.5 mm group did not include grafts with a diameter of 7 mm, which is one of the most common sizes reported being used in clinical practice.27,33 Moreover, in the clinical setting, using ITB grafts with a diameter ≥9 mm may lead to nonanatomic hip reduction with potential hip subluxation. Further, measuring the native labral height at the 9-o’clock position was based on a previously published investigation. 30 The allografts used were frozen ITBs, and results may vary when using other graft options. Finally, this study represents only the time-zero postsurgical state.
Conclusion
In this cadaveric model, CLR using wider ITB allografts (>6.5 mm) restored the distractive force and distance to the suction seal rupture to values comparable with hips with an intact labrum. Wider ITB allografts outperformed narrow ITB allografts, demonstrated by a significantly higher force to rupture the suction seal and increased distraction before the rupture.
Footnotes
Submitted November 5, 2021; accepted April 1, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: Grafts for this study were provided by AlloSource. M.B.B. has received consulting fees from Arthrex, Smith & Nephew, Stryker, and Vericel. S.K. has received a grant from Arthrex and support for education from Smith & Nephew and Micromed. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.